Embed Size (px)
Citation preview

How to Do a Lot With a Little: Surgical Site Infection (SSI) Surveillance
in Ambulatory Surgical Centers (ASCs)Angela Vassallo, MPH, MS, CIC, FAPIC
Clinical Improvement Advisor, Infection PreventionHealth Services Advisory Group (HSAG)
Wednesday, March 21, 2018

Before We Begin
HousekeepingPlease do not put us on hold.
Write any questions into the “chat” box.– Discussion portion is at the end of the presentation.– Participants will be muted until the discussion.
We will email responses to questions to all participants.Recording and the presentation from today’s webinar will be posted on the HSAG website by next week.
2Health Services Advisory Group (HSAG). California ASC Infection Prevention Initiative. Available at: https://www.hsag.com/en/medicare-providers/states-of-service/california/improve-safe-hand-hygiene-and-safe-injection-practices/. Accessed on: March 15, 2018
Introductions
Angela Vassallo, MPH, MS, CIC, FAPICNationally recognized expert in Infection Prevention and lead Infection Preventionist for HSAG’s ASC-Special Innovation Project (ASC-SIP)• Certified in Infection Control (CIC) and Fellow of APIC (FAPIC) • Association for Professionals in Infection Control and Epidemiology (APIC)
– Past-president, CA APIC and Greater LA APIC chapter– Vice-chair, national APIC Communications Committee
• Infectious Disease Association of California (IDAC)– First and only Infection Prevention board member
• LA County Department of Public Health Healthcare-Acquired Infection (HAI) Advisory Committee
– Founding member who represents Infection Preventionists in LA County• Faculty, MPH, MHA, and MS programs
– West Coast University and Providence University• Education
– MPH, University of Texas Health Science Center, School of Public Health, Houston, TX
– MS, Healthcare Management, West Coast University, Los Angeles, CA– BA, International Service, American University, Washington, DC
3
Introductions (cont.)
• Lydia Maldonado, RNDirector of Nursing,Reagan Street Surgery Center
• Shawna May, RNInfection Preventionist,Reagan Street Surgery Center
4

Webinar Objectives
• Discover how to conduct SSI Surveillance in ASCs.
• Describe the 2018 National Healthcare Safety Network (NHSN) criteria for SSIs.
• Examine the bundle components needed to reduce SSIs in ASCs.
5

HSAG is a QIN-QIO
Funded by the Centers for Medicare & Medicaid Services (CMS)
• Medicare Quality Innovation Network–Quality Improvement Organization (QIN-QIO) for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands.
• Largest federal program dedicated to improving health quality at the community level.
• Dedicated to improving healthcare atthe population level.
• Ensures that Medicare beneficiariesget the best quality healthcare.
Department ofHealth & Human
Services
CMS
6
HSAG’s QIN-QIO Territory
7
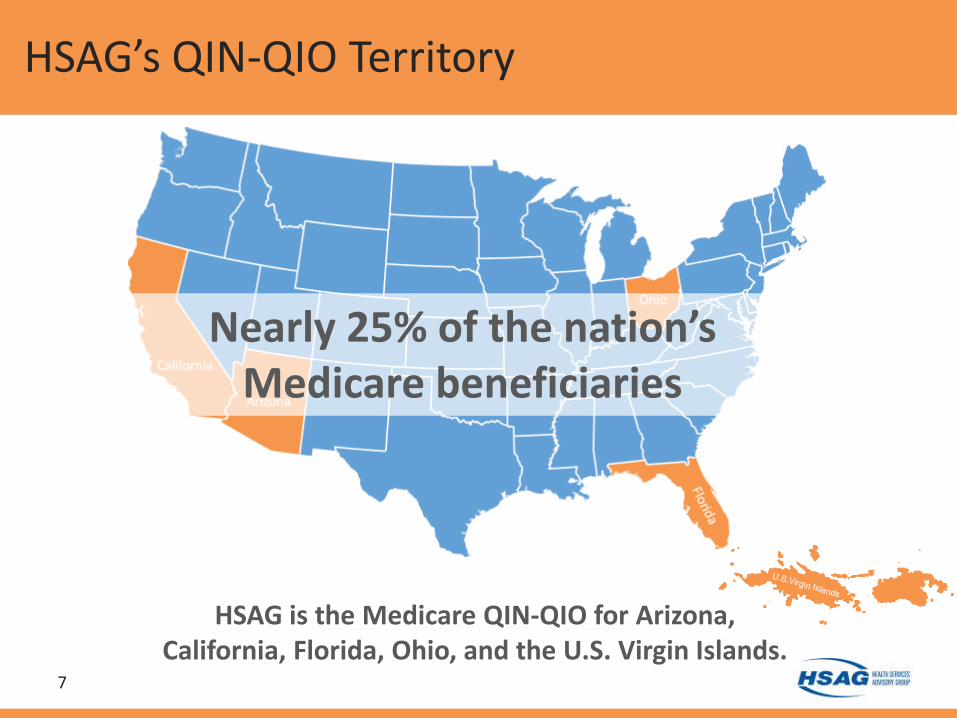
Nearly 25% of the nation’s Medicare beneficiaries
HSAG is the Medicare QIN-QIO for Arizona, California, Florida, Ohio, and the U.S. Virgin Islands.

ASC Special Innovation Project
8

Step One
SSI Surveillance in ASCs
9

Current SSI Surveillance in ASCs
How do ASCs conduct SSI surveillance?• Rely upon sending monthly letters to physicians
and awaiting feedback on SSIs from these letters• Conduct ASC clinic record reviews when possible
infections are identified– This creates limitations as ASC clinic records have
minimal information
• Review any incision & drainage (I&D) cases that come to an ASC
• Implement process measures when and where possible
10

Barriers to SSI Surveillance in ASCs
• No laboratory means no microbiology/wound culture results available.
• Patients are in the ASC for only a short period of time, which makes long-term follow up and clinical record review difficult.
• Patients do not always return if they have problems.– Instead, they go to emergency rooms, hospitals, clinics,
private practices.– ASCs rarely get feedback from outside facilities that see
post-operative (post-op) patients.• Little contact with other facilities creates challenges to
conducting SSI surveillance.
11
It’s difficult to review cases with minimal information!

New Methods for SSI Surveillance in ASCs
• Consider making calls to patients 30–90 days post-op.– Not just calling 24–48 hours post-op
• Build relationships with local hospital infection prevention departments.– Agree to communicate and report possible SSIs
to one another• Get involved with APIC at: https://apic.org/
– 12 APIC chapters in California, spread throughout the state
– CA APIC’s website links to all 12 APIC chapters in California—http://community.apic.org/cacc/home
12

New Methods for SSI Surveillance in ASCs (cont.)
• Attend local APIC chapter meetings– Learn best practices and meet other Infection
Preventionists• Lifelines to call during surveys really help!
– Many chapters host regular conference calls so that you don’t have to leave your facility
• Refer to Centers for Disease Control and Prevention’s (CDC’s) SSI Resources—https://www.cdc.gov/hai/ssi/ssi.html– Use NHSN criteria for SSI surveillance
• Voluntarily report SSI data to NHSN• 6 states currently require ASCs to report SSIs to NHSN
13

Step Two
CDC’s NHSN
14

NHSN Recommendations on SSI Surveillance
Post-discharge surveillance for outpatient operative proceduresshould include reviews of:
• Surgery clinic patient records– Nurse and physician notes
• Surgeon surveys by mail or telephone (“monthly letters”)
• Patient surveys by mail or telephone
15CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

NSHN SSI Criteria
SSI Criteria, 2018: 3 types of SSIs1. Superficial (30 days)2. Deep incisional (30–90 days)3. Organ/space (30–90 days)
“An NHSN Operative Procedure is a procedure that takes place during an operation where at least one incision (including laparoscopic approach and cranial Burr holes) is made through the skin or mucous membrane, or reoperation via an incision that was left open during a prior operative procedure
ANDtakes place in an operating room (OR), C-section room, interventional radiology room, or a cardiac catheterization lab.”
16CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Superficial SSI
Must meet the following criteria:• Date of event for infection occurs within 30 days after
any NHSN operative procedure (where day 1 = the procedure date)
AND• Involves only skin and subcutaneous tissue of the incision
AND…
17CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Superficial SSI (cont.)
Patient has at least one of the following: a) Purulent drainage from the superficial incision.b) Organisms identified from an aseptically-obtained specimen
from the superficial incision or subcutaneous tissue by a culture or non-culture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment (for example, not active surveillance culture/testing [ASC/AST]).
c) Superficial incision that is deliberately opened by a surgeon or other physician and culture or non-culture based testing is not performed.
ANDPatient has at least one of the following signs or symptoms: pain or tenderness, localized swelling, erythema, or heat. d) Diagnosis of a superficial incisional SSI by the surgeon or other
physician.
18CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

SSI Reporting Instructions
The following do not qualify as criteria for meeting the NHSN definition of Superficial SSI: • Diagnosis/treatment of cellulitis (redness/warmth/swelling),
by itself, does not meet criterion “d” for superficial incisional SSI. Conversely, an incision that is draining or that has organisms identified by culture or non-culture based testing is not considered a cellulitis.
• A stitch abscess alone (minimal inflammation and discharge confined to the points of suture penetration).
• A localized stab wound or pin site infection—Such an infection might be considered either a skin or soft tissue (ST) infection, depending on its depth, but not an SSI– Note: A laparoscopic trocar site for an NHSN operative procedure is
not considered a stab wound.
19CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Deep Incisional SSI
Must meet the following criteria: • The date of event for infection occurs within 30 or 90 days after
the NHSN operative procedure (where day 1 = the procedure date) AND
• Involves deep soft tissues of the incision (for example, fascial and muscle layers)
ANDPatient has at least one of the following: • Purulent drainage from the deep incision.• A deep incision that spontaneously dehisces, or is deliberately
opened or aspirated by a surgeon, attending physician or other designee
AND…
20CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Deep Incisional SSI (cont.)
• Organism is identified by a culture or non-culture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment (for example, not active surveillance culture/testing [ASC/AST]) or culture or non-culture based microbiologic testing method is not performed.
ANDPatient has at least one of the following signs or symptoms:• Fever• (>38°C); localized pain or tenderness. A culture or non-culture
based test that has a negative finding does not meet this criterion.
• An abscess or other evidence of infection involving the deep incision that is detected on gross anatomical or histopathologic exam, or imaging test.
21CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Organ/Space SSI
Must meet the following criteria: • Date of event for infection occurs within 30 or 90 days after the
NHSN operative procedure (where day 1 = the procedure date) AND
• Infection involves any part of the body deeper than the fascial/muscle layers, that is opened or manipulated during the operative procedure.
AND…
22CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Organ/Space SSI (cont.)
Patient has at least one of the following: • Purulent drainage from a drain that is placed into the
organ/space(for example, closed suction drainage system, open drain, T-tube drain, CT guided drainage).
• Organisms are identified from fluid or tissue in the organ/space by a culture or non-culture based microbiologic testing method which is performed for purposes of clinical diagnosis or treatment (for example, not active surveillance culture/testing [ASC/AST]).
• An abscess or other evidence of infection involving the organ/space that is detected on gross anatomical or histopathologic exam, or imaging test evidence suggestive of infection.
23CDC. Surgical Site Infection (SSI) Event. Available at: https://www.cdc.gov/nhsn/pdfs/pscmanual/9pscssicurrent.pdf. Accessed on: March 15, 2018

Getting Started with NHSN
Assistance with NHSN• HSAG provides assistance to ASCs
– Enrollment and set-up• NHSN offers training
– Self-paced and interactive
Mary Ellen Wiegand, RN, LHRM, CASC, CNORQuality Improvement SpecialistAmbulatory Surgical Centers, HSAG813.865.3446 | [email protected]
24CDC. National Healthcare Safety Network (NHSN) Training. Available at: https://www.cdc.gov/nhsn/training/newtonhsn.html. Accessed on: March 15, 2018

Step Three
Medicare Fee-for-Service (FFS) Data
25

Possible SSI Data Reports
Medicare FFS Data (part-A and part-B claims)• Claims possibly related to post-op
complications from an ASC– Identified 14 days and 30 days post-op– Codes from post-op visits to diverse locations
• Hospitals, emergency rooms, private practices, and ASCs
26 Owens, P. L., Surgical Site Infections Following Ambulatory Surgery Procedures, JAMA, 2014;311(7):709-716.

Possible SSI Data Reports (cont.)
• Cross-referenced at the infection level– Incision and drainage of the knee after a knee
arthroplasty at an ASC would be included– Incision and drainage of the knee after a
colonoscopy at an ASC would not be included
• Example of codes used‒ Infection and complication, abscess, cellulitis,
incision and drainage, osteomyelitis
27 Owens, P. L., Surgical Site Infections Following Ambulatory Surgery Procedures, JAMA, 2014;311(7):709-716.

Example Possible SSI* Data Reports
28* These are example data reports. Because only claims data are used to identify possible SSIs, caution should be taken when reviewing these results as the level of specificity using claims data may be less than other data sources, such as NHSN criteria for SSIs.

29
Step Four
SSI Reduction

SSI Reduction Bundle
• Hair removal– Clipping not shaving– Not in OR!
• Pre-op skin cleansing– Chlorhexidine gluconate (CHG)
based products• Hand hygiene
– Everyone—even the circulator!• Surgical site skin prep
– Alcohol/CHG based products for extended persistence
• Blood glucose monitoring• Safe injection practices
– Disinfect the tops of med vials– One and Only Campaign
• Antibiotic stewardship– HSAG checklist for ASCs
• Environmental cleaning– Are staff trained?– Is there any monitoring of their
processes?• Instrument sterilization
– Biological indicators (BI), chemical indicators (CI), failure plans?
• High-level disinfection– Pre-cleaning– Is there an annual staff training?
(This is not vendor in-services!)• Post-op patient instructions
– CDC patient handout on SSI reduction at discharge
30Berrios-Torres, S.I. et al, Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surgery, 2017;152(8):784-791.

CDPH Adherence Monitoring Tools
31California Department of Public Health (CDPH). Healthcare-Associated Infections (HAI) Program. Available at: https://www.cdph.ca.gov/Programs/CHCQ/HAI/Pages/MonitoringAdherenceToHCPracticesThatPreventInfection.aspx. Accessed on: March 15, 2018

CDC Patient Education on SSIs
32 CDC. Surgical Site Infections FAQs. Available at: https://www.cdc.gov/hai/pdfs/ssi/ssi_tagged.pdf. Accessed on: March 15, 2018.

HSAG Antimicrobial Stewardship Checklist for ASCs
33Health Services Advisory Group (HSAG). Antimicrobial Stewardship Checklist for Ambulatory Surgery Centers (ASCs). Available at: https://www.hsag.com/contentassets/98d1e68f70bc4240832eb3545b6050f6/rbrndcdchsagaschecklistforascs.pdf. Accessed on: March 15, 2018.

Spotlight: Reagan Street Surgery Center
34

Reagan Street Surgery Center
35Reagan Street Surgery Center, 10904 Reagan St, Los Alamitos, CA 90720.http://www.reaganstreetsurgerycenter.com/

Reagan Street Surgery Center (cont.)
• Demographics– Located in Los Alamitos, about 30 miles south of
Los Angeles, just east of Long Beach– Opened in 2005– Affiliated with United Surgical Partners
International (USPI)– Accreditation Association for Ambulatory
Healthcare, Inc. (AAAHC) accredited– CMS certified– HSAG ASC project
36USPI. USPI Home Page. Available at: http://www.uspi.com/. Accessed on: March 16, 2018.AAAHC. AAAHC Home Page. Available at: http://www.aaahc.org/. Accessed on: March 16, 2018.

Reagan Street Surgery Center (cont.)
• Service lines– Gastroenterology, eye, urology, orthopedics, pain,
gynecology, and general surgery– 450 patients per month
• Staff members– 40 employees– 100 surgeons– 14 anesthesiologists
37USPI. USPI Home Page. Available at: http://www.uspi.com/. Accessed on: March 16, 2018.AAAHC. AAAHC Home Page. Available at: http://www.aaahc.org/. Accessed on: March 16, 2018.
Spotlight: Reagan Street Surgery Center
38 Lydia Maldonado, RN, Director of Nursing and Shawna May, RN, Infection Preventionist

Spotlight: Reagan Street Surgery Center (cont.)
SSI surveillance process• Ongoing conversations with medical doctors (MDs)
– Monthly SSI surveillance letters in MD file folders• MDs must review all items in their files• MDs must sign off on the letter and discuss potential cases with Shawna• NHSN SSI criteria attached to each MD’s file and to each monthly letter
– On-boarding for new MDs includes education on NHSN SSI criteria
• Patient education– CDC’s frequently asked questions on SSIs with discharge papers– Letters or emails for 30–90 day follow up– One Medical Passport questions about possible SSIs
39

Spotlight: Reagan Street Surgery Center (cont.)
Infection Prevention Performance Improvement– Automated thermometers: 24/7 monitoring– Challenge pack with every sterilizer load
• Not just implantable device loads or once a day
– Surgical attire: jackets must be worn by everyone
– High-level disinfection: testing the test strips and the solution
– Cleaning process for radiology vests
40

Thank You!
• Reagan Street Surgery Center– Lydia Maldonado, RN, and Shawna May, RN
• California Ambulatory Surgery Association (CASA)– Beth LaBouyer, RN, CNOR, CASC, Executive Director
• AmSurg– Kathy Wilson, VP, Quality
• California APIC– Lisa Kilgore, 2018 President
41

Thank You! (cont.)
• California Department of Public Health (CDPH)Healthcare Acquired Infections (HAI) program– Vicki Keller, RN, MPH, HAI Liaison Program Coordinator
• Los Angeles County Department of Public Health(LACDPH) Acute Communicable Disease Control– Kelsey Oyong, MPH, Epidemiologist
• ASC Quality Collaboration (ASC QC)– Donna Slosburg, BSN, LHRM, CASC, Executive Director
• NHSN/CDC– Daniel Pollock, MD, Surveillance Branch Chief,
Division of Healthcare Quality Promotion
42

References
• Health Services Advisory Group (HSAG). California ASC Infection Prevention Initiative. Available at: https://www.hsag.com/en/medicare-providers/states-of-service/california/improve-safe-hand-hygiene-and-safe-injection-practices/. Accessed on: March 15, 2018
• CDC. Healthcare-associated Infections. Available at: https://www.cdc.gov/hai/ssi/ssi.html. Accessed on: March 15, 2018
• CDC. NHSN. Available at: https://www.cdc.gov/nhsn/index.html. Accessed on: March 15, 2018
• CDC. NHSN Tracking Infections in ASCs. Available at: https://www.cdc.gov/nhsn/ambulatory-surgery/index.html. Accessed on: March 15, 2018.
• Owens, P. L., Surgical Site Infections Following Ambulatory Surgery Procedures, JAMA, 2014;311(7):709-716.
• Berrios-Torres, S.I. et al, Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surgery, 2017;152(8):784-791.
• CDPH. Healthcare-Associated Infections (HAI) Program. Available at: https://www.cdph.ca.gov/Programs/CHCQ/HAI/Pages/MonitoringAdherenceToHCPracticesThatPreventInfection.aspx. Accessed on: March 15, 2018.
43

References (cont.)
• APIC. Spreading Knowledge. Preventing Infection. Available at: https://apic.org/. Accessed on: March 16, 2018.
• California APIC Coordinating Council. California APIC Home Page. Available at: http://community.apic.org/cacc/home. Accessed on: March 16, 2018.
• CDC. Resources for Users New to NHSN. Available at: https://www.cdc.gov/nhsn/training/newtonhsn.html. Accessed on: March 16, 2018.
• CDC. FAQs about Surgical Site Infections. Available at: https://www.cdc.gov/hai/pdfs/ssi/ssi_tagged.pdf. Accessed on: March 16, 2018.
• APIC. Help Prevent Infections for Patients and Their Visitors. Available at: http://professionals.site.apic.org/files/2018/02/SHEA-Brochure_on_healthcare_associated_infections_English.pdf. Accessed on: March 16, 2018.
• Reagan Street Surgery Center. Every Day Giving Excellence Home Page. Available at: http://www.reaganstreetsurgerycenter.com/. Accessed on: March 16, 2018.
• USPI. USPI Home Page. Available at: http://www.uspi.com/. Accessed on: March 16, 2018.
• AAAHC. AAAHC Home Page. Available at: http://www.aaahc.org/. Accessed on: March 16, 2018.
44

Angela Vassallo, MPH, MS, CIC, FAPICClinical Improvement Advisor, Infection Prevention
Health Services Advisory Group (HSAG)480.287.3655 | [email protected]
45
Please complete the evaluation at:
https://goo.gl/qy7dNXIf you registered online for this event, you will also receive the link via email.
A recording of today’s session will be available at:www.hsag.com/events
(Click on today’s event date to access the recording link)
46

This material was prepared by Health Services Advisory Group, the Medicare Quality Improvement Organization for California, under contract with the Centers for Medicare & Medicaid Services
(CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily reflect CMS policy. Publication No. CA-11SOW-ASC-03142018-01









![The Little [Marketing] Engine that Could: How to Do a Lot with a Little - By Cathy Thomson](https://img.pdfslide.us/doc/110x75/54528bc1af795963148b97da/the-little-marketing-engine-that-could-how-to-do-a-lot-with-a-little-by-cathy-thomson.jpg)



















