Embed Size (px)
Citation preview

How should we treat apraxia of speech?
Rosemary Varley
Language & Communication, UCL

Speech learning/intervention• How much is our philosophy of therapy influenced by general culture
of education (and language teaching in particular)?
• Teacher/therapist instructs by sharing declarative/conscious/explicit knowledge of [X] with learner.
• Therapists knows about articulatory phonetics; this knowledge shared with patient; patient acquires knowledge & relearns speech control.• Microstructural (also articulatory-kinematic or sound production therapy).
• Therapy rebuilds segmental plans & provides practice in combining gestures to form cohesive syllables:
• Typically, ‘easy’ sounds combined with set of maximally different vowels.

Evidence-Base for Microstructural Therapy
• Wambaugh, et al. (2006). J. Medical Speech-Language Pathology. Treatment Guidelines for Acquired Apraxia of Speech: A Synthesis and Evaluation of the Evidence• Majority of research on microstructural/articulatory therapies• Outcomes: Learning of targeted gesture/syllable but poor
generalisation of learning• If therapy uses nonsense syllables, therapy might lead to little
functional gain in speech.
• Cochrane Review (2009): “No evidence was found for the treatment of AOS.”
• Therapists view as hard-to-treat condition.
3

Concerns about being explicit
• Speakers have explicit knowledge about some aspects of language (e.g. vocabulary), but in other areas knowledge is procedural & implicit (syntax, speech control), Ullman (2001).
• Articulatory therapy based on premise that declarative knowledge converted to procedural knowledge.
• Internal focus of attention (e.g. directing attention to position of muscles) leads to less automaticity in complex motor skill learning that an external focus (Wulf, et al., 2001. Quart. J. Expt. Psych.).
• Ballard et al. (2011). Motor Control. Poorer retention of novel speech movement in healthy learners with kinematic feedback on location of tongue (EPG), than those without feedback.

Microstructural Therapy
Whole wordTherapy
Sub-components of movements
Whole words/utterances
Isolated motor processinge.g. non-speech gestures;
nonsense syllables
Connectivity: sensory-perceptual; linguistic
Declarative/conscious knowledge
Procedural knowledge
Errorful learning Errorless learning
5

Therapy Dose• Ample evidence that low-dose therapy ineffective in achieving
significant behavioural gains (e.g., Pulvermüller, et al. 2001; Bhogal, et al.,2003; Bowen et al., 2012; Leff & Howard, 2012).
• Challenge of achieving high-dose intervention in cost-effective way.
• Use of computer self-managed therapy model.
6

Example Interfaces

Intervention Study
• 51 participants with chronic AOS+
(min. 5 months post-onset).
• Loaned laptop. Advised to use intervention regularly for short periods (‘little and often’). Supported by visiting T in early stages. Program records user interactions.
• 6-week intervention period
• Study design: Cross-over• Participants complete two ‘interventions’: active (speech) vs. sham (visual)• 4-week rest phase between interventions• Randomised to two groups: speech-first vs. sham-first
8

Tx 2 (6 weeks)
Tx 1 (6 weeks)
Baselines (x2) &
Randomisation
Speech
Sham
Sham
Speech
Re-test
Maintenance (8 weeks)
N = 51
N = 44

Visual Sham Intervention
10

Outcome Measures
11
• Speech Production repetition & naming single words; plus spontaneous speech samples at baseline & maintenance
• 3 word sets (35 words each)
• Untreated behaviours• Written word-picture matching (PALPA 48, Kay et al., 1992)• Spoken sentence-picture matching (CAT, Swinburn et al., 2004).
• Cost-effectiveness assessment
Treated Phonetically-matched Untreated
Non-matchedUntreated
Dog Door Game
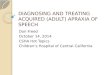
Generalisation to Un-Tx Words
Tx: ‘Dog’ P-match ‘Door’ U-tx.‘Game’Significant
improvementz -3.825 p<.0001
Significant improvement
z -2.884 p<.004
No change
Whiteside et al (2012) Neuropsychological Rehabilitation 12
B1
Pho
n M
atch
B2
Pho
n M
atch
PTx
Spe
ech
Pho
n M
atch
PTx
Sha
m P
hon
Mat
ch
Mai
nten
ance
Pho
n M
atch
0.00
5.00
10.00
15.00
20.00
'Flu
ent'
scor
e
*
B1
Tre
ated
B2
Tre
ated
PTX
Spe
ech
Tre
ated
PTx
Sha
m T
reat
ed
Mai
nten
ance
Tre
ated
0.00
5.00
10.00
15.00
20.00
'Flu
ent'
sco
re
*
B1
Fre
q M
atch
B2
Fre
q M
atch
PTx
Spe
ech
Fre
q M
atch
PTx
Sha
m F
req
Mat
ch
Mai
nten
ance
Fre
q M
atch
0.00
5.00
10.00
15.00
20.00
'Flu
ent'
sco
re
ns

Compliance with ‘little and often recommendation’
•Program use (hours:mins in 42 day period)• Speech program: 3:32 – 50:29; M=16:48• Sham program: 0:41 – 50:09; M=14:54•No significant difference between
sham/speech-first groups in level of use of either program
13

Summary & Conclusions
• Intervention study with large sample of patients, administered single treatment protocol.
• Self-administered, IT-based therapy may represent cost-effective way of resolving dosage problem.
• Word-level therapy for AOS was effective.
• Effects most evident on treated word forms.
• Gains on treated words maintained.
• Evidence of generalisation to phonetically-similar untreated words (although no wholescale generalisation).
14

CollaboratorsSandra Whiteside & Patricia Cowell
(University of Sheffield)
Research team
Lucy Dyson; Lesley Inglis; Abigail Roper: Tracey Young
Additional collaborators
SLTs across South Yorkshire, & in particular Rotherham NHS
Funders
The Health Foundation; BUPA Foundation: University of Sheffield/HEIF4 knowledge transfer grants
15

Conflict of Interest Statement
Sword Software
• Software program is commercially available
• ‘Inventors’ Varley, Whiteside & Cookmartin receive share of royalties from sales
16

Thank youVarley, R. A. & Whiteside, S. P. 2001. What is the underlying impairment in acquired apraxia of speech? Aphasiology, 15, 39-49.
Varley, R. 2011. Rethinking aphasia therapy: a neuroscience perspective. International Journal of Speech-Language Pathology, 13, 1, 11-20.
Whiteside, S.P., Inglis, A.L., Dyson, L., Roper, A., Harbottle, A., Ryder, J., Cowell, P.E., & Varley, R.A. 2012. Error reduction therapy in reducing struggle and grope behaviours in apraxia of speech. Neuropsychological Rehabilitation, 22, 267-294.
17

Input 1• Computer models errorless spoken word-picture matching
Input 2• Computer models errorless spoken-written word matching
Input 3• Interactive: Participant performs spoken word-picture matching task
Input 4• Interactive: Participant performs spoken-written word matching task
Input 5• Computer models errorless spoken lexical decision task
Input 6• Interactive: Participant performs spoken lexical decision task
http://www.propeller.net/sword.htm

Output 1• Observe video of speaker saying target word
Output 2• Imagined production of words
Output 3• Immediate repetition of words
Output 4• Delayed repetition
Output 5• Repetition with audio-recording & playback
Output 6• Practice of target words in sentences
Output 7• Production of word in isolation, with cue support if needed