Embed Size (px)
Citation preview
How InterQual® Software Improves the Financial Health of the Critical Access Hospital
Eboney White
Sr. Product Consultant
Dena Heyman
Sr. Sales Executive
June 15, 2015
2
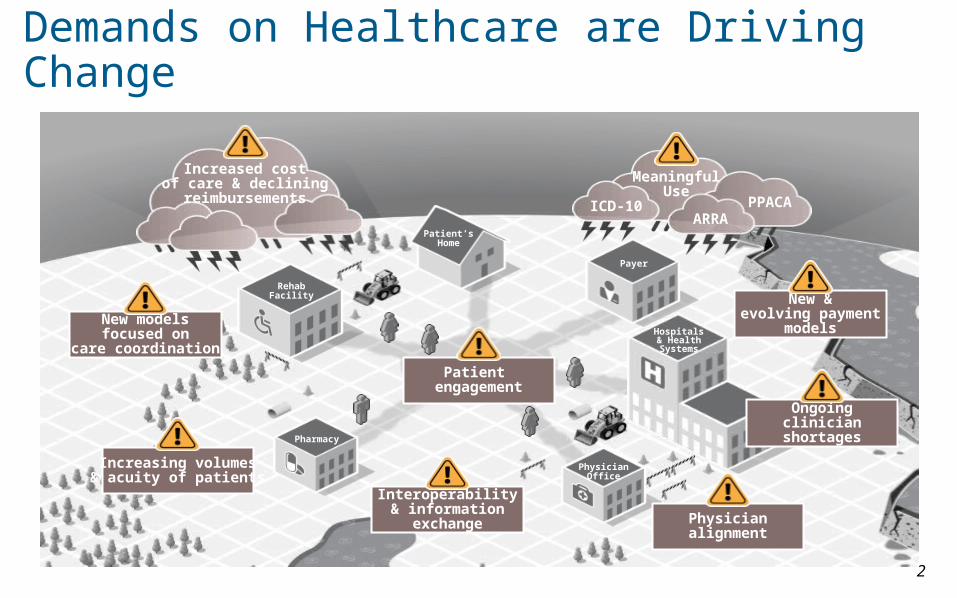
Demands on Healthcare are Driving Change
RehabFacility
Patient’sHome
Payer
Hospitals& HealthSystems
PhysicianOffice
Pharmacy
Increased costof care & declining
reimbursements
MeaningfulUse
ICD-10ARRA
PPACA
New modelsfocused on
care coordination
Increasing volumes& acuity of patients
Interoperability& information
exchange Physicianalignment
Ongoingclinician
shortages
New &evolving payment
models
Patient engagement

Hospital CFOs: Top 10 Challenges
Med
icare
redu
ctio
ns
Declin
ing
or fl
at IP
vol
umes
Med
icaid
redu
ctio
ns
Incr
easin
g op
erat
ing
cost
s
Bad d
ebt
Payer
neg
otia
tions
RAC/oth
er a
udits
Other
Reven
ue c
ycle
Inve
stm
ents
/cap
ital
0
10
20
30
40
Source: B. Herman, “The State of Healthcare Finance: 9 Major Survey Findings From Hospital CFOs,” Becker’s Hospital Review, February 6, 2014
No. of Responses
InterQual® and the Critical Access Hospital
InterQual® Clinical Content1. Gold Standard Evidenced Based Medicine 2. Influence Claims Submission Patterns and Outcomes3. Request Reimbursement and File Appeals with Confidence
CareEnhance Review Manager Enterprise4. Increase Revenue Stream5. Better Financial Support Documentation6. Reduce Bad Debt7. Streamline Case Review for Denials8. Gain insight for Process Improvement and Financial Gain
5Copyright © 2015 McKesson Corporation and/or one of its subsidiaries. Confidential and proprietary.
Our Community
6
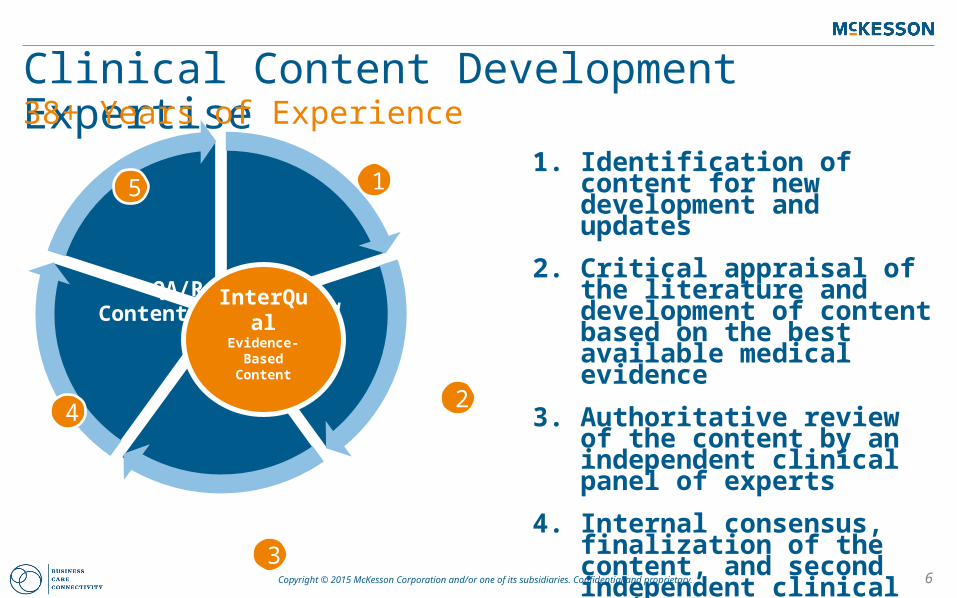
Clinical Content Development Expertise38+ Years of Experience
Content Development
Critical Apprai
sal
Authoritative Review
Content
Validation
QA/Release
InterQualEvidence-Based
Content
1
2
3
4
51. Identification of content for new
development and updates
2. Critical appraisal of the literature and development of content based on the best available medical evidence
3. Authoritative review of the content by an independent clinical panel of experts
4. Internal consensus, finalization of the content, and second independent clinical review
5. Quality assurance review of the content and software prior to general availability
Copyright © 2015 McKesson Corporation and/or one of its subsidiaries. Confidential and proprietary.

7Copyright © 2015 McKesson Corporation and/or one of its subsidiaries. Confidential and proprietary.
InterQual Evidence-Based Content
• Procedures
• Imaging
• Durable Med Equip
• Molecular Diagnostics
• Specialty Rx Non-Onc
• Specialty Rx Onc
• Specialty Referral
• SIMplus™
• Acute Adult
• Acute Pediatric
• Long Term Acute Care
• Acute Rehabilitation
• SAC / SNF
• Home Care
• Outpatient Rehab and Chiropractic
• Geriatric Psychiatry
• Adult Psychiatry
• Adolescent Psychiatry
• Child Psychiatry• Substance Use
Disorders and Dual Diagnosis
• Residential and Community Based Treatment
• Coordinated Care Content
Care Planning Level of Care Behavioral Health Care Management
Spanning the Continuum of Care
Pre-AuthorizationAcute and Post
Acute Settings of Care
Behavioral HealthComplex Case and
Disease Management

8
Case Study
42-year-old male presenting to ED for dull RUQ pain
Should he be admitted? Should he have an open or laparoscopic cholecystectomy ($9,768)? Does he get
admitted for observation ($1741) or acute ($5,142) while we wait for imaging?
Re-admitted to the hospital 8 days after elective laparoscopic cholecystectomy for gallstones because
of dull right upper quadrant (RUQ) pain that increased with meals. Physical examination disclosed no
abnormalities except for mild RUQ tenderness and fever (100.0 °F, 37 °C).
Should we do an US ($154)? CT ($536)? MRI ($546)? HIDA Scan ($767)?
What is the cause of multiple inconclusive diagnostics?
Are we going to get reimbursed? Are we going to get denied?
The Case for Clinical Decision Support
*All Prices from Healthcare Bluebook.
9
On Average, Medicare Paid Nearly Three Times More for a Short Inpatient Stay Than an Observation Stay and
Beneficiaries Paid Almost Two Times More
In total, Medicare paid $5.9 billion for short inpatient stays, an average of $5,142 per stay.
In contrast, it paid $2.6 billion for observation stays, an average of $1,741 per stay.
Clinical Decision Support Helps to Get it Right the First Time
Source: Memorandum Report: Hospitals' Use of Observation Stays and Short Inpatient Stays for Medicare Beneficiaries , OEI-02-12-00040

10
Demonstration
11
Q & A
12Copyright © 2015 McKesson Corporation and/or one of its subsidiaries. Confidential and proprietary.
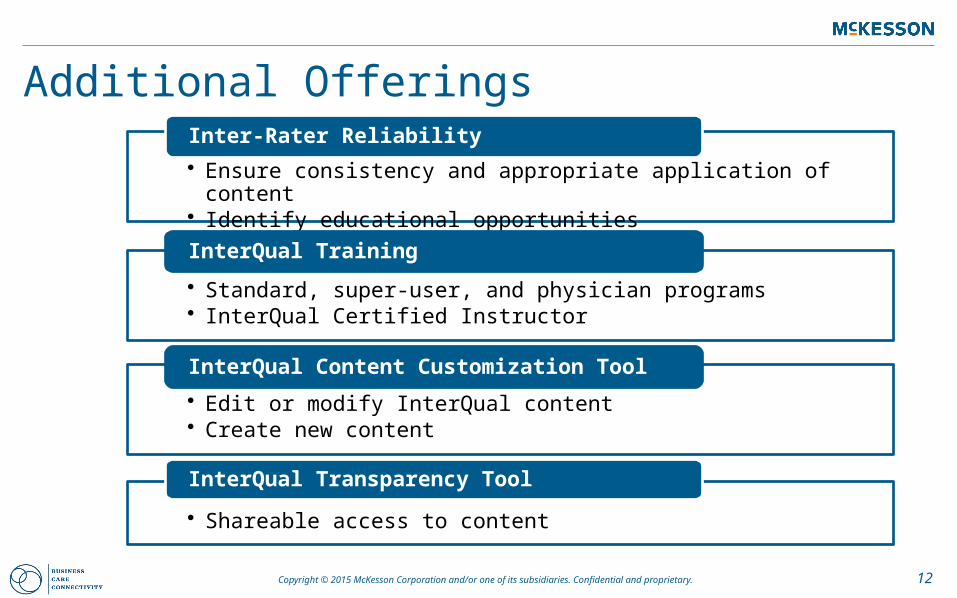
Additional Offerings
• Ensure consistency and appropriate application of content• Identify educational opportunities
Inter-Rater Reliability
• Standard, super-user, and physician programs• InterQual Certified Instructor
InterQual Training
• Edit or modify InterQual content• Create new content
InterQual Content Customization Tool
• Shareable access to content
InterQual Transparency Tool
13Copyright © 2015 McKesson Corporation and/or one of its subsidiaries. Confidential and proprietary.
Technology OptionsSimple to Robust
• InterQual® Mobile
• IQ View
• IQ Online• CareEnhance ®
Review Manager
• Clear Coverage™
View Only Interactive Workflow Auto Authorization









![Modeling and Analysis of Induction Machines under Broken ... · 21 22 2 2 31 32 3 3 sr sr sr n sr e T sr rs sr sr sr n sr e ... Therefore the resistance matrix [R r]is a symmetric(n+1)](https://img.pdfslide.us/doc/110x75/5e83e33adae9df101c14911a/modeling-and-analysis-of-induction-machines-under-broken-21-22-2-2-31-32-3-3.jpg)



















