Embed Size (px)
DESCRIPTION
c b
Citation preview

How I do it.
P. Ronan O’Connell, MD, FRCSI
Mater Misericordiae Hospital,
Dublin, Ireland
and
Angelo Stuto, MD
Ospedale ‘s Maria degli Angeli’
Pordenone, Italy
Learning Objectives
1) Patient selection and preparation for PPH
2) Technique of performing PPH
3) Key points to avoid mishaps

Background
The great majority of patients who present with anorectal symptoms attribute their
symptoms to hemorrhoids. Therefore a careful clinical history and proctological
examination is needed to identify those patients with hemorrhoidal disease most likely
to benefit from hemorrhoidectomy.
The etiology of hemorroidal disease is uncertain and the subject of several
hypotheses. Thompson et al have shown that hemorroidal cushions are part of normal
anatomy (1). Fluctuations in the volume of the hemorrhoidal cushions may parallel
changes in intra abdominal pressure and play a role in preventing leakage of stool
during periods of increased intra rectal pressure. Abnormal enlargement of the
hemorrhoidal cushions may occur with constipation, chronic straining at stool and in
the presence of raised intra abdominal pressure, e.g. pregnancy. In these situations
venous distension leads to hemorrhoidal enlargement, mucosal thinning, stretching of
the hemorroidal suspensory ligaments resulting in bleeding and prolapse.
Conventional hemorrhoidectomy, either by open Milligan-Morgan or the closed
Ferguson technique, is designed to excise all potentially symptomatic hemorrhoidal
tissue. In doing so both external skin tags and internal hemorrhoids are excised,
including part of the highly sensate anoderm below the dentate line. Postoperative
pain is a frequent and often prolonged problem. Recent studies have shown that
perioperative laxative (2) and antibiotic (3) use can reduce the severity of
postoperative pain, nevertheless postoperative pain is problematic.

The procedure for prolapse and hemorrhoids originally developed by Dr Antonio
Longo, represents a radical alternative in surgical treatment of hemorrhoids (4). The
object is not to excise the haemorrhoids but to reposition the prolapsed distal anorectal
mucosa, including the hemorrhoidal cushions, to their original anatomic site by the
excision and stapling of a cuff of redundant distal rectal mucosa. In doing so the blood
flow to the hemorroidal cushions may be reduced. To date six randomised clinical
trials attest to the efficacy of the procedure, reduced postoperative pain and earlier
return to work (Table 1 refs 5 – 10) .
Technique
Patient Selection:
The PPH operation is suitable for patients with Grade III or Grade IV hemorrhoids
and selected patients with symptomatic rectal mucosal prolapse. The patient must be
suitable for either general or regional anaesthesia. Patients with large external
hemorrhoids or skin tags must know that these will not be excised as part of the
operation but that most reduce in size in the weeks following surgery. Occasionally
later excision of residual tags maybe required. The internal hemorrhoidal component
should be reducible under anaesthetic. The final decision concerning which
operative technique to be used (PPH or conventional) must be made in the
operating room. Informed consent of the potential risks, benefits and alternative
treatments must be provided. Patient information leaflets are helpful.

Patient Preparation:
There is evidence that perioperative use of lactulose reduces post-operative pain in
patients undergoing conventional hemorrhoidectomy (2). No data exist concerning
use in stapled hemorrhoidectomy but until proven otherwise it would seem reasonable
practice to recommend use in patients undergoing PPH. A more persuasive argument
can be made for use of perioperative metronidazole (3). Again a randomised clinical
trail has shown benefit in open hemorrhoidectomy, however pelvic sepsis has been
reported as a complication of stapled hemorrhoidectomy (11). It is the authors’
practice to use a cleaning enema on the morning of operation.
Patient Positioning:
The PPH operation may be performed in either the prone jack-knife or lithotomy
positions depending on surgeon preference and patient physique. In the lithotomy
position it is important that the hips are fully flexed to expose the entire perineum.
This position has the advantage in women of facilitating vaginal examination during
the operation. This is important to prevent accidental inclusion of the posterior vaginal
wall in the staple line. Skin preparation and draping is standard. A gauze swab can
usefully be inserted into the lower rectum and withdrawn to show the extent of
hemorrhoidal and mucosal prolapse.

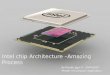
Step 1: CAD insertion
Four quadrant nylon sutures are inserted at the anal verge, cut long and held with
hemostat forceps. Traction on these sutures facilitates insertion of the Circular
Anal Dilator (CAD) and obturator (Ethicon Endosurgery) . The obturator is
inserted first without the circular anal dilator then withdrawn and reinserted with the
circular anal dilator. The obturator is then removed. Full insertion of the dilator is
important. The nylon sutures are now tied to hold the dilator in place. The top of the
hemorrhoidal columns and the lower rectal mucosa should be visible (Fig 1)
Figure 1: CAD inserted in anal canal
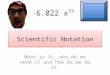
Step 2: Purse string
The purse string suture in next inserted. A 2/0 polypropylene suture on a 30mm round
bodied needle is suitable. Great care must be exercised to position the suture
correctly 2 cm above the top of the hemorrhoidal columns. This is a more reliable
landmark as the height of the hemorrhoidal columns is variable and the dentate line
may not be clearly visible. The object is not to include the hemorrhoidal tissue itself,

rather a cuff of rectal mucosa directly above the hemorrhoidal complex. The suture is
mucosal and submucosal and should not include rectal muscularis propria (Fig 2). The
operator must ensure a continuous mucosal purse string and avoid gaps that might
later lead to bridges of stapled mucosa. In women a digital vaginal examination is
performed to ensure the purse string has not tethered the posterior vaginal wall.
It is important not to pull the purse string closed while checking its position as this
may make insertion of the stapler more difficult.
Figure 2: Insertion of purse
string suture

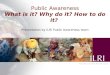
Step 3: Stapler insertion
A suitable circular stapling instrument (PPH 33mm, Ethicon Endosurgery) is opened
to its full extent and inserted into the anal canal ensuring the head is positioned above
the purse string. The purse string is then tied with a single throw and the ends pulled
through the holes in the stapler head using the suture-threading instrument (Fig 3).
Figure 3: Tying the
purse string

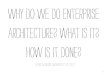
Step 4: Stapler Closure
The suture ends may then be held or tied with a double throw to allow easy traction on
the purse string. The head is then closed to its fullest extent by rotating the closure
mechanism on the end of the shaft in a clockwise direction (Fig 4). It is important to
ensure proper alignment of the instrument in the axis of the anal canal. Using the
PPH 33mm instrument, closure is confirmed by the presence of the red position
marker within the green firing zone on the handle of the instrument. Care is taken in
females that the posterior vaginal wall is not included within the head of the
instrument.
Figure 4: Stapler closure

Step 4: Firing the Stapler
The stapler is fired by releasing the safety mechanism and closing the handles in a
single motion. The purse string suture is not divided as it is during anterior resection
because the suture remains within the instrument head and the ends are within the
shaft. Many surgeons prefer to keep the instrument fully closed for 30 seconds to
improve hemostasis and to allow staple formation.
Step 5: Removing the Stapler
The instrument is removed by opening the head and rotating the closure mechanism
one half turn in an anticlockwise direction. A common error is to open the stapler
head too widely at this point, which may trap mucosa within the opened instrument
head. This makes removal difficult and can damage the anastomosis. A gauze swab
should be inserted into the anal canal to facilitate hemostasis while excised doughnut
of mucosa is removed from the instrument head and sent for histological examination.
The CAD should not be removed with the stapling instrument as this facilitates
checking the staple line for bleeding.
Step 6: Checking the Staple Line
The staple line is checked for bleeding by reinsertion of the proctoscope. Hemostasis
is confirmed in each quadrant. Bleeding points should be under sewn using a 3/0
absorbable suture.

On completion of the operation it can be seen that a hemorrhoidectomy has not
actually been performed, instead the rectal mucosal prolapse has been excised and the
hemorrhoidal cushions repositioned within the anal canal. The operation is completed
by insertion of a degradable sponge dressing.
Step 7: Post operative Care
Post-operative analgesia in the form of a non-steroidal anti-inflammatory drug is
appropriate (the authors favour tenoxicam or diclofenac). Lactulose 30ml up to three
times daily and metronidazole are continued orally for five days. Patients may be
discharged on the evening of or day following operation. Urinary retention is an
occasional problem in males, who should be discouraged from drinking excess fluids
on the evening of operation. Patients should be warned that passage of small amounts
of blood is common in the days following operation. Patients should be told to contact
their surgeon if there is increasing anorectal pain, fever or impaction of feces as these
symptoms may indicate perineal infection. Patients should be encouraged to resume
normal daily activities as soon as possible.

Table 1: Results of randomised clinical trials of PPH versus conventional
hemorrhoidectomy No pain hospital return to
patients stay normal activity Mehigan et al 5 40 less same sooner Rowsell et al 6 22 less shorter sooner Ho et al 7 119 less same sooner Ganio et al 8 100 less shorter sooner Boccasanta et al9 80 less shorter sooner Shalaby & Desoky10 200 less shorter sooner

References:
1. Thompson WHF. The nature of haemorrhoids. Br J Surg, 1975; 62:542-5
2. London NJ, Bramley PD, Windle R. Effect of four days of preoperative
lactulose on posthaemorrhoidectomy pain: results of placebo controlled trial.
BMJ 1987; 295:363-4
3. Carapeti EA, Kamm MA, McDonald PJ, Phillips RK. Double –blind
randomised controlled trial of effect of metronidazole on pain after day-case
haemorrhoidectomy Lancet 1998; 351: 169-72.
4. Longo A. Treatment of haemorrhoidal disease by reduction of mucosa and
haemorrhoidal prolapse with a circular suturing device: a new procedure.
Proceedings of the 6th World Congress of Endoscopic Surgery, Rome, 1998
5. Mehigan BJ, Monson JRT, Hartley JE. Stapling procedure for haemorrhoids
versus Milligan-Morgan haemorrhoidectomy: randomised controlled trial.
Lancet 2000; 355: 782-5
6. Rowsell M, Bello M, Hemmingway DM. Circumferential mucosectomy
(stapled haemorrhoidectomy) versus conventional haemorrhoidectomy:
randomised controlled trial. Lancet, 2000; 355:779-81
7. HoY-H, Cheong WK, Tsang C, Ho J, Eu KW, Tang CL et al. Stapled
hemorrhoidectomy – cost effectiveness. Randomized controlled trial including

incontinence scoring anal manometry and endoanal ultrasound assessments at
up to three months. Dis Colon Rect, 2000; 43: 1666-75
8. Ganio E, Altomare DF, Gabrielli F, Milito G, Canuti S. Prospective
randomised multi-centre trial comparing stapled with open
haemorrhoidectomy. Br J Surg, 2001; 88: 669-674
9. Shalaby R, Desoky A. Randomised clinical trial of stapled versus Milligan-
Morgan haemorrhoidectomy. Br J Surg, 2001; 88: 1049-53
10. Boccasanta P, Capretti PG, Venturi M, Cioffi U, De Simone M, Salamina G et
al. Randomised controlled trial between stapled circumferential mucosectomy
and conventional circular hemorrhoidectomy in advanced hemorrhoids with
external mucosal prolapse. Am J Surg, 2001; 182:64-8
11. Molloy RG, Kingsmore D. Life threatening pelvic sepsis after stapled
haemorrhoidectomy Lancet, 2000; 355:810
Acknowledgement:
The video to accompany this text was produced with the technical assistance of
Johnson and Johnson and Ethicon Endosurgery, Europe. The figures are reproduced
from the video with permission of Ethicon Endosurgery, Europe.