Embed Size (px)
Citation preview

Atrial Arrhythmia Detection, Prevention and t ial yt ia etectio , eve tio a dTherapy AlgorithmHow Do They Work?y
Muhammad MunawarDepartment of Cardiology and Vascular Medicine, Faculty
of Medicine, University of IndonesiaJakarta, Indonesia

• Why atrial arrhythmia (AF) is important in pacemaker patientsimportant in pacemaker patients
• Atrial arrhythmias (AF) supression y ( ) pworkCli i l i l• Clinical trials

Why atrial fibrillation is important in pacemaker patientpacemaker patient
• AF increase morbidity• StrokeStroke• Heart failure
T h di i d d di th• Tachycardia induced cardiomyopathy• AF increase mortality

Risks of Atrial FibrillationRisks of Atrial Fibrillation
• Stroke• Patients with AF are 5 times more likely toPatients with AF are 5 times more likely to
have a stroke than the general population• Cause of 75 000 cases of stroke annually• Cause of 75,000 cases of stroke annually • 23% of all strokes in the U.S.
SJM CRMD RESEARCH BRUSSELS, BELGIUM
(First Call Research Network on 01-OCT-98) and NationsBanc Montgomery Securities

Risks of Atrial FibrillationRisks of Atrial Fibrillation
• Long-term Mortality Rates Framingham Study61.5% 57.6%
60%
70%
Long term Mortality Rates Framingham Study
50%
60%
30.0%20.9%30%
40%
10%
20%
0%Men Women
No AF
Benjamin EJ et al. Circulation 1998; 98: 946-52.
No AFAF Present
Atrial arrhythmias (AF) suppression work

H th iH th iHypothesis Hypothesis
• Suppression of paroxysmal and possibly persistent AF can be achieved by stimulation at one or moreAF can be achieved by stimulation at one or more sites using a variety of overdrive or PAC responsive algorithmsresponsive algorithms.
• Proposed mechanism(s)Proposed mechanism(s)• Reduced dispersion of refractoriness• Improved atrial homogeneityp g y• Reduction in triggers

Options to Stabilize Options to Stabilize S AFS AFor Suppress AFor Suppress AF
• Alternate sites of stimulationBi t i l ti l ti• Bi-atrial stimulation
• Dual-site atrial stimulation• Bachmann’s bundle or interatrial septump• Low septal pacing• Coronary sinus
• Overdrive algorithms• Elevated base rate• PAC responsive algorithm (ELA)• Consistent Atrial Pacing (Medtronic)• AF Suppression™ (St Jude Medical)• AF Suppression (St. Jude Medical)

Mechanism of AF/AT SuppressionMechanism of AF/AT Suppression
1. Pace conditioning 2. PAC suppression2. PAC suppression3. Post-PAC response4 P t i4. Post-exercise response 5. Post-AF response6. Rate soothing
Mitchell ARJ, Sulke N. Europace 2004; 6: 351

Pace conditioningPace conditioning
• Adjusts the atrial pacing rate to just above the underlying intrinsic rhythm in such a way that the
i i d f l 95% f h iatrium is paced for at least 95% of the time

P diti iPace conditioning

PAC SuppressionPAC Suppression
• aims to reduce the incidence of PACs by increasing the heart rate upon detection of a PAC


Post PAC responsePost-PAC response
• prevents pauses after PACs by controlling the atrial rate in the two beats after a PAC


Post exercise responsePost-exercise response
• Aims to prevent the rapid heart-rate drop that can occur after exercise by enabling a post-exercise rate

Post-exercise Response

Rate soothingRate soothing
• Aims to prevent ATs by overdrive pacing the atrium at a rate that is only just above the sinus rate

Post AF responsePost AF response

AF Suppression Starts

AF Suppression Continues

Atrial Rhythm Classification (ARC)Atrial Rhythm Classification (ARC)ARC differentiates atrial flutter (AFL Region) from atrial fibrillation (AF Region) using Rate, Range, andatrial fibrillation (AF Region) using Rate, Range, and Standard Deviation.
AFib zone therapy
Range Standard Deviation
SVT zone therapy
Deviation
• AFL Region arrhythmias receive SVT zone therapy
• AF Region arrhythmias receive AFib zone therapy

Clinical trials

ADOPT A Clinical TrialADOPT-A Clinical Trial
Pacemaker Implant •ProspectiveSt d Pacemaker ImplantTrilogy DR DAOIntegrity AFx DR
•Prospective•Patient Blinded•Randomized
StudyDesign
DDDR PacingAF Suppression-ON
DDDR PacingAF Suppression-OFF
Follow-upBaseline, 30, 90, 180 days
D i A
Follow-upBaseline, 30, 90, 180 days
D i ADevice AssessmentQOL
Device AssessmentQOL
Symptomatic AF Episodesvia Event Recorder
Symptomatic AF Episodesvia Event Recorder
ADOPT A Clinical TrialADOPT-A Clinical Trial
Atrial Pacing% Atrial Beats Paced*
Atrial Pacing
AF Suppression OFF 67.9
*p<0 0001
AF Suppression ON 92.9*p<0.0001

ADOPT A Clinical TrialADOPT-A Clinical Trial
S t ti AF B d
4 44%5.0%
Symptomatic AF Burden
2 63%
4.44%
3.19%3 0%3.5%4.0%4.5%
%)
(n = 288) p < 0.05AFs OFF
AFs ON2.63%
1.73%1.37%
1.93%
1 5%2.0%2.5%3.0%
AF
Bur
den
(% AFs ON
0 0%0.5%1.0%1.5%A
0.0%
1-Month 3-Month 6-MonthFollow up

ADOPT A Clinical TrialADOPT-A Clinical Trial
AFs OFF AFs ONAF Burden Reduction
Total Patients 158 130
Patients with AF Days 81 73Patients with AF Days 81 73
Total AF Days 682 421
Total Follow-upDuration (Days)
27,359 22,526
AF Burden 2.493% 1.869%
AF Burden Reduction 25.03%

ADOPT A Clinical TrialADOPT-A Clinical Trial
AF Episode Reduction
9
108.3 ± 4.1
AF Episode Reduction
7
89
odes p = < 0.0001
8.1 ± 4.2 AFs OFF
AFs ON
45
6
AF
Epis
4.3 ± 11.5
2
3
4
Mea
n 3.2 ± 8.5
0
1
6 M th P i t I l t I l t t 6 M th6 Months Prior to Implant Implant to 6 Months

ADOPT A Clinical TrialADOPT-A Clinical Trial
Hospitalizations
100Freedom to first hospitalization (n = 288)
Hospitalizations
96
98
100
zatio
n*
AFs OFF
AFs ON
p= NS
92
94
96
Hos
pita
liz
88
90
92
(%) w
/o H
88 0 30 60 90 120 150 180Duration (Days)
6% Reduction in Hospitalizationsp

ADOPT A Clinical TrialADOPT-A Clinical Trial
100
Freedom from First Cardioversion (n=288)
96
98
over
sion
94
96
/o C
ardi
o
AFs OFFp = 0.0925
90
92
(%) w
/
AFs ON
0 30 60 90 120 150 180(Duration) Days
63% reduction in Cardioversions

ADOPT A Clinical TrialADOPT-A Clinical Trial
• Conclusion • AF Suppression pacing appears to be safe andAF Suppression pacing appears to be safe and
to reduce AF burden in sinus node dysfunction patients with paroxysmal or persistent AF.patients with paroxysmal or persistent AF.
• AF Suppression pacing offers incremental benefit to DDDR pacing alonebenefit to DDDR pacing alone.

AT500™ Pacing System U S Clinical ExperienceU.S. Clinical Experience
Two Large US Trials:g• ASPECT1
n=298 implanted, 277 intention-to-treat analysis (138 septal),35 centers, 6 month follow-up (crossover at 3 months);35 centers, 6 month follow up (crossover at 3 months); Single-blind study,Lead site randomized to RA septal or non-septalIntervention pacing algorithms ON vs. OFF
Primary endpoint: AT/AF frequency• ATTEST2
n=368 implanted 324 in efficacy cohortn=368 implanted, 324 in efficacy cohort,28 centers, 3 month follow-up; Single-blind studyAll therapies ON vs. OFF (Intervention and ATP)
Primary endpoint: AT/AF burden and frequencyPrimary endpoint: AT/AF burden and frequency
1 AT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc. 2 Lee M, Weachter R, Pollak S, et al. For the ATTEST Investigators. JACC 41:In Press 2003

AT500™ Pacing SystemASPECT Trial Design
Enrollment
ASPECT Trial Design
Enrollment(n=298)
Non-Septal Randomization Septal Atrial LeadAtrial Lead
N = 150
Septal Atrial LeadN = 148(Implant)
ON OFFCrossover:
1 month run in
Randomization
ON OFF
Randomization(1 month) (1 month)
ON
OFF
OFF
ON
- 1 month run-in- 3 month periods
for each phase
ON
OFF
OFF
ON
Clinical Follow-up Programming at discretion
of Physicianof Physician
AT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc.

AT500™ Pacing SystemASPECT Trial Results
Rx OFF2
(No changes in device-recorded AT/AF Burden or frequency with specialized algorithms ON vs. OFF)
20
25/d
ay)
10
12 Rx ON
15
20
piso
des /
8
hr/d
ay)
10
5
ency
(ep
6
urde
n(h
5
FFr
eque
2
4
AFB
0
AF
0Septal Non Septal Non SeptalSeptalSeptal Non-Septal Non-SeptalSeptal
Padelletti L, et al. PACE 2002;24(Part II):NASPE Abstract.
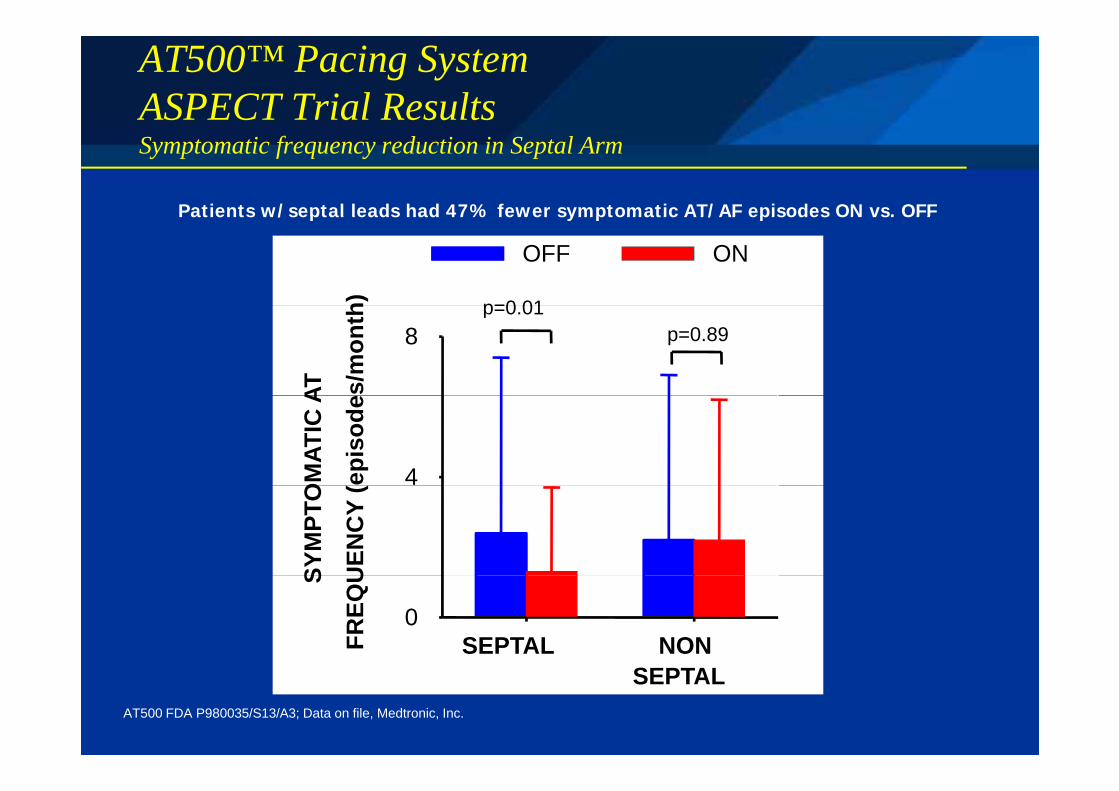
AT500™ Pacing SystemASPECT Trial Results
Patients w/septal leads had 47% fewer symptomatic AT/AF episodes ON vs. OFF
Symptomatic frequency reduction in Septal Arm
h)
OFF ON
p=0 01
Patients w/septal leads had 47% fewer symptomatic AT/AF episodes ON vs. OFF
AT s/m
ont h
8p=0.01
p=0.89O
MAT
IC A
epis
ode
4
SYM
PTO
UEN
CY
(
S
FREQ
U
0SEPTAL NON
SEPTALAT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc.

AT500™ Pacing SystemClinical ResultsClinical Results
• ASPECT1,2,3
• No change in frequency or burden of AT/AF episodes when prevention algorithms were enabledSignificant reduction in frequency of symptomatic AT/AF• Significant reduction in frequency of symptomatic AT/AF episodes when the atrial lead was placed in the septum
• Significant reduction in frequency of premature atrial i ( ) i b h l d l l dcontractions (PACs) in both septal and non-septal lead
placement groups• Patients with non-septal lead placement and high frequencyPatients with non septal lead placement and high frequency
PACs may represent a responder group for intervention algorithms
1 AT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc. 2 f S C 2002 2 68 ( S #6 9)2 Padeletti L, Pererfellner H, Adler S, et al. PACE 2002, Part II;24:687 (NASPE Abstract #659)3 Harvey M, Holbrook R, Young M, et al. JACC 2003; 41:Abstract #1017-5

AT500™ Pacing SystemATTEST Trial Design
Enrollment
ATTEST Trial Design
Class I / II Indications for Dual
Chamber Pacing
EnrollmentBrady + AT/AF
(n=368)+ At least 1 episode of paroxysmal or persistent AT/AF
(n 368)
Randomization
Prevention &
persistent AT/AF documented by ECG in last year
and 1 symptomatic
(at 1 month)
Prevention & ATP TherapiesON vs. OFF
and 1 symptomatic episode in past
3 monthsON
3 mosOFF3 mos
Clinical Follow-upProgramming at discretion of physicianProgramming at discretion of physician
AT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc.

AT500™ Pacing SystemATTEST Trial Results
18000
20000(ATP Did Not Significantly Alter Episode Duration)
14000
16000
18000
Therapies ON
odes
10000
12000
14000Therapies OFF
of E
piso
6000
8000
10000
umbe
r o
2000
4000Nu
0 1-10 10-60 1-4 4-12 12-24 24-72 >72min min hr hr hr hr hr
Episode DurationEpisode Duration Lee M, Weachter R, Pollak S, et al. For the ATTEST Investigators. JACC 41:In Press 2003AT500 FDA P980035/S13/A3; Data on file, Medtronic, Inc.

AT500™ Pacing SystemClinical ResultsClinical Results
• ATTEST1
• 99.9% (99.7% GEE) Positive Predictive Value for detection of AT/AF episode (based upon Investigator review)
• 54% (41% GEE) ATP therapy success rate for device-defined AT( ) py• Median % of atrial pacing was 98% ON vs. 75% OFF group• No incidence of ventricular pro-arrhythmia • No significant reduction in AT/AF burden, total frequency orNo significant reduction in AT/AF burden, total frequency or
symptomatic AT/AF frequency ON vs. OFF
Note: Median % of ventricular pacing was 97% in the ONNote: Median % of ventricular pacing was 97% in the ON group while only 30% of patients were diagnosed with AVB, suggesting high level of RV-pacing may have minimized affect of the atrial therapiesminimized affect of the atrial therapies.
1 Lee M, Weachter R, Pollak S, et al. For the ATTEST Investigators. JACC 41:In Press 2003

SAFE Study DesignSAFE Study DesignIMP
Week6-8 M6 M12 M18 M24
Septal Position + DAO = ON
Septal Position + DAO =OFF
RRAA Position + DAO = ON
RAA Position + DAO = OFF
Prospective, parallel, randomized, multiProspective, parallel, randomized, multi--center studycenter study

The problem of successful of AF suppressionThe problem of successful of AF suppression
• Anti-arrhythmias to be used• The sites of atrial pacingThe sites of atrial pacing• Progression of computer technology
Ch i i t ti t• Choosing appropriate patients• Maybe DDD pacemaker for bradycardia has little
effect for AT/AF supression• Detrimental effect of apex RV ventricular
pacing (‘ventricular pro-arrhythmic pacing’)

ConclusionConclusion
• The AF suppression technology in pacemaker patient is still being progress
• There are clearly groups of patients who benefit from AF suppression algorithm but there are alsofrom AF suppression algorithm but there are also many who do not
• Reduced ventricular pacing is also very important• Reduced ventricular pacing is also very important