Embed Size (px)
DESCRIPTION
Es el momento de explayarse hablando de la empowermend de usuarios. Espero lo disfruten.
Citation preview
Author's Accepted Manuscript
Incorporating Customer Empowerment in Mo-bile Health
M.N. Almunawar, M. Anshari, Mustafa Z. Younis
PII: S2211-8837(15)00066-0DOI: http://dx.doi.org/10.1016/j.hlpt.2015.08.008Reference: HLPT153
To appear in: Health Policy and Technology
Cite this article as: M.N. Almunawar, M. Anshari, Mustafa Z. Younis,Incorporating Customer Empowerment in Mobile Health, Health Policy andTechnology, http://dx.doi.org/10.1016/j.hlpt.2015.08.008
This is a PDF file of an unedited manuscript that has been accepted for publication.As a service to our customers we are providing this early version of the manuscript.The manuscript will undergo copyediting, typesetting, and review of the resultinggalley proof before it is published in its final citable form. Please note that duringthe production process errors may be discovered which could affect the content,and all legal disclaimers that apply to the journal pertain.
www.elsevier.com/hlpt
Incorporating Customer Empowerment in Mobile Health
M.N. Almunawar, M. Anshari, and Mustafa Z. Younis Mohammad Nabil Almunawar School of Business & Economics, Universiti Brunei Darussalam Muhammad Anshari CEC & Joint Appointment e-Government Innovation Centre, Universiti Brunei Darussalam Mustafa Z. Younis Tenured Professor, Department of Health Policy & Management Jackson State University Jackson, MS 39213
Incorporating Customer Empowerment in Mobile Health
Abstract The adoption of mobile services in many business sectors offers various business opportunities. But at the same time poses a great challenge for service providers and business organizations to grab the opportunities. Accessing mobile services through mobile devices equipped with powerful operating systems and a myriad of applications (Apps) such as smart phones or tablet computers are very handy and convenient. As most people are dependent on their smart phones for various reasons, mobile services accessible through smart phones are demanded. The healthcare industry should grab this opportunity by offering mobile health (mHealth). mHealth should be designed to offer customers a greater role in the decision making processes related to their health. Thus, customers (patients) will not only enjoy healthcare services online such as making appointments, viewing health records and having consultations through their smart phones or other mobile devices, but they can also participate and contribute to the discussion in information and knowledge sharing forums. In other words, consumers will be empowered through mHealth. The aim of this paper is to present a model of mHealth that incorporates customer empowerment in three dimensions: personal dimension (mPersonal), social dimension (mSocial), and medical dimension (mMedical). In addition to literature review, a survey has been conducted to grab user perception as well as requirements for the model. The model can be used as a roadmap for healthcare organizations in embracing mHealth with customer empowerment embedded their services. Keywords: Customer empowerment, mHealth, Mobile Personal (mPersonal), Mobile Social (mSocial), Mobile Medical (mMedical),
Introduction
Managing a good relationship between a healthcare organization and its customers (patients) in
healthcare management is important to create mutual understanding, trust, and customers’ participation
in healthcare related processes and decision-making. A good relationship is believed to improve patients’
satisfaction, which in turn makes them loyal customers (Richard & Ronald, 2008). Therefore, serious
attention must be given to values of pleasing customers, satisfying their needs, and building a long lasting
relationship. Empowering customers through mobile health (mHealth) services can be an interesting
application of Information and Communications Technology (ICT) in embracing customers’ expectations
and best practices in healthcare organizations (Anshari & Almunawar, 2012). The trend in healthcare
services is the transformation from physical-based services, where a complete physical presence is
necessary, to mobile services where some healthcare activities can be performed such as preventing
disease, promoting health, and providing e-health services (Haux et al., 2002). As the penetration of
mobile technology into the market is high and keeps growing, the adoption of mHealth in healthcare
service also grows, as it can help improve the quality of service of healthcare provision (Anshari et al.,

2013). For instance, healthcare organizations may offer health promotion and services through social
networks embedded in mobile applications (Apps).
Nowadays customers can easily access mobile services and activate them in social networks using their
smart phones. They can share and discuss their healthcare issues through their smart phones. This
implies that customers can actively participate and contribute in healthcare using their smart phones or
other mobile devices. mHealth should be designed to let customers actively participate in healthcare
processes and decision making. Accessing such an mHealth may encourage customers to take more
responsibilities for their own health and help each other through information and knowledge-sharing. In
addition, mHealth provides customers the ability to access and control information flow that fits their
personalized needs.
mHealth can extend healthcare services through smart mobile devices in multiple types of interactions
such as between healthcare staff and customers, between two or more customers, and customers’ self-
service (Anshari et al., 2012a; Almunawar et al., 2012). At this point in time, not many discussions in the
literature have proposed a model of mHealth that extends state-of-the-art healthcare services to
customers. In addition, current discussions in literature have not included the comprehensive issues of
customer empowerment in mHealth setting. This paper attempts to fill the knowledge gap of how
healthcare organizations can develop mechanisms by encouraging patients’ responsibility to take a
greater role in the healthcare process. This can occur through empowerment, delivery arrangements that
will meet the increasing demand, and expectation of patients equipped with mobile technology. The study
proposes a model to enhance the existing theory of empowerment through mobile approach. The model
is expected to contribute in expanding dimensions of the mHealth system employing the possible
perspective of empowerment.
We start by analyzing various related issues through a literature study. We then propose a model and its
e-components based the results of this analysis and a survey. Next we present methodology, implications
of the proposed model and discussion. The paper ends with a conclusion.
Literature Review
Healthcare services need to be transformed from the traditional view where patients are solely considered
as recipients of care, to partners of care so that they can participate actively on healthcare processes and
decision making. For instance, effective chronic disease care and education requires patients and health
care staffs to collaborate in the development of self-management plans that integrate the clinical
expertise of health care professionals with the concerns, priorities and resources of the patient (Anderson
& Funnell, 2005; Feste & Anderson, 1995). The new view implies empowerment of patients (customers)
since they are treated as partners, and not merely recipients.
Empowerment of patients has been discussed in the health literature over the past few decades. The
process of empowerment has been acknowledged as an alternative to compliance with multi-ways
interactions. Healthcare providers need to prepare new services that reflect the new view and to have a
proper strategy on how to strengthen the relationship with their customers (Almunawar & Anshari, 2011).
Table 1 shows the type of empowerment supported from literature based on the outcomes.
Empowerment can be grouped either from the point of view of healthcare provider–patient interaction
(Skelton, 1997; Paterson, 2001; Dijkstra et al., 2002; van Dam et al., 2003; Maliski et al., 2004; Kettunen
et.al, 2006), or from the point of view of the patient alone (Anderson et al., 1995; McCann et al., 1996;
Davison et al., 1997; Desbiens et al., 1998; Howorka et al., 2000; Golant et al., 2003; Loft et al., 2003;
Chang et al., 2004), or both (McWilliam et al., 1997; Golant et al., 2003; Maliski et al., 2004).
Empowerment of personal, community, and combination will be discussed in the following section.

Table 1: Type of Empowerment
Type Outcomes
Personal 1. Empowerment strategies through e-health less negative definitions of illness as well as improved self management by patients (Segal, 1998).
2. Manage or prevent diseases and their recovery by themselves (Jones, 1993; Bergsma, 2004).
3. Personal empowerment (patient alone); self-belief to act on their own behalf in a manner that best meets their healthcare goals. Personal Determination; Ability to choose (Chang et al., 2004; Paterson, 2001).
4. E-health; empower knowledge bases of medicine and personal electronic records accessible to consumers over the Internet (Eysenbach 2001).
Community/Group 1. Organizational influences on the process of community empowerment (Laverack and Labonte, 2000)
2. Community development, individuals contribute to a common goal within a collective process of social change (Bergsma, 2004)
3. Patient 2.0 Empowerment is the active participation of the citizen in his or her health and care pathway with the interactive use of Information and Communication Technologies (Bos et al, 2008).
Combine (Personal – Healthcare organization)
1. Empowerment approaches must operate at various levels of individual and community (Raymond, 2012)
2. Patient empowerment focuses on control in individuals’ experience of health, disease and illness, as well as the roles of health care organizations, communities and the broader health care system health (Harris and Veinot, 2004)
3. Offering customized information of proven quality according to the patient’s individual informational needs may be a key success factor for computer supported patient empowerment, therefore availability of a system must be supported by an organization (Hoffmann et al., 2004)
4. Based on evidence-based e-health studies, propose directions for best practices to develop e-health that promotes patient empowerment. The possibilities and the practical benefits of e-health for self-management. Relationship between patient and professional: Ensuring that channels for e-communications and information exchanges are in place (Alpay et al, 2010)
5. Healthcare provider–patient interaction; empowerment is considered to engage customers in the process of conversation and education in which knowledge, values and power are shared (Brennan and Safran, 2005)
Source: Authors’ Compilation
Medical Empowerment
Empowerment may include healthcare provider–patient relationship, disease or illness self-management
and its treatment, which leads to a boost in personal satisfaction due to the increase in responsibility of
one’s own well-being (Aujoulat et al., 2007). Some new systems were developed to help patients freely
access their medical record for example, Personally Controlled Electronic Health Records (PCEHR) in
Australia, which was released on 2012. PCEHR enables better access to important health information
held in dispersed records across the country. PCEHR can be considered as medical empowerment
where patients in Australia are able to view their important medical records and related information
whenever and wherever they need. In addition, they can share their health records with trusted
healthcare providers (NEHTA, 2014).
We propose medical empowerment electronically, where patients are allowed to view their medical
records through mHealth system. Healthcare organizations still control medical records and they can
decide which records to be shared. In addition patients are allowed to modify their personal data using
their smart mobile devices.
Personal Empowerment
McWilliam et al. (1997) emphasizes that empowerment is a result of both interactive and personal
processes, where the emergence of “power” (or potential) is facilitated by caring relationships.
Empowerment as an interactive process suggests that power is ‘‘transferred’’ by one person to another,
whereas empowerment as a personal process suggests that power is ‘‘created’’ by and within the person.
Although the expected outcomes are similar, more power over one’s life, the nature of the two processes
is very different (Aujoulat et al., 2007). Segal (1998) mentions that there is evidence that coaching
patients using empowerment strategies through e-health leads to broadened, less negative definitions of
illnesses as well as improved self-management of patients. However, without the healthcare provider’s
commitment to responding properly, the benefits of empowerment are unlikely to emerge.
In addition, health education is important. Individuals must maintain healthy lifestyles, be aware of life
changes, manage, or prevent diseases and this leads to their recovery of their own health issues and
physical capabilities, which is considered as a health enhancing process (Jones, 1993; Bergsma, 2004).
There must be a mechanism to incorporate the self-management of patients into e-health systems
(Almunawar & Anshari, 2014).
Social Empowerment
The emergence of Web 2.0 has changed the ways in which many organizations operate, including
healthcare services. The booming numbers of social networking and support groups for patients on the
Internet and their influence on health behavior are only beginning to be explored and remain an important
area for future research (Rimer et al., 2004). The concept of social networks defines organizations as
systems that contain objects such as people, groups, and other organizations linked together by a range
of relationships (Askool & Nakata, 2010). Some organizations are building online social networks to
engage customers and import ideas such as innovative services, new products, and technologies (Lafley
& Charan, 2008). Social networks can be used as enablers in creating close and long-term relationships
between an organization and its customers (Askool & Nakata, 2010; Anshari et al., 2012b). In addition,
social networks may play a significant role in managing customer relationships and stimulate fundamental
changes in consumer behaviors (Greenberg, 2009). Gibson (1991) defines empowerment as a process of
helping people assert control over the factors, which affect their lives. It encompasses both the individual
responsibility in healthcare and the broader institutional or societal responsibilities in enabling people to
assume responsibility for their own health. Therefore, it is important to consider embedding social network
into mHealth systems to provide social empowerment for patients and communities at large.
Empowerment in mHealth
Customer empowerment in mHealth has three dimensions, personal, social, and medical dimensions, as
depicted in Figure 1. Mobile personal or mPersonal is mainly to support personalization which allows
customers to control their personal information, mobile medical or mMedical allows customers view their
health records, and mobile social or mSocial allows customers interact among them to share information,
knowledge and experience.
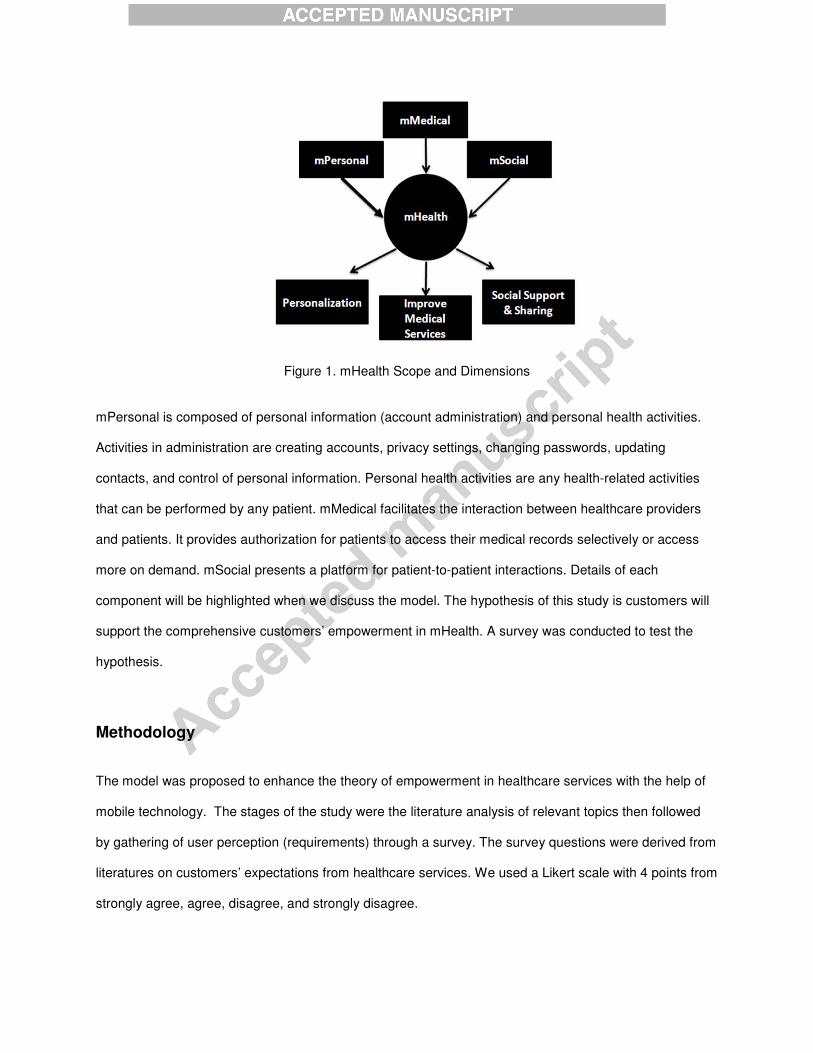
Figure 1. mHealth Scope and Dimensions
mPersonal is composed of personal information (account administration) and personal health activities.
Activities in administration are creating accounts, privacy settings, changing passwords, updating
contacts, and control of personal information. Personal health activities are any health-related activities
that can be performed by any patient. mMedical facilitates the interaction between healthcare providers
and patients. It provides authorization for patients to access their medical records selectively or access
more on demand. mSocial presents a platform for patient-to-patient interactions. Details of each
component will be highlighted when we discuss the model. The hypothesis of this study is customers will
support the comprehensive customers’ empowerment in mHealth. A survey was conducted to test the
hypothesis.
Methodology
The model was proposed to enhance the theory of empowerment in healthcare services with the help of
mobile technology. The stages of the study were the literature analysis of relevant topics then followed
by gathering of user perception (requirements) through a survey. The survey questions were derived from
literatures on customers’ expectations from healthcare services. We used a Likert scale with 4 points from
strongly agree, agree, disagree, and strongly disagree.
The survey was conducted in major hospitals (Ripas Hospital), 5 clinics, and 10 home care centers in
Brunei Darussalam (Brunei) from February to March 2011. There were 366 respondents participating for
the survey, and they represent a fair share of the public. The time taken to complete the questionnaire on
average was 6 minutes. There were survey liaisons who distributed the questioners and answering
questions for any queries from respondents. The 17-items survey instrument that was tailored to the
population for this study was divided into three sections. The first section included 6 items about
demographics’ traits of respondents where we learnt on our respondent gender composition, age,
employment type, educational level, computer literacy, and the time they spend on the Internet. The
survey respondents ranged from 20 or younger - 50 years old, representing a fair sample of the country’s
population. Eleven items in the second part asked about features of empowerment in e-health services as
derived from reference model. At last section, participants were asked to write anything regarding their
expectations and comments regarding the proposed features of empowerment in e-health. Valid
percentage calculations were calculated by SPSS for each item. Based on the literature analysis and
survey results, we proposed the model of patient’ empowerment to mHealth services.
The model will be used to develop a prototype system for further testing in real healthcare scenario. The
outcome of this study is the prototype of the system based on the proposed model. However, in this
paper we have only included the survey result and the proposed model since development of prototype is
ongoing project.
Survey Results
To analyze the reliability of the questionnaire items used in this study, Cronbach’s alpha is used to
measure internal consistency. Cronbach’s alpha is 0.850 for mPersonal’s cluster, 0.720 for mMedical,
and 0.890 for mSocial those values indicate a relatively high internal consistency and reliability of the
study. Table 2 explains the demographic characteristics of the samples. It is important to note that
respondents who regularly visit healthcare centres between the ages of 20 to 50 years are the potential
users of mHealth notably because of their basic Internet literacy and this is the critical success factor for
empowerment through mHealth. It is important to note that Internet literacy in Brunei is high.

Item Percent
Gender Male 46
Female 54
Age 20 years or younger 13
21 - 30 38
31 - 40 31
41 - 50 18
Education Completed high school only 41
Completed more than high school
59
Internet Usage At least daily 73
< daily to weekly 18
Weekly to monthly 9
Table 2: Demographic information of respondents
As internet and mobile penetration in Brunei is high, the expectation to receive services through the
Internet that can be accessed with their mobile devices is also high. The survey reveals that the
expectations of customers/patients towards mHealth, where they can access services using their mobile
devices are very promising. The survey questions gathered both the agreement and disagreement of
participants if empowerment services were introduced in an e-health system. Questions in the
questionnaire can be grouped into three sections, which are related to mPersonal, mMedical and mSocial
(Table 3).
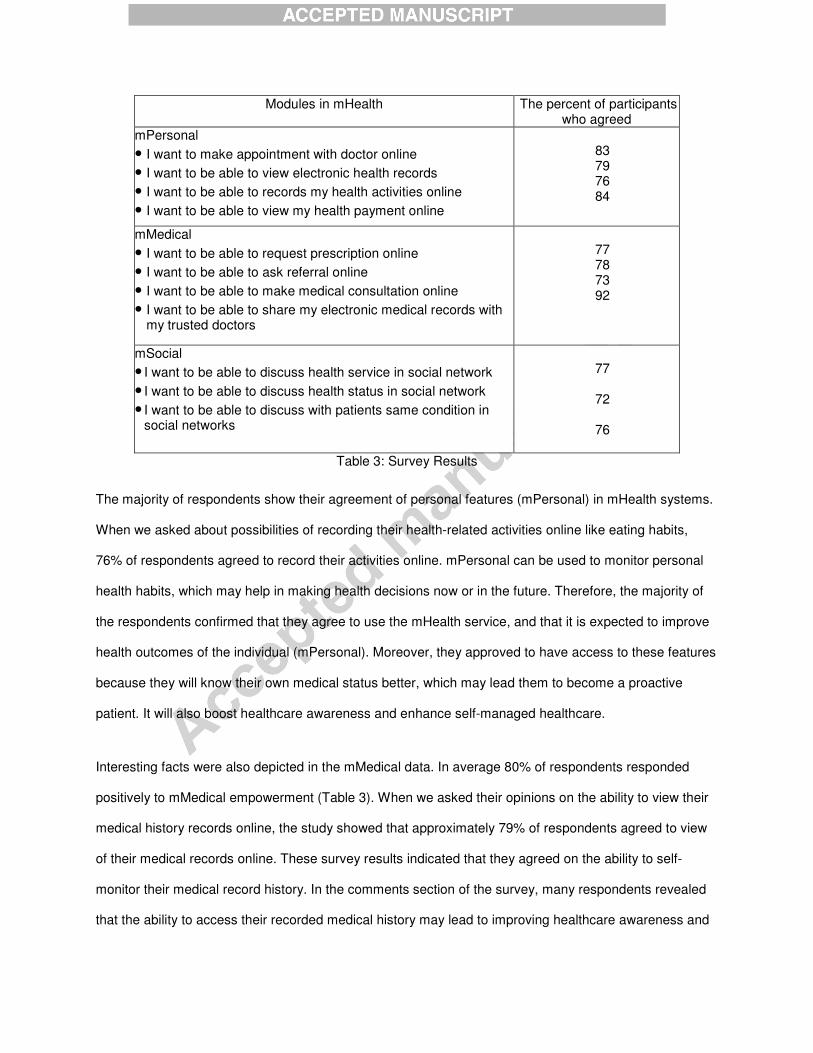
Modules in mHealth The percent of participants who agreed
mPersonal
• I want to make appointment with doctor online
• I want to be able to view electronic health records
• I want to be able to records my health activities online
• I want to be able to view my health payment online
83 79 76 84
mMedical
• I want to be able to request prescription online
• I want to be able to ask referral online
• I want to be able to make medical consultation online
• I want to be able to share my electronic medical records with my trusted doctors
77 78 73 92
mSocial
• I want to be able to discuss health service in social network
• I want to be able to discuss health status in social network
• I want to be able to discuss with patients same condition in social networks
77
72
76
Table 3: Survey Results
The majority of respondents show their agreement of personal features (mPersonal) in mHealth systems.
When we asked about possibilities of recording their health-related activities online like eating habits,
76% of respondents agreed to record their activities online. mPersonal can be used to monitor personal
health habits, which may help in making health decisions now or in the future. Therefore, the majority of
the respondents confirmed that they agree to use the mHealth service, and that it is expected to improve
health outcomes of the individual (mPersonal). Moreover, they approved to have access to these features
because they will know their own medical status better, which may lead them to become a proactive
patient. It will also boost healthcare awareness and enhance self-managed healthcare.
Interesting facts were also depicted in the mMedical data. In average 80% of respondents responded
positively to mMedical empowerment (Table 3). When we asked their opinions on the ability to view their
medical history records online, the study showed that approximately 79% of respondents agreed to view
of their medical records online. These survey results indicated that they agreed on the ability to self-
monitor their medical record history. In the comments section of the survey, many respondents revealed
that the ability to access their recorded medical history may lead to improving healthcare awareness and

promote self-managed healthcare.
Another example of empowerment in mHealth is having consultations online. For example, when patients
are assigned a diet program, they do not have to travel all the way to a hospital because they can have
access to this same program through the online service provided. This module can save both time and
money. For health professionals, this module will help monitor their patients’ progress online, which is
convenient for both parties. Online appointment is the ability of the patient to make appointments for
medical visits online. The survey revealed that the majority of respondents (83%) preferred having the
ability to make an appointment online. The results show that the empowerment of the modules is in line
with their expectations of the service. When referred to online prescription sub-modules, the majority of
respondents tended to request their preferred or trustworthy interaction online. The survey showed that
most Bruneians agreed that requesting refills for prescriptions online definitely offers time-efficiency. In
addition, the majority of them agreed to view their payment and insurance coverage online to keep up-to-
date on their payment information and to avoid miscalculation. The survey results confirmed the
hypothesis that there is a tendency for participants to participate in mHealth service when the service is
readily available. Then, based on the survey and the literature that we study, we proposed a model of
mHealth to provide a roadmap in developing a prototype of mHealth especially by highlighting the three
components of empowerment in the next section.
The Model of mHealth
Empowerment is an important feature that can be used as a strategy in mHealth services and the survey
results confirm that customers need empowerment through their mobile services. As discussed in the
literature study, empowerment refers to the process of gaining influence or control over events and
outcomes of importance (Fawcett et al., 1994). Empowering customers can be seen as an effort to build
loyalty and trust between a healthcare organization and its patients. Empowerment encourages patients
to take responsibility for their personal health and make decisions about their own healthcare. Patients
are empowered in the sense of controlling the process of interaction to their healthcare providers and
among patients themselves. However, providing empowerment in any state of interaction is a challenging

task.
The three dimensions of interaction proposed in the previous section are further explained in a circular
model as shown in Figure 2. Based on the model, healthcare organizations can implement the
empowerment in their services into three dimensions. For instance, patients are able to generate the
contents of their health records. Empowered customers can make records that can help healthcare staff
get better concepts of the patients’ condition.
Figure 2 explains three domain areas of mHealth service that are possibly taken into consideration in the
process of decomposing mHealth scenario. The model extends the role of customers into three distinct
functions as personal, social, and medical. Each role comprises of a set of objects that detail the function
and arrange activities within mHealth’s context between customers of the healthcare provider. We adopt
the object-oriented approach as it supports extendibility so that new objects or entities can be easily
derived from existing ones if they are needed.
Figure 2. The mHealth Model
We use an object-oriented approach to construct the model. Each object has properties and operations.
There are three main objects in the model, namely mPersonal, mSocial, and mMedical. mPersonal is an
object for personal activities which records health status and services. mPersonal consists of properties
Identity/Profile (ID), Personal Habits (HB), Exercise (EX), Emotional and Spiritual (SE), Personal Health
Plan (HP), and Personal Account (AC). More properties can be added depending upon the need and
urgency. Object mSocial consists of all objects that relate to social networks and media. Among the
properties of this object are conversation (CS), knowledge management (KM), and resolution (RS).
Finally, mMedical consists of objects that encompass activities of checkups, I/P treatment, and O/P
treatment. The properties of the object are e-appointment (EA), examination (XM), treatment (TM), and e-
prescription (EP). Each object can be a composite object (object contains an object or objects). For
instance, object XM may be made up of chronic disease (cc) and non-chronic disease (nc). Chronic
diseases are comprised of diabetes (da), cancer (ca), obesity (ob), etc.
mPersonal
At the individual level, empowerment can be achieved through a process of recognizing, promoting, and
enhancing one’s personal abilities to meet one’s own needs, solve one’s own problems, and mobilize the
necessary resources in order to feel in control of one’s life. mPersonal is an individual habit and lifestyle
which affect the overall health status. Empowering at this level comprises improving basic habits, physical
exercises, and emotional factors. Patients may have full control over any mHealth activities in this
module. For instance, customers can use operations provided in this object to update, edit, and delete
their own exercise activities through their mHealth system.
mMedical
mMedical defines interaction between customers and their healthcare organization in the process of
healthcare and health decision making. Activities in mMedical may be comprised of checkups, outpatient
treatment (O/P), inpatient treatment (I/P) with the purpose to provide a comprehensive medical view and
history. Furthermore, checkups, inpatient treatment, and outpatient treatment are the activities that
patients mostly have direct interaction with the provider (e.g., consultation, physical treatment). In many
cases, the healthcare provider provides limited access to patients in accessing their own electronic
medical records (EMRs). mMedical facilitates patients to exercise rights and authorizations in accessing
their medical records. For instance, healthcare providers may grant access for customers to view their
examination records (XM).
mSocial
mSocial can generate a way to strengthen the relationship between organizations and their customers.
However, conversations taking place among customers on a social network can influence the image of
the healthcare provider (Almunawar et al., 2012). Social networks of mHealth allow customers to share
experiences as well as promoting consulting opportunities. The connections of customers in social
networks generate the value and significance of mHealth.
Customer to customer interactions can affect to customers participations, interactions, and empowerment
in mHealth service. In the model, customer-to-customer interaction is designated mSocial. mSocial
enables interaction, conversation, and networking among customers/patients and between healthcare
providers and patients. mSocial adds value to the network such as multi-way conversations and sharing
of experience, information and knowledge. One central feature of network empowerment is that of making
use of the individual’s competence to collectively initiate changes. Interaction between patients is the part
of social life to collectively relate the conversation to share experiences, symptom histories, treatment
strategies, types of medicines consumed, long-term planning, etc. Patients benefit from feedback,
support, encouragement, and collective knowledge sharing.
Limitation and Future Direction
The study has several limitations. In order to gather customers’ perceptions on customer empowerment in
mHealth, the surveys were conducted in Brunei to understand the customer behaviour only in the country.
Furthermore, the proposed model needs further development in terms of prototyping so that the model
can be tested in a real healthcare setting. In this study, the researchers examined only participants who
are purposely involved with the testing process of the prototype. The study excludes clinical aspects of
participants that may affect their health literacy, health status, and is only concerned with the customer's
perspective on customer satisfaction through mHealth. Last but not the least, the research has the
potential to comprise many aspects of e-health and mHealth services. The next step is to develop a
prototype that implements the model to see the effect of empowerment on customer satisfaction and
health literacy.
Conclusion
The model integrates the wider scope of empowerment into three distinct roles, i.e., personal, social, and
medical. The model fills the gap in drawing dimensions of mHealth towards extending customers’
empowerment. In addition, it gives direction for any healthcare organization in providing mHealth
systems. The model in this paper presented the empowerment types (i.e., integration, participation, and
interaction) that are beneficial for customers and healthcare organizations. Furthermore, the integrated
approach can help healthcare organizations in defining which scope of empowerment they will implement
in the organization. The modular approach will assist healthcare organizations to initiate empowerment by
stages and later on to measure the empowerment process and performance. This study contributes to
understanding mHealth with comprehensive drawings of its dimensions. Moreover, it promotes the
process of extending the role of patients from recipients of care to partners of care. mHealth provides a
comprehensive perspective of patients as individual health actors, social health agents, and medical care
partners. The model identified possible theoretical mechanisms that might account for ways in which
mHealth provides a platform for building relationships between a healthcare provider, patients/customers,
and community at large.
References
Anderson, R. M., & Funnell, M. M. Patient empowerment: reflections on the challenge of fostering the
adoption of a new paradigm. Patient education and counseling 2005; 57(2), 153-157.
Anderson, R.M., Funnel, M.M., Butler, P.M., Arnold, M.S., Fitzgerald, J.T., & Feste, C. Patient
empowerment: results of a randomised control trial. Diabetes Care 1995; 18:943–9.
Anshari, M. & Almunawar, M.N. Framework of social customer relationship management in e-health
services. Journal of e-Health Management, Volume 2012, Article ID 766268, DOI:
10.5171/2012.766268
Anshari, M., Almunwar, M.N., Wint, Z., Low, P.K.C., & Younis, M. Adopting customers’ empowerment and
social networks to encourage participation in e-health services. Journal of Health Care Finance,
2013;40 (2), 17-41.
Anshari, M., Almunawar, M.N., Low, P.K.C., & Al-Mudimigh A.S. Empowering clients through e-health in
healthcare services: Case Brunei. International Quarterly of Community Health Education, 2012a ;
33(2), 191-221.
Anshari, M., Almunawar, M. N., Low, P. K. C., & Wint, Z. Customer empowerment in healthcare
organisations through CRM 2.0: Survey results from Brunei tracking a future path in e-health
research. ASEAS – Austrian Journal of South-East Asian Studies, 2012b; 5(1), 139-151.
Almunawar, M.N., Wint, Z., Low, K.C.P., & Anshari, M. Customer’s expectation of e-Health systems in
Brunei. Journal of Health Care Finance, 2012;38(4), 36-49.
Almunawar, M. N., & Anshari, M. Empowering customers in electronic health (e–health) through social
customer relationship management. International Journal of Electronic Customer Relationship
Management, 2014; 8(1), 87-100.
Almunawar, M.N. & Anshari, M. (2011). Improving customer service in healthcare with CRM 2.0. GTSF
Business Review (GBR), 2011; 1(2), 228-234.
Askool, S. S., & Nakata, K. Scoping study to identify factors influencing the acceptance of social CRM. In
Management of Innovation and Technology (ICMIT), 2010 IEEE International Conference on (pp.
1055-1060). IEEE.
Aujoulat, I., d’Hoore, W., & Deccache, A. Patient empowerment in theory and practice: polysemy or
cacophony?. Patient education and counseling, 2007; 66(1), 13-20.
Bergsma, L. J. Empowerment Education: The Link between Media Literacy and Health Promotion.
American Behavioral Scientist, 2004; 48(2), 152-164.
Chang, L.C., Li, I.C., & Liu, C.H. (2004). A study of the empowerment process for cancer patients using
Freire’s dialogical interviewing, J Nurs Res, 2004;12:41–9.
Davison, B.J. & Degner, L.F. Empowerment of men newly diagnosed with prostate cancer. Cancer Nurs
1997; 20:187–96.
Desbiens, S.A., Wu, A.W. Yasui, Y., Lynn, J., Alzola, C., Wenger, N.S., Connors, A.F., Phillips, R.S.,
Fulkerson, W. Patient empowerment and feedback did not decrease pain in seriously ill
hospitalised patients. Pain 1998;75:237–48.
Dijkstra, R., Braspenning, J., Grol, R. Empowering patients: how to implement a diabetes passport in
hospital care. Patient Educ Couns 2002;47:173–7.
Fawcett, S. B., White, G. W., Balcazar, F. E., Suarez-Balcazar, Y., Mathews, R. M., Paine-Andrews, A., ...
& Smith, J. F. A contextual-behavioral model of empowerment: Case studies involving people with
physical disabilities. American Journal of Community Psychology, 1994; 22(4), 471-496.
Feste, C., & Anderson, R. M. Empowerment: from philosophy to practice. Patient education and
counseling 1995; 26(1), 139-144.
Haux, R., Ammenwerth, E., Herzog, W., & Knaup, P. Health care in the information society. A prognosis
for the year 2013. International Journal of Medical Informatics, 2002; 66(1), 3-21.
Howorka, K, Pumprla, J.,Wagner-Nosiska, D., Grillmayr, H., Schlusche, C, & Schabmann, A. Empowering
diabetes out-patients with structured education: short-term and long-term effects of functional
insulin treatment on perceived control over diabetes. J Psychosom Res, 2002; 48:37–44.
Jones, P. S., & Meleis, A. I. Health is empowerment. Advances in Nursing Science, 1993; 15(3), 1-14.
Golant, M., Altman, T., & Martin, C. Managing cancer side effects to improve quality of life: a cancer
psychoeducation program. Cancer Nurs 2003; 26:37–44.
Gibson, C. H. A concept analysis of empowerment. Journal of advanced nursing, 1991; 16(3), 354-361.
Greenberg, P. CRM at the speed of light: social CRM 2.0 Strategies, tools, and techniques for engaging
your customers. McGraw-Hill Osborne Media, 2009.
Lafley, A. G., & Charan, R. The game-changer: how every leader can drive everyday innovation. New
York: Crown Business, 2008.
Loft M, Mc William C, & Ward-Griffin, C. Patient empowerment after total hip and knee replacement.
Orthop Nurs 2003;22:42–7.
Kettunen, T., Liimatainen, L., Villberg. J., Perko, U. Developing empowering health counseling
measurement. Preliminary results. Patient Educ Couns, 2006; 64:159–66.
McWilliam, C. L., Stewart, M., Del Maestro, N., Pittman, B. J., Brown, J. B., McNair, S., & Patterson, M. L.
Creating empowering meaning: an interactive process of promoting health with chronically ill older
Canadians. Health Promotion International, 1997;12(2), 111-123.
Maliski, S.L., Clerkin, B., & Letwin, M.S. Describing a nurse case manager intervention to empower low-
income men with prostate cancer. Oncol Nurs Forum 2004;31:57–64.
McCann. S, & Weinman, J. Empowering the patient in the consultation: a pilot study. Patient Educ Couns
1996; 27:227–34
McWilliam, C.L., Stewart, M., Brown. J.B., McNair, S., Desai, K., Patterson, M.L., Del Maestro, N.,
Pittman, B.J. Creating empowering meaning: an interactive process of promoting health with
chronically ill older Canadians. Health Promot Int 1997;12:111–23.
NEHTA, The Personally Controlled eHealth Record System (PCEHR). Retrieved December 12, 2014,
from http://www.nehta.gov.au
Paterson, B. Myth of empowerment in chronic illness. J Adv Nur 2001;34:574–81.
Richard, L.S. & Ronald, M.E. Lessons from theory & research on clinician-patient communication In
Glanz, K., Rimer, B. K., & Viswanath, K. (Eds.). (2008). Health behavior and health education:
theory, research, and practice, 2008; pp 236-269. John Wiley & Sons.
Rimer, B. K., Briss, P. A., Zeller, P. K., Chan, E. C., & Woolf, S. H. Informed decision making: what is its
role in cancer screening?. Cancer, 2004; 101(S5), 1214-1228.
Segal, L. The importance of patient empowerment in health system reform. Health Policy, 1998;44(1), 31-
44.
Skelton, A.M. Patient education for the millennium: beyond control and emancipation? Patient Educ
Couns 1997; 31:151–8.
van Dam, H.A., van der Horst. F., van den Borne. B., Ryckman. R., Crebolder. H. Provider–patient

interaction in diabetes care: effects on patient self-care and outcomes. A systematic review. Patient
Educ Couns 2003;51:17–28.
About the authors:
Mohammad Nabil Almunawar, PhD, is a Senior Lecturer, School of Business and Economics, Universiti of Brunei Darussalam, Brunei Darussalam. He can be reached at [email protected] or [email protected] Muhammad Anshari, PhD, is a researcher at Continuing Education Centre (CEC) & Joint Appointment at e-Government Innovation Centre, Universiti Brunei Darussalam. He can be reached at [email protected]. Mustafa Z. Younis, PhD, is Professor of Health Economics & Finance, Department of Health Policy & Management, Jackson State University in Jackson, Mississippi.
Highlights
The articles highlights the adoption of mobile services in business and health sector and it’s
impact on consumer empowerment. It present a model of mHealth that incorporates customer
empowerment in three dimensions: personal dimension (mPersonal), social dimension (mSocial),
and medical dimension (mMedical). In addition to literature review, a survey has been conducted
to grab user perception as well as requirements for the model. The model can be used as a
roadmap for healthcare organizations in embracing mHealth with customer empowerment
embedded their services.