Embed Size (px)
DESCRIPTION
Â
Citation preview
Houston Methodist Hospital
6565 Fannin St., Houston, TX 77030
877.790.DOCS
houstonmethodist.org/ni
LEADING MEDICINE YESTERDAY, TODAY AND TOMORROWAt Houston Methodist, we have a proud tradition of
revolutionizing medicine. Our past achievements
have built a legacy that spans multiple decades and
disciplines, and that same culture of excellence
inspires us to be the pioneers of tomorrow.
THAT’S THE DIFFERENCE BETWEEN PRACTICING MEDICINE AND LEADING IT.
Our commitment to advancing medicine with global impact
begins in Houston, Texas, where we pioneer a better tomorrow
through research, innovation and breakthroughs to rewrite the
future of health.
LEADINGNEUROSCIENCES
2 0 1 4 - 2 0 1 5 Y E A R I N R E V I E W
Educating for Tomorrow
Houston Methodist Hospital
6565 Fannin St., Houston, TX 77030
877.790.DOCS
houstonmethodist.org/ni
LEADING MEDICINE YESTERDAY, TODAY AND TOMORROWAt Houston Methodist, we have a proud tradition of
revolutionizing medicine. Our past achievements
have built a legacy that spans multiple decades and
disciplines, and that same culture of excellence
inspires us to be the pioneers of tomorrow.
THAT’S THE DIFFERENCE BETWEEN PRACTICING MEDICINE AND LEADING IT.
Our commitment to advancing medicine with global impact
begins in Houston, Texas, where we pioneer a better tomorrow
through research, innovation and breakthroughs to rewrite the
future of health.
LEADINGNEUROSCIENCES
2 0 1 4 - 2 0 1 5 Y E A R I N R E V I E W
10
CONTENTSPIONEERING THE PATH: AN OVERVIEW 04
LEADERS IN NEUROIMAGING 06REVOLUTIONIZING NEUROREGENERATIVE MEDICINE 10OPERATING ON THE INOPERABLE: DEEP BRAIN SURGERY 12SUCCESSFUL CASE STUDIES FOR COMPLEX NEUROSURGERY 14
HISTORICAL FIRST: SCALP AND SOLID ORGAN TRANSPLANT 16MITOCHONDRIAL SMART BOMBS TARGET BRAIN TUMORS 18NONINVASIVE TREATMENTS FOR STUTTERING 20GROUNDBREAKING STROKE STUDY 21PURSUING MEDICAL DISCOVERIES IN ALZHEIMER’S DISEASE 22LEADING MEDICINE IN STROKE CARE 26T CELLS SUPPRESS ALS PROGRESSION 28ADVANCES IN NEUROMUSCULAR THERAPIES 30DIAGNOSING CONCUSSION IMMEDIATELY: HEAD HEALTH INITIATIVE 32THE DESTRUCTIVE COMPONENTS OF SUBARACHNOID HEMORRHAGE 34A PARADIGM SHIFT IN ANEURYSM TREATMENT 35NOVEL APPROACHES IN SPINE SURGERY 36FORGING THE WAY IN DEEP BRAIN STIMULATION 38EDUCATING FOR TOMORROW 40ACADEMIC PROGRAMS AND NEW HIRES 42
24
28
18
12
02
LEA
DIN
G N
EUR
OS
CIEN
CES
Our extraordinary physicians and medical team at the Houston Methodist Neurological Institute and the Stanley H. Appel Department of Neurology have continued to provide the highest standard of diagnostic and clinical care in 2015. This clinical expertise is based on the translational and transformational research of our faculty, and has established us globally as a center of excellence. During the last year, we have focused our efforts on neurodegenerative diseases, including Alzheimer’s disease, Parkinson’s disease and amyotrophic lateral sclerosis (ALS), as well as cerebrovascular disease and stroke. This emphasis has brought us closer to understanding the pathogenesis of many devastating neurological diseases and prompted the initiation of many new therapies.
In patients with ALS, we have identified immune-mediated neuroinflammation as a potential target of interventional therapy. The loss of functional T-regulatory (Treg) lymphocytes accelerates ALS, and has formed the basis of a novel clinical trial in which we remove these Treg cells from ALS patients, expand them ex vivo, assure the restoration of their suppressive function, and transplant them back into the same patient from which they were removed. We are also studying the role of immunotherapy in patients with chronic inflammatory demyelinating polyneuropathy and myasthenia gravis, who exhibit dysfunction of Tregs.
The Nantz National Alzheimer Center maintains its position at the forefront of Alzheimer’s research with a number of clinical trials. One trial, the Anti-Amyloid Treatment in Asymptomatic Alzheimer’s (A4) study, is a landmark investigational clinical trial for the prevention or delay of memory loss in Alzheimer’s, administering a monoclonal antibody that targets beta amyloid in the brain, a known precursor of the disease. The Alzheimer’s center is working with our Concussion Center as well as General Electric (GE) and the National Football League (NFL) to develop magnetic resonance imaging (MRI) technology that will help detect traumatic brain injury at the time of concussion. Our aim is to achieve a better understanding of how concussion and traumatic brain injury lead to chronic traumatic encephalopathy, depression and dementia long after the injury has healed, with the ultimate goal of preventing the cataclysmic decline.
The Eddy Scurlock Stroke Center has continued its legacy of transformational therapies in stroke. We have participated in a study investigating the infusion of stem cells to provide benefit up to 48 hours post-ischemic stroke. We have partnered with Duke University in a phase I trial of umbilical stem cells and their therapeutic potential for cell reovery in stroke patients. Our latest and most innovative study has used transcranial magnetic stimulation to enhance recovery from debilitating stroke.
Our national and international status is made possible by highly motivated, committed physicians and medical staff who render superior patient care. Credit extends to our outstanding residents who perpetuate our educational mission to train the nation’s most promising leaders in neurology and translational neuroscience.
Stanley H. Appel, MDChair, Stanley H. Appel Department of Neurology Houston Methodist Neurological Institute
MESSAGE FROM THE STANLEY H. APPEL DEPARTMENT OF NEUROLOGY CHAIR
As chair of the Department of Neurosurgery, it is a privilege to be part of one of the busiest and largest neurosurgery programs in the nation. Our 17 neurosurgeons and two interventional neuroradiologists complete more than 5,000 cases a year. The combined total of cases is incredible when we look at our outcomes, which far exceed what is expected. The Houston Methodist Neurological Institute continues to rank in U.S. News & World Report’s “Best Hospitals” list and, in 2015, was No. 16 in neurology and neurosurgery. Our faculty members also include neurorehabilitation, pain management, psychiatry, neuro-oncology and interventional neuroradiology, who help provide outstanding services to our patients.
In 2015, our department continued to grow at all levels. We recruited Phillip Horner, PhD, a world-class stem cell biologist, to serve as vice chair of research and head of the neuroregenerative medicine program. We added Ivo Tremont, MD, as lead in neuro-oncology, Michelle Dang, MD, to pain services, and Inna D`Empaire, MD, to psychiatry.
Last year saw the approval of the Center for Restorative and Regenerative Neurosurgery to build on our current centers. Our Cerebrovascular Center provides our patients with an integrated, multidisciplinary group of surgeons, physicians and health professionals specifically trained in the realm of cerebrovascular disease. The team collectively has more experience in cerebrovascular disease than the vast majority of programs in the world. The experience and skills allow us to provide care for a large variety of cerebrovascular disorders, such as brain aneurysms, arteriovenous malformations, spinal vascular malformations, Moyamoya disease, cavernous malformations, brain tumors and stroke. We increasingly use a subcortical approach to explore new techniques in the resection of lesions in previously inoperable areas of the brain.
With the increase of minimally invasive therapies comes a paradigm shift in the way spinal disorders are treated. As part of the Spine Center, our spine surgeons are proficient in the use of advanced, image-guided, minimally invasive spine procedures, which increases successful outcomes and minimizes recovery times.
At the Kenneth R. Peak Center for Brain and Pituitary Tumor Treatment, headed by David Baskin, MD, we continue to tackle the cellular pathogenesis of brain cancer with chemotherapy-directed “smart bombs.” Specially bioengineered nanosyringes target the mitochondria in cancers and deliver up to three times the amount of a traditional chemotherapy dosage selectively into individual brain cancer cells. This center is on the road to becoming one of the premier brain tumor programs in the world.
We also continue to operate one of the busiest functional neurosurgery programs in the world, led by Richard Simpson, MD, in the provision of surgical options for Parkinson’s disease, movement dysfunction and chronic pain.
We have a strong commitment to training the next generation of neurosurgeons. Our outstanding neurosurgery residency program provides training in the highest standards of care, which is integrated throughout our top-level research and leading-edge technology. The large volume of cases make our residents outstanding surgeons. Our basic science research laboratories are expanding and now have a formal brain tumor, cerebrovascular and neuroregenerative medicine laboratories in addition to the exoskeleton work, flow dynamics and neuropsychology clinical laboratories.
From research to patient care to training our neurosurgeons of the future, the Houston Methodist Department of Neurosurgery remains stalwart in its commitment to leading medicine.
Gavin W. Britz, MD, MPH, MBA, FAANSChair, Department of Neurosurgery Houston Methodist Neurological Institute
MESSAGE FROM THE DEPARTMENT OF NEUROSURGERY CHAIR
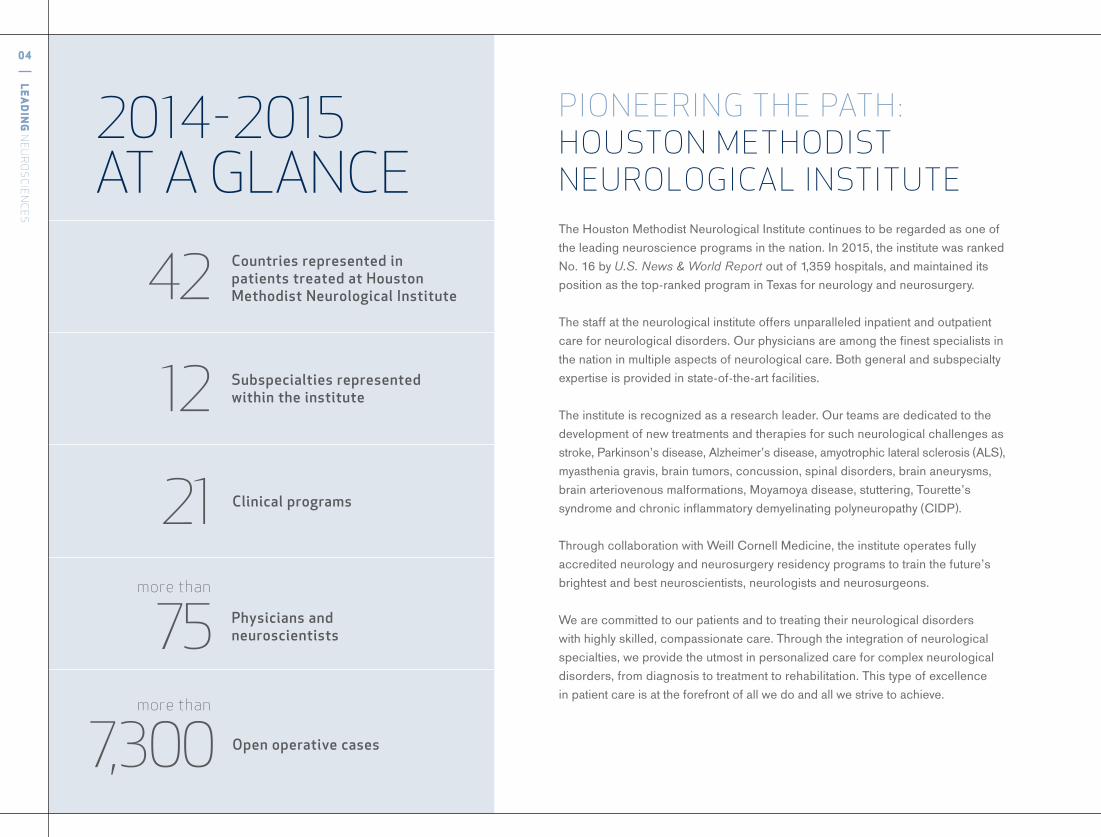
2014-2015 AT A GLANCE
more than
more than
Countries represented in patients treated at Houston Methodist Neurological Institute42
12
21
Subspecialties represented within the institute
Physicians and neuroscientists
Open operative cases7,300
75
Clinical programs
04
LEA
DIN
G N
EUR
OS
CIEN
CES
PIONEERING THE PATH: HOUSTON METHODIST NEUROLOGICAL INSTITUTEThe Houston Methodist Neurological Institute continues to be regarded as one of the leading neuroscience programs in the nation. In 2015, the institute was ranked No. 16 by U.S. News & World Report out of 1,359 hospitals, and maintained its position as the top-ranked program in Texas for neurology and neurosurgery.
The staff at the neurological institute offers unparalleled inpatient and outpatient care for neurological disorders. Our physicians are among the finest specialists in the nation in multiple aspects of neurological care. Both general and subspecialty expertise is provided in state-of-the-art facilities.
The institute is recognized as a research leader. Our teams are dedicated to the development of new treatments and therapies for such neurological challenges as stroke, Parkinson’s disease, Alzheimer’s disease, amyotrophic lateral sclerosis (ALS), myasthenia gravis, brain tumors, concussion, spinal disorders, brain aneurysms, brain arteriovenous malformations, Moyamoya disease, stuttering, Tourette’s syndrome and chronic inflammatory demyelinating polyneuropathy (CIDP).
Through collaboration with Weill Cornell Medicine, the institute operates fully accredited neurology and neurosurgery residency programs to train the future’s brightest and best neuroscientists, neurologists and neurosurgeons.
We are committed to our patients and to treating their neurological disorders with highly skilled, compassionate care. Through the integration of neurological specialties, we provide the utmost in personalized care for complex neurological disorders, from diagnosis to treatment to rehabilitation. This type of excellence in patient care is at the forefront of all we do and all we strive to achieve.
NEUROLOGY• Stanley H. Appel, MD
Chair, Stanley H. Appel Department of Neurology
• Tetsuo Ashizawa, MD• Mohammad Al Baeer, MD• David R. Beers, PhD• David Chiu, MD• Howard S. Derman, MD• Kasey Gildersleeve, MD• Santosh A. Helekar, MD, PhD• Eugene C. Lai, MD, PhD• Joseph C. Masdeu, MD, PhD• Brooke N. McQueen, MD• Amy Naquin-Chappel, MD• William G. Ondo, MD• Belen Pascual, PhD• Milvia Y. Pleitez, MD• Gustavo C. Román, MD, DrHC• David B. Rosenfield, MD• Sheetal Shroff, MD• Ericka P. Simpson, MD• R. Glenn Smith, MD, PhD• Bryan M. Spann, DO, PhD• Abraham P. Thomas, MD• Ron Tintner, MD• Amit Verma, MD• John J. Volpi, MD• Olga Waln, MD• Weihua Zhao, MD, PhD• Igor Cherches, MD• Everton Edmondson, MD• Randolph Evans, MD• Julia Jones, MD• Brian Loftus, MD• Steven Lovitt, MD• Greg McLauchlin, MD
NEUROSURGERY• Gavin W. Britz, MD, MPH, MBA, FAANS
Chair, Department of Neurosurgery• Glenn B. Anderson, MD• David Baskin, MD, FAANS, FACS• J. Bob Blacklock, MD• David Cech, MD• Eugene V. Golanov, MD, PhD• Robert G. Grossman, MD• Paul J. Holman, MD• Philip J. Horner, PhD• Christof Karmonik, PhD• Rob G. Parrish, MD, PhD• Martyn Sharpe, PhD• Richard Simpson Jr., MD, PhD• Gill E. Sviri, MD, MSc• Todd Trask, MD• G. Alexander West, MD, PhD• Jonathan Zhang, MD• Alfonso Aldama-Luebbert, MD• Taylor Gist, MD• Richard Harper, MD• Warren Parker, MD• Andrew C. Roeser, MD
NEUROPSYCHOLOGY• Veronica J. Burton, PhD• Mario Dulay, PhD• Kenneth Podell, PhD
NEURO-ONCOLOGY• Ivo Tremont, MD
NEURO -OPHTHALMOLOGY• Andrew G. Lee, MD• Sushma Yalamanchili, MD
INTERVENTIONAL NEURORADIOLOGY• Orlando Diaz, MD• Richard Klucznik, MD
NEURORADIOLOGY• Steve Fung, MD
NEUROREHABILITATION• Jenny M. Lai, MD• Purvi Desai, MD• Marie Frando, MD• Teresa D. Kaldis, MD• Lawrence H. Nguyen, MD• Luz Viviana Tastard, MD
PAIN MANAGEMENT• Michelle N. Dang, MD
PSYCHIATRY• Ranjit Chacko, MD• Inna D'Empaire, MD• Alric D. Hawkins, MD
NEUROPATHOLOGY• Suzanne Powell, MD• Andreana Rivera, MD• Hidehiro Takei, MD
NEUROLOGICAL INTENSIVE CARE• Anakara Sukumaran, MD• Michael Zwillman, MD
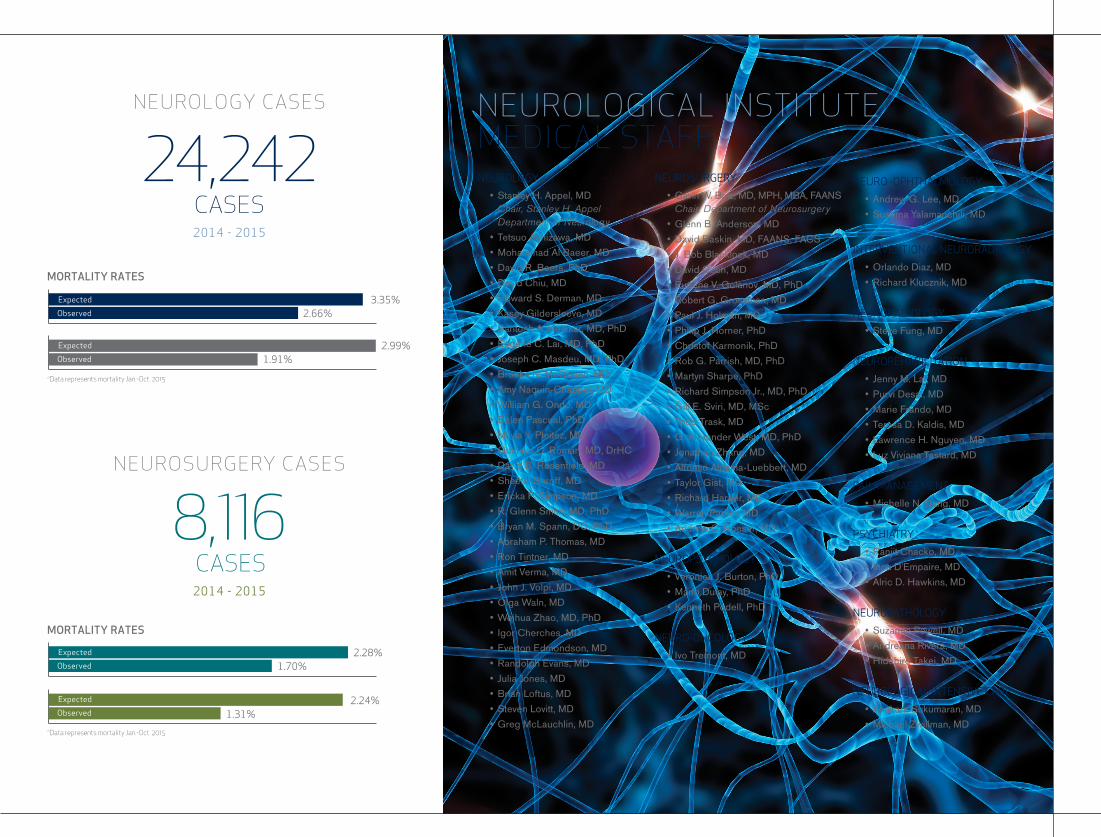
NEUROLOGICAL INSTITUTEMEDICAL STAFFMORTALITY RATES
MORTALITY RATES
*Data represents mortality Jan.-Oct. 2015
*Data represents mortality Jan.-Oct. 2015
2.28%1.70%
2.24%1.31%
3.35%2.66%
2.99%1.91%
Expected
Observed
Expected
Observed
Expected
Observed
Expected
Observed
MORTALITY RATES
MORTALITY RATES
*Data represents mortality Jan.-Oct. 2015
*Data represents mortality Jan.-Oct. 2015
2.28%1.70%
2.24%1.31%
3.35%2.66%
2.99%1.91%
Expected
Observed
Expected
Observed
Expected
Observed
Expected
Observed
8,116 CASES2014-2015
NEUROLOGY CASES
NEUROSURGERY CASES
24,242
CASES2014-2015
06
LEA
DIN
G N
EUR
OS
CIEN
CES
At the Houston Methodist Neurological Institute,
the comprehensive and integrative scope of
neuroimaging expands the boundaries of
diagnostic procedures and discovery every day.
Highly sophisticated technology coupled with
the skills and talents of our scientists and
physicians allow us to access the physiology of
the brain and its molecular biology in ways never
believed possible. These innovations allow us
to study and treat brain disease and the
consequences of injury.
LEADERS IN NEUROIMAGING
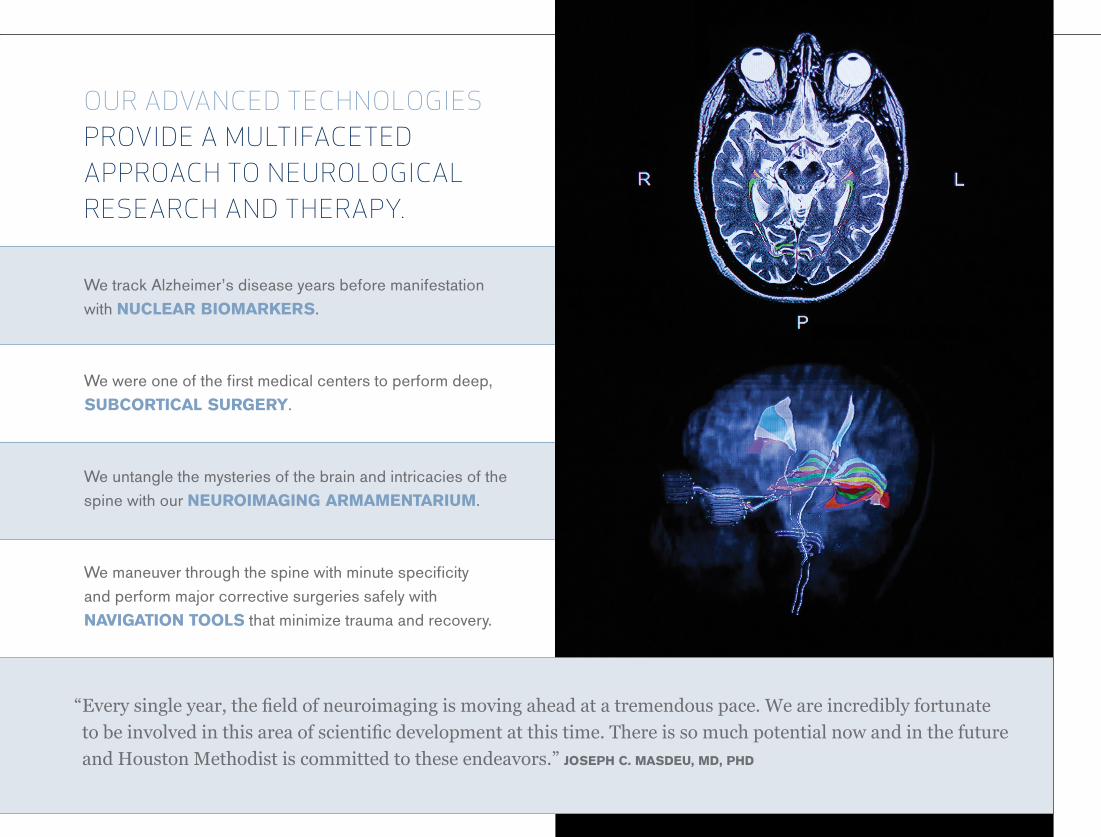
We track Alzheimer’s disease years before manifestation with NUCLEAR BIOMARKERS.
We were one of the first medical centers to perform deep, SUBCORTICAL SURGERY.
We untangle the mysteries of the brain and intricacies of the spine with our NEUROIMAGING ARMAMENTARIUM.
We maneuver through the spine with minute specificity and perform major corrective surgeries safely with NAVIGATION TOOLS that minimize trauma and recovery.
OUR ADVANCED TECHNOLOGIES PROVIDE A MULTIFACETED APPROACH TO NEUROLOGICAL RESEARCH AND THERAPY.
“Everysingleyear,thefieldofneuroimagingismovingaheadatatremendouspace.Weareincrediblyfortunate
tobeinvolvedinthisareaofscientificdevelopmentatthistime.Thereissomuchpotentialnowandinthefuture
andHoustonMethodistiscommittedtotheseendeavors.”JOSEPH C. MASDEU, MD, PHD
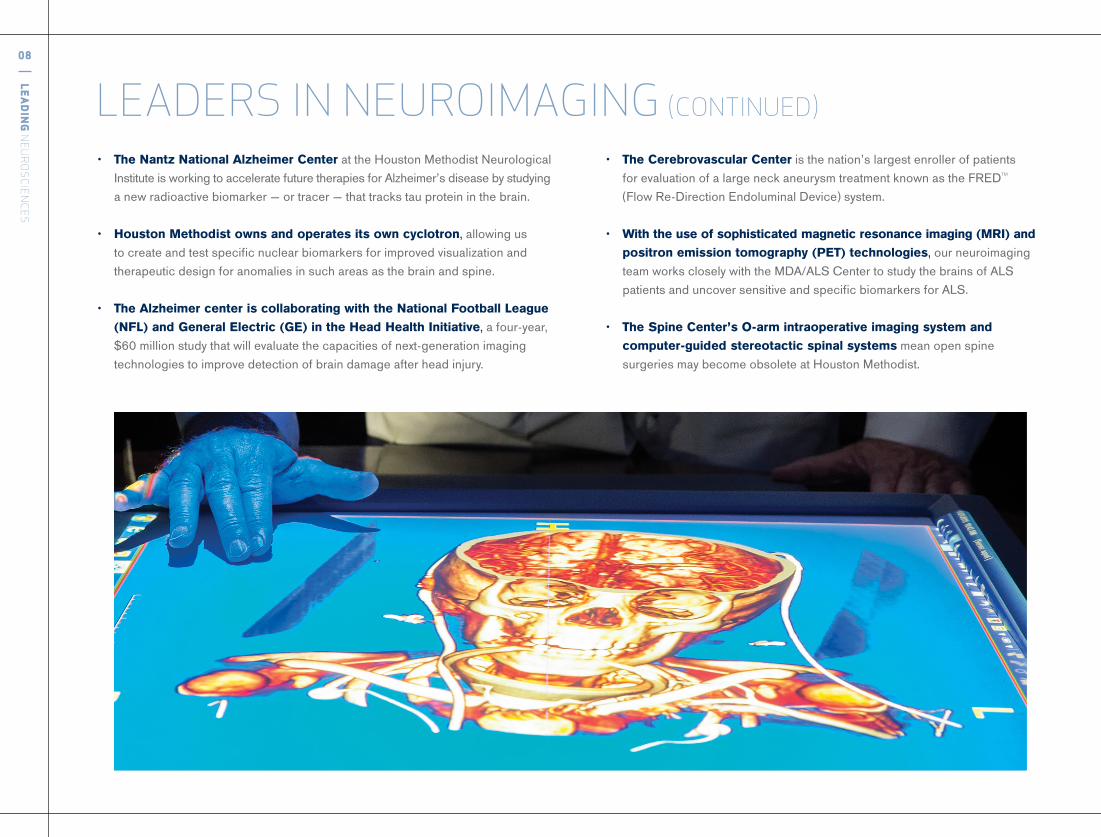
• The Nantz National Alzheimer Center at the Houston Methodist Neurological Institute is working to accelerate future therapies for Alzheimer’s disease by studying a new radioactive biomarker — or tracer — that tracks tau protein in the brain.
• Houston Methodist owns and operates its own cyclotron, allowing us to create and test specific nuclear biomarkers for improved visualization and therapeutic design for anomalies in such areas as the brain and spine.
• The Alzheimer center is collaborating with the National Football League (NFL) and General Electric (GE) in the Head Health Initiative, a four-year, $60 million study that will evaluate the capacities of next-generation imaging technologies to improve detection of brain damage after head injury.
08
LEA
DIN
G N
EUR
OS
CIEN
CES
• The Cerebrovascular Center is the nation’s largest enroller of patients for evaluation of a large neck aneurysm treatment known as the FRED™ (Flow Re-Direction Endoluminal Device) system.
• With the use of sophisticated magnetic resonance imaging (MRI) and positron emission tomography (PET) technologies, our neuroimaging team works closely with the MDA/ALS Center to study the brains of ALS patients and uncover sensitive and specific biomarkers for ALS.
• The Spine Center’s O-arm intraoperative imaging system and computer-guided stereotactic spinal systems mean open spine surgeries may become obsolete at Houston Methodist.
LEADERS IN NEUROIMAGING (CONTINUED)
10
LEA
DIN
G N
EUR
OS
CIEN
CES
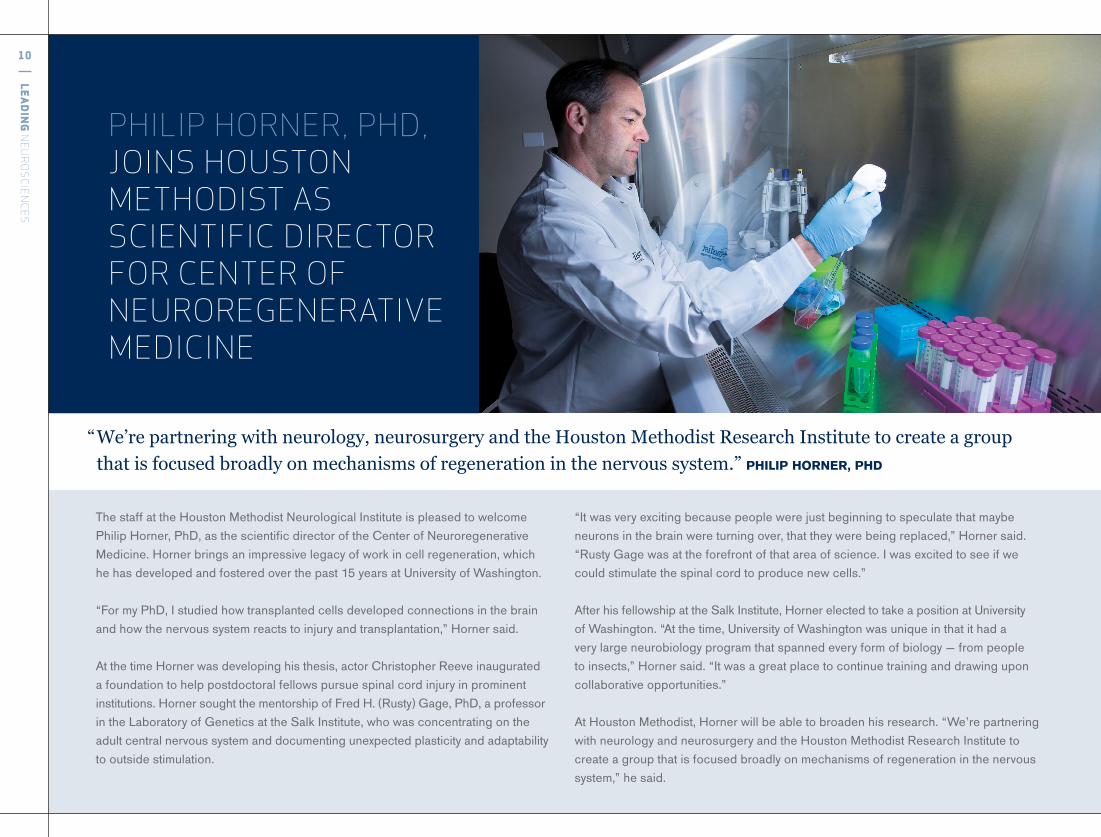
PHILIP HORNER, PHD, JOINS HOUSTON METHODIST AS SCIENTIFIC DIRECTOR FOR CENTER OF NEUROREGENERATIVE MEDICINE
The staff at the Houston Methodist Neurological Institute is pleased to welcome Philip Horner, PhD, as the scientific director of the Center of Neuroregenerative Medicine. Horner brings an impressive legacy of work in cell regeneration, which he has developed and fostered over the past 15 years at University of Washington.
“For my PhD, I studied how transplanted cells developed connections in the brain and how the nervous system reacts to injury and transplantation,” Horner said.
At the time Horner was developing his thesis, actor Christopher Reeve inaugurated a foundation to help postdoctoral fellows pursue spinal cord injury in prominent institutions. Horner sought the mentorship of Fred H. (Rusty) Gage, PhD, a professor in the Laboratory of Genetics at the Salk Institute, who was concentrating on the adult central nervous system and documenting unexpected plasticity and adaptability to outside stimulation.
“It was very exciting because people were just beginning to speculate that maybe neurons in the brain were turning over, that they were being replaced,” Horner said. “Rusty Gage was at the forefront of that area of science. I was excited to see if we could stimulate the spinal cord to produce new cells.”
After his fellowship at the Salk Institute, Horner elected to take a position at University of Washington. “At the time, University of Washington was unique in that it had a very large neurobiology program that spanned every form of biology — from people to insects,” Horner said. “It was a great place to continue training and drawing upon collaborative opportunities.”
At Houston Methodist, Horner will be able to broaden his research. “We’re partnering with neurology and neurosurgery and the Houston Methodist Research Institute to create a group that is focused broadly on mechanisms of regeneration in the nervous system,” he said.
“We’repartneringwithneurology,neurosurgeryandtheHoustonMethodistResearchInstitutetocreateagroup
thatisfocusedbroadlyonmechanismsofregenerationinthenervoussystem.”PHILIP HORNER, PHD
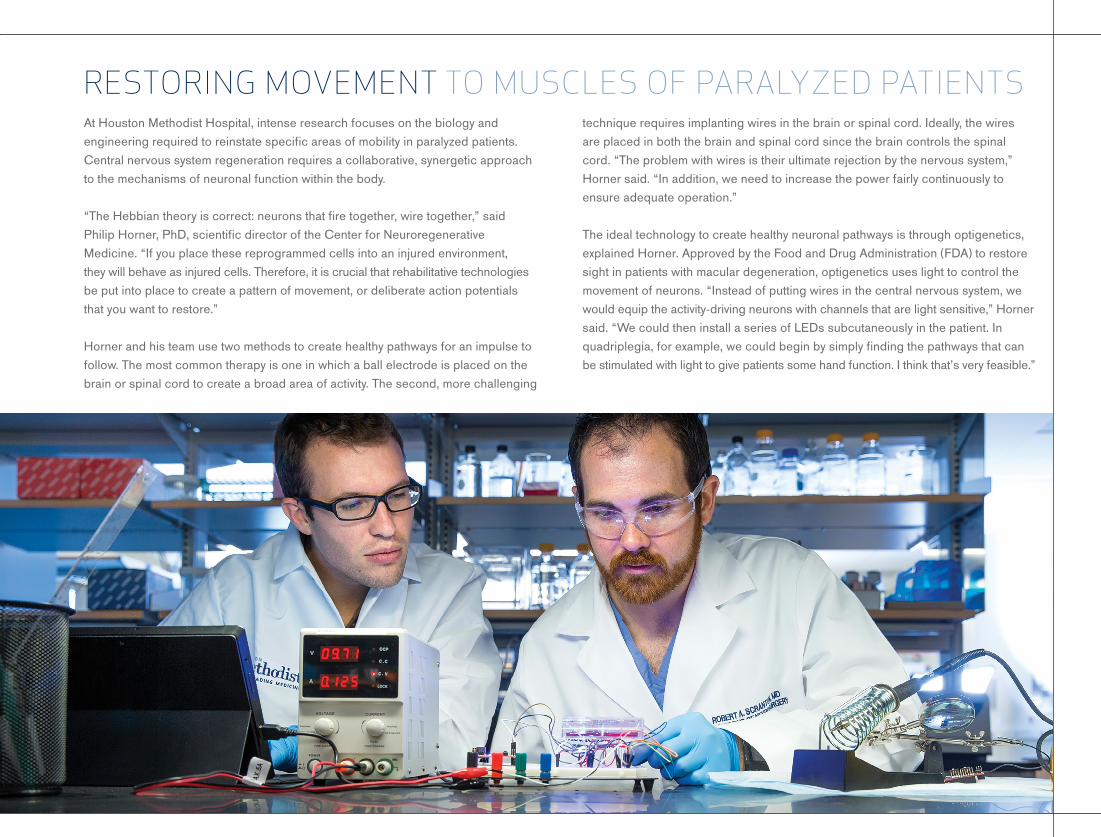
At Houston Methodist Hospital, intense research focuses on the biology and engineering required to reinstate specific areas of mobility in paralyzed patients. Central nervous system regeneration requires a collaborative, synergetic approach to the mechanisms of neuronal function within the body.
“The Hebbian theory is correct: neurons that fire together, wire together,” said Philip Horner, PhD, scientific director of the Center for Neuroregenerative Medicine. “If you place these reprogrammed cells into an injured environment, they will behave as injured cells. Therefore, it is crucial that rehabilitative technologies be put into place to create a pattern of movement, or deliberate action potentials that you want to restore.”
Horner and his team use two methods to create healthy pathways for an impulse to follow. The most common therapy is one in which a ball electrode is placed on the brain or spinal cord to create a broad area of activity. The second, more challenging
RESTORING MOVEMENT TO MUSCLES OF PARALYZED PATIENTStechnique requires implanting wires in the brain or spinal cord. Ideally, the wires are placed in both the brain and spinal cord since the brain controls the spinal cord. “The problem with wires is their ultimate rejection by the nervous system,” Horner said. “In addition, we need to increase the power fairly continuously to ensure adequate operation.”
The ideal technology to create healthy neuronal pathways is through optigenetics, explained Horner. Approved by the Food and Drug Administration (FDA) to restore sight in patients with macular degeneration, optigenetics uses light to control the movement of neurons. “Instead of putting wires in the central nervous system, we would equip the activity-driving neurons with channels that are light sensitive,” Horner said. “We could then install a series of LEDs subcutaneously in the patient. In quadriplegia, for example, we could begin by simply finding the pathways that can be stimulated with light to give patients some hand function. I think that’s very feasible.”
Withthisadvancedtechnology,neurosurgeonscansafelymaneuverthroughthefoldsandfragilefibersofthebrain.
12
LEA
DIN
G N
EUR
OS
CIEN
CES
houstonmethodist.org/ni
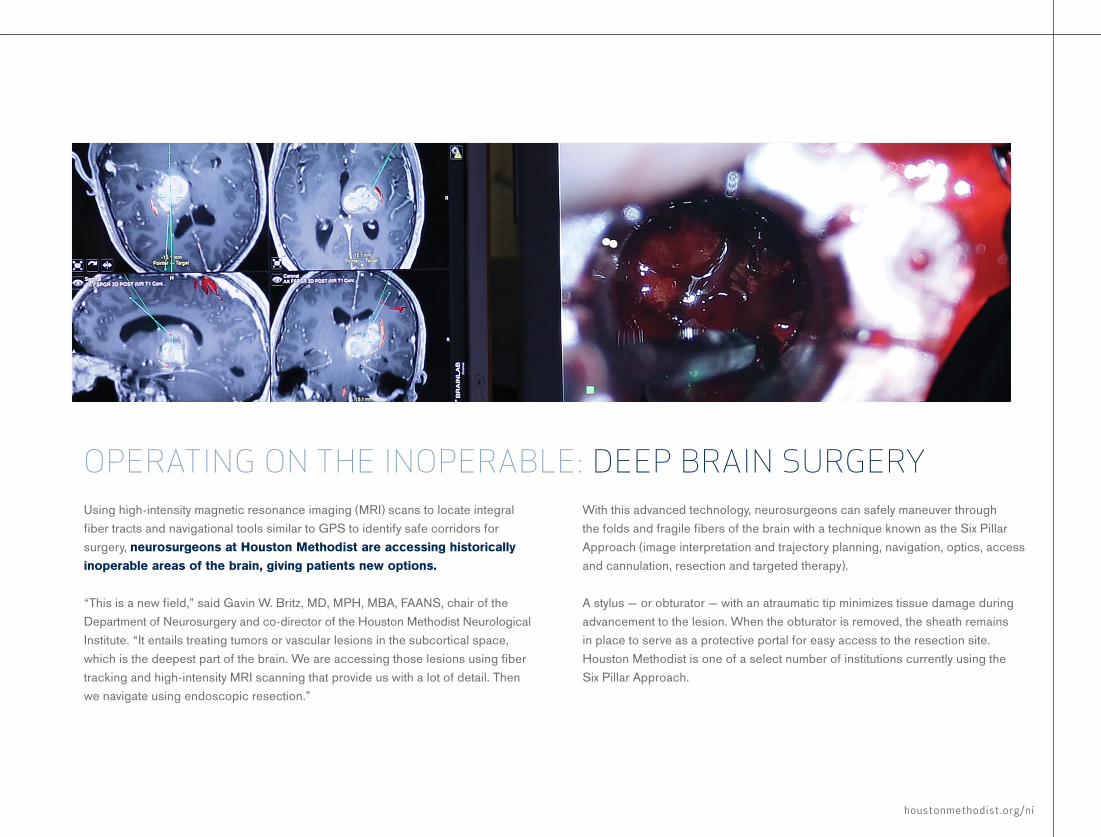
Using high-intensity magnetic resonance imaging (MRI) scans to locate integral fiber tracts and navigational tools similar to GPS to identify safe corridors for surgery, neurosurgeons at Houston Methodist are accessing historically inoperable areas of the brain, giving patients new options.
“This is a new field,” said Gavin W. Britz, MD, MPH, MBA, FAANS, chair of the Department of Neurosurgery and co-director of the Houston Methodist Neurological Institute. “It entails treating tumors or vascular lesions in the subcortical space, which is the deepest part of the brain. We are accessing those lesions using fiber tracking and high-intensity MRI scanning that provide us with a lot of detail. Then we navigate using endoscopic resection.”
OPERATING ON THE INOPERABLE: DEEP BRAIN SURGERYWith this advanced technology, neurosurgeons can safely maneuver through the folds and fragile fibers of the brain with a technique known as the Six Pillar Approach (image interpretation and trajectory planning, navigation, optics, access and cannulation, resection and targeted therapy).
A stylus — or obturator — with an atraumatic tip minimizes tissue damage during advancement to the lesion. When the obturator is removed, the sheath remains in place to serve as a protective portal for easy access to the resection site. Houston Methodist is one of a select number of institutions currently using the Six Pillar Approach.
14
LEA
DIN
G N
EUR
OS
CIEN
CES
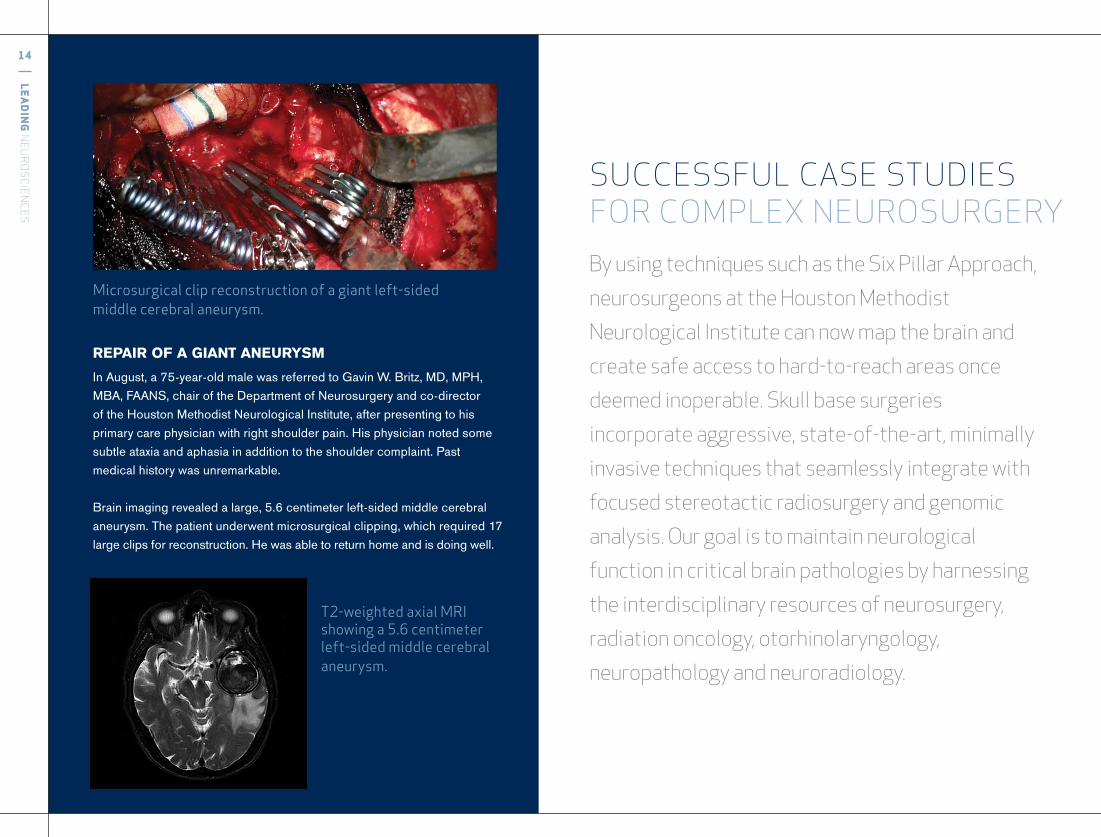
REPAIR OF A GIANT ANEURYSM In August, a 75-year-old male was referred to Gavin W. Britz, MD, MPH, MBA, FAANS, chair of the Department of Neurosurgery and co-director of the Houston Methodist Neurological Institute, after presenting to his primary care physician with right shoulder pain. His physician noted some subtle ataxia and aphasia in addition to the shoulder complaint. Past medical history was unremarkable.
Brain imaging revealed a large, 5.6 centimeter left-sided middle cerebral aneurysm. The patient underwent microsurgical clipping, which required 17 large clips for reconstruction. He was able to return home and is doing well.
SUCCESSFUL CASE STUDIES FOR COMPLEX NEUROSURGERYBy using techniques such as the Six Pillar Approach,
neurosurgeons at the Houston Methodist
Neurological Institute can now map the brain and
create safe access to hard-to-reach areas once
deemed inoperable. Skull base surgeries
incorporate aggressive, state-of-the-art, minimally
invasive techniques that seamlessly integrate with
focused stereotactic radiosurgery and genomic
analysis. Our goal is to maintain neurological
function in critical brain pathologies by harnessing
the interdisciplinary resources of neurosurgery,
radiation oncology, otorhinolaryngology,
neuropathology and neuroradiology.
Microsurgicalclipreconstructionofagiantleft-sidedmiddlecerebralaneurysm.
T2-weightedaxialMRIshowinga5.6centimeterleft-sidedmiddlecerebralaneurysm.
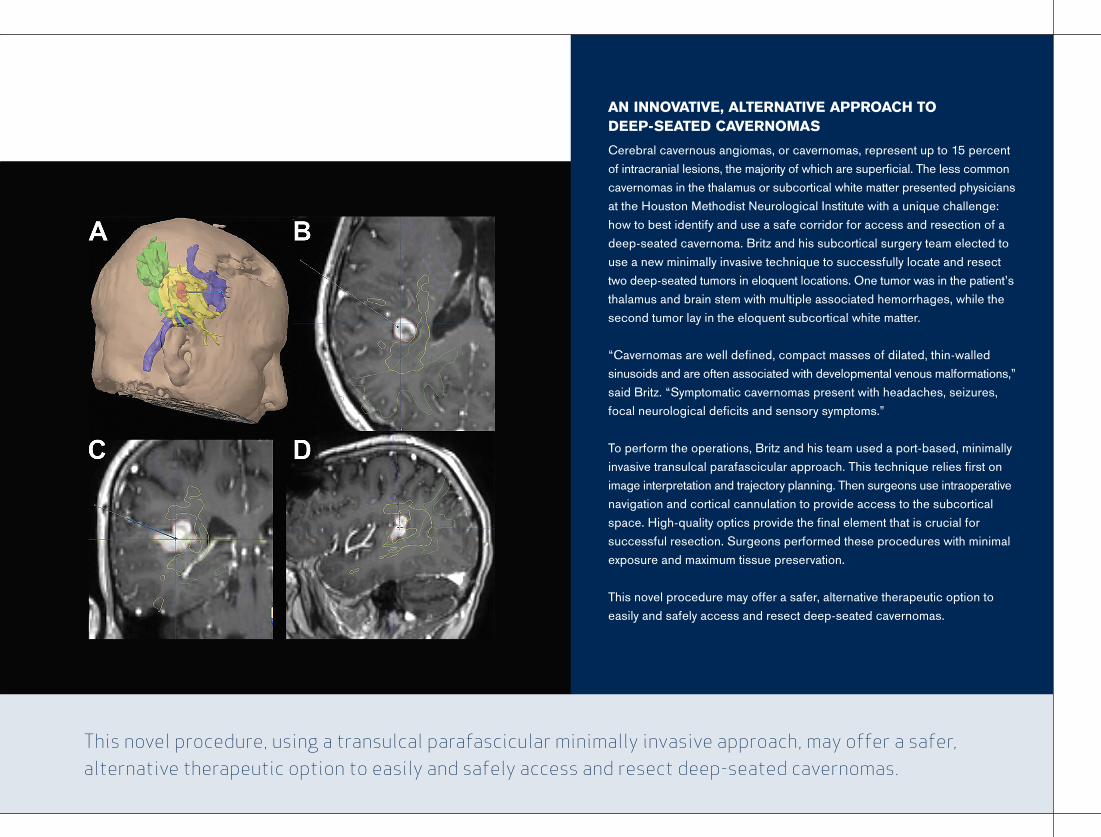
AN INNOVATIVE, ALTERNATIVE APPROACH TO DEEP-SEATED CAVERNOMASCerebral cavernous angiomas, or cavernomas, represent up to 15 percent of intracranial lesions, the majority of which are superficial. The less common cavernomas in the thalamus or subcortical white matter presented physicians at the Houston Methodist Neurological Institute with a unique challenge: how to best identify and use a safe corridor for access and resection of a deep-seated cavernoma. Britz and his subcortical surgery team elected to use a new minimally invasive technique to successfully locate and resect two deep-seated tumors in eloquent locations. One tumor was in the patient’s thalamus and brain stem with multiple associated hemorrhages, while the second tumor lay in the eloquent subcortical white matter.
“Cavernomas are well defined, compact masses of dilated, thin-walled sinusoids and are often associated with developmental venous malformations,” said Britz. “Symptomatic cavernomas present with headaches, seizures, focal neurological deficits and sensory symptoms.”
To perform the operations, Britz and his team used a port-based, minimally invasive transulcal parafascicular approach. This technique relies first on image interpretation and trajectory planning. Then surgeons use intraoperative navigation and cortical cannulation to provide access to the subcortical space. High-quality optics provide the final element that is crucial for successful resection. Surgeons performed these procedures with minimal exposure and maximum tissue preservation.
This novel procedure may offer a safer, alternative therapeutic option to easily and safely access and resect deep-seated cavernomas.
This novel procedure, using a transulcal parafascicular minimally invasive approach, may offer a safer, alternative therapeutic option to easily and safely access and resect deep-seated cavernomas.
16
LEA
DIN
G N
EUR
OS
CIEN
CES
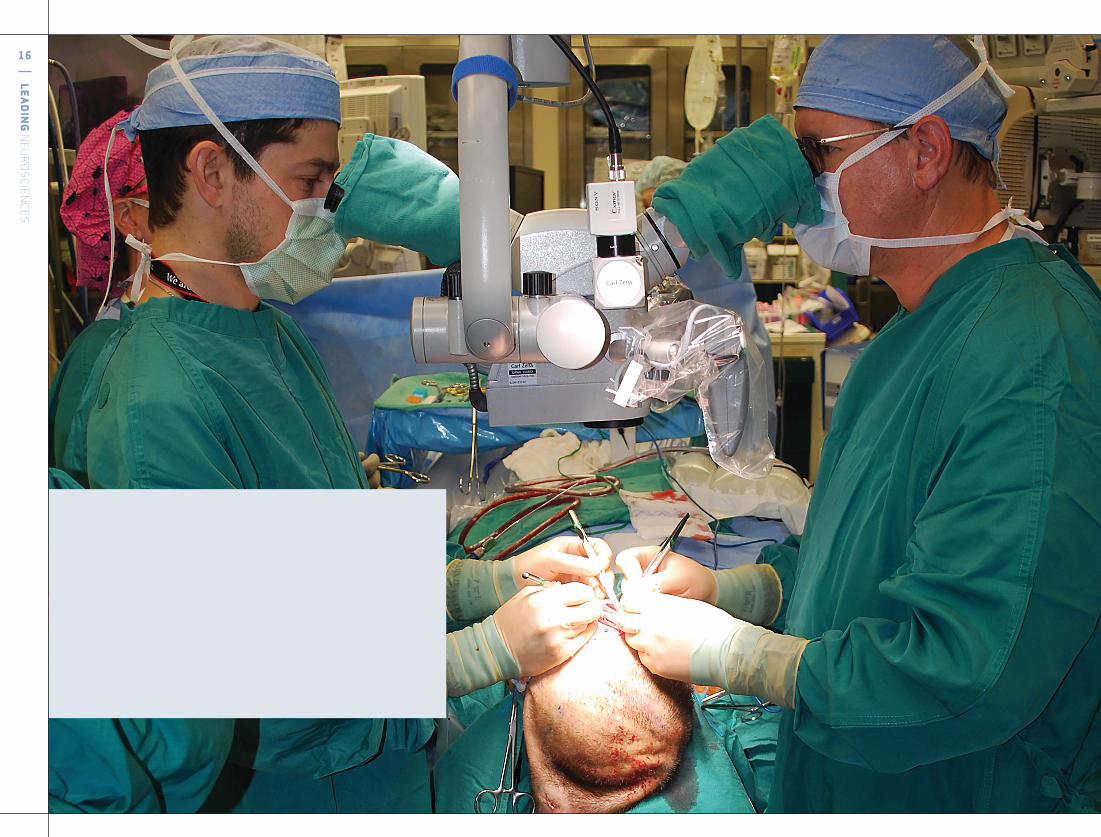
Thesurgeriesrequiredtheskillsofmorethan50healthcareprofessionalsinamarathonoperationthatlastedmorethan15hours.
houstonmethodist.org/ni
In a landmark transplant event, surgical teams from Houston Methodist and The University of Texas MD Anderson Cancer Center came together to perform the world’s first scalp and skull transplant while also transplanting a kidney and pancreas. The surgeries required the skills of more than 50 health care professionals in a marathon operation that lasted more than 15 hours.
The patient, James Boysen, was a 55-year-old software developer from Austin, Texas. He was successfully treated for leiomyosarcoma in 2006, which left a patch of dead bone and a deep wound on his head that penetrated the full thickness of his skull down to his brain. Boysen previously received a double organ transplant of a kidney and pancreas in 1992, due to comorbidities associated with diabetes. When these organs began to fail, a second solid organ transplant was not possible due to his scalp and skull wound. Paradoxically, the immunosuppression drugs compromised the healing of the head wound.
“The area of the skull that required the transplant was anatomically challenging because it was directly over the sagittal sinus and a critical blood vessel, which, if injured or damaged, could be a big problem,” said Todd W. Trask, MD, Houston Methodist neurosurgeon. “After some intricate carpentry to get the donor bone to fit the area of the skull, I inserted little plates and screws to hold the bone in place. Then the plastic surgeon took over.”
Transplant surgery for composite tissue has never before been done simultaneously with solid organ transplantation. Boysen is doing quite well posttransplant.
A HISTORICAL FIRST: SCALP AND SOLID ORGAN TRANSPLANT
Thisisthefirsttimetransplantsurgeryforcompositetissuehasbeenperformedsimultaneouslywithsolidorgantransplantation.
18
LEA
DIN
G N
EUR
OS
CIEN
CES
EducatingforTomorrow
Houston Methodist is revolutionizing the way cancer is treated. At the Kenneth R. Peak Center for Brain and Pituitary Tumor Treatment and Research, Director David S. Baskin, MD, heads an extensive research program to study and treat human glioblastoma, the most aggressive and common form of malignant primary brain tumors.
Baskin and his team, in collaboration with the Rice University Center for Nanoscale Science, are developing very tiny syringe-like delivery vehicles for the treatment of brain cancer, including glioblastoma.
“We’ve developed a nanosyringe that will make injections selectively into individual brain cancer cells,” Baskin said.
To create this nanosyringe, the team builds a nontoxic structure with antioxidant properties. The interior of the nanotube is lipophilic and hydrophobic. Chemotherapy drugs that have been redesigned with similar lipophilic and hydrophobic properties are placed inside the nanotube. Because the structure is hydrophobic, the
MITOCHONDRIAL SMART BOMBS: EFFECTIVELY TARGETING BRAIN TUMORS
chemotherapeutic agents are securely held inside the nanotubes in the aqueous environment of the bloodstream. Peptide sequences, designed to bind to antigens on the surface of tumor-specific cancer cells, are adsorbed onto the exterior of the nanosyringe. Upon contact with the cell membrane, the nanotube’s lipophilic and hydrophobic components transfer into the lipophilic and hydrophobic portions of the cancer cell membrane, thus creating a type of nanoinjection.
Nanosyringes have been tested in cell culture and in immunocompromised murine models that have been injected with human glioblastoma cells. In all models, the nanosyringes have demonstrated high efficacy with no discernable toxicity. “Additional cancer cell lines have been tested in these models, including triple negative breast cancer, pancreatic cancer, non-small-cell lung cancer and ovarian cancer, and the results are similarly extremely positive,” Baskin said.
Perhaps equally important, the nanosyringes can be used to counteract a common mechanism of chemotherapy resistance.
“Many cancers develop and upregulate drug pumps that actually pump the chemotherapeutic agent back out of the cell before it can kill the cancer cell,” Baskin said. “The nanosyringes can be used to selectively poison these drug pumps and prevent the expulsion of the chemotherapeutic agent from the cell.” In studies conducted in Peak Center laboratories, drug pumps incapacitated with nanosyringes can increase chemotherapeutic efficacy almost tenfold, permitting the use of a fraction of the normal dose and markedly reducing side effects of the drugs.
In studies conducted in Peak Center laboratories, drug pumps incapacitated with nanosyringes can increase chemotherapeutic efficacy almost tenfold, permitting the use of a fraction of the normal dose and markedly reducing side effects of the drugs.
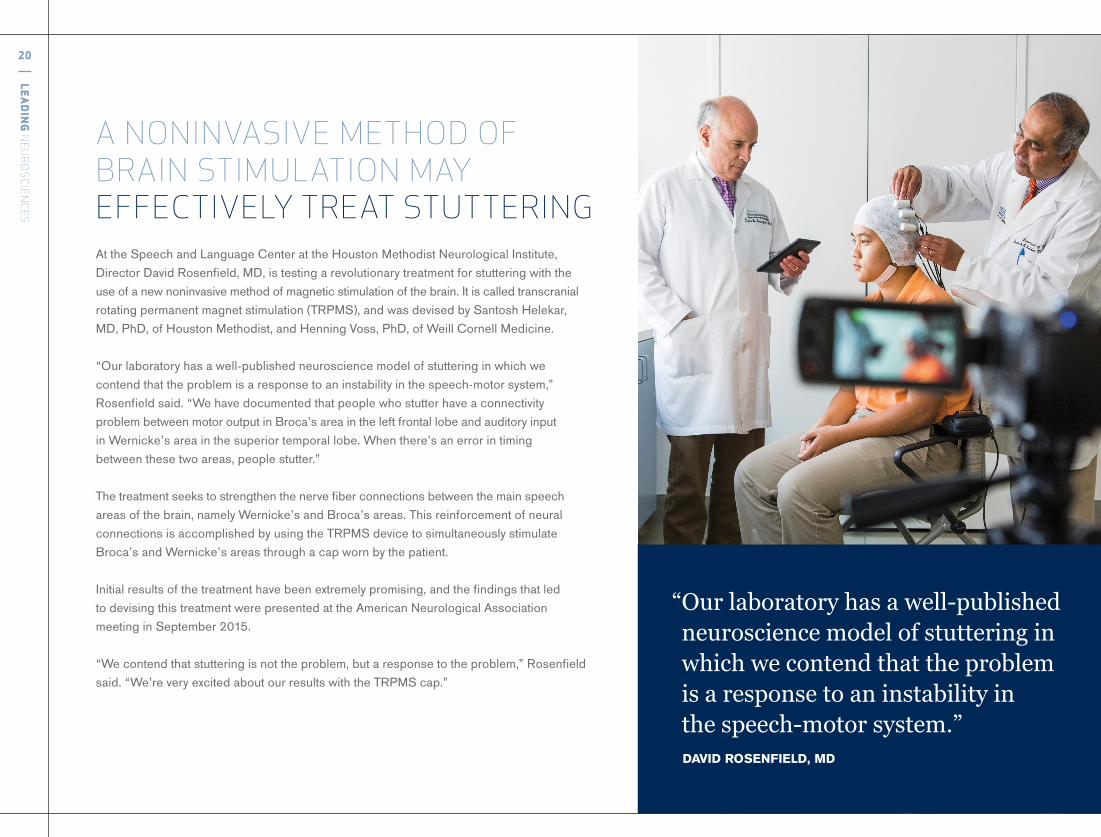
At the Speech and Language Center at the Houston Methodist Neurological Institute, Director David Rosenfield, MD, is testing a revolutionary treatment for stuttering with the use of a new noninvasive method of magnetic stimulation of the brain. It is called transcranial rotating permanent magnet stimulation (TRPMS), and was devised by Santosh Helekar, MD, PhD, of Houston Methodist, and Henning Voss, PhD, of Weill Cornell Medicine.
“Our laboratory has a well-published neuroscience model of stuttering in which we contend that the problem is a response to an instability in the speech-motor system,” Rosenfield said. “We have documented that people who stutter have a connectivity problem between motor output in Broca’s area in the left frontal lobe and auditory input in Wernicke’s area in the superior temporal lobe. When there’s an error in timing between these two areas, people stutter.”
The treatment seeks to strengthen the nerve fiber connections between the main speech areas of the brain, namely Wernicke’s and Broca’s areas. This reinforcement of neural connections is accomplished by using the TRPMS device to simultaneously stimulate Broca’s and Wernicke’s areas through a cap worn by the patient.
Initial results of the treatment have been extremely promising, and the findings that led to devising this treatment were presented at the American Neurological Association meeting in September 2015.
“We contend that stuttering is not the problem, but a response to the problem,” Rosenfield said. “We’re very excited about our results with the TRPMS cap.”
A NONINVASIVE METHOD OF BRAIN STIMULATION MAY EFFECTIVELY TREAT STUTTERING
“Ourlaboratoryhasawell-publishedneurosciencemodelofstutteringinwhichwecontendthattheproblemisaresponsetoaninstabilityin thespeech-motorsystem.”
DAVID ROSENFIELD, MD
20
LEA
DIN
G N
EUR
OS
CIEN
CES
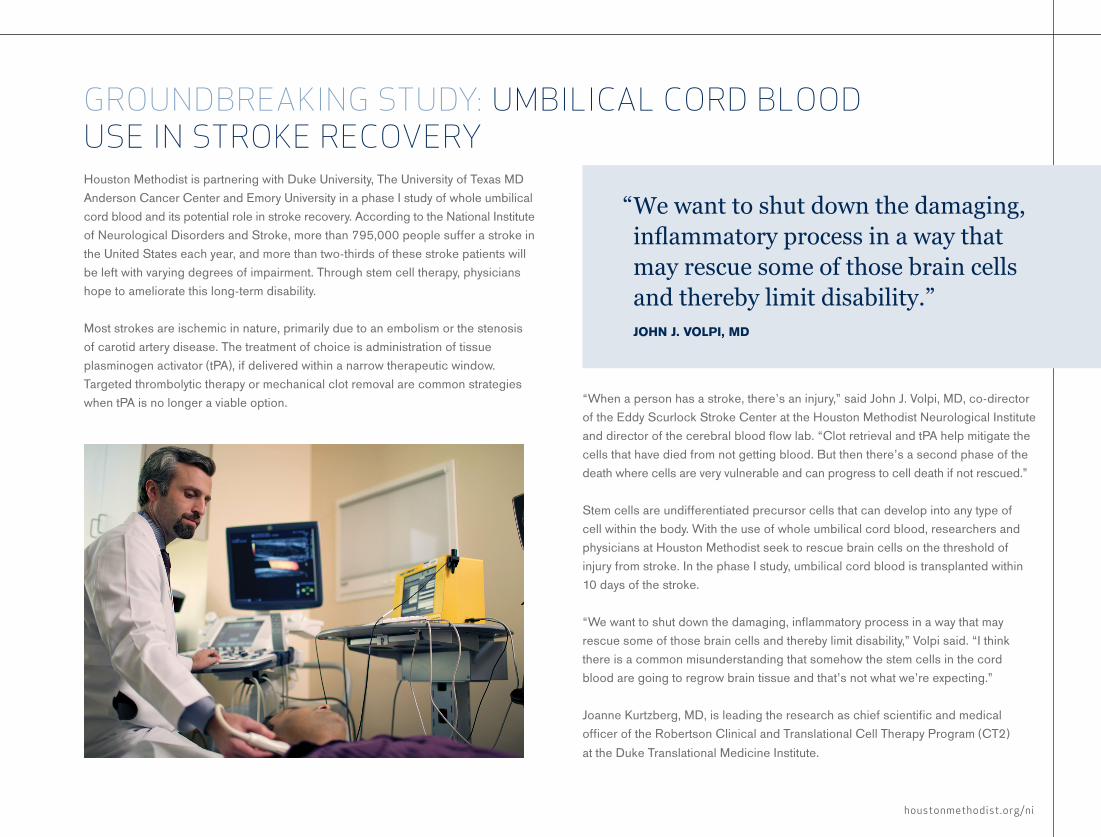
Houston Methodist is partnering with Duke University, The University of Texas MD Anderson Cancer Center and Emory University in a phase I study of whole umbilical cord blood and its potential role in stroke recovery. According to the National Institute of Neurological Disorders and Stroke, more than 795,000 people suffer a stroke in the United States each year, and more than two-thirds of these stroke patients will be left with varying degrees of impairment. Through stem cell therapy, physicians hope to ameliorate this long-term disability.
Most strokes are ischemic in nature, primarily due to an embolism or the stenosis of carotid artery disease. The treatment of choice is administration of tissue plasminogen activator (tPA), if delivered within a narrow therapeutic window. Targeted thrombolytic therapy or mechanical clot removal are common strategies when tPA is no longer a viable option. “When a person has a stroke, there’s an injury,” said John J. Volpi, MD, co-director
of the Eddy Scurlock Stroke Center at the Houston Methodist Neurological Institute and director of the cerebral blood flow lab. “Clot retrieval and tPA help mitigate the cells that have died from not getting blood. But then there’s a second phase of the death where cells are very vulnerable and can progress to cell death if not rescued.”
Stem cells are undifferentiated precursor cells that can develop into any type of cell within the body. With the use of whole umbilical cord blood, researchers and physicians at Houston Methodist seek to rescue brain cells on the threshold of injury from stroke. In the phase I study, umbilical cord blood is transplanted within 10 days of the stroke.
“We want to shut down the damaging, inflammatory process in a way that may rescue some of those brain cells and thereby limit disability,” Volpi said. “I think there is a common misunderstanding that somehow the stem cells in the cord blood are going to regrow brain tissue and that’s not what we’re expecting.”
Joanne Kurtzberg, MD, is leading the research as chief scientific and medical officer of the Robertson Clinical and Translational Cell Therapy Program (CT2) at the Duke Translational Medicine Institute.
GROUNDBREAKING STUDY: UMBILICAL CORD BLOOD USE IN STROKE RECOVERY
“Wewanttoshutdownthedamaging,inflammatoryprocessinawaythatmayrescuesomeofthosebraincellsandtherebylimitdisability.”
JOHN J. VOLPI, MD
houstonmethodist.org/ni

22
LEA
DIN
G N
EUR
OS
CIEN
CES
houstonmethodist.org/ni
At Houston Methodist, physicians and scientists are closer to understanding Alzheimer’s disease with the study of a new radioactive biomarker, or tracer, that can track abnormal levels and tangles of abnormal tau protein in the brain with positron emission tomography (PET) scans.
Recent studies have shown that tau may be a more definitive indication of Alzheimer’s disease than beta amyloid.
The Nantz National Alzheimer’s Center at the Houston Methodist Neurological Institute is one of the first U.S. medical centers to test this newly discovered radioactive tau tracer, called [18F]AV-1451.
“A PET tau tracer is extremely useful to measure brain changes in people with Alzheimer’s,” said Joseph C. Masdeu, MD, PhD, director of the Alzheimer center and principal investigator for this tracer application. “We have found that areas of the brain that contain excess abnormal tau have decreased metabolic activity, meaning they work poorly. Tau PET gives us an objective picture of the brain damage caused by the disease.”
Tracers labeled with fluorine-18 [18F]AV-1451 are easier to use than those labeled with carbon-11 because fluorine-18 has a longer half-life. This allows the tracer to be transported from the cyclotron, where the synthesis occurs, to relatively distant injection locations. [18F]AV-1451 will be used to detect the neurofibrillary tangles that are aggregates of hyperphosphorylated tau.
NEW TAU TRACER IMPROVES ALZHEIMER’S DISEASE TRACKING
TheNantzNationalAlzheimer’sCenterattheHoustonMethodistNeurologicalInstituteisoneofthefirstU.S.medicalcenterstotestthisnewlydiscoveredradioactivetraceroftau,called[18F]AV-1451.
The Nantz National Alzheimer Center at Houston Methodist Neurological Institute is part of a national breakthrough clinical trial focused on an investigational treatment to prevent or delay the onset of the memory loss characteristic of Alzheimer’s disease in people predisposed to this disorder. The A4 study, also known as the Anti-Amyloid Treatment in Asymptomatic Alzheimer’s study, is for individuals ages 65 to 85 who may be at risk for memory loss related to Alzheimer’s disease, but who have no outward signs of the disease and have normal thinking and memory abilities.
According to the Alzheimer’s Association, 5.3 million Americans have Alzheimer’s disease, and an estimated 5.1 million of these individuals are 65 years of age or older. Alzheimer’s is the sixth leading cause of death in the United States. Among the top 10 ranked morbidities, it is the only one that cannot be prevented, cured or slowed in its progression.
The investigational treatment used in A4 is solanezumab, a monoclonal antibody that targets the excess beta amyloid in the brain. The goal of the study is to slow possible Alzheimer’s-related damage in the brain and delay symptoms of memory loss.
Using positron emission tomography (PET), researchers and clinicians have found that beta amyloid forms plaques in the brains of people with Alzheimer’s 10-20 years before they exhibit initial symptoms. Scientists believe accumulation of amyloid
FIGHTING ALZHEIMER’S DISEASE AT ALL STAGESplays a key role in the eventual development of Alzheimer’s-related memory loss by inducing the excess production in the brain of another hallmark protein: an abnormal form of the protein tau.
The team is led by Joseph C. Masdeu, MD, PhD, director of the Alzheimer center and principal investigator of the A4 study at Houston Methodist. The center will be one of a handful of study sites to scan patients for abnormal tau, which forms tangles of fibers that likely destroy nerve cells and spread brain damage.
“It is encouraging to be able to detect excess amyloid with PET technology in people predisposed to Alzheimer’s and then try to lower it with solanezumab,” Masdeu said. “But there appears to be a point in the development of Alzheimer’s disease where removing amyloid does not reverse or arrest disease progression, because too much abnormal tau has already been generated. For this reason, it is important to use PET to measure the amount of abnormal brain tau as well.”
Approximately 1,000 adults are expected to participate in more than 60 study sites across the United States, Canada and Australia. The three-year study is funded by the National Institute on Aging, Eli Lilly and Company, and several philanthropic organizations. The A4 study is coordinated by the Alzheimer’s Disease Cooperative Study (ADCS).
TheNantzNationalAlzheimerCenteratHoustonMethodistNeurologicalInstituteispartofanationalbreakthroughclinicaltrialfocusedonaninvestigationaltreatmenttopreventordelaytheonsetofthememorylosscharacteristicofAlzheimer’sinpeoplepredisposedtothisdisorder.
24
LEA
DIN
G N
EUR
OS
CIEN
CES
“HoustonMethodististheonlystudy locationinTexastoofferthisrandomized,double-blind,placebo-controlledstudy. Ourgoalistofindoutifthisdrugisa viableoptionforourpatients.” JOSEPH C. MASDEU, MD, PHD
NOBLE CLINICAL TRIAL Physicians and researchers at the Alzheimer center are working to slow the progression of brain cell deterioration in patients with mild to moderate Alzheimer’s disease through the NOBLE clinical trial.
Initiated by the ADCS, NOBLE will compare the neuroprotective profile of T-817MA, a neuroprotective drug that acts on beta amyloid-induced neurotoxicity and memory deficits, to placebo in 450 patients with mild to moderate Alzheimer’s. Patients must have a current six-month drug history of taking donepezil (Aricept®) or donepezil or rivastigmine (Exelon), with or without memantine (NamendaTM) for symptom management.
Using biomarkers, PET has shown that abnormal amounts of beta amyloid are evident in the brain as early as 20 years before initial symptoms develop. In previous studies, T-817MA has been shown to mitigate amyloid-induced learning deficits in experimental Alzheimer’s models.
Houston Methodist is the only study location in Texas to offer this randomized, double-blind, placebo-controlled study. Approximately two-thirds of study participants will receive T-817MA.
“Previous studies in murine models have shown this drug may prevent the destruction of brain cells, which would result in improved memory and cognition,” said Joseph C. Masdeu, MD, PhD, principal investigator of this study and director of the Alzheimer center. “Our goal is to find out if this drug is a viable option for our patients.”
The NOBLE study is sponsored by Toyama Chemical Co., Ltd., and FUJIFILM Group, and is being conducted by ADCS. Supported by the National Institute on Aging, ADCS is the largest Alzheimer’s disease therapeutic research consortium in the United States. Approximately 50 clinical sites nationwide will offer the study to patients with mild to moderate Alzheimer’s. Houston Methodist expects to enroll approximately 20 patients.
26
LEA
DIN
G N
EUR
OS
CIEN
CES
The Cerebrovascular Center at the Houston Methodist Neurological Institute is dedicated to continuously advancing stroke treatment and preventing poststroke disability. Clinical trials underway at the center seek to improve pharmacologic and procedural therapies for the more than 795,000 people in the United States who will experience a stroke this year.
Houston Methodist is one of approximately 60 sites currently participating in the Systematic Evaluation of Patients Treated with Neurothrombectomy Devices for Acute Ischemic Stroke Registry (STRATIS), led by Richard P. Klucznik, MD, medical director of interventional radiology at Houston Methodist and co-director of the cerebrovascular center. Funded by Covidian, STRATIS will evaluate the use of Covidien endovascular stroke devices in patients diagnosed with acute ischemic stroke. The Solitaire 2 revascularization device is Covidien’s most recent mechanism for stroke treatment.
LARGE CLOT REMOVAL IN ISCHEMIC STROKE“The Solitaire device is a stent that goes up inside the clot and expands. As it expands, it catches the clot, which we can then pull out,” Klucznik said. “If this doesn’t fully evacuate the clot, we can use another device, like a suction apparatus, to help get the clot out.”
Candidates for this registry will have a large vessel blockage that is refractory to treatment with tPA due to the size of the clot.
“The study requires that the clot be blocking a major blood vessel to a hemisphere or to the basilar artery at the back of the head,” Klucznik said. “Our time restriction with the Solitaire device is also wider than with tPA. We have about a six-hour window.”
The STRATIS registry is a prospective, multicenter, non-randomized, observational registry with an expected enrollment of 1,000 patients.
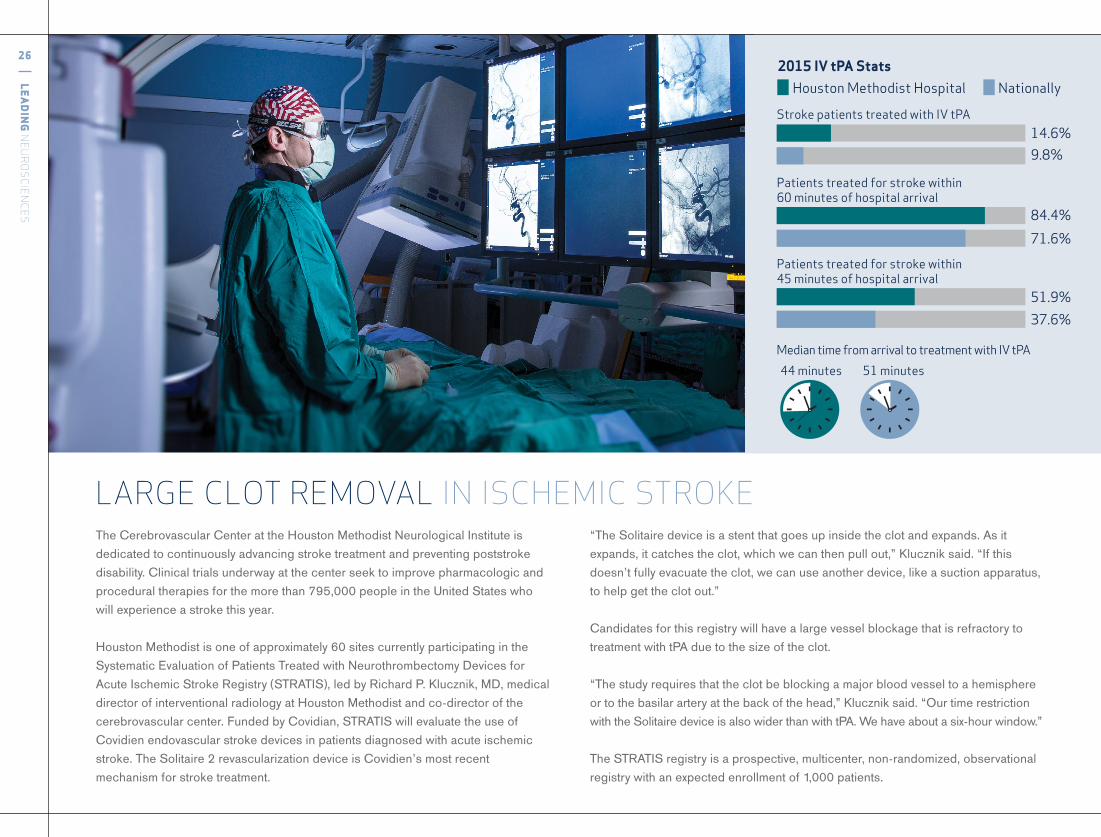
9.8%
84.4%
71.6%
51.9%
37.6%
Stroke patients treated with IV tPA
Patients treated for stroke within 60 minutes of hospital arrival
Patients treated for stroke within 45 minutes of hospital arrival
44 minutes 51 minutes
14.6%
Houston Methodist Hospital Nationally
Median time from arrival to treatment with IV tPA
2015 IV tPA Stats
houstonmethodist.org/ni
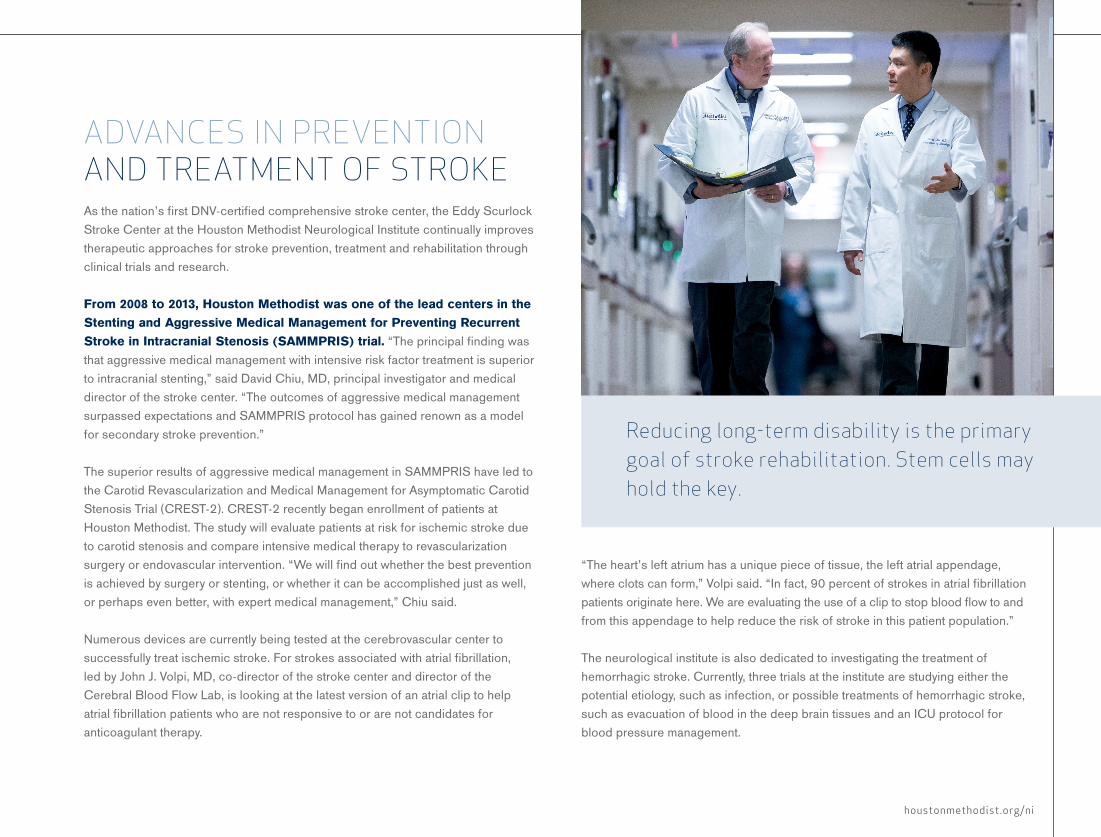
As the nation’s first DNV-certified comprehensive stroke center, the Eddy Scurlock Stroke Center at the Houston Methodist Neurological Institute continually improves therapeutic approaches for stroke prevention, treatment and rehabilitation through clinical trials and research.
From 2008 to 2013, Houston Methodist was one of the lead centers in the Stenting and Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial. “The principal finding was that aggressive medical management with intensive risk factor treatment is superior to intracranial stenting,” said David Chiu, MD, principal investigator and medical director of the stroke center. “The outcomes of aggressive medical management surpassed expectations and SAMMPRIS protocol has gained renown as a model for secondary stroke prevention.”
The superior results of aggressive medical management in SAMMPRIS have led to the Carotid Revascularization and Medical Management for Asymptomatic Carotid Stenosis Trial (CREST-2). CREST-2 recently began enrollment of patients at Houston Methodist. The study will evaluate patients at risk for ischemic stroke due to carotid stenosis and compare intensive medical therapy to revascularization surgery or endovascular intervention. “We will find out whether the best prevention is achieved by surgery or stenting, or whether it can be accomplished just as well, or perhaps even better, with expert medical management,” Chiu said.
Numerous devices are currently being tested at the cerebrovascular center to successfully treat ischemic stroke. For strokes associated with atrial fibrillation, led by John J. Volpi, MD, co-director of the stroke center and director of the Cerebral Blood Flow Lab, is looking at the latest version of an atrial clip to help atrial fibrillation patients who are not responsive to or are not candidates for anticoagulant therapy.
“The heart’s left atrium has a unique piece of tissue, the left atrial appendage, where clots can form,” Volpi said. “In fact, 90 percent of strokes in atrial fibrillation patients originate here. We are evaluating the use of a clip to stop blood flow to and from this appendage to help reduce the risk of stroke in this patient population.”
The neurological institute is also dedicated to investigating the treatment of hemorrhagic stroke. Currently, three trials at the institute are studying either the potential etiology, such as infection, or possible treatments of hemorrhagic stroke, such as evacuation of blood in the deep brain tissues and an ICU protocol for blood pressure management.
ADVANCES IN PREVENTION AND TREATMENT OF STROKE
Reducing long-term disability is the primary goal of stroke rehabilitation. Stem cells may hold the key.

28
LEA
DIN
G N
EUR
OS
CIEN
CES
A multidisciplinary team of researchers and physicians at the Houston Methodist Neurological Institute, led by Stanley H. Appel, MD, director of the institute and chair of the Stanley H. Appel Department of Neurology, has continued its intensive investigations into the etiology and pathophysiology of amyotrophic lateral sclerosis (ALS). Multiple mechanisms of motor neuron injury have been implicated based on the more than 30 different genetic causes of familial ALS. The Houston Methodist Research Insitute team in the Edwards ALS Research Laboratory has focused its efforts on the neuroinflammation in patients with these genetic mutations, as well as in the majority of sporadic cases with no known mutation. The underlying hypothesis is that regardless of how neuronal injury begins, immune-mediated neuroinflammation dictates the final common pathway and is a target for potential therapeutic intervention.
“We used a genetic murine model of human ALS to define the potential roles of the innate immune microglia and the adaptive immune T cells,” Appel said. “During early stages in the murine model, the disease progresses slowly, and protective microglia (M2) and T cells (regulatory T cells/Th2 Treg) predominate, while in later rapid progression of disease, proinflammatory microglia (M1) and T cells (Th1) predominate.
“To determine the role of T cells, researchers David Beers and Jenny Henkel in our group crossed the transgenic murine model with one that had no T cells. Death ensued earlier rather than later, which was not what we anticipated. We assumed the T cells were detrimental, but it turns out the opposite is true:
T CELLS SUPPRESS PROGRESSION OF DISEASE IN ALS PATIENTS
T cells are protective. In fact, a subpopulation of T cells, regulatory T lymphocytes (Tregs), actually suppress disease progression.”
In the murine model, decreased Treg cells were associated with more rapid progression; transplanting Tregs into the transgenic murine models dramatically slowed disease and prolonged survival.
To determine whether immune parameters in ALS patients were similar to the murine models, Jenny Henkel, PhD, investigated the levels of Treg in ALS patients and found that decreased Tregs were associated with faster progression and shorter survival. These findings suggest that increasing the number and function of Tregs could have a therapeutic benefit for patients.
Based on these novel findings, a therapeutic trial of Treg is planned and will be carried out in collaboration with Merit Cudkowicz, MD, and her team at the Massachusetts General Hospital Department of Neurology. The study is sponsored by ALSFindingaCure, funded by the Ruzzuto Foundation and GE.
“We are currently carrying out the necessary validation of our Treg expansion in collaboration with Dr. Katy Rezvani and Dr. Elizabeth Shpall, both of The University of Texas MD Anderson Cancer Center. We will then submit our application to the FDA seeking approval to transplant healthy cells back into the same patient,” Appel said. “After all of our hard work over many years, we are excited about the opportunity to benefit our very deserving ALS patients.”
“WeassumedtheTcellsweredetrimental,butitturnsouttheoppositeistrue:Tcellsareprotective.”STANLEY H. APPEL, MD
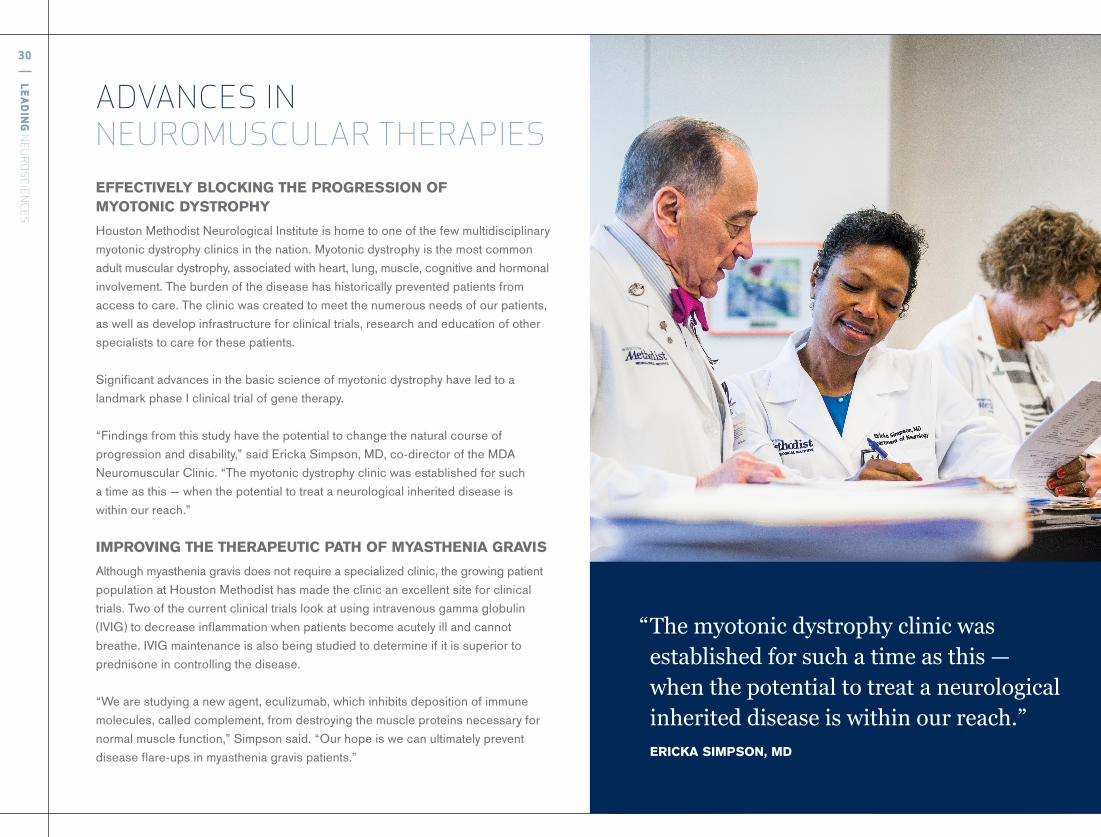
EFFECTIVELY BLOCKING THE PROGRESSION OF MYOTONIC DYSTROPHY Houston Methodist Neurological Institute is home to one of the few multidisciplinary myotonic dystrophy clinics in the nation. Myotonic dystrophy is the most common adult muscular dystrophy, associated with heart, lung, muscle, cognitive and hormonal involvement. The burden of the disease has historically prevented patients from access to care. The clinic was created to meet the numerous needs of our patients, as well as develop infrastructure for clinical trials, research and education of other specialists to care for these patients.
Significant advances in the basic science of myotonic dystrophy have led to a landmark phase I clinical trial of gene therapy.
“Findings from this study have the potential to change the natural course of progression and disability,” said Ericka Simpson, MD, co-director of the MDA Neuromuscular Clinic. “The myotonic dystrophy clinic was established for such a time as this — when the potential to treat a neurological inherited disease is within our reach.”
IMPROVING THE THERAPEUTIC PATH OF MYASTHENIA GRAVIS Although myasthenia gravis does not require a specialized clinic, the growing patient population at Houston Methodist has made the clinic an excellent site for clinical trials. Two of the current clinical trials look at using intravenous gamma globulin (IVIG) to decrease inflammation when patients become acutely ill and cannot breathe. IVIG maintenance is also being studied to determine if it is superior to prednisone in controlling the disease.
“We are studying a new agent, eculizumab, which inhibits deposition of immune molecules, called complement, from destroying the muscle proteins necessary for normal muscle function,” Simpson said. “Our hope is we can ultimately prevent disease flare-ups in myasthenia gravis patients.”
ADVANCES IN NEUROMUSCULAR THERAPIES
“Themyotonicdystrophyclinicwasestablishedforsuchatimeasthis— whenthepotentialtotreataneurologicalinheriteddiseaseiswithinourreach.”ERICKA SIMPSON, MD
30
LEA
DIN
G N
EUR
OS
CIEN
CES
NEW TRIALS FOR THE TREATMENT OF CIDP Simpson and her team are actively collecting data in a study of the potential benefits of Treg cells and the autoantibody response in chronic inflammatory demyelinating polyneuropathy (CIDP). It is believed that the pathogenesis of CIDP could result from a combination of cell-mediated and humoral mechanisms acting together to generate an atypical response and ultimately damage peripheral nerves.
“We are demonstrating that Tregs, which are associated with decreased inflammation, correlate with clinical improvement,” Simpson said. “When Tregs are decreased, the disease becomes more pronounced and active. When these cells are increased with immunoglobulin treatment, motor function is enhanced.”
Simpson and the neuromuscular clinic team continue to evaluate subcutaneous administration of IVIG, which potentially provides more steady state concentrations in the body. In addition, because current IVIG therapy is complex and costly, subcutaneous administration might prove more accessible for patients.
The neuromuscular center has recently partnered with the Houston Methodist Foundation to establish the Ronald and Julie Dokell CIDP/Neuromuscular Clinic and Research Division to advance clinical research and care for CIDP patients. “Our goal is to build a clinical research center not only to treat patients, but also to conduct clinical trials and studies,” Simpson said. “We will operate the CIDP center with the same philosophy and style that has been so successful for our ALS clinic.”
“WhenTregsaredecreased,thediseasebecomesmorepronouncedandactive.Whenthesecellsareincreasedwithimmunoglobulintreatment,motorfunctionisenhanced.” ERICKA SIMPSON, MD
Houston Methodist Hospital is collaborating with the National Football League (NFL) and General Electric (GE) in a four-year, $60 million initiative to evaluate the capacities of next-generation imaging technologies to accelerate detection of brain damage after head injury. More than a million people are treated for traumatic brain injuries (TBI) each year in the United States.
Known as the Head Health Initiative, this endeavor will focus on improving the diagnostic capability of magnetic resonance imaging (MRI) in mild head trauma, and will be guided by an advisory board comprising multidisciplinary medical professionals from several institutions. The Nantz National Alzheimer Center at the Houston Methodist Neurological Institute has been selected as one of three locations in the United States to participate in the first phase of this project.
DIAGNOSING CONCUSSION IMMEDIATELY: HEAD HEALTH INITIATIVE
32
LEA
DIN
G N
EUR
OS
CIEN
CES
“Theinvestigationaltechnologylooksattheentirebraintodeterminebiomarkersforpotentialdiagnosis,outcomepredictionandtherapymanagement forpatientswithmildTBI.” JOSEPH C. MASDEU, MD, PHD
LEADING THE WAY IN CONCUSSION PREVENTION AND TREATMENTThe Houston Methodist Concussion Center is one of the nation’s leading facilities for recognition, treatment, outreach services and research in brain trauma. The center unites industry leaders, professional sports organizations and a highly skilled collective medical team to offer comprehensive evaluation and treatment for TBI, with an emphasis on sports-related concussion.
“In sports-related head injuries, it is important to consider the cervical spine, the skull, the visual system and the balance system, in addition to the brain,” Podell said. “Any one of these areas can be affected in any combination.”
AMONG THE COUNTRY’S LARGEST OUTREACH PROGRAMS Providing education about proper assessment and care of the sports-related head injury is a top priority for the concussion center. With collaborative support from GE and the Houston Texans, the center is home to one of the largest U.S. outreach programs for sports-related head injuries. Approximately 50 athletic trainers work closely with regional junior high and high schools, as well as amateur and professional sports groups in southeast Texas to educate parents, athletic directors and athletes on injury prevention and detection.
“Not only do we educate hundreds of coaches, athletic trainers, health care professionals, parents and student athletes each year about concussions, but we started a Return to Learn program, where we go to different schools to educate the teachers and administrators on helping students return to school after a sports concussion,” Podell said.
Joseph C. Masdeu, MD, PhD, director of the Alzheimer center, is the principal investigator for Houston Methodist and is a member of the advisory board.
Concussions are among the most difficult injuries for physicians to diagnose and treat because current imaging technology typically cannot detect the presence of a mild TBI. The first phase of this project, led by GE, is designed to improve the diagnostic capability of MRI for mild head trauma.
Masdeu and the Alzheimer center team are working closely with the Houston Methodist Concussion Center, under the leadership of Kenneth Podell, PhD, to identify potential patients for this clinical study.
“For every 100 individuals who have a concussion, about 40 will have residual problems a year later,” Masdeu said. “Some suffer from depression or are just not as functional as they were before. We do not yet fully understand what happens in the brains of those 40 people after concussion. The attempt of this study is to improve MRI so that we can detect changes in the brain immediately.
“The investigational technology looks at the entire brain to determine biomarkers for potential diagnosis, outcome prediction and therapy management for patients with mild TBI.”
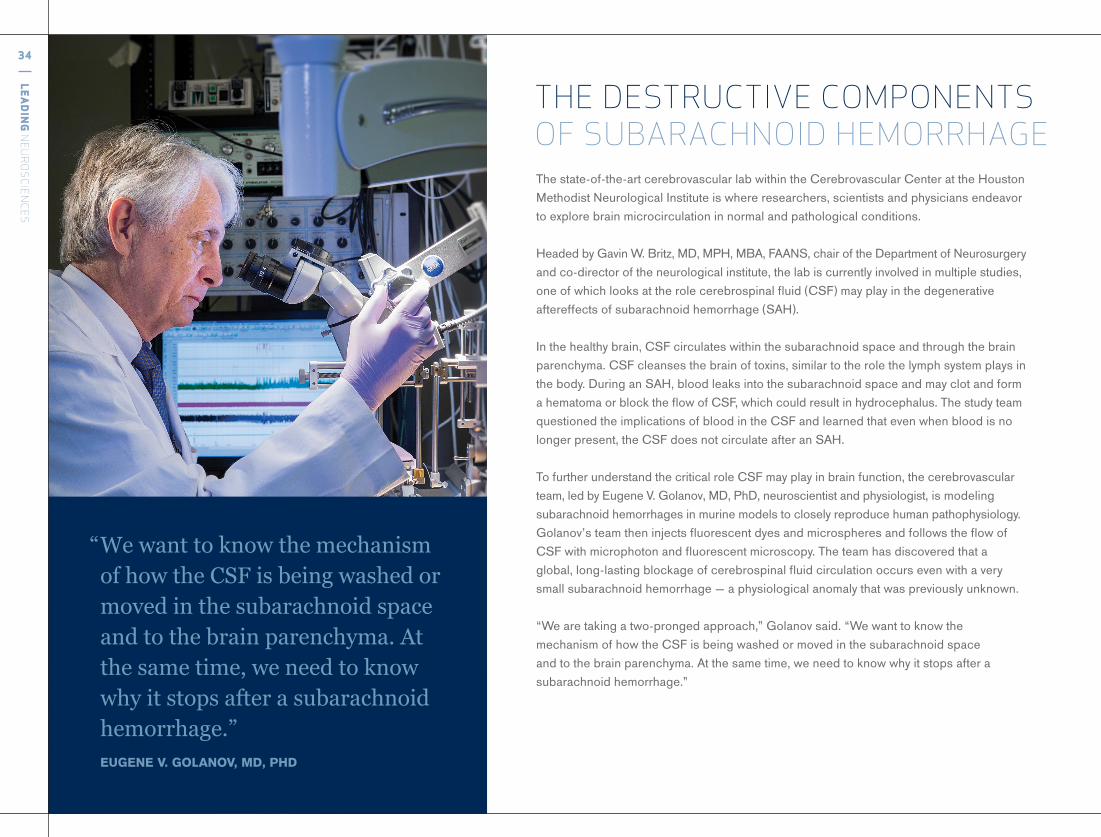
The state-of-the-art cerebrovascular lab within the Cerebrovascular Center at the Houston Methodist Neurological Institute is where researchers, scientists and physicians endeavor to explore brain microcirculation in normal and pathological conditions.
Headed by Gavin W. Britz, MD, MPH, MBA, FAANS, chair of the Department of Neurosurgery and co-director of the neurological institute, the lab is currently involved in multiple studies, one of which looks at the role cerebrospinal fluid (CSF) may play in the degenerative aftereffects of subarachnoid hemorrhage (SAH).
In the healthy brain, CSF circulates within the subarachnoid space and through the brain parenchyma. CSF cleanses the brain of toxins, similar to the role the lymph system plays in the body. During an SAH, blood leaks into the subarachnoid space and may clot and form a hematoma or block the flow of CSF, which could result in hydrocephalus. The study team questioned the implications of blood in the CSF and learned that even when blood is no longer present, the CSF does not circulate after an SAH.
To further understand the critical role CSF may play in brain function, the cerebrovascular team, led by Eugene V. Golanov, MD, PhD, neuroscientist and physiologist, is modeling subarachnoid hemorrhages in murine models to closely reproduce human pathophysiology. Golanov’s team then injects fluorescent dyes and microspheres and follows the flow of CSF with microphoton and fluorescent microscopy. The team has discovered that a global, long-lasting blockage of cerebrospinal fluid circulation occurs even with a very small subarachnoid hemorrhage — a physiological anomaly that was previously unknown.
“We are taking a two-pronged approach,” Golanov said. “We want to know the mechanism of how the CSF is being washed or moved in the subarachnoid space and to the brain parenchyma. At the same time, we need to know why it stops after a subarachnoid hemorrhage.”
THE DESTRUCTIVE COMPONENTS OF SUBARACHNOID HEMORRHAGE
“WewanttoknowthemechanismofhowtheCSFisbeingwashedormovedinthesubarachnoidspaceandtothebrainparenchyma.Atthesametime,weneedtoknowwhyitstopsafterasubarachnoidhemorrhage.”
EUGENE V. GOLANOV, MD, PHD
34
LEA
DIN
G N
EUR
OS
CIEN
CES
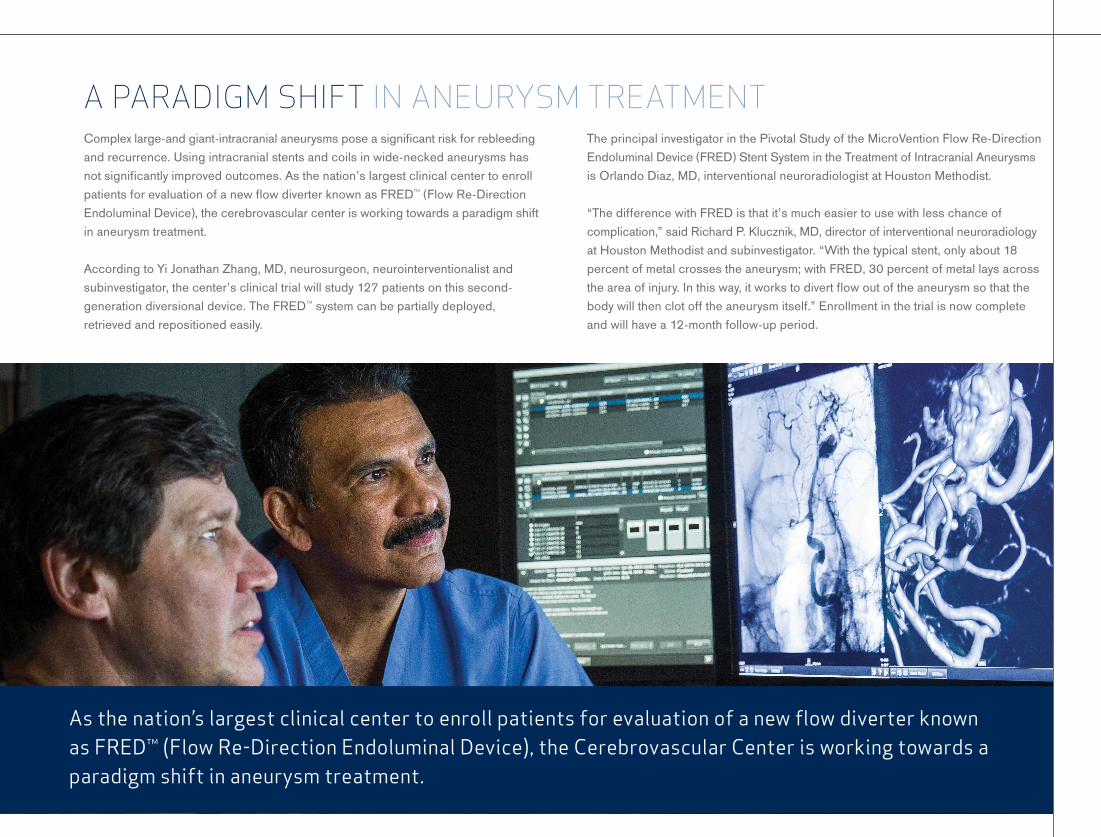
Complex large-and giant-intracranial aneurysms pose a significant risk for rebleeding and recurrence. Using intracranial stents and coils in wide-necked aneurysms has not significantly improved outcomes. As the nation’s largest clinical center to enroll patients for evaluation of a new flow diverter known as FRED™ (Flow Re-Direction Endoluminal Device), the cerebrovascular center is working towards a paradigm shift in aneurysm treatment.
According to Yi Jonathan Zhang, MD, neurosurgeon, neurointerventionalist and subinvestigator, the center’s clinical trial will study 127 patients on this second-generation diversional device. The FRED™ system can be partially deployed, retrieved and repositioned easily.
The principal investigator in the Pivotal Study of the MicroVention Flow Re-Direction Endoluminal Device (FRED) Stent System in the Treatment of Intracranial Aneurysms is Orlando Diaz, MD, interventional neuroradiologist at Houston Methodist.
“The difference with FRED is that it’s much easier to use with less chance of complication,” said Richard P. Klucznik, MD, director of interventional neuroradiology at Houston Methodist and subinvestigator. “With the typical stent, only about 18 percent of metal crosses the aneurysm; with FRED, 30 percent of metal lays across the area of injury. In this way, it works to divert flow out of the aneurysm so that the body will then clot off the aneurysm itself.” Enrollment in the trial is now complete and will have a 12-month follow-up period.
A PARADIGM SHIFT IN ANEURYSM TREATMENT
Asthenation’slargestclinicalcentertoenrollpatientsforevaluationofanewflowdiverterknownasFRED™(FlowRe-DirectionEndoluminalDevice),theCerebrovascularCenterisworkingtowardsaparadigmshiftinaneurysmtreatment.
“Ithinkwe’redefinitelydoingthemostmodern,sophisticatedsurgeryforscoliosis,andwearepushingtheboundariesofminimallyinvasivetechniquestoapplytothispatientpopulation.”
PAUL HOLMAN, MD
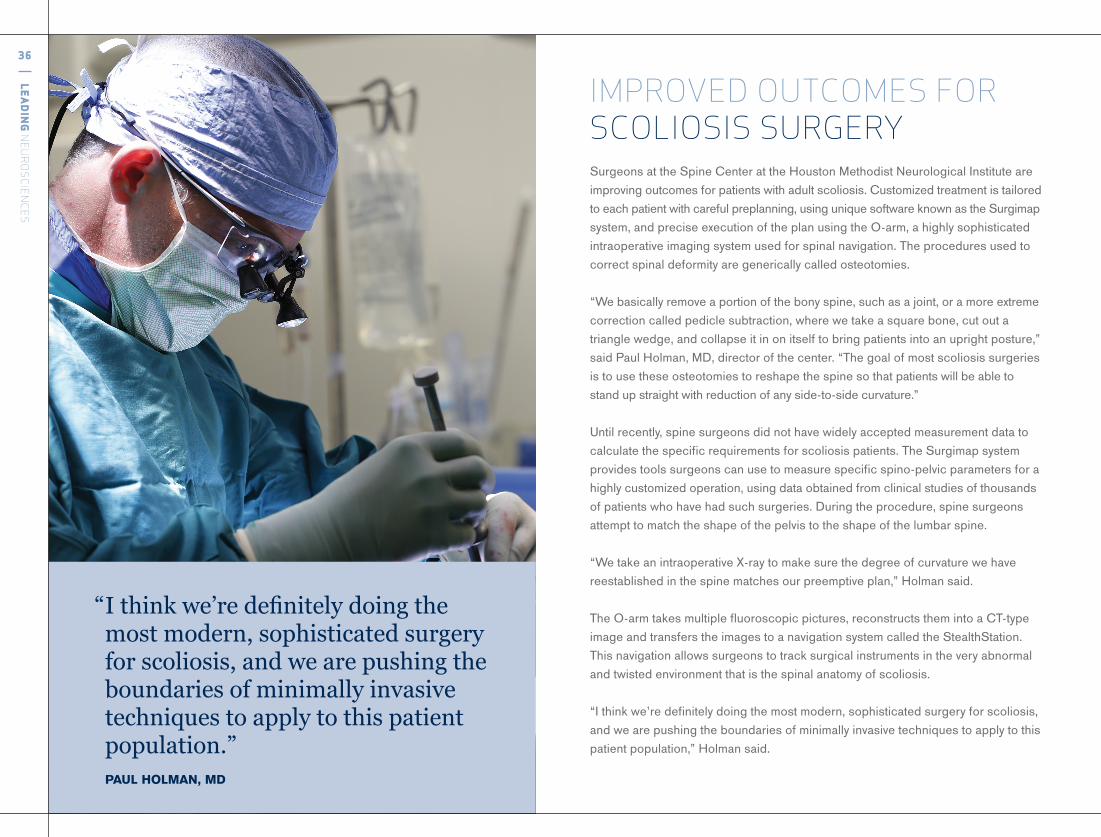
Surgeons at the Spine Center at the Houston Methodist Neurological Institute are improving outcomes for patients with adult scoliosis. Customized treatment is tailored to each patient with careful preplanning, using unique software known as the Surgimap system, and precise execution of the plan using the O-arm, a highly sophisticated intraoperative imaging system used for spinal navigation. The procedures used to correct spinal deformity are generically called osteotomies.
“We basically remove a portion of the bony spine, such as a joint, or a more extreme correction called pedicle subtraction, where we take a square bone, cut out a triangle wedge, and collapse it in on itself to bring patients into an upright posture,” said Paul Holman, MD, director of the center. “The goal of most scoliosis surgeries is to use these osteotomies to reshape the spine so that patients will be able to stand up straight with reduction of any side-to-side curvature.”
Until recently, spine surgeons did not have widely accepted measurement data to calculate the specific requirements for scoliosis patients. The Surgimap system provides tools surgeons can use to measure specific spino-pelvic parameters for a highly customized operation, using data obtained from clinical studies of thousands of patients who have had such surgeries. During the procedure, spine surgeons attempt to match the shape of the pelvis to the shape of the lumbar spine.
“We take an intraoperative X-ray to make sure the degree of curvature we have reestablished in the spine matches our preemptive plan,” Holman said.
The O-arm takes multiple fluoroscopic pictures, reconstructs them into a CT-type image and transfers the images to a navigation system called the StealthStation®. This navigation allows surgeons to track surgical instruments in the very abnormal and twisted environment that is the spinal anatomy of scoliosis.
“I think we’re definitely doing the most modern, sophisticated surgery for scoliosis, and we are pushing the boundaries of minimally invasive techniques to apply to this patient population,” Holman said.
IMPROVED OUTCOMES FOR SCOLIOSIS SURGERY
36
LEA
DIN
G N
EUR
OS
CIEN
CES

Compared to traditional open surgery for spinal abnormalities, patients who undergo minimally invasive spine surgery will have a shorter recovery time, a less extensive hospital stay, and less blood loss. Surgeons navigate along the spine using an endoscope, fluoroscopic visualization or computer navigation system, like a GPS.
Spinal stenosis is common in aging patients. The lumbar spine narrows and compresses nerves, and mobility is eventually lost. According to G. Alexander West, MD, chief of neurosurgery and director of spine services for Houston Methodist West Hospital, spine surgery is the definitive treatment for this debilitating condition. With age, however, comes the increased risk associated with surgery.
“Sometimes the risks of open surgery are too great, which is tragic because if you lose your mobility, you lose your independence,” West said. “With minimally invasive surgery, we accomplish the same goals with much lower risk. My oldest patient was 97, and she left the next morning. She was up and around and basically gained her independence, where before she couldn’t even walk to the mailbox without symptoms.”
A minimally invasive approach is also now possible for other spinal abnormalities that were traditionally considered major operative procedures. “We create a port for access, where we are able to maneuver instruments in and out,” West said. “The smallest channel I use is 7 mm. From that port I can access the spinal canal and the disk space.
“When we can do these types of traditional surgeries through a percutaneous system, the difference is dramatic. How well those patients recover, how long they stayed in the hospital, and how rapid their recovery is affects their overall quality of life.”
Many spine surgery patients are able to return home the same or next day and resume their general activities soon thereafter, rather than undergo an extensive period of rehabilitation and recovery.
DECREASED DISABILITY WITH MINIMALLY INVASIVE SPINE SURGERY
houstonmethodist.org/ni

38
LEA
DIN
G N
EUR
OS
CIEN
CES
The Houston Methodist Neurological Institute is one of the few facilities that offers asleep deep brain stimulation (DBS) for patients with movement disorders such as Parkinson’s disease and dystonia. With the use of a real-time magnetic resonance imaging (MRI) scanner, neurosurgeons are able to locate the target area within the brain, see the electrodes as they enter the brain, and guide the electrodes to the exact target area while the patient is asleep.
Once the patient is asleep, surgeons drill burr holes for placement of the electrodes and mount small towers that will display markers on the MRI scanner. “Towers indicate how to create a safe trajectory to our target. Once the scans indicate we’re on target, we make the final placement with the electrode and scan to see if the electrode is properly set,” said Richard Simpson, MD, neurosurgeon at the neurological institute and renowned DBS expert.
DBS is achieved via an implanted pacemaker that sends electrical impulses to targeted areas in the brain via the implanted electrodes. Although the mechanism of action is not fully understood with DBS, it is hypothesized that in Parkinson’s disease, for example, the stimulation may induce chemical changes in the brain. Long-term stimulation may actually induce DNA changes in cellular activity.
DBS has been shown to reduce stiffness, tremors and dyskinesia in Parkinson’s disease and other forms of dystonia. Parkinson’s disease and dystonia are the only two movement disorders that have received FDA approval for DBS treatment. “The potential for asleep DBS, especially deep-seated brain procedures, is substantial,” said Simpson. “This would include tumor biopsies, epilepsy surgery, lesions and the removal of deep hematomas.”
FORGING THE WAY IN DEEP BRAIN STIMULATION
With the use of a real-time MRI scanner, neurosurgeons are able to locate the target area within the brain, see the electrodes as they enter the brain, and guide the electrodes to the exact target area while the patient is asleep.

HOUSTON METHODIST: GLOBAL EDUCATIONAL REACH2015 HOUSTON METHODIST STATISTICS
GLOBAL HEALTH CARE SERVICESLEARNERS: 1,207
29 countries697 CME credit hours awarded
8 International partnerships58 Institutions16 Lectures
RESEARCH EDUCATION LEARNERS: 363128 Postdoctoral trainees112 Graduate students63 Summer students
6 Undergraduate students7 High school students
CONTINUING MEDICAL EDUCATION
PHYSICIAN LEARNERS: 10,141
103 Courses
OTHER LEARNERS
Rotating residents: 430Nursing students: 1,191Pharmacy students: 315
Allied health students: 141
GRADUATE MEDICAL EDUCATION
2015 residents: 2622018 fellows: 303
HOUSTON METHODISTINSTITUTE FOR TECHNOLOGY,INNOVATION & EDUCATION℠
2006-2014 learners: 35,0002015 learners: 6,697
554 Courses
40
LEA
DIN
G N
EUR
OS
CIEN
CES
The Houston Methodist Institute for Technology, Innovation & Education®SM, known as MITIE — one of the largest and most comprehensive education facilities in the world — is a place where surgeons and other health care providers continually refine their skills and acquire new expertise to perform at optimal levels throughout their careers.
To address the challenges of the modern operating room (OR), physicians and researchers at MITIE are designing a virtual intelligence system. The complexity of larger medical teams and overlapping technologies in the OR requires surgeons to interpret and evaluate an abundance of data while performing surgical procedures. To improve performance and decrease variability, the Intelligent OR brings surgeons and computational scientists together to develop safer, more accurate methods of managing patient care in real time.
“In today’s operating room, we are overwhelming surgeons with information from multiple technology platforms and staff who can distract them from the procedure at hand,” said Brian Dunkin, MD, a Houston Methodist endoscopic surgeon and medical director of MITIE. “The Intelligent OR is designed to provide surgeons and staff with necessary information at the point of care without unneeded distractions.”
Inside the Intelligent OR is the Smart Trocar, a device with a small camera that can attach to a traditional laparoscopic trocar and connect to a Real-time Interactive Navigation Assistance (RETINA) system. RETINA uses multiple technologies to track changes in the body during surgery. In most cases, each step of an operation requires a different surgical tool. The Smart Trocar and RETINA work in concert to track tools identified by a unique color. With this, the RETINA system can track the progress of a surgery.
THE WORLD’S FIRST VIRTUAL INTELLIGENCE FOR THE OPERATING ROOM
“Currently, surgeons cannot track multiple technologies or see what is happening in the body during surgery in a satisfactory way because a system that can analyze overlapping technologies has not been developed yet,” Dunkin said. “RETINA brings the information together, analyzes it, and provides the surgeon with the necessary, real-time information.”
The Intelligent OR also houses the Smart OR, a group of sensors placed at specific locations of the OR that detect automatically key steps of the surgery, such as when a patient is brought in and moved out of the room.
“By adding sensors to the operating room, we are able to track a variety of data points,” said Marc Garbey, PhD, research director of MITIE and professor of computational science at the University of Houston. “We believe the ability to track instrumentation and movement in the operating room will increase efficiency and reduce costs.”
Intelligent OR technology will help surgeons perform operations and image-guided procedures more efficiently and accurately. Incorporation of an intelligence system that combines and computes essential OR data will allow surgeons to focus on the patient and the operation in the provision of an unparalleled level of care.
houstonmethodist.org/ni
42
LEA
DIN
G N
EUR
OS
CIEN
CES
A seven-year residency program in neurosurgery provides extensive exposure to advanced operative techniques, neurophysiology, neuropathology and neuroradiology. The program includes a full year of protected research time and eight months of focused subspecialty exposure in preparation for careers in research or clinical practice.
A four-year accredited adult neurology residence program offers comprehensive training in clinical neurology and mentorship in the clinical and basic sciences that provides a strong foundation for the practicing neurologist and physician-scientist. The program has a high faculty-to-resident ratio, which allows residents access to training, yet also challenges them to be autonomous.
A one-year accredited postgraduate clinical neurophysiology fellowship program is comprised of all aspects of clinical neurophysiology and encompasses electromyography (EMG), electroencephalography (EEG), nerve conduction, sleep, evoked potentials, intraoperative monitoring and additional clinical testing modalities.
A one-year accredited neuromuscular medicine fellowship focuses on clinical neuromuscular medicine and includes electro-diagnostic medicine, neuropathology, clinical/translational experience and rehabilitation. The neuromuscular fellowship provides a large and varied clinical experience with more than 75 neuromuscular patients evaluated each week, from both inpatient and outpatient services.
ACADEMIC PROGRAMS & COURSESNeurology and neurosurgery grand rounds present the latest information about the nervous system and neurological disorders. Grand rounds provide an excellent venue for presentations by visiting professors. World-class scientists, researchers, neurologists and neurosurgeons present their work to the group in an environment of collaboration and scientific inquiry.
Annual skull base, cerebrovascular and spine courses for residents and fellows provide a hands-on cadaveric sequence designed to educate senior neurosurgery residents and fellows in the latest techniques in neurosurgery. In addition to anatomy, the course presents common microsurgical, endoscopic and endovascular approaches to the brain and spine, indications for use and complication avoidance.
The subcortical surgery group holds annual meetings to discuss subcortical procedures and lessons learned from the Six Pillar Approach to deep brain surgery. Numerous topics are discussed, such as the principles of white matter image interpretation and trajectory planning, principles and pitfalls of cannulations, and optimizing efficiency and precision during all phases of resection. Labs provide demonstrations of procedural techniques.
Last September, the Houston Methodist Neurological Institute held the eighth annual Advances in Neurology Symposium. The program emphasizes Houston Methodist’s evidence-based strategies for the current treatment of neurological disorders and cutting-edge research in novel therapeutics.

Department of Neurosurgery
Stanley H. Appel Department of Neurology
44
LEA
DIN
G N
EUR
OS
CIEN
CES
GLENN ANDERSON, MD, joined Houston Methodist Willowbrook Hospital as medical director of neurosurgery. Anderson has practiced neurosurgery for more than 13 years and has extensive experience in the fields of brain tumors, cerebral aneurysms and arteriovenous malformations.
TETSUO ASHIZAWA, MD, joined the Houston Methodist Neurological Institute as director of neuroscience research. Ashizawa, formerly executive director of the McKnight Brain Institute at the University of Florida, organized and developed interdisciplinary neuroscience research programs involving multiple colleges and departments. As a physician-scientist, he is studying neurogenetic disorders caused by expansions of DNA sequences that are connected end-to-end and abnormally repeated.
VERONICA J. BURTON, PhD, joined Houston Methodist as a board-certified neuropsychologist with extensive experience in the assessment and treatment of neurological and psychological disorders.
MICHELLE DANG, MD, an anesthesiologist with a special interest in interventional pain management, joined the Pain Management Center in the Houston Methodist Neurological Institute. Dang is board certified in anesthesiology.
TOP QUALITY UHC AWARDHouston Methodist is the recipient of a top quality award from UHC, an alliance of the nation’s leading academic medical centers. This year, UHC ranked Houston Methodist No. 8 among 102 peer hospitals — our highest ranking since the award was established in 2005.
AANS TOP HONORS FOR RESIDENTS IN TOP GUN COMPETITION Two neurosurgical residents, Brandon Liebelt, MD, and Sean Barber, MD, have thoroughly surpassed their competition to win best overall team in this year’s Tenth Annual Neurosurgical Top Gun Competition at the American Association of Neurological Surgeons (AANS) meeting.
ACCOLADES NEW HIRES
In 2015, Houston Methodist Hospital’s Rehabilitation Services’ facility was awarded full accreditation in the areas of Adult Inpatient Rehabilitation Program as well as the Stroke Specialty Program.
The American Heart Association and American Stroke Association recognize Houston Methodist Hospital for achieving 85 percent or higher compliance with all Get With The Guidelines®- Stroke Achievement Measures and 75 percent or higher compliance with five or more Get With The Guidelines®-Stroke Quality Measures.
PHILIP J. HORNER, PhD, joined the Houston Methodist Neurological Institute’s new Center for Neuroregenerative Medicine as scientific director. Horner is an expert on the use of stem cells to replace damaged brain and spinal cord tissue, as well as adult central nervous system regeneration, stem cells and gene therapy. Horner comes from the University of Washington School of Medicine, where he was a professor of stem cell biology and neural repair in the Department of Neurological Surgery.
WILLIAM G. ONDO, MD, joined the Houston Methodist Neurological Institute as director of the Movement Disorders Clinic. Ondo has more than 20 years of experience treating Parkinson’s disease, dystonia, tremor, restless legs syndrome and other movement disorders. Ondo has published 250 original articles and book chapters, edited two text books, and gives lectures across the country.
SHEETAL SHROFF, MD, joined the Houston Methodist Neurological Institute as a board-certified neurologist. Shroff’s research focuses on clinical trials of investigational new drugs for the treatment of myasthenia gravis, muscular dystrophy and chronic inflammatory demyelinating polyneuropathy.
ROBERT GLEN SMITH, MD, joined Houston Methodist Neurological Institute as a board-certified neurologist. Prior to his appointment, Smith completed clinical and research training at Baylor College of Medicine where he served as a faculty member for more than a decade. In 2004, Smith became vice chair of the department of neurology at The University of Texas Medical Branch at Galveston, where he oversaw the creation of the UTMB Stroke Center and Epilepsy Monitoring Unit.
IVO W. TREMONT, MD, joined Houston Methodist Neurological Institute as a board-certified neuro-oncologist. Tremont initially trained in internal medicine and medical oncology. After completion of a research fellowship sponsored by the American Cancer Society, he achieved board certification in neurology, neuro-oncology, and hospice medicine and palliative care. Tremont’s current, active field of study is neuro-oncology, with emphasis in gliomas and in leptomeningeal metastases from breast cancer.
G. ALEXANDER WEST, MD, PhD, joined Houston Methodist West Hospital as chief of neurosurgery and director of spine services. West brings with him significant experience in minimally invasive spine surgeries and general neurological operations using the least invasive, state-of-the-art procedures. West is certified by the American Board of Neurological Surgery and is the author of numerous peer-reviewed articles.
THE SYNAPSE, THE HOUSTON METHODIST NEUROLOGICAL INSTITUTE’S PHYSICIAN ENEWSLETTER
More than 7,000 neurologists and neurosurgeons in the United States read The Synapse. Earn CME credit while accessing the work of leading clinicians and researchers and learn about leading-edge discoveries, innovations, procedures and treatments for neurological disorders.
VISIT houstonmethodist.org/physician-subscribe to subscribe.
46
LEA
DIN
G N
EUR
OS
CIEN
CES
houstonmethodist.org/ni
In 1951, Houston Methodist relocated to the Texas Medical Center from downtown Houston. Since that time, the hospital’s footprint has expanded exponentially. New construction has begun on the Houston Methodist campus that will enable us to continue to grow and meet our mission of providing comprehensive, integrated and multidisciplinary care to the people we serve.
This new facility will function as an epicenter of care and will house all services for diagnosis, treatment and rehabilitation of neurological conditions. The health professionals housed within this new structure will collaborate across the Houston Methodist system and complement the Houston Methodist Research Institute and Houston Methodist Institute for Technology, Innovation & Education (MITIE®), one of the largest and most comprehensive education and research facilities in the world.
Phase I of new construction will be located on our north campus and is slated for completion in 2017. The new North Tower will account for 745,000 to 923,000 square feet and will include:
· EXPANDED OR SUITE WITH FOUR HYBRIDS AND I-MRI
· ICU/UNIVERSAL BED FLOORS (102 BEDS)
· SIX ACUTE BED FLOORS (216 BEDS)
· TWO SHELLED BED FLOORS (72 BEDS)
· 24 BED VIP UNIT
· HELIPAD
· CONFERENCE FACILITIES
Specific to neurology and neurosurgery care, our new building will offer:
· 36 ICU BEDS
· 72 ACUTE CARE BEDS
· 2 OPERATING ROOMS WITH I-MRI
At Houston Methodist, we have the flexibility, skill, technology and vision to provide exemplary neurological care to meet the needs of our community while we continue to lead medicine.
EXPANDING DELIVERY OF COMPREHENSIVE, INTEGRATED CARE
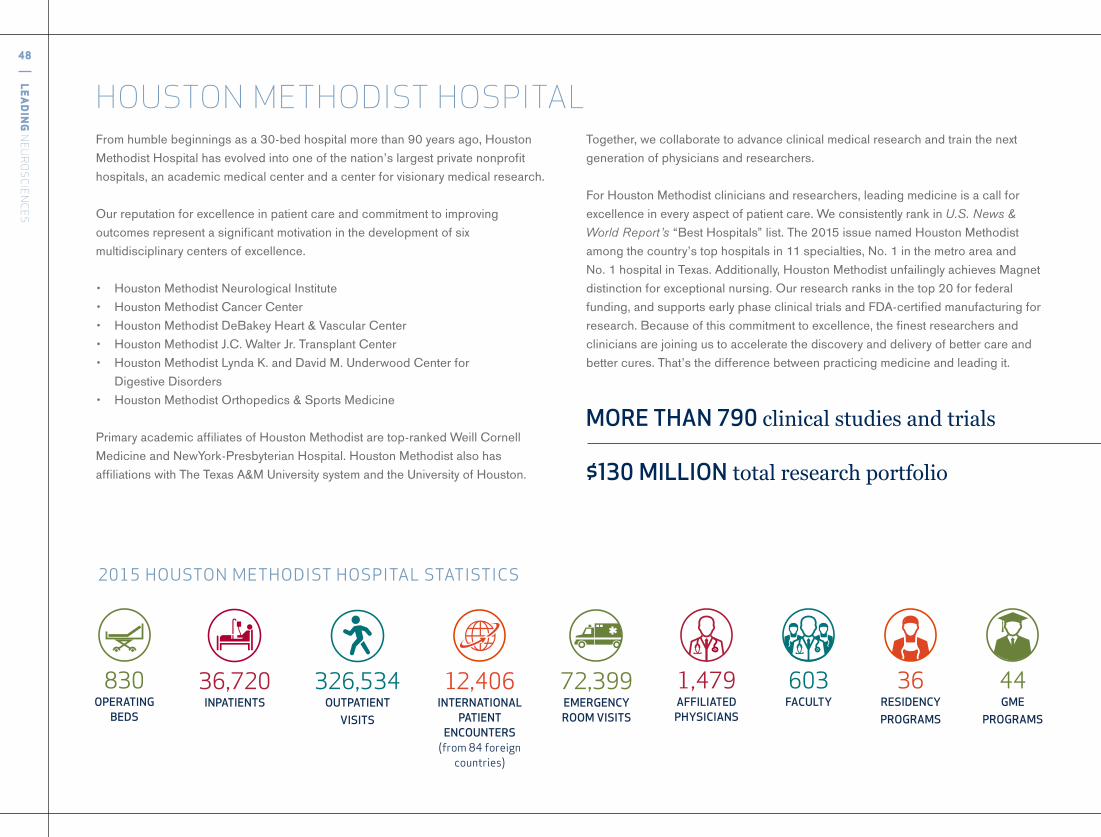
48
LEA
DIN
G N
EUR
OS
CIEN
CES
From humble beginnings as a 30-bed hospital more than 90 years ago, Houston Methodist Hospital has evolved into one of the nation’s largest private nonprofit hospitals, an academic medical center and a center for visionary medical research.
Our reputation for excellence in patient care and commitment to improving outcomes represent a significant motivation in the development of six multidisciplinary centers of excellence.
• Houston Methodist Neurological Institute• Houston Methodist Cancer Center• Houston Methodist DeBakey Heart & Vascular Center• Houston Methodist J.C. Walter Jr. Transplant Center• Houston Methodist Lynda K. and David M. Underwood Center for
Digestive Disorders• Houston Methodist Orthopedics & Sports Medicine
Primary academic affiliates of Houston Methodist are top-ranked Weill Cornell Medicine and NewYork-Presbyterian Hospital. Houston Methodist also has affiliations with The Texas A&M University system and the University of Houston.
HOUSTON METHODIST HOSPITALTogether, we collaborate to advance clinical medical research and train the next generation of physicians and researchers.
For Houston Methodist clinicians and researchers, leading medicine is a call for excellence in every aspect of patient care. We consistently rank in U.S. News & World Report’s “Best Hospitals” list. The 2015 issue named Houston Methodist among the country’s top hospitals in 11 specialties, No. 1 in the metro area and No. 1 hospital in Texas. Additionally, Houston Methodist unfailingly achieves Magnet distinction for exceptional nursing. Our research ranks in the top 20 for federal funding, and supports early phase clinical trials and FDA-certified manufacturing for research. Because of this commitment to excellence, the finest researchers and clinicians are joining us to accelerate the discovery and delivery of better care and better cures. That’s the difference between practicing medicine and leading it.
MORE THAN 790 clinicalstudiesandtrials
$130 MILLION totalresearchportfolio
2015HOUSTONMETHODISTHOSPITALSTATISTICS
12,406INTERNATIONAL
PATIENT ENCOUNTERS
(from84foreigncountries)
36,720INPATIENTS
72,399EMERGENCY ROOM VISITS
1,479AFFILIATED PHYSICIANS
603FACULTY
44GME
PROGRAMS
36RESIDENCY PROGRAMS
326,534OUTPATIENT
VISITS
830OPERATING
BEDS
Visit houstonmethodist.org/research to see all the ways we’re leading research.
©2015 Time Inc. FORTUNE and 100 Best Companies to Work For are registered trademarks of Time Inc. and are used under license. FORTUNE and Time Inc. are not affiliated with, and do not endorse products or services of Houston Methodist.
LEADERS IN RESEARCH At Houston Methodist, we are dedicated to defining the future of
medicine. We engineer discoveries in the lab to become clinically
useful products, channel the best innovations through early-stage
clinical trials, and actively transition those innovations to our
industry partners. Our commitment to the full cycle of discovery
and delivery sets us apart as leaders who provide patients from
around the world access to the latest health care advances.

Houston Methodist Hospital
6565 Fannin St., Houston, TX 77030
877.790.DOCS
houstonmethodist.org/ni
LEADING MEDICINE YESTERDAY, TODAY AND TOMORROWAt Houston Methodist, we have a proud tradition of
revolutionizing medicine. Our past achievements
have built a legacy that spans multiple decades and
disciplines, and that same culture of excellence
inspires us to be the pioneers of tomorrow.
THAT’S THE DIFFERENCE BETWEEN PRACTICING MEDICINE AND LEADING IT.
Our commitment to advancing medicine with global impact
begins in Houston, Texas, where we pioneer a better tomorrow
through research, innovation and breakthroughs to rewrite the
future of health.
LEADINGNEUROSCIENCES
2 0 1 4 - 2 0 1 5 Y E A R I N R E V I E W











![ECMO Admission [1220] General - Houston Methodist](https://img.pdfslide.us/doc/110x75/616a274c11a7b741a34f61e2/ecmo-admission-1220-general-houston-methodist.jpg)




![Acute Renal Failure Admission [598] - Houston Methodist](https://img.pdfslide.us/doc/110x75/6286e32aaf282029e7716915/acute-renal-failure-admission-598-houston-methodist.jpg)












