Embed Size (px)
Citation preview

Hospital Hospital Emergency Emergency
ManagementManagementThe safety officer wrote
the disaster plan!
What am I supposed to do?

Hospital emergency management has changed over the past few years...
Until recently, hospitals planned response to mass
casualty disasters (Alert 1), fire, and a few natural
disasters (tornado, earthquake) that could
impact the facility.

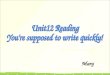
UK Hospital Hazard Vulnerability Analysis
Event 2002 RatingMass Casualty Incident (Hazmat) 30
Hostage Situation 30Civil Disturbance 30
Bomb Threat 30Earthquake 30
Hazmat Exposure, Internal 30Mass Casualty Incident (Trauma) 30
Terrorism, Biological 30Terrorism, Chemical 30
HVAC Failure 30Information Systems Failure 28
Communications Failure 20Tornado 20
Unavailability of Supplies 20Mass Casualty Incident (Medical) 20
Infant Abduction 20Fire, Internal 20
Ice Storm 18Temperature Extremes 16
Epidemic 15Hazmat Exposure, External 15
Generator Failure 10Electrical Failure 10
Medical Gas Failure 10Labor Action 9
Severe Thunderstorm 9Drought 8
Medical Vacuum Failure 8Flood, Internal 8
Blizzard 6Sewer Failure 4Fuel Shortage 4Steam Failure 4VIP Situation 4
Structural Damage 4Water Failure 4
Snow Fall 3Forensic Admission 3Fire Alarm Failure 2
Wild Fire 1Flood, External 1
Transportation Failure 1
Now hospitals conductan annual hazard vulnerability analysis and come upwith a list ofemergencies that looks like this…
This list takes into account•probability•impact on institution•institutional preparedness

Emergency Management has evolved beyond response planning. It includes:
• Mitigation• Preparedness• Response and• Recovery

Because of the numbers and kinds of emergencies that can impact a hospital, most begin planning with a basic infrastructure...
Safety Officer Security Officer
Public Inform ationOfficer
Liaison Officer
Logistics Chief Planning Chief Finance Chief Operations Chief
Incident Com m ander

JCAHO and NFPA 99 require an “all-hazards” incident command structure that... • Can be coordinated with the
command system in the community• Uses the same terminology as the
community ICS• Is flexible enough to allow activation
and deactivation of components, based on the specific event

Both JCAHO and NFPA also require a structure that explicitly allows for the management of...
• Patient care• Staff/family support• Logistics of critical supplies• Media• Security

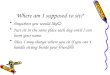
Hospital Em ergency Incident Com m and SystemHEICS
P u b lic In fo rm ation O ffice r L ia ison O ffic e r
S a fe ty an d S ec u rity O ffice r
D am ag e A ssess m en t an dC on tro l O ffice r
S an ita tion S ys tem sO ffice r
F ac ilit iesU n it L ead er
C om m u n ica tion s U n itL ead er
Tran sp orta tion U n itL ead er
M ateria ls S u p p ly U n itL ead er
N u trit ion a l S u p p lyU n it L ead er
L og is t ic s C h ie f
S itu a tion -S ta tu sU n it L ead er
L ab or P oo lU n it L ead er
M ed ic a l S ta ffU n it L ead er
P atien t Track in gO ffice r
P a tien t In fo rm ationO ffice r
N u rs in gU n it L ead er
P lan n in g C h ie f
T im eU n it L ead er
P rocu rem en tU n it L ead er
C la im sU n it L ead er
C os tU n it L ead er
F in an c e C h ie f
M ed ic a l S ta ffD irec to r
S u rg ic a l S ervicesU n it L ead er
M atern a l C h ildU n it L ead er
C rit ica l C areU n it L ead er
G en era l N u rs in gC are U n it L ead er
O u t P a tien t S ervic esU n it L ead er
In -P a tien t A reasS u p erviso r
Triag eU n it L ead er
Im m ed ia te Trea tm en tU n it L ead er
D e layed Trea tm en tU n it L ead er
M in or Trea tm en tU n it L ead er
D isc h arg eU n it L ead er
M org u eU n it L ead er
Trea tm en t A reasS u p erviso r
M ed ic a l C areD irec to r
L ab ora to ryU n it L ead er
R ad io log yU n it L ead er
P h arm acyU n it L ead er
C ard iop u lom on aryU n it L ead er
A n c illa ry S ervic esD irec to r
S ta ff S u p p ortU n it L ead er
P s ych o log ica l S u p p ortU n it L ead er
D ep en d en t C areU n it L ead er
H u m an S ervicesD irec to r
O p era tion s C h ie f
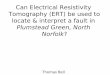
In c id en t C om m an d er

What is HEICS?
• An “all-hazards” command structure
• A universal link with outside resources

HEICS provides...
• A dependable chain of command• Improved communication through common
language• Flexibility• Prioritization of tasks• Organized documentation system• Effective mutual aid planning
The Fayette County Healthcare Emergency Planning Committee has adopted HEICS.As a result, all acute care hospitals will begin using the HEICS structure.

HEICS Tools
• Organization chart• Job Action Sheets • Forms

Basic Units of HEICS Organization • Incident Commander• Section Chiefs• Directors• Unit Leaders• Officers
+
Each situation is unique and requires a different implementation
strategy.
Some positions will need to be filled immediately. Others may not be needed for hours or days.
Some may not be needed at all.
= Command Center
PI OfficerSafety OfficerSecurity OfficerLiaison

Five sections…one mission...
To respond to the emergency at hand.• Command Center • Logistics• Planning• Finance• Operations

Command CenterDefines the mission and ensures its
completion.

LogisticsProvides for a working environment and adequate materials to meet the
overall medical objective.

PlanningDetermines and provides for the
continuance of each medical objective. Prompts and drives all HEICS officers
to develop short- and long-range action plans.

FinanceProvides funding for present medical objective and stresses facility-wide
documentation to maximize financial recovery and reduction of liability.

OperationsCarries out the medical objective to
the best of the hospital’s ability.

University of Kentucky HospitalEm ergency Incident Com m and System
HEICS
P u b lic In fo rm a tio n O ff ice rP R -o n -ca ll
L ia iso n O ff ice rT o m i R o ss
S a fe ty O ff ice rT o m i R o ss
S h a ro n B e rry
S e c u rity O ff ice rJo s e ph F rye
Je ff S hu tt
D a m a g e A s se ss m e nt a ndC o n tro l O ff ice r
L e o F os te r
S a n ita tio n S yste m sO ff ice r
M a tt M u e lle r
F a c ilit ie sU n it L e ad erE d M c C lu re
C o m m un ica tion s U n itL e ad er
Ja n B a tesJa m es W e llm an
T ra n spo rta tion U n itL e ad er
Jo e M a llek
M a te ria ls S u pp ly U n itL e ad er
M a ry S k e en
N u trit io n a l S u p p lyU n it L e ad er
F lo yd D re x le r
L o g is tics C h ie fD a v id A llen
S a n dra C h a m b e rs
S itua tion -S ta tusU n it L e ad er
V ick y B ra d ley
L a bo r P o o lU n it L e ad er
Ja m e s P a tte rsonM a rg a re t L on g hu rst
M e d ic a l S ta ffU n it L e ad er
Ja n W illia m s
P a tien t T rack ingO ff ice r
Jo d ie M a rt inH a ro ld M iles
P a tie n t In fo rm ationO ff ice r
C a ro l D icke yL in D u d ik
N u rs ingU n it L e ad erP a t P o w e rs
S ha n e S tra tton
P la n n in g C h ie fS a n dra C h a m b e rs
J im Z em b ro d t
T im eU n it L e ad er
P ro cu re m e ntU n it L e ad er
C la im sU n it L e ad er
C o s tU n it L e ad er
F in a nc e C h ie fM u rra y C la rkL a rry M o o re
M e d ic a l S ta ffD ire c to r
K e v in N e lson
S u rg ic a l S e rv icesU n it L e ad er
T rish S e a b o lt
M a te rna l C h ildU n it L e ad er
G w e n M o re la nd
C rit ica l C a reU n it L e ad er
D ennis S z cz ygie ls k i
Jo hn B urton
G e n era l N u rs ingC a re U n it Le a d er
G a yle P la nk
O u t P a tie n t S erv icesU n it L e ad er
T rin a V a n G u ild e r
In -P a tien t A re asS u p erv iso r
K a th le e n K op s er
T ria geU n it L e ad erP a tty S tu rt
Im m e d ia te Tre a tm e ntU n it L e ad er
L in d a H o ltz c law
D e la ye d Tre a tm e ntU n it L e ad er
M in o r T re a tm e ntU n it L e ad er
D isc h a rgeU n it L e ad er
B e v H an so n -T u c ker
M o rg ueU n it L e ad erB a rb B u sh
T re a tm e n t A re asS u p erv iso r
C o lle e n S w a rtzP a u l F e rre ll
M e d ic a l C a reD ire c to r
H O A
L a b ora to ryU n it L e ad erB a rb B u sh
T e re sa E ickh o rn
R a d io lo gyU n it L e ad er
S h e ryl A b e rcro m b ieK e v in C o n n e lly
P h a rm a cyU n it L e ad er
Jo h n A rm itste ad
C a rd iop u lo m o n a ryU n it L e ad erB a rb A tk ins
B rya n C o llins
A n c illa ry S e rv icesD ire c to r
A n n S m ithB a rb A tk ins
S ta ff S u p po rtU n it L e ad er
K a ren G ra h am
P s ycho lo g ica l S up p o rtU n it L e ad er
D o n n a F a rra r
D e pe n de n t C a reU n it L e ad er
B o nn ie Th o rn ton
H u m an S erv icesD ire c to r
C a ro l B a rn e tt
O p e ra tio n s C h ie fA n n S m ith
K a ren S te fan iak
In c ide n t C o m m an d erJo s e ph C layp o o l
A d m in is tra to r-o n -c a ll

Job Action Sheets• Your disaster response job descriptions• Tell you
– What you are going to do– When you are going to do it– To whom you are going to report it after
you have done it.
Universal titles and missions allow emergency responders from a variety of agencies to
communicate.

HEICS Forms
• Used with job assignments• Can be altered in any way
necessary
Documentation = $$$Documentation = $$$

The Language of The Language of Emergency Emergency
ManagementManagement

• To specific disaster plans (to reflect HEICS structure)
• Emergency code names (to make consistent with other hospitals and emergency responders)
• JCAHO Emergency Management standards

Advance planning forAdvance planning for
Medical Care DirectorMedical Care Director• Establishing an Operations
Section Center, including locations and staffing
• Assessing staffing, supply, equipment needs in patient care settings.
• Emergency inpatient discharge. (See Nursing Unit Leader.)
• Communicating with patient care areas. (See Communications Unit Leader.)
The Operations Chief will require written plans for:

Advance planning forAdvance planning for
Medical Staff DirectorMedical Staff Director
• Establishing a physician labor pool. (See Medical Staff Unit Leader.)
• Credentialing volunteer medical staff. (See Medical Staff Unit Leader.)
• Assessing physician staffing needs and assigning physicians.
The Operations Chief will require written plans for:

• Assessing inpatients for early discharge. (See Nursing Staff Unit Leader.)
• Establishing alternate inpatient care sites within the facility.
• Assessing staffing, supply, equipment needs in patient care settings.
The Operations Chief will require written plans for:
Advance planning forAdvance planning for
In-Patient AreasIn-Patient Areas

• Establishing emergency treatment areas, including location and staffing.
• Assessing staffing, supply, and equipment needs in treatment areas. (See Medical Care Director.)
• Assessing security needs in treatment areas.
• Moving patients through treatment areas to discharge or admission.(See Transportation Leader.)
Advance planning forAdvance planning for
Treatment AreasTreatment Areas
The Operations Chief will require written plans for:

• Inventorying available blood supply.
• Evaluating ancillary services’ capacity to perform services required by emergency.
• Tracking patients to ensure results reporting. (See Patient Tracking Officer.)
• Assessing staffing, supply, and equipment needs.)
The Operations Chief will require written plans for:
Advance planning forAdvance planning for
Ancillary ServicesAncillary Services

• Establishing staff psychological support and debriefing areas, including location and staffing.
• Establishing a dependent care area, including location and staffing.
• Identifying dependents.• Assessing materials and
supply needs.
Advance planning forAdvance planning for
Human ServicesHuman Services The Operations Chief will require written plans for:
• Establishing Human Services Center, including location and staffing.
• Implementing emergency discharge procedures. (See Nursing Staff Unit Leader.)
• Establishing staff rest, nutrition, and sleeping areas, including location and staffing.
• Keeping staff updated regarding emergency status. (See Situation-Status Unit Leader.)

The Planning Chief will require written plans:
Advance planning forAdvance planning for
Situation-Status Unit Situation-Status Unit
Maintenance and recovery of computer
systems
Security of medical records

Advance planning forAdvance planning for
Labor Pool
• Establishing the labor pool, including location and staffing
• Registration and credentialing of volunteer staff
The Planning Chief will require written plans for:

Advance Planning forAdvance Planning forLogistics of
Critical SuppliesCritical Supplies
The logistics section chief will require a written plan and procedures for procuring, handling, and distributing...
� Pharmaceuticals� Medical supplies� Food supplies� Linen� Water� Critical Equipment

Advance planning forAdvance planning for
CommunicationsCommunicationsLogistics
The logistics section chief will require a written plan and procedures for communicating with…
In addition, the chief will require an...
� Other areas/departments within hospital
� Other facilities� External agencies
� Alternative communications plan for all major communication systems

Advance planning forAdvance planning for
Transportation Transportation Logistics
The logistics section chief will require a written plan and procedures for transportation of...
� Patients � Staff� Equipment
to or from other facilities � Staff to and from
hospital during bad weather
� Critical supplies

Advance planning forAdvance planning for
Medical Staff UnitMedical Staff Unit• Establishing a
physician labor pool, including location and staffing
• Registration and credentialing of volunteer medical staff
The Planning Chief willrequire written plans for:

Advance planning forAdvance planning for
Nursing UnitNursing Unit • Emergency
Inpatient discharge
• Patient Tracking • Release of
Patient Information
• Recalling Nursing Staff
The Planning Chief willrequire written plans for: