Embed Size (px)
DESCRIPTION
Hospital at Home Collaboration: Odense Municipality Department of Emergency Medicine Odense University Hospital Department of Health Science and Technology, Aalborg University Centre for Applied Health Services Research Systematic Anygroup Lindpro
Citation preview

HOSPITAL AT HOME ANETTE TANDERUP MD, PH.D.-STUDENT
Denmark, Odense University Hospital, Department of Geriatric medicine

Hospital at Home
Supervisors: Jesper Ryg, MD, Ph. D., Post doc. Annmarie Touborg Lassen, MD, Ph.D.,
Professor, Head of Research Unit of Emergency Medicine.
Anne Lee, Executive Officer, MSc (Health), RN
Jens-Ulrik Rosholm: MD, Ph.D. Clinical associate professor.

Hospital at Home
Collaboration: Odense Municipality Department of Emergency Medicine Odense
University Hospital Department of Health Science and Technology,
Aalborg University Centre for Applied Health Services Research Systematic Anygroup Lindpro

Hospital at Home
Funding: University of Southern Denmark Research Foundation of Odense
University Hospital Patient@home The Velux Foundation
No competing interests exist

Introduction: In the future there will be an increasing
number of acutely ill geriatric patients. There is some evidence that being treated in your own home instead of being admitted to the hospital is beneficial for some geriatric patients
Hospital at Home
Caplan Age and Ageing 2006Zisberg J Am Geriatr Soc 2011Leff Ann Intern Med 2005 Leff J Am Geriatr Soc 2009

Hospital at Home
Objectives: Feasibility of “Hospital at Home” (HH)
supported by telemedicine

Hospital at Home
Method: Within the first 24 hours after
admittance to the medical emergency department (MED) geriatric patients are assessed for their appropriateness and willingness to continue the admission in their own home

Hospital at Home
≥ 65 years Admitted to the
MED Not resident in the municipality of Odense
Living in nursing home
Not a geriatric patient
Not in need of at least 48 H additional admission
Terminal patientsIsolated patientsDifficulty speaking or understanding DanishParticipants in another research project In need of treatment or care
that is not possible in this HH set-up (see table)Patients with severe cognition
decline (acute or permanent) Patients not suitable for HH after assessment by doctor, nurse, and physiotherapist Patient or patients spouse do
not wish to participate
Patients suitable for HH

Hospital at Home
HH Set-up: Nurses from the municipality perform
daily care, security checks and triage Geriatric doctor and nurse do “ward
round” daily Physiotherapist will attend when needed The patients can be transferred back to
the hospital 24/7 in case of deterioration, technical breakdown etc.

Hospital at Home
Measurement Maximum frequency
Blood sample Once a day
ECG Once a day
Vital signs ( BP, RF, HR, Sat, Temp, GCS) Triage
Every 3th hour
Diuresis Every 3th hour
Treatment Restrictions
Oxygen Maximum 2LOnly via nasal cannula
Fluid therapy Subcutaneous fluidOnly isotonic Maximum 2L pr. day
Nutrition Meal schemeSupplemental nutrition drinks
Medicin Per oralSubcutaneous injections Intramuscular injectionsI v antibiotics
Blood transfusion Only erythrocytes

Hospital at Home
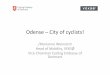
Technical set-up: Telemedicine is used for safety and
communication. An alarm is automatically generated by smoke/fire, falls, “leaving” the house, deterioration in vital signs, and unusual movement pattern at night. Patients, relatives, and personal can also activate the alarm.
Alarms go to a call-center nurse who can contact the patient by a call-system where communication and visual inspection is possible. The right help can thus be provided

Hospital at Home
Patient homeHospital Call center
Geriatric nurse
Geriatric doctor
Alarm Technology
?

Hospital at Home
Results: Inclusion is still running and the results
are not yet analyzed. The acceptability, practicality, implementation, and demand for HH will be addressed

Hospital at Home
Data: Data will be analyzed with the MAST-
model
K. K. The MAST manual 2010. Available from: http://www.mast-model.info/

Hospital at Home
Safety: Steering committee Safety committee Approval from ethical committee Approval from the Danish Data
Protection Agency

Hospital at Home
Ethic considerations Technology must not replace warm
hands! ”You do not se the elderly, when they are
”set free” by welfaretechnology that removes human contact”.
”Technology can survey, but only humans can watch”.
Birkler J, Politiken 090215