Embed Size (px)
DESCRIPTION
Citation preview

APUDomas AND CARCINOID SYNDROME
Dr. JIGYASA SHAHANIModerator: Dr. FAREED AHMED

-Term given to an embryologically related groupof tumours of endocrine organs. They are believed to arise from neuroendocrine cells,
which are derived from neural crest,and, whose normal function is to serve at neuroendocrine interface.
-APUD= amine precursor uptake and decarboxylation. -Tumours of this system = APUDomas; secretehormone of the tissue of origin -The term was coined in about 1974; has since been revised and called NEUROENDOCRINEGASTROENTEROPANCREATIC TUMOURS;
APUDomas

Cells with these properties have been grouped together as the APUD system.
They contain characteristic granules on electron microscopy
They secrete polypeptides or amines or both
APUD CELLS

The cells included here are:
The chromaffin cell system- These are found in the adrenal medulla and in association with the paravertebral plexuses.
The non-chromaffin cells of the paraganglia (Carotid body, glomus jugulare).
The argentaffin (Kultschitzky) cells.( found in the intestine). Similar cells occur in the salivary glands, pancreas, and bronchial mucosa. The argyrophil cells. These are widely distributed in the intestine.
Apud cells.....

Neural crest cells are a transient , multi- potent,migratory cell population unique to vertebrates that give rise to a diverse cell lineage including melanocytes,craniofacial cartilage and bones,smooth muscle , peripheral and enteric neurons and glia.
EMBRYOLOGY OF NEURAL CREST CELLS:-

After gastrulation,neural crest cells are specified at the border of the neural plate and the non neural ectoderm. During neurulation,the border of the neural plate,also known as the neural folds,converge at the dorsal midline to form the neural tube. Subsequently,neural crest cells from the roof plate of the neural tube undergo an epithelial to mesenchymal transition,delaminating from the neuroepithelium and migrating through the periphery where they differentiate into varied cell types.
EMBRYOLOGY OF NEURAL CREST CELLS:-

Neuroendocrine tumors are:
CHARACTERISTICS OF NET’s
-Rare-Usually small, <1cm-Slow growing over months to years-Usually metastasize before becomingsymptomatic, often when tumour > 2cm-Expression is episodic, may be silent for years- often misdiagnosed-Complex diagnosis requiring advanced radiographic studies.

-In the past all NET’s were termed carcinoid; -Has since been classified into: 1. CARCINOID 2. NON-CARCINOID -According to WHO 5 major categories: i. well differentiated endocrine tu’s ii. Well differentiated endocrine ca’s iii. Poorly differentiated endocrine ca’s iv. Mixed endocrine and exocrine ca’s v. Neuro-endocrine – like lesions
CLASSIFICATION:

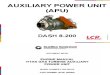
Carcinoid 56%Insulinomas 17%Unknown 15%Gastrinomas 9%VIPomas 2%Glucagonomas 1%Somatostatinomas 1%Annual
Incidence of GEP-NETs

Other neuroendocrinal cells are present in the stomach and small intestine
These are responsible for secretion of VIP,cholecystokinin, gastrin,5HT, etc
They includePancreatic islet cells, Thyroid C cells,Parathyroid cells,Melanocytes,Hypothalamic neuroendocrine cells,Some cells of the anterior pituitary, and The autonomic neurons
GEP-NETs

NON CARCINOID TUMORS

Usually present with symptoms or manifestations caused by mechanical effects of their presence, growth, and metastasis; or caused by the effect of their particular endocrine product.
- Slow growing; delay diagnosis – 4-6years - Pattern of growth varies; with the
exception of 90% of insulinomas, almost all have long term malignant potential.
PRESENTATION

-hormone: insulin, proinsulin -Clinical features: hypoglycaemia, wt gain, CVS Symptoms (17%), neuroglycopaenic symptoms -site: >95% pancreas; mostly small - >10% malignant - about 50% undetected before Sx -diagnosis: 72hr fast – hypoglycaemia, Elevated C-peptide and proinsulin -localization: CT, MRI, selective arteriography, selective portovenous sampling
INSULINOMAS:

Surgery: -Most insulinomas are benign and can be Enucleated. Medical: -Metastatic islet cell tumour: i. diazoxide; or ii. Streptozotocin + 5-FU
TREATMENT

-Syndrome: Zollinger-Ellison -Hormone: gastrin -Clinical features: abdo pain, peptic ulceration, diarrhoea, gastric hypersecretion -site: duodenum – 70%; pancreas – 25% - >50% malignant -Diagnosis: increased serum gastrin
>1000pg/ml basal acid output >15mEq/hr -localization: CT/MRI/US –less useful -Somatostatin receptor scin. – sensitive test
GASTRINOMA

Surgery: -Cure rate of 33% in patients with sporadic
cases -If patient has no hepatic metastasis and
limited surgical risk then a distal pancreatectomy, LN Dissection and duodenal exploration.
Medical: -Octreotide Rx for progressive metastatic Gastrinoma – 53% response rate.
TREATMENT

-large; originate almost entirely in pancreas -Hormone: glucagon -Clinical features: hyperglycemia, necrolytic
migratory erythema, DVT, depression -site: >50% pancreas -Diagnosis: elevated levels of glucagon
>500pg/ml -Localization: CT/MRI/selective angiography
GLUCAGONOMA:

Surgery - tumours are found in the tail + body of
pancreas -If tumour can still be localized – resection -Preoperative planning: TPN containing amino- acids, (steroids, Zn supplementation, Abics: Useful for the rash) Medical: -Long term chemotherapy: streptozotocin +/- 5-
FU - Response rate of 30%
TREATMENT

-Large tumours -Hormone: somatostatin -Clinical features: hyperglycemia,
gallstones, wt. loss,steatorrhoea -site: pancreas – 56%; upper intestine – 44% - 70-80% malignant. -Diagnosis: GTT, increased SLI levels, SLI in resected tumour -localization: CT/MRI/selective arteriography
SOMATOSTATINOMA

Surgery: -Due to the high malignant potential, if
tumour can be localized, should be resected. -Metastasis need to be excluded if Whipples
procedure is considered. -At surgery a cholecystectomy should also
be done Medical: -Optimal form of chemotherapy yet to be
determined.
TREATMENT

-Syndrome: WHDA -Hormone: vasoactive intestinel polypeptide -Clinical features: secretory diarrhoea, Hypokalaemia, achlorhydia, met. Acidosis, Flushing, wt. loss -site: pancreas – 90% - >50% malignant -Diagnosis: elevated levels of VIP >160-
225pg/ml -Localization: CT/MRI/Angiography
VIPOMAS

Surgery: -If tumour found excision should be
attempted -Even with metastasis debulking is indicated Medical: -Long term octreotide useful for control of diarrhoea as well as benefit with tumour arrest or regression. - Chemotherapy is rarely of benefit
TREATMENT

They originate in the enterochromaffin cells of the intestine and have the ability to produce various peptides and hormones.
Previously categorised by their embryological origin – foregut, midgut & hindgut.
Revised classification has taken into account tumour location, histological grade and proliferative index
Neuro-endocrine tumours of the gastrointestinal tract (carcinoids) are rare tumours
CARCINOID TUMOURS:

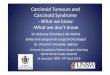
Origin of carcinoid tumors
Digestive sys-tem 64%
Bron-chopul-monary
Others
28%
8%

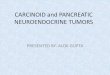
GIT0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
small intestinecolon & rectumstomachothers
Distribution in the GIT

-Typical small neoplasm occurring in submucosa
-Growth of the tumor is slow; vast majority are < 1cm ( 5% > 2cm)
-It grows outward leaving the mucosa intact -As it reaches the serosa it can cause a
desmoplastic reaction and lead to kinking of the bowel
PATHOLOGY

Carcinoid syndrome is almost uniquely associated with midgut carcinoids (neuro-endocrine tumours of the gastrointestinal tract)
Carcinoid syndrome was first described by Thorson and co-workers in 1954
Systemic symptoms are caused by an excess of biogenic amines, peptides and other factors (serotonin, tachy- and bradykinins and histamine) in the circulation only after liver metastases.
Carcinoid Syndrome

Diarrhoea (±80% of patients), mainly caused by serotonin excess, also histamine, kallikrein, prostaglandin, substance P and motilin
Flushing (± 94% ), linked to several humoral factors – tachykinins, serotonin & histamine. Provoked by e.g. nuts & cheese, certain drugs & alcohol
Carcinoid heart disease (± 40% ), characterised by so-called ‘plaques’ at the right side of the heart with involvement of the tricuspid and pulmonary valves and endocardium
Pellagra (± 5% ) characterised by dermatitis,
diarrhoea & dementia – result of niacin deficiency
Intermittent bronchial obstruction (10%) often accompanies flushing,
Carcinoid crisis – rare, potentially fatal – provoked by anaesthesia /surgery if not treated sufficiently with somatostatin analogues
Symptoms

Carcinoid tumours less than 1cm in diameter & confined to the mucosa and submucosa generally remain subclinical for years.
Larger than 1 cm – generally malignant & have metastasized to regional lymph nodes and later to the liver and other locations.
Patients have generally been complaining for years of intermittent abdominal discomfort, erroneously diagnosed as a functional disorder such as irritable bowel.
Intermittent intestinal obstruction due to kinking of the small bowel can occur at a later stage as a result of the desmoplastic reaction in the mesentery
Clinical Presentation

Incidence of midgut (neuro-)endocrine tumours is ± 0.2-2/100 000 population/year
Equal distribution between males & females Incidence is higher in black than white people Most prevalent location is the terminal ileum
close to the ileocaecal valve Is often multiple In up to 15% of patients other malignancies such
as gastrointestinal adenocarcinoma and breast cancer have been demonstrated
Epidemiology

Biochemical diagnosis includes measurements of serum chromogranin A and urinary excretion of 5-HIAA. Estimation of plasma serotonin is facultative
Tumour imaging - transabdominal ultrasound is the initial imaging
procedure in most patients with metastasized carcinoids.
◦ Contrast-enhanced three-phase CT or MRI followed by needle biopsy for pathology can be performed.
◦ In-pentetreotide scintigraphy is positive in 80-90% of patients
◦ Echocardiography is mandatory in patients with carcinoid heart disease
Diagnostic procedures

SURGERY: -Based on site, size and presence/absence
of metastasis. -<1cm: no nodal involvement – segmental
resect. ->1cm: + nodes – wide excision of bowel
and mesentery. -For tumours with widespread metastasis,
Sx is still of benefit.
TREATMENT:

-Is directed to patients with malignant carcinoid syndome and those with widespread metastasis. -Somatostatin analogues ( sandostatin): relief of symptoms (diarrhoea + flushing); also tumor regression (17%) -Serotonin receptor antagonists: used with limited
success. (methysergide no longer used) -Cytotoxic chemotherapy: agents used Streptozotocin + 5-FU/cyclophoshamide (33%)
MEDICAL THERAPY

Targeted chemotherapy agents have been approved in Pancreatic Neuroendocrine Tumors by the FDA based on improved progression free survival
EVEROLIMUS is labelled for patients with unresectable,locally advanced or metastatic disease. The safety and effectiveness of everolimus in carcinoid tumors have not been established.
SUNITINIB is labelled for treatment of progressive,well differentiated PNETs in patients with unresectable,locally advanced or metastatic disease
Platinum & Etoposide combination is sometimes given in pulmonary carcinoids.
CHEMOTHERAPY

This is a type of radioisotope therapy where the tumor is treated intravenously with a peptide or hormone conjugated to a radionuclide or radioligand. This is also called as peptide receptor radionuclide therapy or hormone delivered radiotherapy and can attack all lesions in the body .
Typically radiolabelling octreotate to lutetium 177, yttrium 90 or indium 111 is done.
This is a highly targetted and effective therapy with minimal side effects in tumors with high levels of cell surface somatostatin receptors. Radiation is taken up at the sites of tumor or excreted in urine.
HORMONE DELIVERED RADIOTHERAPY

Metastasis to liver can be treated by hepatic artery treatments based on the observation that tumor cells get nearly all their nutrients from the hepatic artery. Hepatic artery embolization or chemoembolization occludes the blood flow to the tumor achieving significant shrinkage in over 80% of cases.
Selective internal radiation therapy deliver radioactive microsphere by injection into the hepatic artery.
OTHER THERAPIES

Radiofrequency ablation is used when a patient has relatively few metastases.
Cryoablation has been less successful for GEP-NETs than RFA.
Other therapies.......

EPOTHILONE B:- A novel cytotoxic agent It is a potent anti angiogenesis agent. It acts by blocking the polymerization of
tubulin in blood vessels Action is similar to that of taxane More suitable for slow growing tumors.
NEWER DRUG

-Best prognosis of all small bowel tu’s -Resection of localized tu – 100% survival
rate -65% for patients with regional disease; - 25-35% for patients with distant
metastasis.
PROGNOSIS:

multiple endocrine neoplasia type 1 (MEN1) multiple endocrine neoplasia type 2 (MEN2) von Hippel-Lindau (VHL) disease neurofibromatosis type 1 tuberous sclerosis Carney complex
FAMILIAL SYNDROMES

ALGORITHM OF OVERALL CARE

Immediate onset of a debilitating and life-threatening condition associated with carcinoid syndrome
May occur spontaneously or may be precipitated by anesthesia, chemotherapy, infection, stress, catecholamines, tumor manipulation or embolization procedures
Symptoms include prolonged severe flushing, diarrhea, hypotension,tachycardia, severe dyspnea, peripheral cyanosis and sometimes hemodynamic instability.
Appropriate precautions include immediate therapy and close monitoring before, during and after surgical treatment.
CARCINOID CRISIS

Prophylactic administration of octreotide must be given by continuous intravenous infusion at a dose of 50 μg/h for 12 hours prior to and at least 48 hours after the procedure to prevent a cardiovascular carcinoid crisis.
Carcinoid Crisis - Prevention

ANAESTHETIC CONSIDERATIONS

For anaesthetic purposes,patients with carcinoid tumors should be regarded as suffering from a multi-system disease and so require thorough pre-planning f/b post operative management in a high dependency environment.
Main aims are to maintain normal haemodynamics and prevention of occurrence of carcinoid crisis.
Principles of anaesthetic management for carcinoid

History and Examination: signs/symptoms suggestive of ongoing
uncontrolled hormonal activity-diarrhoea,flushing,skin lesions,carcinoid syndrome.
Cardiovascular history-reduced exercise tolerance,orthopnoea,paroxysmal dyspnoea,peripheral oedema
Even if patients lack symptoms,there is potential for unpredictable,uncontrolled hormone release precipitated by anaesthetic/surgical stimulus.
Pre-operative assessment

INVESTIGATIONS: CXR-carcinoid lesions or miliary shadowing of
lungs. ECG- RVH ECHO- Rt.side carcinoid S.Electrolytes-effects of chronic diarrhoea LFT- deranged when liver is infiltrated. CBC- diffuse marrow spread Clotting studies Cross match sample 24 hr urine- 5HIAA
Preop assessment.....

Titration of adrenergic,histaminic and serotonergic receptor blocking drugs to maximum effect.
Monitoring intravascular volume status Octreotide infusion 50 microgram/hr for at
least 12 h immediately before surgery and 48 h after surgery should reduce tumor hormonal activity.
PRE-OPERATIVE PREPARATION

REGIONAL ANAESTHESIA: Thoracic epidural insertion before induction of GA
is a reasonable technique to help achieve good pain relief and reduce post operative atelectasis.
It provides excellent analgesia thereby reducing the risk of carcinoid crisis. However,potential hypotension may require vasoconstrictors that may lead to exaggerated response.
The balance of risks would seem to favour the use of epidurals with drug volumes and concentrations cautiously titrated to blood pressure response.
ANAESTHETIC TECHNIQUES

GENERAL ANAESTHESIA: The primary aim is to provide stable,controlled
conditions and avoiding stimulatory factors. Reliable large bore access in case of rapid volume
loss Availability of fluid warmers Use of rapid infusion system are sensible
standards. Stable induction,adequate depth of anaesthesia
before intubation and maintenance of anaesthesia& analgesia peri-operatively are key to preventing instability.
ANAESTHETIC TECHNIQUES

Histamine releasers are AVOIDED- eg. atracurium,mivacurium,morphine
Suxamethonium has been implicated in release of peptides from liver as a result of depolarization induced fasciculations. To be AVOIDED.
Ramifentanyl 0.05-0.2 microgram/kg/min may have a role in optimizing intubating conditions,provision of titrable analgesia & intraop BP control.
Monitoring-ECG,Pulse oximetry,Non-invasive BP,Temp.,EtCO2,arterial& CVP monitoring,Pulmonary a.floatation catheter, oesophageal doppler.
General Anaesthesia.....

There is a risk of hypo or hypertension developing intraoperatively
The response to inotropes or vasopressors is unpredictable. Norepinephrine and epinephrine can be hazardous in carcinoid patients
Practically,small doses of phenylephrine has been helpful.
Aprotinin – a kallikrien antagonist has a significant place in symptomatic control peroperatively.
INTRA-OPERATIVE MANAGEMENT

If prolonged vasocontriction is required,vasopressin can be used.
Vasoactive hormone release intraop is best treated with iv boluses of 20-50microgram of octreotide titrated to hemodynamic response
Blood loss monitoring is very important. For prolonged hypertension,labetolol
infusion have been used.
INTRA-OPERATIVE MANAGEMENT

As with the intra-operative management, post-operative care focuses on the provision of stable cardio-respiratory conditions and adequate analgesia.
High-dependency care is recommended. Ongoing hormonal control of the tumour is important as post-operative crisis are possible and surgery may have been aimed at reducing the bulk of carcinoid tumour present, rather than eliminating it.
Intravenous and then subcutaneous octreotide follow-up will help control any further hormone release and there may well be residual, hormonally active tumour remaining.
Forty-eight hours of invasive monitoring, analgesia and fluid management may be required to ensure safe recovery from the surgery.
POST OPERATIVE MANAGEMENT

There has been a review of the biology of enteroendocrine tumours over the past 1-2 decades, and significant advances have been made. There is a need for enhanced awareness of theheterogenous features of these tumours as well asmultiplicity of modalities available for their treatment. Increasing acceptance of the more aggressive and
customized treatment with recognition that favorable responses in these pts result from sequential use of multiple modalities.
CONCLUSION

Miller’s Anaesthesia-7th edition Churchill and Davidson-5th & 6th editions Oxford journal- CEACCP 2011;11(1):9-13 Int Anesthesiol Clin 1997;35(4):129-42 http://pharmalicensing.com
REFERENCES

THANK YOU