Embed Size (px)
Citation preview
9/21/19
1
Linda J. Hood, Ph.D.Professor, Hearing and Speech Sciences,
Director, Auditory Physiology Research Laboratory,Vanderbilt University, USA
Visiting Professor, Faculty of Education, Division of Speech and Hearing Sciences, University of Hong Kong, HONG KONG
International Key Scientist, The Hearing CRC – Cooperative Research Centre, AUSTRALIA
A Clinical Mismatch: Implications for understanding and managing neural hearing loss
1
The Cross-Check PrincipleJerger JF, Hayes D. 1976. The cross-check principle in pediatric audiometry. Archives of Otolaryngology 102, 614-620.
Abstract“We discuss a method of pediatric audiologic assessment that employs the "cross-check principle". That is, the results of a single test are cross-checked by an independent test measure. Particularly useful in pediatric evaluations as cross-checks of behavioral test results are impedance audiometry and brain-stem-evoked response audiometry (BSER).”
Cross-check:Measure 1Measure 2Measure 3
All should agree
✔
The importance of behavioral and physiologic cross-checks
2
The Cross-Check Principle
• Behavioral responses– Detection thresholds, speech recognition– Other suprathreshold measures
• Physiologic responses– Tympanometry, wideband acoustic immittance (WAI)– Otoacoustic emissions (OAE)– Auditory evoked potentials– Middle-ear muscle reflex (MEMR)– Medial olivocochlear reflex (MOCR)
3
An Audiologic Test Strategy
The combination of:• Tympanograms• Middle ear muscle reflexes• Otoacoustic emissions
…can provide objective information to distinguish conductive, sensory, and neural hearing loss.
Berlin, Hood, Morlet et al.
4
An Audiologic Test Strategy
• Tymps abnormal, MEMRs elevated/absent, OAEs absent - Conductive
• Tymps normal, MEMRs normal, OAEs normal - Thresholds < 35 dB HL
• Tymps normal, MEMRs normal, OAEs absent - Thresholds most likely between 35-60 dB HL
• Tymps normal, MEMRs elevated/absent, OAEs absent - Thresholds > 60 dB HL or neural
• Tymps normal, MEMRs absent, OAEs present - Auditory neuropathy/dys-synchrony; neural disorder
The combination of: Tympanograms, middle-ear muscle reflexes, OAEs…
Berlin, Hood, Morlet et al.
5
Gravel & Hood, 1999Test Battery Approach
Observation Audiometry(cross-check &
auditory function)
ABRFS (AC & BC)
Click-neuro
TympanometryAMEMR
EOAE
Birth - 4 mos
ABRFS (AC &BC) & click-neuro(cross-check & documentphysiologic function)
VRAEar-specific
TympanometryAMEMR
EOAE
5/6 mos - 24 mos
ABRFS (AC & BC) & click-neuro(cross-check & documentphysiologic function)
Play AudiometryEar-specific
TympanometryAMEMR
EOAE
24 mos- 4 yrs
Comprehensive Audiologic Assessment(includes in-depth case history)
6
9/21/19
2
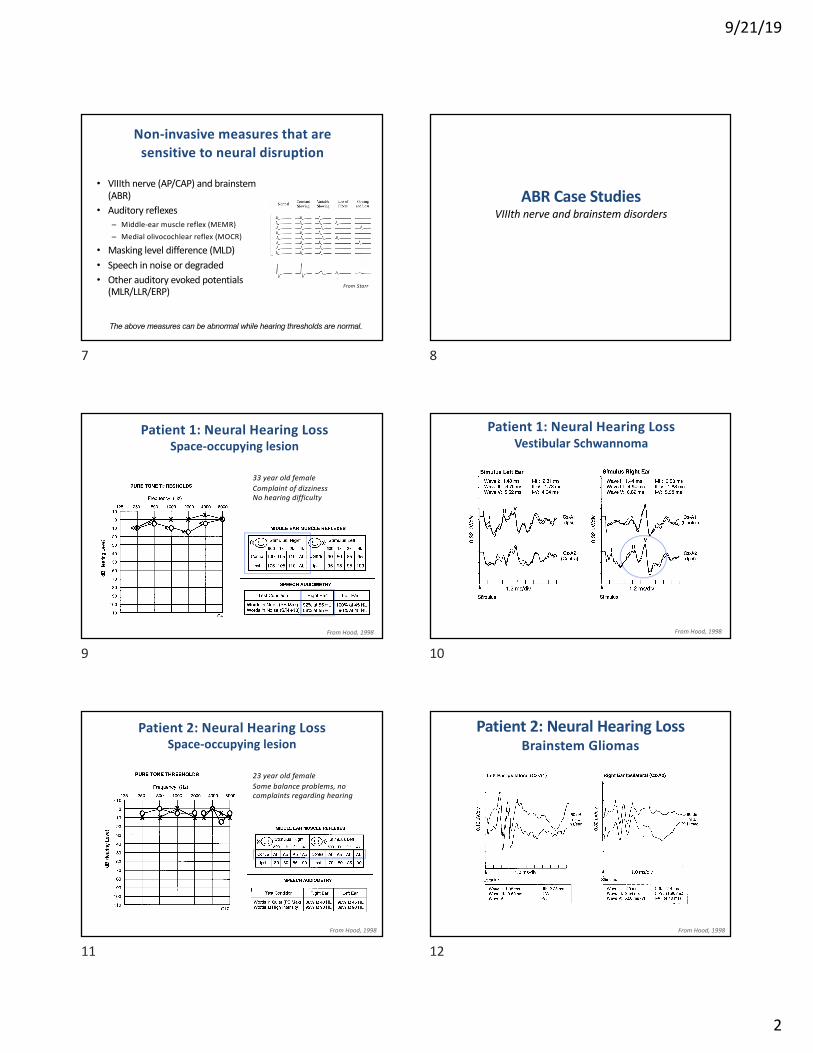
Non-invasive measures that are sensitive to neural disruption
• VIIIth nerve (AP/CAP) and brainstem (ABR)
• Auditory reflexes– Middle-ear muscle reflex (MEMR)– Medial olivocochlear reflex (MOCR)
• Masking level difference (MLD)• Speech in noise or degraded• Other auditory evoked potentials
(MLR/LLR/ERP)
The above measures can be abnormal while hearing thresholds are normal.
From Starr
7
ABR Case StudiesVIIIth nerve and brainstem disorders
8
Patient 1: Neural Hearing LossSpace-occupying lesion
33 year old femaleComplaint of dizzinessNo hearing difficulty
From Hood, 1998
9
Patient 1: Neural Hearing LossVestibular Schwannoma
From Hood, 1998
10
Patient 2: Neural Hearing LossSpace-occupying lesion
23 year old femaleSome balance problems, no complaints regarding hearing
From Hood, 1998
11
Patient 2: Neural Hearing LossBrainstem Gliomas
From Hood, 1998
12
9/21/19
3
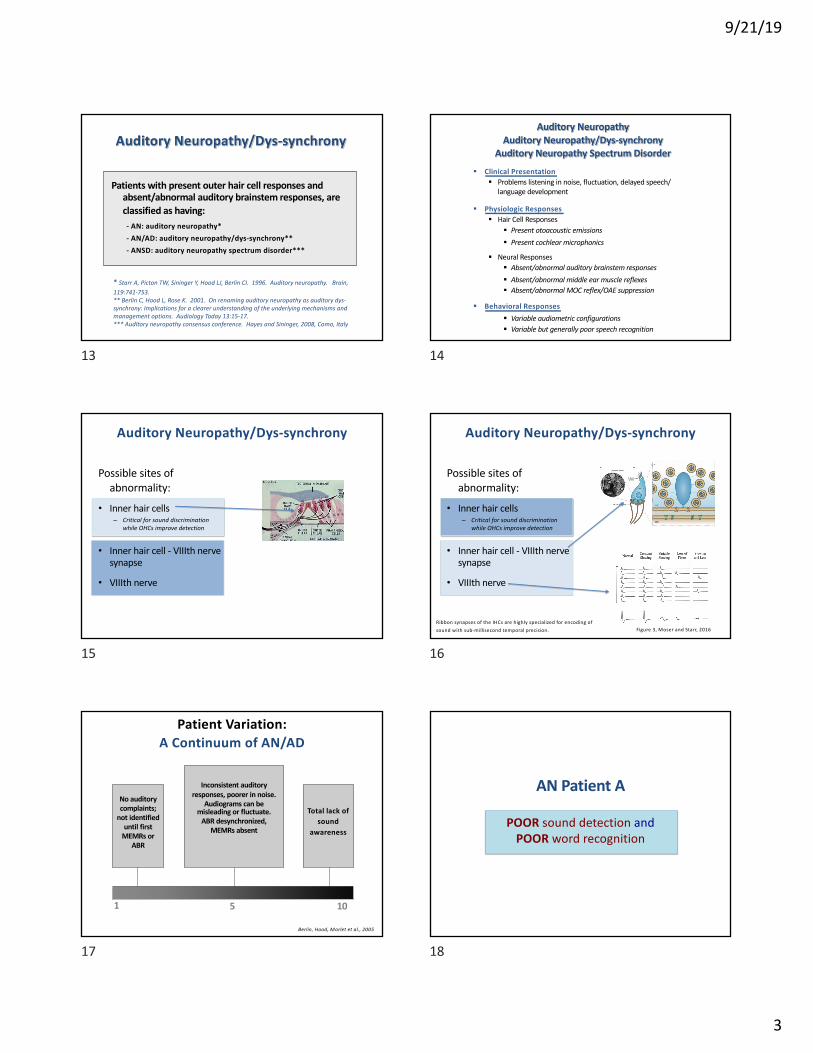
Patients with present outer hair cell responses and absent/abnormal auditory brainstem responses, are classified as having:
- AN: auditory neuropathy*- AN/AD: auditory neuropathy/dys-synchrony**- ANSD: auditory neuropathy spectrum disorder***
Auditory Neuropathy/Dys-synchrony
* Starr A, Picton TW, Sininger Y, Hood LJ, Berlin CI. 1996. Auditory neuropathy. Brain, 119:741-753.** Berlin C, Hood L, Rose K. 2001. On renaming auditory neuropathy as auditory dys-synchrony: Implications for a clearer understanding of the underlying mechanisms and management options. Audiology Today 13:15-17.*** Auditory neuropathy consensus conference. Hayes and Sininger, 2008, Como, Italy
13
Auditory NeuropathyAuditory Neuropathy/Dys-synchrony
Auditory Neuropathy Spectrum Disorder
§ Clinical Presentation§ Problems listening in noise, fluctuation, delayed speech/
language development
§ Physiologic Responses§ Hair Cell Responses
§ Present otoacoustic emissions§ Present cochlear microphonics
§ Neural Responses§ Absent/abnormal auditory brainstem responses§ Absent/abnormal middle ear muscle reflexes§ Absent/abnormal MOC reflex/OAE suppression
§ Behavioral Responses§ Variable audiometric configurations§ Variable but generally poor speech recognition
14
Auditory Neuropathy/Dys-synchrony
Possible sites of abnormality:
• Inner hair cells– Critical for sound discrimination
while OHCs improve detection
• Inner hair cell - VIIIth nerve synapse
• VIIIth nerve
15
Auditory Neuropathy/Dys-synchrony
Possible sites of abnormality:
• Inner hair cells– Critical for sound discrimination
while OHCs improve detection
• Inner hair cell - VIIIth nerve synapse
• VIIIth nerve
Figure 3, Moser and Starr, 2016Ribbon synapses of the IHCs are highly specialized for encoding of sound with sub-millisecond temporal precision.
16
Inconsistent auditory responses, poorer in noise.
Audiograms can be misleading or fluctuate.
ABR desynchronized,MEMRs absent
No auditorycomplaints;
not identifieduntil first
MEMRs or ABR
Total lack of sound
awareness
5 101
Patient Variation:A Continuum of AN/AD
Berlin, Hood, Morlet et al., 2005
17
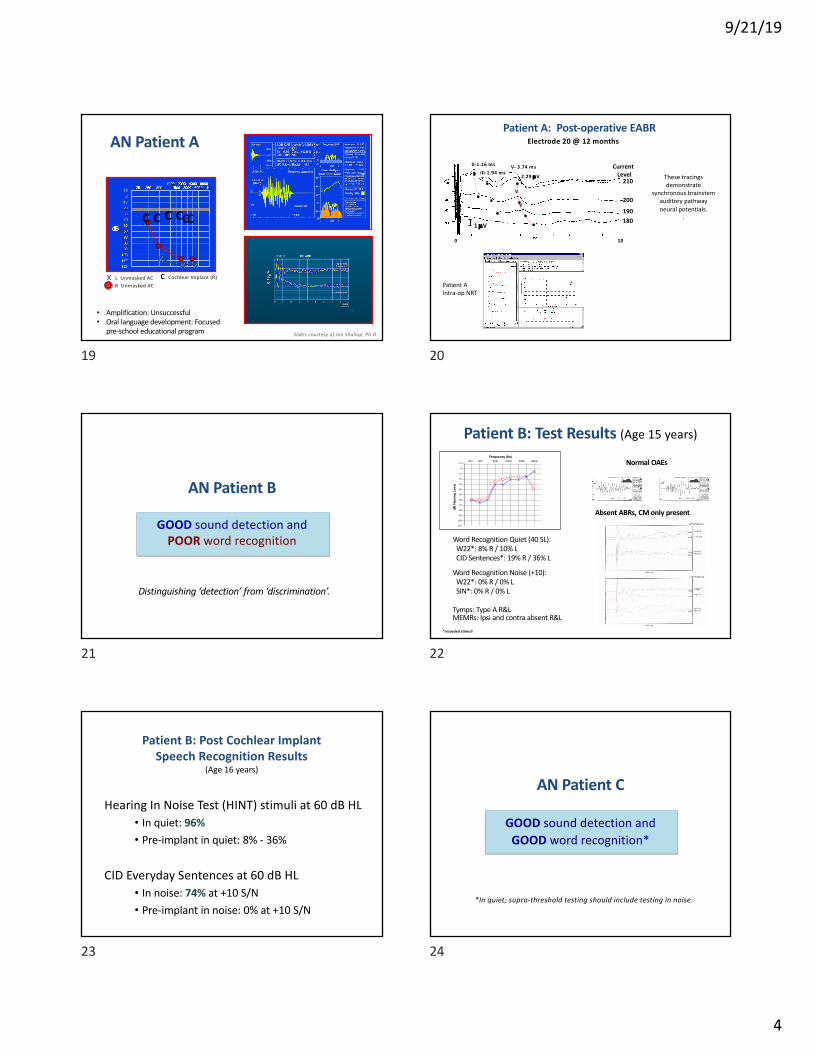
AN Patient A
POOR sound detection and POOR word recognition
18
9/21/19
4
x
x
xx
C C C C CC
x L Unmasked ACR Unmasked AC
C Cochlear Implant (R)
AN Patient A
• Amplification: Unsuccessful• Oral language development: Focused
pre-school educational program Slides courtesy of Jon Shallop, Ph.D.
19
Patient A: Post-operative EABRElectrode 20 @ 12 months
Case C Post-op EABR
II-1.16 msIII-1.94 ms
V- 3.74 ms
V
V
2.29 µV
1 µV
0 10
...
Current Level
210
200
190180
..
... .
These tracings demonstrate
synchronous brainstem auditory pathwayneural potentials.
.
Patient A Intra-op NRT
20
AN Patient B
GOOD sound detection and POOR word recognition
Distinguishing ‘detection’ from ‘discrimination’.
21
Patient B: Test Results (Age 15 years)
1 2 3 4 5 6 7 8 9 10 11110
100
90
80
70
60
50
40
30
20
10
0
-10
Frequency (Hz)250 500 1000 2000 4000 8000
dB H
earin
g Le
vel
B C
*recorded stimuli
Word Recognition Quiet (40 SL):W22*: 8% R / 10% LCID Sentences*: 19% R / 36% L
Word Recognition Noise (+10):W22*: 0% R / 0% LSIN*: 0% R / 0% L
Tymps: Type A R&LMEMRs: Ipsi and contra absent R&L
Normal OAEs
Absent ABRs, CM only present
22
Patient B: Post Cochlear Implant Speech Recognition Results
(Age 16 years)
Hearing In Noise Test (HINT) stimuli at 60 dB HL• In quiet: 96% • Pre-implant in quiet: 8% - 36%
CID Everyday Sentences at 60 dB HL• In noise: 74% at +10 S/N• Pre-implant in noise: 0% at +10 S/N
23
AN Patient C
GOOD sound detection and GOOD word recognition*
*In quiet; supra-threshold testing should include testing in noise.
24
9/21/19
5
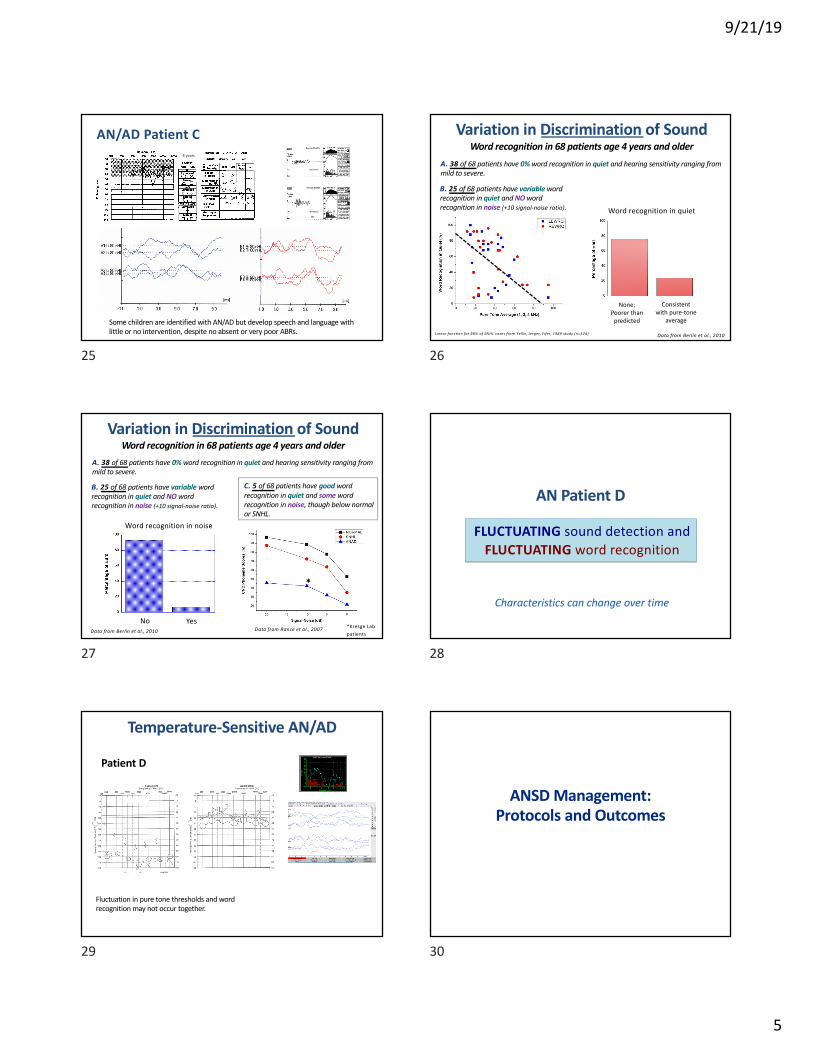
AN/AD Patient C
Some children are identified with AN/AD but develop speech and language with little or no intervention, despite no absent or very poor ABRs.
4 years
25
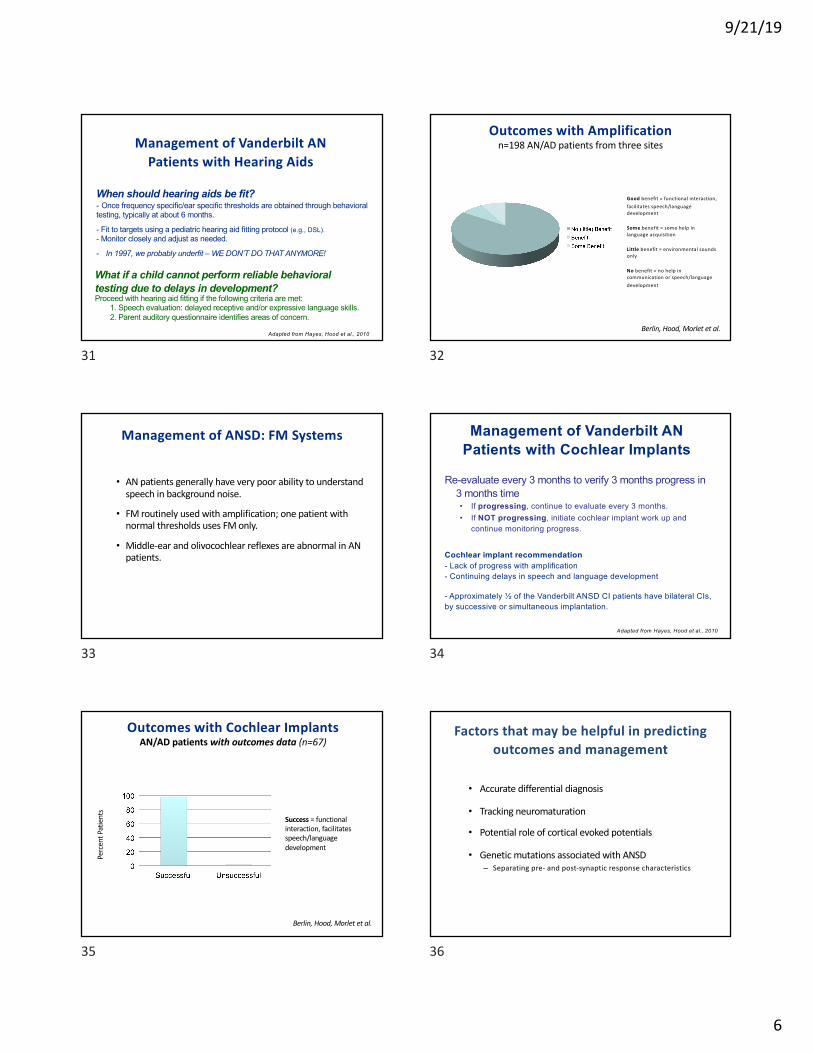
Variation in Discrimination of SoundWord recognition in 68 patients age 4 years and older
Linear function for 98% of SNHL cases from Yellin, Jerger, Fifer, 1989 study (n=324)
A. 38 of 68 patients have 0% word recognition in quiet and hearing sensitivity ranging from mild to severe.
B. 25 of 68 patients have variable word recognition in quiet and NO word recognition in noise (+10 signal-noise ratio).
None;Poorer than
predicted
Consistent with pure-tone
average
Word recognition in quiet
Data from Berlin et al., 2010
26
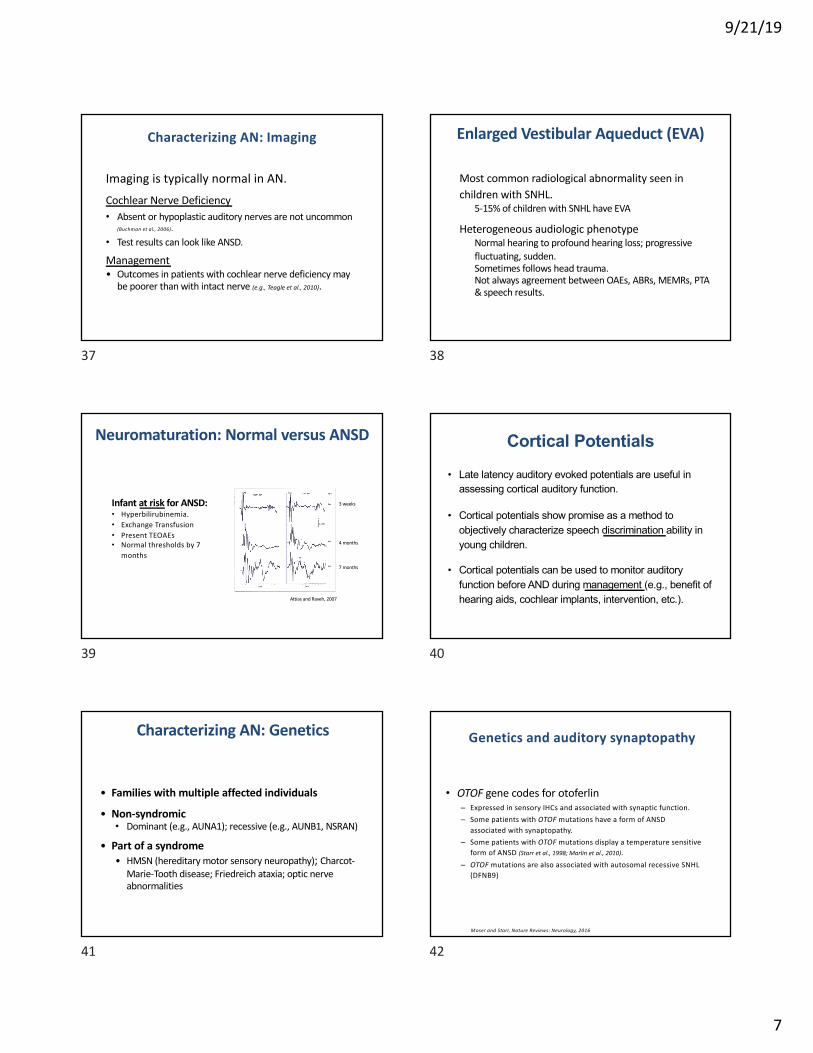
Variation in Discrimination of SoundWord recognition in 68 patients age 4 years and older
A. 38 of 68 patients have 0% word recognition in quiet and hearing sensitivity ranging from mild to severe.
B. 25 of 68 patients have variable word recognition in quiet and NO word recognition in noise (+10 signal-noise ratio).
C. 5 of 68 patients have good word recognition in quiet and some word recognition in noise, though below normal or SNHL.
Data from Rance et al., 2007
*
*Kresge Lab patients
Word recognition in noise
No YesData from Berlin et al., 2010
27
AN Patient D
FLUCTUATING sound detection and FLUCTUATING word recognition
Characteristics can change over time
28
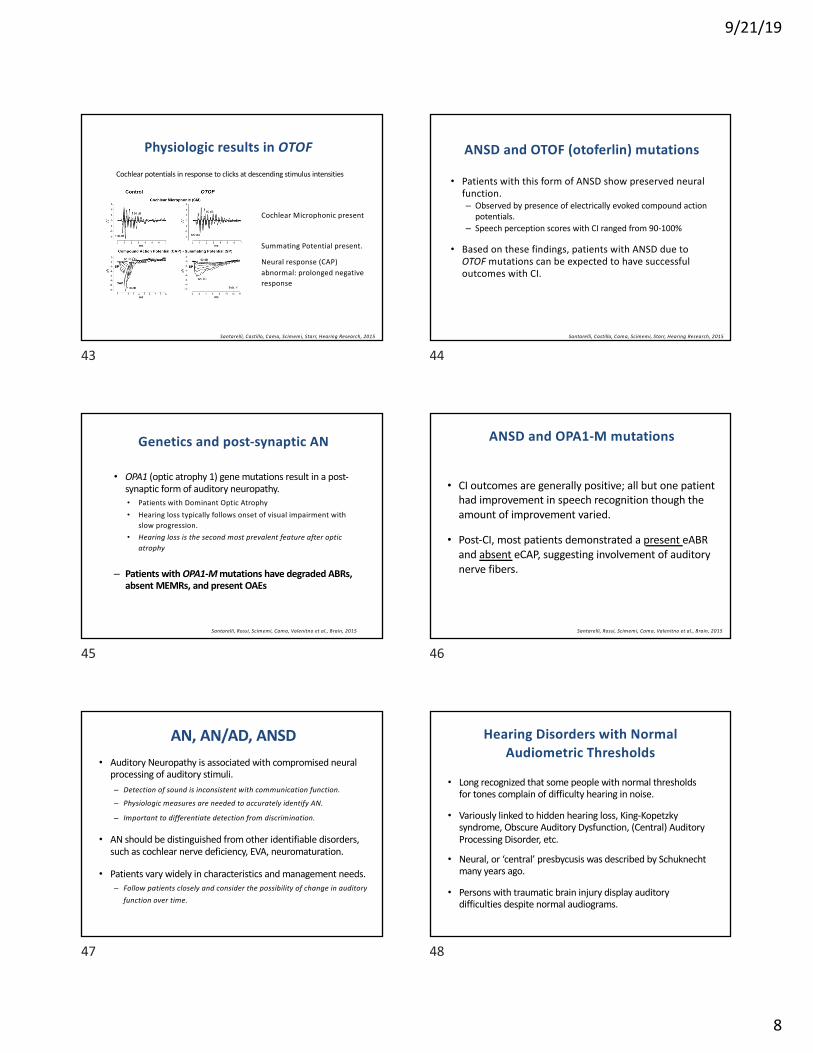
Temperature-Sensitive AN/AD
Fluctuation in pure tone thresholds and word recognition may not occur together.
Patient D
29
ANSD Management: Protocols and Outcomes
30
9/21/19
6
Management of Vanderbilt AN Patients with Hearing Aids
Adapted from Hayes, Hood et al., 2010
What if a child cannot perform reliable behavioral testing due to delays in development?Proceed with hearing aid fitting if the following criteria are met:
1. Speech evaluation: delayed receptive and/or expressive language skills.2. Parent auditory questionnaire identifies areas of concern.
When should hearing aids be fit?- Once frequency specific/ear specific thresholds are obtained through behavioral testing, typically at about 6 months.
- Fit to targets using a pediatric hearing aid fitting protocol (e.g., DSL).- Monitor closely and adjust as needed.
- In 1997, we probably underfit – WE DON’T DO THAT ANYMORE!
31
Outcomes with Amplificationn=198 AN/AD patients from three sites
Good benefit = functional interaction, facilitates speech/language development
Some benefit = some help in language acquisition
Little benefit = environmental sounds only
No benefit = no help in communication or speech/language development
Berlin, Hood, Morlet et al.
32
Management of ANSD: FM Systems
• AN patients generally have very poor ability to understand speech in background noise.
• FM routinely used with amplification; one patient with normal thresholds uses FM only.
• Middle-ear and olivocochlear reflexes are abnormal in AN patients.
33
Cochlear implant recommendation- Lack of progress with amplification- Continuing delays in speech and language development
- Approximately ½ of the Vanderbilt ANSD CI patients have bilateral CIs, by successive or simultaneous implantation.
Management of Vanderbilt AN Patients with Cochlear Implants
Re-evaluate every 3 months to verify 3 months progress in 3 months time• If progressing, continue to evaluate every 3 months.• If NOT progressing, initiate cochlear implant work up and
continue monitoring progress.
Adapted from Hayes, Hood et al., 2010
34
Outcomes with Cochlear ImplantsAN/AD patients with outcomes data (n=67)
Perc
ent P
atie
nts
Success = functional interaction, facilitates speech/language development
Berlin, Hood, Morlet et al.
35
Factors that may be helpful in predicting outcomes and management
• Accurate differential diagnosis
• Tracking neuromaturation
• Potential role of cortical evoked potentials
• Genetic mutations associated with ANSD– Separating pre- and post-synaptic response characteristics
36
9/21/19
7
Characterizing AN: Imaging
Imaging is typically normal in AN.
Cochlear Nerve Deficiency • Absent or hypoplastic auditory nerves are not uncommon
(Buchman et al., 2006).
• Test results can look like ANSD.
Management• Outcomes in patients with cochlear nerve deficiency may
be poorer than with intact nerve (e.g., Teagle et al., 2010).
37
Enlarged Vestibular Aqueduct (EVA)
Most common radiological abnormality seen in children with SNHL.
5-15% of children with SNHL have EVA
Heterogeneous audiologic phenotypeNormal hearing to profound hearing loss; progressive fluctuating, sudden.Sometimes follows head trauma.Not always agreement between OAEs, ABRs, MEMRs, PTA & speech results.
38
Neuromaturation: Normal versus ANSD
Infant at risk for ANSD:• Hyperbilirubinemia.• Exchange Transfusion• Present TEOAEs• Normal thresholds by 7
months
Attias and Raveh, 2007
3 weeks
7 months
4 months
39
Cortical Potentials
• Late latency auditory evoked potentials are useful in assessing cortical auditory function.
• Cortical potentials show promise as a method to objectively characterize speech discrimination ability in young children.
• Cortical potentials can be used to monitor auditory function before AND during management (e.g., benefit of hearing aids, cochlear implants, intervention, etc.).
40
Characterizing AN: Genetics
• Families with multiple affected individuals
• Non-syndromic • Dominant (e.g., AUNA1); recessive (e.g., AUNB1, NSRAN)
• Part of a syndrome• HMSN (hereditary motor sensory neuropathy); Charcot-
Marie-Tooth disease; Friedreich ataxia; optic nerve abnormalities
41
• OTOF gene codes for otoferlin– Expressed in sensory IHCs and associated with synaptic function. – Some patients with OTOF mutations have a form of ANSD
associated with synaptopathy.– Some patients with OTOF mutations display a temperature sensitive
form of ANSD (Starr et al., 1998; Marlin et al., 2010). – OTOF mutations are also associated with autosomal recessive SNHL
(DFNB9)
Moser and Starr, Nature Reviews: Neurology, 2016
Genetics and auditory synaptopathy
42
9/21/19
8
Cochlear potentials in response to clicks at descending stimulus intensities
Cochlear Microphonic present
Summating Potential present.
Neural response (CAP) abnormal: prolonged negative response
Physiologic results in OTOF
Santarelli, Castillo, Cama, Scimemi, Starr, Hearing Research, 2015
43
ANSD and OTOF (otoferlin) mutations
• Patients with this form of ANSD show preserved neural function.– Observed by presence of electrically evoked compound action
potentials.– Speech perception scores with CI ranged from 90-100%
• Based on these findings, patients with ANSD due to OTOF mutations can be expected to have successful outcomes with CI.
Santarelli, Castillo, Cama, Scimemi, Starr, Hearing Research, 2015
44
• OPA1 (optic atrophy 1) gene mutations result in a post-synaptic form of auditory neuropathy.• Patients with Dominant Optic Atrophy • Hearing loss typically follows onset of visual impairment with
slow progression.• Hearing loss is the second most prevalent feature after optic
atrophy
– Patients with OPA1-M mutations have degraded ABRs, absent MEMRs, and present OAEs
Genetics and post-synaptic AN
Santarelli, Rossi, Scimemi, Cama, Valenitno et al., Brain, 2015
45
• CI outcomes are generally positive; all but one patient had improvement in speech recognition though the amount of improvement varied.
• Post-CI, most patients demonstrated a present eABRand absent eCAP, suggesting involvement of auditory nerve fibers.
ANSD and OPA1-M mutations
Santarelli, Rossi, Scimemi, Cama, Valenitno et al., Brain, 2015
46
AN, AN/AD, ANSD • Auditory Neuropathy is associated with compromised neural
processing of auditory stimuli.– Detection of sound is inconsistent with communication function.
– Physiologic measures are needed to accurately identify AN.
– Important to differentiate detection from discrimination.
• AN should be distinguished from other identifiable disorders, such as cochlear nerve deficiency, EVA, neuromaturation.
• Patients vary widely in characteristics and management needs.– Follow patients closely and consider the possibility of change in auditory
function over time.
47
Hearing Disorders with Normal Audiometric Thresholds
• Long recognized that some people with normal thresholds for tones complain of difficulty hearing in noise.
• Variously linked to hidden hearing loss, King-Kopetzkysyndrome, Obscure Auditory Dysfunction, (Central) Auditory Processing Disorder, etc.
• Neural, or ‘central’ presbycusis was described by Schuknecht many years ago.
• Persons with traumatic brain injury display auditory difficulties despite normal audiograms.
48
9/21/19
9
Cochlear Synaptopathy: A Paradigm Shift
Previously Thought: Temporary threshold shift (TTS) is only temporary with complete recovery.
A new way of thinking about the effects of noise on hearing.
Kujawa and Liberman (2009) reported loss of cochlear neural synapses following noise exposure in an animal model. • After a temporary threshold shift:
• Thresholds returned to normal.• Cochlear hair cell function was preserved.• BUT… neural connections were permanently disrupted.
49
General SummaryNeural disorders and auditory thresholds
– Patients with ANSD, central APD, and other neural or synaptic disorders require characterization of supra-threshold function to accurately describe and manage their auditory difficulties.
– Sensitive evaluation methods, beyond the audiogram, and genetics provide information about site of lesion and underlying mechanisms.
– Speech in noise testing should be a routine clinical procedure!
Applying the “Cross-Check Principle” continues to be an important key in audiologic evaluation.
C ro s s -c h e c k :
M e as u re 1M e as u re 2
M e as u re 3
A ll s h o u ld ag re e
✔
50
Current research supported by the NIH-NIDCD. Past research supported by the NIH-NIDCD, Oberkotter Foundation, Deafness Research Foundation, American Hearing Research Foundation, National Organization for Hearing Research, Marriott Foundation, Kam’s Fund for Hearing Research, Vanderbilt University Development Funds, Vanderbilt Bill Wilkerson Center
The Hood Lab at Vanderbilt UniversityPresent: Mary Edwards Ferguson AuD, Lauren Roberts AuD, Jordan Racca BA, Janice Creel, Steven Carter BA, Javier Santos BA, Jeff Wise BA, Laura Tatro BA, Rachel Kirby BA, Krystina Schultz BA.
Past: : Heather McCaslin AuD, Ray Li, Sarah Camera BA, Susan Reynolds AuD, John Lee AuD, Carol Pang AuD, Sarah Steele AuD, Lindsey Rentmeester AuD, Kelsey Hatton AuD, Susan Stangl AuD, Kristen D’Onofrio AuD, Christopher Spankovich AuD PhD, Erin Maloff PhD, Claire Umeda AuD, Liz Agboola BA
Current Collaborators: Rafael Delgado PhD, John Durrant PhD, Beth Prieve PhD, Alexandra Key PhD, Sharon Kujawa PhD, Stephane Maison PhD, Dan Polley PhD, Charles Liberman PhD
Consultants: Glenis Long PhD, Carrick Talmadge PhD
VanderbiltUniversity
Collaborators at the Kresge Hearing Research LaboratoryLouisiana State University Health Sciences Center, New Orleans, Louisiana: Charles I. Berlin PhD, Thierry Morlet PhD, Harriet Berlin MS, Leah Barter MS, Jill Bordelon MCD, Shanda Brashears AuD, Jennifer Jeanfreau AuD, Bronya Keats PhD, Annette Larmieu PhD, Li Li MD, Elizabeth Montgomery AuD, Kelly Rose Mattingly MA, Patti St. John AuD, Sonya Tedesco MCD, Melanie Thibodeaux MCD, Han Wen MSBE, Diane Wilensky MS
51





























