Embed Size (px)
DESCRIPTION
Homicidal Incised Wounds Thorax
Citation preview

SA MEDIESE TYDSKRIF DEEL 65 10 MAART 1984 385
Homicidal penetrating incised woundsof the thoraxAn autopsy study of 52 cases
J. J. MOAR
Summary
During March-June and August-September 1981, 245medicolegal autopsies were conducted by the authorat the Johannesburg and Diepkloof government mortuaries. In 52 cases (21,2%) penetrating incisedwounds of the thorax were found to be the cause ofdeath. These involved diverse and often multiplethoracic structures - ventricles, atria, interventricularseptum, lungs, and, in particular, blood vessels. Inmost of these cases death was ascribed to eitherexsanguination and the attendant hypovolaemic shockor, in those wounds involving the pericardium andmyocardium, cardiac tamponade.
Several findings emerged from this study. (I) an.abysmally low number of the victims (5,8%) reached amedical facility alive; (ii) no females were seen, and the21 - 3O-year age group predominated (46,2%); (iit)80,8% had arrived at the casualty departmentduring aweekend; (iv) 71,2% had received a single fatal penetrating incised wound; (v) nearly two-thirds of thewounds seen were inflicted over the precordial area;(vI) almost 80% of the victims had a positive bloodal~hollevel,-thisranging from 10 mg/dl to 340 mg/dl;(vii) there was a paucity of blunt force injuries inaddition to the primary penetrating incised wound/s;and (viii) there was a low percentage of 'defence'wounds among these victims of homicidal assaults.
S AIr lied J 1984; 65: 385-389.
The infliction of penetrating incised wounds of the thorax bymeans ofa sharp-edged or pointed instrument dates back to earlyrecorded history and probably to prehistoric times as well. Theearly writings of mankind (from the Ancient Sumerians andEgyptians to the Ancient Greeks and Romans), contain manydescriptions of penetrating wounds and their treatment by thephysicians ofthe day. The most famous example, Homer's Iliad,records 147 battlefield injuries, ofwhich 106 were spear wounds(80% mortality), 17 sword thrusts (100% mortality), 12 arrowwounds (42% mortality) and the rest sling wounds. Of thesewounds, 67 (46%) were inflicted on the chest. .
The advent of modem firearms appears to have made littleimpact on the use ofthe knife or its analogues as an instrument ofviolence - here the ordinary household utensil or workshop tool
Department of Forensic Medicine, University of the Witwatersrand, JohannesburgJ. J. MOAR, M.B. CH.B.
Panly based on a dissertation submitted for the degree of M.Med. (Forensic Pathol.) of theUniversity of the Witw3tCrsrand.
acquires the medicolegal connotation ofa weapon. Furthermore,should the victim of an anack by such a weapon die, it falls to theforensic pathologist to ascertain the nature of the injuriessustained and their role in the causation of death. In cases inwhich the victim reaches a medical facility alive and is operatedupon, initial accurate documentation of the wound and itsrelevant external features can be of vital importance not only inreconstructing the fatal incident but also in correlating thewound with the causative weapon. That this is not alwayspossible (for example, a laterally situated chest wound may beutilized for the insertion of an intercostal drain, therebydistorting its original dimensions) is regrenable but understandable in view of the circumstances - the patient is inextremis and all other considerations must be ·cast aside in theanempt to save a life.
Subjects and methods
During March-June and August-September 1981,245 medicolegal autopsies were conducted by the author at the Johannesburgand Diepkloof government mortuaries. In 52 of these (21,2%)penetrating incised thoracic wounds involving diverse and oftenmultiple thoracic structures (ventricles, atria, lungs and bloodvessels) were found. Major vessels such as the aorta, pulmonaryarteries, subclavian veins and superior vena cava were involved,as well as lesser ones such as the internal thoracic artery andintercostal vessels. In most cases death was ascribed to eitherexsanguination and the anendant hypovolaemic shock or, inthose wounds involving the pericardium and myocardium,cardiac tamponade. In view of the overwhelming number ofsubjects who were dead on arrival at a medical facility, the role, ifany, of contributory factors such as cardiac arrhythmias couldnot be determined.
All of the subjects were victims of homicidal assaults withsharp-edged or pointed weapons; there were no cases ofaccidental injury or suicide. Age, sex and race were noted in eachcase, as well as the time ofday and day ofthe week. Whether thesubject reached hospital dead or alive was also noted and, if thelaner, so was the duration of inhospital survival. Except for the 3subjects who died in hospital, the precise time ofdeath could notbe ascertained; hence neither the postmortem interval (definedas the period from death until discovery or autopsy) nor thesurvival period (the period from time of injury until time ofdemise) could be determined. This is in contrast to normalanatomical pathology autopsies - the patient dies in hospitaland knowledge ofthe exact time ofdeath enables the postmorteminterval to be accurately determined. In assessing the survivalperiod, use of the electron microscope to detect the presence ofmyofibroblasts in the healing edges of wounds l
-6 may help to
surmount this problem in future.The number of fatal or potentially fatal wounds was noted, as
were the external site/sand size thereof, the direction ofthe tracktaken by the offending weapon and the structure in which thisterminated. The anatomical distribution of the injuries wasnoted and organ involvement analysed. Associated fmdings were
386 SA MEDICALJOURNAL VOLUME 65 10 MARCH 1984
Results
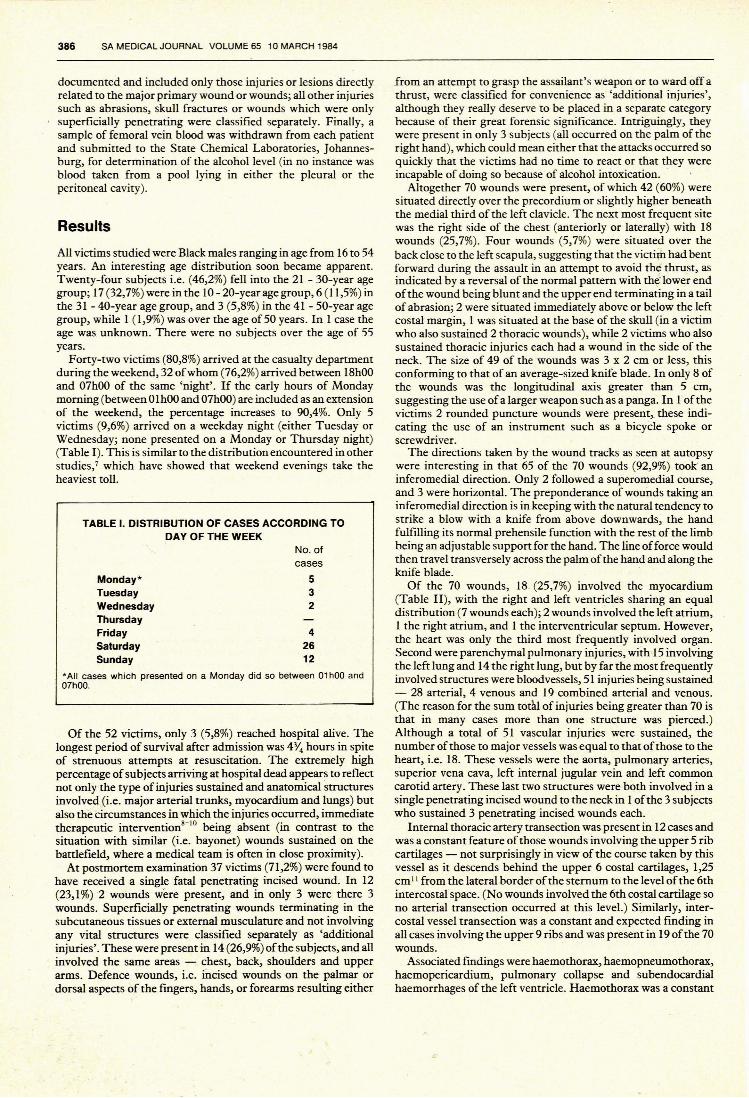
*AII cases which presented on a Monday did so between 01hOO and07hOO.
TABLE I. DISTRIBUTION OF CASES ACCORDING TODAY OF THE WEEK
documented and included only those injuries or lesions directlyrelated to the major primary wound or wounds; all other injuriessuch as abrasions, skull fractures or wounds which were onlysuperficially penetrating were classified separately. Finally, asample of femoral vein blood was withdrawn from each patientand submitted to the State Chemical Laboratories, Johannesburg, for determination of the alcohol level (in no instance wasblood taken from a pool lying in either the pleural or theperitoneal cavity).
from an attempt to grasp the assailant's weapon or to ward off athrust, were classified for convenience as 'additional injuries',although they really deserve to be placed in a separate categorybecause of their great forensic significance. Intriguingly, theywere present in only 3 subjects (all occurred on the palm of theright hand), which could mean either that the attacks occurred soquickly that the victims had no time to react or that they wereincapable of doing so because of alcohol intoxication. .
Altogether 70 wounds were present, of which 42 (60%) weresituated directly over the precordium or slightly higher beneaththe medial third of the left clavicle. The next most frequent sitewas the right side of the chest (anteriorly or laterally) with 18wounds (25,7%). Four wounds (5,7%) were situated over theback close to the left scapula, suggesting that the victim had bentforward during the assault in an attempt to avoid the thrust, asindicated by a reversal of the normal pattern with the lower endof the wound being blunt and the upper end terminating in a tailof abrasion; 2 were situated immediately above or below the leftcostal margin, 1 was situated at the base of the skull (in a victimwho also sustained 2 thoracic wounds), while 2 victims who alsosustained thoracic injuries each had a wound in the side of theneck. The size of 49 of the wounds was 3 x 2 cm or less, thisconforming to that of an average-sized knife blade. In only 8 ofthe wounds was the longitudinal axis greater than 5 cm,suggesting the use ofa larger weapon such as a panga. In 1ofthevictims 2 rounded puncture wounds were present,.. these indicaring the use of an instrument such as a bicycle spoke orscrewdriver.
The directions taken by the wound tracks as seen at autopsywere interesting in that 65 of the 70 wounds (92,9%) took' aninferomedial direction. Only 2 followed a superomedial course,and 3 were horizontal. The preponderance of wounds taking aninferomedial direction is in keeping with the natural tendency tostrike a blow with a knife from above downwards, the handfulfilling its normal prehensile function with the rest of the limbbeing an adjustable support for the hand. The line of force wouldthen travel transversely across the palm ofthe hand and along theknife blade.
Of the 70 wounds, 18. (25,7%) involved the myocardium(Table 11), with the right and left ventricles sharing an equaldistribution (7 wounds each); 2 wounds involved the left atrium,1 the right atrium, and 1 the interventricular septum. However,the heart was only the third most frequently involved organ.Second were parenchymal pulmonary injuries, with 15 involvingthe left lung and 14 the right lung, but by far the most frequentlyinvolved structures were bloodvessels, 51 injuries being sustained- 28 arterial, 4 venous and 19 combined arterial and venous.(The reason for the sum tot~lof injuries being greater than 70 isthat in many cases more than one structure was pierced.)Although a total of 51 vascular 'injuries were sustained, thenumber ofthose to major vessels was equal to that ofthose to theheart, i.e. 18. These vessels were the aorta, pulmonary arteries,superior vena cava, left internal jugular vein and left commoncarotid artery. These last two structures were both involved in asingle penetrating incised wound to the neck in 1ofthe 3 subjectswho sustained 3 penetrating incised wounds each.
Internal thoracic artery transection was present in 12 cases andwas a constant feature of those wounds involving the upper 5 ribcartilages - not surprisingly in view of the course taken by thisvessel as it descends behind the upper 6 costal cartilages, 1,25cm 11 from the lateral border of the sternum to the level ofthe 6thintercostal space. (No wounds involved the 6th costal cartilage sono arterial transection occurred at this level.) Similarly, intercostal vessel transection was a constant and expected finding inall cases involving the upper 9 ribs and was present in 19 ofthe 70woupds. '
Associated fmdings were haemothorax, haemopneumothorax,haemopericardium, pulmonary collapse and subendocardialhaemorrhages of the left ventricle. Haemothorax was a constant
42612
No. ofcases
532
Monday*TuesdayWednesdayThursdayFridaySaturdaySunday
All victims studied were Black males ranging in age from 16 to 54years. An interesting age distribution soon became apparent.Twenty-four subjects i.e. (46,2%) fell into the 21 - 30-year agegroup; 17 (32,7%) were in the 10 - 20-year age group, 6 (11,5%) inthe 31 - 40-year age group, and 3 (5,8%) in the 41 - 50-year agegroup, while 1 (1,9%) was over the age of 50 years. In 1 case theage was unknown. There were no subjects over the age of 55years.
Forty-two victims (80,8%) arrived at the casualty departmentduring the weekend, 32 ofwhom (76,2%) arrived between 18hOOand 07hoo of the same 'night'. If the early hours of Mondaymorning (between 01 hoo and 07hoo) are included as an extensionof the weekend, the percentage increases to 90,4%. Only 5victims (9,6%) arrived on a weekday night (either Tuesday orWednesday; none presented on a Monday or Thursday night)(Table I). This is similar to the distribution encountered in otherstudies,7 which have showed that weekend evenings take theheaviest toll.
Of the 52 victims, only 3 (5,8%) reached hospital alive. Thelongest period of survival after admission was 4% hours in spiteof strenuous attempts at resuscitation. The extremely highpercentage ofsubjects arriving at hospital dead appears to reflectnot only the type of injuries sustained and anatomical structuresinvolved (i.e. major arterial trunks, myocardium and lungs) butalso the circumstances in which the injuries occurred, immediatetherapeutic intervention8
-1O being absent (in contrast to the
situation with similar (i.e. bayonet) wounds sustained on thebattlefield, where a medical team is often in close proximity).
At postmortem examination 37 victims (71,2%) were found tohave received a single fatal penetrating incised wound. In 12(23,1%) 2 wounds were present, and in only 3 were there 3wounds. Superficially penetrating wounds terminating in thesubcutaneous tissues or external musculature and not involvingany vital structures were classified separately as 'additionalinjuries'. These were present in 14 (26,9%) ofthe subjects, and allinvolved the same areas - chest, back, shoulders and upperarms. Defence wounds, i.e. incised wounds on the palmar ordorsal aspects of the fmgers, hands, or forearms resulting either
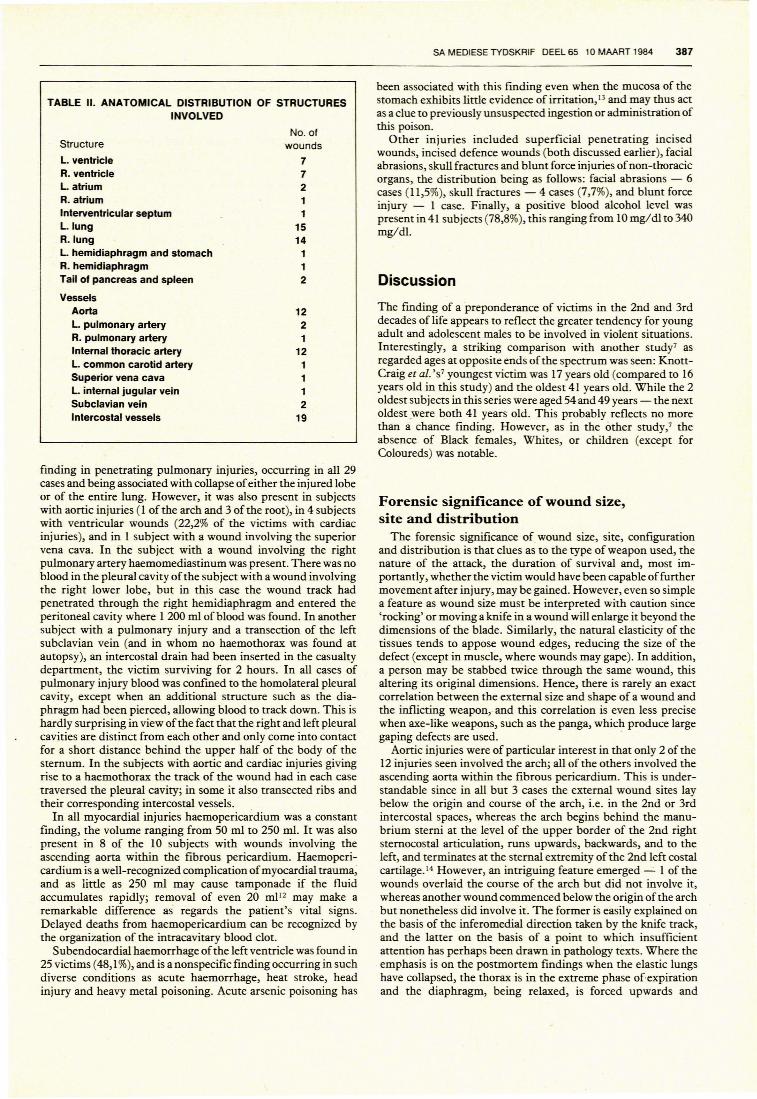
TABLE 11. ANATOMICAL DISTRIBUTION OF STRUCTURESINVOLVED
Structure
L. ventricleR. ventricleL. atriumR. atriumInterventricular septumL. lungR.lungL. hemidiaphragm and stomachR. hemidiaphragmTail of pancreas and spleen
VesselsAortaL. pulmonary arteryR. pulmonary arteryInternal thoracic arteryL. common carotid arterySuperior vena cavaL. internal jugular veinSubclavian veinIntercostal vessels
No. ofwounds
77211
1514
112
1221
121112
19
SA MEDIESE TYDSKRIF DEEL 65 10 MAART 1984 387
been associated with this finding even when the mucosa of thestomach exhibits little evidence of irritation, 13 and may thus actas a clue to previously unsuspected ingestion or administration ofthis poison.
Other injuries included superficial penetrating incisedwounds, incised defence wounds (both discussed earlier), facialabrasions, skull fractures and blunt force injuries ofnon-thoracicorgans, the distribution being as follows: facial abrasions - 6cases (11,5%), skull fractures - 4 cases (7,7%), and blunt forceinjury - 1 case. Finally, a positive blood alcohol level waspresent in 41 subjects (78,8%), this ranging from 10 mg/d! to 340mg/d!.
Discussion
The finding of a preponderance of victims in the 2nd and 3rddecades of life appears to reflect the greater tendency for youngadult and adolescent males to be involved in violent situations.Interestingly, a striking comparison with another study7 asregarded ages at opposite ends ofthe spectrum was seen: KnonCraig et al. 'S7 youngest victim was 17 years old (compared to 16years old in this study) and the oldest 41 years old. While the 2oldest subjects in this series were aged 54 and 49 years - the nextoldest .were both 41 years old. This probably reflects no morethan a chance finding. However, as in the other study/ theabsence of Black females, Whites, or children (except forColoureds) was notable.
finding in penetrating pulmonary injuries, occurring in all 29cases and being associated with collapse ofeither the injured lobeor of the entire lung. However, it was also present in subjectswith aortic injuries (l of the arch and 3 of the root), in 4 subjectswith ventricular wounds (22,2% of the victims with cardiacinjuries), and in 1 subject with a wound involving the superiorvena cava. In the subject with a wound involving the rightpulmonary artery haemomediastinum was present. There was noblood in the pleural cavity of the subject with a wound involvingthe right lower lobe, but in this case the wound track hadpenetrated through the right hemidiaphragm and entered theperitoneal cavity where 1 200 ml of blood was found. In anothersubject with a pulmonary injury and a transection of the leftsubclavian vein (and in whom no haemothorax was found atautopsy), an intercostal drain had been inserted in the casualtydepartment, the victim surviving for 2 hours. In all cases ofpulmonary injury blood was confined to the homolateral pleuralcavity, except when an additional structure such as the diaphragm had been pierced, allowing blood to track down. This ishardly surprising in view of the fact that the right and left pleuralcavities are distinct from each other and only come into contactfor a short distance behind the upper half of the body of thesternum. In the subjects with aortic and cardiac injuries givingrise to a haemothorax the track of the wound had in each casetraversed the pleural cavity; in some it also transected ribs andtheir corresponding intercostal vessels.
In all myocardial injuries haemoperic~diumwas a constantfinding, the volume ranging from 50 ml to 250 m!. It was alsopresent in 8 of the 10 subjects with wounds involving theascending aorta within the fibrous pericardium. Haemopericardium is a well-recognized complication ofmyocardial trauma,and as little as 250 ml may cause tamponade if the fluidaccumulates rapidly; removal of even 20 mil 2 may make aremarkable difference as regards the patient's vital signs.Delayed deaths from haemopericardium can be recognized bythe organization of the intracavitary blood clot.
Subendocardial haemorrhage of the left ventricle was found in25 victims (48,1%), and is a nonspecific finding occurring in suchdiverse conditions as acute haemorrhage, heat stroke, headinjury and heavy metal poisoning. Acute arsenic poisoning has
Forensic significance of wound size,site and distribution
The forensic significance of wound size, site, configurationand distribution is that clues as to the type of weapon used, thenature of the anack, the duration of survival and, most importantly, whether the victim would have been capable offurthermovement after injury, may be gained. However, even so simplea feature as wound size must be interpreted with caution since'rocking' or moving a knife in a wound will enlarge it beyond thedimensions of the blade. Similarly, the natural elasticity of thetissues tends to appose wound edges, reducing the size of thedefect (except in muscle, where wounds may gape). In addition,a person may be stabbed twice through the same wound, thisaltering its original dimensions. Hence, there is rarely an exactcorrelation between the external size and shape of a wound andthe inflicting weapon, and this correlation is even less precisewhen axe-like weapons, such as the panga, which produce largegaping defects are used. .
Aortic injuries were of particular interest in that only 2 of the12 injuries seen involved the arch; all of the others involved theascending aorta within the fibrous pericardium. This is understandable since in all but 3 cases the external wound sites laybelow the origin and course of the arch, i.e. in the 2nd or 3rdintercostal spaces, whereas the arch begins behind the manubrium sterni at the level of the upper border of the 2nd rightsternocostal articulation, runs upwards, backwards, and to theleft, and terminates at the sternal extremity of the 2nd left costalcartilage. 14 However, an intriguing feature emerged - 1 of thewounds overlaid the course of the arch but did not involve it,whereas another wound commenced below the origin of the archbut nonetheless did involve it. The former is easily explained onthe basis of the inferomedial direction taken by the knife track,and the laner on the basis of a point to which insufficientanention has perhaps been drawn in pathology texts. Where theemphasis is on the postmortem findings when the elastic lungshave collapsed, the thorax is in the extreme phase of'expirationand the diaphragm, being relaxed, is forced upwards and
or locked in a cupboard is hardly likely to have arrived there of itsown accord!).
Blood ethanol level(mg/dl)
0- 4050- 90
100-140150-290300-390400+
388 SA MEDICAL JOURNAL VOLUME 65 10 MARCH 1984
backwards by the abdominal organs. In contrast, in the living,erect subject the organs are under the influence of gravity,resulting in their downward displacement and hence accountingfor the seeming discrepancy between the external site ofa woundand the visceral involvement thereof.
The involvement ofthe precordium in nearly two-thirds oftheinjuries seen is due to the fact that this area is a site ofprediliction, a 'target' site, in any homicidal assault, and anumber of surveyslS have tended to bear this out. There is anatural tendency to strike at the heart as the target organ ofchoice. Confirming that the left thoracic area was a site ofprediliction was the finding that the external sites of the 4abdomin~ penetrating incised wounds (3 involving the tail ofthepancreas and 1 the left hemidiaphragm and stomach) all overlaythe left costal margin..
Regarding the question of survival after injury, as a generalrule arterial injuries are more rapidly fatal than venous ones ofequal calibre, and large-vessel injuries are more rapidly fatal thanones to smaller vessels ofthe same type. An occasional exceptionis when the injured structure is a transected elastic artery retraction of the severed ends of the vessels may create somedegree of haemostasis delaying fatal outcome.
In considering myocardial' injuries, remarkable cases are onrecord 16 of patients surviving several weeks after sustainingpenetrating myocardial wounds, the extent of injury only beingdiscovered at autopsy. In these instances survival is directlyrelated to the size of the defect and, in particular, that of thepericardial defect. A large traumatic laceration of the pericardium will usually result in severe haemorrhage either into themediastinum or the pleural cavity or externally through thewound. Should a small penetrating injury such as that producedby a bicycle spoke be sustained, normal haemostasis can occur,sealing off the pericardial defect by means of clot formation.Blood can then accumulate in the pericardial cavity and theultimate outcome will then depend on the rapidity of itsaccumulation. It has been suggested that clot formation withinthe myocardial wound is directly proportional to the thickness ofcardiac wall penetrated, 17 but it should be borne in mind that theunique anatomy of the heart with its intricate interlacing ofmuscle fibres also plays a role since myocardial contraction tendsto appose these fibres, limiting blood flow and initiatingcoagulation in the damaged area through release of tissuethromboplastins. Both of these factors are possibly responsiblefor the fact that ventricular wounds are less rapidly fatal thanatrial ones.
The medicolegal significance of the above concerns thequestion of movement, or rather the possibility of movement,after injury; this is sometimes raised by defence counsels to inferthat the accused could not have been aware of the severity of hisassault - a wound which is not rapidly exsanguinating andwhich may allow continued consciousness and movement on thevictim's part allows the suggestion that the intention was merelyto deter by wounding rather than to kill. However, this is a legalmatter with which the pathologist should not unduly concernhimself. He should direct his attention to those situations inwhich the question of movement after injury has a more directmedicolegal bearing, such as when a blood-stained knife is foundsome distance from a body and the question then arises whetherone is dealing with homicide or suicide. In other words, could thedeceased have stabbed himself, dropped the weapon and thenstaggered some distance to die in another spot? Or was hestabbed to death by an assailant who dropped the weapon somedistance from the body in his haste to get away? These arequestions which are sometimes exceedingly difficult to answer- corroborative evidence, such as fmgerprints on a weapon'shandle, does not always offer elucidation. One fmal point to bemade is that the possibility of movement after injury should notresult in the erroneous conclusion that death was accidental orsuicidal (a body with penetrating incised wounds found buried
Forensic significance of defence woundsThese are incised wounds on the palmar or dorsal aspects of
the fmgers, hands or forearms resulting either from an attempt tograsp the assailant's weapon or to ward off a thrust, and werepresent in 3 of the victims. Is the fmding of defence wounds avalid medicolegal observation, and do they indicate that themode of death was homicidal rather than suicidal? This pointwas raised as far back as 1894 in the British court ~se of R. v.Deakin. 18 In this case the deceased was found with a ~ut throat.However, other incised wounds were present on the palmaraspect ofthe left thumb, in the interdigital space betw~en the leftthumb and index finger, and over the dorsal aspects of bothhands. Defence counsel put forward the suggestion that deathwas suicidal and the judge, after questioning the medical wimess,stated that it passed his comprehension how wounds on thehands could have any bearing on a wound of the throat. Thedoctor quite rightly replied that a single cut could not be judgedin isolation.
Forensic significance of other injurie~
These comprised either superficial penetrating incised woundsor various blunt force injuries. Superficial penetrating incisedwounds were seen in only slightly more than one-quarter ofthevictims, two-thirds of the victims having received a single fatalwound. This would appear to indicate a singular degree ofintent,with the assailant bent on inflicting a single fatal thrust ratherthan a number of tentative, non-life-threatening wounds.
Blunt force injuries to abdominal viscera were present in only1 subject, involving haemorrhage into the body of the pancreasand root ofthe mesentery beneath the 4th part ofthe duodenum.This would seem to indicate that in those instances where theassailant chooses to use a knife as his weapon little attention isdirected to inflicting blunt force injuries as well. The paucity offacial abrasions (11,5%) and skull fractures (7,7%) is also inkeeping with this.
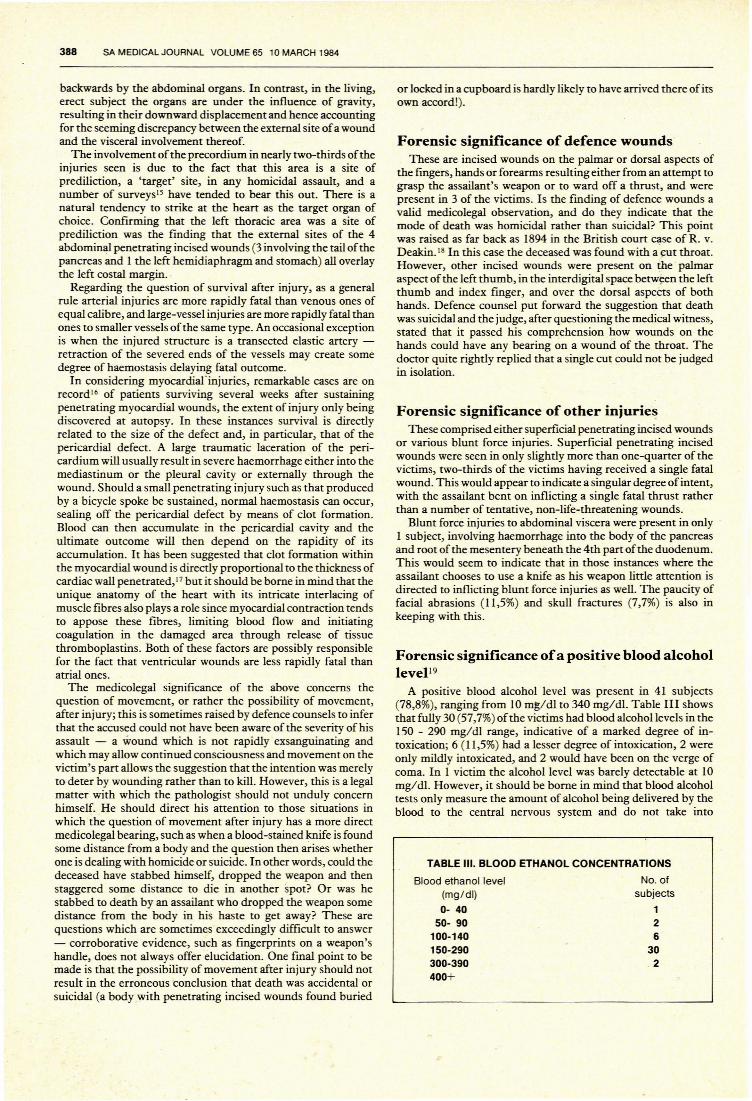
Forensic significance ofa positive blood alcohollevel19
A positive blood alcohol level was present in 41 subjects(78,8%), ranging from 10 mg/dl to 340 mg/dl. Table III showsthat fully 30 (57,7%) ofthe victims had blood alcohol levels in the150 - 290 mg/dl range, indicative of a marked degree of intoxication; 6 (11,5%) had a lesser degree of intoxication, 2 wereonly mildly intoxicated, and 2 would have been on the verge ofcoma. In 1 victim the alcohol level was barely detectable at 10mg/dl. However, it should be borne in mind that blood alcoholtests only measure the amount of alcohol being delivered by theblood to the central nervous system and do not take into
TABLE Ill. BLOOD ETHANOL CONCENTRATIONS
No. ofsubjects
126
30.2
consideration tissue tolerance. Blood alcohol tests cannot, therefore, provide a precise guide to the degree of intoxication whichwas present, and any opinion given in coun should be guarded.This point has been well stressed by Cooper et al. 20
Anumber ofquestions are sometimes raised in court regardingpostmortem blood alcohol levels. The first involves the actualmethod of collection and is usually the initial line of attackadopted by a cross-exarnining anomey. It cannot be stressedenough that all postmortem samples for chemical analysesshould be collected, stored and transported in appropriatecontainers, which means that all glassware, syringes, and needlesused in collecting specimens must be chemically clean andshould not have come into contact with volatile organic fluids.The simple precaution of leaving as little space as possiblebetween the 'sample and the top of the container should also befollowed to prevent any alcohol evaporation. Regarding thecollection site, although there is no significant difference in thealcohol levels of blood samples from the intact heart chambersand the femoral vessels,21-2 autopsy samples from pooled bloodin the peritoneal or pleural cavities are unsatisfactory. Bloodwhich has pooled in body cavities during anatomic dissection isliable to become contaminated, either by diffusion of alcoholfrom the stomach after death or directly by gastric contentswhich have leaked into these sites from perforations or ruptures.Blood should therefore be taken from the femoral or subclavianveins.
Other questions are whether ethanol and other alcohols can beproduced in the body after death or in vitro as a result ofimproper storage of blood obtained at autopsy, and whether anormal endogenous blood alcohol level exists during life.Although the answer to the laner is still controversial,24 bloodalcohol levels are generally believed to be negligible in theabsence of ingested alcohol. So-called endogenous alcohol inhuman blood exists at a concentration ofless than 0,15 mg!dl butputrefactive changes before autopsy or during blood storage mayresult in alcohol production by fermentation of proteins andcarbohydrates by enzymes, bacteria or fungi. 21-24 The problem iscompounded by the fact that refrigeration of a cadaver will notprevent bacterial production of ethanol.25,26 Cases have beendescribed where bodies have been refrigerated after motorvehicle accidents, no obvious putrefaction being present andblood being placed in test tubes containing fluoride. 27 Nevertheless, the blood samples contained enteric Gram-negative rodssuch as Enterobacter agglomerans, Citrobacter freundii and Klebsiella oxytoca, and both the Klebsiella and the Citrobaeter provedcapable of fermenting glucose to ethanol in refrigerated humanplasma at 4°C. Therefore, when blood alcohol concentration islikely to play a part in legal proceedings, the sample should betaken as soon as possible after death. If this is not possible,vitreous humour, which is not readily contaminated withbacteria and fungi/HO should also be taken at autopsy.
Within certain limitations, postmortem alcohol specimens canbe used to estimate blood alcohol levels at various times beforedeath, basing such calculations on the assumption that the bloodalcohollevel decreases from its peak at a fairly constant rate of 15mg/dl (0,015%) during each hour until death.3l However, itshould be borne in mind that certain conditions lower toleranceto alcohol, contributing to death at levels which are not usuallyfatal. Such conditions include chronic obstructive airwaysdisease, arteriosclerotic cardiovascular disease, drugs such as
SA MEDIESE TYDSKRIF DEEL 65 10 MAART 1984 389
barbiturates,32 narcotics and antihistamines, and poisoning withcarbon tetracWoride or carbon monoxide.
Sincere thanks are due to Professor N. J. Schepers for the manyvaluable suggestions and criticisms he made during the course ofpreparation of the manuscript.
REFERENCES
I. Bhawan J. The myofibroblast. Am] Dermacopalhol1981; 3: 73-78.2. Gabbiani G, Ryan GB, Majno G. Presence of modified fibroblasts in
granulation tissue and their possible role in wound contraction. Experienlia1971; 27: 549-550.
3. Gabbiani G, Hirschel BJ, Ryan GB. Granulation tissue as a contractile organ- a srudy of structure and function.] Exp Med 1972; 135: 719-734.
4. Gabbiani G, Le Lous M, Bailey AJ. Collagen and myofibroblasts ofgranulation tissue - a chemical, ultrastrucrural, and immunological srudy.Virciwws Arch (Cell. Palhol) 1976; 21: 133-145.
5. Seemayer TA, Schiirch W, Lagace R. The myofibroblast: biologic, pathologic,and theoretical considerations. Palhol Annu 1980; 15: 443-470.
6. Lipper S, Kahn LB, Reddick RL. The myofibroblast. Palhol Annu 1980; 15:409.
7. Knon-Craig CJ, Przybojewski JZ, Bamard PM. Penetrating wounds of thehean and great vessels - a new therapeutic approach. S Afr Med] 1982; 62:316-320.
8. Sugg WL, Rea WJ, Ecker RR el al. Penetrating wounds ofthe hean: an analysisof 459 cases.] Thorac Cardiovasc Surg 1968; 56: 531-545.
9. Szentpetery S, Lower RR. Changing concepts in the treatment of penetratingcardiac wounds.] Trauma 1977; 17: 457-461.
10. Lemos PCP, Okumura M, Azevedo AC el al. Cardiac wounds: experiencebasefl on a series of 121 operated cases.] Cardiovasc Surg 1976; 17: 1-8.
11. Johnston TB, Davies DV, Davies F, eds. The internal thoracic anery. In:Gray's Analamy. 32nd ed. London: Longmans, Green, 1958: 770.
12. Shires TG. Trauma. In: Schwartz SI, ed. Principles of Surgery. 3rd ed. NewYork: Mcgraw-Hill, 1979: 221.
13. Smith, Sir S.: Forensic Medicine. 7th ed. London, J & A Churchill, 1940: 479.14. Johnston TB, Davies DV, Davies F, eds. The arch of the aorta. In: Gray's
Analomy. 32nd ed. London: Longmans, Green, 1958: 731.15. Adelson L. A survey of 250 consecutive fatal criminal 'cunings'. In: Gerber
SA,ed. TheParhologyofHomicide. Isted. Springfield, Ill.: Charles CThomas,1974: 339-340.
16. Taylor AS. Wounds of the hean. In: Simpson K, ed. Principles of MedicalJurisprudence, vol. I. 12th ed. London: J & A Churchill, 1965: 248.
17. Asfaw I, Arbulu A. Penetrating wounds ofthe pericasdium and heart. Surg ClinNorlh Am 1977; 57: 37-48.
18. Taylor AS. Medicolegal narure of wounds. In: Simpson K, ed. Principles ofMedical]urisprudence, vol. I. 12th ed. London: J & A Churchill, 1965: 215.
19. Freimuth He. Forensic aspects of alcohol. In: Spitz WU, Fisher RS, eds.Medicolegallnvestigalion ofDealh. 1st ed. Springfield, Ill.: Charles C Thomas,1973: 483.
20. Cooper WE, Schwiir TG, Smith LS. Alcohol, Drugs and Road Traffic. CapeTown: Jura, 1979.
21. Plueckhahn VD. AIcohollevels in autopsy he2rt blood.]Forensic Med 1968; 15:12-21.
22. Plueckhahn VD. The significance ofblood alcohollevels at autopsy. Med] A USI1967; 2: 118-124.
23. Plueckhahn VD. The significance of alcohol and sugar determinations inautopsy blood. Med] AusI 1970; 1: 46-51.
24. Harger RN. Ethyl alcohol. In: Stewan CP, Stolman A, eds. Toricology Mechanisms andA nalYlical Melhods, vol. 11, New York: Academic Press, 1961:85-151.
25. Blume P, Lakarua DJ. The effect of mictobial contamination of the bloodsample on the determination ofethanol levels in serum. Am]Clin Palho11973;60: 700-702.
26. Christopoulos G, Kirch ER, Gearien JE. Determination ofethanol in fresh andputrefied postmortem tissues.] ChromalOgr 1973; 87: 455-472.
27. Vuori E, Renkonen O-V, Lindbohm R. Validiry of postmortem blood alcoholvalues. Lancer 1983; ii: 761-762.
28. Blackmore DJ. The bacterial production of ethyl alcohol.] Forensic Sci Sac1968; 8: 73-78.
29. Correy JEL. Methods ofassessing the effect ofmicrobes in blood and urine onethanol levels. In: Proceedings of lhe 81h Internalional Conference on Alcohol,Drugs and Traffic SafelY, Stockholm, 15-19 June 1980: 600-613.
30. Zumwalt RE, Bost RO, Sunshine I. Evaluation of ethanol concentrations indecomposed bocties.] Forensic Sci 1982; 27: 549-554.
31. Rentoul E, Smith H. Glaisler's Medical]urisprudence and Toricology. 13th ed.Edinburgh: E & S Livingstone, 1973: 593-611.
32. Jener WW, McLean R. Poisoning by the synergistic effect of phenobarbitaland ethyl alcohol: an experimental srudy. Arch Palhol Lab Med 1943; 36:112-122. .