Embed Size (px)
Citation preview
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 1/25
Official reprint from UpToDate www.uptodate.com ©2016 UpToDate
AuthorMichael J Corwin, MD
Section EditorsGeorge B Mallory, MDTeresa K Duryea, MD
Deputy EditorAlison G Hoppin, MD
Sudden infant death syndrome: Risk factors and risk reduction strategies
All topics are updated as new evidence becomes available and our peer review process is complete.Literature review current through: Feb 2016. | This topic last updated: Feb 16, 2016.
INTRODUCTION — Sudden infant death syndrome (SIDS), also called crib or cot death, is the leading cause ofinfant mortality between one month and one year of age in the United States. Since the 1990s, however, newstudies in pathology and epidemiology have provided the basis for an important evolution in the understanding ofSIDS.
The risk factors for and measures to reduce the risk of SIDS are discussed in this topic review. Clinicalmanagement for the family of an infant who has succumbed to SIDS and alternate diagnostic considerations arediscussed separately. (See "Sudden unexpected infant death including SIDS: Initial management".)
DEFINITION — SIDS is defined as the sudden death of an infant younger than one year of age, which remainsunexplained after a thorough case investigation, including performance of a complete autopsy, examination of thedeath scene, and review of the clinical history [1,2].
This definition emphasizes the necessity of autopsy, death scene investigation, and review of the clinical historywhen making the diagnosis of SIDS, to exclude other explanations for the sudden unexpected infant death thatcan mimic SIDS (table 1). The evaluation of an infant who has died of suspected SIDS and alternate diagnosticconsiderations are discussed separately. (See "Sudden unexpected infant death including SIDS: Initialmanagement".)
Due in part to potential inconsistencies in the diagnosis of SIDS, the term "sudden unexpected infant death"(SUID) is often used to describe all unexpected infant deaths. The SUID designation can then be subdivided intoexplained SUID and unexplained SUID. Unexplained SUID generally includes those cases considered SIDS bythe medical examiner, as well as some cases that are not considered SIDS but lack a clear explanation due touncertain circumstances. Some reports in the literature use the term "unexplained SUID" instead of "SIDS" toavoid inconsistencies between medical examiners in reporting SIDS as a cause of death.
SIDS has similar risk factors to other sleeprelated infant deaths, including those attributed to suffocation,asphyxia, and entrapment. Therefore, these are now addressed together in recommendations for a safe infantsleeping environment [3]. This topic review will use the term "SIDS," but much of the discussion about risk factorsand preventative measures applies to other sleeprelated infant deaths.
EPIDEMIOLOGY — SIDS is the leading cause of infant mortality between one month and one year of age in theUnited States [4]. The risk of SIDS in the United States is <1 per 1000 live births [57]. Higher rates (two to threetimes the national average) are found in black and American Indian/Alaskan native children [8,9]. Adisproportionately high rate (15 to 20 percent) of SIDS cases occurs in child care settings [3,10,11]. The risk ofSIDS is slightly increased in boys (multivariate OR 1.49 [95% CI 1.141.83] in one large European casecontrolstudy) [12].
The incidence of SIDS has declined dramatically in countries that have adopted policies encouraging nonpronesleeping ("Back to Sleep" campaigns). The initial campaigns were in Europe, Australia, and New Zealand [13]. Inthe United States, the incidence of SIDS has declined by more than 50 percent since the mid1980s, and thegreatest reduction occurred after 1992, when the American Academy of Pediatrics (AAP) issued arecommendation to reduce the risk of SIDS by placing infants in a supine position for sleep [3,1315]. Between
®®
Home Logout
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 2/25
1992 and 2001, the SIDS rate in the United States fell from 1.2 to 0.56 per 1000 live births, while the proportion ofinfants sleeping in the supine position increased from 13 to 72 percent [16,17]. The rate of SIDS then remainedconstant between 2001 and 2006 [9]. Similar declines have occurred in other countries after campaigns toencourage nonprone sleeping [18,19].
Data from the National Institute of Child Health and Human Development (NICHD) Collaborative SIDS Studyhave helped to define the epidemiologic features of SIDS (table 2) [20]. This landmark study was a multicenter,populationbased, casecontrolled project that included 10 percent of the live births in the United States; the studywas published in 1988, prior to the widespread use of supine sleep positioning. The pathologic diagnoses wereconfirmed by an independent panel of forensic pathologists.
In the NICHD study, the median age for SIDS deaths was 11 weeks, the peak incidence was between 2 and 4months, and 90 percent occurred before 6 months of age [20]. Approximately 2 percent of cases occur after ninemonths of age [21]. A few sudden unexpected deaths resembling SIDS have been described within the first 24hours of life [2224]. This unique distribution strongly suggests that critical stages of development or maturationaffect the risk of SIDS. The most important conclusion from this study was that no strong predictive and/ordiagnostic characteristics of mothers or infants can be identified in most SIDS victims that would permit clinicallyuseful screening for highrisk infants.
RISK FACTORS — Numerous risk factors for SIDS have been identified in observational and case controlstudies. Those that are consistently identified as independent risk factors include [3]:
More than 95 percent of SIDS cases are associated with one or more risk factors, and in many cases, the riskfactors are modifiable (usually sleeping position, sleep environment, or parental smoking) [25]. Risk factors forSIDS are discussed below. Those that can be modified to decrease the risk of SIDS are also discussed in thesection on prevention. (See 'Prevention' below.)
Maternal risk factors — There are two major maternal risk factors for SIDS that are independent of birth weight[12,20]:
These factors increased the risk of SIDS two to fourfold in the National Institute of Child Health and HumanDevelopment (NICHD) Collaborative SIDS Study [20].
Maternal smoking is an important modifiable risk factor for SIDS, and SIDS rates increase with the amountsmoked [26,27]. The strongest effect is from smoking during pregnancy, but exposure of an infant to secondhandsmoke is an additional independent risk factor [28,29]. Smoking prevention/intervention programs have thepotential to substantially lower SIDS rates [26,30]. Several studies have shown abnormal cardiovascularresponses to stimuli (eg, headup tilt, hypoxemia, or CO2 exposure) and impaired arousal to stimuli in infants born
Maternal factors:
Young maternal age•Maternal smoking during pregnancy•Late or no prenatal care•
Infant and environmental factors:
Preterm birth and/or low birth weight•Prone sleeping position•Sleeping on a soft surface and/or with bedding accessories such as loose blankets and pillows•Bedsharing (eg, sleeping in parents' bed)•Overheating•
Maternal smokingAge of the mother under 20 years
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 3/25
to mothers who smoked during pregnancy, suggesting a possible mechanism for this association [3136]. (See"Secondhand smoke exposure: Effects in children", section on 'Sudden infant death syndrome'.)
Maternal drug abuse and all its associated phenomena are also associated with an excessive number of SIDSdeaths [37,38]. In one report, a fivefold increase in SIDS risk was reported for infants of substanceabusingmothers in the Los Angeles area [39]. It is not known if this association is related primarily to the biologic effect ofdrugs in utero, an increased risk of prematurity and low birth weight, and/or other postnatal conditions(socioeconomic, environmental, or parenting behavior). One study found an association between a report of infantmaltreatment and subsequent sudden unexpected infant death (SUID), after adjustment for several known SIDSrisk factors (hazard ratio 3.22, 95% CI 2.663.89) [40]. It is possible that the observed association is attributable tocommon risk factors that were not captured in the analysis, including maternal smoking or substance use, or infantsleep position. Alternatively, some of the association may be attributable to unrecognized child maltreatment(intentional or neglect).
Maternal alcohol use is an important risk factor for SIDS in some populations [41]. In a populationbased casecontrol study among Northern Plains American Indians, SIDS was significantly associated with periconceptionalmaternal alcohol use (adjusted odds ratio 6.2, 95% CI 1.623.3) and first trimester binge drinking (adjusted OR 8.2,95% CI 1.935.3) [42].
Pregnancy complications associated with an increased risk of SIDS include placenta previa, abruptio placenta,premature rupture of membranes, and elevated maternal alphafetoprotein [7,4345]. The increased risk associatedwith these complications appears to be independent of their relationship with preterm birth.
Infant risk factors
Prematurity — Preterm infants are at a higher risk for SIDS than term infants [4649]. Among low and very lowbirth weight infants, the SIDS rate has consistently been three to fourfold higher than in term infants [49]. Thegestational age of peak vulnerability for SIDS appears to occur four to six weeks earlier among preterm than terminfants [46]. It is unclear whether the population of low birth weight infants is experiencing a decline in the rate ofSIDS similar to that in the general population. A decline in SIDS rates among preterm infants was noted in NewZealand [48] but not in Sweden [50]. Preterm infants are subject to the same risk factors for SIDS as term infants,as discussed in greater detail below [48,51,52].
Supine positioning for sleep substantially reduces the risk for SIDS among premature infants. Traditionally, therewere some concerns that supine positioning of premature infants may reduce oxygenation in premature infants, asmeasured by peripheral pulse oximetry. However, two small studies have suggested that this may not be thecase, at least among infants who are older than 32 weeks postmenstrual age (ie, gestational age measured fromthe last menstrual period), and not in the acute phase of a respiratory illness [53,54]. Moreover, another study thatincluded infants as young as 26 weeks gestational age found that cerebral oxygenation was improved in thesupine compared with prone sleep position, with the maximal effect of sleep position at two to three monthschronological age [55]. A direct connection between cerebral oxygenation and arousal response or SIDS risk hasnot been established. Nonetheless, these findings lend additional support to the American Academy of Pediatrics'(AAP) recommendation that preterm infants be placed supine for sleep as soon as possible, generally by 32 weekspostmenstrual age [9,56].
The importance of supine sleep position for premature infants was demonstrated in a populationbased casecontrol study in England, in which the parents of 325 SIDS cases and 1300 agematched control infants wereinterviewed [51]. In multivariate analysis, infants who were small at birth (<37 weeks and/or <2500 g) were fivetimes more likely to die of SIDS than infants who were born at term or >2500 g. However, when infants who weresmall at birth were placed to sleep on their side or prone, they were 15 and 24 times more likely, respectively, todie of SIDS than infants who were not small at birth who were placed on their backs to sleep.
Low birthweight — Infants born small for gestational age (SGA) have an increased risk for SIDS [7,51,57].Low birthweight has a weak but significant association with SIDS risk even after adjustment for gestational age
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 4/25
and several other factors known to be associated with low birthweight, including maternal tobacco use andhypertension.
Sibling of SIDS victim — Siblings of SIDS victims have a five to sixfold increase in risk for SIDS [5861].However, assuming a SIDS rate of 0.56 per 1000 live births (0.06 percent) [16,17], the risk in subsequent siblingsfor most families remains less than 1 percent.
The small but increased risk of SIDS in siblings of SIDS victims is probably due to a combination of biologic and/orepidemiologic factors. However, it has not been possible to identify the relative importance of these factorsbecause many of the risk factors for SIDS are the same as those for other causes of infant mortality [58]. In somecases, for example, deaths from inborn errors of metabolism may have been mistaken for SIDS. In other cases,the deaths may have resulted from child abuse or were in some way related to severe deprivation and poverty[62]. (See "Sudden unexpected infant death including SIDS: Initial management", section on 'Differentialdiagnosis'.)
Twins — In cohort studies, linking data from birth and death records, the crude risk of SIDS among twins isapproximately twice that of singletons [5,6,63]. The increased risk is in part attributable to the higher proportion oftwins that are preterm and/or of low birth weight [5,6]. However, in subset analyses of some studies, the risk ofSIDS among twins born at ≥37 weeks gestation [63] or with birth weight ≥3000 g [6] remained increased comparedwith singletons as described below:
History of apnea — Apnea or otherwise impaired respiratory function likely falls within the final commonpathway of many of the proposed mechanisms for SIDS. However, a history of apnea, apparent lifethreateningevent (ALTE), or other abnormalities in breathing patterns are not clinically useful predictors of SIDS risk, andmonitoring for apnea using standard cardiorespiratory monitors does not reduce SIDS risk. (See "Use of homecardiorespiratory monitors in infants" and "Apparent lifethreatening event in infants", section on 'ALTE does notimply SIDS risk'.)
This was illustrated by the following studies:
Sleep position — The prone sleeping position is the strongest modifiable risk factor for SIDS. In casecontrolstudies, odds ratios for the risk of prone sleeping or nonsupine sleeping range between 2.3 and 13.1 [9,12,6570].Additional support for this association comes from the decreased rate of SIDS in various countries followingrecommendations to place infants on their back or side to sleep [14,16,17,7173]. Supine positioning also isbeneficial for infants born prematurely, as discussed above. (See 'Prematurity' above.)
Avoidance of side positioning is also important, perhaps because the probability of rolling from the side to theprone position is greater than that of rolling from the supine to the prone position (see 'Epidemiology' above) [7477]. As the proportion of infants placed to sleep in the prone position has decreased, the relative contribution of
37 to 38 weeks: Relative risk (RR) 1.3139 to 40 weeks: RR 1.47≥41 weeks: RR 2.09Birthweight ≥3000 g: RR 2.98
In casecontrol studies, a history of apnea or cyanosis is not specifically increased in SIDS victims [20].Approximately 5 percent of parents of SIDS victims recall cyanotic episodes during the months before death,but this not substantially different from parent recall of cyanotic episodes in control infants and may beinfluenced by recall bias.
Prospective studies have failed to identify respiratory abnormalities that correlate with known SIDS riskfactors: in a large series of infants followed longitudinally with cardiorespiratory monitors, neither"conventional" (apnea 20 to 30 seconds) nor "extreme" events (apnea >30 seconds) correlated with theprimary epidemiologic risk factors for SIDS, including time of night of the apnea and the infant's age [64].(See "Management of apnea of prematurity".)
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 5/25
sidesleeping to SIDS risk has increased [51,74,7881], as suggested by the following studies:
The increased risk among infants unaccustomed to the side or prone position highlights the importance of supinepositioning for every sleep [3].
Sleep environment — Various aspects of the sleep environment, including the sleep surface, sleepwear, bedding,room temperature, and whether or not the bed or room is shared with parents also appear to affect the risk ofSIDS, as illustrated below.
In a populationbased casecontrol study, the risk of SIDS was increased for infants placed on the side andfound in the prone position (adjusted odds ratio 8.7) [79]. In the same study, the risk of SIDS was alsoincreased among infants who were usually placed supine but were placed on their sides or prone for the lastsleep (OR 6.9 and 8.2, respectively).
Other casecontrol studies have demonstrated an increased risk of SIDS when infants unaccustomed to theprone position are placed in the prone position [82,83].
A populationbased study noted decreases in SIDS mortality associated with nonprone sleep positioning anddocumented further decreases associated with specifically supine positioning of infants for sleep [84].
Use of infant "sleep positioners" to position infants on their side has also been associated with several casesof infant deaths, as reported in a safety alert by the United States Food and Drug Administration (FDA) [85].Between 1997 and 2011, the deaths of 13 infants in the United States were linked to use of infant sleeppositioners [86]. Most of the infants had been placed on their side in the positioner to sleep, and were foundprone or with the positioner against their face.
Soft sleeping surface – Use of a soft sleeping surface is a consistent risk factor for SIDS in several casecontrol studies, especially in association with prone positioning [87]. In one study, soft bedding increased therisk of SIDS fivefold, and the combination of prone positioning and soft bedding increased the risk 21fold(95% CI 7.856.2) [88]. Other forms of soft bedding (eg, sofa or recliner chair, polystyrene beads, natural fibermattresses) also have been associated with an increased risk of SIDS [8991]. Sheepskin bedding has beenassociated with an increased risk for SIDS when infants are placed in the prone position [92,93]. Sleepsurfaces marketed commercially with claims that they reduce SIDS risk have not been adequately tested foreither safety or benefit [3].
Loose bedding – Loose bedding accessories such as blankets, quilts, and pillows also increase the risk ofSIDS by as much as fivefold, independent of sleeping position [94,95]. The association appears to bemediated by the loose bedding covering the head or otherwise obstructing airflow [96,97].
Crib bumper pads – In particular, crib bumper pads have been associated with infant deaths by"suffocation," including at least 48 infant deaths in the United States over a sevenyear period from 2006 to2012 [98,99]. This rate appears to be increasing, despite recommendations against the use of bumper padsby the AAP, Canadian Pediatric Society, and others [3,100].
Bedsharing – A variety of studies report an association between SIDS risk and infants sharing a bed withtheir parents [77,101106]. In a metaanalysis, the combined odds ratio (OR) for bedsharing versus non bedsharing infants was 2.89 (95% CI 1.994.18) [103]. The risk of bed sharing was greatest for infants youngerthan three months of age (OR, 10.37; 95% CI 4.4424.21) or for infants of mothers who smoke (OR, 6.27;95% CI 3.949.99). Similar findings were reported in a large metaanalysis that included 1472 cases of SIDSand 4679 controls from the United Kingdom, Europe, and Australasia [107]. Although overall SIDS rates werelow, bedsharing significantly increased SIDS risk in young infants even with no other SIDS risk factors. Forinfants <3 months of age, the adjusted odds ratio for bedsharing was 5.1 (95% CI 2.311.4). The riskattributable to bedsharing was increased up to 15fold in infants with additional SIDS risk factors, includingbottlefeeding, and parental smoking and drinking. In addition, there is a consistent association betweenincreased risk of SIDS and sharing a couch or sofa with parents during sleep [18,88,101,102,108]. Other
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 6/25
Protective factors — The following factors are somewhat protective against SIDS. However, these effects aregenerally weak and are outweighed by the modifiable risk factors described above.
factors that increase the risk of bedsharing include soft sleeping surfaces, additional bedding such aspillows and blankets, the presence of multiple bedsharers, and consumption of alcohol by the bedsharingadult [9].
The issue of bedsharing has been controversial. This is in part because the risk of bedsharing may berelatively low if none of the additional risk factors outlined above are present, and because of potentialbeneficial effects of bedsharing on breastfeeding or parental sleep [109112]. In addition, bedsharing is acommon practice in many cultures: in one study from the United States, 13.5 percent of families with younginfants reported bedsharing as a usual practice in 2010, up from 6.5 percent in 1993 [113]. Nonetheless, weagree with the AAP recommendation against bedsharing, although roomsharing is encouraged [3]. This isbecause bedsharing usually means that the infant sleeps on a surface that is designed for adults, andbecause some of the other factors that contribute to the risk of bedsharing cannot be predicted or controlled.Moreover, breastfeeding and parental sleep can still be supported by roomsharing. For convenience, theinfant's bed or bassinet can be placed in close proximity to the parents' bed. There is no evidence to suggestthat the risk of bedsharing can be reduced by the use of "cosleeper" devices that are placed within theparents' bed.
Guidelines in the United States and Australia suggest that twins and higherorder multiples also not sleep inthe same crib, although this is a common practice [9,114,115]. This suggestion is based on a lack ofevidence for either the safety or benefits of bedsharing by twins, and because these infants are likely tohave other risk factors for SIDS, such as low birthweight and/or prematurity.
Car seats and other sitting devices – Use of a car seat or other sitting device (stroller, swing, or infantcarrier) for sleep has been associated with some sleeprelated infant deaths [9]. This is because the sittingposition tends to potentiate gastroesophageal reflux and may reduce oxygenation in young infants [116,117].In addition, some cases have been reported in which an infant suffered suffocation after a car seataccidentally overturned when placed on a soft bed or couch [118]. Other deaths have been associated withthe use of sling carriers (adultworn soft infant carriers) for young infants [119,120]. Use of a car seat for cartravel has safety benefits that clearly outweigh the small risk of SIDS associated with sleep in thesedevices. Therefore, the AAP recommends against routine use of car seats for sleep outside of a car butcontinues to strongly recommend their use for car travel [121].
Overheating – The risk of SIDS increases with the amount of clothing or blankets on an infant and withroom temperature, but it is not clear whether these risks are mediated by headcovering and rebreathing or byoverheating [9]. In a populationbased casecontrol study among Northern Plains American Indians, SIDSwas significantly associated with two or more layers of clothing on the infant (adjusted OR 6.2, 95% CI 1.426.5) [42]. Another study noted an increased risk with swaddling or in heated rooms [90].
Swaddling – Whether swaddling of infants increases or decreases the risk for SIDS is unclear, and maydepend on sleeping position. Swaddling increases the risk for SIDS associated with prone sleeping position[90]. By contrast, limited evidence suggests that swaddling in the supine position does not increase SIDSrisk and might actually be protective [94]. This may be because swaddling keeps the infant in the unsafe orsafe sleeping position, respectively. Swaddled infants are less likely to be aroused by external stimuli, butthis effect is not seen in infants who are routinely swaddled, and it is unclear if this is clinically relevant ininfants who are in the supine position [122,123].
Roomsharing – Roomsharing, without bedsharing, between parents and infants appears to reduce the riskof SIDS [12,88,101,102,108]. In a casecontrol study from New Zealand in which 393 infants who died fromSIDS were compared with 1592 controls, the relative risk associated with sleeping in the prone position wasreduced by approximately 80 percent if the infant slept in the same room as an adult [124]. A similarreduction in the risk of SIDS was not seen if the infant shared a room with another child. Having the infant
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 7/25
PATHOGENESIS — A triplerisk model for SIDS has been proposed, suggesting that SIDS occurs in infants withunderlying vulnerability (eg, genetic pattern, brainstem abnormality) who experience a trigger event (eg, airflowobstruction, maternal smoking or infection), at a vulnerable developmental stage of the central nervous or immunesystem [77,149151].
Underlying vulnerability
Brain abnormalities — Emerging evidence suggests a brainstem abnormality or maturational delay related toneuroregulation or cardiorespiratory control is a critical contributor to the pathogenesis of SIDS. This hypothesis issuggested by the following findings:
Abnormalities in serotonin (5HT) signaling in the brain have been implicated as a mechanism. Several studies ofinfants who succumbed to SIDS have demonstrated subtle alterations or "delayed maturation" in the arcuatenucleus and other regions of the brain that participate in ventilatory and blood pressure responses to hypoxia andhypercarbia [156159]. Furthermore, specific abnormalities of serotonin signaling have been shown, includingdecreased 5HT(1A) receptor binding in the medullary areas [160162]. Male infants had particularly low binding,consistent with the clinical observation of a male predominance in SIDS cases [161]. Affected infants appear tohave a deficiency in serotonin and its key biosynthetic enzyme, tryptophan hydroxylase, in the medulla [162].Because serotonin signaling in the medulla is known to influence a broad range of autonomic processes, thesefindings are consistent with the hypothesis that SIDS is related to serotoninmediated dysregulation of theautonomic nervous system. Furthermore, serotonin signaling is altered by exposure to nicotine [160,163], providinga potential explanation for the association between maternal smoking and SIDS risk.
sleep in close proximity to the mother (but on separate surfaces) also supports breastfeeding.
Pacifier use – Use of a pacifier ("dummy," "soother") during sleep appears to reduce the risk of SIDS. Thiswas shown in a metaanalysis of seven studies, in which the multivariate summary odds ratio was 0.71[95% CI 0.590.85] for usual pacifier use and 0.39 [95% CI 0.310.50] for pacifier use during last sleep [125].The mechanism for this association is unclear; studies conflict as to whether there is a lowered arousalthreshold during pacifier use [126129] (see 'Pathogenesis' below). Because of this apparent reduction in risk,the AAP suggests offering a pacifier during sleep, provided that it does not interfere with establishment ofbreast feeding [3].
Breastfeeding – The association between breastfeeding and risk of SIDS is inconsistent [80,88,130134],and analysis in some studies is complicated by confounding factors (eg, maternal age, smoking) [135139].However, a metaanalysis that controlled for potentially protective factors, such as smoke exposure andsociodemographic factors, concluded that breastfeeding has an independent protective effect against SIDS(multivariable summary odds ratio for any breastfeeding was 0.55 [95% CI 0.440.69]) [140].
Fan use – In a populationbased casecontrol study performed in California, use of a fan was associated witha 72 percent reduction in SIDS risk (adjusted odds ratio 0.28, 95% CI 0.100.77) [141]. The effect wasgreater for infants with other environmental SIDS risk factors, including prone or side sleeping, bed sharing,and warmer room temperature. The study was limited by low participation rates and recall bias, and needsconfirmation by prospective studies.
Immunizations – SIDS is not associated with diphtheriatetanuspertussis (DTP) vaccine or other vaccines[142144]. In fact, immunization may lower the risk of SIDS [145148].
Maternal and antenatal risk factors indicating a less than optimal intrauterine environment have beendescribed for infants who later died of SIDS [20,152,153]. These observations suggest that the presumedbrain disorder may originate before birth. (See 'Maternal risk factors' above.)
Subtle abnormalities in the regulation of cardiac, respiratory, and sleep arousal patterns have been observedin infants who subsequently succumbed to SIDS [154,155].

15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 8/25
In one of the studies cited above [162], 95 percent of the infants dying of SIDS had one or more additional riskfactors for SIDS (eg, prone position, intercurrent illness before death, male sex, or prematurity), and 88 percenthad two or more risk factors. These observations underscore the notion that SIDS results from the simultaneousoccurrence of multiple events.
Genetic factors — The role that genetic factors play in susceptibility to SIDS is not clear. On the one hand,the overall low rate of SIDS in siblings, the lack of concordance in twins, and the finding that likesex twins are atno greater risk than unlikesex twins [5,6] suggest that SIDS is not a genetic disorder. On the other hand, theidentification of gene polymorphisms in SIDS victims suggests that specific genetic polymorphisms may interactwith specific environmental risk factors to increase the susceptibility to SIDS in critical situations [164,165].Specific genetic polymorphisms in the following genes have been proposed to play a role in SIDS [164,165]:
Environmental triggers — Little is known about the mechanism of death in SIDS. One report described heart rateand respiratory effort wave form data recorded by memory monitors in three children who died while beingmonitored and whose autopsies reported SIDS as the cause of death [189]. Bradycardia, not apnea, was thepredominant feature in these infants' deaths. One major caveat to interpreting this report is that the home monitorscould not have detected obstructive apnea and did not record oxyhemoglobin saturation data.
Genes encoding cardiac ion channels [166171] or proteins involved in myocardial conduction [172]Serotonin transporter gene [173177], or monoamine oxidase A (MAOA) gene, which affects serotonergic andnoradrenergic transmission [178,179]
Genes involved in the development of the autonomic nervous system [180,181]Partial deletions of complement component C4 [182]Interleukin10 promoter gene [183185]Testisspecific Y like gene [186], which is expressed in the fetal brain [187]Genes encoding heat shock proteins [175,188]
Prone position – The mechanism for the increase in SIDS risk with the prone position is not known. Somestudies have suggested that the prone position predisposes to suffocation, precipitated by decreased arousal[190193], the type of bedding, and overheating [74,87,89,90,194,195].
Decreased arousal in the prone position was suggested by a study of Belgian infants, in which prone sleepposition was associated with longer duration of sleep, longer obstructive events, decreased behavioralarousal, longer interval between obstruction and arousal, and overall decreased reaction (arousal or sigh) toobstructive events [190]. In another study, arousal thresholds during both active and quiet sleep, were higherin infants younger than five to six months of age [191]. Measures of cerebral oxygenation are lower in theprone compared with supine position, particularly in preterm infants [55], but an association between cerebraloxygenation and arousal threshold has not been established.
Accidental suffocation in the prone position was suggested by a study of 25 infant deaths that occurredduring sleep in the prone position on cushions filled with polystyrene beads, accidental suffocation byrebreathing was found to be the most likely cause of death in most of the infants [89]. The cushion wasthought to allow limited movement of the infant's head to obtain fresh air, and the estimated amount ofsubsequent rebreathing was lethal in a rabbit model. Similarly, in a study of 393 cases of SIDS in NewZealand, infants who were found in the prone position with their face down were more likely to be younger,have a low birthweight, and to have used sheepskin bedding or pillows as compared with infants with SIDSfound in other positions (prone with face to side, supine, or side) [196]. This finding suggests that infantsdying of SIDS in the face down prone position represent a distinct subgroup, and that the mechanism ofSIDS may differ depending on specific circumstances related to the infant's sleeping position.
Cardiac dysfunction – Some studies have suggested the control of cardiac function may be abnormal ininfants at risk for SIDS, but results have been inconsistent. One large, prospective study found mildlyincreased heart rates in infants who subsequently died of SIDS [197]. Others have described prolonged QT
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskredu… 9/25
Developmental timing — SIDS usually occurs between the second and fourth months of life, a period ofremarkable developmental changes in cardiac, ventilatory, and sleep/wake patterns in otherwise normal infants.This coincidence of timing suggests that SIDS infants are vulnerable to sudden death during a critical period ofautonomic maturation.
PREVENTION — Although a number of epidemiologic and physiologic factors are associated with an increasedrisk for SIDS, as described above, these factors cannot prospectively identify the infant at high risk for SIDS.Therefore, modifiable risk factors should be addressed for all infants, to reduce the risk of SIDS [206208].Attention to these modifiable risks should begin in the newborn nursery because sudden unexpected deaths inassociation with such risk factors have been reported as early as the first day of life [22], and appropriate rolemodeling by nursery staff has been shown to increase maternal adherence to recommendations [209]. Resourcesincluding training videos for families, child care providers, and medical professionals, are available from theNational Center for Education in Maternal and Child Health [210].
The following recommendations are made by the American Academy of Pediatrics (AAP) [3], the CanadianPaediatric Society (CPS) [207], and/or the United Kingdom Department of Health [208,211]. The recommendationsapply to infants up to one year of age. The data underlying these recommendations are primarily casecontrolstudies, which were described above. (See 'Risk factors' above.)
Prenatal measures
(see 'Maternal risk factors' above)
Sleep position and environment
intervals on electrocardiographic analysis [198] or sodium channel mutations associated with long QTsyndrome in postmortem tissues [199,200]. However, given the limitations of small sample sizes in crosssectional studies of rare conditions, the incidence and role of cardiac abnormalities in SIDS remainscontroversial. Based on a study of the prevalence of functionally significant genetic variants associated withlong QT syndrome, such abnormalities appear to be present in fewer than 10 percent of SIDS cases. (See"Clinical features of congenital long QT syndrome", section on 'Sudden infant death syndrome'.)
Infection – Infection is clearly the cause in a subgroup of explained sudden unexpected deaths in infancy,but its role in SIDS remains unclear [201]. Autopsy findings in infants dying from SIDS have somesimilarities with those of infants dying of toxemic shock, although there may be minimal inflammatory tissuereaction. This raises the possibility that some cases of SIDS may have an infectious trigger, leading to atoxic shocklike event [202,203]. Implicated organisms include enteric bacteria (enterotoxigenic S. aureusand E. coli), and mild viral infections [202204]. Variations in the innate immune system, includingpolymorphisms that result in an exaggerated proinflammatory response, have been found in a higherproportion of SIDS cases than in controls [183,185,202]. (See 'Genetic factors' above.)
Distinguishing between autopsy findings that represent perimortem contamination and those that suggestinfection as a trigger for SIDS is challenging and controversial. More than 70 percent of postmortembacteriological samples grow organisms when cultured, but this is not sufficient to attribute infection as acause or trigger for death. However, one wellconducted study found that infants dying of SIDS were morelikely to harbor organisms that are potentially pathogenic, as compared with infants dying from clearly noninfectious causes (eg, accidents or congenital heart disease) [205]. The bacterial colonization documented inthis study could also be explained as an epiphenomenon, caused by another established epidemiological riskfactor for SIDS such as prone sleeping, but not directly implicated as a cause of death.
Smoking and other substances – Mothers should avoid use of tobacco, alcohol, and illicit drugs duringpregnancy, as well as after birth.
Prenatal care – Pregnant women should receive regular prenatal care.
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 10/25
Supine sleep position – All infants, including infants with a history of prematurity, should be placed to sleepon their backs (supine) for every sleep, even if they are able to roll from their backs to the prone position[208]. Side sleeping is no longer recommended. (See 'Sleep position' above.)
The recommendation for supine sleeping also applies to infants with gastroesophageal reflux becausenormal infants effectively protect their airway after an episode of reflux. A rare exception is an infantwith impaired swallowing mechanisms due to neurologic dysfunction. The head of the mattress shouldnot be elevated because this is not effective for reducing reflux. (See "Gastroesophageal reflux ininfants", section on 'Positioning therapy'.)
•
Sitting devices, including car seats, infant carriers, strollers, and swings, should not be used for routinesleep. (See 'Sleep environment' above.)
•
Infant "sleep positioners" (wedges and other positioning devices) should not be used, as described inan FDA Safety Alert [85].
•
Infants should be placed supine for sleep throughout the first year of life. After six months of age, therisk of SIDS decreases substantially but is not eliminated (see 'Epidemiology' above). If an infant isjust learning to roll into the prone position during sleep, the parent should initially turn his or her backinto the supine position [208]. Once the infant can roll from supine to prone and from prone to supine,the infant can then be allowed to remain in the sleep position that he or she assumes [9]. It remainsimportant to avoid having soft or loose bedding in the infant's sleep environment, to prevent suffocationor entrapment if the infant rolls. For the same reason, the parent should not use bedding, pillows, ordevices to try to keep the infant in a particular sleep position.
•
Firm sleep surface – Infants should always be placed to sleep in a crib or bassinet on a firm surface that iscertified for use as infant bedding. The following sleep surfaces may be dangerous and should be AVOIDED(see 'Sleep environment' above):
Beds designed for older children and adults, including those with bedrails.•
Soft sleep surfaces, including polystyrenefilled cushions and sheepskin bedding.•
Roomsharing without bedsharing – Infants should sleep in the parents' room for the first six months, in acrib (or cradle or bassinet) but NOT in the parents' bed. They should not sleep on or share a sofa, recliner,armchair, or other type of cushioned chair. (See 'Protective factors' above.)
Avoid soft objects and bumper pads in the bed – Soft objects (eg, pillows, stuffed animals) and looseblankets should be kept out of the crib, bassinet, or cradle. Bumper pads appear to be particularly dangerousand should not be used. The infant's head should remain uncovered. If blankets are used, the infant's feetshould be placed at the bottom of the crib and the blankets tucked around the mattress to prevent the infantfrom moving into a position in which the head could be covered by the blanket (figure 1). Infant sleep clothing("sleeper" or "sleep sac") is a safe alternative to a blanket, provided that the sleep clothing is appropriatelysized and selected to avoid overheating. (See 'Sleep environment' above.)
Avoid overheating – Overheating should be avoided; the infant should be lightly clothed for sleep, and thebedroom temperature should be comfortable for a lightly clothed adult. If the infant is dressed in a sleeper, nomore than a thin blanket should be necessary. Infants should not sleep next to a radiator or heater, or indirect sunshine. (See 'Sleep environment' above.)
Pacifier use – We suggest offering a pacifier at sleep initiation because of some evidence that this isprotective against SIDS, even if the pacifier subsequently falls out of the infant's mouth. (See 'Protectivefactors' above.)
The pacifier should not be attached to a strap or cord because this can present a strangulation risk. It shouldbe used when placing the infant to sleep but not reinserted once the infant is asleep. The AAP suggests
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 11/25
Other measures
No benefit from home monitors — There is no evidence to support the role of home cardiorespiratory (CR)monitors in SIDS prevention, and the AAP recommends against prescribing home monitors for this purpose [3].
Hypotheses proposed during the 1970s suggested that infants with a history of apnea or an apparent lifethreatening event (ALTE) are at risk for SIDS even if they are otherwise asymptomatic, and that death could beprevented by CR monitoring. However, studies done over the past decade have failed to confirm the relationshipbetween SIDS and apnea. Moreover, studies of infants with a history of ALTE and others considered to be at riskfor SIDS (such as siblings of SIDS victims) were unable to show any benefit of CR monitoring in preventing SIDSdeaths. These issues are discussed in detail separately. (See "Use of home cardiorespiratory monitors in infants"and "Apparent lifethreatening event in infants", section on 'ALTE does not imply SIDS risk'.)
Counseling parents of asymptomatic infants with risk factors for SIDS who request a home monitor may bechallenging. If parents are concerned about SIDS and request a monitor, we suggest that the clinician engagethem in a focused conversation about the potential benefits and risks of using a home monitor before making thedecision. (See "Use of home cardiorespiratory monitors in infants", section on 'Asymptomatic infants with riskfactors for sudden infant death syndrome'.)
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education materials, "The Basics" and"Beyond the Basics." The Basics patient education pieces are written in plain language, at the 5 to 6 gradereading level, and they answer the four or five key questions a patient might have about a given condition. Thesearticles are best for patients who want a general overview and who prefer short, easytoread materials. Beyondthe Basics patient education pieces are longer, more sophisticated, and more detailed. These articles are writtenat the 10 to 12 grade reading level and are best for patients who want indepth information and are comfortablewith some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to print or email thesetopics to your patients. (You can also locate patient education articles on a variety of subjects by searching on"patient info" and the keyword(s) of interest.)
delaying the introduction of the pacifier until one month of age for breastfed infants to ensure thatbreastfeeding is firmly established [212]. There is some concern that pacifier use may increase the risk ofacute otitis media (AOM) [213]. However, the incidence of AOM is relatively low during the first six monthsof life when the risk of SIDS is greatest. (See "Breastfeeding: Parental education and support" and "Acuteotitis media in children: Epidemiology, microbiology, clinical manifestations, and complications", section on'Risk factors'.)
Smoking and other substances – Mothers should avoid smoking, alcohol, and illicit drug use after birth aswell as during pregnancy. Postnatal exposure of infants to tobacco smoke should be avoided; providersshould encourage the parents to quit smoking and to set a firm rule against smoking in the house or car. (See'Maternal risk factors' above and "Secondhand smoke exposure: Effects in children", section on 'Suddeninfant death syndrome' and "Control of secondhand smoke exposure", section on 'The home environment'.)
Breastfeeding – Breastfeeding is recommended for possible effects on reducing the risk of SIDS, in additionto other benefits. (See 'Protective factors' above and "Infant benefits of breastfeeding".)
"Tummy time" – Prone positioning is encouraged when the infant is awake and observed to facilitate thedevelopment of shoulder girdle strength and avoidance of occipital plagiocephaly [109]. (See "Overview ofcraniosynostosis".)
th th
th th
Basics topics (see "Patient information: Sudden infant death syndrome (SIDS) (The Basics)")
Beyond the Basics topics (see "Patient information: Sudden infant death syndrome (SIDS) (Beyond theBasics)")
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 12/25
SUMMARY AND RECOMMENDATIONS
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Centers for Disease Control and Prevention (CDC). Sudden infant death syndromeUnited States, 19831994. MMWR Morb Mortal Wkly Rep 1996; 45:859.
2. Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of anexpert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol1991; 11:677.
3. Task Force on Sudden Infant Death Syndrome. SIDS and Other SleepRelated Infant Deaths: Expansion ofRecommendations for a Safe Infant Sleeping Environment. Pediatrics 2011; 128:1030.
4. Center for Disease Control and Prevention. Sudden unexpected infant death and sudden infant deathsyndrome. Available at: http://www.cdc.gov/sids/ (Accessed on February 23, 2012).
Sudden infant death syndrome (SIDS) is defined as the sudden death of an infant less than one year of age,which remains unexplained after a thorough case investigation, including performance of a complete autopsy,examination of the death scene, and review of the clinical history. (See 'Definition' above.)
SIDS is the leading cause of infant mortality between one month and one year of age in the United States.The rate of SIDS peaks between two and four months of age, and 90 percent of cases occur before sixmonths of age. (See 'Epidemiology' above.)
The mechanism of sudden death is unknown. The most compelling hypothesis involves a brainstemabnormality or maturational delay related to neuroregulation or cardiorespiratory control, combined with atrigger event such as airflow obstruction. The mechanism most likely involves abnormalities of serotonin (5HT) signaling. (See 'Pathogenesis' above.)
A number of risk factors for SIDS have been identified (table 2). These include exposure to cigarette smoke,maternal age <20 years, prematurity, prone sleeping position, soft bedding, and overheating. Apnea ofprematurity, although a marker for prematurity, is not a risk factor for SIDS. (See 'Risk factors' above.)
To minimize the risk for SIDS, we recommend each of the following measures (see 'Sleep position andenvironment' above):
We recommend that all infants, including those with a history of prematurity who are older than 32weeks postmenstrual age, be placed to sleep on their backs (supine) for every sleep (Grade 1B). Sidesleeping is not recommended. (See 'Sleep position' above.)
•
We recommend that infants should sleep on a firm sleep surface (crib, cradle, or bassinet) withoutpillows or other soft objects, crib bumper pads, loose bedding, excessive clothing or sleep positioners(figure 1) (Grade 1B). We also recommend AGAINST bedsharing (Grade 1B), although roomsharingis encouraged. (See 'Sleep environment' above.)
•
Expectant mothers should avoid smoking during pregnancy because of effects on SIDS risk, in additionto other adverse effects of smoking. Exposure of an infant to secondhand smoke after delivery alsoprobably increases SIDS risk. (See 'Maternal risk factors' above and 'Other measures' above.)
•
Measures that may help protect against SIDS risk include breastfeeding and use of a pacifier whenplacing the infant to sleep. These effects are weak and are outweighed by the modifiable risk factorsdescribed above. (See 'Protective factors' above.)
•
The use of home monitors has not been proven to reduce the incidence of SIDS and is not recommended forthis purpose. (See 'No benefit from home monitors' above.)
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 13/25
5. Malloy MH, Freeman DH Jr. Sudden infant death syndrome among twins. Arch Pediatr Adolesc Med 1999;153:736.
6. Platt MJ, Pharoah PO. The epidemiology of sudden infant death syndrome. Arch Dis Child 2003; 88:27.7. Getahun D, Amre D, Rhoads GG, Demissie K. Maternal and obstetric risk factors for sudden infant deathsyndrome in the United States. Obstet Gynecol 2004; 103:646.
8. Mathews TJ, Menacker F, MacDorman MF, Centers for Disease Control and Prevention, National Center forHealth Statistics. Infant mortality statistics from the 2002 period: linked birth/infant death data set. Natl VitalStat Rep 2004; 53:1.
9. Task Force on Sudden Infant Death Syndrome, Moon RY. SIDS and other sleeprelated infant deaths:expansion of recommendations for a safe infant sleeping environment. Pediatrics 2011; 128:e1341.
10. Moon RY, Sprague BM, Patel KM. Stable prevalence but changing risk factors for sudden infant deathsyndrome in child care settings in 2001. Pediatrics 2005; 116:972.
11. KiechlKohlendorfer U, Moon RY. Sudden infant death syndrome (SIDS) and child care centres (CCC). ActaPaediatr 2008; 97:844.
12. Carpenter RG, Irgens LM, Blair PS, et al. Sudden unexplained infant death in 20 regions in Europe: casecontrol study. Lancet 2004; 363:185.
13. Willinger M, Hoffman HJ, Hartford RB. Infant sleep position and risk for sudden infant death syndrome:report of meeting held January 13 and 14, 1994, National Institutes of Health, Bethesda, MD. Pediatrics1994; 93:814.
14. American Academy of Pediatrics AAP Task Force on Infant Positioning and SIDS: Positioning and SIDS.Pediatrics 1992; 89:1120.
15. Positioning and sudden infant death syndrome (SIDS): update. American Academy of Pediatrics Task Forceon Infant Positioning and SIDS. Pediatrics 1996; 98:1216.
16. Mathews TJ, Menacker F, MacDorman MF. Infant mortality statistics from the 2001 period linked birth/infantdeath data set. Natl Vital Stat Rep 2003; 52:1.
17. Centers for Disease Control and Prevention. CDC Wonder. Compressed Mortality File. Underlying CauseofDeath wonder.cdc.gov/mortSQL.html (Accessed on January 05, 2006).
18. Blair PS, Sidebotham P, Berry PJ, et al. Major epidemiological changes in sudden infant death syndrome: a20year populationbased study in the UK. Lancet 2006; 367:314.
19. Hauck FR, Tanabe KO. International trends in sudden infant death syndrome: stabilization of rates requiresfurther action. Pediatrics 2008; 122:660.
20. Hoffman HJ, Damus K, Hillman L, Krongrad E. Risk factors for SIDS. Results of the National Institute ofChild Health and Human Development SIDS Cooperative Epidemiological Study. Ann N Y Acad Sci 1988;533:13.
21. ShapiroMendoza CK, Tomashek KM, Anderson RN, Wingo J. Recent national trends in sudden,unexpected infant deaths: more evidence supporting a change in classification or reporting. Am J Epidemiol2006; 163:762.
22. Poets A, Steinfeldt R, Poets CF. Sudden deaths and severe apparent lifethreatening events in term infantswithin 24 hours of birth. Pediatrics 2011; 127:e869.
23. Pejovic NJ, Herlenius E. Unexpected collapse of healthy newborn infants: risk factors, supervision andhypothermia treatment. Acta Paediatr 2013; 102:680.
24. Thach BT. Deaths and near deaths of healthy newborn infants while bed sharing on maternity wards. JPerinatol 2014; 34:275.
25. Ostfeld BM, Esposito L, Perl H, Hegyi T. Concurrent risks in sudden infant death syndrome. Pediatrics2010; 125:447.
26. MacDorman MF, Cnattingius S, Hoffman HJ, et al. Sudden infant death syndrome and smoking in theUnited States and Sweden. Am J Epidemiol 1997; 146:249.
27. Alm B, Milerad J, Wennergren G, et al. A casecontrol study of smoking and sudden infant death syndromein the Scandinavian countries, 1992 to 1995. The Nordic Epidemiological SIDS Study. Arch Dis Child 1998;78:329.
28. Golding J. Sudden infant death syndrome and parental smokinga literature review. Paediatr Perinat
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 14/25
Epidemiol 1997; 11:67.29. Mitchell EA, Milerad J. Smoking and the sudden infant death syndrome. Rev Environ Health 2006; 21:81.30. Taylor JA, Sanderson M. A reexamination of the risk factors for the sudden infant death syndrome. J Pediatr
1995; 126:887.31. Cohen G, Vella S, Jeffery H, et al. Cardiovascular stress hyperreactivity in babies of smokers and in babies
born preterm. Circulation 2008; 118:1848.32. ViskariLähdeoja S, Hytinantti T, Andersson S, Kirjavainen T. Heart rate and blood pressure control in infants
exposed to maternal cigarette smoking. Acta Paediatr 2008; 97:1535.33. Schneider J, Mitchell I, Singhal N, et al. Prenatal cigarette smoke exposure attenuates recovery from
hypoxemic challenge in preterm infants. Am J Respir Crit Care Med 2008; 178:520.34. Richardson HL, Walker AM, Horne RS. Maternal smoking impairs arousal patterns in sleeping infants. Sleep
2009; 32:515.35. StéphanBlanchard E, Chardon K, Léké A, et al. In utero exposure to smoking and peripheral chemoreceptor
function in preterm neonates. Pediatrics 2010; 125:e592.36. Ali K, Wolff K, Peacock JL, et al. Ventilatory response to hypercarbia in newborns of smoking and
substancemisusing mothers. Ann Am Thorac Soc 2014; 11:933.37. Kandall SR, Gaines J, Habel L, et al. Relationship of maternal substance abuse to subsequent sudden
infant death syndrome in offspring. J Pediatr 1993; 123:120.38. Fares I, McCulloch KM, Raju TN. Intrauterine cocaine exposure and the risk for sudden infant death
syndrome: a metaanalysis. J Perinatol 1997; 17:179.39. Ward SL, Bautista D, Chan L, et al. Sudden infant death syndrome in infants of substanceabusing mothers.
J Pediatr 1990; 117:876.40. PutnamHornstein E, Schneiderman JU, Cleves MA, et al. A prospective study of sudden unexpected infant
death after reported maltreatment. J Pediatr 2014; 164:142.41. StrandbergLarsen K, Grønboek M, Andersen AM, et al. Alcohol drinking pattern during pregnancy and risk of
infant mortality. Epidemiology 2009; 20:884.42. Iyasu S, Randall LL, Welty TK, et al. Risk factors for sudden infant death syndrome among northern plains
Indians. JAMA 2002; 288:2717.43. KlonoffCohen HS, Srinivasan IP, Edelstein SL. Prenatal and intrapartum events and sudden infant death
syndrome. Paediatr Perinat Epidemiol 2002; 16:82.44. Li DK, Wi S. Maternal preeclampsia/eclampsia and the risk of sudden infant death syndrome in offspring.
Paediatr Perinat Epidemiol 2000; 14:141.45. Smith GC, Wood AM, Pell JP, et al. Secondtrimester maternal serum levels of alphafetoprotein and the
subsequent risk of sudden infant death syndrome. N Engl J Med 2004; 351:978.46. Malloy MH, Hoffman HJ. Prematurity, sudden infant death syndrome, and age of death. Pediatrics 1995;
96:464.47. Sowter B, Doyle LW, Morley CJ, et al. Is sudden infant death syndrome still more common in very low
birthweight infants in the 1990s? Med J Aust 1999; 171:411.48. Thompson JM, Mitchell EA, New Zealand Cot Death Study Group. Are the risk factors for SIDS different for
preterm and term infants? Arch Dis Child 2006; 91:107.49. Bigger HR, Silvestri JM, Shott S, WeeseMayer DE. Influence of increased survival in very low birth weight,
low birth weight, and normal birth weight infants on the incidence of sudden infant death syndrome in theUnited States: 19851991. J Pediatr 1998; 133:73.
50. Alm B, Norvenius SG, Wennergren G, et al. Changes in the epidemiology of sudden infant death syndromein Sweden 19731996. Arch Dis Child 2001; 84:24.
51. Blair PS, Platt MW, Smith IJ, et al. Sudden infant death syndrome and sleeping position in preterm and lowbirth weight infants: an opportunity for targeted intervention. Arch Dis Child 2006; 91:101.
52. Bhat RY, Hannam S, Pressler R, et al. Effect of prone and supine position on sleep, apneas, and arousal inpreterm infants. Pediatrics 2006; 118:101.
53. Kassim Z, Donaldson N, Khetriwal B, et al. Sleeping position, oxygen saturation and lung volume inconvalescent, prematurely born infants. Arch Dis Child Fetal Neonatal Ed 2007; 92:F347.
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 15/25
54. Elder DE, Campbell AJ, Galletly D. Effect of position on oxygen saturation and requirement in convalescentpreterm infants. Acta Paediatr 2011; 100:661.
55. Fyfe KL, Yiallourou SR, Wong FY, et al. Cerebral oxygenation in preterm infants. Pediatrics 2014; 134:435.56. American Academy of Pediatrics Committee on Fetus and Newborn. Hospital discharge of the highrisk
neonate. Pediatrics 2008; 122:1119.57. Malloy MH. Size for gestational age at birth: impact on risk for sudden infant death and other causes of
death, USA 2002. Arch Dis Child Fetal Neonatal Ed 2007; 92:F473.58. Guntheroth WG, Lohmann R, Spiers PS. Risk of sudden infant death syndrome in subsequent siblings. J
Pediatr 1990; 116:520.59. Beal SM, Blundell HK. Recurrence incidence of sudden infant death syndrome. Arch Dis Child 1988; 63:924.60. Oyen N, Skjaerven R, Irgens LM. Populationbased recurrence risk of sudden infant death syndrome
compared with other infant and fetal deaths. Am J Epidemiol 1996; 144:300.61. Carpenter RG, Waite A, Coombs RC, et al. Repeat sudden unexpected and unexplained infant deaths:
natural or unnatural? Lancet 2005; 365:29.62. Beal SM. Siblings of sudden infant death syndrome victims. Clin Perinatol 1992; 19:839.63. Getahun D, Demissie K, Lu SE, Rhoads GG. Sudden infant death syndrome among twin births: United
States, 19951998. J Perinatol 2004; 24:544.64. Hoppenbrouwers T, Hodgman JE, Ramanathan A, Dorey F. Extreme and conventional cardiorespiratory
events and epidemiologic risk factors for SIDS. J Pediatr 2008; 152:636.65. Engelberts AC, de Jonge GA. Choice of sleeping position for infants: possible association with cot death.
Arch Dis Child 1990; 65:462.66. Fleming PJ, Gilbert R, Azaz Y, et al. Interaction between bedding and sleeping position in the sudden infant
death syndrome: a population based casecontrol study. BMJ 1990; 301:85.67. Mitchell EA, Scragg R, Stewart AW, et al. Results from the first year of the New Zealand cot death study. N
Z Med J 1991; 104:71.68. Beal SM, Finch CF. An overview of retrospective casecontrol studies investigating the relationship between
prone sleeping position and SIDS. J Paediatr Child Health 1991; 27:334.69. Guntheroth WG, Spiers PS. Sleeping prone and the risk of sudden infant death syndrome. JAMA 1992;
267:2359.70. Taylor JA, Krieger JW, Reay DT, et al. Prone sleep position and the sudden infant death syndrome in King
County, Washington: a casecontrol study. J Pediatr 1996; 128:626.71. Dwyer T, Ponsonby AL, Blizzard L, et al. The contribution of changes in the prevalence of prone sleeping
position to the decline in sudden infant death syndrome in Tasmania. JAMA 1995; 273:783.72. Gardner P, Hudson B. Advance report of final mortality statistics, 1993. Monthly Vital Statistics Report, vol.
44, National Center for Health Statistics, Hyattsville, Maryland, 1996.73. Gibson E, Fleming N, Fleming D, et al. Sudden infant death syndrome rates subsequent to the American
Academy of Pediatrics supine sleep position. Med Care 1998; 36:938.74. Fleming PJ, Blair PS, Bacon C, et al. Environment of infants during sleep and risk of the sudden infant
death syndrome: results of 19935 casecontrol study for confidential inquiry into stillbirths and deaths ininfancy. Confidential Enquiry into Stillbirths and Deaths Regional Coordinators and Researchers. BMJ 1996;313:191.
75. Willinger M, Hoffman HJ, Wu KT, et al. Factors associated with the transition to nonprone sleep positions ofinfants in the United States: the National Infant Sleep Position Study. JAMA 1998; 280:329.
76. Waters KA, Gonzalez A, Jean C, et al. Facestraightdown and facenearstraightdown positions in healthy,pronesleeping infants. J Pediatr 1996; 128:616.
77. Trachtenberg FL, Haas EA, Kinney HC, et al. Risk factor changes for sudden infant death syndrome afterinitiation of BacktoSleep campaign. Pediatrics 2012; 129:630.
78. Mitchell EA. The changing epidemiology of SIDS following the national risk reduction campaigns. PediatrPulmonol Suppl 1997; 16:117.
79. Li DK, Petitti DB, Willinger M, et al. Infant sleeping position and the risk of sudden infant death syndrome in
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 16/25
California, 19972000. Am J Epidemiol 2003; 157:446.80. Mitchell EA, Tuohy PG, Brunt JM, et al. Risk factors for sudden infant death syndrome following the
prevention campaign in New Zealand: a prospective study. Pediatrics 1997; 100:835.81. HelwegLarsen K, Lundemose JB, Oyen N, et al. Interactions of infectious symptoms and modifiable risk
factors in sudden infant death syndrome. The Nordic Epidemiological SIDS study. Acta Paediatr 1999;88:521.
82. Mitchell EA, Thach BT, Thompson JM, Williams S. Changing infants' sleep position increases risk ofsudden infant death syndrome. New Zealand Cot Death Study. Arch Pediatr Adolesc Med 1999; 153:1136.
83. L'Hoir MP, Engelberts AC, van Well GT, et al. Sudden unexpected death in infancy: epidemiologicallydetermined risk factors related to pathological classification. Acta Paediatr 1998; 87:1279.
84. Mitchell EA, Hutchison L, Stewart AW. The continuing decline in SIDS mortality. Arch Dis Child 2007;92:625.
85. United States Food and Drug Administration Safety Alert, 9/29/10. Available at:http://www.fda.gov/Safety/MedWatch/SafetyInformation/SafetyAlertsforHumanMedicalProducts/ucm227733.htm.
86. Centers for Disease Control and Prevention (CDC). Suffocation deaths associated with use of infant sleeppositionersUnited States, 19972011. MMWR Morb Mortal Wkly Rep 2012; 61:933.
87. Mitchell EA, Scragg L, Clements M. Soft cot mattresses and the sudden infant death syndrome. N Z Med J1996; 109:206.
88. Hauck FR, Herman SM, Donovan M, et al. Sleep environment and the risk of sudden infant death syndromein an urban population: the Chicago Infant Mortality Study. Pediatrics 2003; 111:1207.
89. Kemp JS, Thach BT. Sudden death in infants sleeping on polystyrenefilled cushions. N Engl J Med 1991;324:1858.
90. Ponsonby AL, Dwyer T, Gibbons LE, et al. Factors potentiating the risk of sudden infant death syndromeassociated with the prone position. N Engl J Med 1993; 329:377.
91. Rechtman LR, Colvin JD, Blair PS, Moon RY. Sofas and infant mortality. Pediatrics 2014; 134:e1293.92. Mitchell EA, Thompson JM, Ford RP, Taylor BJ. Sheepskin bedding and the sudden infant death syndrome.
New Zealand Cot Death Study Group. J Pediatr 1998; 133:701.93. Vennemann MM, Bajanowski T, Brinkmann B, et al. Sleep environment risk factors for sudden infant death
syndrome: the German Sudden Infant Death Syndrome Study. Pediatrics 2009; 123:1162.94. Wilson CA, Taylor BJ, Laing RM, et al. Clothing and bedding and its relevance to sudden infant death
syndrome: further results from the New Zealand Cot Death Study. J Paediatr Child Health 1994; 30:506.95. Scheers NJ, Dayton CM, Kemp JS. Sudden infant death with external airways covered: casecomparison
study of 206 deaths in the United States. Arch Pediatr Adolesc Med 1998; 152:540.96. Mitchell EA, Thompson JM, Becroft DM, et al. Head covering and the risk for SIDS: findings from the New
Zealand and German SIDS casecontrol studies. Pediatrics 2008; 121:e1478.97. Blair PS, Mitchell EA, HeckstallSmith EM, Fleming PJ. Head covering a major modifiable risk factor for
sudden infant death syndrome: a systematic review. Arch Dis Child 2008; 93:778.98. Thach BT, Rutherford GW Jr, Harris K. Deaths and injuries attributed to infant crib bumper pads. J Pediatr
2007; 151:271.99. Scheers NJ, Woodard DW, Thach BT. Crib Bumpers Continue to Cause Infant Deaths: A Need for a New
Preventive Approach. J Pediatr 2016; 169:93.100. Canadian Paediatric Society. Position statement (CP 200402) Recommendations for safe sleeping
environments for infants and children. Paediatr Child Health 2004; 9:659 www.cps.ca (Accessed onDecember 18, 2008).
101. Blair PS, Fleming PJ, Smith IJ, et al. Babies sleeping with parents: casecontrol study of factors influencingthe risk of the sudden infant death syndrome. CESDI SUDI research group. BMJ 1999; 319:1457.
102. Tappin D, Ecob R, Brooke H. Bedsharing, roomsharing, and sudden infant death syndrome in Scotland: acasecontrol study. J Pediatr 2005; 147:32.
103. Vennemann MM, Hense HW, Bajanowski T, et al. Bed sharing and the risk of sudden infant deathsyndrome: can we resolve the debate? J Pediatr 2012; 160:44.
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 17/25
104. Lahr MB, Rosenberg KD, Lapidus JA. Bedsharing and maternal smoking in a populationbased survey ofnew mothers. Pediatrics 2005; 116:e530.
105. Horsley T, Clifford T, Barrowman N, et al. Benefits and harms associated with the practice of bed sharing: asystematic review. Arch Pediatr Adolesc Med 2007; 161:237.
106. Ruys JH, de Jonge GA, Brand R, et al. Bedsharing in the first four months of life: a risk factor for suddeninfant death. Acta Paediatr 2007; 96:1399.
107. Carpenter R, McGarvey C, Mitchell EA, et al. Bed sharing when parents do not smoke: is there a risk ofSIDS? An individual level analysis of five major casecontrol studies. BMJ Open 2013; 3.
108. McGarvey C, McDonnell M, Chong A, et al. Factors relating to the infant's last sleep environment in suddeninfant death syndrome in the Republic of Ireland. Arch Dis Child 2003; 88:1058.
109. Changing concepts of sudden infant death syndrome: implications for infant sleeping environment and sleepposition. American Academy of Pediatrics. Task Force on Infant Sleep Position and Sudden Infant DeathSyndrome. Pediatrics 2000; 105:650.
110. Mosko S, Richard C, McKenna J. Infant arousals during motherinfant bed sharing: implications for infantsleep and sudden infant death syndrome research. Pediatrics 1997; 100:841.
111. Does bed sharing affect the risk of SIDS? American Academy of Pediatrics. Task Force on InfantPositioning and SIDS. Pediatrics 1997; 100:272.
112. McGarvey C, McDonnell M, Hamilton K, et al. An 8 year study of risk factors for SIDS: bedsharing versusnonbedsharing. Arch Dis Child 2006; 91:318.
113. Colson ER, Willinger M, Rybin D, et al. Trends and factors associated with infant bed sharing, 19932010:the National Infant Sleep Position Study. JAMA Pediatr 2013; 167:1032.
114. SIDS and KIDS safe sleeping: Cobedding twins. Australia (2010). Available at:http://www.sidsandkids.org/wpcontent/uploads/Cobeddingtwins1.pdf.
115. Hutchison BL, Stewart AW, Mitchell EA. The prevalence of cobedding and SIDSrelated child care practicesin twins. Eur J Pediatr 2010; 169:1477.
116. Kornhauser Cerar L, Scirica CV, Stucin Gantar I, et al. A comparison of respiratory patterns in healthy terminfants placed in car safety seats and beds. Pediatrics 2009; 124:e396.
117. Côté A, Bairam A, Deschenes M, Hatzakis G. Sudden infant deaths in sitting devices. Arch Dis Child 2008;93:384.
118. PollackNelson C. Fall and suffocation injuries associated with inhome use of car seats and baby carriers.Pediatr Emerg Care 2000; 16:77.
119. United States Consumer Products Safety Commission. Infant deaths prompt warning about sling carriers forbabies, 3/12/2010. Available at: http://www.cpsc.gov/cpscpub/prerel/prhtml10/10165.html (Accessed onDecember 13, 2011).
120. Bergounioux J, Madre C, CrucisArmengaud A, et al. Sudden deaths in adultworn baby carriers: 19 cases.Eur J Pediatr 2015; 174:1665.
121. Committee on Injury, Violence, and Poison Prevention, Durbin DR. Child passenger safety. Pediatrics 2011;127:788.
122. Richardson HL, Walker AM, Horne RS. Minimizing the risks of sudden infant death syndrome: to swaddle ornot to swaddle? J Pediatr 2009; 155:475.
123. Richardson HL, Walker AM, Horne RS. Influence of swaddling experience on spontaneous arousal patternsand autonomic control in sleeping infants. J Pediatr 2010; 157:85.
124. Scragg RK, Mitchell EA, Stewart AW, et al. Infant roomsharing and prone sleep position in sudden infantdeath syndrome. New Zealand Cot Death Study Group. Lancet 1996; 347:7.
125. Hauck FR, Omojokun OO, Siadaty MS. Do pacifiers reduce the risk of sudden infant death syndrome? Ametaanalysis. Pediatrics 2005; 116:e716.
126. Franco P, Scaillet S, Wermenbol V, et al. The influence of a pacifier on infants' arousals from sleep. JPediatr 2000; 136:775.
127. Kahn A, Sawaguchi T, Sawaguchi A, et al. Sudden infant deaths: from epidemiology to physiology. ForensicSci Int 2002; 130 Suppl:S8.
128. Odoi A, Andrew S, Wong FY, et al. Pacifier use does not alter sleep and spontaneous arousal patterns in
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 18/25
healthy termborn infants. Acta Paediatr 2014; 103:1244.129. Hanzer M, Zotter H, Sauseng W, et al. Pacifier use does not alter the frequency or duration of spontaneous
arousals in sleeping infants. Sleep Med 2009; 10:464.130. l'Hoir MP, Engelberts AC, van Well GT, et al. Casecontrol study of current validity of previously described
risk factors for SIDS in The Netherlands. Arch Dis Child 1998; 79:386.131. Wennergren G, Alm B, Oyen N, et al. The decline in the incidence of SIDS in Scandinavia and its relation to
riskintervention campaigns. Nordic Epidemiological SIDS Study. Acta Paediatr 1997; 86:963.132. Kraus JF, Greenland S, Bulterys M. Risk factors for sudden infant death syndrome in the US Collaborative
Perinatal Project. Int J Epidemiol 1989; 18:113.133. Brooke H, Gibson A, Tappin D, Brown H. Casecontrol study of sudden infant death syndrome in Scotland,
19925. BMJ 1997; 314:1516.134. Gilbert RE, Wigfield RE, Fleming PJ, et al. Bottle feeding and the sudden infant death syndrome. BMJ 1995;
310:88.135. Bertini G, Perugi S, Dani C, et al. Maternal education and the incidence and duration of breast feeding: a
prospective study. J Pediatr Gastroenterol Nutr 2003; 37:447.136. Amir LH, Donath SM. Does maternal smoking have a negative physiological effect on breastfeeding? The
epidemiological evidence. Breastfeed Rev 2003; 11:19.137. Donath SM, Amir LH, ALSPAC Study Team. The relationship between maternal smoking and breastfeeding
duration after adjustment for maternal infant feeding intention. Acta Paediatr 2004; 93:1514.138. Noble L, Hand I, Haynes D, et al. Factors influencing initiation of breastfeeding among urban women. Am J
Perinatol 2003; 20:477.139. Vingraite J, Bartkeviciute R, Michaelsen KF. A cohort study of term infants from Vilnius, Lithuania: feeding
patterns. Acta Paediatr 2004; 93:1349.140. Hauck FR, Thompson JM, Tanabe KO, et al. Breastfeeding and reduced risk of sudden infant death
syndrome: a metaanalysis. Pediatrics 2011; 128:103.141. ColemanPhox K, Odouli R, Li DK. Use of a fan during sleep and the risk of sudden infant death syndrome.
Arch Pediatr Adolesc Med 2008; 162:963.142. Hoffman HJ, Hunter JC, Damus K, et al. Diphtheriatetanuspertussis immunization and sudden infant
death: results of the National Institute of Child Health and Human Development Cooperative EpidemiologicalStudy of Sudden Infant Death Syndrome risk factors. Pediatrics 1987; 79:598.
143. Griffin MR, Ray WA, Livengood JR, Schaffner W. Risk of sudden infant death syndrome after immunizationwith the diphtheriatetanuspertussis vaccine. N Engl J Med 1988; 319:618.
144. JonvilleBéra AP, AutretLeca E, Barbeillon F, et al. Sudden unexpected death in infants under 3 months ofage and vaccination status a casecontrol study. Br J Clin Pharmacol 2001; 51:271.
145. Fleming PJ, Blair PS, Platt MW, et al. The UK accelerated immunisation programme and suddenunexpected death in infancy: casecontrol study. BMJ 2001; 322:822.
146. Mitchell EA, Stewart AW, Clements M. Immunisation and the sudden infant death syndrome. New ZealandCot Death Study Group. Arch Dis Child 1995; 73:498.
147. MacIntyre CR, Leask J. Immunization myths and realities: responding to arguments against immunization. JPaediatr Child Health 2003; 39:487.
148. Vennemann MM, Höffgen M, Bajanowski T, et al. Do immunisations reduce the risk for SIDS? A metaanalysis. Vaccine 2007; 25:4875.
149. Guntheroth WG, Spiers PS. The triple risk hypotheses in sudden infant death syndrome. Pediatrics 2002;110:e64.
150. Rognum TO, Saugstad OD. Biochemical and immunological studies in SIDS victims. Clues tounderstanding the death mechanism. Acta Paediatr Suppl 1993; 82 Suppl 389:82.
151. Filiano JJ, Kinney HC. A perspective on neuropathologic findings in victims of the sudden infant deathsyndrome: the triplerisk model. Biol Neonate 1994; 65:194.
152. Hoffman HJ, Hillman LS. Epidemiology of the sudden infant death syndrome: maternal, neonatal, andpostneonatal risk factors. Clin Perinatol 1992; 19:717.
153. Li DK, Wi S. Maternal placental abnormality and the risk of sudden infant death syndrome. Am J Epidemiol
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 19/25
1999; 149:608.154. Hunt CE. Sudden infant death syndrome. In: Respiratory Control Disorders in Infants and Children,
Beckerman RC, Brouillette RT, Hunt CE (Eds), Williams & Wilkins, Baltimore 1992.155. Schechtman VL, Lee MY, Wilson AJ, Harper RM. Dynamics of respiratory patterning in normal infants and
infants who subsequently died of the sudden infant death syndrome. Pediatr Res 1996; 40:571.156. Panigrahy A, Filiano J, Sleeper LA, et al. Decreased serotonergic receptor binding in rhombic lipderived
regions of the medulla oblongata in the sudden infant death syndrome. J Neuropathol Exp Neurol 2000;59:377.
157. Biondo B, Lavezzi A, Tosi D, et al. Delayed neuronal maturation of the medullary arcuate nucleus in suddeninfant death syndrome. Acta Neuropathol 2003; 106:545.
158. Kinney HC, Randall LL, Sleeper LA, et al. Serotonergic brainstem abnormalities in Northern Plains Indianswith the sudden infant death syndrome. J Neuropathol Exp Neurol 2003; 62:1178.
159. Filiano JJ, Kinney HC. Arcuate nucleus hypoplasia in the sudden infant death syndrome. J Neuropathol ExpNeurol 1992; 51:394.
160. Machaalani R, Say M, Waters KA. Serotoninergic receptor 1A in the sudden infant death syndromebrainstem medulla and associations with clinical risk factors. Acta Neuropathol 2009; 117:257.
161. Paterson DS, Trachtenberg FL, Thompson EG, et al. Multiple serotonergic brainstem abnormalities insudden infant death syndrome. JAMA 2006; 296:2124.
162. Duncan JR, Paterson DS, Hoffman JM, et al. Brainstem serotonergic deficiency in sudden infant deathsyndrome. JAMA 2010; 303:430.
163. Say M, Machaalani R, Waters KA. Changes in serotoninergic receptors 1A and 2A in the piglet brainstemafter intermittent hypercapnic hypoxia (IHH) and nicotine. Brain Res 2007; 1152:17.
164. Opdal SH, Rognum TO. The sudden infant death syndrome gene: does it exist? Pediatrics 2004; 114:e506.165. Hunt CE. Geneenvironment interactions: implications for sudden unexpected deaths in infancy. Arch Dis
Child 2005; 90:48.166. Wang DW, Desai RR, Crotti L, et al. Cardiac sodium channel dysfunction in sudden infant death syndrome.
Circulation 2007; 115:368.167. Arnestad M, Crotti L, Rognum TO, et al. Prevalence of longQT syndrome gene variants in sudden infant
death syndrome. Circulation 2007; 115:361.168. Van Norstrand DW, Valdivia CR, Tester DJ, et al. Molecular and functional characterization of novel
glycerol3phosphate dehydrogenase 1 like gene (GPD1L) mutations in sudden infant death syndrome.Circulation 2007; 116:2253.
169. Otagiri T, Kijima K, Osawa M, et al. Cardiac ion channel gene mutations in sudden infant death syndrome.Pediatr Res 2008; 64:482.
170. Tan BH, Pundi KN, Van Norstrand DW, et al. Sudden infant death syndromeassociated mutations in thesodium channel beta subunits. Heart Rhythm 2010; 7:771.
171. Tester DJ, Tan BH, MedeirosDomingo A, et al. Lossoffunction mutations in the KCNJ8encoded Kir6.1K(ATP) channel and sudden infant death syndrome. Circ Cardiovasc Genet 2011; 4:510.
172. Van Norstrand DW, Asimaki A, Rubinos C, et al. Connexin43 mutation causes heterogeneous gap junctionloss and sudden infant death. Circulation 2012; 125:474.
173. Narita N, Narita M, Takashima S, et al. Serotonin transporter gene variation is a risk factor for sudden infantdeath syndrome in the Japanese population. Pediatrics 2001; 107:690.
174. WeeseMayer DE, Zhou L, BerryKravis EM, et al. Association of the serotonin transporter gene with suddeninfant death syndrome: a haplotype analysis. Am J Med Genet A 2003; 122A:238.
175. Rahim RA, Boyd PA, Ainslie Patrick WJ, Burdon RH. Human heat shock protein gene polymorphisms andsudden infant death syndrome. Arch Dis Child 1996; 75:451.
176. Opdal SH, Vege A, Rognum TO. Serotonin transporter gene variation in sudden infant death syndrome. ActaPaediatr 2008; 97:861.
177. Nonnis Marzano F, Maldini M, Filonzi L, et al. Genes regulating the serotonin metabolic pathway in the brainstem and their role in the etiopathogenesis of the sudden infant death syndrome. Genomics 2008; 91:485.
178. Klintschar M, Heimbold C. Association between a functional polymorphism in the MAOA gene and sudden
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 20/25
infant death syndrome. Pediatrics 2012; 129:e756.179. Courts C, Grabmüller M, Madea B. Monoamine oxidase A gene polymorphism and the pathogenesis of
sudden infant death syndrome. J Pediatr 2013; 163:89.180. WeeseMayer DE, BerryKravis EM, Zhou L, et al. Sudden infant death syndrome: casecontrol frequency
differences at genes pertinent to early autonomic nervous system embryologic development. Pediatr Res2004; 56:391.
181. Cummings KJ, Klotz C, Liu WQ, et al. Sudden infant death syndrome (SIDS) in African Americans:polymorphisms in the gene encoding the stress peptide pituitary adenylate cyclaseactivating polypeptide(PACAP). Acta Paediatr 2009; 98:482.
182. Opdal SH, Vege A, Stave AK, Rognum TO. The complement component C4 in sudden infant death. Eur JPediatr 1999; 158:210.
183. Summers AM, Summers CW, Drucker DB, et al. Association of IL10 genotype with sudden infant deathsyndrome. Hum Immunol 2000; 61:1270.
184. Opdal SH, Opstad A, Vege A, Rognum TO. IL10 gene polymorphisms are associated with infectious causeof sudden infant death. Hum Immunol 2003; 64:1183.
185. Korachi M, Pravica V, Barson AJ, et al. Interleukin 10 genotype as a risk factor for sudden infant deathsyndrome: determination of IL10 genotype from waxembedded postmortem samples. FEMS Immunol MedMicrobiol 2004; 42:125.
186. Puffenberger EG, HuLince D, Parod JM, et al. Mapping of sudden infant death with dysgenesis of thetestes syndrome (SIDDT) by a SNP genome scan and identification of TSPYL loss of function. Proc NatlAcad Sci U S A 2004; 101:11689.
187. Opdal SH, Rognum TO. New insight into sudden infantdeath syndrome. Lancet 2004; 364:825.188. Courts C, Grabmüller M, Madea B. Functional singlenucleotide variant of HSPD1 in sudden infant death
syndrome. Pediatr Res 2013; 74:380.189. Meny RG, Carroll JL, Carbone MT, Kelly DH. Cardiorespiratory recordings from infants dying suddenly and
unexpectedly at home. Pediatrics 1994; 93:44.190. Groswasser J, Simon T, Scaillet S, et al. Reduced arousals following obstructive apneas in infants sleeping
prone. Pediatr Res 2001; 49:402.191. Horne RS, Ferens D, Watts AM, et al. The prone sleeping position impairs arousability in term infants. J
Pediatr 2001; 138:811.192. Wong FY, Witcombe NB, Yiallourou SR, et al. Cerebral oxygenation is depressed during sleep in healthy
term infants when they sleep prone. Pediatrics 2011; 127:e558.193. Wong F, Yiallourou SR, Odoi A, et al. Cerebrovascular control is altered in healthy term infants when they
sleep prone. Sleep 2013; 36:1911.194. Chiodini BA, Thach BT. Impaired ventilation in infants sleeping facedown: potential significance for sudden
infant death syndrome. J Pediatr 1993; 123:686.195. Guntheroth WG, Spiers PS. Thermal stress in sudden infant death: Is there an ambiguity with the
rebreathing hypothesis? Pediatrics 2001; 107:693.196. Thompson JM, Thach BT, Becroft DM, et al. Sudden infant death syndrome: risk factors for infants found
face down differ from other SIDS cases. J Pediatr 2006; 149:630.197. Southall DP, Stevens V, Franks CI, et al. Sinus tachycardia in term infants preceding sudden infant death.
Eur J Pediatr 1988; 147:74.198. Schwartz PJ, StrambaBadiale M, Segantini A, et al. Prolongation of the QT interval and the sudden infant
death syndrome. N Engl J Med 1998; 338:1709.199. Ackerman MJ, Siu BL, Sturner WQ, et al. Postmortem molecular analysis of SCN5A defects in sudden
infant death syndrome. JAMA 2001; 286:2264.200. Plant LD, Bowers PN, Liu Q, et al. A common cardiac sodium channel variant associated with sudden infant
death in African Americans, SCN5A S1103Y. J Clin Invest 2006; 116:430.201. Weber MA, Ashworth MT, Risdon RA, et al. The role of postmortem investigations in determining the cause
of sudden unexpected death in infancy. Arch Dis Child 2008; 93:1048.202. Highet AR. An infectious aetiology of sudden infant death syndrome. J Appl Microbiol 2008; 105:625.
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 21/25
203. Goldwater PN. SIDS pathogenesis: pathological findings indicate infection and inflammatory responses areinvolved. FEMS Immunol Med Microbiol 2004; 42:11.
204. Goldwater PN. Sterile site infection at autopsy in sudden unexpected deaths in infancy. Arch Dis Child2009; 94:303.
205. Weber MA, Klein NJ, Hartley JC, et al. Infection and sudden unexpected death in infancy: a systematicretrospective case review. Lancet 2008; 371:1848.
206. Creery D, Mikrogianakis A. Sudden infant death syndrome. Clin Evid 2005; :434.207. Recommendations for safe sleeping environments for infants and children. Paediatr Child Health 2004;
9:659.208. Reducing the risk of cot death. Available at: http://www.patient.co.uk/health/reducingtheriskofcotdeath
(Accessed on October 15, 2013).209. Colson ER, Joslin SC. Changing nursery practice gets innercity infants in the supine position for sleep.
Arch Pediatr Adolesc Med 2002; 156:717.210. National Center for Education in Maternal and Child Health at Georgetown University; SUID/SIDS Gateway.
Available at: www.ncemch.org/suidsids (Accessed on July 29, 2015).211. Mitchell EA. Recommendations for sudden infant death syndrome prevention: a discussion document. Arch
Dis Child 2007; 92:155.212. Howard CR, Howard FM, Lanphear B, et al. Randomized clinical trial of pacifier use and bottlefeeding or
cupfeeding and their effect on breastfeeding. Pediatrics 2003; 111:511.213. Uhari M, Mäntysaari K, Niemelä M. A metaanalytic review of the risk factors for acute otitis media. Clin
Infect Dis 1996; 22:1079.
Topic 6366 Version 37.0
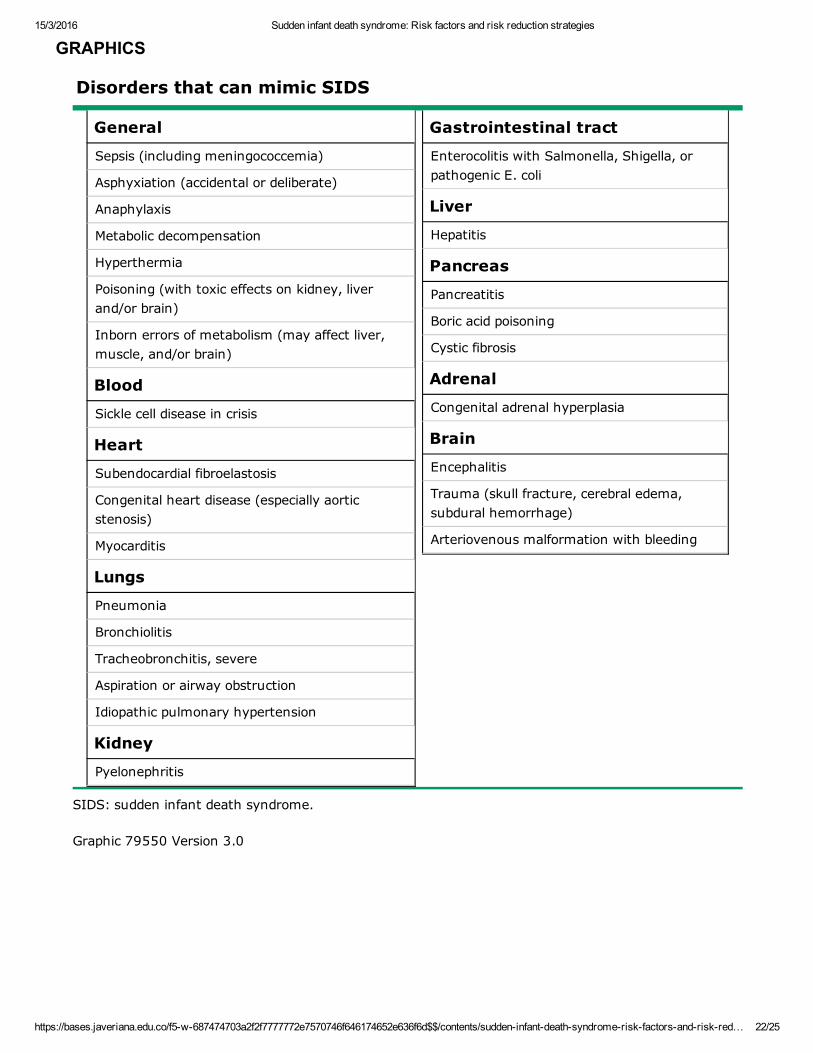
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 22/25
GRAPHICS
Disorders that can mimic SIDS
General
Sepsis (including meningococcemia)
Asphyxiation (accidental or deliberate)
Anaphylaxis
Metabolic decompensation
Hyperthermia
Poisoning (with toxic effects on kidney, liverand/or brain)
Inborn errors of metabolism (may affect liver,muscle, and/or brain)
Blood
Sickle cell disease in crisis
Heart
Subendocardial fibroelastosis
Congenital heart disease (especially aorticstenosis)
Myocarditis
Lungs
Pneumonia
Bronchiolitis
Tracheobronchitis, severe
Aspiration or airway obstruction
Idiopathic pulmonary hypertension
Kidney
Pyelonephritis
Gastrointestinal tract
Enterocolitis with Salmonella, Shigella, orpathogenic E. coli
Liver
Hepatitis
Pancreas
Pancreatitis
Boric acid poisoning
Cystic fibrosis
Adrenal
Congenital adrenal hyperplasia
Brain
Encephalitis
Trauma (skull fracture, cerebral edema,subdural hemorrhage)
Arteriovenous malformation with bleeding
SIDS: sudden infant death syndrome.
Graphic 79550 Version 3.0
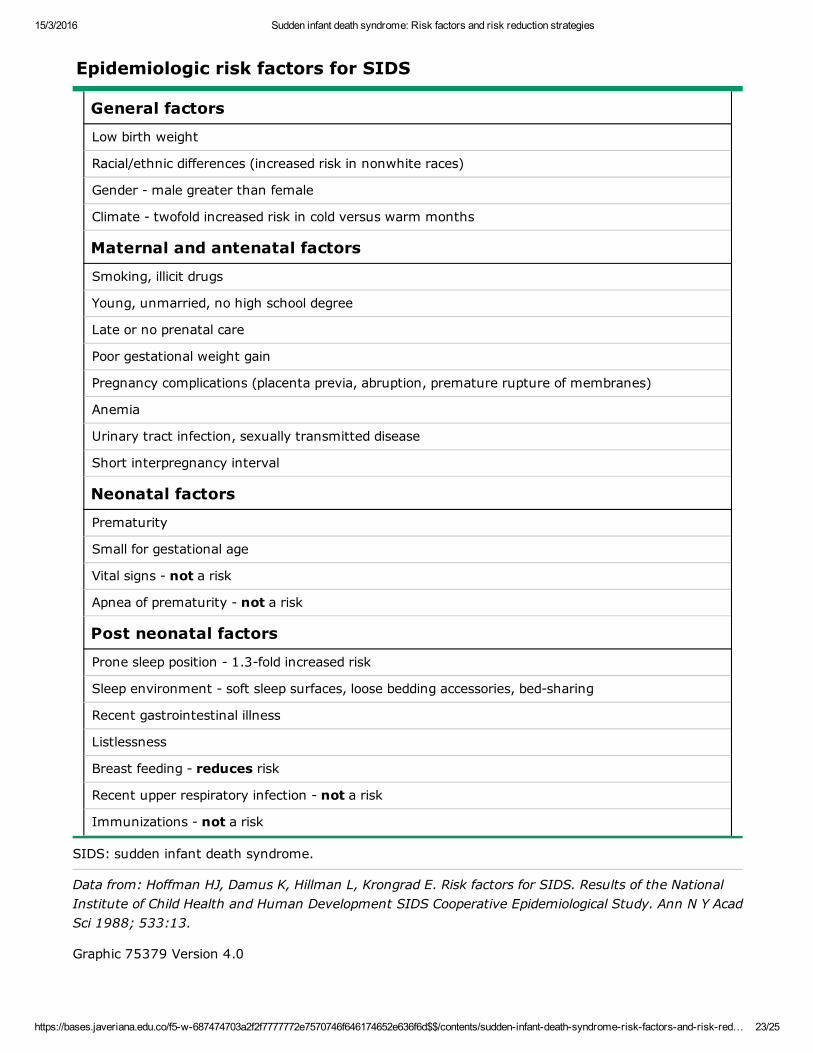
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 23/25
Epidemiologic risk factors for SIDS
General factors
Low birth weight
Racial/ethnic differences (increased risk in nonwhite races)
Gender male greater than female
Climate twofold increased risk in cold versus warm months
Maternal and antenatal factors
Smoking, illicit drugs
Young, unmarried, no high school degree
Late or no prenatal care
Poor gestational weight gain
Pregnancy complications (placenta previa, abruption, premature rupture of membranes)
Anemia
Urinary tract infection, sexually transmitted disease
Short interpregnancy interval
Neonatal factors
Prematurity
Small for gestational age
Vital signs not a risk
Apnea of prematurity not a risk
Post neonatal factors
Prone sleep position 1.3fold increased risk
Sleep environment soft sleep surfaces, loose bedding accessories, bedsharing
Recent gastrointestinal illness
Listlessness
Breast feeding reduces risk
Recent upper respiratory infection not a risk
Immunizations not a risk
SIDS: sudden infant death syndrome.
Data from: Hoffman HJ, Damus K, Hillman L, Krongrad E. Risk factors for SIDS. Results of the NationalInstitute of Child Health and Human Development SIDS Cooperative Epidemiological Study. Ann N Y AcadSci 1988; 533:13.
Graphic 75379 Version 4.0
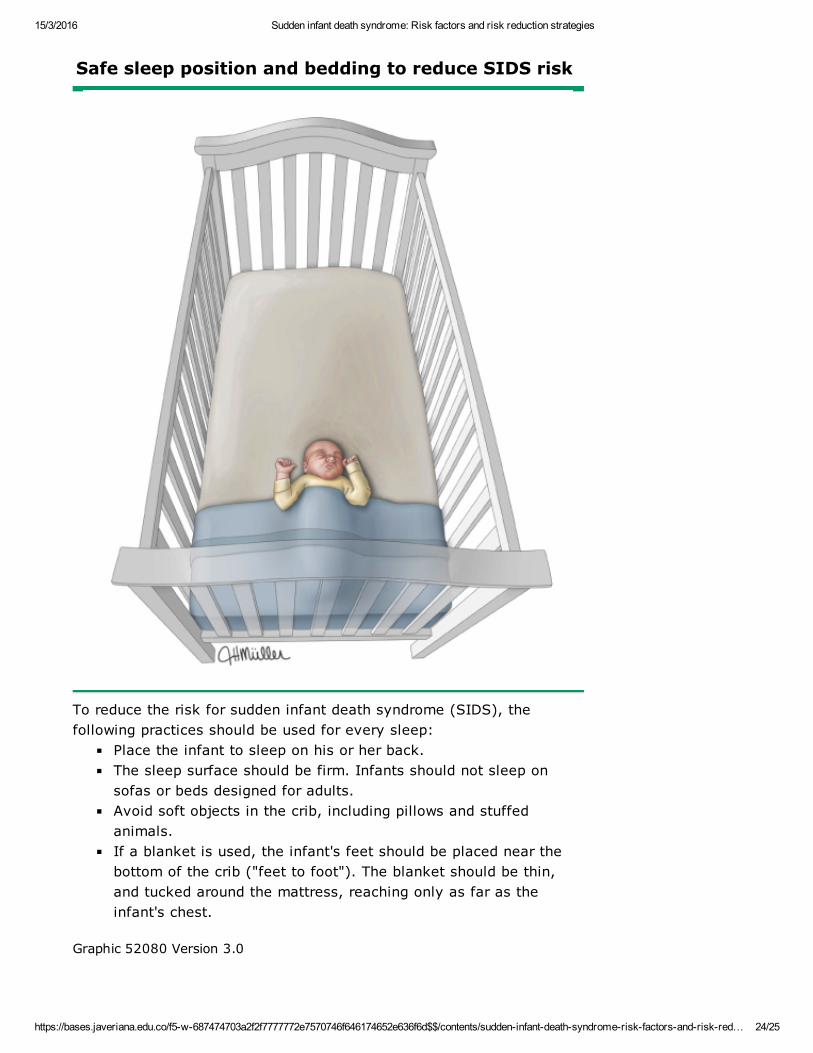
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 24/25
Safe sleep position and bedding to reduce SIDS risk
To reduce the risk for sudden infant death syndrome (SIDS), thefollowing practices should be used for every sleep:
Place the infant to sleep on his or her back.The sleep surface should be firm. Infants should not sleep onsofas or beds designed for adults.Avoid soft objects in the crib, including pillows and stuffedanimals.If a blanket is used, the infant's feet should be placed near thebottom of the crib ("feet to foot"). The blanket should be thin,and tucked around the mattress, reaching only as far as theinfant's chest.
Graphic 52080 Version 3.0
15/3/2016 Sudden infant death syndrome: Risk factors and risk reduction strategies
https://bases.javeriana.edu.co/f5w687474703a2f2f7777772e7570746f646174652e636f6d$$/contents/suddeninfantdeathsyndromeriskfactorsandriskred… 25/25
Disclosures: Michael J Corwin, MD Nothing to disclose. George B Mallory, MD Nothing to disclose. Teresa K Duryea, MD Nothing todisclose. Alison G Hoppin, MD Nothing to disclose.Contributor disclosures are reviewed for conflicts of interest by the editorial group. When found, these are addressed by vetting through amultilevel review process, and through requirements for references to be provided to support the content. Appropriately referencedcontent is required of all authors and must conform to UpToDate standards of evidence.Conflict of interest policy
Disclosures


![Clinical features of abruptio placentae as a prominent ... · abruptio placentae at presentation [3]. As abruptio placentae is one of the leading causes ... weeks are also eligible](https://img.pdfslide.us/doc/110x75/5b2ae1867f8b9afd328b4b75/clinical-features-of-abruptio-placentae-as-a-prominent-abruptio-placentae.jpg)


























