Embed Size (px)
Citation preview

1
Home Care Auditing:What’s all the MOOing About?
Home Care Auditing:What’s all the MOOing About?About?About?
Catherine NilandAHIA 2008 Annual ConferenceSeptember 2008
Catherine NilandAHIA 2008 Annual ConferenceSeptember 2008
Objectives
• Overview of Home Care• Medicare Home Care Prospective Payment
System• Financial and Operational controls
Copyright 2008 Trinity Health – Novi, Michigan 2
Medicare Home Care Conditions of Participation• Patient must require skilled care (RN, PT, Speech therapy)• No willing or able caregiver available• Services must be provided on an intermittent basis
– May be daily for a short duration or less frequently over a longer period of time
– Cannot be for one-time only visits, with few exceptions• Plan of Care must be completed and signed by the
Copyright 2008 Trinity Health – Novi, Michigan 3
• Plan of Care must be completed and signed by the physician prior to billing final claim
• Services must be reasonable and necessary• Services must be provided in a place of residence used as
the patient’s home (may be home, senior apartment, assisted living facility, etc.)
• Patient must be homebound• Episode of care is 60 days; may have unlimited number of
episodes as long as above criteria met

2
Home Bound Status
• Must be determined prior to start of care• Patient must be confined to the home
– A normal inability to leave home;– Leaving home would require a considerable and taxing effort;– Leaving home requires the assistance of another person.
• Confinement due to medical psychiatric or physical
Copyright 2008 Trinity Health – Novi, Michigan 4
• Confinement due to medical, psychiatric, or physical condition
• May leave home infrequently for medical appointments or non-medical reasons for short duration (i.e. attend church)
• Attendance at Adult Day Care does not disqualify homebound status (Program Memorandum A-01-21 2/6/01)
Plan of Care• Plan of Care (form 485) must be completed prior to
provision of care– Must indicate type, duration and frequency of
all services and treatment orders– May be verbal order initially
• With subsequent episodes of care new or updated Plan of
Copyright 2008 Trinity Health – Novi, Michigan 5
• With subsequent episodes of care, new or updated Plan of Care required, along with new orders
• Verbal orders received during episode of care modify the plan of care
• Physician MUST sign the Plan of Care and all verbal orders prior to billing final claim for the episode
Type of Services
• Skilled Nursing Care– Care that may only be performed by RN (or LPN in
certain circumstances)– Includes wound care, medication administration, and
patient/caregiver education• Home Health Aide
Copyright 2008 Trinity Health – Novi, Michigan 6
Home Health Aide– Provide assistance with Activities of Daily Living (such
as bathing, grooming, dressing, walking, etc.)– May perform some light housekeeping duties in addition
to ADL assistance; however, homemaker-type services alone are not covered by Medicare
– May only be provided with other skilled services

3
Type of Services
• Physical Therapy– Provided by licensed therapist or therapy assistant; may
not be performed by therapy aide– Includes instruction for a Home Exercise Program (HEP)
• Speech TherapyPerformed b licensed therapist
Copyright 2008 Trinity Health – Novi, Michigan 7
– Performed by licensed therapist – Includes cognitive and/or speech therapy
• Occupational Therapy– May only be provided as an adjunct to Physical &/or
Speech therapy; can continue after other skilled services are discontinued
– Provided by licensed therapist and/or assistant, no aides
Type of Services
• Social Work– May assist the patient with other needs, such as
arranging for housekeeping services, transportation, obtaining DME, etc.
– May also arrange for other services, such as N t iti /di t li
Copyright 2008 Trinity Health – Novi, Michigan 8
Nutrition/dietary counseling– May only be provided when another skilled service is
provided
no PPS !!!
Copyright 2008 Trinity Health – Novi, Michigan 9
Cartoon by Tom Wilson© Universal Press Syndicate
no PPS !!!

4
Home Care Prospective Payment System
• Implemented October 2000; major revision effective 1/1/08
• Affects Part A payment only• Established Consolidated Billing for all disciplines,
non-routine supplies outpatient therapies and
Copyright 2008 Trinity Health – Novi, Michigan 10
non routine supplies, outpatient therapies, and some wound care treatments
• Requires OASIS (Outcomes and ASsessment Information Set) completion by home health clinicians (RN, PT, SLP)
OASIS Assessment• Required at start of episode, resumption of care, and end of
episode – Specific time frames required for each assessment
• Within 5 days of Start of Care• Within last 5 days of 60 Day episode• Within 48 hours after d/c from inpatient admission greater than 24 hours• Transfer to new HHA or d/c and readmit to same HHA within 60 days
At di h
Copyright 2008 Trinity Health – Novi, Michigan 11
• At discharge– Must be encoded and submitted within 30 days of the assessment
• 105 items make up current version B-1(MO questions)• 23 items used to help determine Home Health Resource
Group (HHRG) Medicare payment– Assessment items grouped by Clinical (C), Functional (F), and
Service (S) DomainsNOTE: Home care Medicare payment driven by clinician
documentation NOT physician documentation
OASIS Reimbursement Items• Clinical Domain
– Diagnosis Coding• MO230 Primary Diagnosis• MO240 Secondary Diagnoses• MO246 Case Mix Diagnosis (if V or E code in MO230)
– Wounds• MO450/460 pressure ulcers
MO476 t i l
Copyright 2008 Trinity Health – Novi, Michigan 12
• MO476 stasis ulcers• MO488 wounds
– Also Pain, Vision, Dyspnea, Bowel incontinence, Ostomy• Functional Domain
– MO650, MO660, MO670, MO680, MO690, MO700– Dressing, Bathing, Toileting, Transfers, and Locomotion
• Service Domain– MO110 1st - 2nd episode or 3rd or later episode– MO826 Number of projected therapy visits

5
Home Health Resource Group (HHRG)
• Once OASIS completed, reimbursable items from each domain is used to determine the HHRG
• Represented by 6 digit alpha-numeric code
CxFxSx– 1st 2 characters represent clinical domain score
Copyright 2008 Trinity Health – Novi, Michigan 13
– 2nd 2 characters represent functional domain score– 3rd 2 characters represent service domain score
• HHRG of C1F1S1 indicates lowest level of service, C3F3S5 is highest
• HHRG translated to HIPPS (Health insurance prospective payment system) code for billing purposes
HIPPS Codes
• HIPPS is 5 character code – 1st position character is number 1 to 5; represents severity level (#
therapy visits and episode sequence)– 2nd position character is A, B, or C; represents Clinical Domain
score– 3rd position is F, G, or H; represents Functional Domain score
Copyright 2008 Trinity Health – Novi, Michigan 14
– 4th position is K, L, M, N, or P; represents Service Domain score– 5th position is either S, T, U, V, W, X or 1, 2, 3, 4, 5, 6; alpha
represents non routine supplies (NRS) provided and numeric represents no NRS provided
C1F1S1 1st episode/no therapy/no NRS would be: 1AKF1C3F3S5 4th episode/20+ therapy/ NRS 99 points would be: 5CHPX
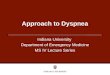
See Exhibit A for calculation table
Calculation Table- Exhibit AAll Episodes
1 2 3 4 5 10 to 4 0 to 6 0 to 2 0 to 8 0 to 7 C15 to 8 7 to 14 3 to 5 9 to 16 8 to 14 C2
9+ 15+ 6+ 17+ 15+ C30 to 5 0 to 6 0 to 8 0 to 7 0 to 6 F1
6 7 9 8 7 F27+ 8+ 10+ 9+ 8+ F3
G
(grouping step): 1 to 5ABC
2
3H
F
Clinical Severity Level: (by point scores- Pseudocode
Appendix Table 5)Functional Severity Level:
(by point scores- Pseudocode Appendix Table 5)
Definitions of Severity Levels by Grouping Step:1st & 2nd Episodes 3rd+ Episodes0 to 13 therapy visits
14 to 19 therapy visits
0 to 13 therapy visits
14 to 19 therapy visits
20+ therapy visits
HIPPS Code
For this level
In HIPPS position:Enter this value:
Copyright 2008 Trinity Health – Novi, Michigan 15
7+ 8+ 10+ 9+ 8+ F3
6 16 to 17 6 16 to 17 S27 to 9 18 to 19 7 to 9 18 to 19 S3
10 10 S411 to 13 11 to 13 S5
NRS-1 S 1NRS-2 T 2NRS-3 U 3NRS-4 V 4NRS-5 W 5NRS-6 X 699+
NRS-Supplies Severity Level: (by NRS point scores-
Pseudocode Appendix Table 7)
NRS provided
no NRS provided
5
0
S1
15 to 2728 to 48
1 to 14
4LMNP
H
K
Appendix Table 5)
Services Utilization Level: (by number of therapy visits)
NRS Points
0 to 5 14 to 15 0 to 5 14 to 15 20+ (one group)
49 to 98

6
PPS Reimbursement
• Reimbursement split into Request for Anticipated Payment (RAP) and Final Claim– Initial RAP payment 60% of reimbursement; claim 40%– RAP/claim payment split 50% with subsequent episodes– RAP not considered claim except for purposes of False Claims Act
RAP establishes in the Common Working File which
Copyright 2008 Trinity Health – Novi, Michigan 16
• RAP establishes in the Common Working File which agency is providing service for an episode
• RAP must be submitted within 60 days of start of episode or will be denied; may resubmit if delayed beyond 60 days
• Claim won’t be paid without RAP on file (except in certain circumstances)
How the PPS Works- Quick Summary
• Complete the OASIS by performing an initial assessment
• Use decision tree logic to determine an initial Home Health Resource Group (HHRG) score
• Submit a Request for Anticipated Payment (RAP) and receive 60% reimbursement (initial episode) or 50% for
Copyright 2008 Trinity Health – Novi, Michigan 17
receive 60% reimbursement (initial episode) or 50% for subsequent episodes
• Perform an end-of-episode assessment and submit a claim with the final HHRG score
• Receive final adjusted payment
• For subsequent episodes, end-of episode assessment used to determine next episode HHRG
LUPA
Low Utilization Payment Adjustment (LUPA)• 4 or fewer visits in the episode• Adjustment to HHRG reimbursement amount• Additional add-on ($91.80) for LUPA that occurs as the only
episode or the 1st episode of home care benefit use
Copyright 2008 Trinity Health – Novi, Michigan 18
– New benefit effective 1/1/08– Requirements:
• 4 or fewer visits• HIPPS code on claim begins with “1” or “2” indicating early episode• Claim admission date and “from” date are the same• Source of Admission is not B or C

7
PEP
• Partial Episode Payment (PEP)– Prorated payment adjustment when patient changes
HHA during an episode• New 60 day period begins when patient transfers from one
agency and goes to another or• When patient discharged and readmitted to same HHA during
Copyright 2008 Trinity Health – Novi, Michigan 19
When patient discharged and readmitted to same HHA during same 60-day episode
– 1st HHA or episode gets prorated HHRG; 2nd HHA or readmitted episode gets full HHRG
Non- Routine Supplies (NRS)
• Prior to 1/1/08 home care agencies generally did not bill for non-routine supplies; reimbursement poor and not worth effort to collect data
• Effective 1/1/08, additional reimbursement now available from $14 to $551 per episode
Copyright 2008 Trinity Health – Novi, Michigan 20
$ $ p p• OASIS responses used to calculate amount of
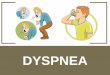
reimbursement (indicated by HIPPS 5th character)• See Exhibit B for calculation table (Table 7 of
Pseudocode Appendix Tables)
Table 7- Exhibit B
(1) (2) (3)ROW VARIABLE DESCRIPTION Points
1 Primary diagnosis = Anal fissure, fistula and abscess 152 Other diagnosis = Anal fissure, fistula and abscess 133 Primary diagnosis = Cellulitis and abscess 144 Other diagnosis = Cellulitis and abscess 85 Primary diagnosis = Diabetic ulcers [* SEE NOTE] 206 Primary diagnosis = Gangrene 11
HHA PPS Grouper 0202 Logic January 28, 2008 Pseudocode APPENDIX TABLES
Table 7: Nonroutine Medical Supplies (NRS): Case-Mix Adjustment Variables and Point Scores(Table taken from Table 10A of Final Rule CMS-1541-FC)
SELECTED SKIN CONDITIONS:
Copyright 2008 Trinity Health – Novi, Michigan 21
6 Primary diagnosis = Gangrene 117 Other diagnosis = Gangrene 88 Primary diagnosis = Malignant neoplasms of skin 159 Other diagnosis = Malignant neoplasms of skin 4
10 Primary or Other diagnosis = Non-pressure and non-stasis ulcers[* SEE NOTE] 1311 Primary diagnosis = Other infections of skin and subcutaneous tissue 1612 Other diagnosis = Other infections of skin and subcutaneous tissue 713 Primary diagnosis = Post-operative Complications 2314 Other diagnosis = Post-operative Complications 1515 Primary diagnosis = Traumatic Wounds and Burns 1916 Other diagnosis = Traumatic Wounds and Burns 817 Primary or other diagnosis = V code, Cystostomy care 1618 Primary or other diagnosis = V code, Tracheostomy care 2319 Primary or other diagnosis = V code, Urostomy care 2420 OASIS M0450 = 1 or 2 pressure ulcers, stage 1 421 OASIS M0450 = 3+ pressure ulcers, stage 1 622 OASIS M0450 = 1 pressure ulcer, stage 2 1423 OASIS M0450 = 2 pressure ulcers, stage 2 22

8
Table 7- Appendix B Continued24 OASIS M0450 = 3 pressure ulcers, stage 2 2925 OASIS M0450 = 4+ pressure ulcers, stage 2 3526 OASIS M0450 = 1 pressure ulcer, stage 3 2927 OASIS M0450 = 2 pressure ulcers, stage 3 4128 OASIS M0450 = 3 pressure ulcers, stage 3 4629 OASIS M0450 = 4+ pressure ulcers, stage 3 5830 OASIS M0450 = 1 pressure ulcer, stage 4 4831 OASIS M0450 = 2 pressure ulcers, stage 4 6732 OASIS M0450 = 3+ pressure ulcers, stage 4 7533 OASIS M0450e = 1(unobserved pressure ulcer(s)) 1734 OASIS M0470 = 2 (2 stasis ulcers) 635 OASIS M0470 = 3 (3 stasis ulcers) 1236 OASIS M0470 = 4 (4+ stasis ulcers) 2137 OASIS M0474 = 1 (unobservable stasis ulcers) 9
Copyright 2008 Trinity Health – Novi, Michigan 22
37 OASIS M0474 1 (unobservable stasis ulcers) 938 OASIS M0476 = 1 (status of most problematic stasis ulcer: fully granulating) 639 OASIS M0476 = 2 (status of most problematic stasis ulcer: early/partial granulation) 2540 OASIS M0476 = 3 (status of most problematic stasis ulcer: not healing) 3641 OASIS M0488 = 2 (status of most problematic surgical wound: early/partial granulation) 442 OASIS M0488 = 3 (status of most problematic surgical wound: not healing) 14
43 OASIS M0550=1(ostomy not related to inpt stay/no regimen change) 2744 OASIS M0550=2 (ostomy related to inpt stay/regimen change) 4545 Any `Selected Skin Conditions` (rows 1-42 above) AND M0550=1(ostomy not related to inpt stay/no regimen
change)14
46 Any `Selected Skin Conditions` (rows 1-42 above) AND M0550=2(ostomy related to inpt stay/ regimen change) 1147 OASIS M0250 (Therapy at home) =1 (IV/Infusion) 548 OASIS M0520 = 2 (patient requires urinary catheter) 949 OASIS M0540 = 4 or 5 (bowel incontinence, daily or >daily) 10
NOTE:* If episode receives points for diabetic ulcers, it cannot also receive points for “Non-pressure and non-stasis ulcers.”
OTHER CLINICAL FACTORS:
Why CMS Changed the Home Care PPS
“We have tried to strike a balance between simplicity and complexity. The new system is more complex than the old system but this a natural outgrowth of our attempt to pay more accurately for the range and intensity of home health services that can be
Copyright 2008 Trinity Health – Novi, Michigan 23
provided to our beneficiaries.”
42 CFR part 484 Medicare Program; Home Health Prospective Payment System Refinement and Rate Update for Calendar year 2008; Final Rule
Federal Register, August 29, 2007, page 49770
Remember:PPS stands for “Please
Copyright 2008 Trinity Health – Novi, Michigan 24
PPS stands for Please Pay SOMETHING”!!!!
Michael O. Leavitt,
US Secretary of Health and Human Services

9
ICD-9 Coding
Accurate diagnosis coding is critical• Non-specific code use can impact amount reimbursed
– “Not otherwise specified code” when specific information available – 730.20 for osteomyelitis site unspecified gains no points; 730.26 for
lower leg gains 2 or 5 case mix points
• Diagnosis documented but not included in OASIS
Copyright 2008 Trinity Health – Novi, Michigan 25
• Diagnosis documented but not included in OASIS– Diabetes adds 2 to 5 points to the case mix score for a 1st episode.
Even if patient is stable, diabetes can affect resources used, and should be included.
• In above 2 examples, 2 points could change HHRG from C1 to C2, with increase of $323
• Correct coding guidelines apply- and if it isn’t documented by the physician it can’t be coded
Consolidated BillingRequires that all services related to the treated condition,
including medications and supplies, to be included in the HHRG payment. Exception: any osteoporosis medication is included, whether related to condition or not.
Excludes:• Physician professional services
Copyright 2008 Trinity Health – Novi, Michigan 26
– Including Physician-provided therapy– Technical component of physician services must be billed to and
reimbursed by the HHA• Dialysis services• Epoetin Alfa (Epogen) for dialysis patients• Ambulance services• Durable Medical Equipment• Customized prosthetic devices
Consolidated Billing
Exclusion, continued:•Certain chemotherapy items and their administration•Services that are exceptionally costly, intense, or emergent are also excluded.
CMS has an Excel workbook file containing
Copyright 2008 Trinity Health – Novi, Michigan 27
CMS has an Excel workbook file containing complete lists of all codes ever subject to consolidated billing provision of HH PPS. It is available online at:
http://www.cms.hhs.gov/HomeHealthPPS/03_coding&billing.asp

10
Copyright 2008 Trinity Health – Novi, Michigan 28
Intake and Insurance Verification
• Physician order received prior to start of care• Payer information verified
– Appropriate pre-certs and referrals obtained prior to start of care
– Medicare as Secondary Payer (MSP) Questionnaire completed appropriately
Copyright 2008 Trinity Health – Novi, Michigan 29
completed appropriately• Health Insurance Query for Home Health (HIQH) to
verify no other agency providing care• When required, Advance Beneficiary Notice
(HHABNs) is obtained and completed appropriately• Tracking of 485 to ensure signature obtained prior
to billing
Claims Submission• Pre-billing audits for RAP:
– Verbal Start of Care order on file– 1st visit and initial assessment completed– The RAP contains one HIPPS code – “From” and “Through” dates match the date of first service– Verify episode timing (check Common Working File)
• Pre-Billing audits for claim:
Copyright 2008 Trinity Health – Novi, Michigan 30
Pre Billing audits for claim:– Signed and dated Plan of Care on file – Signed and dated interim orders on file– OASIS has been electronically transmitted to the appropriate site
(MAC or state agency)– Clinical documentation for each visit on file– Claim has same HIPPS code as RAP– Claim includes line item details– “From” date is same as RAP; “Through” date is discharge date or
day 60

11
Claims Submission
• For RAPs and claims submitted electronically, review the RTP (Return to Provider) file daily, or when received– Timely resubmission needed for RAPs– Errors identified should be tracked and corrected
Copyright 2008 Trinity Health – Novi, Michigan 31
• Repeated errors could result in False Claims Act violation
• Unpaid claims can be reviewed in the Medicare Common Working File to check status
Charge Capture and Billing
• How are services charged? Old method- DAL (daily activities log); most agencies now use EMR with process flow.
• Documentation of services provided• Reconciliation of charges submitted to charges billed
M th d f billi t thi d t
Copyright 2008 Trinity Health – Novi, Michigan 32
• Method of billing to third party payers:– Frequency– Charge entry – Paper or electronic
• Identifying and monitoring of unbilled accounts– Unbilled because Plan of Care not signed?
• Denials
Discontinuation of Medicare Coverage
• Medicare requires 48-hours notification of the client when Medicare Home Care coverage will end– Includes discontinuation due to non-skilled level of care,
lack of homebound status, or exhaustion of benefits– Not required if service ends due to an emergent situation
Copyright 2008 Trinity Health – Novi, Michigan 33
• Notice must include reason for discontinuation, effective date, and appeal process
• Notification should include client signature; proof of attempt to deliver notification when signature not obtainable may be acceptable

12
Copyright 2008 Trinity Health – Novi, Michigan 34
Co-Pays
• As of July 1, 2008 Medicare still does not require a co-pay for traditional Medicare patients for home care services.
• Most Medicare Advantage programs do require a co-pay.
Copyright 2008 Trinity Health – Novi, Michigan 35
p y• Risks:
– Identify need to collect (payer type)– Identify appropriate amount– Obtain co-pay – Write-offs when not obtained (documented proof of
attempt to collect)
Cash Receipts and Collections
• Method of receiving payment- electronic, mail, lockbox, etc
• Receipt Logs security, oversight, and use• Reconciliation of cash receipts and cash deposits• Bank reconciliation
Copyright 2008 Trinity Health – Novi, Michigan 36
• Bank reconciliation• Use of collection agencies• Procedures for charity care and bad debt write-offs• Reserves for doubtful accounts and contractual
write-offs• Discounts applied that are not contractual

13
Accounts Receivable
• Verify credit balances and reconcile to the appropriate ledger
• Compare timeliness of posting RAP and final claim– Investigate if recurring delay in the billing and posting
cycle timeR i i f t i bl b l t
Copyright 2008 Trinity Health – Novi, Michigan 37
• Review aging of accounts receivable balances to verify timely procedures– 40 to 60 Days is preferred range– Percentage older than 120 days should be no greater
than 10% (< 5% preferred)• Percentage of PEP adjustments should be less
than 2%
System Security
• Use of laptops– Electronic access (single use password)
• Location used- client home, caregiver home, agency office
– Physical security • Client home, caregiver home, caregiver vehicle, agency office
Copyright 2008 Trinity Health – Novi, Michigan 38
– System backup• Protected Health Information (PHI)
– Copy of Plan of Care, patient education left in home; who can access it?
• What policy/procedures are in place should there be a breech of privacy/security?
Additional Risks
Some additional areas to consider in auditing:• Background checks for new hires/OIG screening
– Proposed Home Health Aide mandated screening• Software glitches
CMS errors with 5th HIPPS character default to letter (S
Copyright 2008 Trinity Health – Novi, Michigan 39
– CMS errors with 5th HIPPS character- default to letter (S-X) rather than number, which indicates non-routine supplies USED

14
HOME CARE AUDITING
Auditing
Copyright 2008 Trinity Health – Novi, Michigan 40
Cartoon by Dave Harbaugh
Audit
References• CMS Home Care website:
www.cms.hhs.gov/HomeHealthPPS/
• CMS Home Health Agency Center (links to numerous CMS home care-related sites)
http://www.cms.hhs.gov/center/hha.asp
Copyright 2008 Trinity Health – Novi, Michigan 41
p g p
• Medicare Benefit Policy Manual, Publication 100-02, Chapter 7, Home Health Services
www.cms.hhs.gov/manuals/Downloads/bp102c07.pdf
• Medicare Claims Processing Manual, Publication 100-04, Chapter 10, Home Health Agency Billing
www.cms.hhs.gov/manuals/downloads/clm104c10.pdf
References continued
• OASIS Implementation Manual, January 2008
www.cms.hhs.gov/oasis then select User Manual
• Code of Federal Regulations for Home Care-42 CFR Section 484. Table of Contents found at
Copyright 2008 Trinity Health – Novi, Michigan 42
http://www.access.gpo.gov/nara/cfr/waisidx_07/42cfr484_07.html

15
Catherine Niland, RN, BS, CHC, CHCQMOrganizational Integrity Manager, Trinity Health Novi, MI
Copyright 2008 Trinity Health – Novi, Michigan 43

All Episodes
1 2 3 4 5 10 to 4 0 to 6 0 to 2 0 to 8 0 to 7 C15 to 8 7 to 14 3 to 5 9 to 16 8 to 14 C2
9+ 15+ 6+ 17+ 15+ C30 to 5 0 to 6 0 to 8 0 to 7 0 to 6 F1
6 7 9 8 7 F27+ 8+ 10+ 9+ 8+ F3
6 16 to 17 6 16 to 17 S27 to 9 18 to 19 7 to 9 18 to 19 S3
10 10 S411 to 13 11 to 13 S5
NRS-1 S 1NRS-2 T 2NRS-3 U 3NRS-4 V 4NRS-5 W 5NRS-6 X 6
515 to 2728 to 48
NRS Points
99+
NRS-Supplies Severity Level: (by NRS point scores-
Pseudocode Appendix Table 7)
Medicare Home Care PPS HIPPS Code Calculation for Episodes Starting 1/1/08 or later1/28/2008
NRS provided
H
K
01 to 14
no NRS provided
NP
Enter this value:(grouping step): 1 to 5
ABCFG
Clinical Severity Level: (by point scores- Pseudocode
Appendix Table 5)Functional Severity Level:
(by point scores- Pseudocode Appendix Table 5)
Services Utilization Level: (by number of therapy visits)
20+ (one group)
S1
2
3
4LM
14 to 19 therapy visits
0 to 13 therapy visits
0 to 5 14 to 15 0 to 5 14 to 15
14 to 19 therapy visits
20+ therapy visits
HIPPS Code
For this level
In HIPPS position:
49 to 98
Definitions of Severity Levels by Grouping Step:1st & 2nd Episodes 3rd+ Episodes0 to 13 therapy visits

(1) (2) (3)ROW VARIABLE DESCRIPTION Points
1 Primary diagnosis = Anal fissure, fistula and abscess 152 Other diagnosis = Anal fissure, fistula and abscess 133 Primary diagnosis = Cellulitis and abscess 144 Other diagnosis = Cellulitis and abscess 85 Primary diagnosis = Diabetic ulcers [* SEE NOTE] 206 Primary diagnosis = Gangrene 117 Other diagnosis = Gangrene 88 Primary diagnosis = Malignant neoplasms of skin 159 Other diagnosis = Malignant neoplasms of skin 4
10 Primary or Other diagnosis = Non-pressure and non-stasis ulcers[* SEE NOTE] 1311 Primary diagnosis = Other infections of skin and subcutaneous tissue 1612 Other diagnosis = Other infections of skin and subcutaneous tissue 713 Primary diagnosis = Post-operative Complications 2314 Other diagnosis = Post-operative Complications 1515 Primary diagnosis = Traumatic Wounds and Burns 1916 Other diagnosis = Traumatic Wounds and Burns 817 Primary or other diagnosis = V code, Cystostomy care 1618 Primary or other diagnosis = V code, Tracheostomy care 2319 Primary or other diagnosis = V code, Urostomy care 2420 OASIS M0450 = 1 or 2 pressure ulcers, stage 1 421 OASIS M0450 = 3+ pressure ulcers, stage 1 622 OASIS M0450 = 1 pressure ulcer, stage 2 1423 OASIS M0450 = 2 pressure ulcers, stage 2 2224 OASIS M0450 = 3 pressure ulcers, stage 2 2925 OASIS M0450 = 4+ pressure ulcers, stage 2 3526 OASIS M0450 = 1 pressure ulcer, stage 3 2927 OASIS M0450 = 2 pressure ulcers, stage 3 4128 OASIS M0450 = 3 pressure ulcers, stage 3 4629 OASIS M0450 = 4+ pressure ulcers, stage 3 5830 OASIS M0450 = 1 pressure ulcer, stage 4 4831 OASIS M0450 = 2 pressure ulcers, stage 4 6732 OASIS M0450 = 3+ pressure ulcers, stage 4 7533 OASIS M0450e = 1(unobserved pressure ulcer(s)) 1734 OASIS M0470 = 2 (2 stasis ulcers) 635 OASIS M0470 = 3 (3 stasis ulcers) 1236 OASIS M0470 = 4 (4+ stasis ulcers) 2137 OASIS M0474 = 1 (unobservable stasis ulcers) 938 OASIS M0476 = 1 (status of most problematic stasis ulcer: fully granulating) 639 OASIS M0476 = 2 (status of most problematic stasis ulcer: early/partial granulation) 2540 OASIS M0476 = 3 (status of most problematic stasis ulcer: not healing) 3641 OASIS M0488 = 2 (status of most problematic surgical wound: early/partial granulation) 442 OASIS M0488 = 3 (status of most problematic surgical wound: not healing) 14
43 OASIS M0550=1(ostomy not related to inpt stay/no regimen change) 2744 OASIS M0550=2 (ostomy related to inpt stay/regimen change) 4545 Any `Selected Skin Conditions` (rows 1-42 above) AND M0550=1(ostomy not related to inpt stay/no regimen change) 14
46 Any `Selected Skin Conditions` (rows 1-42 above) AND M0550=2(ostomy related to inpt stay/ regimen change) 1147 OASIS M0250 (Therapy at home) =1 (IV/Infusion) 548 OASIS M0520 = 2 (patient requires urinary catheter) 949 OASIS M0540 = 4 or 5 (bowel incontinence, daily or >daily) 10
HHA PPS Grouper 0202 Logic January 28, 2008 Pseudocode APPENDIX TABLES
NOTE:* If episode receives points for diabetic ulcers, it cannot also receive points for “Non-pressure and non-stasis ulcers.”
Table 7: Nonroutine Medical Supplies (NRS): Case-Mix Adjustment Variables and Point Scores(Table taken from Table 10A of Final Rule CMS-1541-FC)
SELECTED SKIN CONDITIONS:
OTHER CLINICAL FACTORS:
Abt Associates Inc.Questions: <[email protected]> 1 Table 7 NRS Casemx Adj Variabls