Embed Size (px)
Citation preview

Dyspnea: The top things you
need to you know!
Dr. Megan Sellick & Dr. Lawrence Lee
Edmonton Zone Palliative Care Program
Faculty / Presenter Disclosure
• Faculty: Dr. Lawrence Lee
• Relationships with commercial interests:
• Grants/Research Support: none
• Speakers Bureau/Honoraria: none
• Consulting Fees: none
• Other: none
Faculty / Presenter Disclosure
• Faculty: Dr. Megan Sellick
• Relationships with commercial interests:
• Grants/Research Support: none
• Speakers Bureau/Honoraria: none
• Consulting Fees: none
• Other: none
Disclosure of Commercial
Support
• This program has received financial support
from: none
• This program has received in-kind support
from: none
Objectives
By the end of our time together, you will be able to :
• Recognize the subjective nature of dyspnea
• Provide an initial management plan for dyspnea
(non-pharmacological and pharmacological)
• Briefly describe “palliative sedation” and describe the medication
used
Dyspnea
This man has metastatic lung cancer.
Which of the following is the best
measure of his dyspnea?
A- respiratory rate
B- use of accessory breathing muscles
C- oxygen requirements
D- oxygen saturations
E- all of the above
F- none of the above (patient’s report is
best)
Dyspnea
Definition:
“feeling like one cannot breathe well enough”
American Thoracic Society:
“a subjective experience of breathing discomfort that
consists of qualitatively distinct sensations that vary in
intensity.”
Dyspnea
Overall Management Approach:
Screen+Assess
Identify Cause(s)
Management
Underlying Cause
Symptoms
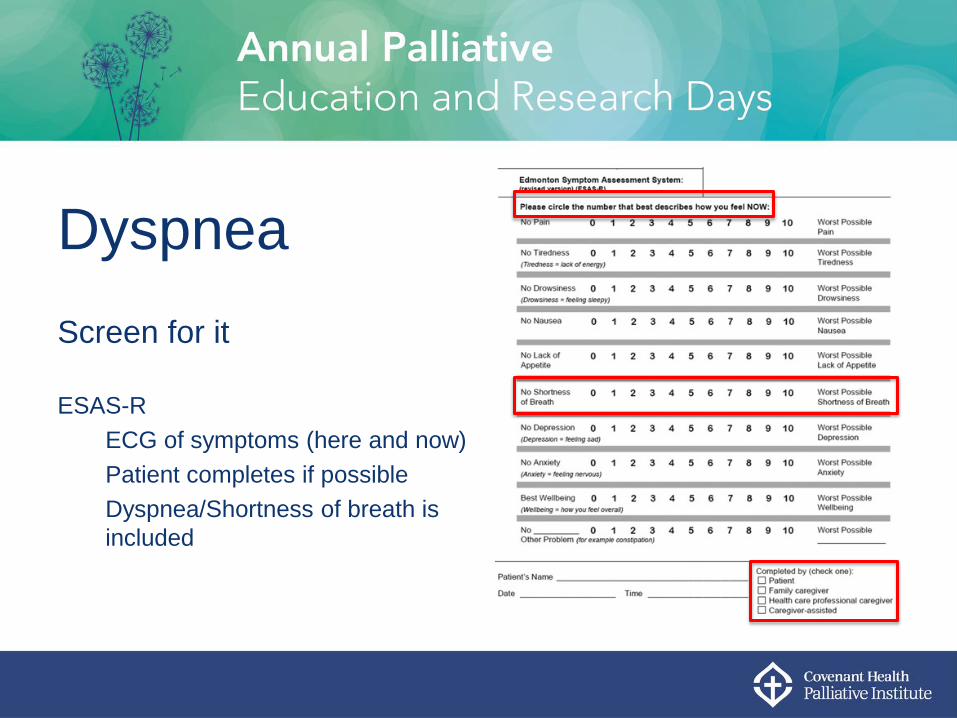
Dyspnea
Screen for it
ESAS-R
ECG of symptoms (here and now)
Patient completes if possible
Dyspnea/Shortness of breath is
included
Dyspnea
Assessment:
History
Duration
Onset
Pattern
Severity: Rest vs Exertion
Triggers/Alleviating Factors
Physical Examination
Dyspnea
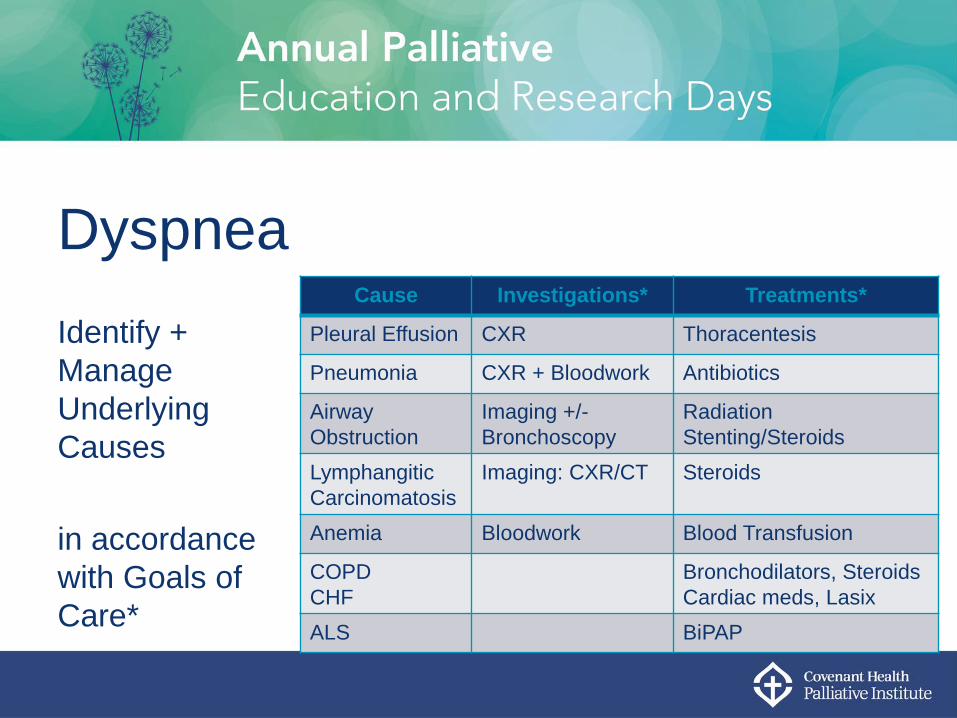
Identify +
Manage
Underlying
Causes
in accordance
with Goals of
Care*
Cause Investigations* Treatments*
Pleural Effusion CXR Thoracentesis
Pneumonia CXR + Bloodwork Antibiotics
Airway
Obstruction
Imaging +/-
Bronchoscopy
Radiation
Stenting/Steroids
Lymphangitic
Carcinomatosis
Imaging: CXR/CT Steroids
Anemia Bloodwork Blood Transfusion
COPD
CHF
Bronchodilators, Steroids
Cardiac meds, Lasix
ALS BiPAP
Dyspnea
Symptomatic Management: Non-Pharmacological
Fan
Position: leaning forward, head up
Avoid irritants
Avoid exacerbating activities: mobilization, transfers, constipation
Dyspnea
*Symptomatic Management: Pharmacological
Oxygen
Opioids
Other Therapies
Dyspnea
Symptomatic Management: Oxygen
Useful for patients with hypoxia
Use cautiously in patients with severe COPD (ie. CO2 retainers)
Role in non-hypoxic patients less clear: some may still benefit
Not clear whether it is the oxygen or the airflow that is helpful
Dyspnea
Symptomatic Management: Oxygen
When used for comfort, oxygen should be titrated to:
A-Improved Oxygen Saturations (ie. O2>95%)
B-Reduce Tachypnea (ie. Decrease respiratory rate)
C-Decrease Work of Breathing
D-All of the Above
E-None of the above (titrate to decrease pt’s sensation of dyspnea)
Dyspnea
Symptomatic Management: Oxygen
When using O2 for comfort:
No need to start if the patient is not complaining of dyspnea
No need to continue measuring oxygen saturations at end of life
Increase O2 around periods when patient has more dyspnea (ie. Could increase on
exertion)
Dyspnea
Symptomatic Management: Opioids
Which is the following is true regarding the use of opioids for dyspnea:
A- They block lung opioid receptors to decrease the sensation of dyspnea
B- Opioids diminish the sensation of being short of breath in the brain
C- They reduce the respiratory rate and allow the patient to rest
D- All of the above
E- None of the above
Dyspnea
Symptomatic Management: Opioids
Opioids are safe and effective for dyspnea
When you “start low and go slow”, low risk of respiratory depression
Similar to cancer pain, they can be provided ATC + PRN
(ie. Morphine 2.5 mg PO q6h + q1h PRN for shortness of breath)
Diminish the sensation of dyspnea in the brain
Nebulized opioids do not show significant benefit
Dyspnea
Symptomatic Management: Anxiolytics
Anti-psychotics: helpful in managing dyspnea-related anxiety
Haldol 1 mg PO/SC q12h-q4h ATC + q1h PRN
Olanzapine 2.5-5 mg PO/Zydis q12h-q4h ATC + q1h PRN
Nozinan 6.25-25 mg PO/SC q12h-q4h ATC + q1h PRN
Dyspnea
Palliative Sedation • Process of inducing/maintaining deep and permanent sleep in order to relieve
refractory symptoms in palliative pts who are close to death.
NOT EUTHANASIA
• Most common indications: delirium, dyspnea
• ?Risk of hastening death → No evidence!
• Midazolam: Benzodiazepine with short t1/2 easily titratable by SC infusion
Dyspnea
Palliative Sedation: Communicating with Family • Discuss proactively
• Review understanding of illness/prognosis, goals of care
• Sedation used only if symptoms refractory to all other measures
• Patient will lose ability to communicate
• Usually irreversible, with death from underlying illness occurring within days
Dyspnea
Take Home Messages • Dyspnea is what the patient self-reports
• Screen for dyspnea
• Determine and treat underlying causes when possible/appropriate
• Use oxygen if it helps and titrate it to comfort, not oxygen saturations
• Opioids are safe and effective for symptomatic management of dyspnea
• Treat the anxiety component of dyspnea if it is present
• Palliative sedation is available for intractable dyspnea