Embed Size (px)
Citation preview
5/18/2016
1
©2012 M FM ER | s lide-1
Left Atrial Closure, Indications & Options
Dav id R. Holmes, Jr., M.D.
Mayo Clinic, Rochester
Oregon Cardiov ascular SymposiumPortland, OR
May 2016
©2012 M FM ER | s lide-2
Presenter Disclosure Information
David R. Holmes, Jr., M.D.
“Left Atrial Closure, Indications & Options”
The following relationships exist related to this presentation:
Both Mayo Clinic and I hav e a financial interest in
technology related to this research. That technology
has been licensed to Boston Scientific.
©2016 M FM ER | 3530051-3
Worldwide Prevalenceof Atrial Fibrillation
5/18/2016
2
©2016 M FM ER | 3530051-4
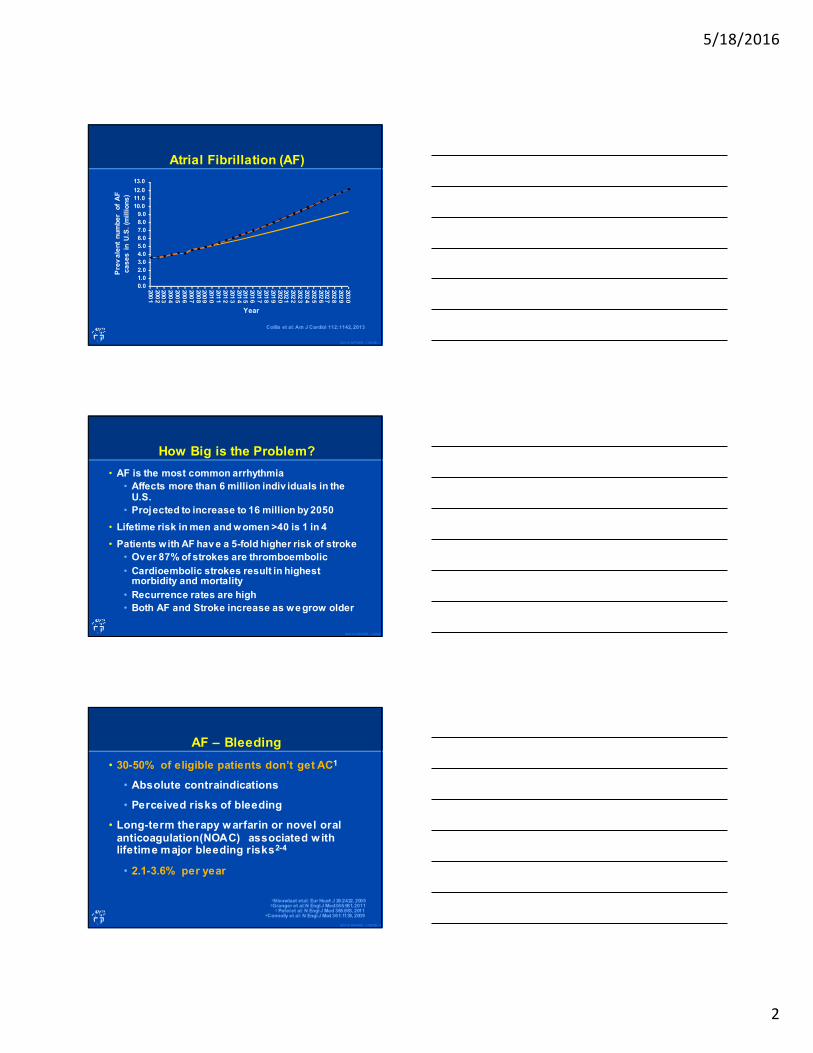
Atrial Fibrillation (AF)
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
9.0
10.0
11.0
12.0
13.0
200
1200
2200
3200
4200
5200
6200
7200
8200
9201
0201
1201
2201
3201
4201
5201
6201
7201
8201
9202
0202
1202
2202
3202
4202
5202
6202
7202
8202
9203
0
Colilla et al: Am J Cardiol 112:1142, 2013
Pre
va
len
t n
um
be
r o
f A
F
ca
se
s i
n U
.S.
(mil
lio
ns
)
Year
©2012 M FM ER | s lide-5
How Big is the Problem?
• AF is the most common arrhythmia
• Affects more than 6 million indiv iduals in the U.S.
• Projected to increase to 16 million by 2050
• Lifetime risk in men and women >40 is 1 in 4
• Patients with AF hav e a 5-fold higher risk of stroke
• Ov er 87% of strokes are thromboembolic
• Cardioembolic strokes result in highest morbidity and mortality
• Recurrence rates are high
• Both AF and Stroke increase as we grow older
©2016 M FM ER | 3530051-6
AF – Bleeding
• 30-50% of eligible patients don’t get AC1
• Absolute contraindications
• Perceived risks of bleeding
• Long-term therapy warfarin or novel oral
anticoagulation(NOAC) associated w ith lifetime major bleeding risks2-4
• 2.1-3.6% per year
1Nieuwlaat et al: Eur Heart J 26:2422, 20052Granger et al: N EnglJ Med 365:981, 2011
3 Patel et al: N EnglJ Med 365:883, 20114Connolly et al: N EnglJ Med 361:1139, 2009
5/18/2016
3
©2016 M FM ER | 3530051-7
AF – AC
• Other concerns and contraindications with OAC include:1-2
• Patients with renal and liver dysfunctions (for NOAC)
• High risk of falls
• Noncompliance
• Those requiring dual antiplatelet therapy after stenting
• For warfarin:
• Additional issues with drug and diet interaction
• Need for monitoring
• Narrow therapeutic window with time in therapeutic range of only 50% to 60%
1Holbrook et al: Arch Intern Med 165: 1095, 20052Gersh et al: Rev Esp Cardiol 64:260, 2011
©2012 M FM ER | s lide-8
NOACS versus WarfarinMeta-Analysis
• Prespecified meta-analysis of 71,683 patients
• RE-LY, ROCKET AF, ARISTOTLE, ENGAGE,
AF-TIMI 48
• Main outcomes
• Stroke and systemic embolism
• Ischemic stroke, hemorrhagic stroke
• All cause mortality, MI
• Major bleeding, ICH, GI bleeding
Ruff et al: Lancet 383:955-62, 2014
©2012 M FM ER | s lide-9
NOACS versus Warfarin
• NOACS:
• Significant ↓ in all cause mortality
• RR 0.90, 95% CI 0.85-0.95
• Significant ↓ in ICH
• RR 0.48, 95% CI 0.39-0.59
• Significant ↑ in GI bleeding
• RR 1.25, 95% CI 1.01-1.55
Ruff et al: Lancet 383:955-62, 2014
5/18/2016
4
©2012 M FM ER | s lide-10
Novel Oral Anticoagulants Discontinuation and Bleeding Rates
TreatmentDiscontinuation
rate in study (%)
Major bleeding
(rate/year) (%)
Dabigatran1 (150 mg) 21 3.1
Rivaroxaban2 24 3.6
Apixaban3 22 2.1
1. Connolly SJ: N Engl J Med, 2009
2. Patel MR: N Engl J Med, 20113. Granger CB: N EnglJ Med, 2011
©2012 M FM ER | s lide-11
Intracerebral Hemorrhage and NOACs
• Multicenter observation German study
• 38 stroke units 2012-2014
• 61 consecutive patients w ith non-traumatic NOAC associated ICH
• 45 (74%) qualified for hematoma expansion analysis
Purrucker et al: JAMA Neurol, 2015
©2012 M FM ER | s lide-12
Intracerebral Hemorrhage and NOACsPerspective
• Hematoma volume and location at baseline similar to those associated w ith VKA
• Intraventricular hematoma extension similar to VKA (38% NOAC, 36-56% VKA)
Purrucker et al: JAMA Neurol, 2015
5/18/2016
5
©2012 M FM ER | s lide-13
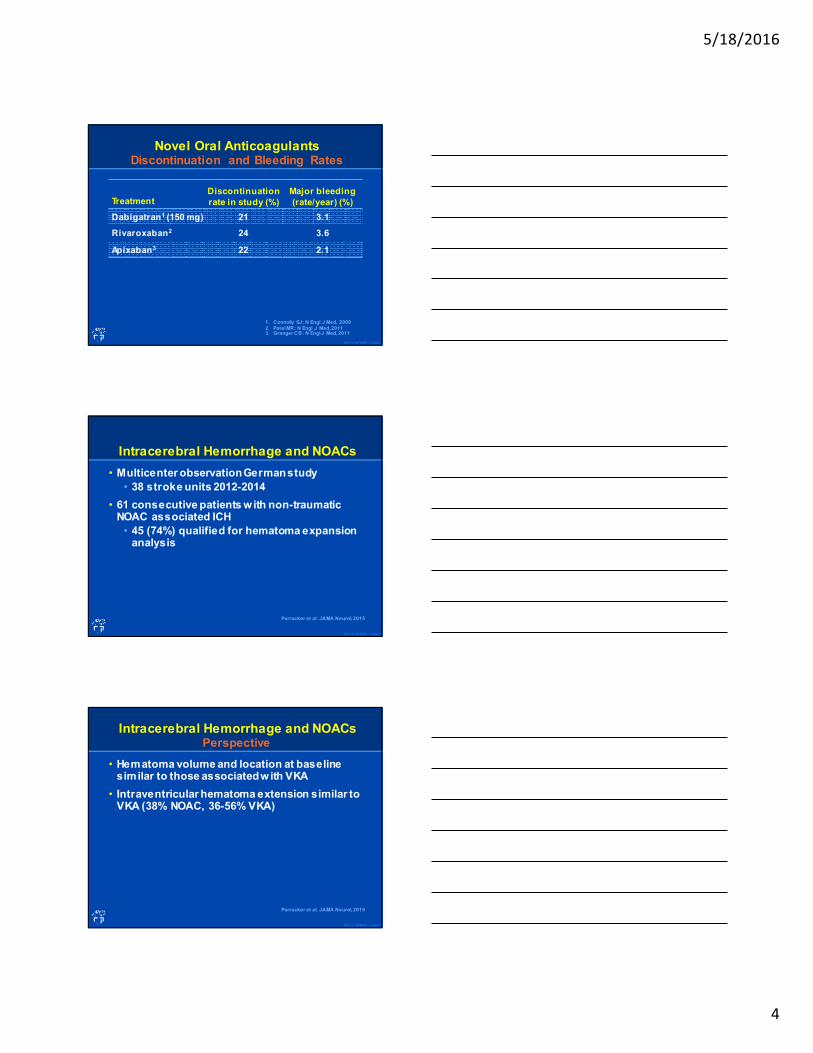
Location of Thrombi in Left Atrium
0 20 40 60 80 100
Stoddard: JACC, 1995
Manning: Circ, 1994
Aberg: Acta Med Scan, 1969
Tsai: JFMA, 1990
Klein: Int J Card Imag, 1993
Manning: Circ, 1994
Klein: Circ, 1994
Leurig: JACC, 1994
Hart: St roke, 1994
Total
Blackshear et al: Ann Thoracic Surg 61, 1996
Location frequency (% )
Left atrial appendage Left atrium
91% in LAA
©2012 M FM ER | s lide-14
Disappearing LAA Thrombus Resulting in Stroke
Pa
rek
h A
, E
zek
ow
itz
M e
t a
l: C
irc
114
:e51
3, 2
006
©2012 M FM ER | s lide-15
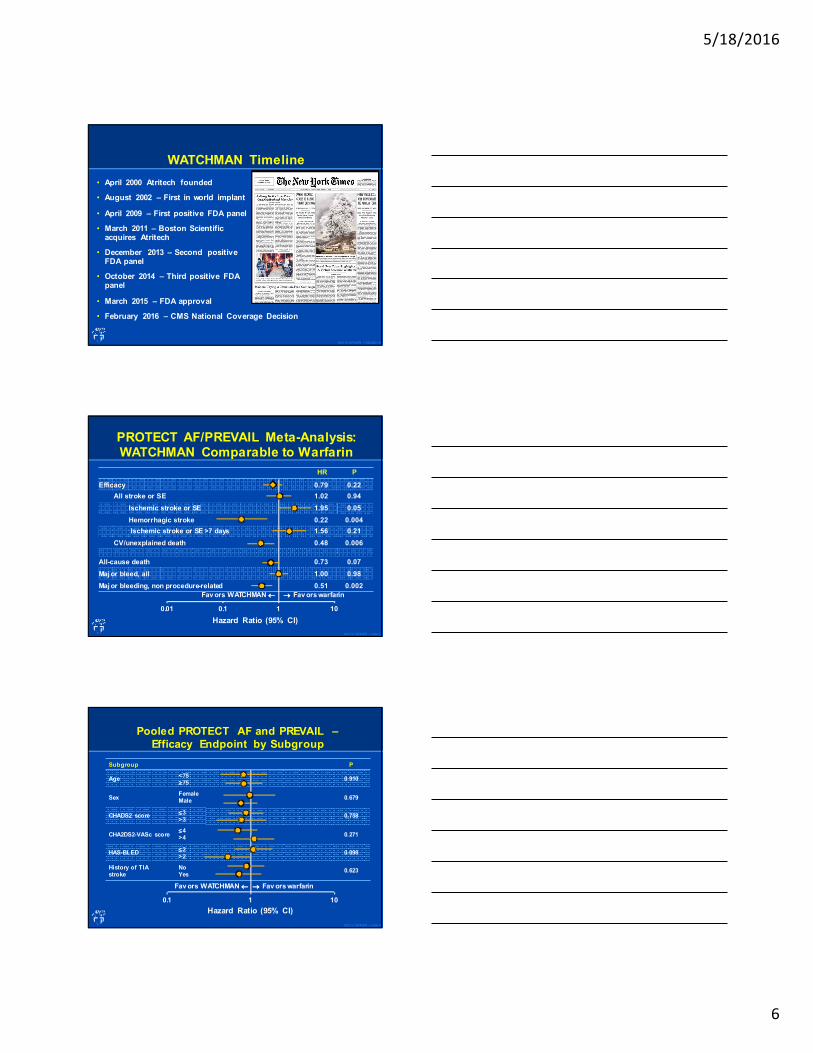
LAA Closure for Stroke Prevention in Non-Valvular AF
Bergmann MW et al: EuroIntervention 2014;10:497-504
5/18/2016
6
©2016 M FM ER | 3522200-16
WATCHMAN Timeline
• April 2000 Atritech founded
• August 2002 – First in world implant
• April 2009 – First positive FDA panel
• March 2011 – Boston Scientific acquires Atritech
• December 2013 – Second positive FDA panel
• October 2014 – Third positive FDA panel
• March 2015 – FDA approval
• February 2016 – CMS National Coverage Decision
©2012 M FM ER | s lide-17
PROTECT AF/PREVAIL Meta-Analysis: WATCHMAN Comparable to Warfarin
HR P
Efficacy 0.79 0.22
All stroke or SE 1.02 0.94
Ischemic stroke or SE 1.95 0.05
Hemorrhagic stroke 0.22 0.004
Ischemic stroke or SE >7 days 1.56 0.21
CV/unexplained death 0.48 0.006
All-cause death 0.73 0.07
Maj or bleed, all 1.00 0.98
Maj or bleeding, non procedure-related 0.51 0.002
0.01 0.1 1 10
Hazard Ratio (95% CI)
Fav ors WATCHMAN ←←←← →→→→ Fav ors warfarin
©2012 M FM ER | s lide-18
Subgroup P
Age<75≥≥≥≥75
0.910
SexFemaleMale
0.679
CHADS2 score≤≤≤≤3>3
0.758
CHA2DS2-VASc score≤≤≤≤4>4
0.271
HAS-BLED≤≤≤≤2>2
0.098
History of TIAstroke
NoYes
0.623
0.1 1 10
Pooled PROTECT AF and PREVAIL –
Efficacy Endpoint by Subgroup
Hazard Ratio (95% CI)
→→→→ Fav ors warfarinFav ors WATCHMAN ←←←←
5/18/2016
7
©2012 M FM ER | s lide-19
Conclusions: In patients with NVAF at increased risk
for stroke or bleeding who are candidates for chronic
anticoagulation, LAAC resulted in improv ed rates of
hemorrhagic stroke, cardiov ascular/unexplaine d death,
and nonprocedural bleeding compared to warfarin.
©2012 M FM ER | s lide-20
Left Atrial Appendage Closure What Have We Learned
• The hypothesis that in patients w ith
nonvalvular atrial fibrillation that stroke results from LAA thrombus is correct
• Benefit of LAA occlusion remains stable
• >90% of patients can be taken off of warfarin w ithout harm and some patients
may never need warfarin at all if they
receive a device
• There is a learning curve, the more you do,
the better you are at doing it
©2012 M FM ER | s lide-21
Stroke and Atrial FibrillationAlternative to Warfarin or NOACS
• Patients who could be treated with warfarin/NOACS
• Patients who choose not to be treated with warfarin/NOACS
• Contraindications to warfarin/NOACS
• In concert with ablation
5/18/2016
8
©2015 M FM ER | 3455847-22
Indications for Use
The WATCHMAN Device is indicated to reduce the risk
of thromboembolism from the left atrial appendage in patients with non-valvular atrial fibrillation who:
• Are at increased risk for stroke and systemic
embolism based on CHADS2 or CHA2DS2-VASc scores and are recommended for anticoagulation therapy;
• Are deemed by their physicians to be suitable for
warfarin; and
• Have an appropriate rationale to seek a non-pharmacologic alternative to warfarin, taking into
account the safety and effectiveness of the device compared to warfarin
©2012 M FM ER | s lide-23
Individual Institutional
LAA Occlusion Program
Components
©2012 M FM ER | s lide-24
• FDA = Approval
• FDA = IFU
• FDA ≠ CMS approval for reimbursement
• CMA approval ≠ FDA IFU
• Corrected CMS = Reimbursement (sort of)
5/18/2016
9
©2012 M FM ER | s lide-25
LAACRegistry Components
• The patient is enrolled in, and the MDT and hospital must participate in a prospective, national, audited registry that 1) consecutively enrolls LAAC patients and 2) tracks the following annual outcomes for each patients for a period of at least four years from the time of the LAAC:
• Operator-specific complications
• Device-specific complications including device thrombosis
• Stroke, adjudicated, by type
• Transient ischemic attack (TIA)
• Systemic embolism
• Death
• Major bleeding, by site and severity
©2016 M FM ER | 3522200-26
NCDR LAAC Registry
SCAI/ACC/HRS Institutional and Operator
Requirements for Left Atrial Appendage Occlusion
“The writing committee strongly believes that participation in anational registry should be mandatory for all LAA occlusion programs.”
http://www.scai.org/Assets/e6b13791-37bc-4c6c-88ebe5348dca2ed4/
635852762599830000/scai-2015-12-10-laacrequirements-pdf
http://cvquality.acc.org/NCDR-Home/Registries/Hospital-Registries.aspx
©2016 M FM ER | 3522200-27
US Reimbursement StatusCMS National Coverage Decision (2/8/16)
Criteria for coverage
• CHADS2 score ≥≥≥≥2 or CHA2DS2-VAScscore ≥≥≥≥3
• A formal shared decision making interaction w ith an independent noninterventionalphysician using an evidence-based decision tool on oral anticoagulation in patientswith NVAF
• Suitable for short-term warfarin but deemed unable to take long term oral anticoagulation
5/18/2016
10
©2016 M FM ER | 3522200-28
US Reimbursement StatusCMS National Coverage Decision (cont)
• Implanted in a hospital with an established structural heart disease and/or electrophysiology program and performed by an interventional cardiologist, electrophysiologstor cardiovascular surgeon meeting the following criteria
• Has received training prescribed by the manufacturer on the safe and effective use of the device prior to performing LAAC
• Has performed ≥≥≥≥25 interventional cardiac procedures that involve transseptal puncture through an intact septum
• Continues to perform ≥≥≥≥25 interventional cardiac procedures that involve transseptal puncture throughan intact septum, of which at least 12 are LAAC, overa 2-year period
©2012 M FM ER | s lide-29
LAACRegistry Components
• The patient is enrolled in, and the MDT and hospital must participate in a prospective, national, audited registry that 1) consecutively enrolls LAAC patients and 2) tracks the following annual outcomes for each patients for a period of at least four years from the time of the LAAC:
• Operator-specific complications
• Device-specific complications including device thrombosis
• Stroke, adjudicated, by type
• Transient ischemic attack (TIA)
• Systemic embolism
• Death
• Major bleeding, by site and severity
©2012 M FM ER | s lide-30
• The Centers for Medicare & Medicaid Services (CMS) covers percutaneous left atrial appendage closure (LAAC) for non-valvular atrial fibrillation (NVAF) through Coverage with Evidence Development (CED) under 1862(a)(1)(E) of the Social Security Act with the following conditions:
• LAA closure devices are covered when the device has received Food & Drug Administration (FDA) Premarket Approval (PMA) for that device’s FDA-approved indication and meet all of the conditions specified below:
• CHADS2 – ≥2
• CHADS2DS2-VASc – ≥3
• Shared decision making with independent non-interventional MD
• Suitable for short-term AC but deemed unable or unsuitable for long-term
• Trained physicians
• Enrolled in a registry
5/18/2016
11
©2012 M FM ER | s lide-31
Background
• LAAO with Watchman Dev ice was approved by FDA in 2015 based on PROTECT AF and PREVAIL RCT’s and companion Registries
• Dev elopment of PMS Registry a condition of approv al planned to begin enrollment 2nd quarter 2016
• Between approv al but before PMS study, commercial cases continued and were entered into a procedural data base by Watchman clinical specialists using standardized forms
©2012 M FM ER | s lide-32
Study Objective & Timeline
2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
PROTECT AF N=800
CAP1 N=566
PREVAIL N=463
CAP2 N=463
EWOLUTION
N=1025
Commer-
cial
N=1683
PROTECT AF
59 Centers449 Procedures
CAP1
26 Centers566 Procedures
PREVAIL
41 Centers50 Operators (24 New)
265 Procedures
CAP2
47 Centers
579 Procedures
EWOLUTION
47 Centers
1019 Procedures
Commercial
47 Centers1683 Procedures
• Assess procedural performance in commercial cases performed after FDA approval but before PMS study
• Compare procedural performance with pre FDA approval data obtained in PROTECT AF, PREVAIL RCT’s ,companion Registries (CAP1 and CAP 2) and Ewolution Registry
©2012 M FM ER | s lide-33
Materials and Methods
• Watchman dev ice: self expanding nickel titanium structure ranging in diameter from 21-33 mm, cov ered on left atrial surface by permeable fabric cov er and anchored at the LAA ostium
• IFU for FDA approv al identified patient selection criteria to include
• High risk for stroke
• Increased risk for bleeding
• Able to take short term anticoagulation
• Not felt to be a good candidate for long termanticoagulation
5/18/2016
12
©2012 M FM ER | s lide-34
Patient Recruitment andProcedural Performance
• 1,683 consecutive patients undergoing clinically indicated Watchman placement accordingly to FDA IFU selection criteria
• Informed site consent in each patient
• Procedures performed by physicians trained in LAAO
• Trained experienced Watchman clinical specialists in attendance in each case
• Details of each procedure recorded on standardized forms
©2012 M FM ER | s lide-35
Procedural Performance Details
• Anatomic LAA size and shape
• Specific guide catheter for LAA intubation
• Device size
• Number of devices used and percentage of recapture attempts
• Procedural success and device release
• Operator assessed residual leak
• Procedural duration
©2012 M FM ER | s lide-36
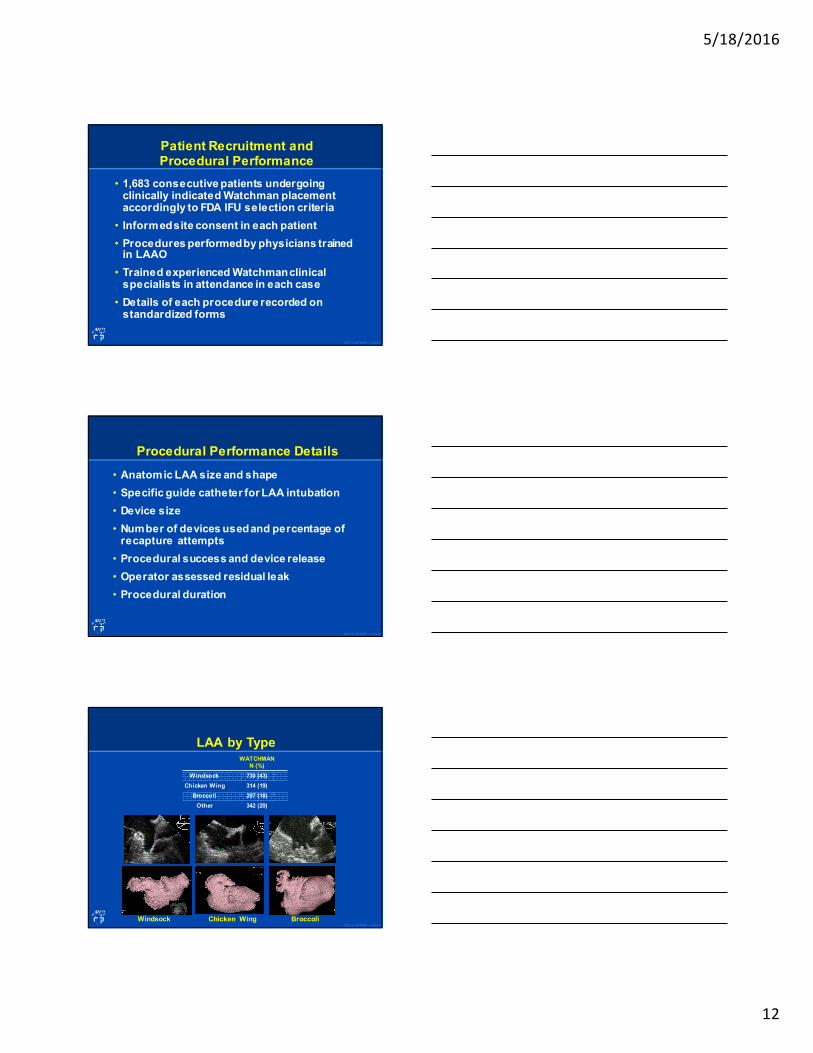
LAA by TypeWATCHMAN
N (%)
Windsock 730 (43)
Chicken Wing 314 (19)
Broccoli 297 (18)
Other 342 (20)
Windsock Chicken Wing Broccoli
5/18/2016
13
©2012 M FM ER | s lide-37
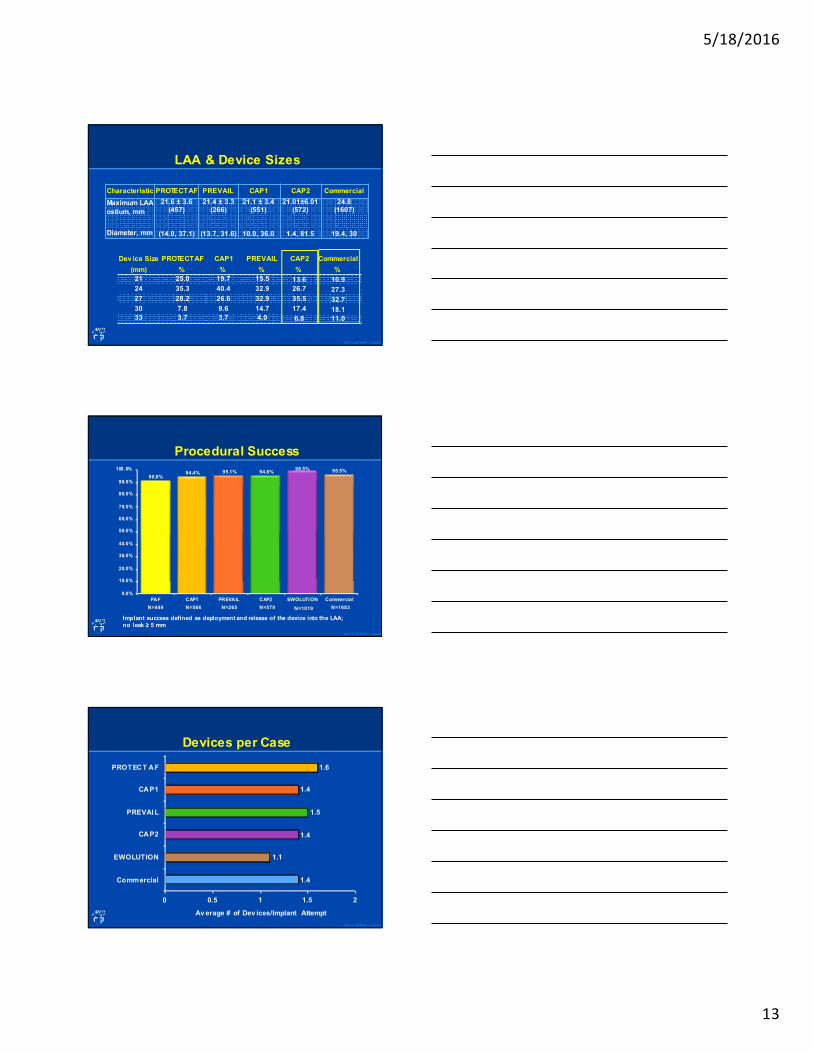
LAA & Device Sizes
Characteristic PROTECT AF PREVAIL CAP1 CAP2 Commercial
Maximum LAA
ostium, mm
Diameter, mm
21.6 ± 3.6(457)
(14.0, 37.1)
21.4 ± 3.3(266)
(13.7, 31.6)
21.1 ± 3.4(551)
10.0, 36.0
21.01±6.01 (572)
1.4, 81.5
24.8 (1607)
19.4, 30
Dev ice Size
(mm)
PROTECTAF
%
CAP1
%
PREVAIL
%
CAP2
%
Commercial
%
21 25.0 19.7 15.5 13.6 10.9
24 35.3 40.4 32.9 26.7 27.3
27 28.2 26.6 32.9 35.5 32.7
30 7.8 9.6 14.7 17.4 18.133 3.7 3.7 4.0 6.8 11.0
©2012 M FM ER | s lide-38
Procedural Success
90.9%94.4% 95.1% 94.8%
98.5% 95.5%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
PAF CAP1 PREVAIL CAP2 EWOLUTION Commercial
N=449 N=566 N=265 N=579 N=1019 N=1683
Implant success defined as deployment and release of the device into the LAA; no leak ≥ 5 mm
©2012 M FM ER | s lide-39
Devices per Case
1.4
1.1
1.4
1.5
1.4
1.6
0 0.5 1 1.5 2
Commercial
EWOLUTION
CAP2
PREVAI L
CAP1
PROTECT AF
Av erage # of Dev ices/Implant Attempt
5/18/2016
14
©2012 M FM ER | s lide-40
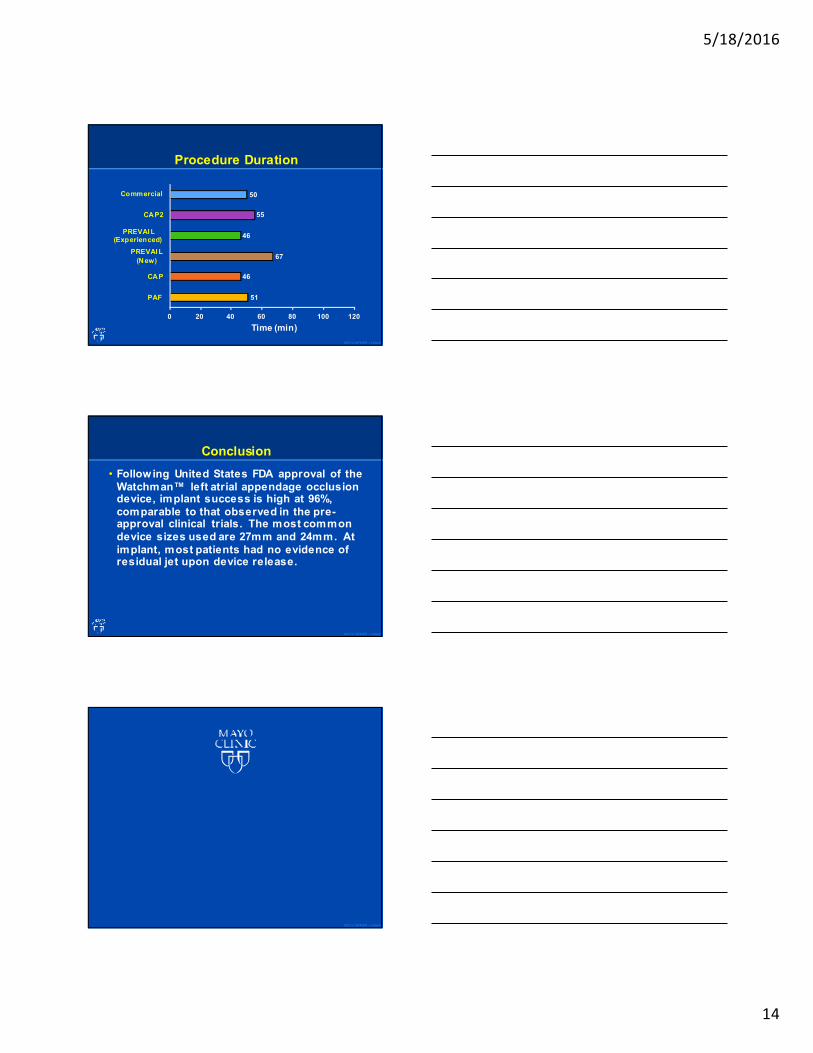
Procedure Duration
51
46
67
46
55
50
0 20 40 60 80 100 120
PAF
CAP
PREVAI L
(New)
PREVAI L(Experienced)
CAP2
Commercial
Time (min)
©2012 M FM ER | s lide-41
Conclusion
• Following United States FDA approval of the
Watchman™ left atrial appendage occlusion device, implant success is high at 96%,
comparable to that observed in the pre-approval clinical trials. The most common
device sizes used are 27mm and 24mm. At
implant, most patients had no evidence of residual jet upon device release.
©2012 M FM ER | s lide-42