Embed Size (px)
Citation preview

HKU leads the Asia's first genetically
modified hematopoietic stem cell
transplantation for late juvenile
metachromatic leukodystrophy patient
(MLD)
Press Conference
May 20, 2015 1

Speakers
Dr Lian Qizhou
Assistant Professor
Department of Ophthalmology & Department of Medicine
Li Ka Shing Faculty of Medicine, HKU
Professor Zhuo Jiacai
Clinical Professor and Head of Division of Hematology
The Second People’s Hospital of Shenzhen
(The First Affiliated Hospital of Shenzhen University)
2

Courtesy from Dr Guili Nadinin
MLD is a devastating
lysosomal storage disease
3

The Prevalence of MLD
Three Types of MLD observed
1.Infant Onset(Age 0-2, 50-60%)
-Early Infant (< Age 1 ) -Late Infant (Age 1-2)
2.Juvenile Onset (Age 2-16, 30-40%)
-Early Juvenile (Age 2-6 ) -Late Juvenile (Age 6-16)
3.Adult Onset(>Age 16, ~5-10%)
Prevalence of MLD globally: 1.4–1.8 per 100,000 live births.
And there is 1,900 new MLD cases every year.
-Global: around 41,000 alive patients
-Mainland China: above 10,000 alive patients
-Hong Kong: estimated 40-50 alive patients
4

No cure for MLD at Present
--Management of most MLD patients: Supportive care
--Developing new technology for MLD:
1.Hematopoietic stem cell transplantation (HSCT):
Bone marrow hematopoietic stem cell, Cord blood hematopoietic stem cell. Uncertain
outcome, confirmed ineffective in late infant onset
2. Enzyme replacement therapy (ERT)
Supply functional ARSA enzyme : high molecular weight protein, hard to pass the
blood–brain barrier (BBB),limited effects
3.Genetically modified hematopoietic stem cell
transplantation(HSCGT): Lentiviral-mediated ARSA overexpression in autologous HSC following re-infusion
5
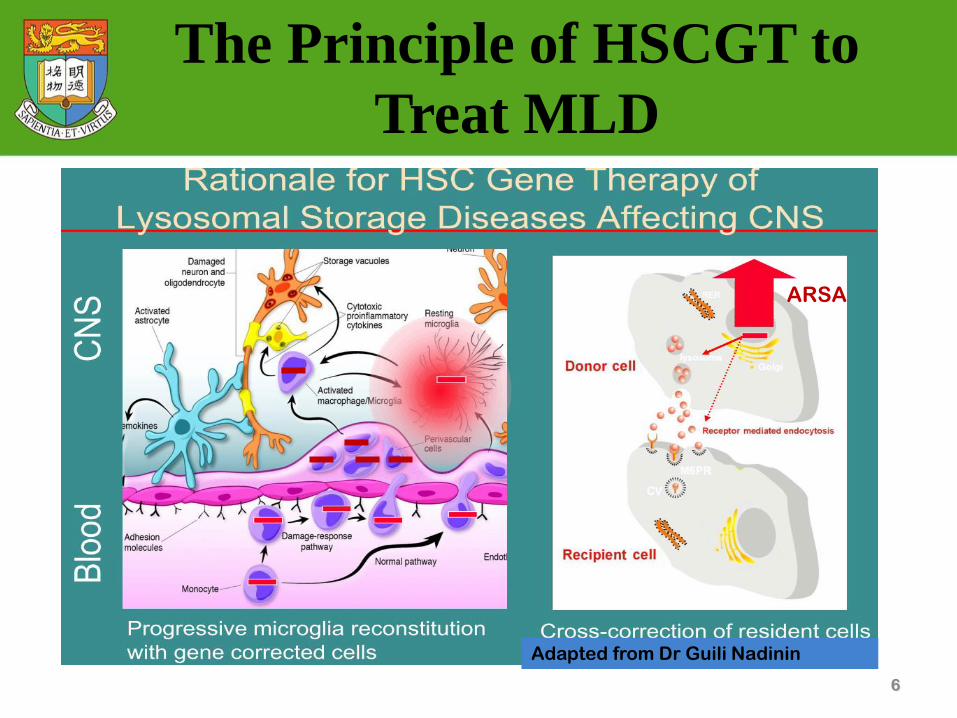
The Principle of HSCGT to
Treat MLD
6
Adapted from Dr Guili Nadinin
ARSA

Advantages of HSCGT for MLD
• Correction of Gene dysfunction in HSC
Expressing high level of functional ARSA; Lentiviral-mediated ARSA
gene insertion sites in host genome can be monitored
• Gene modified-HSC give rise to therapeutic cells
HSCs pass BBB in MLD patients, and give rise to microglia cells to
secrete ARSA enzyme , taken up by the recipient
neural cells
• Ensure to last efficacy in long term: Self-renewal of HSC
• No Immune Rejection: autologous HSC transplant
7

8
HSCGT to Treat Late Infant MLD
at Early Pre-symptomatic Stage
Biffi, et al Science 2013

Rare Disease: Low Awareness
No Typical Symptom at early stage: Over 90% of patients
get wrong diagnosis and treatment
Progression : paralysis and blindness within 1-2 years in Late
infants; 6-8 years in Juvenile
9
Most Identified MLD Patients Have
Developed into Middle-to-Late Stage
Late infant (< Age 2) Early Juvenile (Age 2-6) Late Juvenile (Age 6-16)
http://www.mldfoundation.org/mld-101-progression.html

A Typical Late Juvenile MLD with
Advanced-Stage
10
Dysfunctions of cognitive
and mobility ability
MRI shown
demyelination in
brain
Low ARSA
activity, only
3-5% of healthy
level
ARSA gene
mutations

Procedures of HSCGT
11
HSC mobilization
HSC collection HSC backup
Re-infuse gene modified HSC
Follow-up
Chemotherapy, Wipe out old HSC HSCGT
HSC Purification
Frozen & Quality Checks
Outsource for mass lentiviral
manufacturing (cGMP) Transfer gene into HSC
Gene design and construction
in modified lentiviral vectors
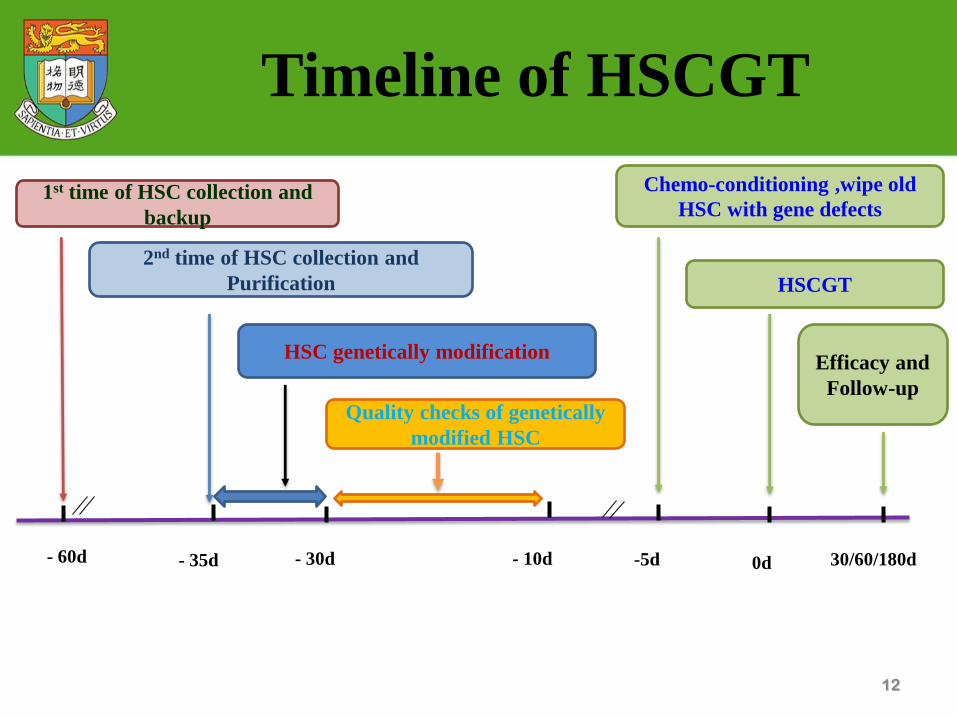
12
Timeline of HSCGT
- 60d
1st time of HSC collection and
backup
2nd time of HSC collection and
Purification
- 35d - 30d - 10d
HSC genetically modification
Quality checks of genetically
modified HSC
-5d 0d
Chemo-conditioning ,wipe old
HSC with gene defects
30/60/180d
HSCGT
Efficacy and
Follow-up

Post-Transplantation(Follow-up)
Improvement
observed
Speech, Emotion,
Reaction
Mobility/Balance
Episodic Seizures,
Bowel movements
Blood: increased
ARSA activity (normal
ranges
76.6±29.9nmol/mg/hr) 13
MRI: no signs of further
deterioration

Improvement of mobility
Post-transplantation
14
2015,Post-Transplantation,
improved mobility/balance
capacity
2014 September, successful
chemo-conditioning &
transplantation
2012-14, 2 weeks per month in
hospital due to cognitive and motor
deterioration

Summary
1.MLD is a devastating lysosomal storage disease caused by a
deficiency of arylsulfatase A(ARSA). Without ARSA to breakdown
accumulated sufaltides, neural system is toxic and presents
progressive damage. Patients die within a few years and no cure in
current clinical management
2.Lentiviral-mediatated HSCGT offers a novel therapeutic
approach. This technology effectively increased ARSA activity and
arrest disease progress, and there is no increased risk of cancer
observed up to date
3.It is still hopeful to rescue MLD onsets with advanced-stage
before neural system is very severely damaged
15

16
Acknowledgements
-HKU stem cells research team members
-Transplantation team members at the
Second People’s Hospital of Shenzhen
-Follow-up team members at The National
Taiwan University Hospital
-Taiwan Juridical Association of MLD Care

Patient’s Sharing
17

Questions & Answers
18