Embed Size (px)
Citation preview

187
INTRODUCTIONHaematological manifestations of humanimmunodeficiency virus (HIV) infection have abroad spectrum, ranging from mild disturbancesto life threatening conditions. Thrombocyto-penia is one of the haematologicalmanifestations that alerts clinicians.1 It is acommon finding in individuals infected withHIV, affecting approximately 40% of patientsduring the course of their illness. 2
Approximately 3% of patients with untreatedHIV with CD4+ count greater than 400/uL haveplatelet count less than 150,000/uL and thisincidence increases to 10% in HIV-seropositivepatients with CD4+ count <400/uL. Clinically,this entity resembles thrombocytopenia seen inpatients with idiopathic thrombocytopenicpurpura (ITP). While several reports on HIV-related thrombocytopenia have beendocumented in the world literature,3 there arefew reports on this topic from India. 4-6
Recognizing the need to create an awarenessregarding asymptomatic thrombocytopenia inpatients presenting HIV infection we document
this case and discuss the therapeutic options thatare available in this scenario.
CASE REPORTA 47-year-old male patient presented with fever,cough with expectoration since 4 months,diarrhoea, malaise and dysphagia since 3months. He was known to have diabetes mellitusand hypothyroidism and was on insulin therapyand thyroxine supplementation for the same. Hewas evaluated elsewhere for these symptomsand was diagnosed to have HIV-1 infection andwas suspected to have pulmonary tuberculosis.His CD4+ count was 94 cells/mm3. There wasevidence of right upper lobe infiltrates in chestradiograph, his sputum tested positive for acid-fast bacilli and he was initiated onantituberculosis treatment. He then reported toour out-pat ient department for furtherevaluation and management.He was moderately built and nourished and wasafebrile. He had hyperpigmented macular andnon pruritic rash over his body. Oral thrush waspresent. His respiratory, cardiovascular andneurological examination was unremarkable.
Case Report:HIV associated thrombocytopenia
N. Chandra,1 P. Bhavnadhar,1 Y. Satyanarayana Raju,1 Uppin Shanthveer2
Departments of 1General Medicine, 2Pathology, Nizam's Institute of Medical Sciences, Hyderabad
ABSTRACTWe report the case of 47-year-old male who presented with fever, cough and expectoration since 4 months anddiarrhoea, malaise and dysphagia since 3 months. He was known to have diabetes mellitus and hypothyroidism andwas receiving insulin and thyroxine supplementation. He was evaluated outside and was found to be co-infected withhuman immunodeficiency virus (HIV 1) and pulmonary tuberculosis and was receiving antituberculous treatment. Hehad hyperpigmented macular and non pruritic rash over his body. Oral thrush was present. Laboratory evaluationshowed thrombocytopenia (20,000/L) with giant platelets; bone marrow aspiration and biopsy revealed normocellularmarrow with increased and hypolobated megakaryocytes. The patient was treated with tenofovir, emtricitabine andefavirenz, antituberculosis drugs and oral fluconazole. Insulin and thyroxine replacement therapy were continued. Hewas diagnosed to have HIV associated thrombocytopenia and was started on dapsone treatment. Two months later, hisplatelet count had become normal. The present case highlights the importance of being aware of HIV associatedthrombocytopenia so as to facilitate the prompt recognition and treatment of this condition.Key words: Human Immunodeficiency Virus, Thrombocytopenia, Haematological manifestations
Corresponding Author: Dr N. Chandra, Associate Professor, Department of General Medicine, Nizam's Institute ofMedical Sciences, Hyderabad. e-mail: [email protected]
Chandra N, Bhavnadar P, Raju YS, Shanthveer U. HIV associated thrombocytopenia. J Clin Sci Res 2012;1:187-91.
Received : 14 May, 2012.
HIV associated thrombocytopenia Chandra et al

188
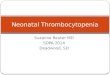
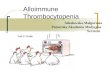
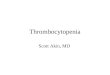
Complete blood count (Table 1) showedthrombocytopenia (20,000/L) with giantplatelets; haemoglobin, total and differentialleucocyte count and erythrocyte sedimentationrate (ESR) were with in normal limits. Serumaspartate aminotransferase [(AST) 45 U/L] andserum alanine aminotransferase [(ALT) 48U/L] were mildly elevated. Serum bilirubin was1 mg/dL. Renal parameters were normal. Uppergastrointestinal endoscopy (UGIE) revealedoro-oesophageal candidiasis. Bone marrowaspiration and biopsy revealed normocellularmarrow with increased and hypolobatedmegakaryocytes (Figures 1, 2 and 3).He was managed with tenofovir, emtricitabine,efavirenz; antituberculosis treatment withrifampicin, isoniazid, pyrazinamide, ethambutol,and oral fluconazole. Insulin treatment andthyroxine replacement therapy were continued.He was diagnosed to have HIV-associatedthrombocytopenia and was started on oraldapsone. At 2-months follow-up, his plateletcount increased to 150,000/mm3 (Table 1) andhe remained free of any haematologicalsymptoms.
Table 1: Complete blood picture report at the time of initial presentation and at 2 months of follow-up
Variable At initial presentation At 2 months follow-upHaemoglobin (g/dL) 13.6 12.8MCV (fL) 84.3MCH (pg) 28.0MCHC (mg/dL) 33.2Total leucocyte count(/mm3) 4200 5800Differential count Neutrophils 76%, Neutrophils 75%,
lymphocytes 23% lymphocytes 21%,eosinophils 2%, monocytes 1%,monocytes 1% eosinophils 1%
Platelet count (/mm3) 20,000 150,000Reticulocyte count (%) 0.5ESR mm (at the end of 1st hour) 15
MCV = mean corpuscular volume; MCH = mean corpuscular haemoglobin;MCHC = mean corpuscular haemoglobin concentration;ESR = erythrocyte sedimentation rate
HIV associated thrombocytopenia Chandra et al
DISCUSSIONReduction in all major blood cell lines has beenrecognized among patients infected with HIV,shortly after the first description of the acquiredimmunodeficiency syndrome (AIDS).Thrombocytopenia is a common finding inindividuals infected with HIV.7 It occurs inpatients from all major risk groups and maypresent with at any time during the course ofHIV infection, from asymptomatic infection toadvanced acquired immunodeficiency syndrome(AIDS). The incidence of platelet abnormalitiesappears to increase with progressiveimmunosuppression.8 In the current era ofcombination antiretroviral therapy, it is morecommonly encountered among patients withuncontrolled HIV replication and hepatitis Cvirus (HCV) co-infection.9
The causes of thrombocytopenia in HIV-infected patients can be divided into two groups:primary HIV-associated thrombocytopenia(PHAT) and secondary thrombocytopenia.10
PHAT is the most common cause of low plateletcounts encountered in HIV-infected patients.Clinically, PHAT is similar to classic ITP. Plateletcounts are often higher in HIV-infected patients,

189
and mild thrombocytopenia occasionallyresolves without therapy.11 The aetiology ofthrombocytopenia in PHAT is complex. The
combination of normal or increased numbersof megakaryocytes in the face of reducednumbers of circulating platelets in bone marrowexamination is seen, as in our case. It suggeststhe presence of ineffective platelet productionand/or increased peripheral destruction. Kineticstudies using radiolabelled autologous plateletsfrom HIV-infected individuals have shown thatboth factors contribute i.e., there is reductionin platelet survival and platelet production.12
Secondary causes of thrombocytopenia aregenerally the result of underlying opportunisticinfections, hypersplenism, malignancy, drugsand other co-morbid conditions.13
After the exclusion of secondary causes ofthrombocytopenia and discontinuation ofpotentially marrow-suppressing medications,there are many therapies available for themanagement of PHAT. Individual circumstancesdictate the necessity and acuity of therapy.Spontaneous remission has been seen in as manyas 18% of patients who have PHAT. In thosewho do not, therapy historically has consistedof institution of zidovudine (AZT).13 Recentstudies14-16 indicate that highly active antiretroviral therapy (HAART) is equally effective.Other t reatment modalit ies includeglucocorticoids, intravenous IgG (IVIG),intravenous anti-D therapy, splenectomy,danazol, dapsone, interferon and vincristine. Inour case we had chosen HAART which hasminimal interactions with anti tuberculartherapy.15-16
In the present patient, oral dapsone wasadministered as it has been shown to raiseplatelets with no major toxicity.17 Dapsone hasshown to be effective in some patients with HIV-related thrombocytopenia.17 Some trials haveshown that dapsone is a safe, inexpensivetreatment. The studies have also confirmed thebeneficial effect of dapsone in patients withchronic idiopathic autoimmunethrombocytopenic purpura.18-19 Glatt andAnand11 propose that patients with symptomaticHIV associated thrombocytopenia be treated
HIV associated thrombocytopenia Chandra et al
Figure 3: Photomicrograph of the bone marrow tre-phine biopsy section showing increased megakaryocytes(Haematoxylin and eosin, 100)
Figure 2: Photomicrograph of the bone marrow aspi-rate showing hypolobated megakaryocytes (arrow)(Geimsa, 200)
Figure 1: Photomicrograph of the peripheral smearshowing giant platelets (Geimsa stain 200)

190
with IVIG, without distinction between anti-Rh(D) and high-dose IVIG. The use of IVIG ishampered by its high cost and the need forhospitalization.HIV-related thrombocytopenia is a complex andincompletely understood phenomenon. Theideal treatment for HIV-relatedthrombocytopenia has not yet been determined.Published data favours the use of AZT. Usedby itself, AZT safely slows HIV infectiousness,but may not always stop it entirely. This mayallow HIV to become AZT-resistant over time,and for this reason AZT is usually used inconjunction with the other nucleoside analoguereverse transcriptase inhibitors, zidovudine ismandated in the World Health Organization's"essential drugs list", which is a list of minimummedical needs for a basic medical health caresystem.12,20
In addition, studies have shown that HAART isequally effective.14 As far as other treatmentsare concerned, most of the effects appear to betransient and risks and benefits should beweighed on a case-by-case basis. Treatmentshould be individualized and it is reasonable toaccept chronic thrombocytopenia even with lowplatelet counts as long as there are no significantbleeding complications.
ACKNOWLEDGEMENTWe wish to acknowledge Dr V.R. Srinivasan,Professor and Head, Department of GeneralMedicine, Nizam's Institute of MedicalSciences, Hyderabad for his guidance andconstant encouragement.
REFERENCES1. Khorvash F, Naeini AE, Behjati M, Jalali M. HIV
associated thrombocytopenia, misdiagnosed asthrombotic thrombocytopenic purpura: a casereport. Cases Journal 2009; 2:175.
2. Jost J, Täuber MG, Lüthy R, Siegenthaler Wl. HIV-associated thrombocytopenia. Schweiz MedWochenschr 1988;118:206-12.
3. Bussel JB, Haimi JS. Isolated thrombocytopeniain patients infected with HIV: treatment withintravenous gammaglobulin. Am J Hematol1988;28:79-84.
4. Hamide A, Ambing H, Kumar K, Rao RS, DasAK. Thrombocytopenia-a manifestation of HIV-1 infection in a heterosexual male. J AssocPhysicians India 1992;40:697-8.
5. Kumar P, Gupta RA, Chandra J, Seth A, Aneja S,Dutta AK. Clinical Course of Children with HIVAssociated Thrombocytopenia. Indian J Pediatr2012;79:1201-5.
6. Dikshit B, Wanchu A, Sachdeva RK, Sharma A,Das R. Profile of hematological abnormalities ofIndian HIV infected individuals. BMC BloodDisord 2009;9:5.
7. Morris L, Distenfeld A, Amorosi E, Karpatkin S.Autoimmune thrombocytopenic purpurain homosexual men. Ann Intern Med 1982;96:714-7.
8. Sloand EM, Klein HG, Banks SM, Vareldzis B,Merritt S, Pierce P. Epidemiology ofthrombocytopenia in HIV infection. Eur JHaematol 1992;48:168-72.
9. Marks KM, Clarke RM, Bussel JB, Talal AH,Glesby MJ. Risk factors for thrombocytopenia inHIV-infected persons in the era of potentantiretroviral therapy. J Acquir Immune DeficSyndr 2009;52:595-9.
10. Peltier JY, Lambin P, Doinel C, Courouce AM,Rouger P, Lefrere JJ. Frequency and prognosticimportance of thrombocytopenia in symptom-freeHIV-infected individuals: a 5-year prospectivestudy. AIDS 1991;5:381-4.
11. Glatt AE, Anand A. Thrombocytopenia in patientsinfected with human immunodeficiencyvirus: treatment update. Clin Infect Dis1995;21:415-23.
12. Ballem PJ, Belzberg A, Devine DV, Kine LysterD, Spruston B, Chambers H, et al. Kinetic studiesof the mechanism of thrombocytopenia in patientswith human immunodeficiency virus infection. NEngl J Med 1992;327:1779-84.
13. Volberding PA, Baker KR, Levine AM. Humanimmunodeficiency virus hematology. Hematology2003:294-313.
14. Caso JAA, Mingo CS, Tena JG. Effects of highlyactive antiretroviral therapy onthrombocytopenia in patients with HIV infection.N Engl J Med 1999;341:1239-40.
15. Centers for Disease Control and Prevention.Managing drug interactions in the treatment ofHIV related tuberculosis. 2007 Available at URL.http://www.cdc.gov/tb/publications/guidelines/TBHIV Drugs/default. Accessed on September 20,2012.
HIV associated thrombocytopenia Chandra et al

191
HIV associated thrombocytopenia Chandra et al
16. Boulle A, Van Cutsem G, Cohen K, HilderbrandK, Mathee S, Abrahams M, et al. Outcome ofnevirapine and efavirenz based antiretroviraltherapy when co administered with rifampicinbased antitubercular therapy. JAMA2008;300:530-9.
17. Durand JM, Lefèvre P, Hovette P, Issifi S, MonginM. Dapsone for thrombocytopenic purpura relatedto human immunodeficiency virus infection. AmJ Med 1991;90:675-7.
18. Durand JM, Lefevre P, Cretel E, Kaplanski G,Soubeyrand J. Dapsone therapy forthrombocytopenia in patients infected with human
immunodeficiency virus. Clin Infect Dis1996;22:1131-2.
19. Godeau B, Oksenhendler E, Bierling P. Dapsonefor autoimmune thrombocytopenic purpura. AmJ HematoI1993;44:70-2.
20. Hirschel B, Chave G, Lüthy T. Zidovudine for thetreatment of thrombocytopenia associated withhuman immunodeficiency virus (HIV). Aprospective study. The Swiss Group for ClinicalStudies on the Acquired ImmunodeficiencySyndrome (AIDS). Ann Intern Med1988;109:718-21.