Embed Size (px)
Citation preview
Hit Hard, Hit Early: When to Treat and With What?
Brian G. Gazzard, MD, Moderator
Julio Montaner, MD
Calvin J. Cohen, MD, MS
Faculty Disclosure
Brian G. Gazzard, MD
No real or apparent conflicts of interest to report.
Julio Montaner, MD
Research grants, advisory boards, speakers bureaus:
Abbott, Argos Therapeutics, Bioject Inc, Boehringer Ingelheim, Bristol-Myers Squibb, Gilead Sciences, GlaxoSmithKline, Hoffmann-La Roche, Janssen-Ortho, Merck Frosst, Panacos, Pfizer, Schering Serono Inc. TheraTechnolgies, Tibotec (J&J), Trimeris
Calvin J. Cohen, MD
Consulting fees, fees for non-CME services, contracted research:
Abbott, Bristol-Myers Squibb, Gilead Sciences, Merck, Pfizer, Tibotec
Hit Hard, Hit Early: When to Treat and With What?Brian G. Gazzard, MA, MD, FRCPConsultant Physician and Research Director, HIV/GUMChelsea & Westminster HospitalLondon, UK
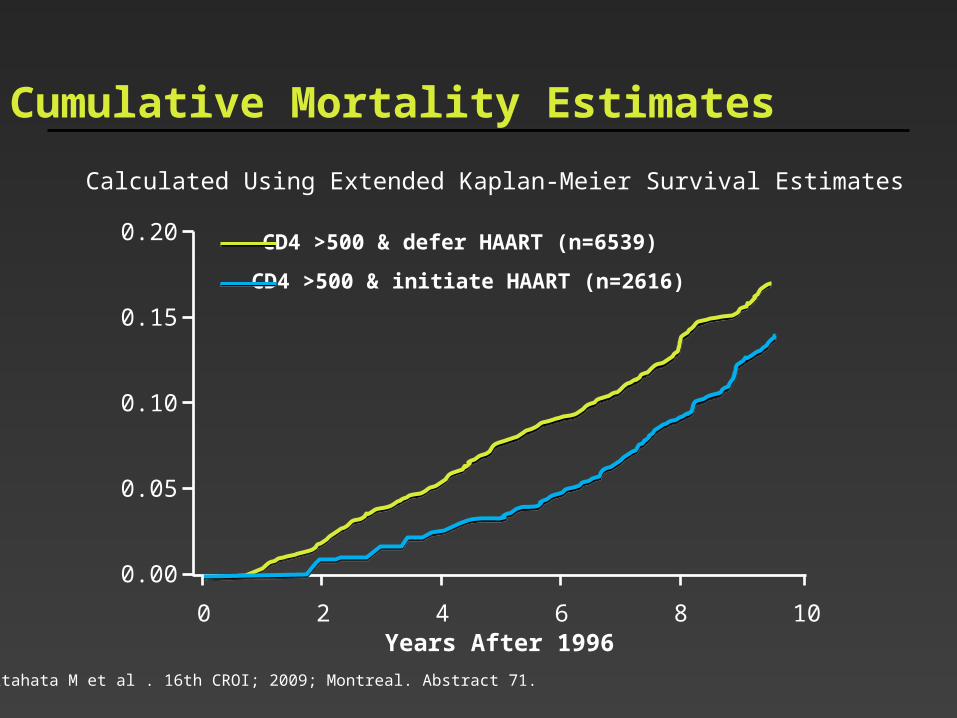
Cumulative Mortality Estimates
Calculated Using Extended Kaplan-Meier Survival Estimates
CD4 >500 & defer HAART (n=6539)
CD4 >500 & initiate HAART (n=2616)
Years After 1996
0.00
0.05
0.10
0.15
0.20
0 2 4 6 8 10
Kitahata M et al . 16th CROI; 2009; Montreal. Abstract 71.
CD4 Threshold (cells/mm3)
0.5
1
2
4
H
azar
d R
atio
0 100 200 300 400 500
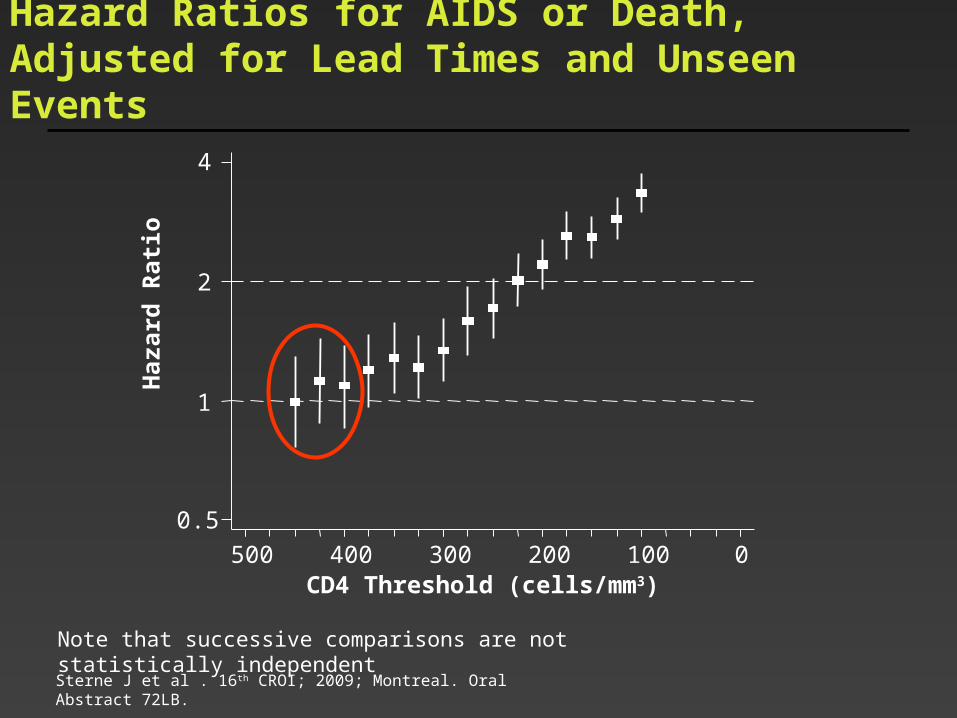
Note that successive comparisons are not statistically independent
Sterne J et al . 16th CROI; 2009; Montreal. Oral Abstract 72LB.
Hazard Ratios for AIDS or Death, Adjusted for Lead Times and Unseen Events
Assume you are HIV positive and have a CD4 count of 500 cc/mL. You have two options. Which would you choose?
1. $10,000 in the bank annually earning compound interest until your CD4 count is 350 cc/mL
2. Start ART immediately
Hit Early?
At what CD4 cell count would you start for the benefit of the patient?
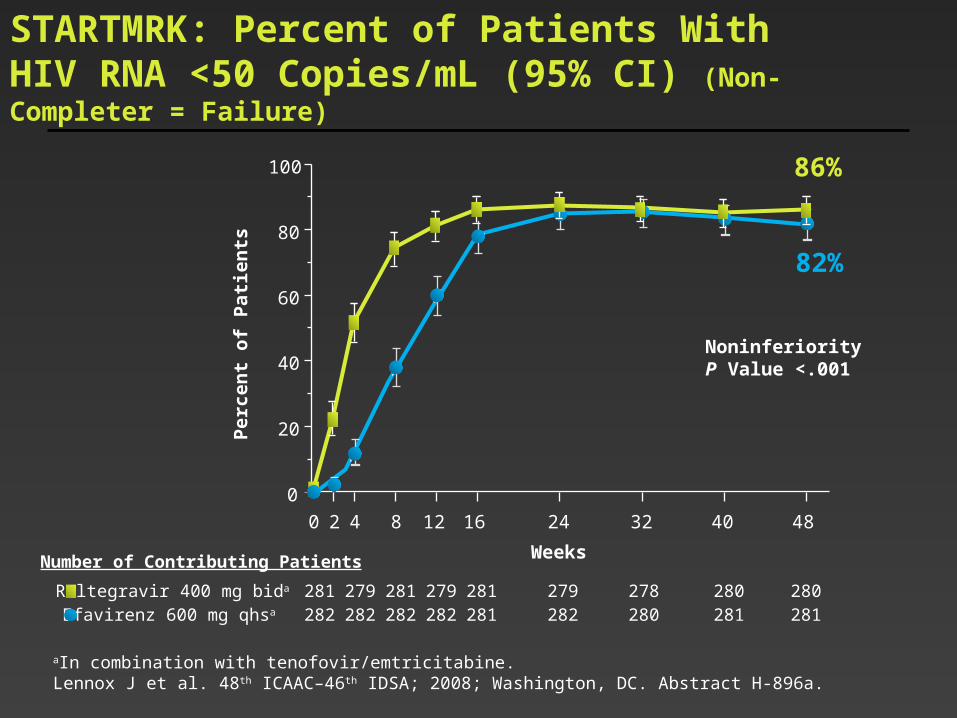
STARTMRK: Percent of Patients With HIV RNA <50 Copies/mL (95% CI) (Non-Completer = Failure)
281 279 281 279 281 279 278 280 280282 282 282 282 281 282 280 281 281
Raltegravir 400 mg bida
Efavirenz 600 mg qhsa
Number of Contributing Patients Weeks
Per
cen
t o
f P
ati
en
ts
0 2 4 8 12 16 24 32 40 48
0
20
40
60
80
100
82%
NoninferiorityP Value <.001
86%
aIn combination with tenofovir/emtricitabine.Lennox J et al. 48th ICAAC–46th IDSA; 2008; Washington, DC. Abstract H-896a.
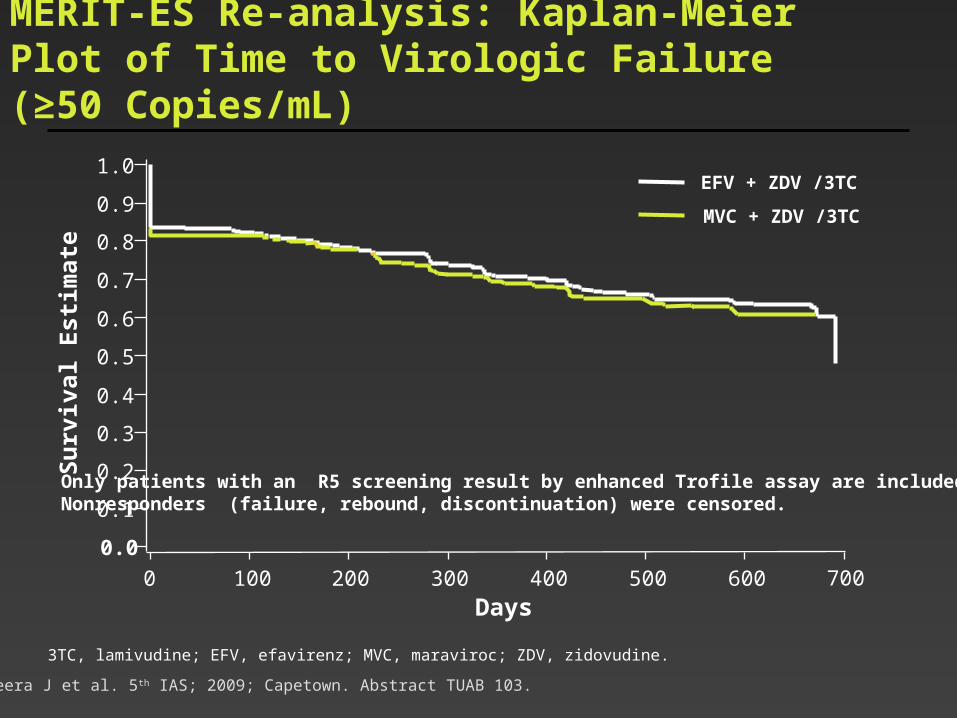
MERIT-ES Re-analysis: Kaplan-Meier Plot of Time to Virologic Failure (≥50 Copies/mL)
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 100 200 300 400 500 600 700
Only patients with an R5 screening result by enhanced Trofile assay are included.Nonresponders (failure, rebound, discontinuation) were censored.
MVC + ZDV /3TC
EFV + ZDV /3TC
Su
rviv
al E
stim
ate
Days
Heera J et al. 5th IAS; 2009; Capetown. Abstract TUAB 103.
3TC, lamivudine; EFV, efavirenz; MVC, maraviroc; ZDV, zidovudine.

Time to Virologic Failure (Plasma HIV RNA >200 log10 copies/mL)
No shorter time to undetectable viral load, but significantly shorter time to virologic failure. Consistent for other HIV RNA thresholds
0.00
0.25
0.50
0.75
1.00
97 97 97 93 91 89ZDV/ABC + TDF/FTC105 105 105 104 103 102ATV/r + TDF/FTC111 111 111 109 109 108EFV/TDF/FTC
Number at risk
0 4 12 24 36 48
Weeks
EFV/TDF/FTC
ATV/r + TDF/FTC
ZDV/ABC + TDF/FTC
Arm HR P
EFV/TDF/FTC 1
ATV/r + TDF/FTC 0.88 0.840
ZDV + ABC + TDF/FTC 3.30 0.012*
ABC, abacavir; ATV/r, ritonavir-boosted atazanavir; EFV, efavirenz; FTC, emtricitabine; TDF, tenofovir; ZDV, zidovudine.
Cooper D. 5th IAS; 2009; Capetown. Abstract LBPEB09.
Hit hard?
What agent would you start with?
Why would you no longer start with efavirenz?





























