Embed Size (px)
Citation preview

History of MS
• 1396: Saint Lidwina van Schiedam
– Relapsing and progressive neurological illness
• 1838: Robert Carswell
– First pathologic drawing of what would later be known as MS

History of MS
• 1868: Jean-Martin Charcot
– Framed the disease and thoroughly described the clinical and pathologic features of MS
– Utilized the previous observations of Carswell, Curveilhier, Hall, Frerichs, and others
– Called it “sclerose en plaque” or disseminated sclerosis
– Charcot’s triad: scanning speech, nystagmus, and intention tremor

History of MS
• ARNMD report of 1922
– Brought together many of the observations made by previous clinicians and pathologists
– Thought the disease was initially inflammatory and later degenerative

History of MS
• 1948: genetic theory
– 23% concordance rate in identical twins
– 10 times more common in families with MS
• Immunological theory
– 1932: hypersensitivity reaction
– 1946: McAlpine
• Suggested that MS was an immune reaction following infection

History of MS
• 1955: McAlpine, Compson, and Lumsden
– Multiple Sclerosis text published and established the name “multiple sclerosis” for the disease

History of MS
• 1950s: North–South gradient
• Faroe Islands
– No record of MS prior to 1949
– 24 cases between 1949 and 1960
– British soldiers occupied Islands in the 1940s
• Infection?

History of MS: More Recently
• Thought to be immune mediated
– Virally triggered in genetically susceptible host
• Treatments
– Acute attacks: ACTH in 1970s–1980s
– Disease modification in 1990s
– Symptomatic management
• Diagnostic tests
– MRI in 1980s
– New MRI techniques

What We Know Now…
• Most common neurological disease of young adults
• Chronic disease of the CNS
– Inflammation, demyelination, axonal degeneration
• Approximately 350,000 cases in US
• 2/3 of MS patients are women
• Associated with Northern European ancestry
• Age of onset: 15–55
– Usually diagnosed in 20s–30s

Statistics
• Incidence = number of new cases beginning in a unit of time within a special population
– Annual incidence per 100,000 population
• Prevalence = number with the diagnosis within the community at one point in time
– Expressed in unit per population
– Provides the best information regarding distribution of the disease

Statistics
• Worldwide distribution
– High prevalence 30+/100,000
• Northern US and Canada
• Most of Europe
• Southern Australia
• New Zealand
• Northeast Russia

Pathology
• White matter lesions in CNS
– Surrounded by plasma cells, immunoglobulins, macrophages, and lymphocytes
• Inflammation
• Myelin injury and destruction
• Axonal injury and destruction

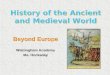
64m 45m
A B
Reprinted with permission from Trapp BD et al. N Engl J Med. 1998;338:278-285. Copyright 1998 Massachusetts Medical Society. All rights reserved.
Demyelination and Axonal Transection

Disease Course
• 85%–90% of patients present with a RR pattern of neurological symptoms
• 10%–15% never have relapses (PP)
• After approximately 10 years, nearly 50% of RR patients will show a progressive pattern to their disease
• This percentage grows with time

Adapted with permission from Lublin FD et al. Neurology. 1996;46:907-911. (http://lww.com)
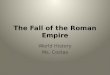
RRMS
PPMS
Dis
abil
ity
Time
Time
Dis
abil
ity
SPMS
PRMS
Time
Time
Dis
abil
ity
Dis
abil
ity
Disease Courses in MS

Weinshenker BG et al. Brain. 1989;112:133-146.
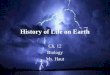
RRMSPPMS
Disease Type at Diagnosis Disease Type at 11–15 Years After Diagnosis (Among Those
With RRMS at Diagnosis)
SPMSRRMS
42%
58%
15%
85%
Natural History Over Time

Symptoms vary widely in incidence and severity.
Symptoms
• Fatigue
• Sensory disturbances
• Visual disturbances
• Elimination dysfunction
• Spasticity
• Pain
• Tremor
• Cognitive
• Gait disturbances

MS Prognosis
• Gender: women , men
• Age of disease onset: <35 years , >35 years
• Monoregional , polyregional
• Complete recovery after relapse , poor recovery after relapse
• Brainstem symptoms (nystagmus, tremor, ataxia, dysarthria)
• High incidence of attacks
• Number of lesions on MRI

Coyle P. Diagnosis and classification of inflammatory demyelinating disorders. In: Burks J, Johnson K, eds. Multiple Sclerosis, Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:81-97.
Diagnosis of MS
• Basic principles
– Demographic profile
• Female, Caucasian, young adult, latitude
– Clinical presentation
• Symptomatic disease, abnormal exam, white matter involvement, consistent
– Laboratory profile
• MRI
• CSF
• Evoked potentials
• Exclusion of other diagnoses

Clinical Presentation
• Sensory tracts
– 21%–55% of patients
– Most common presenting symptom
– Often begins in the limbs and migrates proximally
• Tingling, burning, “Novocain-like,” band-like, squeezing
• Lhermitte’s
• Neuritic pain
• Diminished vibratory sensation
• Impaired position sense
• “Useless hand” syndrome
– Sensory loss, loss of position sense
– Mobility preserved

Clinical Presentation
• Corticospinal tracts
– 32%–41% of patients
• Heaviness, weakness
• Abnormal DTRs
• Positive Babinski response
• Spastic limb weakness

Clinical Presentation
• Brainstem
– Eye movement abnormalities
• Diplopia at onset in about 7% of patients
• Nystagmus, INO
• Bilateral INO is almost pathognomonic for MS
– Vertigo
– Infrequently
• Dysarthria
• Peripheral 7th
• Hearing loss and tinnitus

Clinical Presentation
• Visual pathway
– Optic neuritis
• Presenting symptom in up to 25% of patients
– Dimming or visual loss
– Loss of color vision
– Visual field defect
• Cerebellar
– Gait ataxia, limb ataxia, tremor

Clinical Presentation
• Frontal lobe
– Cognitive dysfunction
– Emotional dysinhibition
• Temporal lobe
– Aphasia
• Corpus callosum
– Cognitive dysfunction

Clinical presentation from:Miller A. Clinical features. In: Cook S, ed. Handbook of Multiple Sclerosis, 3rd edition. New York: Marcel Dekker; 2001:213-224.Paty D. Initial symptoms. In: Burks J, Johnson K, eds. Multiple Sclerosis Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:75-93.
Clinical Presentation• Fatigue
– Present in up to 90% of patients
– Very common but nonspecific
• Elimination: brainstem/spinal cord
– Occasionally present at onset of disease
– Bladder urgency, frequency, hesitation, nocturia
– Bowel constipation, infrequently involuntary bowel movements

Symptoms vary widely in incidence and severity.
Sensory symptoms:Lhermitte’sPainProprioception
Optic neuritis
DiplopiaVertigoDysarthriaINO
TremorAtaxia
Cognitive loss
Emotional disinhibition
Bladder dysfunction
Sources of Symptoms

Diagnosis of MS
• Laboratory profile
– CSF
– Evoked potentials
– Serum evaluation
– MRI

CSF
• Invasive
• Used as supporting evidence or may suggest another diagnosis
• Not indicated if history, exam, and MRI are clearly consistent with MS
• For MS, look for
– Elevated IgG index, presence of oligoclonal bands in CSF, but not serum
• Other diagnoses may demonstrate elevated cell counts and/or elevated protein

Evoked Potential Testing
• Visual, auditory, and somatosensory
• Used less frequently, particularly if history, exam, MRI, and CSF are consistent with the diagnosis of MS
• Can help to document dissemination in space by demonstrating a brainstem or cord lesion
• Looking for slowed conduction described as prolonged evoked response latency

Cohen J, Rensel M. The differential diagnosis and clues to misdiagnosis. In: Burks J, Johnson K, eds.Multiple Sclerosis Diagnosis, Medical Management and Rehabilitation. New York: Demos; 2000:127-138.
Differential Diagnosis
• Infection
– Lyme, syphilis, PML, HIV, HTLV-1
• Inflammatory
– SLE
– Sjögren’s, vasculitis, sarcoidosis, Behçet’s disease
• Metabolic
– B12 deficiency, rare familial diseases
• CNS lymphoma
• Degenerative spinal disease
• Motor neuron disease

Serum Testing
• B12, folate
• RPR, FTA
• HIV
• HTLV-1
• ANA, SS-A, SS-B
• Antiphospholipid antibodies
• ESR, C-reactive protein
• Thyroid function
• Angiotension-converting enzyme
• Anti-acetylcholine receptor antibodies
• Long-chain fatty acids

MRI in MS
• MRI demonstrates approximately 90%–95% of white matter lesions in brain
• MRI demonstrates 50%–75% lesions in spinal cord

Use of MRI
• MRI is a useful tool in helping to make the diagnosis of MS
• MRI may also be helpful in clinical decision making
• Cost and availability are limiting factors in repeated MRIs in the clinical setting

MRI Basics
• MRI uses a strong magnetic field to align the hydrogen nuclei (protons) in the direction of the magnetic field
• A radio frequency electromagnetic pulse is then used to knock the protons off their axes, thus sending them out of alignment with the magnetic field

MRI Basics
• The pulse is then stopped and the protons return to their alignment with the magnetic field
• This return to alignment is known as relaxation
• Different tissues “relax” at different rates, which gives the anatomic contrast seen with the MRI

T1-Weighted Images
• The time it takes the protons to return to their original orientation after the pulse stops is the longitudinal relaxation time or T1
• Emphasizes the differences between the tissues and shows excellent anatomic detail
• Areas of abnormality show up dark on T1, and therefore these images do not often demonstrate pathology best

T1-Weighted Images

T1 With Gadolinium
• Demonstrates breakdown of BBB
• Areas of active inflammation
• New lesions remain enhanced for brief time

T1 With Gadolinium

T1 Hypointensities
• “Black holes”
• Thought to be areas of axonal loss
• Can be “black holes” that are temporary with a new lesion
• Black holes not associated with a new lesion are thought to be areas of permanent damage

T1 Black Holes

T2-Weighted Images
• The time it takes for the protons to dephase and for the signal to die away is known as transverse relaxation time or T2
• Relaxation time for T2 images are usually long
• Show contrast between normal and abnormal tissue better than T1
• Abnormal increases in water content appear bright on T2

Conventional T2 FLAIR
T2-Weighted Images

FLAIR Image

FLAIR Image and T1 Black Holes

T2 BOD
T1/gadolinium postcontrast
disease activity
T1precontrastblack holes
A B
C
T2-FLAIR
D
MS Lesions on MRI

Spinal MRI in MS
• Spinal cord lesions in 75% of MS patients
• Predominantly in C-spine
• Usually dorsolateral or central and 0.5 cm by 1–2 cm, and 1–2 vertebral segments
• Less likely to enhance or cause cord swelling
• More likely to cause progressive disease
• T2 less predictive of disability than atrophy

Cord Lesion


Brain Atrophy
• Cerebral atrophy is a global measure of disease that measures irreversible tissue damage
• Serial measures may reflect disease progression
• “Potentially” the most valid MRI surrogate marker
• May be “faster, simpler, and better” than current measures (Jagust WJ, Noseworthy JH. Neurology. 2000;54:782-783.)

36-year-old womanRRMS (2 years)
43-year-old womanSPMS (19 years)
31-year-old maleHealthy control
BPF 0.87z score = 0
BPF 0.85z score = –2.6
BPF 0.71z score = –20.8
Examples of BPF in MS
Reprinted with permission from Rudick RA et al. Neurology. 1999;53:1698-1704.

McDonald WI et al. Ann Neurol. 2001;50:121-127.
McDonald Diagnostic Criteria
• Preserve traditional diagnostic criteria of 2 attacks of disease separated in space and time
– Must be no better explanation
– Add specific MRI criteria, CSF findings, and analysis of evoked potentials as means of identifying the second “attack”

McDonald Diagnostic Criteria
• Conclude that the outcome of the diagnostic workup should yield 1 of 3 outcomes:
– MS
– Possible MS
– Not MS
• New criteria utilize MRI, CSF, or evoked potential testing when only one lesion found and/or only one attack or when onset is insidious neurological progression
McDonald WI et al. Ann Neurol. 2001;50:121-127.

MRI Evidence of Dissemination in Time
• A gadolinium-enhancing lesion demonstrated in a scan done at least 3 months following onset of clinical attack at a site different from attack
• In absence of gadolinium-enhancing lesions at 3-month scan, follow-up scan after an additional 3 months showing gadolinium-enhancing lesion or new T2 lesion
McDonald WI et al. Ann Neurol. 2001;50:121-127.

McDonald MRI Criteria
• Abnormal MRI consistent with MS defined as:
– Must have at least 3 of the following:
• 1 gadolinium-enhancing lesion or 9 hyperintense lesions if no gadolinium-enhancing lesion
• 1 or more infratentorial lesions
• 1 or more juxtacortical lesions
• 3 or more periventricular lesions
– 1 cord lesion = 1 brain lesion
McDonald WI et al. Ann Neurol. 2001;50:121-127.

Gd-enhancing T2 hyperintense
Juxtacortical Periventricular Spinal Cord
Infratentorial
McDonald MRI Criteria

3 months
T2
Gadolinium
Application of New Diagnostic Criteria

Proposed Diagnostic Criteria
• An effort to expedite diagnosis
• Have become part of inclusion/exclusion for newer clinical trials
• Makes an effort to define clinically isolated syndrome to enable earliest treatment

SPMS
Adapted from Wolinsky JS. Multiple sclerosis. In: Appel SH, ed. Current Neurology. Vol. 13. Chicago, Ill: Mosby Year Book, Inc.; 1993:167-207, with permission from Elsevier.
Natural History of MS
RRMSPreclinical
Time
Dis
abil
ity
Measures of brain volumeRelapses and impairmentMRI burden of diseaseMRI activity
ABCD
A
B
C
D

Immune-Mediated Disease
• Inflammation
• Demyelination
• Axonal degeneration and loss
• Must be knowledgeable about the normal immune system and the dysregulation in MS

Immunological Basis for MS:Normal Immune System
• Protects from pathogens such as
– Bacteria
– Viruses
– Parasites
– Fungi
• Protects through
– Innate immunity
– Adaptive immunity

Macrophage
Pathogen
The Immune System
• Innate immunity
– Immunity to certain pathogens that is common to all healthy individuals
– Does not require prior exposure to the pathogen
– Immediate destruction of some pathogens by phagocytic cells, such as macrophages and neutrophils, and natural killer cells

The Immune System• Adaptive immunity
– Requires exposure to pathogen to stimulate immune system response
– Cellular immunity
• Cytotoxic T cells (CD8)
• Th1 cells (CD4)
– Humoral immunity
• Th2 cells (CD4)
• B lymphocytes
• Antibodies
• Activation of complement

The Immune System
• B cells recognize antigen that is present outside of cells in its natural state
• T cells detect antigen generated inside host cells and presented on the cell surface
• Both B cells and T cells must receive an additional (co-stimulatory) signal in order to be activated

Humoral Immunity
• B cells have specific antibodies on their surface
• They circulate looking for a recognizable antigen
• Under the influence of cytokines released from Th2 cells, B cells give rise to plasma cells that secrete large amounts of antibodies
• Plasma cells do not leave the lymphoid tissue

B cells give rise to plasma cells, which are antibody-producing factories.
Humoral Immunity• Antibodies work by
– Neutralization
• Binding to pathogens andblocking the path to body cells
– Opsonization
• Enabling phagocytic cells torecognize pathogens by coatingthe pathogen
– Complement
• Some antibodies activate a series of proteins called complement that have been circulating, inactive, in the blood. Complement and the antibody combine in a partnership that can react to an antigen and help to destroy it.

Cellular Immunity
• T lymphocytes each have cell-surface receptors
– Distinct from lymphocyte to lymphocyte
– This enables lymphocytes to recognize a wide variety of antigens

Cellular Immunity
• Once a T cell is activated by antigen presentation:
– It proliferates in a process known as clonal expansion
– These activated cells produce cytokines that can activate the “killer” mechanism of macrophages
– Antigen-specific lymphocytes undergo apoptosis once the antigen is removed
– Some antigen-specific lymphocytes persist and are the basis for immunological memory

Cellular Immunity
• The cells that present antigen to T cells are antigen-presenting cells
– Dendritic cells
– Macrophages
– B cells
• These cells display antigen protein particles on specialized cell surface molecules known as MHC

Cellular Immunity
• 2 classes of MHC molecules
– MHC I
– MHC II
• MHC I are recognized by cytotoxic T cells (CD8)
• MHC II are expressed on the surface of macrophages or B cells and are recognized by Th1 or Th2 cells (CD4)

RestingT cell
ActivatedTh1 or Th2
ActivatedTh1 or Th2
ActivatedTh1 or Th2
ActivatedTh1 or Th2
APC(Macrophage)
Virus
MHC II
APC processing virus
Presentation ofvirus protein to resting Th1 cell
T-cellreceptor
Costimulatory molecules
Cellular Immunity

CD4 Cell Cytokine Production
• Th1 cells activate macrophages and produce:
– IFN-– TNF-– IL-2
– Lymphotoxin
• Th2 cells activate B cells and produce:
– IL-4
– IL-5
– IL-10 (regulatory cytokine)
– IL-13
– TGF-

Immune Dysregulation
• T cells that recognize self-antigen are generally deleted in the thymus
• May be a small # of autoreactive cells still present
• In autoimmune illness, the regulatory mechanisms that keep these T cells in check are not working properly
• Without regulation, autoreactive T cells can proliferate

Immune Dysregulation
• Molecular mimicry
– Self-protein is structurally similar to non–self-antigen
– T cells can recognize self-antigens if they bear enough similarity to the non–self-antigen

Immune System in MS
• Th1 cells are stimulated in the periphery by presentation with antigen
– Eg, a virus particle
• Once activated
– They proliferate
– They release cytokines and metalloproteinases that break down the extracellular matrix of the BBB

MS
• Once in the CNS, Th1 cells
– Are presented with a myelin protein
• The myelin protein is similar to the antigen presented in the periphery
– Become reactivated
– Release damaging cytokines
• IFN-, TNF-, IL-2
– Stimulate B-cell activity, antibody production, and complement activation

Th0
ActivatedTh1
ActivatedTh1
ActivatedTh1
APCActivated
Th1
Th1
APC
Periphery CNS
TNF-α
IFN-γ
IL-2MHC-II
Myelin protein
TCR
Antigen
Costimulatorymolecules
MMP
MMP
LFA-1
ICAM
Microglialcell
B cell
MS Immune ResponseBBB

APC ActivatedTh1
ActivatedTh1
ActivatedTh1
ActivatedTh1
Th1
TNF-α
IFN-γ
IL-2
MMP
MMP
MMP
Th0
BBB
B cell
APC
MS Immune Response

Results of Autoimmune Activity Within the CNS
• Neurological symptoms followed by some degree of recovery
– Relapses and remissions
– Little axonal injury or damage
• Permanent damage within the CNS
– Progression
– Axonal damage and loss

IFN
• Inhibits synthesis of inflammatory cytokines
– IFN-, TNF-
• Downregulates expression of MHC II molecules induced by IFN-
• Reduces antigen presentation to T cells
• Inhibits T-cell proliferation
• Downregulates adhesion molecules and promotes BBB integrity

Th0
ActivatedTh1
ActivatedTh1
ActivatedTh1
APCActivated
Th1
Th1
APC
BBB
Periphery CNS
TNF-α
IFN-γ
IL-2
MHC-II
Antigen
Myelin protein
TCR
IFN β Effect on MS Immune Response
IFN
β
IFN
β
IFN
β

Glatiramer Acetate
• Induces suppressor T cells
• Structurally similar to myelin basic protein and when glatiramer acetate–induced T cells are presented with myelin basic protein in the CNS, they are stimulated to proliferate and release cytokines
– TGF-, IL-4, IL-10
• These T cells are thought to suppress pro-inflammatory T cells in a process called bystander suppression

Th0
ActivatedTh2
ActivatedTh2
ActivatedTh2
APCActivated
Th2
Th2
APC
BBB
Periphery CNS
IL-4
IL-6
IL-10
MHC-II
Glatiramer acetateantigen
Myelin protein
TCR
Bystandersuppression on other T cells
Glatiramer Acetate–Induced Immune Response
Glatiramer acetate–induced
T cell
Th2

APCActivated
Th1
ActivatedTh1
ActivatedTh1
ActivatedTh1
Th1
APC
TNF-α
IFN-γ
IL-2
MMP
MMP
MMP
BBB
Antegren
Anti-IL-12
BMS-block costimulatory
Campath
Research in MS
Th0

Summary• Nurses’ role
– Education
– Advocacy
– Support
• Understanding of the disease
– Immune basis
– Clinical features/diagnosis
– MRI
• Understanding MS treatments, symptomatic management, our role, current issues, and current research