Embed Size (px)
Citation preview

PII S0301-5629(99)00028-9
● Original Contribution
HISTOLOGICAL STUDY OF NORMAL AND TUMOR-BEARING LIVERTREATED WITH FOCUSED ULTRASOUND
LILI CHEN, GAIL TER HAAR, DAVID ROBERTSON, JOHN P. M. BENSTED andCHRISTOPHERR. HILL
Joint Department of Physics, Institute of Cancer Research and Royal Marsden Hospital,Sutton, Surrey SM2 5PT UK
(Received11 September1998; in final form 18 February1999)
Abstract—The purpose of this investigation was to study the tissue damage (including blood vessels) on bothnormal and tumor-bearing experimental livers and the course of liver repair after focused ultrasound (FUS)treatment using histological evaluation. A series of experiments were carried outin vivo. Tissue was treated usingarrays of ultrasound exposures with a frequency of 1.7 MHz,in situ spatially averaged focal intensity (ISAL insitu) of 212–266 W/cm2 (corresponding to in situ spatial peak intensity of 382–479 W/cm2), 5–10 s exposureduration and 1.5–3.0 mm exposure separation. Tissue specimens were examined using both light and electronmicroscopy. The damage to the blood vessel walls was studied. The results showed the existence of indirect tissuedamage in both normal and tumor tissue that is outside of the treatment volume, due to disruption of the majorblood vessels supplying the adjacent area. Evidence for liver regeneration was found 2 months after FUStreatment. © 1999 World Federation for Ultrasound in Medicine & Biology.
Key Words:Ultrasound surgery, Tissue ablation, Liver tumors, Histological changes, HSN fibrosarcoma, Liverregeneration.
INTRODUCTION
Recently, the advantages of using magnetic resonance(MR) imaging to guide and monitor focused ultrasoundsurgery (FUS) have been demonstrated by many investiga-tors (Cline et al. 1993, 1994, 1995; Darkazanli et al. 1993;Graham et al. 1999; Hynynen et al. 1994, 1995, 1996;McDannold et al. 1998; Rowland et al. 1997; Walker et al.1998). FUS has long been known to offer the potential ofvery precise “trackless lesioning,” but has only recently,with the advent of high quality methods of medical imag-ing, become a practical possibility. The availability of mod-ern imaging techniques has encouraged a revival of clinicalinterest, and applications in ophthalmology, urology andoncology are being developed. The use of this technique fora range of clinical applications has been reviewed by terHaar (1995) and by Hill and ter Haar (1995).
We have carried out research on the treatment of
discrete hepatic metastases (Chen et al. 1998; ter Haar et al.1989, 1991, 1998; Hill 1994; Hill et al. 1994; Malcolm andter Haar 1996; Rivens 1992; Rowland et al. 1997). It hasbeen demonstrated that the primary mechanism of ultra-sound tissue damage is thermal. The temperature at thefocal peak in rat liver measured using a 0.2-mm diameterneedle thermocouple was 70–100°C (Chen et al. 1993), andthe temperature at the lesion boundary in excised pig livermeasured using MRI was approximately 55°C (Graham etal. 1999). Suggestive evidence has been found that tissuedamage may arise through two different mechanisms: theseare direct, primarily thermal, damage and indirect damageresulting from compromised blood supply. Under the sameexposure conditions, normal liver cells appeared to losetheir structure morphologically more readily than do tumorcells (Chen et al. 1993). It has been shown that it is possible,with careful treatment planning, to damage all the tumorcells within the treatment volume (Chen et al. 1999).
This study is an extension of our previous investiga-tions. A series of specially designed experiments were per-formed to further investigate the mechanisms of tissuedamage and the course of liver repair after ultrasoundtreatment and to extend our understanding of the effect offocused ultrasound on living tissues. These experiments
Dr. Chen’s current address is: Radiology Department, StanfordUniversity, Stanford, CA 94305 USA.
Address correspondence to: Lili Chen, Ph.D., Lucas MRS Im-aging Center, Department of Radiology, Stanford University, 1201Welch Road, Stanford, CA 94306-5488 USA. E-mail: [email protected]
Ultrasound in Med. & Biol., Vol. 25, No. 5, pp. 847–856, 1999Copyright © 1999 World Federation for Ultrasound in Medicine & Biology
Printed in the USA. All rights reserved0301-5629/99/$–see front matter
847

were done on both normal and tumor-bearing (HSN fibro-sarcoma) rat livers. The histological examinations werecarried out using both light and electron microscopy.
MATERIALS AND METHODS
EquipmentThe focused ultrasound treatment equipment used for
this paper has been reported in detail previously (Chen et al.1993; ter Haar et al. 1989). The 1.7-MHz focused ultra-sound field was produced by a plane, 10-cm diameterpiezoelectric ceramic transducer (PZT4), and focused by abiconcave Perspex lens with a focal length of 140 mm.Varying the total acoustic power (measured using a radia-tion force balance in the focal plane) out of the transducerfrom 12 to15 W resulted inin situ spatially averaged focalintensities,in situ ISAL, of 212–266 W/cm2 (correspondingto in situspatial peak intensity of 382–479 W/cm2). In thispaper, “intensity” values are given in terms ofin situ ISAL,as determined under linear conditions. The merit of usingISAL has been described by Hill et al. (1994). Thein situspatially averaged focal intensity ISAL (in situ) was calcu-lated from the free-field spatially averaged focal intensity inwater ISAL (free field) by:
ISAL~in situ! 5 ISAL~free field!e2md, (1)
wherem (0.19 Np/cm) is the ultrasound attenuation co-efficient in liver for the frequency used in this work (1.7MHz), derived from the published data (Kuc et al. 1997)andd is the focal depth. The acoustic field was mappedusing a calibrated polyvinylidene difluoride (PVDF)membrane hydrophone (GEC Marconi, Chelmsford,UK). The focal region of the sound was cigar-shaped,with dimensions (FWHM, full width, half pressure max-imum) of 21 mm along the beam axis and 2.1 mm in thetransverse direction. The relationship between beamproperties and lesion size in rat liver has been reportedelsewhere (Hill et al. 1994; Rivens 1992). The trans-ducer, lens, and the animal to be treated were suspendedin a bath of degassed water. A laser beam was used toposition the area to be treated on the beam axis. A3-coordinate gantry system was used to move the samplein 0.001 mm or greater increments.
Experimental procedures
Study of direct and indirect tissue damage and thecourse of liver repair.To study tissue damage, tissuerepair and the effect of indirect tissue damage due tofocused ultrasound, the 10 Chester Beatty Hooded(CBH) female adult rats (weight, 150–170 g) used forthis study were divided equally into two groups. Prior totreatment, a laparotomy was performed under general
anesthesia using intraperitoneal diazepam (0.05 mL/100g) and intramuscular Hypnorm (0.1 mL/100 g). Theanesthetic lasted up to 3 h. The rat liver was exteriorizedand the animal was mounted in a small cylindrical Per-spex tank with phosphate buffered saline (PBS) at 37°C.Then, this tank was placed in a larger tank of degassedwater. The liver lobe was exposed to a FUS beam with anin situ ISAL of 266 W/cm2, an exposure duration of 10 s,an exposure separation of 2 mm and a focal depth of 2mm below the liver surface.
The first group of 5 rats (Group A) was treated in fivedifferent ways as shown in Fig. 1a–e. In Fig. 1a, the liverwas exposed to a row of exposures along a horizontal lineacross the liver lobe. The distance of the ultrasonic lesion tothe bottom liver edge was 5 mm. An assumption was madeto create indirect liver damage below the exposure line byblocking the blood supply from both hepatic artery andportal vein. With the same assumption, in Fig. 1b, the liverwas exposed to 12 exposures along a horizontal line acrossthe liver lobe. The distance of the ultrasonic lesion to thebottom edge of the liver was 13.3 mm. In Fig.1c, the liverwas exposed to a square array of 4 exposures in the middleof the liver. In Fig. 1d, the liver was exposed to a squarearray of 8 exposures in the middle of the liver. In Fig. 1e,the liver was exposed to 12 exposures along a vertical linefrom the middle of the liver lobe to the bottom liver edge.Those exposure procedures were repeated for a secondgroup of rats (Group B). After ultrasound exposure, the ratswere allowed to recover. Group A was sacrificed 2 monthsafter the ultrasound treatment and Group B was sacrificed 4months after the treatment. The livers were removed andsamples were fixed in methacarn. Histological cross-sec-tions 3mm thickness, taken at 0.5-mm intervals through thewhole liver were stained with hematoxylin and eosin(H&E), and reticulin, and examined using a light micro-scope. During histological examination, particular attentionwas paid to evidence of tissue damage and tissue repair(including liver regeneration) both within, and outside, thetreated volume.
Study of direct and indirect FUS damage, for lightmicroscopy.To study the morphological differences ofcell death between directly and indirectly damaged area,1 rat liver was treated with arrays of ultrasound exposurewith an in situ ISAL of 266 W/cm2 and 5-s exposureduration. The focal depth in tissue was set 2 mm belowthe tumour surface. After treatment, the rat liver wasreplaced into the abdomen, and the rat was allowed torecover. Three days following treatment, the rat waseuthanized. The treated liver lobe was removed and fixedin methacarn. Histological cross-sections, 3mm thick,taken at 1-mm intervals through the liver lobe, werestained with H&E.
848 Ultrasound in Medicine and Biology Volume 25, Number 5, 1998
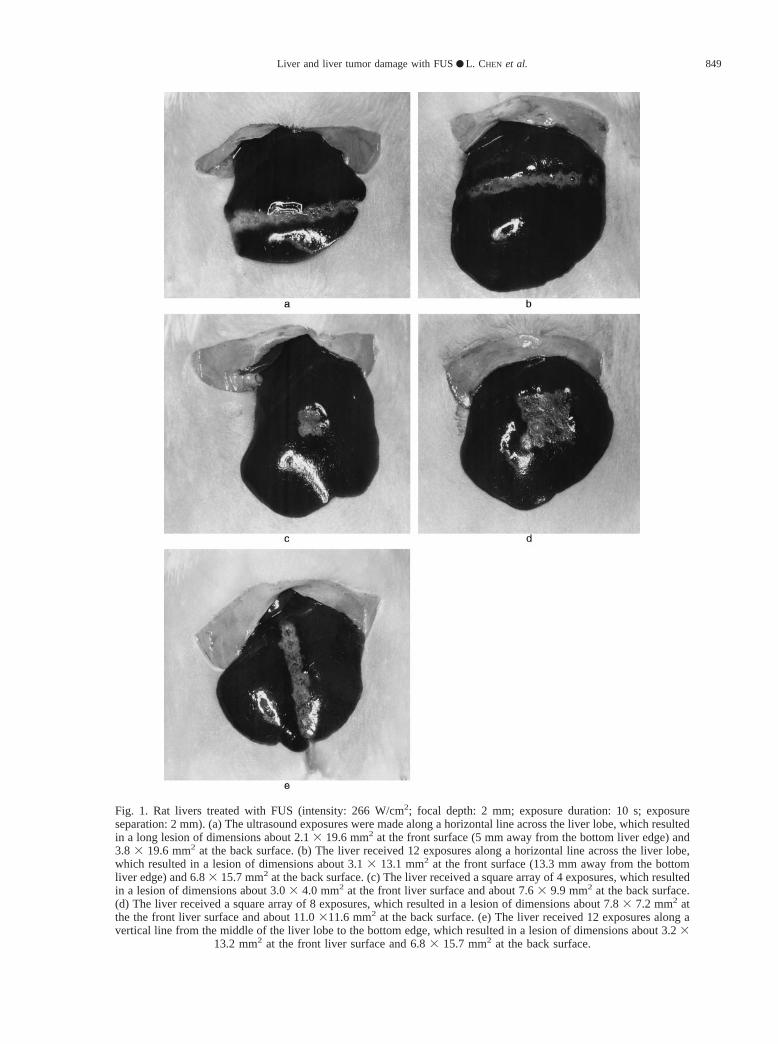
Fig. 1. Rat livers treated with FUS (intensity: 266 W/cm2; focal depth: 2 mm; exposure duration: 10 s; exposureseparation: 2 mm). (a) The ultrasound exposures were made along a horizontal line across the liver lobe, which resultedin a long lesion of dimensions about 2.13 19.6 mm2 at the front surface (5 mm away from the bottom liver edge) and3.8 3 19.6 mm2 at the back surface. (b) The liver received 12 exposures along a horizontal line across the liver lobe,which resulted in a lesion of dimensions about 3.13 13.1 mm2 at the front surface (13.3 mm away from the bottomliver edge) and 6.83 15.7 mm2 at the back surface. (c) The liver received a square array of 4 exposures, which resultedin a lesion of dimensions about 3.03 4.0 mm2 at the front liver surface and about 7.63 9.9 mm2 at the back surface.(d) The liver received a square array of 8 exposures, which resulted in a lesion of dimensions about 7.83 7.2 mm2 atthe the front liver surface and about 11.0311.6 mm2 at the back surface. (e) The liver received 12 exposures along avertical line from the middle of the liver lobe to the bottom edge, which resulted in a lesion of dimensions about 3.23
13.2 mm2 at the front liver surface and 6.83 15.7 mm2 at the back surface.
Liver and liver tumor damage with FUS● L. CHEN et al. 849

For electron microscopy.To further study the his-tological changes in healthy rat liver and in liver tumor-damaged directly and indirectly by FUS, 1 CBH rat wasimplanted with HSN fibrosarcoma (North et al. 1982) bysubcapsular injection of 106 cells suspended in 0.05 mLof Dulbecco’s modified eagle’s medium and 10% fetalcalf serum, into the left liver lobe. Eight days afterimplantation, tumors grew to approximately 8 mm indiameter. A narrow band of tissue including both tumorand healthy liver was exposed to arrays of ultrasoundexposures horizontally across the liver lobe in a similarfashion as that shown in Fig. 1b. The tumor-bearing liverwas exposed to a beam with anin situ ISAL of 261W/cm2 and 10-s exposure duration. The focal depth intissue was set 3 mm below the tumor surface. Aftertreatment, the rat liver was replaced into the abdomen,and the rat was allowed to recover.
The rat was euthanized 24 h following treatmentand the liver was removed. The “directly” (within thetreated volume) and “indirectly” (outside the treated vol-ume) damaged tissue samples for both healthy liver andfor tumor were removed separately and cut into 0.5-mmthick slices using a macrotome (Leica Ltd, UK). Thetissue samples were fixed immediately in 2% glutarade-hyde in 50-mM phosphate buffer PH 7.3, with the os-molarity adjusted to 320 mosmol, and with sucrose,overnight and postfixed in 1% osmium tetroxide. Thesamples were then dehydrated using a graded series ofethanol and embedded in an Epon/Araldite mixture. Sec-tions 0.1mm thick were cut, double stained with uranylacetate and lead citrate, and viewed on a Phillips CM10electron microscope.
Study of blood vessel walls.To study the histolog-ical changes in blood vessel walls with FUS, 2 rat liverswere treated with anin situ ISAL of 212 W/cm2, exposureduration of 8 s, and exposure separation of 1.5 mm. Ratswere euthanized from 1 day to 2 weeks following treat-ment. The livers were removed and fixed in methacarn.Histological cross-sections, 3mm-thick, taken at 1-mmintervals through the lobe, were stained with Van Gieson(VG) and examined microscopically.
RESULTS
Gross observation of direct and indirect liver damageFor rats sacrificed 24 h and 3 days after FUS treat-
ment, the “directly” and “indirectly” damaged tissuecould be distinguished by the naked eye. Tissue with“direct” ultrasound damage showed tissue blanching andthe surface of the liver lobe was rough. The tissue with“indirect” ultrasound damage showed much less tissueblanching and the surface was smooth.
The rats in Groups A and B were euthanized 2 and4 months after the treatment, respectively. The rats were
carefully examined by the naked eye before euthanesia.The rats looked healthy and active. The livers wereremoved. The main difference between the livers re-moved 2 months and 4 months after treatment was thedegree of inflammation due to the response of the host tothe ultrasonic treatment (i.e., the extent to which thegreater omentum was wrapped to the lesion). Liver lobestreated in the same way were similar in shape indepen-dent of whether they were removed 2 months or 4months after the treatment. The liver lobe in Fig. 2a wasexposed to a row of lesions along a horizontal line acrossthe liver 5 mm above the bottom edge as described inFig. 1a. At both 2 and 4 months after FUS exposure, theliver lobes became shorter and only capsular scar tissueremained in the exposed area. It can be seen that theuntreated healthy liver below the lesion “band” had dis-appeared. Presumably, the unexposed healthy liver (5mm from the liver edge) had also been damaged andremoved by phagocytes 2 months after treatment. It isclear that the ultrasound damage induced in this studyincludes both direct (i.e., primarily thermal damage) andindirect damage due to the impairment of the bloodsupply after the ultrasound exposure.
The indirect ultrasound damage appears to becaused by occlusion of the local blood supply after thetreatment and, therefore, depends on the vessel distribu-tion in the tissue. This is demonstrated in Fig. 2b–e,which shows liver lobes treated in different ways corre-sponding to Fig. 1b–e and removed 4 months after thetreatment. Figure 2b shows an exposed liver that wastreated to a row of lesions along a horizontal line acrossthe liver 13.3 mm above the bottom liver edge as de-scribed in Fig. 1b. A large island of healthy liver tissuecan be seen below the lesion “band.” Similar results werealso found in the liver treated in the same way, buteuthanized 2 months after the treatment. The proposedreason for the survival of this island of healthy livertissue is that the lesion length was not enough to pene-trate the whole liver thickness at this location where it isthickest (about 7 to 8 mm). In addition, blood flow insidelarge blood vessels also reduces the temperature eleva-tion around the blood vessels. Undamaged blood vesselswill supply the liver tissue below the treated “band” withnecessary nutrition. Figure 2c–e also shows evidencethat indirect tissue damage is subject to the local bloodsupply and blood vessel distribution.
Histological changes in blood vessel wallsFigure 3a shows a light micrograph of a healthy liver
blood vessel wall. The endothelium, smooth muscle andcollagen fiber can be seen. In sections stained with VG,nuclei of endothelial cells appear black, smooth musclesappear yellow, and collagen fibers appear bright red. Figure3b shows that, 24 h after the ultrasound exposure, torn
850 Ultrasound in Medicine and Biology Volume 25, Number 5, 1998
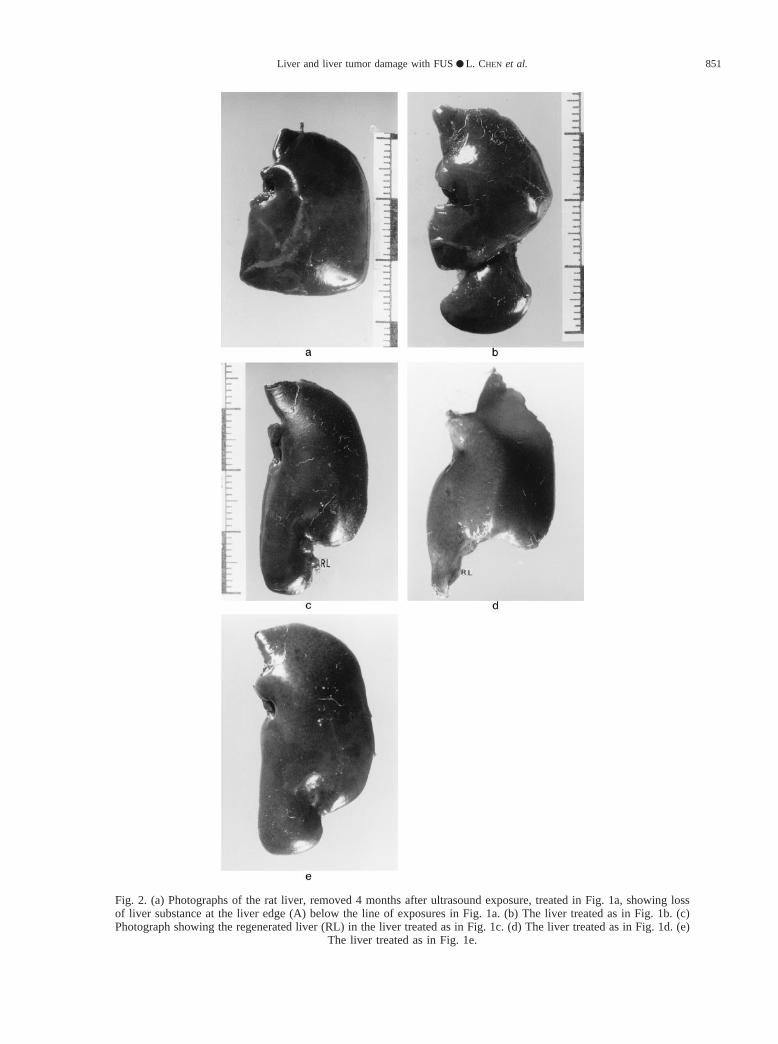
Fig. 2. (a) Photographs of the rat liver, removed 4 months after ultrasound exposure, treated in Fig. 1a, showing lossof liver substance at the liver edge (A) below the line of exposures in Fig. 1a. (b) The liver treated as in Fig. 1b. (c)Photograph showing the regenerated liver (RL) in the liver treated as in Fig. 1c. (d) The liver treated as in Fig. 1d. (e)
The liver treated as in Fig. 1e.
Liver and liver tumor damage with FUS● L. CHEN et al. 851
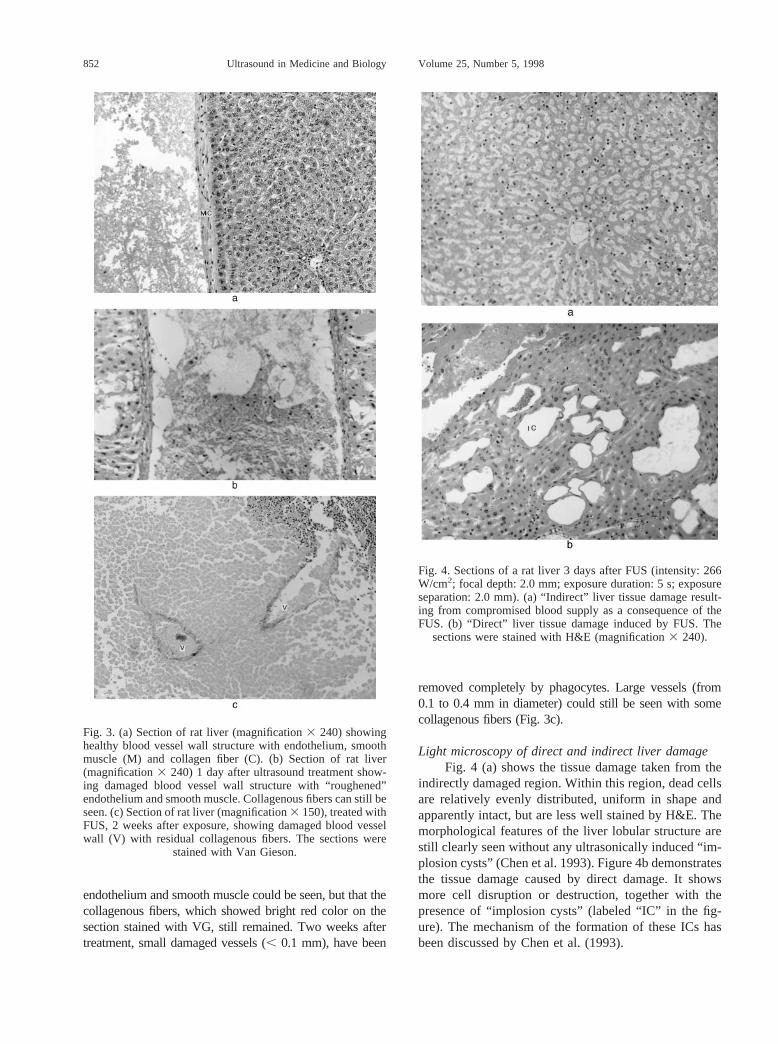
endothelium and smooth muscle could be seen, but that thecollagenous fibers, which showed bright red color on thesection stained with VG, still remained. Two weeks aftertreatment, small damaged vessels (, 0.1 mm), have been
removed completely by phagocytes. Large vessels (from0.1 to 0.4 mm in diameter) could still be seen with somecollagenous fibers (Fig. 3c).
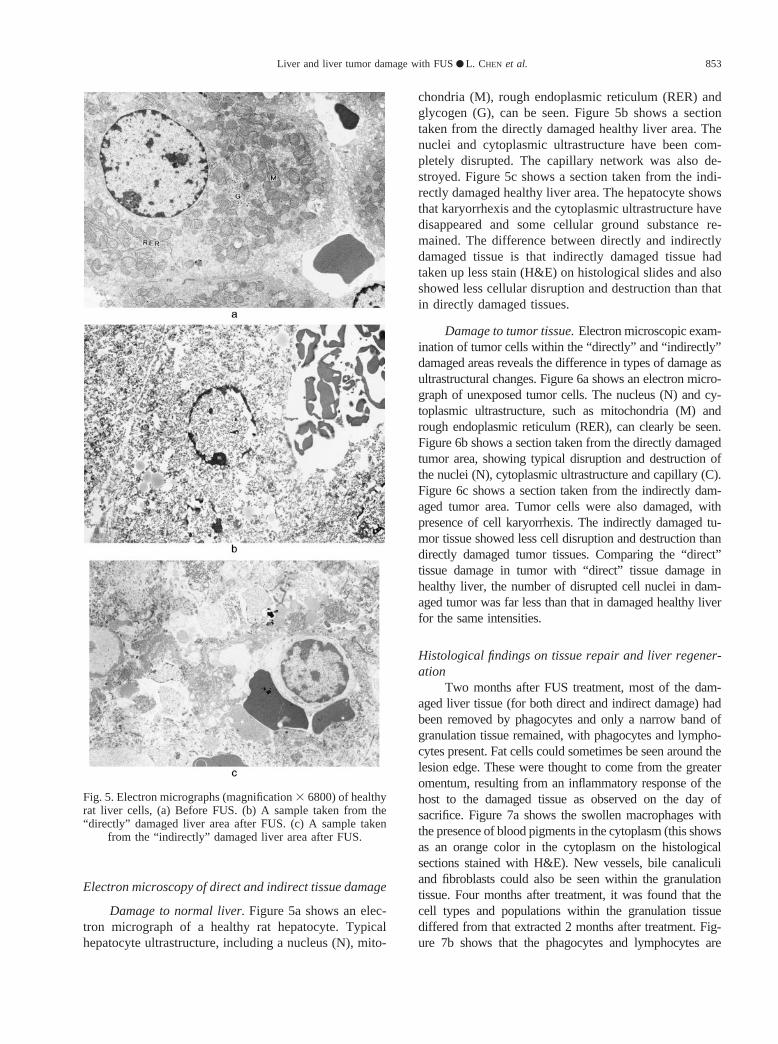
Light microscopy of direct and indirect liver damageFig. 4 (a) shows the tissue damage taken from the
indirectly damaged region. Within this region, dead cellsare relatively evenly distributed, uniform in shape andapparently intact, but are less well stained by H&E. Themorphological features of the liver lobular structure arestill clearly seen without any ultrasonically induced “im-plosion cysts” (Chen et al. 1993). Figure 4b demonstratesthe tissue damage caused by direct damage. It showsmore cell disruption or destruction, together with thepresence of “implosion cysts” (labeled “IC” in the fig-ure). The mechanism of the formation of these ICs hasbeen discussed by Chen et al. (1993).
Fig. 3. (a) Section of rat liver (magnification3 240) showinghealthy blood vessel wall structure with endothelium, smoothmuscle (M) and collagen fiber (C). (b) Section of rat liver(magnification3 240) 1 day after ultrasound treatment show-ing damaged blood vessel wall structure with “roughened”endothelium and smooth muscle. Collagenous fibers can still beseen. (c) Section of rat liver (magnification3 150), treated withFUS, 2 weeks after exposure, showing damaged blood vesselwall (V) with residual collagenous fibers. The sections were
stained with Van Gieson.
Fig. 4. Sections of a rat liver 3 days after FUS (intensity: 266W/cm2; focal depth: 2.0 mm; exposure duration: 5 s; exposureseparation: 2.0 mm). (a) “Indirect” liver tissue damage result-ing from compromised blood supply as a consequence of theFUS. (b) “Direct” liver tissue damage induced by FUS. The
sections were stained with H&E (magnification3 240).
852 Ultrasound in Medicine and Biology Volume 25, Number 5, 1998
Electron microscopy of direct and indirect tissue damage
Damage to normal liver.Figure 5a shows an elec-tron micrograph of a healthy rat hepatocyte. Typicalhepatocyte ultrastructure, including a nucleus (N), mito-
chondria (M), rough endoplasmic reticulum (RER) andglycogen (G), can be seen. Figure 5b shows a sectiontaken from the directly damaged healthy liver area. Thenuclei and cytoplasmic ultrastructure have been com-pletely disrupted. The capillary network was also de-stroyed. Figure 5c shows a section taken from the indi-rectly damaged healthy liver area. The hepatocyte showsthat karyorrhexis and the cytoplasmic ultrastructure havedisappeared and some cellular ground substance re-mained. The difference between directly and indirectlydamaged tissue is that indirectly damaged tissue hadtaken up less stain (H&E) on histological slides and alsoshowed less cellular disruption and destruction than thatin directly damaged tissues.
Damage to tumor tissue.Electron microscopic exam-ination of tumor cells within the “directly” and “indirectly”damaged areas reveals the difference in types of damage asultrastructural changes. Figure 6a shows an electron micro-graph of unexposed tumor cells. The nucleus (N) and cy-toplasmic ultrastructure, such as mitochondria (M) andrough endoplasmic reticulum (RER), can clearly be seen.Figure 6b shows a section taken from the directly damagedtumor area, showing typical disruption and destruction ofthe nuclei (N), cytoplasmic ultrastructure and capillary (C).Figure 6c shows a section taken from the indirectly dam-aged tumor area. Tumor cells were also damaged, withpresence of cell karyorrhexis. The indirectly damaged tu-mor tissue showed less cell disruption and destruction thandirectly damaged tumor tissues. Comparing the “direct”tissue damage in tumor with “direct” tissue damage inhealthy liver, the number of disrupted cell nuclei in dam-aged tumor was far less than that in damaged healthy liverfor the same intensities.
Histological findings on tissue repair and liver regener-ation
Two months after FUS treatment, most of the dam-aged liver tissue (for both direct and indirect damage) hadbeen removed by phagocytes and only a narrow band ofgranulation tissue remained, with phagocytes and lympho-cytes present. Fat cells could sometimes be seen around thelesion edge. These were thought to come from the greateromentum, resulting from an inflammatory response of thehost to the damaged tissue as observed on the day ofsacrifice. Figure 7a shows the swollen macrophages withthe presence of blood pigments in the cytoplasm (this showsas an orange color in the cytoplasm on the histologicalsections stained with H&E). New vessels, bile canaliculiand fibroblasts could also be seen within the granulationtissue. Four months after treatment, it was found that thecell types and populations within the granulation tissuediffered from that extracted 2 months after treatment. Fig-ure 7b shows that the phagocytes and lymphocytes are
Fig. 5. Electron micrographs (magnification3 6800) of healthyrat liver cells, (a) Before FUS. (b) A sample taken from the“directly” damaged liver area after FUS. (c) A sample taken
from the “indirectly” damaged liver area after FUS.
Liver and liver tumor damage with FUS● L. CHEN et al. 853
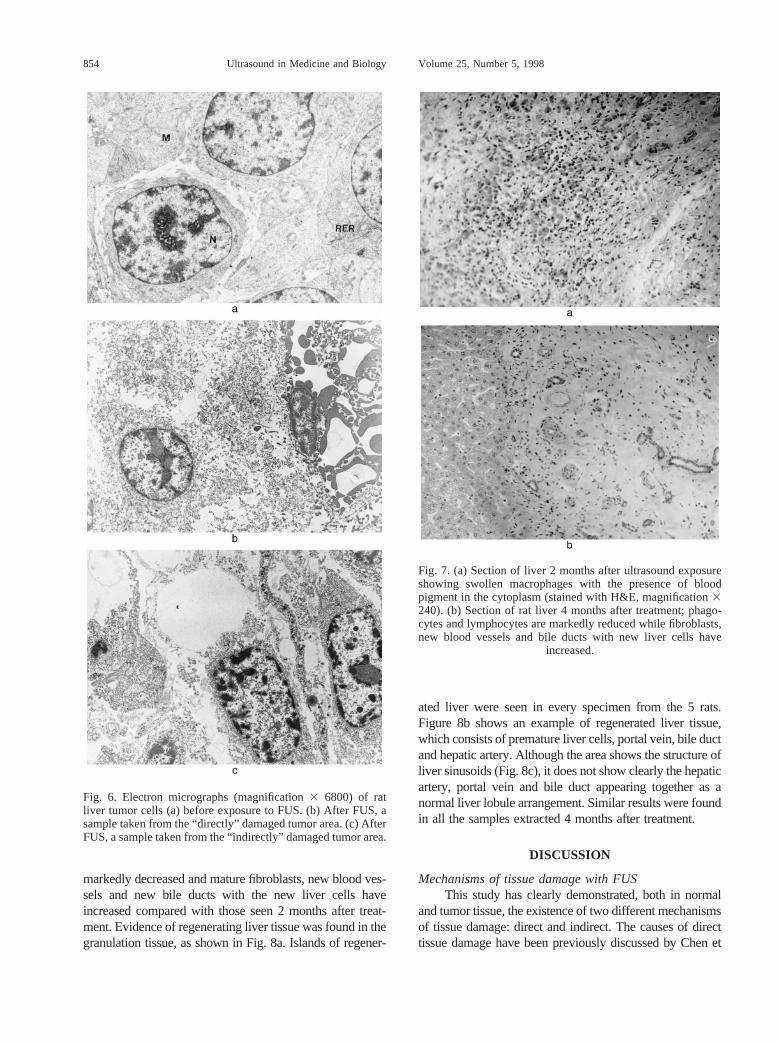
markedly decreased and mature fibroblasts, new blood ves-sels and new bile ducts with the new liver cells haveincreased compared with those seen 2 months after treat-ment. Evidence of regenerating liver tissue was found in thegranulation tissue, as shown in Fig. 8a. Islands of regener-
ated liver were seen in every specimen from the 5 rats.Figure 8b shows an example of regenerated liver tissue,which consists of premature liver cells, portal vein, bile ductand hepatic artery. Although the area shows the structure ofliver sinusoids (Fig. 8c), it does not show clearly the hepaticartery, portal vein and bile duct appearing together as anormal liver lobule arrangement. Similar results were foundin all the samples extracted 4 months after treatment.
DISCUSSION
Mechanisms of tissue damage with FUSThis study has clearly demonstrated, both in normal
and tumor tissue, the existence of two different mechanismsof tissue damage: direct and indirect. The causes of directtissue damage have been previously discussed by Chen et
Fig. 6. Electron micrographs (magnification3 6800) of ratliver tumor cells (a) before exposure to FUS. (b) After FUS, asample taken from the “directly” damaged tumor area. (c) AfterFUS, a sample taken from the “indirectly” damaged tumor area.
Fig. 7. (a) Section of liver 2 months after ultrasound exposureshowing swollen macrophages with the presence of bloodpigment in the cytoplasm (stained with H&E, magnification3240). (b) Section of rat liver 4 months after treatment; phago-cytes and lymphocytes are markedly reduced while fibroblasts,new blood vessels and bile ducts with new liver cells have
increased.
854 Ultrasound in Medicine and Biology Volume 25, Number 5, 1998

al. (1993). In this study, it was found that indirect tissuedamage is strictly due to disruption of the local bloodsupply and is, therefore, dependent on the blood vesseldistribution in the tissue adjacent to the treated volume. Ithas been demonstrated in our previous study that, with thesame focused ultrasound treatment system, the damagedarea was well defined if the focal zone did not include themajor blood vessels supplying the adjacent area (Chen et al.1997). It can been concluded that thermal conductionshould have no significant effect on the tissue damageoutside the focal region in this study. This indirect ultra-sound damage is similar to that reported by Linke et al.(1973) and Rivens (1992), who observed areas of secondaryinfarction in normal rat liver treated with FUS. Clearly, theeffect of indirect tissue damage should be considered inregard to treatment planning for patient cancer treatmentusing focused ultrasound.
In order further to study the difference in tissue dam-age between directly and indirectly damaged tissues, bothdamaged normal liver and tumor tissues were extracted andexamined by electron microscopy. The difference betweenthe directly damaged tissue and indirectly damaged tissue isthe degree of cell disruption and destruction. The number ofdisrupted cell nuclei in directly damaged tumor tissue wasfar less than that in directly damaged normal liver tissue forthe same intensities. It remains to be determined if HSNfibrosarcoma cells are more resistant to ultrasound exposurethan normal liver cells.
Liver regeneration after FUSThe liver has a great capacity for regeneration after
resection, injury, or destruction of its cells, as reported bymany investigators (Becker and Lane 1965; Bucher 1963;Hays 1974; Lane and Becker 1966; Levi and Zeppa 1972).It has been reported that, if a portion of the liver is excisedfrom an experimental animal, the hepatocytes soon undergomitosis and restore the liver to its normal size in a few days.To date, however, there has been no report on liver regen-eration following therapeutic ultrasound treatment.
The evidence of liver regeneration after treatment withFUS has been clearly demonstrated in this paper. Figure 2cand d shows small islands of regenerated liver (RL). Theregenerated liver had a sinusoid structure (Fig. 8c) that ismorphologically similar to the normal liver. However, itdoes not show clearly the hepatic artery, portal vein and bileduct together as a normal liver lobule arrangement. Theregenerating liver tissue appeared morphologically prema-ture compared to the normal liver tissue. Therefore, it isunlikely that these islands of liver tissue could be thenormal liver tissues that had survived the sonication due tothe protection by blood flow from the surrounding vascu-lature. It is unclear if the regenerated young liver will haveall the normal liver functions. It is too early to conclude thatthe treated liver can be completely restored (regenerated) in
Fig. 8. (a) Evidence of regenerating liver cells (L) with newcapillaries, bile canaliculi and fibroblasts. The rat liver wasremoved 2 months after ultrasound treatment (stained withH&E, magnification3 240). (b) Regenerating liver tissue 4months after FUS that consists of liver cells (L), portal vein(V), bile ducts (B) and hepatic artery (A). The sample wastaken from regenerating liver (RL) shown in Fig. 2b: (magni-fication 3 240). (c) Section of rat liver 4 months after FUSexposure showing sinusoid structure in the regenerated livertissue. The section was stained with Reticulin: (magnifica-
tion 3 240).
Liver and liver tumor damage with FUS● L. CHEN et al. 855

terms of its size and function. Although, in this work, thetreated livers were excised either 2 or 4 months after treat-ment, the liver regeneration process seemed to have takenplace at a very slow speed. Presumably, the tissue repair andliver regeneration process after the ultrasound treatment ismore complex than that after surgical excision of a portionof liver. For livers exposed to FUS, the damaged tissues stillremained in the liver lobe. Therefore, necrotic tissue mustbe removed completely before tissue repair by phagocyto-sis, involving polymorphonuclear leucocytes (PMNs), mac-rophages and Kupffer cells. This may have delayed theprocess of liver regeneration. However, it should be men-tioned that there might be significant differences in tissuerepair and regeneration between humans and rats.
Future workThe experimental results obtained from this study are
of significance to the clinical application in treatment ofhepatic metastases with FUS. However, the technique usedfor this study is invasive. In addition, the treated livertumors are much smaller than human liver tumors. Animportant factor in the use of FUS for noninvasive surgeryis the use of high quality imaging techniques to guide andmonitor the tissue damage in real time. The feasibility ofusing magnetic resonance imaging (MRI) for guiding andmonitoring has been investigated by many groups, as pre-viously mentioned. T2-weighted MR imaging seemed to beespecially promising for evaluation of the tissue damage.More recently, it has been demonstrated that the lesion sizesmeasured on T2-weighted MR images correlated well withthe measurements from histology (Chen et al. 1999). Fur-ther vigorous investigation of noninvasive FUS tumor treat-ment on larger animal models, such as pigs, using MRIguidance should be carried out before the technique can beused for clinical trials.
Acknowledgements—This work was supported by program fundingjointly from the UK Cancer Research Campaign and Medical ResearchCouncil to the Physics Department. UK Home Office approval wassought and granted for thein vivo work reported here. We are gratefulto Dr. I. H. Rivens and Sue Clinton for their expert technical assistance.
REFERENCES
Becker FF, Lane BP. Regeneration of mammalian liver. I. Autophago-cytosis during dedifferentiation of the liver cell in preparation forcell division. Am J Pathol 1965;47:783–801.
Bucher NLR. Regeneration of the mammalian liver. Int Rev Cytol1963;15:245–300.
Chen L, Bouley D, Yuh E, D’Arceuil H, Butts K. Study of focusedultrasound tissue damage using MRI and histology. J Magn ResonImaging. 1999 (accepted).
Chen L, Rivens I, ter Haar GR, et al. Histological changes in rat livertumors treated with high-intensity focused ultrasound. UltrasoundMed Biol 1993;19:67–74.
Chen L, ter Haar GR, Hill CR. Influence of ablated tissue on theformation of high intensity focused ultrasound lesions. UltrasoundMed Biol 1997;23:921–931.
Chen L, ter Haar GR, Hill CR, et al. Treatment of implanted rat liver
tumors with focused ultrasound. Ultrasound Med Biol 1998;24(9):1475–1488.
Cline HE, Hynynen K, Hardy CJ, et al. MR temperature mapping offocused ultrasound surgery. MRM 1994;31:628–636.
Cline HE, Hynynen K, Watkins RD, et al. Focused US system for MRimaging-guided tumor ablation. Radiology 1995;194:731–737.
Cline HE, Schenck JF, Watkins RD, et al. Magnetic resonance-guidedthermal surgery. MRM 1993;30:98–106.
Darkazanli A, Hynynen k, Unger E, et al. On-line monitoring ofultrasound surgery with MRI. J Magn Reson Imaging 1993;3:509–514.
Graham SJ, Chen L, Leitch M, et al. Quantifying tissue damage due tofocused ultrasound heating observed by MRI. Magn Reson. Med1999;41:321–328.
Hays DM. Surgical research aspects of hepatic regeneration. SurgGynecolObstet 1974;139:609–619.
Hill CR. Optimum acoustic frequency for focused ultrasound surgery:a general model. Ultrasound Med Biol 1994;20:271–277.
Hill CR, ter Haar GR. Review article: High intensity focused ultrasound-potential for cancer treatment. Br J Radiol 1995;68:1296–1303.
Hill CR, Rivens I, Vaughan MG, et al. Lesion development in focusedultrasound surgery: a general model. Ultrasound Med Biol 1994;20:259–269.
Hynynen K, Chung A, Fjield T, et al. Feasibility of using ultrasoundphased arrays for MRI monitored noninvasive surgery. IEEE TransUltrason Ferroelec Freq Control 1996;43:1043–1052.
Hynynen K, Damianou CA, Colucci V, et al. MR monitoring offocused ultrasonic surgery of renal cortex: experimental and sim-ulation studies. JMRI 1995;5:259–266.
Hynynen K, Darkazanli A, Damianou CA, et al. The usefulness of acontrast agent and gradient-recalled acquisition in a steady-stateimaging sequence for magnetic resonance imaging-guided nonin-vasive ultrasound surgery. Invest Radiol 1994;29:897–903.
Kuc R, Schwartz M, Von Micsky L. Parametric estimation of theacoustic attenuation coefficient slope for soft tissues. IEEE UltrasonSympos Proc 1977;:44–47.
Lane BP, Becker FF. Regeneration of the mammalian liver. II. Surfacealterations during dedifferentiation of the liver cell in preparationfor cell division. Am J Pathol 1966;48:183–196.
Levi JU, Zeppa R. The response of normal rat hepatocytes when exposedto humoral (regenerating) factor. J Surg Res 1972;12:114–119.
Linke CA, Carstensen EL, Frizzell LA, et al. Localized tissue destruc-tion by high-intensity focused ultrasound. Arch Surg 1973;107:887–891.
Malcolm AL, ter Haar GR. Ablation of tissue volumes using highintensity focused ultrasound. Ultrasound Med Biol 1996;22:659–669.
McDannold N, Hynynen K, Wolf D, et al. MRI evaluation of thermalablation of tumors with focused ultrasound. JMRI 1998;8:93–100.
North SM, Styles JM, Hobbs SM, et al. Monoclonal antibodies to ratsarcoma: 1. Immunization procedures and source of lymphoid cellsfor hybridoma production. Immunology 1982;47:397–405.
Rivens IH. Quantitative studies of biological damage induced usinghigh-intensity focused ultrasound. Ph.D. Thesis, University of Lon-don (Institute of Cancer Research) Sutton, Surrey, UK; 1992.
Rowland IJ, Rivens I, Chen L, et al. MRI study of rat liver tumorsfollowing high intensity focused ultrasound surgery. Br J Radiol1997;70:144–153.
ter Harr GR. Ultrasound focal beam surgery. Ultrasound Med Biol1995;20:1089–1100.
ter Haar GR, Rivens I, Andrew V. Phase 1 clinical trial of the use offocused ultrasound surgery for the treatment of soft tissue tumors.SPIE Int Sympos Biomed Optics 1998;3249-31:53–53.
ter Haar GR, Rivens IH, Chen L, et al. High intensity focused ultra-sound for the treatment of rat tumors. Phys Med Biol 1991;36:495–501.
ter Haar GR, Sinnett D, Rivens IH. High intensity focused ultra-sound—a surgical technique for the treatment of discrete livertumors. Phys Med Biol 1989;34:1743–1750.
Walker CL, Foster FS, Plewes DB. Magnetic resonance imaging ofultrasonic fields. Ultrasound Med Biol 1998;24:137–142.
856 Ultrasound in Medicine and Biology Volume 25, Number 5, 1998




![Endoscopic ultrasound-guided biopsy in chronic liver ...scopic ultrasound-guided liver biopsy (EUS-LB) is another method of acquiring liver tissue [8,9]. The feasibility of EUS-LB](https://img.pdfslide.us/doc/110x75/600c40491939a52c585d9ae9/endoscopic-ultrasound-guided-biopsy-in-chronic-liver-scopic-ultrasound-guided.jpg)








![Ultrasound versus liver function tests for diagnosis of ... · [Diagnostic Test Accuracy Review] Ultrasound versus liver function tests for diagnosis of common bile duct stones Kurinchi](https://img.pdfslide.us/doc/110x75/601bcce3144189465e124f14/ultrasound-versus-liver-function-tests-for-diagnosis-of-diagnostic-test-accuracy.jpg)














