Embed Size (px)
Citation preview

HISTOLOGIC ®
Vol. XXXVI, No. 2, December 2003
using an inexpensive and readilyavailable household product thatmay be used as an additive to anytraditional AR solution.
IntroductionThe use of proprietary combinationdewaxing and AR solutions canbecome costly when one considersthat most formalin-fixed tissuesrequire epitope retrieval prior toimmunohistochemical staining formany antigens. While traditionaldewaxing and hydrating solvents arerelatively inexpensive to buy, theypose a potential safety hazard for staffand must be disposed as hazardouswaste that requires compliance withfederal and local laws; this can alsobecome quite costly.
Our laboratory discovered thata readily available householddishwashing liquid may be addedto commonly used antigen retrievalbuffers to create an effective andinexpensive solution that achievessimultaneous dewaxing and antigenretrieval of paraffin sections. Theadditive is prepared by mixing5.0 mL of Dawn® dishwashingdetergent into 1.0 L of deionized
A Novel Approachto Combined Deparaffinizationand Antigen Retrieval for IHC
Gary Ferguson, MT(ASCP); Terri Meetze, MT(ASCP)I;William Armstrong, MD; John B. Carter, MD; Ervin B. Shaw, MD
Lexington Medical CenterWest Columbia, [email protected]
AbstractThe benefits of antigen retrieval (AR) techniques for formalin-fixedparaffin-embedded tissues prior to immunohistochemical (IHC) staininghave been well documented,1 although the actual chemical mechanisms arenot completely understood. Traditional methods of AR are performed ontissues that have been deparaffinized with xylene (or some other paraffinsolvent), and hydrated to water in graded alcohols, after which they areheated to high temperature in a solution of metallic salts or ionic buffer.Various heating sources may be used, some adapted from householdkitchen devices, including the microwave oven, vegetable steamer, orpressure cooker. Even an autoclave may be used. A number of proprietaryproducts now combine deparaffinization and heat-induced epitope retrieval(HIER) in a single solution without the use of organic solvents, offeringenvironmental and work efficiency advantages. The primary drawback tothese commercial dewaxing and AR solutions is their expense andrelatively narrow range of applications. Our laboratory has discovered anovel means for completing dewaxing and heat-induced AR in one step
Managing Editor, Gilles LefebvreScientific Editor, Vinnie Della Speranza,
MS, HTL (ASCP) HT, MT
25
IN THIS ISSUE
A Novel Approach to CombinedDeparaffinization and AntigenRetrieval for IHC ………………………… 25
Troubleshooting Techniques forBielschowsky Silver Stain for SenilePlaques and Neurofibrillary Tangles …… 27
Controls for the Immunohistochemical Staining of Cytology Samples ………… 30
The Gram-Twort Method:A Superior Stain for Bacteria …………… 34
Prion Diseases and Safetyin the Histology Laboratory …………… 36
Mark Your Calendar!Educational Opportunities in 2004 …… 43
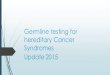
Fig. 1. Estrogen receptor IHC staining in human breast following combined deparaffinization and antigen retrievalwith Dawn® dishwashing detergent. 400X

26
water (0.5%) to create a stockdiluent for AR buffers. In ourlaboratory, we utilize 1 part Dawnbase diluent (0.5%) and 4 partsbuffer to prepare our combinationdewaxing/antigen retrieval solution.This combination solution is usedexactly as one would any antigenretrieval solution, except that slidesare placed into the combinationsolution prior to dewaxing.Immediately following the heatingprocess, sections are placed intopreheated water (which may beheated along with the AR solution),then allowed to cool. The dewaxingby-products remain in the retrievalsolution and are discarded.
The combinations of buffer andadditive solutions are limitless andcan be tailored to meet the antigenretrieval needs of each individuallaboratory. The specific applicationsof the AR solution providing thegreatest performance with eachantibody must be validated byindividual labs and will depend ontissue fixation and staining methodsemployed. Utilizing a countertopelectric pressure cooker, the fol-lowing IHC applications have beenvalidated in our lab using the Dawn(0.5%) additive with Citra® buffer(pH=6.0), or with solutions of Dawnand water only: Calretinin, Ki-67(Mib-1), ER (6F11), PR(PR16),Helicobacter pylori, Her-2-neu,Pan Melanoma cocktail (Mart-1,HMB-45, Tyrosinase), LCA, CD 30(Ber-H2),CD15 (Leu-M1), CD-10,Chromogranin A, Cytokeratin34bE12, S-100, and Vimentin. Theresulting stain intensities and tissuepreservation characteristics rival thebest-performing AR solutions andmethods previously used in ourlaboratory.
MethodsIn order to compare the effectivenessof our newly discovered ARsolution, IHC stains were performedon normal and tumor tissue samplesin triplicate with all of the variousprocedural parameters heldconstant except for the AR solutionused. All of the AR procedureswere carried out using a benchtopelectric pressure cooker. The Citra
and Citra Plus reagents fromBiogenex were received inconcentrate form and diluted withdeionized water to a 10X dilutionfactor before use. The Borg® andReveal® products from Biocarewere received in ready-to-use form.The Dawn base diluent was preparedby adding 5.0 mL to one (1) liter ofdeionized water. To prepare aworking solution of Dawn, one partbase diluent was added to 4 partsdeionized water. Up to 24thoroughly dried slides were placedinto a single plastic Tissue-Tek®
slide carrier holding approximately250 mL of retrieval solution. Thiswas placed into the pressure cookerreservoir along with an equalvolume of deionized water in aseparate dish, surrounded by500 mL of deionized water.Retrieval time was consistently3 minutes at 120°C at approximately20 psi pressure, followed by coolingto 80°-85°C for 15 minutes andrinsing with tap water prior toloading onto the staining instru-ment. All of the stains wereperformed using the VentanaNEXES® automated IHC stainerwith Ventana Enhanced DABdetection reagents. Counterstainingutilized hematoxylin. Other specificprotocol details are described in thetable below.
ResultsThe representative stains fromeach group of AR solutions wereevaluated for tissue preservation,
cell morphology preservation,staining appropriateness withnormal and tumor tissue elements,and signal to background noiseratio. The photomicrographsillustrate a comparable performancewith each of the antibody/tissuecombinations challenged.
ConclusionsAs with all antigen retrievalmethods currently being employedin IHC laboratories, the actualchemical mechanisms at work canonly be theorized. The replacementof organic solvents by detergents isan easily understood effect, withsurfactants acting on liquefiedparaffin. The excellent performanceof this detergent solution in theunmasking or enhancing of tissueantigens may be indicative of thestrong effects of the heating processin the absence of any particularbuffer environment. However, theeffects of the detergent on theantigen sites independent oftemperature cannot be ruled out.In either instance, the use of aDawn dishwashing detergentsolution can provide an effectiveand inexpensive means forcombined deparaffinization andantigen retrieval in one step whenproperly validated in the individualIHC laboratory setting.Dawn® is a registered trademark of Procter & Gamble.
Reference1. Shi S-R,Taylor CR, Gu J. Antigen Retrieval
Techniques: Immunohistochemistry and MolecularMorphology. Eaton Publishing; 2000.
PrimaryIncubation time
Antibody Name Manufacturer (minutes)
Estrogen Receptor Ventana Medical Systems 26
Ki-67 (mib-1) Dako 28
Her-2-neu Dako 32
Pan Melanoma Biocare 28
CD 3 (T-cell) Cell Marque 24
S-100 Ventana Medical Systems 4
CD 30 (Ber-H2) Dako 24
Cytokeratin 34bE12 Dako 32
Chromogranin A Ventana Medical Systems 28
Calretinin Zymed 8
Vimentin Ventana Medical Systems 20
Helicobacter pylori Cell Marque 32

TroubleshootingTechniques forBielschowsky
Silver Stain forSenile Plaques and
NeurofibrillaryTangles
LuAnn Anderson, HT(ASCP)Colleen Forster, HT(ASCP), QIHC
University of MinnesotaDivision of Neuropathology
Minneapolis, [email protected]
AbstractWith the increase in researchdealing with Alzheimer’s disease,the Bielschowsky silver stain hasbecome a routine stain used inmany laboratories. Bielschowskyoriginally introduced the stainin 1902 and its use remainswidespread today. Silver stainingtechniques require very carefulattention to detail for a successfuloutcome. Because of this, it can bedifficult to obtain consistent,reproducible results for one stainfrom run to run. In this study, wewill show some of the commonproblems that may cause staininginconsistencies when using theBielschowsky silver stain method.
IntroductionAlzheimer’s disease is the mostcommon cause of dementia,accounting for approximately60% of known dementia cases.Dementia is a devastating conditionnot only for the patient, but alsothe patient’s family and caregivers.Other diseases can cause dementia,and because there is no antemortemtest that can be used to differentiatethe causes, Alzheimer’s diseasemust be confirmed by postmortemexamination. The Bielschowskysilver stain is the most commonstain used to show the senileplaques and neurofibrillary tangleswhich differentiate Alzheimer’sdisease from other causes ofdementia. Silver stains can be costlyand time-consuming to run. Many
histology technologists becomefrustrated with what appears to besignificant batch-to-batchvariability. Silver stains requiregreat attention to detail andconditions, thus making it difficultto get consistent, reproducibleresults from run to run.
Materials and MethodsModified Bielschowsky Stain.Purpose:To demonstrate nerve fibers andthe presence of neurofibrillarytangles and senile plaques to aidin the diagnosis of Alzheimer’sdisease.
27
Fig. 1. Proper Bielschowsky staining—crisp golden background, nicely stained plaques and tangles. Normal neuronsshow no staining. Human brain, 100X
Fig. 2. Loss of staining and faded background are due to the age of this section (greater than 6 months old).Human brain, 100X

Principle:A preliminary silver impregnationwith silver nitrate is followed byan ammoniacal silver treatment.Silver is deposited on theneurofibrillary tangles and senileplaques and is then reduced tovisible metallic silver (black) bythe action of the formaldehyde
reducing agent. Sections are nottoned with gold chloride, thus agolden background remains.
Fixation:Whole brains are fixed in 10%neutral buffered formalin for2 weeks before sectioning.
Tissue handling:After processing, paraffin sectionsare cut at 6 microns. DO NOT usecharged or coated slides; instead,add about 0.05 g gelatin to waterbath, fill with distilled water, andheat to 40°C. (Adding the gelatinfirst and then filling with waterprevents gelatin from floating onthe top of the water bath anddepositing on slides.) If soakingblocks prior to sectioning, do notuse ammonia to soak. Use plainwater only. Allow slides to air dryovernight before staining. Use onlyglass or plastic slide holders, acid-washed glass coplin jars (seediscussion), and nonmetallicforceps. Run no more than10 slides per batch.
Solutions:20% Aqueous Silver NitrateSilver nitrate (Spectrum Chemicals S1085) …10 gDistilled water ………………50 ml
Make up just prior to use in a clean250 ml flask. This solution shouldbe clear. A cloudy solution isindicative of a glassware problem.Do not use if cloudy.
If solution is not to be usedimmediately, store in the dark.Use for initial staining and thenretain solution.
Ammoniacal SilverTo 50 ml of the silver nitratestaining solution, add FRESHconcentrated ammonium hydroxide(Fisher #A669500) drop by dropuntil precipitate just disappears.Do not add excess ammonia! It isbetter to have a few grains of silverleft at the bottom of the flask.
Ammonia WaterAdd 2 drops of concentratedammonium hydroxide to a coplinjar of distilled water.
DeveloperFormaldehyde(37%-40%) …20 mlDistilled water ………………100 mlConc. nitric acid ……………1 dropCitric acid ……………………0.5 g
28
Fig. 4. Overdevelopment of the Bielschowsky stain, which makes it difficult to distinguish tangles from normalneurons. Human brain, 16X
Fig. 3. The peppering effect in this section is due to silver precipitate and failure of plaques to stain properlywith silver resulting from dirty glassware. Human brain, 160X

Procedure:1. Deparaffinize and hydrate
sections. Rinse all glasswarewell with distilled water beforestaining begins.
2. Stain in 20% silver nitratefor 15 minutes in the dark.Save solution.
3. Put slides into a coplin jar ofdistilled water while doing step 4.
4. Pour silver nitrate back into flaskand add ammonium hydroxidedrop by drop. Mix by swirlingflask until precipitate justdisappears. (A brown precipitatewill form and will disappear withthe addition of ammonia.) Becareful not to add excessammonia. It is better to have asmall amount of silver left in theflask than to use excessammonia. Solution should beclear, not cloudy.
5. Stain slides for 10 minutesin the dark.
6. Remove slides to second coplinjar containing ammonia water.
7. Add 2 drops of developer to theammoniated silver and stir. Putslides into solution and beginchecking by the microscopewhen slides begin to turn brown.Rinse slides in ammonia waterand check staining under themicroscope, watching for plaquedevelopment. Tangles andneurofibrils develop beforeplaques. Rinse in ammonia waterand place back into ammoniatedsilver. Continue checking eachcase every minute or so. Timingof development will vary foreach case, so it is important tocheck each one separately.
When plaques are nicelydeveloped, place slides intocoplin jar of ammonia water.Do not overdevelop or a blackprecipitate will form over theslides and the tissue.Overdevelopment also makes itdifficult to distinguish tanglesfrom normal neurons.
8. Rinse slides in ammonia water,followed by a rinse in distilledwater.
9. Dehydrate, clear, and coverslipimmediately. Do not leave slidesin xylene. This method uses two
changes of fresh xylene, 30 dipseach. Coverslip immediately.
ResultsAxons …………………………blackNeurofibrils …………………blackPlaques ……………brown to black
DiscussionIt has been found that humidityplays a significant role in theconsistency of this stain. Theammonium hydroxide used instep 4 must be fresh and free ofmoisture. When using oldammonium hydroxide which has
29
Fig. 5. Brown, muddy background staining can result from high humidity, old ammonium hydroxide, or when sectionsare left sitting in xylene too long before coverslipping. Human brain, 16X
Fig. 6. Poor Bielschowsky staining due to high humidity. Note loss of background staining and amyloid plaquesthat do not pick up the silver stain. Human brain, 100X

absorbed atmospheric moisture,one will note that it is necessary toadd more at step 4 in order to clearthe precipitate. At the developmentstep, the silver will tend to precipi-tate onto the tissue before theplaques develop, causing a“peppering” effect. The back-ground often turns a dull brown orgreenish color instead of golden.Humidity can also cause unevenstaining within a section or batchof slides. These things can lead tointerpretation problems. Changingto a new bottle of ammoniumhydroxide will resolve these prob-lems. It is suggested that labs usingthis stain order fresh ammoniumhydroxide often, every 1-3 monthsdepending on humidity levels.Store the bottle in a desiccator tohelp keep moisture out.
Development is another criticalissue with this stain. Individualslides will develop at differenttimes, making it necessary tofrequently check the slides micro-scopically during development.Tangles will appear before plaquesin most cases. It takes a littlepractice to get comfortable withdevelopment, so it is recommendedto start with a known positivecontrol and run the stain severaltimes using that control. This willgive the histotech a feel for whenand how plaques develop, andwhen to stop development.Running too large a batch canlead to overstaining of some slides;that is why a limit of no more than10 slides per run is suggested.Overdeveloping the slides cancause too dark a background,which makes it difficult todistinguish normal neuronsfrom tangles.
Another problem area with allsilver stains is glassware. Allglassware used should be acidcleaned frequently. Fill coplin jarsand flasks used to make upreagents with 50% nitric acid andallow to sit for at least 5 minutes,followed by a long wash in distilledwater. In between acid washings,
use full strength bleach and allowto sit overnight. Wash and rinsewell. Dirty glassware will wreakhavoc with this stain, mainly bycausing silver to precipitateeverywhere. Keep two sets ofglassware, consisting of two squarecoplin jars and a 250 ml flask, touse for Bielschowsky stainingexclusively. The use of charged orcoated slides will cause the silver toprecipitate out, leaving a poorlystained section, but a nicelymirrored slide.
Silver nitrate is light sensitive.Store tightly closed bottle in therefrigerator in the dark. Retain thecardboard sleeve which comes withthe silver nitrate and store openedbottles in there. Because thedehydration and clearing stepsneed to be done rapidly, use freshalcohols and xylenes each day.Coverslip immediately—do notleave in xylene.
While all of this may seem tediousinitially, it becomes easier withpractice. You will begin torecognize how much ammoniumhydroxide is needed in step 4, whenthe ammonium hydroxide needs tobe changed, proper developmenttiming, as well as other nuancesinvolved with silver staining. Withpractice, this staining technique willbecomes less problematic toperform and should take about30-40 minutes from start to finish.By paying close attention to detail,the Bielschowsky silver stain canbe a consistent and reliable methodto aid in the diagnosis ofAlzheimer’s disease.
References1. Powers R, Wilson D. Neuropathological diagnosis of
dementia using silver stains and immunohistochemicaltechniques. J Histotechnol. 1996;19(3):236-240.
2. Sheehan DC, Hrapchak B. Theory and Practice ofHistotechnology. 2nd ed. Columbus, Ohio: BatellePress; 1980:254-255.
3. Bancroft JD, Stevens A. Theory and Practice ofHistological Techniques. New York, NY: ChurchillLivingstone; 1977:256, 259.
Controls for theImmunohistochemicalStaining of Cytology
SamplesEthel Macrea
Ventana Medical SystemsTucson, AZ
IntroductionThere seems to be an increasingneed to stain cytology samples suchas fine needle aspirates (FNA) andnon-GYNs with special stains,immunohistochemistry (IHC), andeven in situ hybridization (ISH).This poses staining challenges forthe laboratory in several ways. Firstand foremost, these cytologysamples are not fixed in routinehistological fixatives such asformalin. Secondly, they are notprocessed into paraffin on a tissueprocessor. In this respect cytologypreps are unique in that they areexcluded from routine tissuepreparation techniques. As a result,the use of formalin-fixed, paraffin-embedded (FFPE) tissue controlsfor the IHC staining of cytologysamples does not in fact control forthe manner in which those samplesare prepared, setting the stage forerroneous staining results. Yet formany labs, FFPE tissues may bethe only controls available tovalidate staining runs. With a littleingenuity, this can be overcome.To begin, one must becomeacquainted with what goes on inthe cytology prepping area.
CytologyCytology preps are often describedas GYNs (the cervical/vaginalPAP), non-GYNs (most bodyfluids, effusions, and expectorants),and FNAs (fine needle aspirates oflesions). GYNs may be thetraditional PAP smear, or the ever-increasing liquid phase PAP. Thelatter are generally collected in afixative solution that has beenformulated to work with specific
30

prepping instruments such as theThinPrep® (Cytyc Corp.,Boxborough, MA) or theAutoCyte® (TriPath Imaging Inc.,Burlington, NC). These instrumentsprepare a uniform monolayerof cells that facilitates slideinterpretation under themicroscope. Non-GYNs are bodyfluids from outside the femalegynecologic tract. They includebladder washes, spinal fluid, urine,pleural fluid, thoracenteses,bronchial lavages, etc. Thesesamples are handled in a varietyof ways, and may differsubstantially from one lab toanother. Samples of body fluidsare often spun down in acentrifuge, after which thesupernatant is decanted and thebutton of concentrated cells is usedto make smears. Specimenpreparation may be carried outeither on one of these instrumentspreviously mentioned, or bycentrifugation, or they may simplybe smeared onto a glass slide.Sputum samples require uniquehandling due to their viscousnature; this comes from thepresence of mucous, which is oftendissolved before smears are made.
FNAs are tissue-like samplesextracted through a thin (20, 23,25, 26 gauge) hollow needleattached to a 10 ml disposablesyringe. A Cameco syringe holderallows for enough vacuum toextract the desired cells. The needleis guided into a lesion withradiologic guidance (such asMRI, CATT, or ultrasound).
Palpable, superficial lesions maybe sampled directly without theneed for radiologic guidance.The needle is inserted in severaldirections in order to fill the coreof the needle with cells, which arethen expelled onto glass slides tomake smears. Afterward, theneedle is rinsed in cytology fixative,typically 95% alcohol.
As in histology, fixing the cells isessential to preserving morphology.
However, fixation methods incytology do not necessarily mimicthose used in histology. There areabout four general methods usedto fix cytology preps: wet fixation,wet fixation followed by air drying,spray fixation, and postfixationafter air drying.1 Cytology fixativesinclude a variety of alcoholsolutions (reagent, isopropanol,and ethanol), carbowax, cytologysprays and hair spray, and fixatives(e.g., Saccomanno) that dissolvethe mucoid substance in sputumsamples.2 A variety of proprietarycytological fixatives arecommercially available.
The unique preparation proceduresemployed for cytology sampleswarrant the use of known positivecontrol cells that have beenprepared in the same manner asthe patient samples for IHCstaining, in order to have validinterpretation of staining results.In the absence of this, the stagemay be set for misinterpretation.IHC laboratories typically employprocedures customized tocompensate for the effects offormalin and paraffin processingwhich may have otherwise maskedtissue antigens, yet it cannot be
assumed that carrying out thesesame strategies for epitoperetrieval in cytology samples willyield valid staining results.
ControlsIdeally, cytology controls should bereadily available in the IHC staininglaboratory, although this is typicallynot the case. Stain protocols must betailored through trial and error toachieve optimal results.
It goes without saying that the bestkind of control material wouldcome directly out of the cytologylab, fixed and prepped in the samemanner as any patient cytologysample. In spite of the volume ofmany of the fluids that come intothe cytology lab, cellularity is oftenscant and unpredictable. The fluidmight be centrifuged or used in amonolayering instrument to makethe initial PAP-stained slides forscreening; after this, there may belittle cellular material remaining.Going back to the original samplemay not produce enough cells ofinterest to provide even a few moreslides, and certainly not the largenumber needed for controls.Additionally, if the sample is rathercellular, it is often submitted for a
31
Fig. 1. Slides of cell lines fixed in various cytology fixatives.

32
cell block, thereby consuming theremainder of the sample. The verynature of cytology samples andhow they are used for evaluationusually eliminates the opportunityfor further use in the making ofcontrol slides.
Making Cytology ControlsThere are several approachesthis author has taken that haveprovided satisfactory results.No matter which approach hasbeen used, there is a fair amountof discovery work required untilthe procedure is ready to beimplemented for routine use.
Collecting cells to use as controls:1. Body fluids, FNAs, and
liquid-based PAPs: These cytologysamples may be pooled to createa batch of cells. For example,liquid phase PAPs known to bepositive for either high risk or lowrisk Human Papilloma Virus(HPV) may be pooled to createa stock of cells to use in makingmore ThinPreps. This will beeffective only if there are samplesof adequate cellularity to permitmaking extra slides to be held foruse as controls. Even then, it isimpossible to ensure that therewill be positive cells on every
slide. For non-GYNs, fluids of thesame type may be pooled as well.For example, sputums known tobe positive for AFB orPneumocystis carinii may bepooled in order to make moreslides. This collection of cellsmay be stored in cytologicalfixative for a limited timedepending on which cytologicalfixative is employed. This will onlysucceed if the cytology staff isvigilant in keeping an eye out forsuitable cases.
2. Cell cultures: Cell lines of specifictumor types may be acquiredthrough the American TypeCulture Collection (ATCC). Theseare received as frozen pellets andneed to be grown up in a specificculture medium. To takeadvantage of this particularopportunity, one needs to haveeither the expertise to grow cellsin culture or access to those whodo. With the right expertise, anearly inexhaustible supply ofcells can be maintained. Withoutit, the cells may starve, be grownin the wrong medium, or becomeovercrowded and die. When thecells are ready to harvest, they canbe introduced into an electrolytesolution for transport to thehistology lab or put directly intothe cytology fixative to be used.However, this approach will belimited by the available resourcesfor growing up and maintainingcell populations. It is imperativeto always replace some cells forfuture needs (see Fig. 1).
3. Solid tissue: Solid tissue presentsa great opportunity for collectingcells to use as cytology controls.An arrangement can be madewith the OR suite to pick upunfixed tissues for this application.Immediately begin grossing thesample and, during this process,cells may be collected fromunfixed solid tumors and organsby scraping very lightly across thesurface of the tissue with the edgeof a scalpel blade. The cells arerinsed off the blade’s edge into anappropriate cytological fixative orelectrolyte solution. A light touch
Fig. 2A, 2B. Cells scraped from a lymphoma placed into various cytological fixatives.
A
B

is required to prevent scraping offlarge sheets of cohesive cells.Another approach is to collectcells by using the same kind ofneedle that is used to performFNAs, expelling the contents ofthe needle into the appropriatecytological fixative. Slides arethen made from this collectionof cells. This latter method isespecially suitable for FNAsas these samples tend to becohesive cells (see Fig. 2A, 2B).
Fixing cells to use for controls:1. An electrolyte solution may be
used to collect the cells prior tosorting them into the cytologyfixatives. This is especially helpfulif more than one application isintended for these cells.
2. It is most important to use theexact fixatives that are being usedin one’s cytology department.Many use 95% ethanol for FNAs,and then proprietary fixatives forThinPreps, air-dried slides, etc.Controls should be fixedaccordingly. Any deviation fromthe way it is done in the cytologylab may result in a difference inIHC staining, compromising theeffectiveness of the control.
3. Once the cells are in fixative,preps can be made.
Preparing control slides:1.Again, it is important to mimic
what is done in the cytology lab.If it is possible to use thecytology instruments to makethe preps, all the better.A number of control slides canbe made from the same sampleof cells and then fixed in avariety of ways (see Fig. 3).
2. A small aliquot may be takenfrom this pooling of cells when acontrol is needed. Or, controlscan be made in advance andstored in the appropriatecytological fixative. If thecytology lab makes slides with aspecific fixative followed by airdrying, one should do the same.Alternatively, if the slides are
sprayed after drying, this tooshould be copied. Air-dried andsprayed slides store well in adesiccator or a box withdesiccant in it.
3. Charged glass slides may beuseful in keeping cells adheredto the glass.
ProtocolsCytology samples that are sprayedwith hair spray or any of the manycytological spray fixatives may needto be soaked in 95% alcohol prior tostaining to remove the spray fixative.Air-dried samples may or may notbe placed in PBS or similar bufferprior to IHC staining. Much of thehandling of these prepared slides isgoing to be dictated by the protocolsto be followed. It is likely that someeffort will have to go into discoveringthe best way to handle the slides.
Protocols often need to be adjustedfor the fixatives being used in thecytology preps, with IHC and ISHbeing the most affected. Theseprotocols include proteolyticenzyme digestions, some antigenunmasking processes, incubationtimes, and blocking steps. In mostapplications, an enzyme digestionstep needed for IHC on paraffinmay be eliminated for the cytologysample. ISH, however, will mostlikely require it, but may be lessthan its paraffin counterpart.Endogenous biotin may be higher insome cytology samples, particularlywith bladder washes, urines, FNAsof kidney, and sometimesretroperitoneal masses. However,this is only an issue if a biotin-streptavidin detection method isused. A biotin blocking kit will easilyremedy this. Endogenous peroxidasemay be an issue with bloody sampleswhen using a horseradish peroxidasedetection method. Block with3% hydrogen peroxide. Endogenousalkaline phosphatase may betroublesome with kidney FNAs, butonly if using an alkaline phosphatasedetection method. This can be easilyblocked with levamisole. Hormonereceptors may still require the sameantigen unmasking that is required
for other markers in fixed, paraffin-embedded material such as Ki67 andP53. In some instances, a clone thatworks well for paraffins may notprove to be suitable for alcohol-based fixatives. Whatever changeswill be needed to accommodatecytology samples are mostlydependent upon the choice ofcytology fixative and the stainingprotocol to be followed. Care mustalso be exercised while staining,since cells tend to shed from theslides and fall into solutions whileperforming IHC staining of cytologyslides. This is not new to cytology butis something the histology sectionusually does not encounter. Reusingsolutions should be done only if theyare filtered after use.
Antigen Retention:Most techs who routinely performIHC are familiar with the concept ofloss of antigenicity. Although thecauses are not clearly understood,experience has taught us that itexists. This also applies to cytologycontrols. It has been this author’sexperience that preps fixed in amethanol-based cytology fixativeversus those fixed in an ethanol-based fixative do not necessarilyretain the same degree ofantigenicity for the same periodof time. When keeping a cache ofcytology slides for IHC purposes,they should be monitored forantigen retention. Once the viabletime frame has been determined fora given set of antibodies, toss out oldslides in favor of new ones. Cytologyfixatives also have their own
33
Fig. 3. A cytocentrifuge (like the Sakura Cyto-Tek®)is used to concentrate cells from body fluids whenpreparing IHC control samples..

influences on antigens, so look at allof the fixatives for their separateimpact on antigenicity. Air drying,compared to being kept wet in acytological fixative, may prove to besatisfactory for some applicationsbut not for others. That was ourexperience. Estrogen receptors (ER)and progesterone receptors (PR) didnot perform reliably on slides thatwere air dried following fixation in95% alcohol, but did fine on slidesthat were prevented from dryingand stored in 95% alcohol. Mostcluster differentiation (CD) markersdid well on air-dried slides. Eachlab’s experience may prove to bedifferent.
RNA:RNA is not robust enough towithstand the test of time or anumber of handling techniques.Personal experience has shown thatRNA was not detectable after airdrying slides, while fixed slides thatwere kept wet remained usable.
ConclusionIt is important to remember thatthe intended use of a control slideis to provide evidence that aprocedure was carried out in aprecise manner. For this reason, acontrol slide verifies the conditionsthat were used to run the patientsamples. These conditions shouldmimic the same handling, fixing,and preparation techniques in orderto give one confidence that theprocedure is optimized. Stainingprotocols that are already in placefor routine histology tissues are notnecessarily optimized to facilitatethe same results with a cytologysample. Fixation, just as withhistology tissues, is a key player inthe preservation of cell morphologyand antigenicity. But fixatives goabout the process of denaturing andpreserving cells in different ways.This, along with the methods usedin slide preparation, exerts influenceon final staining outcomes. Thedemand for extra stainingtechniques to be applied tocytological samples is on the rise.HPV testing and FNAs are leadingthe list, followed by non-GYNs for
tumor markers and hormonereceptors. Since cytology offers a lessinvasive means of gathering cells todetermine pathology, it makes senseto make the most of these whenappropriate. In the long run, thefocus is always on patient care.
References1. Leong AS-Y, James CL, Thomas AC. Handbook
of Surgical Pathology. New York, NY: ChurchillLivingstone; 1996:203.
2. Bancroft JD, Gamble M, eds. Theory and Practiceof Histological Techniques. 5th ed. Philadelphia, Pa:WB Saunders; 2002:621-626.
The Gram-TwortMethod: A Superior
Stain for BacteriaRena Fail, HT(ASCP)
Medical University of South Carolina
Charleston, [email protected]
AbstractThe Gram’s stain remains the mostcommon means of identifying gram-positive bacteria in tissue sections.The quality of the stain is frequentlydependent upon the degree ofexpertise of the technologist; poorjudgment in the differentiation stepcan result in over- or under-differentiation of both gram-positive and gram-negative bacteria.Many solvents used in Gram’s stainprocedures are difficult for smalllaboratories to store or to disposeof safely. The Gram-Twort methodis quick and simple to perform andyields results far superior to othermore commonly performedbacterial stains.
DiscussionFirst published in 1884 by HansChristian Joachim Gram, theoriginal Gram’s stain used anilinegentian violet combined withiodine-potassium iodide to stain
gram-positive bacteria. Alcohol wasused to differentiate the organisms.This procedure enabled Gram torecognize two distinct types ofbacteria. Subsequent methodsvaried largely in the solvent usedfor differentiation. Carl Weigert,for example, proposed the use ofaniline oil in this role. Althoughaniline oil differentiates slowly, it isan extremely hazardous chemicalwith which to work. Brown andBrenn used ethyl ether-acetone todifferentiate the gram-positivebacteria followed by picric acid-acetone to differentiate gram-negative bacteria. In a method stillpopular today, underdifferentiationwith ethyl ether-acetone makes itdifficult to discern gram-positivebacteria from surrounding tissueelements, or to stain the gram-negative bacteria. If over-differentiated with picric acid-acetone, the dye is removed fromthe gram-negative bacteria;underdifferentiation leaves thebackground too busy to makeready identification of gram-negative bacteria possible. Othersolvents used for differentiation areacetone, propanol, methanol,butanol, and dioxane. Methanolwas found to work too quickly;butanol too slowly.
A true Gram’s stain is one that usesiodine which forms a precipitatewith crystal violet in the wall ofgram-positive bacteria. The resultingdye precipitate formed is insolublein water. In gram-positive bacteria,the peptidoglycan layer of the cellmembrane is thicker than in gram-negative bacteria. This thicker layerretards extraction of the dye-iodinecomplex. The thinner peptidoglycanlayer of the gram-negative bacteriais unable to retain the crystal violet-iodine complex when exposed tosolvents.1 This results in slowdecolorization of this group oforganisms.2 A 2% solution of crystalviolet has been found to be the idealconcentration for dependableGram’s stain differentiation. Lowerconcentrations typically result inpoor differentiation. The dye will bereplaced with the counterstain in
34

35
gram-negative bacteria, but at aslower rate.3 Prolonged washes inwater should be avoided.
The Gram-Twort stain is both quickand easy to perform. Neutral redgives a lighter stain to the nucleithan most counterstains employed.4The use of fast green as asecondary counterstain for thebackground elements provides agood contrast for both the crystalviolet and fast red; acetone is lesslikely to overdifferentiate the gram-negative bacteria as may occur withother solvents. Gram-negativebacteria are easily visible (Fig. 1). Incontrast, a Brown and Brenn stain(Fig. 2) makes it difficult to discerngram-negative bacteria stained redwith basic fuchsin against the intensered of the nuclei and background.
GRAM-TWORT STAIN5
Fixation: 10% neutral bufferedformalin
Sections: 3-5 microns
Solutions:Lillie’s Crystal Violet
Crystal violet …………………10 g95% ethanol ………………100 ml
Dissolve the crystal violet in the95% ethanol.
Ammonium oxalate ……………4 gDistilled water………………400 ml
Dissolve the ammonium oxalatein the distilled water. Combine thecrystal violet solution and theammonium oxalate solution, stirfor at least 3 hours, then filter.
Lugol’s Iodine
Iodine ……………………………1 gPotassium iodide ………………2 gDistilled water………………100 ml
Neutral Red/Fast GreenStock Solution
0.2% Fast Green:Fast green ……………………0.1 g95% ethanol …………………50 ml
0.2% Neutral Red:Neutral Red …………………0.9 g95% ethanol…………………450 ml
Cover the 2 solutions and stir forseveral hours; leave standingovernight, then filter. Combinethe two solutions.
Working Neutral Red/Fast GreenSolution
Stock solution ………………15 ml Distilled water ………………45 ml
Mix and use immediately in aclosed coplin jar.
Procedure1. Deparaffinize and hydrate
to water.
2. Lay slide flat and filter Lillie’scrystal violet directly onto slide.Stain for 1 minute.
3. Wash briefly in tap water.
4. Place in Lugol’s iodinefor 1 minute.
5. Drain the slide (do not allow todry) and flood with acetone todifferentiate until no more colorwashes off, 2-5 seconds.
6. Rinse in distilled water.
7. Counterstain with neutral red/fastgreen working solution in a closedcoplin jar for 5 minutes.
8. Rinse briefly in distilled water.
9. Dehydrate quickly, clear, andmount.
ResultsGram-positive bacteria ………blue
Gram-negative bacteria ………red
Nuclei ……………………………red
Collagen, varyingred blood cells, shadescytoplasm …………………of green
Fig. 1. The fast green counterstain provides a lighter background, allowing good contrastwith both gram-positive and gram-negative bacteria. Gram-Twort stain, bacteria controltissue. 1000X
Fig. 2. The dark background staining from the Brown and Brenn technique makes itdifficult to discern gram-positive and gram-negative bacteria. Brown and Brenn stain,bacteria control tissue. 1000X

36
It is important that the slide notbe permitted to dry beforedifferentiation in acetone. If theslide dries, it will greatly lengthenthe differentiation time. Prolongedperiods in ethanol will remove thedyes from both gram-positive andgram-negative bacteria.
References1. Kiernan JA. Histological and Histochemical Methods:
Theory and Practice. 3rd ed. New York, NY: OxfordUniversity Press; 2003:122-123.
2. Humason GL. Animal Tissue Techniques. 3rd ed.San Francisco, Calif: W.H. Freeman and Co; 1972:380.
3. Thompson SW. Selected Histochemical andHistopathological Methods. Springfield, Ill:Charles C. Thomas; 1966:1005-1023.
4. Bancroft JD, Stevens A. Theory and Practice ofHistological Techniques. 3rd ed. New York, NY:Churchill Livingstone; 1990:289-292.
5. Histology methods. University of Bristol, Departmentof Clinical Veterinary Pathology Web site. Available at:http://www.bris.ac.uk/Depts/PathAndMicro.
Prion Diseasesand Safety in the
Histology LaboratoryPhyllis Scalzo, HT(ASCP)
National Prion Disease Pathology Surveillance Center
Case Western Reserve University Cleveland, OH
Prion diseases, or transmissiblespongiform encephalopathies(TSEs), are fatal neurodegenerativediseases found in humans andanimals. TSEs have raised concernsabout public health safety as wellas biosafety in operating rooms,autopsy services, and laboratories,especially the histology laboratory,because of the difficulty inneutralizing their infectious agents,called prions. Formaldehydeprocessing is known to kill virtuallyall infectious organisms but, dueto their unique mechanism, prionsare resistant to conventionalfixatives and decontaminationmethods, posing a serious challengeto the histologist.
It came as a surprise to thescientific community when it was
discovered that prions, theinfectious agent of TSEs, arejust proteins which, unlike bacteriaand viruses, lack nucleic acid.1The process of normal proteinmanufacturing actually beginsin the nucleus of the cell, wherethe genomic DNA, the blueprintfor all proteins, is stored.Messenger RNA, a copy of theDNA blueprint, travels from thenucleus to the cell cytoplasm whereit assembles the amino acidsneeded to build the variousproteins. Normal or cellular prionprotein (PrPC) is made in this way.However, PrPC is destined to betransported to the surface of thecell. Thus, as with all proteins thatare associated with cell membranes,PrPC is actually assembled andundergoes initial modifications inthe endoplasmic reticulum (ER),a cell organelle made of elongatedmembranes. While it is beingassembled, PrPC remains attachedto the membranes of the ER by acomplex molecule made of sugarsand fat called the glycol-lipidanchor. During assembly, sugars arealso attached to PrPC molecules, asPrPC is a glycoprotein. The
presence of sugars generates threemajor forms, called glycoforms, ofPrPC: highly glycosylated (with twosugars attached), intermediate (withone sugar), and unglycosylated(lacking sugars). Next, PrPC istransferred to the Golgi apparatus,another membranous organellesimilar to the ER, where the sugarsare modified to take on their finalconfiguration, and PrPC is readyfor the second leg of its journeyin the cell. Packed in vesiclesformed from the Golgi apparatus,PrPC is carried to the cellmembrane where it is positioned sothat it hangs by the anchor outsideof the cell. This critical locationexposes PrPC to any harmful agentsthat may be present in theextracellular space1 (see Fig. 1).
The basic event that triggers priondiseases is the change in shape orconformation of PrPC. This protein,which is normally flexible andsoluble, is converted into a form,called scrapie PrP or PrPSc, which isrigid and tends to form largeaggregates. Because of thisaggregate-forming property, PrPSc
captures nearby PrPC molecules,
Fig. 1. Diagrammatic representation showing that the main cellular location of the prion protein (PrP) is the cellmembranes, depicted here as a rail-like structure; PrP is attached to the membrane by the GPI (glycosylphosphatidylinositol) anchor and hangs from the cell into the extracellular space; glycans (••) and specialized regions of the prionprotein (depicted in yellow and red) are indicated.

37I n n o v a t i o n y o u c a n t r u s t
Visit our web site at www.sakuraus.com
I n t r o d u c i n g . . .
T h e T i s s u e - T e k ® r e v o l u t i o ni n c l i n i c a l p a t h o l o g y .
Total automation, sophisticated technology—innovating laboratory performance.
Achieve specimen preparation in 2 hours, enabling same-day results.
©2003 Sakura Finetek U.S.A., Inc.

transforming them into copies ofthemselves. Through this process,PrPSc increases in number until itcauses the disease. The mechanismis shared by all prion diseases.
Human prion diseases have aprevalence of one case per1 million of the general population.
They exist in three forms: sporadic,familial (or inherited), andacquired by infection. Sporadicprion diseases are by far the mostcommon, accounting for 85% of allprion diseases. In the sporadicform, the PrPC to PrPSc conversionoccurs spontaneously as a mishapduring protein manufacturing,
which often happens late in life.The familial form, which accountsfor about 15% of prion diseases, isdue to the presence of a defect ormutation in the gene encodingPrPC. The mutated PrP is unstableand, with time, converts into PrPSc,triggering the disease. In the formacquired by infection, PrPSc comesfrom the outside, generally fromcontaminated food or as aconsequence of medical or surgicalinterventions. The iatrogenic formcan be transmitted through theuse of contaminated surgicalinstruments, human-derivedpituitary hormone therapy,and transplants of dura mater(the outer brain covering) andcornea. Approximately 270 prioncases of the iatrogenic form havebeen documented worldwide2
(see Tables 1 & 2).
Most human prion diseases beginclinically at the age of 50-60 yearswith progressive mentaldeterioration that soon becomesassociated with progressiveunsteadiness and clumsiness, visualdeterioration, and myoclonus(muscle twitching). The patient isusually mute and immobile in theterminal stages, and in most casesdeath occurs within months. The
38
Table 1: Classification of Human Prion Disease
Sporadic Creutzfeldt-Jakob Disease (CJD)Fatal insomnia
Familial Creutzfeldt-Jakob Disease(inherited) Fatal familial insomnia (FFI)
Gerstmann-Straussler-Scheinker disease
Acquired by infection Iatrogenic (CJD)Kuruvariant CJD
Table 2: Classification of Animal Prion Disease
Probably all acquired Scrapieby infection Bovine spongiform encephalopathy
Chronic wasting diseaseTransmissible mink encephalopathyTransmissible spongiform encephalopathyof domestic and captive animals
2B2AFig. 2. Histological sections: (A) normal brain tissue; neuronal cell bodies (arrow) and other cells and vessels are separated by neuropil, ie, tissue-containing cell processes;(B) brain tissue from a patient with sporadic Creutzfeldt-Jakob disease (sCJD) (H&E); the tissue shows moderate spongiform degeneration which appears as multiple vacuolesin the neuropil (arrows). 20X

histopathological hallmark of priondiseases is spongiformdegeneration that leaves the brainriddled with many microscopicvacuoles and is typically associatedwith varying degrees of astrogliosisand loss of neurons. In some rarerprion diseases, like fatal familialinsomnia (FFI), spongiformdegeneration may be lacking whileselective neuronal loss and gliosisare prominent. In other diseases,like Gerstmann-Straussler-Scheinker disease (GSS) andvariant Creutzfeldt-Jakob disease(vCJD), amyloid plaquescontaining abnormal PrP areprominent1,2 (see Figs. 2 & 3).
It was known for many years thatabnormal prion protein affectedanimals, but animal prion diseaseswere not considered harmful tohumans. In the 1980s, a priondisease called bovine spongiformencephalopathy, or BSE, affectedcattle in the United Kingdom(UK). Quickly BSE became anepidemic. More than 180,000 headsof cattle were proven to have BSE,but an estimated one to two millioninfected animals unwittinglyentered the market and wereconsumed. The BSE epidemic wasapparently triggered and sustained
by the practice of feeding cattlewith diets enriched in proteinsoriginating from other affectedanimals, most likely cattle andsheep. (Sheep have been knownto carry another prion disease,scrapie, which apparently is nottransmissible to humans.)When the high protein diets werediscontinued, BSE receded.
However, in the mid 1990s, a newprion disease, called variant CJD(vCJD), appeared in the UK.Variant CJD affects humans andappears to be acquired from eatingcontaminated beef1,2 (see Fig. 4).
As of February 2003, 140 cases ofvCJD have been reported—130 inthe UK, 6 in France, and 1 each in
39
Fig. 3. Immunostaining with a monoclonal antibody to PrP: (A) normal brain; normal PrP is undetectable in normal brain; (B) sCJD brain; there is a fine punctate immunostainingcorresponding to small deposits of putative scrapie PrP. 20X. Courtesy of Diane Kofskey.
3A 3B
Fig. 4. Graph representing the time course of the BSE and vCJD epidemics. Note the bimodal incidence of the twodiseases with 8-year separation of the two corresponding peaks. Courtesy of the International Life Sciences Institute.

Italy, Ireland, Canada, and the US.However, in the Canadian and UScases, the diseases were most likelyacquired in the UK. Variant CJDis different from the classical CJDin that it generally begins at amean age of 27 years (range 16-74)with behavioral changes, pain,and abnormal sensations in theextremities. Only in later stagesdo CJD-like signs appear.The mean disease duration is16 months (range 9-38). The
neuropathological changes arecharacterized by spongiosis andthe presence of florid or daisy-likeplaques—PrP-containing amyloidcore surrounded, like petals, byvacuoles (see Fig. 5).
The finding of BSE, and even morethe vCJD, prompted Europeancountries to establish prionsurveillance centers. In 1997, theNational Disease Pathology Centerwas established in Cleveland, Ohio
at Case Western Reserve University,headed by Dr. Pierluigi Gambetti.The goal of the surveillance is tomonitor, characterize, and storeall cases of suspected and provenhuman prion disease which occurin the United States. Moreimportantly, it serves as a centerequipped with highly trained andexperienced personnel accustomedto handling the demands ofworking with infectious material.It is highly recommended by theWorld Health Organization(WHO) to contact the centerwhenever there is a case ofsuspected human prion disease.Although one case has beenreported in Canada, there is noevidence supporting the presenceof BSE in the US, although theextensive testing that led to thediscovery of the disease in othercountries has not been carried outhere. In contrast, chronic wastingdisease (CWD), a disease of deerand elk first observed in the 1960sand recognized as a prion diseasein 1978, is now known to be presentin free range or captive deer andelk in Colorado, Wyoming,Nebraska, South Dakota,Wisconsin, New Mexico, Illinois,Minnesota, Montana, Oklahoma,and Kansas. Concern has beenraised regarding the possibility thatthe prion associated with CWDmight be transmitted to humans ina similar way. However, theexamination of several cases ofprion disease in hunters andregular consumers of deer and elkmeat has yielded no evidence thatCWD is transmitted to humans.
The special characteristicsexhibited by prions require carefulattention to facilities, equipment,policies, and procedures. Earlydetection of potential cases andhaving the essential engineeringcontrols in place are critical toprion risk management.
Routine autopsies and processingof formalin-fixed tissue requirebiosafety level 2 precautions,ie, procedures must be conductedin a dedicated area, preferably
40
Fig. 5. Histological and immunostained section of brain from a patient with variant CJD (vCJD) (H&E).(A) The hallmark of vCJD is the presence of florid plaques (arrow), ie, an amyloid plaque. (B) The immunostainingfor PrP is very intense, especially in the florid plaques surrounded by vacuoles. 20X
5A
5B

inside a biosafety cabinet, andusing absorbent pads to eliminatespread of fixative and othercontaminated liquids.3 Duringprocessing, personnel are requiredto wear disposable garments(nitrile gloves, laboratory coat,apron, and face shield). Formalin-fixed tissue blocks should be placeddirectly into cassettes, thenpostfixed with concentrated(96%-100%) formic acid for 1 hourfollowed by an additional48 hours in 10% buffered formalin.This treatment does notsignificantly affect histologyand immunohistochemistry. If adedicated processor and stainerare not available, processing andstaining are done by hand usingdisposable containers. Duringsectioning of the blocks, excessparaffin is collected in biohazardbags. Coverslipped slides aresoaked for 2 hours in 2N NaOH.Each block is sealed with paraffin,labeled “CJD precaution,” and filedseparately from other cases.3,4
Decontamination requires robustuse of sodium hydroxide. Dry waste(paper towels, disposable garments,excess paraffin) must be disposedin double biohazard bags forincineration. Liquid waste(formalin, alcohol, xylene) is placedin plastic containers with NaOHto a final concentration of 1N. Ingeneral, the use of 1N NaOH and/orautoclaving is recommended for theinstruments that can tolerate suchtreatment. Instruments (forceps,knives, cutting boards, scissors) aresoaked in 25% bleach (1:4 dilutionof commercial bleach) immediatelyafter use, autoclaved at 132oC for4.5 hours, and rinsed in water. Forequipment that can’t be autoclaved:soak overnight or soak in 3 changesof 1N NaOH for 30 minutes each,then rinse copiously with water.Dispose the liquid as biohazardwaste. For contaminated surfacesthat can tolerate NaOH: apply1N NaOH to the surface, allowing15 minutes of contact, and wipewith 0.025M acetic acid, washthoroughly with water and wipesurface dry. If a spill occurs or tissue
comes in contact with a surface,cover the area with paper towelssoaked in 1N NaOH, continuouslykept moist, for 1-2 hours.1-4
The dreaded event, of course,is when tissue that has beenprocessed under normal conditionsis found to be prion positive.It is during these times that caremust be taken to backtrackand begin the arduous taskof decontamination. However,decontamination of largeinstruments (processors andstainers) is not an easy task.It requires a plan incorporatingthe Centers for Disease Control andPrevention (CDC) guidelines andmanufacturer recommendations.Depending on the degree ofcontamination, equipment may haveto be replaced.
Although prion diseases are muchbetter understood and diagnosedtoday, strict adherence to thespecific guidelines established bythe CDC and the World HealthOrganization are imperative whenworking with prion-infected tissue.The National Pathology DiseaseSurveillance Center, available at:www.cjdsurveillance.com, under theguidance of the CDC, is availablefor prompt referral of these cases.
References1. Gambetti P, Peterson B, Parchi P, Chen SC, Capellari S.
In: Prion Biology and Diseases. New York, NY: ColdSpring Harbor Laboratory Press; 1999:509-569.
2. World Health Organization. WHO infection controlguidelines for transmissible spongiformencephalopathies. Department of CommunicableDiseases Surveillance and Response, March 1999.Available at:http://www.cjdsupport.org.au/who_infection_control_guidelines.htm.
3. CDC-BMBL. Prions. Agent summary statements—section VII-D. July 2002. Available at:http://www.cdc.gov/od/ohs/biosafety/bmbly/bmblys7d.htm.
4. Taylor D, Woodgate SL, Atkinson MJ. Inactivation ofthe bovine spongiform encephalopathy agent byrendering procedures. Vet Rec. 1995;137(24):605-610.
41
Sometimes once is not enough.
That’s why Sakura features theHistoLogic® Archives on itsweb site at www.sakuraus.com.Whether you want to reviewrecent advances or decades-oldinnovations in histology, youcan find ample material inour archives.
The HistoLogic® Archivesenable users to access articlesfrom past HistoLogic® issuesdating back to 1971. Just typein a keyword in our archivesearch engine or look up anarticle by subject category.It’s that simple.
The HistoLogic® Archives.Another resource thatdemonstrates Sakuradedication to histology.
AccessHistoLogic®
Archives

Tissue-Tek® Accu-Edge®
Microtome Blades
Fulfill your unique microtome/cryostat needswith the latest advance from Sakura:the Tissue-Tek® Cryo3
®.
• Rapid chamber ozone disinfection withoutexposure to liquid toxic chemicals or residue
• Password-protected chamber access• Customizable system configurations
• Unique Cryomold® method ensures standardizedspecimen orientation and faster sectioning
• Easy-to-use anti-roll rake for technique-independent sectioning
Greater efficiency through constant innovation:the hallmark of all Sakura products, ensuringquality laboratory results with optimum efficiency.
Sakura Finetek USA, Inc.1750 West 214th Street
Torrance, CA 90501 U.S.A.Phone: (800) 725-8723
Innovation You Can Trust
©2003 Sakura Finetek U.S.A., Inc.Visit our web site at www.sakuraus.com
Tissue-Tek® Glas™
Coverslipper
Continuing our traditionof innovation
Tissue-Tek® Cryo3®
Microtome/Cryostat
Tissue-Tek® DRS™ 2000Automated Slide Stainer
Tissue-Tek® VIP™ 5Tissue Processor
Tissue-Tek® SCA™
Automated Coverslipper

43
January 16 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Basic Principles of Fixation”Speaker: Barry Rittman, PhD
Univ of Texas Health Sciences Center at Houston
January 21 National Society for Histotechnology TeleconferenceTitle: “New Innovations for Double and Triple
IHC Stain Technology”Speaker: David Tacha, PhD, HT(ASCP)
Biocare MedicalWalnut Creek, CA
Contact: NSH office (301) 262-6221
February 18 National Society for Histotechnology TeleconferenceTitle: “T&B Staining in Immunohistochemistry”Speaker: Alvin W. Martin, MD, & Sheron Lear, HTL(ASCP)
University of LouisvilleLouisville, KY
Contact: NSH office (301) 262-6221
February 20 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Apoptosis TUNEL IHC on Paraffin & Plastic Sections”Speaker: Frances Swain, HT(ASCP)
University of Arkansas for Medical SciencesLittle Rock, AR
March 6 Arkansas Society for HistotechnologySite: Conway, ARContact: Donna Montague (501) 526-6147
Carolyn Black (501) 686-6539Email: [email protected]
March 17 National Society for Histotechnology TeleconferenceTitle: “Sectioning Artifacts: Causes and Cures”Speaker: Peggy A. Wenk, BA, BS, HTL(ASCP)SLS
William Beaumont HospitalRoyal Oak, MI
Contact: NSH office (301) 262-6221
March 18-20 Tennessee Society for HistotechnologySite: Marriott-Vanderbilt Hotel, Nashville, TNContact: Rhonda Schalk (865) 481-1172Email: [email protected]
March 19 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Tissue Engineering for the Histologist”Speaker: Linda Jenkins, HT(ASCP)
Clemson UniversityClemson, SC
April 15-18 Texas Society for HistotechnologySite: Holiday Inn Park Plaza, Lubbock, TXContact: Donna Willis (817) 878-5644
Cliffa Vaughn (915) 690-6604Email: [email protected]
April 16 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Grossing Procedures for the Histotech”Speaker: Michael LaFriniere PA, HT(ASCP)
Memorial HospitalChattanooga, TN
April 21 National Society for HistotechnologyTeleconferenceTitle: “Basic Methods for Producing High Quality Slides
of Paraffin Embedded Bone”Speaker: Robert A. Skinner, BS, HTL(ASCP)
University of Arkansas for Medical SciencesLittle Rock, AR
Contact: NSH office (301) 262-6221
April 23-24 Colorado Society for HistotechnologySite: Stanley Hotel, Estes Park, COContact: John McGinley (970) 491-3041Email: [email protected]
April 28-30 Iowa, Minnesota, Wisconsin Tri-State MeetingSite: Holiday Inn, Dubuque, IAContact: Judi Stasko (515) 663-7445
Pam Hesch (507) 284-4220Email: [email protected]
April 29 - May 1 Histology Society of OhioSite: Clarion Westgate, Toledo, OHContact: Susan Yoakam (419) 291-3702Email: [email protected]
April 30 - May 1 New York State Histotechnological SocietySite: Holiday Inn, Saratoga Springs, NYContact: Judy LaDuc (518) 897-2247Email: [email protected]
April 30 - May 2 Florida Society for HistotechnologySite: Embassy Suites, Deerfield Beach, FLContact: Jerry Santiago (800) 277-4613 x2874
May 1 Massachusetts Society for Histotechnology Spring SymposiumSite: Boston Symphony HallContact: Jason Burrill (978) 658-6000 x1652Email: [email protected]
May 1-2 Washington State Histology SocietySite: Richland, WAContact: Linda Cherepow (206) 667-1378
Martha Pope (509) 375-2930Email: [email protected]
May 13-14 Illinois Society of HistotechnologistsContact: Marge Horn (312) 791-5486
May 14 ASCP Teleconference12:00 pm Central Time (800) 621-4142Title: “Microwave Technology in the Rapid Processing
of Transplant Biopsies”Speaker: Lillian Antonio
Mount Sinai Medical Center, New York City
May 19 National Society for Histotechnology TeleconferenceTitle: “Staining and Demonstration of Microorganisms”Speaker: M. Lamar Jones, BS, HT(ASCP)
LSU Health Sciences, Shreveport, LAContact: NSH office (301) 262-6221
May 20-22 Michigan Society of HistotechnologistsSite: Crown Plaza, Grand Rapids, MIContact: Paula Bober (313) 745-2540
May 20-24 NSH Region III hosted by Alabama Society for HistotechnologySite: Wynfrey Hotel, Birmingham, ALContact: Rita Humphrey (205) 939-9639
Michael LaFriniere (423) 495-6117Email: [email protected]
May 21 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “A Practical Approach to Image Analysis”Speaker: Donna Montague, MS
University of Arkansas for Medical SciencesLittle Rock, AR
June 3-5 Arizona Society for HistotechnologySite: Grace Inn-Ahwatukee, Phoenix, AZContact: Karen Lahti (480) 857-0977Email: [email protected]
June 3-5 NSH Region II hosted by Maryland Society of HistotechnologistsSite: Holiday Inn Select North, Timonium, MDContact: Terri Decarli (410) 787-4187
Renate Jaacks (410) 879-9012Email: [email protected]
June 4-5 Louisiana Society for HistotechnologySite: Holiday Inn Select, Kenner, LAContact: Jane Goodman (504) 897-8830
June 16 National Society for Histotechnology TeleconferenceTitle: “Peripheral Nerve Biopsies: Anatomy, Useful Stains,
Preparation and Case Examples”Speaker: Jon D. Wilson, MD
William Beaumont Hospital, Royal Oak, MIContact: NSH office (301) 262-6221
June 18 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Transporting Lab Samples—The New Regulations”Speaker: Linda Durbin
EXAKT Technologies Inc.Oklahoma City, OK
(continued on page 44)
√ Mark Your Calendar!Educational Opportunities in 2004

To receive your own copy of HistoLogic,® or to have someone added to themailing list, submit home address to: Sakura Finetek U.S.A., Inc.,1750 West 214th Street, Torrance, CA 90501.
The editor wishes to solicit information, questions, and articles relating tohistotechnology. Submit these to: Vinnie Della Speranza, HistoLogic® Editor,165 Ashley Avenue,Suite 309,Charleston,SC 29425.Articles,photographs,etc,will not be returned unless requested in writing when they are submitted.
PRESORTEDSTANDARD
U.S. POSTAGEPAID
ELMHURST, ILPERMIT #1Sakura Finetek U.S.A., Inc.
1750 West 214th StreetTorrance, CA 90501
HISTOLOGIC ®
44
June 18 ASCP Teleconference12:00 pm Central Time (800) 621-4142Title: “A Guide to Maintenance of Histology Equipment”Speaker: Dawn Truscott, HT(ASCP)
Richard Allan Scientific Co.Kalamazoo, MI
July 16 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Back to Basics: Troubleshooting the H&E Stain”Speaker: Joan Vesey, HT(ASCP)
Richard Allan Scientific Co.Kalamazoo, MI
July 21 National Society for Histotechnology TeleconferenceTitle: “Taking the ASCP Qualification in
Immunohistochemistry (QIHC) Exam”Speaker: Patsy Ruegg, HT(ASCP)QIHC
IHCtech, Inc.Aurora, CO
Contact: NSH office (301) 262-6221
August 20 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Microwave Usage in Today’s Histology Lab”Speaker: Donna Willis, HT/HTL(ASCP)
Harris Methodist HospitalFt. Worth, TX
September 17 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Tissue Culture”Speaker: Gillian Rittman, O.N.C.
University of Texas Health Science CenterHouston, TX
September 18-23 National Society for HistotechnologySymposium/ConventionSite: Toronto, CanadaContact: NSH office (301) 262-6221
October 15 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “In-situ Hybridization for HPV”Speaker: Jerry Santiago, BS, HTL(ASCP)QIHC
Ventana Medical Systems
November 17 National Society for Histotechnology TeleconferenceTitle: “The Necessity and Stages of Team Development”Speaker: H. Skip Brown, BS, HT(ASCP)
Lab Management ConsultantsSt. Louis, MO
Contact: NSH office (301) 262-6221
November 19 University of Texas Health Sciences Ctr/ San AntonioTeleconference 12:00 pm Central Time (800) 982-8868Title: “Optimal Handling Procedures for Skeletal
Muscle Biopsies”Speaker: Vinnie Della Speranza, MS, HTL(ASCP)
Medical University of South Carolina
December 15 National Society for Histotechnology TeleconferenceTitle: “Bloodborne Pathogens: Are You Covered?”Speaker: Maureen Doran, BA, HTL(ASCP)
SIU School of MedicineCarbondale, IL
Contact: NSH office (301) 262-6221
√ Mark Your Calendar!Educational Opportunities in 2004
(cont’d from page 43)