Embed Size (px)
Citation preview

HIPERTENSION ARTERIALY
ARRITMIAS
José Luis SerraJefe
Area de Arritmias y Marcapasos
Sanatorio Allende
Hospital Córdoba

Circulation 2011;123:327-334

CARDIOPATIA HIPERTENSIVA
Patología de HVI Hipertrofia del miocito Fibroblastos: hiperplasian, en miofibroblastos Expansion de colágeno intersticial y perivascular Hipertrofia de celulas musculares lisas de la pared vascular Cambios en densidad capilar intramiocárdica Engrosamiento arteriolar

CARDIOPATIA HIPERTENSIVA
Mecanismos responsables de la HVI
SobrecargaNeurohormonas: SRAA-A, CatecolaminasFactores de crecimientoCitokinas
GENETICA

CARDIOPATIA HIPERTENSIVA
En HTA ocurre con mas frecuencia:
Sin HVI: Ligero incremento de ESV y EVs
Con HVI:Fibrilación Auricular: su incidencia aumenta 40 a 50 % Arritmia Ventricular: incremento hasta 9 vecesFV / MS: mas frecuencia (31 vs 10 %)

MECANISMOS ARRITMOGENICOS EN LA HIPERTROFIA

HIPERTROFIA VENTRICULAR

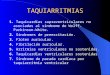
J Am Coll Cardiol 2008;51:802-809Schematic Illustrating How Fibrosis Disrupts Myocyte Coupling
FIBROSIS

MECANISMOS ARRITMOGENICOS EN LA HIPERTROFIA
Hipertrofia Fibrosis miocárdica
Enfermedade coronaria Microangiopatía Disbalance oferta /demanda
Disbalances neurovegetativos Picos hipertensivos Anormalidades metabólicas, hipokalemia
Alteraciones en la:• Conducción• Despolarización• Repolarización• Automatismo aumentado• Actividad gatillada

Ventricular Arrhythmias in Patients with Hypertensive Left Ventricular Hypertrophy
N Engl J Med 1987; 317:787-792
Condición N. Holter. TV no S
HTA con HVI (ECG) 50 14 (28%) *
HTA sin HVI (ECG) 50 4 ( 8%) *
Controles, sin HTA 50 1 ( 2%)
* P < 0,05

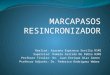
Association Between Persistent Pressure Overload and Ventricular Arrhythmias in Essential Hypertension
Hypertension. 1996;28:284-289
126 HTA esenciales. Holter MAPA Ecocardiograma
EVs en 71%
Lown ≥ 2 vs 0-1: + edad (54 vs 45 a) + tiempo de HTA (5.4 vs 2.8 a), + HVI + hipertensión nocturna

Total PVBs per 24 hours in 126 hypertensive subjects grouped by nocturnal BP reduction and echocardiographic LV hypertrophy (LVH).
Hypertension 1996;28:284-289
Association Between Persistent Pressure Overload and Ventricular Arrhythmias in Essential Hypertension
Hypertension. 1996;28:284-289

HVI y prevalencia de Arritmia Ventricular en Hipertensos. Med Klin (Munich). 2008 Oct 15;103(10):705-11.
192 patients con HTA, HVI, sin enf coronaria. Tipo: Concéntrica, excéntrica, asimétrica Severidad : leve, moderada, severa
Prevalencia de AV por Holter y ergometría
Correlación Si, con severidad No, con tipo de HVI

HTA
HVI
ARRITMIA VENTRICULAR

INDICADORES DE RIESGO DE ARRITMIA y MUERTE SUBITA
Biohumorales: neurohormonas ECG:
• Despolarización:
QRS
Potenciales ventriculares tardios. • Repolarización:
QTc
Dispersión del QT
Microalternancia de la onda T• Balance neurovegetativo
Variabilidad de la FC Imágenes
• Ecocardiografía• RMN

Increased Left Ventricular Mass and Hypertrophy Are AssociatedWith Increased Risk for Sudden Death
J Am Coll Cardiol 1998;32:1454 –9
Framingham Heart Study
3,661 sujetos
>40 a de edad
14 a de seguimiento
Prevalencia de HVI: 21.5%.
HR para MS = 1.45 (IC 95% = 1.10 to 1.92, p = 0.008) por cada 50-g/m de incremento en la masa VI.
60 60 60 M.S.

Cumulative incidence of sudden cardiac death, adjusting for competing risk of death from other causes, in relation to quartiles of baseline QRS duration.
.Eur Heart J 2009;30:2908-2914
QRS duration predicts sudden cardiac death in hypertensive patients undergoing intensive medical therapy: the LIFE study
QRS < 88 ms
QRS > 110 ms

LBBB and CV morbidity and mortality in hypertensive patients with LVH: the LIFE study.
J Hypertens. 2008 Jun;26(6):1244-9.
HTA con HVI
564 pts con BCRI
BCRI: independientemente asociado a:
Muerte CV: HR= + 1.6 (95% IC 1.12-2.27, P < 0.05)
MS: HR= + 3.5 (95% IC 1.89-6.63, P < 0.001)

QT Dispersion and Left Ventricular Hypertrophy in Elderly Hypertensive and Normotensive Patients
ANGIOLOGY 2008 59: 605-612
60 HTA
48 controles
Medición de dispersión de QTc, Arritmias V e HVI
HTA + HVI (P = .006) + dispersión del QTc (P = .004)
Los HVI + incidencia de Lown's score (P < .001), + dispersión del QTc (P < .001).

RESONANCIA MAGNETICA CARDIACA
Marcadora de:
HipertrofiaDilatación, disfunción sistólicaFibrosis

Noninvasive Detection of Fibrosis Applying Contrast-Enhanced Cardiac Magnetic Resonance in Different Forms of Left Ventricular Hypertrophy:
Relation to Remodeling
J Am Coll Cardiol. 2009;53(3):284-291.

HTA, con HVI
+ AV + MS

Es la arritmia per sé un mecanismo importante
en la MS?
La prevención, o la regresión de HVI en HTA:
disminuye la incidencia de MS?

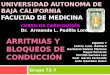
Regression of Electrocardiographic Left Ventricular Hypertrophy During Antihypertensive Therapy and Reduction
in Sudden Cardiac Death . The LIFE Study
Circulation 2007;116:700–705
9193 pts 55 to 80 a, HTA esencial HVI por ECG
Seguimiento medio = 4.8 a
MS = 190 pts (2%)

Figure 1. Kaplan-Meier curves for occurrence of SCD in losartan- and atenolol-treated hypertensive patients with LV hypertrophy.
Circulation 2007;116:700-705
Regression of Electrocardiographic Left Ventricular Hypertrophy During Antihypertensive Therapy and Reduction in Sudden Cardiac Death
The LIFE StudyCirculation 2007;116:700–705

Figure 2. Modified Kaplan-Meier curves showing the rate of SCD according to time-varying presence or absence of ECG LV hypertrophy according to gender-specific Cornell voltage-duration product partitioned at 2000, 2500, and 3000 mm · ms.
Circulation 2007;116:700-705
Regression of Electrocardiographic Left Ventricular Hypertrophy During Antihypertensive Therapy and Reduction in Sudden Cardiac Death
The LIFE StudyCirculation 2007;116:700–705

HTA Y
FIBRILACION AURICULAR

Miocardiopatías Valvulopatía Mitral Hipertensión Arterial Diabetes Hipertiroidismo
Cirugía Cardíaca Cardiopatías Congénitas Pericarditis Enfermedad Pulmonar Solitaria
– Neurogénicas– Inducidas por Taquicardia
SITUACIONES CLINICAS ASOCIADAS A FIBRILACION AURICULAR

“Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates”
38 años de seguimiento en el Estudio Framingham :
• HTA: aumento de riesgo de FA– 1,5 en hombres, – 1,4 en mujeres
• Predictores ecocardiográficos para FA:– Agrandamiento de AI (39% de incremento de riesgo por cada 5-mm )
– Espesor de pared VI (28% por 4-mm incremento).
– Fracción de Acortamiento de VI (34% por 5% decremento)
American Journal of Cardiology, 1998;82: 2N

Incidence of Atrial Fibrillation According to Quartiles of Pulse Pressure Estimates of cumulative incidence of atrial fibrillation according to quartile of pulse pressure.
Mitchell, G. F. et al. JAMA 2007;297:709-715
Presión de Pulso y riesgo de aparición de FAFramingham Heart Study: 5331 => 35 años y libres de FA inicialmente
Incidencia acumulativa de FA a 20 años: 5.6% para una PP < 40 mm Hg 23.3% para una PP > 61 mm Hg

Tsang, T. S. M. et al. J Am Coll Cardiol 2002;40:1636-1644
Age-adjusted cumulative survival without nonvalvular atrial fibrillation (NVAF) by diastolic function profile
Riesgo de FA a 5 años, ajustado a edad:
1%
12%14%
21% .
Olmsted County, Minnesota, población > 65 años
SOBREVIDA LIBRE DE FIBRILACION AURICULARSEGUN FUNCION DIASTOLICA

Vaziri, S. M. et al. Hypertension 1995;25:1155-1160
Bar graphs show age-adjusted prevalence of left atrial enlargement according to 8-year average systolic pressure in men and women
Influencia de la Presión Arterial sobre el tamaño de la Auricula IzquierdaThe Framingham Heart Study
HIPERTENSION ARTERIAL
Y
DILATACION AURICULAR

Vaziri, S. M. et al. Hypertension 1995;25:1155-1160
Bar graphs show age-adjusted prevalence of left atrial enlargement according to 8-year average pulse pressure in men and women
Influencia de la Presión Arterial sobre el tamaño de la Auricula IzquierdaThe Framingham Heart Study

VOLUMEN DE AURICULA IZQUIERDA:
VALOR PRONOSTICO

Tsang, T. S. M. et al. J Am Coll Cardiol 2002;40:1636-1644
Age-adjusted cumulative survival without nonvalvular atrial fibrillation (NVAF) by left atrial volume indexed to body surface area (LAVI)
Olmsted County, Minnesota, población > 65 años
SOBREVIDA LIBRE DE FIBRILACION AURICULARSEGUN VOLUMEN DE AURICULA IZQUIERDA

• Genética• Edad• Factores adquiridos:
– Taquicardia– Anormalidades en Presión /Volúmen– Fibrosis– Inflamación – Isquemia
Aurículas conRemodelamiento eléctrico- estructuralDisparadores Moduladores
SNA Hormonas Medio interno
F.A.
Paroxística
Permanente - Crónica
Persistente
S.R-A-A

Bode, F. et al. Circulation 2000;101:2200-2205
Effect of atrial pressure on AF inducibility and AF duration in isolated rabbit heart during
baseline
Spontaneous AF after pressure increase from 12.5 to 15 cm H2O. Premature depolarizations and runs of nonsustained AF (*) evolved
“Canales activados por estiramiento”Incrementan vulnerabilidad para FA

Effects of Acute Atrial Dilation on Heterogeneity in Conduction in the Isolated Rabbit Heart
S C.M. EIJSBOUTS, M A. ALLESSIE
Incremento agudo de la presión intra-atrial
Activación de los canales activados por estiramientoDesacoplamiento de las uniones gap Deterioro de conducción, líneas de bloqueo
J Cardiovasc Electrophysiol,2003;14:269

Burstein, B. et al. J Am Coll Cardiol 2008;51:802-809
Inter-relaciones entre estiramiento, cardiomiocitos y fibroblastos

S.R-A-A
Presión
DilataciónHipertrofia Fibrosis Inflamación
Alteración en refractariedadconducción
FIBRILACION AURICULAR
HTA

BLOQUEO DEL SISTEMA RENINA-ANGIOTENSINA Y
FIBRILACION AURICULAR

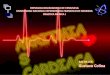
J Am Coll Cardiol 2005;45:712-719
Kaplan-Meier curves illustrating new-onset electrocardiogram-verified atrial fibrillation during follow-up
The Losartan Intervention For Endpoint reduction in hypertension (LIFE)
881 pts, HTA / HVI“Nueva FA”= 290 pts

Gerdts, E. et al. Hypertension 2007;49:311-316
Mean left atrial diameter at baseline and at annual echocardiograms in patients randomly assigned to atenolol- (--) or losartan- (---) based
antihypertensive treatment (*P<0.01 vs baseline within group)
The Losartan Intervention For Endpoint reduction in hypertension (LIFE)
881 ptsHTA, HVI
881 pts, HTA / HVI

JAMA 2006;296:1242-1248
Figure. Rate of New-Onset Atrial Fibrillation Rate is according to time-varying presence or absence of electrocardiographic left ventricular hypertrophy according to sex-specific Cornell voltage-duration product criteria
partitioned at 2440 mm × msec.
The Losartan Intervention For Endpoint reduction in hypertension (LIFE)
831 pts, HTA. HVIPts con regresión o no presencia
= nueva FA en 14,9%o pt-añoPts con persistencia o desarrollo
= nueva FA en 19,0%o pt-año

Schneider, M. P. et al. J Am Coll Cardiol 2010;55:2299-2307
Prevention of Atrial Fibrillation by Renin-Angiotensin System Inhibition.
A Meta-Analysis
J Am Coll Cardiol, 2010; 55:2299

Prevention of Atrial Fibrillation by Renin-Angiotensin System Inhibition.
A Meta-Analysis
Fogari 1= 222 pts con HTA leve, FA previa: Losartan/Amiod vs Amlodipina/AmiodFogari 2= 369 pts con HTA leve, FA previa: Ramipril o Valsartan vs AmlodipinaFogari 3= 296 pts con HTA leve, FA previa y diabetes: Valsartan/Amlodipina vs Atenolol/Amlod
J Am Coll Cardiol, 2010; 55:2299

CONCLUSIONES
HTA: factor de riesgo para arritmias SVs y Vs.
En HTA: factores de riesgo / marcadores de Arritmias: Disfunción diastólica Agrandamiento de AI HVI Ensanchaniento del QRS BCRI
En HTA: La presencia de HVI y de Arritmia Ventricular =
+ riesgo de Mort CV y MS

MUCHAS GRACIAS POR LA ATENCION