Embed Size (px)
Citation preview

HW
Amiowdttpiei
siibgg
tfigttsnMnate
HSPAt
D
A
9
ip Disarticulation and Hemi-Pelvectomyilliam Parrish, MD
citwpct
sdb(pasnauabo
icccpss
pcoiTorcm
IS
DT
mputations through the hip joint or pelvis are most oftenindicated for radical treatment of neoplasia when a pri-
ary malignant soft tissue or osseous tumor of the extremitynvolves several compartments, the sciatic nerve, or the fem-ral neurovascular structures. The goal of these procedureshen performed for neoplastic indications is to provide localisease control. If a primary malignant bone tumor involveshe hip joint or a large portion of the ilium, a hemi-pelvec-omy may be indicated. If the tumor involves only a limitedortion of the pelvis but no neurovascular structures, an
nternal hemi-pelvectomy may be possible to preserve thextremity. Amputations through the hip joint or pelvis resultn very similar functional results.
Less often, such amputations may be required in theetting of vascular catastrophe, such as prosthetic graftnfection or nonhealing of above-knee amputation. Otherndications may include severe trauma with extensiveone or soft tissue loss and neurovascular injury, or ag-ressive infectious diseases such as necrotizing fasciitis oras gangrene.Surgical planning for hip disarticulation or hemi-pelvec-
omy should be based on imaging studies which clearly de-ne the vascular status of the extremity, the anatomic mar-ins of a tumor, or the extent of tissue loss or necrosis fromrauma or an infection. CT scan will provide the best imageso define osseous structures. MRI is most useful for definingoft tissue extension of a tumor, relationship of a tumor toeurovascular structures, and extent of marrow involvement.RI is also helpful in defining the limits of cellulitis or muscle
ecrosis that may occur with aggressive infections. Appropri-te vascular studies such a doppler ultrasound, digital sub-raction angiography, or venography may be useful whenvaluating the patient with vascular disease.
ip Disarticulation:urgical Techniqueositions with all surgical procedures, the operating surgeon must
ake primary and personal responsibility for correct identifi-
epartment of Orthopedics and Rehabilitation, Penn State Hershey MedicalCenter, College of Medicine of the Pennsylvania State University, 500University Drive, Hershey, PA.
ddress reprint requests to Dr. William Parrish, Department of Orthopedicsand Rehabilitation, Penn State Hershey Medical Center, College of Med-icine of the Pennsylvania State University, 500 University Drive, Her-
tshey, PA 17033. E-mail: [email protected]
6 1524-153X/05/$-see front matter © 2005 Elsevier Inc. All rights reserved.doi:10.1053/j.optechgensurg.2005.08.001
ation of the patient and operative site/side. Before position-ng, a regional anesthetic should be introduced and induc-ion of the general anesthetic completed. Epidural anestheticsith an indwelling catheter provide an excellent means ofostoperative pain control. In addition, a regional anesthetican be highly beneficial by reducing the incidence of phan-om pain postoperatively.
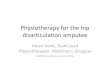
A Foley catheter is placed while the patient is in theupine position. The patient is then moved into a lateralecubitus position and stabilized with the aid of a “beanag” or other similar apparatus (Fig. 1). The operativeipsilateral) side will be facing up. An axillary roll is thenlaced beneath the chest wall in the contralateral axilla tovoid pressure on the brachial plexus and neurovasculartructures. The contralateral arm must be carefully andaturally positioned on an arm board without unusualngulation of any joint or pressure against the radial andlnar nerves. The ipsilateral arm is often best positioned inn overhead cradle with generous padding. Foam pads orlankets should also be used to protect the peroneal nervef the contralateral leg and ankle.It is important to perform the skin preparation and drap-
ng as widely as possible so that the surgical field is notompromised. Failure to “prep and drape” a wide field mayause great difficulty in placing correct incisions, and in-reases the risk of contamination of the surgical field. Patientositioning, skin preparation, and placement of drapeshould be done under the direct supervision of the operatingurgeon or a very trusted associate.
After antiseptic skin preparation, a U-shaped drape islaced under the operative leg as close to the midline glutealleft as possible (while excluding the anus). The anterior armf the drape is brought along the base of the scrotum, extend-ng to the umbilicus and ending at the level of the sternum.he posterior arm of the U-drape extends along the midlinef the spine to the lower margin of the twelth rib. A secondectangular drape is then used to complete the surgical fieldonnecting the two ends of the U-drape along the lowerargin of the rib cage.
ncisionee Figs. 1 and 2.
issectionhe anterior limb of the incision is developed by exposing
he femoral triangle. The femoral triangle is found in the

sveiiitamf
r“Pgtafmwsla
ptsnbpi
cmr
fitrobiamp
owoflrgatttgtio
i
to the
Hip disarticulation and hemi-pelvectomy 97
ubfascial space of the proximal thigh. The femoral artery,ein, and nerve pass through this anatomic area as theyxit the pelvis beneath the inguinal ligament and descendnto the leg. The position of the neurovascular structuresn the femoral canal are nerve, artery, vein, and lymphaticsn a lateral to medial progression (NAVL). The femoralriangle is bounded by the adductor longus muscle medi-lly, the sartorius muscle laterally, and the inguinal liga-ent superiorly. The iliopsoas and pectineus muscles
orm the floor of the femoral triangle (Fig. 2).The most reliable landmark for identification of the femo-
al vessels is the inguinal ligament, specifically the inferiorshelving” edge, sometimes referred to as Poupart’s ligament.articularly in patients with previous arterial surgery in theroin, the inguinal ligament can be the only constant struc-ure. Division of the sartorius muscle at its origin will furtherid in exposing the femoral neurovascular structures in theemoral triangle. Once exposed, the femoral artery and vein
ust be encircled, controlled, and individually suture ligatedith nonabsorbable monofilament suture of 3-0 or larger
ize. The femoral nerve is then gently placed under tension,igated as it exits beneath the inguinal ligament, divided, andllowed to retract into the pelvis.
The greater saphenous vein enters the femoral vein veryroximally and may need to be separately ligated. In addi-ion, the obturator, pudendal, and superficial epigastric ves-els may require separate ligation. The lateral femoral cuta-eous nerve should be identified as it exits the pelvis justeneath the anterior superior iliac spine. This should belaced under gentle traction, ligated, and allowed to retract
Figure 1 Posterior view of patient positioning and placemThe incision for hip disarticulation (dotted line) beginsanterior superior iliac spine (ASIS) and proceeds caudcourses posteriorly within the gluteal crease and then curtubercle. Shown in Fig 2 is the anterior component of thhemi-pelvectomy (solid line), the incision passes postersuperior iliac spine (PSIS). At this point, the incision is dithen posteriorly along the gluteal crease to the ischiumtoward the inferior pubic ramus, continuing on to the pufrom the pubic symphysis, along the inguinal ligament,
nto the pelvis. The round ligament in a woman or spermatic A
ord in a male may be encountered during dissection of theidline part of the incision. These should be exposed but not
esected with the specimen.Once these neurovascular structures have been identi-
ed and divided, the dissection continues through the softissues toward the hip joint. Proceeding anterior to poste-iorly, the iliopsoas muscle is released from its insertionnto the lesser trochanter of the femur. Circumflexranches of the femoral vessels may be encountered dur-
ng the dissection. The pectineus and adductor musclesre transected at their origins on the bony pelvis. Careust be taken to ligate the obturator vessels during thisart of the dissection.As the dissection is carried posteriorly, all the muscles
riginating on the ischium are released at their origin. Thisill include the gracilis and the hamstring muscles. This partf the dissection is most easily completed with the leg in aexed, abducted, and externally rotated position. The poste-ior limb of the incision is then developed by dividing theluteus maximus muscle and releasing the gluteus mediusnd minimus muscles from their insertions on the greaterrochanter. This will provide exposure of the deep posteriorhigh including the sciatic nerve and the short external rota-ors of the hip. The sciatic nerve should be placed underentle traction, securely ligated, divided, and allowed to re-ract proximally beneath the piriformis muscle. The remain-ng external rotator muscles are then released from their fem-ral insertion.Attention is then redirected to the anterior limb of the
ncision. The dissection from the greater trochanter to the
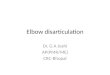
incisions for hip disarticulation and hemi-pelvectomy.ximately one fingerbreadth inferior and medial to theward the greater trochanter. From there, the incisioneriorly within the medial thigh crease to reach the pubicion, extending from the pubic tubercle to the ASIS. Forrom the ASIS along the iliac crest toward the posteriorpostero-laterally to the tip of the greater trochanter, andncision then courses within the thigh crease anteriorly
physis. Figure 2 shows the anterior incision extendingASIS.
ent ofappro
ally toves ante incisiorly frected. The ibic sym
SIS is completed by dividing the tensor fascia lata and re-

lrtlts
CTs
atasantsc
98 W. Parrish
easing the rectus femoris muscle from its origin on the ante-ior inferior iliac spine. The hip capsule is the incised aroundhe lip of the acetabulum, and the hip joint dislocated. Theigamentum teres is divided by electrocautery, completinghe amputation, and allowing removal of the limb from theurgical field.
losurehe surgical field is then thoroughly irrigated and in-
Figure 2 Anterior view of the incisions and deep dissectithe patient’s right side are the incisions for the two procedcourse along the inguinal ligament. For hip disarticulahemi-pelvectomy, it extends to the pubic symphysis befand into the medial thigh crease. Posteriorly, both incisioThe hip disarticulation incision then turns superiorly to ctravels from the greater trochanter superiorly, posteriorlyThe posterior component follows the iliac crest back toside of the patient shows the deep dissection for both hin the chapter text.
pected for hemostasis. The short external rotator muscles a
nd gluteus medius muscles are then approximated withhe obturator externus and iliopsoas muscles to cover thecetabulum. One or two large drains are then placed in theurgical bed and the gluteus maximus flap is mobilizednteriorly with suturing of the gluteus fascia to the ingui-al ligament (Fig. 3). Deep dermal sutures are placed andhe skin is closed with interrupted sutures or staples. Aterile dressing is placed on the wound and may be se-ured with a long six inch elastic wrap that is secured
hip disarticulation and hemi-pelvectomy. Depicted onoth begin at the anterior superior iliac spine (ASIS) ande incision turns posteriorly at the pubic tubercle; forving posterior along the lateral border of the perineum
s within the gluteal crease toward the greater trochanter.directly back to the ASIS. The hemi-pelvectomy incision
edially toward the posterior superior iliac spine (PSIS).IS. These relationships are also shown in Fig 1. The leftticulation and hemi-pelvectomy, as explained in detail
on forures. B
tion, thore curns pasourse, and mthe ASip disar
round the waist.

PTRoftc
drltvt
two laruring o
Hip disarticulation and hemi-pelvectomy 99
ostoperative Carehe drains should be left in place until output is minimal.emoval of the drains too quickly will result in the devel-pment of a seroma in the large space deep to the glutealascia. The epidural catheter should be left in place for 48o 72 hours for pain control. Sustained release oral nar-
Figure 3 Hip disarticulation before closure with the glutewound. Acetabular coverage is obtained by approximatingwith the obturator externus and iliopsoas muscles. One orgluteus maximus flap is then mobilized anteriorly with sut
otic pain medications should be started while the epi- t
ural is in place and should be titrated to the patient’s painequirements as the epidural is weaned. Once the incisionine is completely healed, the patient is referred to pros-hetics to initiate fabrication of prosthesis. A preoperativeisit with a prosthetist can be most helpful for the patiento understand the concept and process of prosthetic fit-
The transected and ligated vessels are seen deep in theort external rotator muscles and gluteus medius musclesge drains can be placed in the surgical bed if desired. Thef the gluteus fascia to the inguinal ligament.
al flap.the sh
ing.

HSPPwPmdtudFtd
wptciiitfddspO
IPofOprtbopa
DTemeoamamtvwatw
4stmtmfi
rmtttsds
bcmswsatd
anpednrniitttm
tspissgcppnt
CTob
100 W. Parrish
emi-Pelvectomy:urgical Techniqueositionositioning the patient for a hemi-pelvectomy is in manyays similar to positioning for a hip disarticulation (Fig. 1).reoperative preparation for this procedure should include aechanical bowel prep on the night before surgery. A beta-ine-soaked vaginal sponge may be packed into the rectumo prevent contamination of the surgical field due to manip-lation of the retroperitoneum during the surgical proce-ure. A stent should be placed in the ipsilateral ureter and aoley catheter in the urinary bladder while the patient is inhe supine position. This makes it easier to identify the ureteruring surgery and decreases the risk of injury to it.The patient is moved into a relaxed lateral decubitus position
ith placement of an axillary roll and appropriate padding ofressure points. For a hemi-pelvectomy, the patient is posi-ioned on the OR table so the flexion break in the table isentered between the lower ribs and the iliac crest. The beds then flexed which opens the space between the ribs andliac crest, making the exposure of the retroperitoneum eas-er. The patient is placed into a relaxed lateral position so thathe trunk and pelvis can be moved forward or backward toacilitate surgical exposure. The arms are positioned and pad-ed as described for hip disarticulation. Skin preparation andraping is performed in similar fashion. Although these stepshould not be delegated to subordinates, the principles ofositioning and preparation should be familiar to the entireR team.
ncisionosterior flap hemi-pelvectomy is the most common variantf this procedure. This method utilizes the gluteus maximusor closure much as was described for a hip disarticulation.ccasionally, a tumor may involve the posterior aspect of theelvis or gluteus maximus, necessitating the use of an ante-ior flap hemi-pelvectomy. The anterior flap hemi-pelvec-omy utilizes an anterior based myocutaneous flap that isased on the femoral vessels. The incision used will dependn the type of flap required. This chapter will describe theosterior flap hemi-pelvectomy. The incisions are outlinednd described in Figs. 1 and 2.
issectionhe dissection begins at the posterior superior iliac spine andxtends anteriorly along the iliac crest and the inguinal liga-ent to the pubic symphysis. The retroperitoneal space is
xposed by releasing the insertion of the abdominal musclesn the iliac crest and inguinal ligament. The peritoneal sacnd contents are retracted medially with the ureter. The com-on iliac artery and vein are identified as well as the internal
nd external iliac vessels. The level of ligation of these vesselsay be determined by the position of the tumor. For a pos-
erior flap hemi-pelvectomy, preservation of the internal iliacessel or at least the first branch (the superior gluteal artery)ill result in better flap viability because the superior gluteal
rtery supplies the gluteus maximus. Once the level of liga-ion is determined, the appropriate vessels are suture ligated
ith monofilament nonabsorbable suture no smaller than t-0. Surgeons not familiar with handling of large vesselshould obtain assistance from a vascular surgeon, especially ifhe vessels are heavily calcified or aneurysmal. The iliopsoasuscle is divided near the inguinal ligament. In most cases,
he iliacus will be included in the surgical specimen and theajority of the psoas muscle preserved. The femoral nerve isnally identified, ligated, and divided (Fig. 2).The perineal dissection is then performed. The bladder is
etracted along with the urethra and protected with a broadalleable retractor. The ischiorectal space is the exposed as
he dissection is extended along the inferior pubic ramus andhe ischium by releasing the muscles of the pelvic floor ashey insert on the boney pelvis. The bladder, urethra, andpermatic cord should be protected during this part of theissection. An osteotome is then used to divide the pubicymphysis.
The posterior segment of the dissection is then completedy extending the incision from the PSIS to the greater tro-hanter, then along the inferior border of the gluteus maxi-us, connecting to the perineal incision and region of dis-
ection. If possible, the gluteus maximus muscle is preservedith the posterior flap; however, it may be necessary with
ome tumors to sacrifice the gluteus maximus to achieve ancceptable surgical margin. This myocutaneous or fasciocu-aneous flap is then developed in an anterior to posteriorirection.As the flap is developed posteriorly, the superior gluteal
rtery should be preserved in those cases using a myocuta-eous gluteus flap. The superior gluteal artery will exit theelvis through the greater sciatic notch and is tightly adher-nt to the bone in this location. Once the posterior flap iseveloped, the deep posterior hip musculature and sciaticerve will be visible. The piriformis muscle is divided toeveal the sciatic nerve as it exits the pelvis. The very largeerve must be firmly ligated, divided, and allowed to retract
nto the pelvis. The inferior gluteal artery will exit the pelvisnferior to the piriformis muscle. This artery should be iden-ified and ligated to avoid bleeding. The thick broad sacro-uberous ligament will then be encountered extending fromhe lateral border of the sacrum to the ischial tuberosity, andust be divided.Once division of the soft tissues and neurovascular struc-
ures are completed, attention is then directed to final step:acral osteotomy. The standard hemi-pelvectomy is com-leted by passing a series of osteotomes through the sacro-
liac joint. A blunt ribbon retractor is placed through theciatic notch into the pelvis along the anterior margin of theacro-iliac joint to protect the anterior structures. The sur-eon then directs the osteotomes serially through the joint toomplete the amputation. The amputation specimen isassed from the surgical field and hemostasis obtained. Theresacral area is highly vascular with great potential for ve-ous bleeding, which must be controlled with suture liga-ures or electrocautery.
losurehe surgical field should then be irrigated with several litersf fluid and closed over large drains. Closure is accomplishedy bringing the gluteus maximus flap forward and suturing
he gluteus fascia to the external oblique and rectus abdomi-
nraptw
CHi
sialbp
SC
Hip disarticulation and hemi-pelvectomy 101
us fasciae of the abdominal wall. Scarpa’s fascia may bee-approximated according to the surgeon’s preference,long with the desired method of skin closure. The rectalacking should be removed and a bulky dressing placed onhe wound, secured with a large elastic bandage around theaist.
onclusionip disarticulation and hemi-pelvectomy procedures result
n major functional disabilities, but do not preclude the re- P
umption of an acceptable quality of life. Aggressive rehabil-tation enables most of these patients to ambulate with fore-rm crutches, which many patients choose in preference to aarge unwieldly prosthesis. Amputation support groups cane instrumental in helping patients make both emotional andhysical adjustments to their disability.
uggested Readinglark MA, Thomas JM: Major amputation for soft-tissue sarcoma. Br J Surg
90:102-107, 2003
az IB: Major palliative amputations. Surg Clin N Am 13:543-547, 2004