Embed Size (px)
Citation preview

A Thesis submitted in conformity with the requirements for the Degree of Master's of Science, Graduate Department of Pharmacology, in the
University of Toronto
PHARMACOTHERAPY OF KELOID SCARS
Copyright O 2000 by Michael Hillmer
Michael Hillmer
National Library 1*1 of Canada Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographic Services senrices bibliographiques
395 Welkgton Street 395, rue Wellington ûttawaON K 1 A W Onawa ON K I A ON4 Canada Canada
The author has granted a non- exclusive licence dowing the National Library of Canada to reproduce, loan, distribute or seli copies of this thesis in microform, paper or electronic formats.
The author retains ownership of the copyright in this thesis. Neither the thesis nor substantial extracts fiom it may be p ~ t e d or othenvise reproduced without the author's permission.
L'auteur a accordé une licence non exclusive permettant à la Bibliothèque nationale du Canada de reproduire, prêter, distribuer ou vendre des copies de cette thèse sous la forme de microfichelnlm, de reproduction sur papier ou sur format électronique.
L'auteur conserve la propriété du droit d'auteur qui protège cette thèse. Ni la thèse ni des extraits substantiels de celle-ci ne doivent être imprimés ou autrement reproduits sans son autorisation.
Phannacotherapy o f Keloid Scars M.Sc., 2000
Michael Hillmer Department of Phmacology, University of Toronto
Abstract
Keloid scars nise from exuberant ussue growth; increased extraceiiular matria (EChI)
production combined with decreased ECM degradation. Dnrkcr-skinnrd people are
predisposed to keloid scars formation. The efficacy of triamcinolone, compared to
mrthylprednisolone, and dexamethasone was rvaluated by their abilitirs to prevent
inflammation induced in rats, as well as in an athymic mousc: modrl. Surgicdly excisrd
human keloid scar Ussue was subcur~nrously implantrd into the micr. The glucocorucoids
(GC) were injrcted into the keloid scar tissue. A histologicai scale was uscd to determine the
efficacies of the GCs in both models. A hydroxyproiine (OH-P) assay was done to
determine the levrls of collagen synthesis in the keloid tissue. No GC ueaunent showed
consistent advanrage in prevention or amelioration of Kcloid scars in thrsr animal models.
Both models are imperfect for solutions to clinical problems and ideally study of novel
Keloid scars therapies should be conducted in patients.
Acknow ledgements
Many people had a hand in bnnging this project to fruition. Kirsten Culver from Dr.
Szechtman's Lab taught me how to perform surgery on rodents. Dr. Shinya Ito translated
an important article from Japanese to English. 1 would like to thank my advisor, Dr. Neil
Shear for his help and advice. The administrative staff at the Centre for Evaluation oi
Medicine al1 contributed to this project. particularly Doris Hutchinson. Dr. MacLeod's
executive assistant.
Dr. Sam Salama generously donated his time and enthusiasm and helped me to l e m
about dermatopathology and assisted in the interpretation of the histology for this project.
I would also like to extend my thanks to The Father Sem O'Sullivan Research Centre
for the scholarship that 1 received from them and for the funding of this project.
My sincerest thanks must go to my supervisor Dr. Stuart MacLeod. Without his guidance
and support, this project would have not been possible. Despite a hectic schedule, Dr.
MacLeod alwûys found time to consult with me and provide valuable advice and wisdom.
List of Figures
Figure 1. Clinical appearance of keloid scars
2. Normal skin histology
3. Keloid histology
4. Structure of collagen
5. Synthesis and formation of collagen fibres
6. Representation of the formation of keloid scas
7. Overview of Factors Leading to Keloid Scars
8. Histology of an untreated keloid scar and a keloid scar treated with triamcinolone
9. Outline of' regulatory mechanisms in place in the hypothalamic-pituitq-adrenal axis
LO. Structures of triamcinolone. methylprednisolone, and dexûmethasone
1 1. Sequence of wound-healing events in an athymic mouse
12. General n t tissue histology - dermis, subcutaneous fat, and skeletal muscle
13. General rat tissue histology
14. Histology of Study 1 : Rat tissue carrageenan- induced inflammatory - 1 .O% one week, 1 .O% two weeks
15. Histology of study 1 : Rat tissue carrageenan- induced inflammatory - 2.0% one week. 2.0% two weeks
Paee
iii
Figure
Histology and qualitative descriptions of study 2: Rat tissue at one week after treatment with triamcinolone. dexamethasone. methylprednisolone, and control
Histology and qualitative descriptions of study 2: Rat tissue at two weeks after treatment with triamcinolone. dexamethasone. rnethylprednisolone. and control
Histology and qualitative descriptions of study 2: Rat tissue rit three weeks after treatment with uiamcinolone, dexamethasone. methylprednisolone, and control
Histology and qualitative descriptions of study 2: Rat tissue at four weeks after treatment with triamcinolone, dexamethasone, methylprednisolone. and control
Keloid histology: control - 2 weeks -keloid implant I . image of calcium deposits within keloid tissue
Keloid histology: rnethylprednisolone 4 weeks - keloid implant 1, image of multinucleated histiocytes (giant cells) present within keloid tissue
Keloid histology: control - 4 weeks keloid implant 1, keloid tissue is largely overtaken by granulation 1 tissue
Keloid histology: methylprednisolone 4 weeks - keloid implant 1, acute inflammation with neutrophils within keloid tissue
24. Keloid histology: keloid implant 1 treated with triamcinolone. dexamethasone. methylprednisolone, and no treatment at two weeks
25. Keloid histology: keloid implant 1 treated with triamcinolone, dexamethasone, methylprednisolone, and no treatment at four weeks
26. Keloid histology: keloid implant 2 treated with triamcinolone. dexarnethasone. methylprednisolone, and no treatment at two weeks
27. Keloid histology: keloid implant 2 treated with uiamcinolone. dexamethasone. methylprednisolone, and no treatment at four weeks
28. Keloid histology: keloid implant 3 treated with triamcinolone. dexamethasone, methylprednisolone, and no treatment at two weeks
29. Keloid histology: keloid implant 3 treated with triamcinolone. dexamethasone. meth y lprednisolone. and no treatment at four weeks
30. Gram stain of keloid implant 1, treated with triamcinolone for 2 weeks and keloid implant 3, treated with dexamethasone for 2 weeks
3 1. Hydroxyproline levels for keloid implants 1,2, and 3 for control, triamcinolone, dexamethasone, and methylprednisolone treatments
32. Average change in mass for athymic mice with keloid implants 1,2, and 3 treated with conuol, triamcinolone, dexamethasone, and methylprednisolone treatments
33. Necropsy report for a rat
34. Necropsy report for an ath p i c mouse
35. Hydroxyproline elution profile
List of Tables
Table Paee Glucocorticoids and their physiological effec ts
Glucocorticoids and their physiological effects on the immune system
Relative Potencies and Equivalenr doses of test glucocorticoids
Outline of Histological Results
Histological sconng of nt histology after one week of control, triamcinolone, methylprednisolone, and dexamethasone
Histological sconng of rat histology after two weeks of control, triamcinolone, methylprednisolone, and dexamethasone
Histological scoring of nt histology after three weeks of control, uiamcinolone. methylprednisolone, and dexamethasone
Histological sconng of rat histology after four weeks of control, triamcinolone, methylprednisolone, and dexarnethasone
Histological sconng from keloid implant 1 treated with trimcinolone, methylprednisolone, dexamethasone and no treatment at two and four weeks.
Paee 10. Histological sconng from keloid
implant 2 treated with triamcinolone. meth y lpredniso lone. dexamethasone and no treatment at two and four weeks.
1 1. Histological sconng from keloid implant 3 treûted with triamcinolone. mcthylprcdnisolonc, dcxamcthasonc and no treatment at two and four weeks.
12. Bacterial infections from individual keloid sections from keloid implant 1
13. Bacterial infections from individual keloid sections from keloid implant 2
14. Bacterial infections from individual keloid sections from keloid implant 3
15. Summary of various studies involving the treatment of keloid scars with glucocorticoids
99
LOO
101
vii
List of Abbreviations
5-HT ACTH ADP AREB ASA CAF CBG CRM ECM ELAM FPD GR GRE HPA ICAM IFN a FNB LFNY IL NSAID PDGF PITC TGF-P TGF-a TNF a
Adrenocorticotropic Hormone Adenosine Diphosphate Animal Research and Ethics Board Acetasalicylic Acid Central Animal Facility Corticosteroid Binding Protein Corticotropin Releasing Hormone Extracellular Matrix Endothelial Leukocyte Adhesion Molecule Fibroproli ferative Disorder Glucocorticoid Receptor Glucocorticoid Responsive Element Hypothalamic-Pituitary- Adrenal Intracellular Adhesion Molecule Interferon Alpha Interferon Beta Interferon Gamma Interieukin Non-Steroidal Anti-Inflammatory Drug Platelet Derived Growth Factor Phen ylisothiocyanate Transforming Growth Factor Beta Transforming Growth Factor Alpha Tumour Necrosis Factor Alpha
List of Abbreviations
Table of Contents
Abstract
Acknowledgements
List of Figures
List of Tables
1
ii
iii
vi
viii
Introduction
Materials & Methods
Results
Discussion
Conciusions
Appendicies
References
Pharmacotherapy of Keloid Scars
Inttoductioa
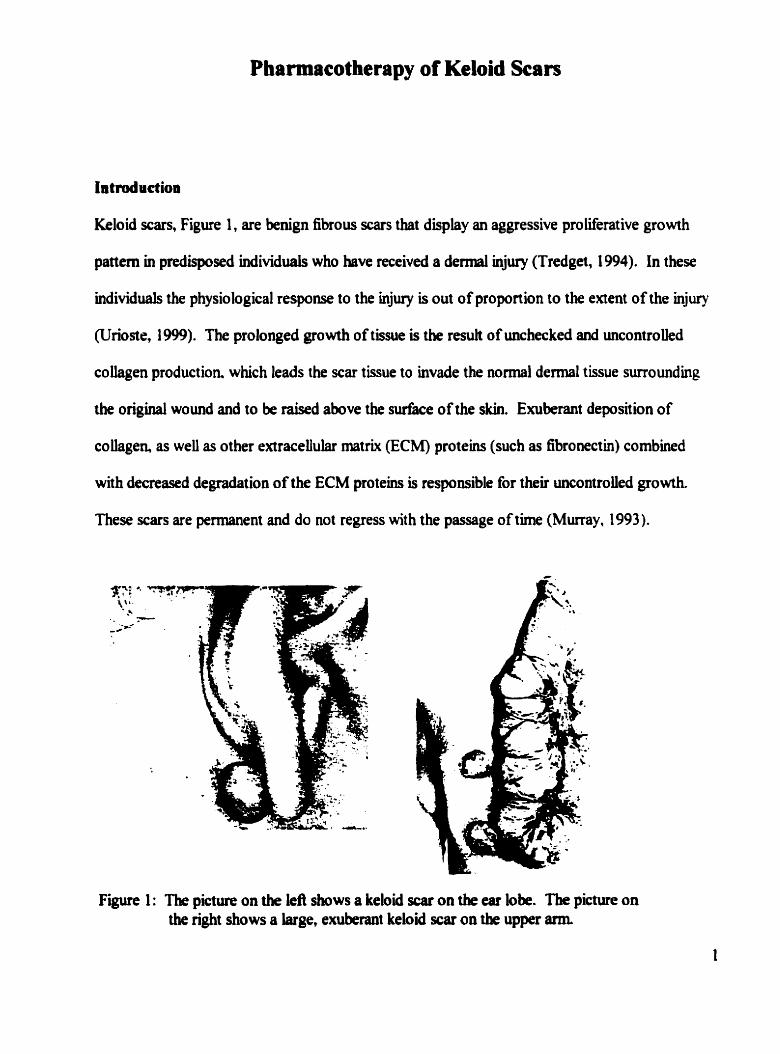
Kcloid scars, Figure 1, are benign fibrous scars that display an aggressive proliferat ive growth
pattern in predisposed individuais who have received a d e d injury (Tredget, 1994). in these
individuals the physiological response to the injury is out of proportion to the extent of the injury
(Urioste, 1 999). The prolonged growth of tissue is the result of unchecked and uncontroiled
coliagen production. which leads the scar tissue to invade the normal d e m l tissue surrounding
the original wound and to be raised above the surface of the skin. Exuberant deposition of
coihgen, as weii as other extracellular matrix (ECM) proteins (such as fibronectin) combined
with decreased degradation of the ECM proteins is responsible for their uncontrolied growth.
These scars are permanent and do not regress with the passage of tirne (Murray, 1993).
Figure 1 : The picture on the kfl shows a keloid s w on the ear lobe. The p i c m on the right shows a large, emiberant keloid scar on the upper arm
Keloid scars are variable in appearance and size, See Figure 1 (Nemeth, 1993). They cm be
mdular or penddous in form and range from the size of a pea to a bulbous m a s which may
spread over an entire shoulder or upper arm. The type of injury does not predict the final
appearance of the scar. The only prediction that can be made is that the scar will begin to form
at the site of injury (Nemeth, 1993).
Spontaneous generat ion of keloids has been reported, however this is an unlikely pathogenesis.
It is safe to assume that because keloids often arise fiom trivial injuries which could easily be
forgotten that the formation is not spontaneous, rather the remit of a minor injury which was not
noticed (Tredget, 1994). The t ime between injury and scar formation c m be highly variable
which also d e s it unlikely that keloid scar formation is spontaneous. Keloid scar tissue can
begin to form at any tirne within a year of injury. or as Oluwasanmi (1974) repris, up to 24
years can elapse before keloids occur.
Retz first wrote about the keloid scar in 1770 and is credited with the first documented
description. Starting in 1817, Aliirt wrote extensiwîy about the keloid scar which he tirst
named "cbancroid". Subsequently he changed the nam of the scar to cheloid (modem spelling:
keloid) (Muir, 1990). However, the Yorubas of Western Nigeria have sculptures dating back to
the 13' century depicting keloid scars. Their cuhure is well acquainted with these scats, which
is documnted by k i r stories and folk meâiciue (Oluwasanmi, J.O., 1974,1979).
These scars are part of a larger M y of conditions known as the fibroproliferative disorders
(FPD), which also incluàes hypertropbic scan and various types of fibrosis (Tredgett, 1994).
The diifference between other members of the FPD W y and keloid scars is that the latter
form afler a wound in the dennis. Whereas, the former occurs at some other site such as the luag
or the kidney. FPDs are non-neoplastic and can resuh in significant morbidity because of theù
exuberant growth. These disordm &are a cornmin ciinicai manifiestation in which they all
display excessive cellular prolûeration leading to uncontroled tissue growth (Tredget, 1994).
Clinicaiiy, keloid SCSUS are identified by their raised appearance, growth beyond the confines of
the original wound and thick glassy coilagen fibres, visible &er histological examination. The
formation of keloid scan is associated with pruritus and pain due to the accumulation of mast
celis (Murray, 1993). Many people who s a e r fiom keloid scars seek treatment because they are
often cosmetically disfigwing and psychologicaiiy damaging, in addition to being pamful
(Datubo-Brown, 1990).
E pidemiology
The epidemiology of keloid formation shows that although individuds of any age can form
keloid scars, the majority of kelo id patients fa11 between the ages of 1 0 end 30 (Murray, 1 993).
ïhe incidence of scarring is higher among dark-skinned people. It has been estimated through
d o m sampling that the incidence of keloid formation ranges iiom 6% to 16% in Atncan
populations (Datubo-Brown, 1 990). Aihady and Sivanantharajah, 1 969, reported that the
incidence of SC- in biacks and Asians is between 5: 1 and 1 5: 1 (Urioste, 1 99)
No statistical difference bas been demonstrateci between the age of onset and mcidence ktween
genders (Murray, 1993). Hospital records show that except for the piilms of hands and soles of
3
fet , every part of the body is susceptible to keloid scarring (Oluwasapmi, 1979). Wound tension
is an important factor in the development of these lesions. Therefore, locations such as the
shoulder or intrascapular area can be more prone to formation of keloids (Oluwasanmi, 1974).
Interestingly, there has never been a reported case of an albino who has developed a keloid scar
(Datub-Brown, 1 990).
Keloids and Hypertrophie Scan
Keloid rars have a closely related member in the FPD family. The hypertrophic scar shares
many of the sarne characteristics with the keloids. It is uiiflear what the exact relationship
between these two types of scars reaily is. Both lesions are very simüar in appearance, which
can make clinical diagnosis very ditncult (Murray, 1994). Each scar is raised above the surface
of the surrounding skin. However an important distinction lies in that keloids extend beyond the
boundaries of the original wound, whereas hypertrophic tissue do not. Keloid scars present with
a deep red or purple appearance, while hypertrophic scars are generdy white or pink in colour.
The latter genedy arise afker severe bums or deep derrnal trauma, whereas the fonner can
develop fiom relatively minor injuries.
A i m b Udicator highlighting the dflerences baween these two scars, despite k i r smiüar
appearance, is the fhct that hypertrophic scars regress naturaiiy over a period of time (Nemeth,
1 993), in contmt to keloid scars, which are not known to amliorate without medical
intervention @atubo-Brown, 1990). These ciifferences make th diagnosis important because of
the resulting implications for treatrnent. There is little need to treat a hypertrophic scar because
surgicd treatment .
Hbtopathoiogy
Th true characterist ic of a keloid scar can only be determined by histological examination
(Eldsas, et cil., 1997). Keloid r a r s appear as nodular, fibroblastic proliferations. The dermis
is ahost completely replaced by broad eosinophilic bundles of collagen. A few fibrobksts and
mucoid ma& are visible between the fibres. Transmission electron rnicroscopy studies show
tbat the vessels at the periphery of the scar are usually partially or completely occluded, leading
to hypoxic conditions within the scar. Kischer & Brody, 198 1, proposed that these
circumstances might lead to the distinctive coüagen nodules or whorls. Unlike hypertrophic
s m , keloids have few or may completely iack any a-smooth muscle actin (Tredget et al..
1997). Hyalinisat ion of the coliagen, a characteristic used for clinical identification of the keloid
scar, is hardly noticeable in the hypertrophic scar (McKee, 1996). Keloid scars are generaily
aceUular, perhaps resulting fiom the actions of apoptosis.
Hypertrophie scars are simüar to keloids in many respects, they show increased colagen b d l e s
tbat d l lie parallel to the epitheiial d a c e . It is important to note that hypertrophic scars do not
possess the wdules that are characteristic of keloid hlstology. The number of fibmblasts is
beased and there is often granulomatous foreign body reaction (Urioste et al., 1 999).
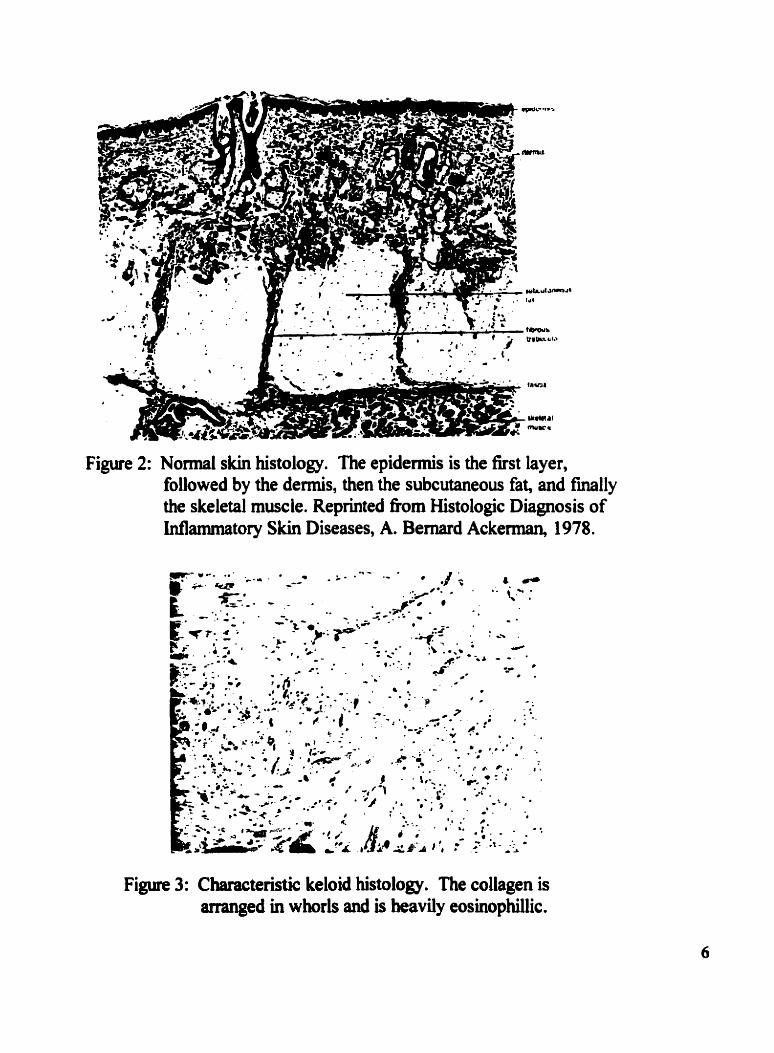
Figure 2: N o d skin histology. The epidermis is the first layer, followed by the dermis, then the subcutaneous fat, and finally the skeletal muscle. Reprinted fiom Histologie Diagnosis of Mammatory Skin Diseases, A. Bernard Ackerman, 1978.
Figure 3: Characteristic keloid histology. The coliagen is arranged in whorls and is heavily eosinophillic.
S Wa Physiology
The skin forxns a non-specific protective M e r over the surface of the exterior of the body. Its
purpose is to protect the body fiom infeçtion, foreign bodies, harmhl sunlight, and to regulate
body temperature. Furthemore, the s b serves to preserve the s t a b i of tbe body's irmer
environment, as weil as providing a physical and mechanical support structure to maintain the
body's inner architecture (CampbeU, 1 993).
Pro tective Ro le
(i) Physicul Bawier
The fist defence is a physical M e r which consists of a double-layered membrane covering the
entire body and is continuous with the mucous membranes of the body's orifices. Most microbes
and Wuses cannot penetrate this M e r d e s s there are abrasions or other breaks in the
continuity of the skkL
(ii) Chernical Burrier
The skin also offers chernical defences, which are contained in its secretions. The secretions
fiom oil and sweat glands have a pH ranging fkom 3-5 m a h g the conditions inhospitable for
many microbes. Saliva, tears, and, mucous also contain dmicrobial enzymes such as
lysozyme which digest the cell walls of many bacteria. The actions of P-Defensin-2 are also an
miportant chernical defeiise agallist extemal pathogens.
Ultrastructure
The skin consists of three broad regions; the subcutaneous layer, the demis, and the epidermis.
(i) Epidennis
The epidermis which consists of many sublayers, is the outermost layer of the skin and is
exposed to the extemal environment. In the basal kyer (the living epidermis), new cells are
constantly b&g reproduced, pusbing older ceiis to the surface. As skin celh move hrther away
fiom their source of nourishrnent, they flatten and shrink. They move out of the basal layer and
lose their nuclei and organelies and become part of the c o d e d layer (the dead epidermis), and
tum into a Weless protein cded keratin.
Afkr serving a bief protective function, the keratinocytes are imperceptibly sloughed. This
process of a living cers evolution, called keratinization, takes about 4 weeks.
Keratinocytes, or dead skin ce%, consthte about 95 percent of the epidermal celis and hct ion
as a barrier, keeping hamiW substances out and preventing water and other essential substances
h m escaping the body. The other 5 percent of epidermal celis are melanocytes, which
manufacture and distriaute rnelanin, the protein that adds pigment to skin and protects the body
h m uhraviolet rays. Skin color is deter- by the amount of protem produced by these ceiis,
not by the nurnkr of melanocytes, which is fhiriy constant in al1 races.
Hair and naits are specidized keratin structures and are considereû part of the epidermis. While
anmials use fur and claws for protection and defense, tkse corresponding stnictures are largely
8
(ii) Demis
The de&, lybg beneath the epidermis, is composed of a m s h of strong elastic fibres
consisting of water, geClike and elsstic materials (prîmarily cokgen and elasth). These two
proteins are responsible for giving skin its strength and elastic properties. The dermai layer is
anchored to the subcutaneous fat below. Embedded in this layer are systems and structures
cornmon to other organs such as lymph channels, blood vessels, nerve fibers, and muscle cells,
but unique to the dermis are hair follicles, sebaceous glands. and sweat glands.
Like the epidermis, the hair foüicle manufactures a keratin structure, hair. These follicles are
found everywhere on the body except for the palms and soles, though moa of the hairs produced
are fine. light hairs that, quite unlike the hair of the scalp, are scarcely visible to the naked eye.
The sebaceous g h d s are attached to the hair follicles and through the follicles excrete an oiiy
substance cailed sebum, which b t h lubricates and
protects the skin. On most of the skin sudiace scbum appears constantly and petceptibly, but in
areas with a higher concentration of sebaceous glands, such as the îace and back, there are wide
variations in the amount of sebum produced.
There are two distinctive sweat-producing glands, the a p o c ~ e and the eccrine. The later glands
are an advanced end extensive system of temperature control. S e v d müüon of these glands are
àistriiuted over the entire body, with the highest concentration in the piilms, soles, forehead, and
lltlderarm~.
Sweat, a dilute salt solution, evaporates fiom the skin's surface to cool the body. Excessive
sweatuig without replacement of lost water can cause heat stroke. E c c ~ e glands sweat in
response to physical activity and hot environmnts, but emotional stress and eating spicy foods
can also cause perspiring.
The dennis also reguktes heat through a network of tiny blood vessels. In hot weather these
vessels dilate to give off heat, causing the skin to flush. In cold weather, they constrict.
conserving heat, causing pailor. The blood in these vessels nourishes the skin and provides
protection for the cellular and fluid systems.
(iii)Submtaneous layer
The subcutaneous layer consists prunarily of îatty tissue. The tissue provides a fiel repository,
in addition to its insulating and protective properties.
The Normal Wound Healing Proeem
The continuity of the body's skin is crucial to our abrüties to prevent infections. Any breach in
this protective M e r presents niany risks kluding mfections, blood los, hbility to regulate
temperature properly, and l o s of internai structure. Therefore, it is not without surprise that the
wound heaiing process acts quickly and efficiently to repair any disturbances in thc skin's
continuity .
HtmoiHarb
The first events to occur d e r a dennal injury lead to the achievement of hemostasis. Damaged
10
blood vessels release red blood celis, as wel as uther constituents. The blood vesseis around the
wound site constrict within a few minutes d e r an injury to reduce the amount of blood lost to
kmrrhage (Mutsaers, et al., 1997).
The rnost important ceil m initiahg the formation of a fibrin plug and achieving hernostasis is
the platelet . The role of the platelets is to promote tissue regeneration. Exposed fibrillar
collagen and locdy generated thrombin are respomibIe for the influx of platelets into the
wound site.
The inconhg platelet s undergo degranulation which releases a hoa of cpo kines (suc h as TGF-
P, TGF-a, PDGF), cellular mediators (such as ADP, thromboxane-A2.5-HT. von Willebrand
factor VIII) and structural components including fibrinogen, firbronectin, and thrombo plasth,
which also act as nucleation sites for further platelet aggregation. These substances released by
degranulatmg platelets are also resonsible for causing the vessels to dilate and hcrease their
permeability (Mut saers, et al., 1 997).
Tbe Clotting Cascade
The extravasation of blood constituents fiom the damaged blood vessels is also responsible for
the initiation of the clotting response mediated by the exthsic and intrinsic pathways. The
response by the intrinsic pathway is tumed on by the exposure of blood to subendothelid tissues
at the wound site. The end product of four reaction SeQuences is the enqme thtombin, which is
nsponsible for converthg fibrinogen to fibria The extriasic pathway is turned on by the
interaction of k t o r VII, a circulatmg glycoprotein, and thromboplastin, which is released by
endothelid celis after injury. This interaction lads to an activated factor W which also leads to
11
the generation of thrombin.
Each of tbese pathways shares a common mechanism for initiation. The damage resulting from
the wound exposes a surface where proemynes can be adsorbed. In the normal cellular
environment, the actions of the proenzymes are pnvented by many inhibitors. When the
proenzyme is adsorbed, an enviroment is created that is diiciently free of inhibitors which
dows the enzymes to exert their physiological response ( M c k , 19%)
The presence of thrombin leads to the conversion of fibrinogen to fibrin by forming a fibrin
matrix. This conversion is what causes coagulation to occur. The matrix is responsible for the
primary hemostasis of the wound, as weil as serving as the scaffolding on which the new
extracellular matrix will be consmcted. The formation of the provisional matrix also serves to
init iate the infiammatory cascade.
Stages of Wound Healing
1) Iafiammatoy Stage
Many of the factors released dutmg hcmostasis are resonsible for inducing the migration of
idammatory cells to the wound site. For example, Hagenïui factor activation leads to the
formation of bradykinin, as weîl as the initiation of the alternative and complement cascades
which are responsible for generating anaphylatoxins C3a anci C5a These molecules increase
vesse1 permeabiiity and attrect neutrophils and monocytes which account for tbe majority of the
white blood ceiis aniving at the injury site. The cytokines and growth factors are also
chernotactic for endothelia1 cells anà nbroblasts. ï he collection of macrophages, fibroblasts, and
newly formed vasculatwe housed within a scafFoldhg of fibronectin, coiîagen, and hyaluronk
acid is referred to as granulation tissue (Mutsaers, et al., 1997).
The infiammatory stage is capable of geneiating a response that is out of proportion to the injury
aad it is because of this overreaction that this stage is responsible for giving rise to the
fibroproliferative disorders Experimental evidence (outiined below) points towards TGF-P as
the principal cause of this overreaction (Border and Ruoslahti 1992).
2) Pmliferative Stage
The proliferative stage is fùrther broken down into re-epithelization, angiogenesis. fibroplasia,
and wormd contraction. Epithelial cek migrate to the wound site within 24 hours of the injury
(Kirsner and Eaglstein, 1993) and are responsible for reestabiishing the epideml barrier. The
composition of the granulation tissue appears to be crucial in ailowing the epitheüal barrier to be
completed. TGF-P and TGF-a both play a role in cellular signahg which promotes epidermal
migration. There are five known isoforms of TGF-P, three of which are expressed by
mammalian ceUs (Roberts and Spom, 1993). TGF-P is responsible for fibroblast chemotaxis.
extraceiiuhr m a t h production (increased collagen deposition), and protease inhiiitor
production. While the exact role of TGF-a in the wound repair process is unknown, it has been
shown to stimulate reepitheiization in animal models which streagthens its potential role in
huma. wound heaüng (Roberts and Spom 1993.)
3) Remodelling Stage
The final event is the remodehg stage where the final shape of the scar tissue is achieved by
synthesizing and degrading ECM proteins (Tredgett, 1994). This phase begins concunently with
the formation of granulation tissue. The new ECM proteins are laid domi at the edge of the
wound site and form a matrix for incomhg celis, such as myofibroblasts, which are responstble
for wound contraction. ûver tirne, more collagen is synthesized and proteoglycans are laid down
to give the skin strength and resistance to deformation (Unoste, 1999).
Collagen is the major structural component of skin. It foms the backùone of the ECM anci the
abüity of fibroblasts, epithelial ceUs, srnooth muscles ceh and myofibroblasts to synthesize new
collagen allows the skin to maintain its inte& (McKee, Pathology of the Sb). There are now
approximately 30 recognized genes that code for coUagen and over 20 distinct coüagen species
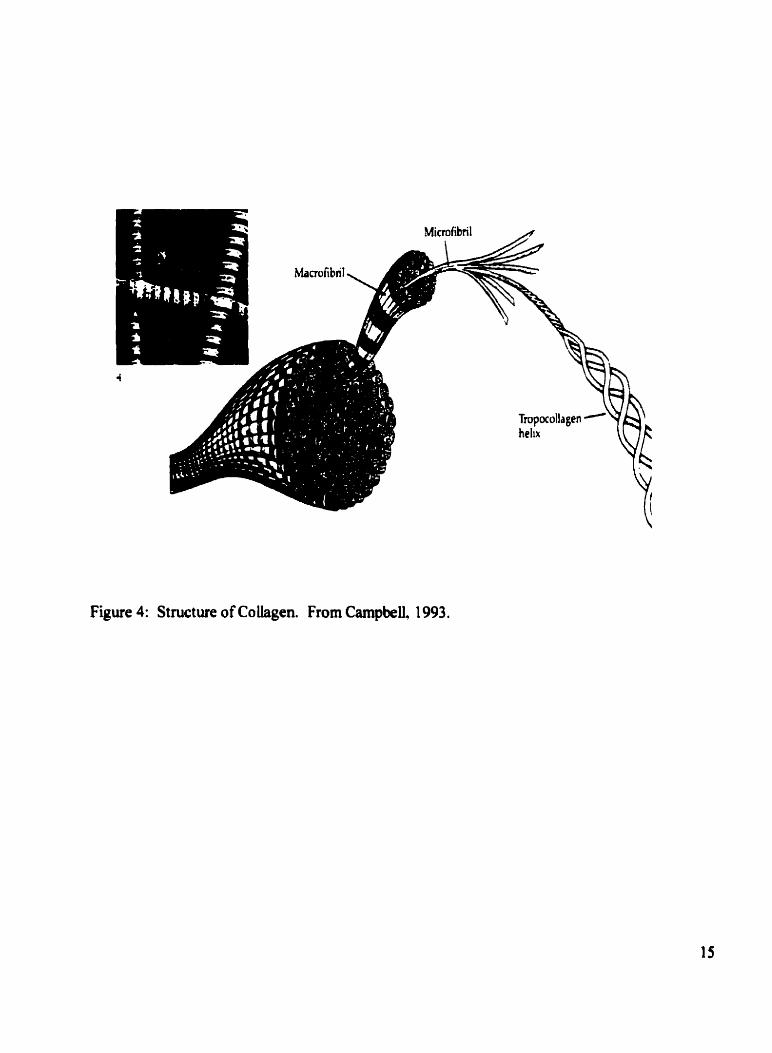
located on seven different chromosomes. Collagen is a right-handed homotrimer with a
molecular weight of 300 000 Daltons (See Figure 4). Each a c h i n is a lefi-handed helix and is
approximately 95 000 Dahons. The general amino acid sequence of the a chain is a repeating
set of three with glycine occupying the third position. The first two sites are variable. but are
often occupied by proline and hydroxyproiine.
Tmpüollagen -Y& helix
Figure 4: Structure of Coüagen. From Campbell. 1993.
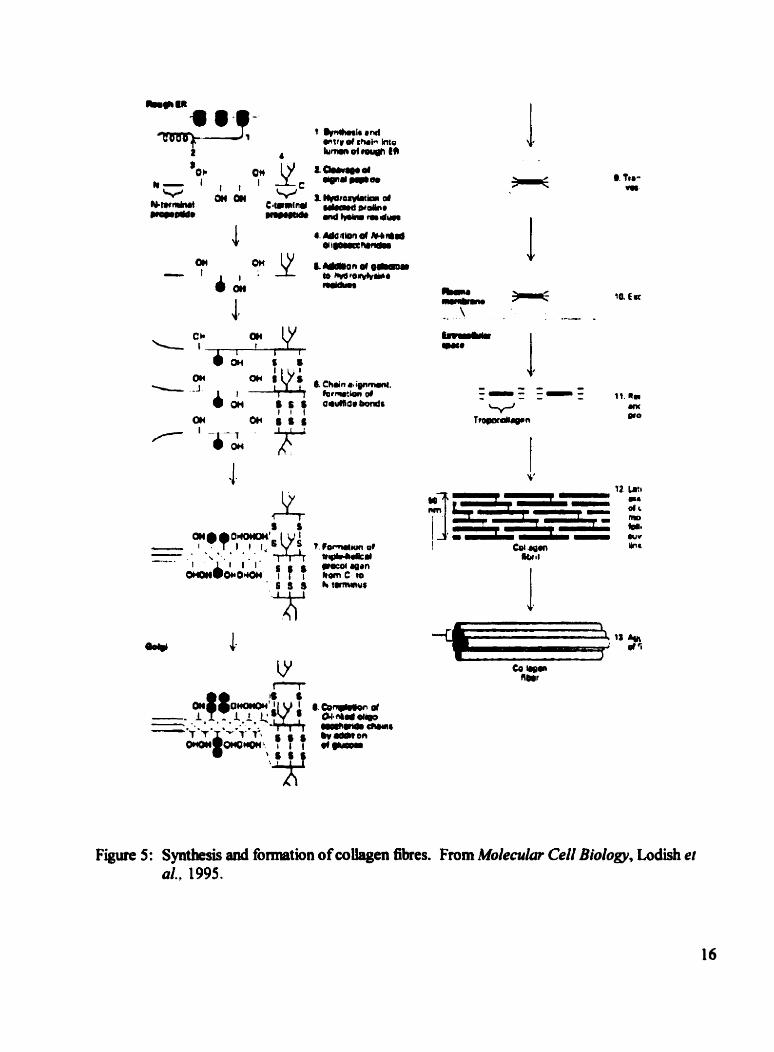
Figure 5: Syntbesis and fomiation of collagen fibres. From Molemlm CeU Biology, Lodish et al., 1995.
Collagen is synthesized as insoluble procollagen a chains (See Figure 5). Prolyl and lysyl
hydroxlase hydroxylate proline and lysine residues, respectively. Galactose and glucose are
added to the newly formed coiiagen rnolecule by coüagen galactosyhransferase and coiiagen
g lucosyhrasfeiase. Further modifications include glycosyiat ion and format ion of disulfide
bonds. The collagen molecule is then secreted in vesicles into the intraceiiular milieu where two
ends are cleaved by amino and carboxy-terminal peptidases. The lysyl residues are oxidized by
lysyl oxidase. The cobgen molecule is m w reedy to become part of the ECM.
CoUagen exists as meny different genetic subtypes which are given the desigation 1-XIII. The
dflerent layers of the skin contain dflerent types of coüagen. The dermis consists mainly of
type I coUagen (85-90%), type III cokgen (8-1 1 %), and type V coUagen (2-
4%). Type VI coiiagen surrounds the d e m l nerves and blood vessels. Type VI1 coUagen fonns
the majonty of dermal vessels.
The final outcome of a heaiing wound is divided into intentions. Healing by k t intention is the
joining of two edges of a wound to cornplete heaüng without a scar or granulation. This is the
outcorne that surgeons try to achieve. Heaüng by second intention is wound closw in which the
edges are sepmted, granulation tissue develops and tissue quickly giows to replace the
granulations resulting in a thin scar. Healing by third intention occurs when tissue grows more
slowly to overtake the granulation tissue which results in a larger scar (Glaaze, 1992).
Formation of Scrr Tissue
Mature scar tissue arkes when inhiitory fàctors (such as interferon a, f3, and y are released by
leukocytes, fibroblasts, and T-lymphocytes, respectively) begin to outnurnber the angiogenic
factors that characterizeâ the granulation tissue. Scar remodeling occurs over the six to twelve
months and achieves approximately 70980% of its original tende arength (Urioste et al.. 1999).
Patbogesesi of Keloid Scars
The pathogenesis of keloid scars is stiU poorly understood. However, the tools of molecular and
ceU biology have begun to provide sorne evidence pointhg towards the etiologic factors. During
the inDammatory stage of the wound healing process, components of the immune system flood
into the wound site with the goal of fighting infection and recruiting the fibroblasts that wiii
synthesize the new skin. If the inflaMnatory stage is prolonged or the response is particularly
exuberant, it is possible to envision a scenario in which too many fibroblasts migrate to the
wound site and begin producing more coilagen than is required.
One particular growth factor, transforming growth factor-fl (TGF-P), has been impücated in the
omet of keloid scars. TGF-P is a crucial cytokine in the wound repair process. Its many roles
klude; chemoattractant for monocytes and leukocytes, induction of angiogenesis, and control of
production of other cytokines. TGF-P is capable of auto-inducing the production of more TGF-
p, as well as inducing the synthesis of matrix proteins, such as hnec t i n , t emin ,
proteogiycans, and coilagen. TGF-p also inhibits the a b o i of enzymes to degrade the cellular
matrix. It is t h e final characteristics that leû Border and Ruosiahti (1992) to refer to the bbdark
side" of TGF-$ in tissue repair, which can lead to excessive scaning and fibrosis.
Numerous studies have shown TGF-P's important role in the wound healing process. Beck et.
. . a1.,1993, used intravenously admuiistrated TGF-P to miprove wound heahg in rats whose
abiity to heal and k e n lowered by age or glucocorticoid administration.
Conversely, Shah et. al. (1992) were able to control rama$ in rats by using neutralizing
antibdies to TGF-P.
Bettinger et al.. 1996, demonstrated that TGF-B increased the arnount of collagen synthesis, as
weii as increasing the amount of procoihgen type I mRNA levels in keloid fibroblasts when
compared with normal fibroblasts.
TGF-P resuhs in further proliferation by causing the aggregation of other rnatrix proteins through
stmiulating the production of fibronectin and proteoglycans. niis cytokine also causes a
reduct ion in the amount of coliagenase and an increase in the amount of cohgenase inhibitors
(Ignotz et al., 1 986). The kreased sensitivity towards TGF-P could either be the result of
increased levels of TGF-fl or a greater number of receptors within the keloid fibroblast.
Mature Scar 111 ji f j]jljl1jj
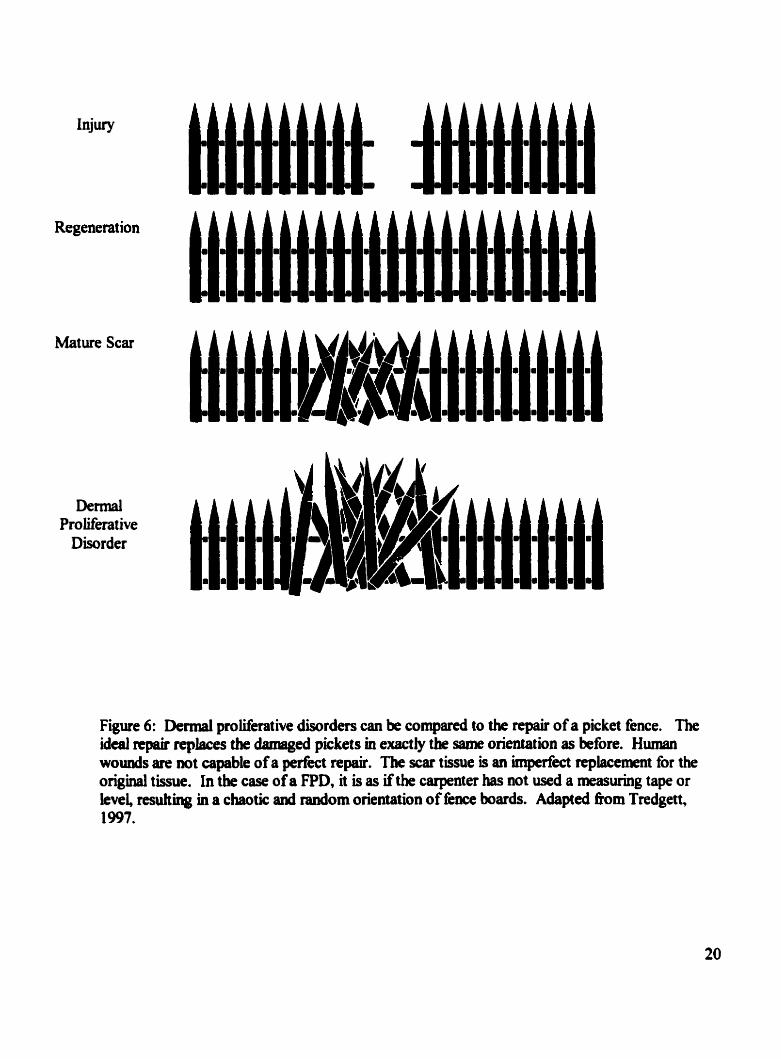
Figure 6: Demial pmliferative disorciers can be compared to the repair of a picket fence. The ideai repair replaces the danisged pickets in exact@ the same orientation as before. Huiaan wounds are not capable of a perfect repair. The scar tissue is an hperfect replacement for the original tissue. in the case of a FPD, it is as if the carpenter has wt used a measuring tape or level nsuhing in a chaotic and random orientation of fence boards. Adspted h m Tredgett, 1997.
Type 1 and VI cokgen genes have increased expression levels in keloid fibroblasts, perhaps due
to tbe actions of TGF-P (Pehonen, 199 1 ). Prolyl hydoxyiase is a crucial enzyme in the
production of collagen. Its activity is a marker of the amount of collagen begin produced. The
actinty of this enzyme has been shown to krease in keloid tissue (Abergel, 1987).
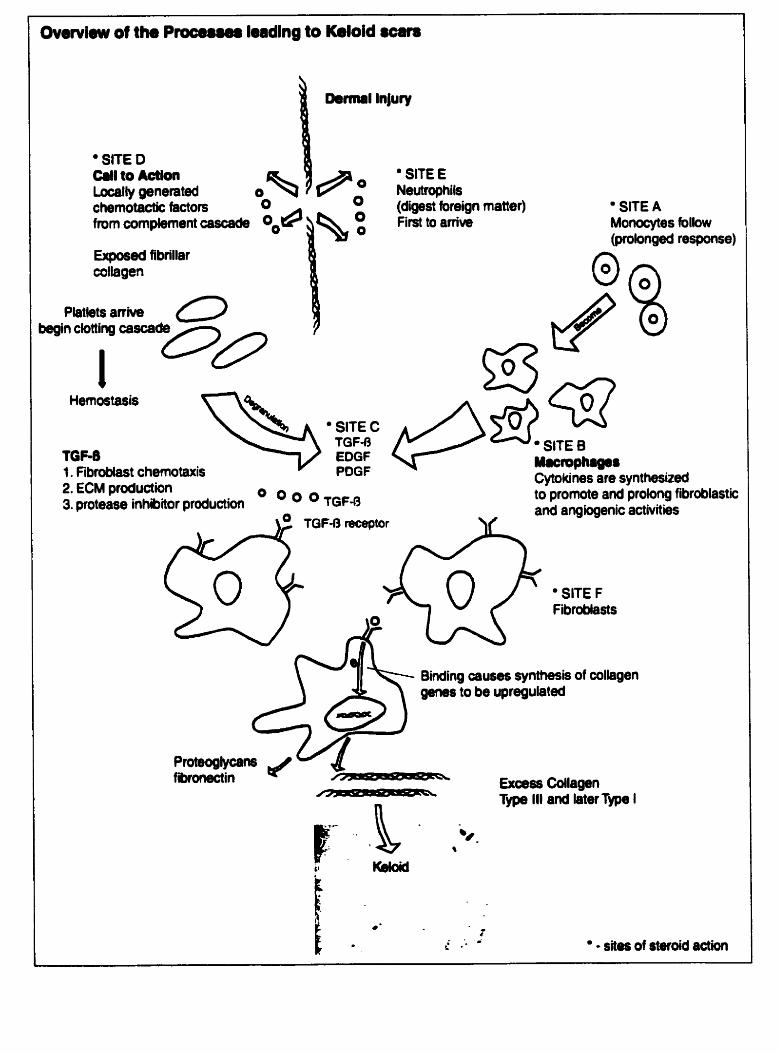
Ovewiew of th. Pmceu# lwdlng to Keloid sccm
Dermal lnjury
' SITE D CI11 to Action Locally generated O chernotactic factors
1 % Ho O O
fmm compkwnt cascade O "P O O
Exposed fibrillar coltagen
P h t b & ( ~ ~ h 0 begin clotting cascade
1 Hernostasis
' SITE C TGF-R
TGF-ô EOGF 1. Fibroôlast chernotaxis POGF 2. €CM production 3. proteme inhibitor production TGF-0
' SITE E Neutrophils (digest foreign matter) ' SITE A First to amve Monocytes foliow
(ptobnged response)
SITE 8 Maciophago8 Cytokines are synthesixed to promote and prolong fibroblastic and angiogenic activities
' SITE F Fibroblasts
Binding causes synttiesis of collagen genes to be upregulated
Pioteoglycans fibranectin - Excess Cdlagen
n Type III and later Type I
4'
* - t L. .- ' - sites of steroid action
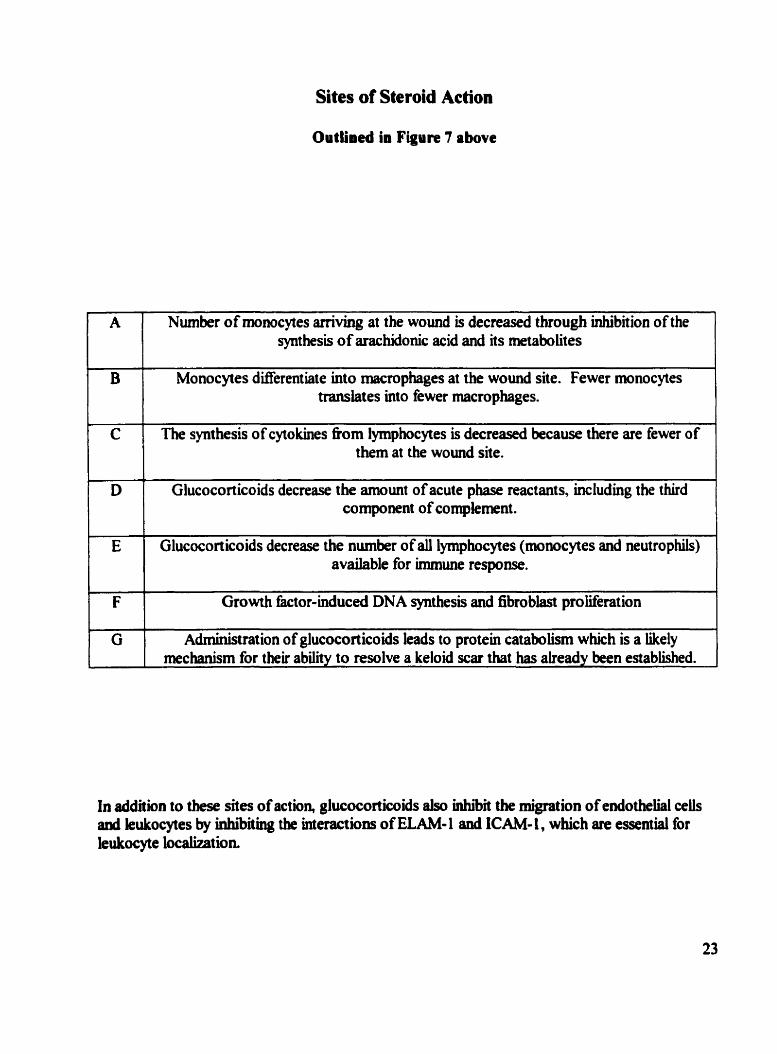
Sites of Steroid Action
Outlined in Figure 7 above
A Number of monocytes arriving at the wound is decreased through inhibition of the synthesis of aracbidonic acid and its metabolites
B Monocytes dserentiate into macrophages at the wound site. Fewer monocytes translates into fewer macrophages.
1
C
i D The synthesis of cytokines fiom lymphocytes is decreased because there are fewer of
hem at the wound site.
Glucocorticoids decrease the amount of acute phase reactants, hcluding the third component of complernent .
E Glucoconicoids decrease the number of all lymphocytes (monocytes and neutrophils) available for immune response.
F
in addition to these sites of action, glucocorticoids also i n h i the migration of endothelial cek and leukocytes by inhibithg the interactions of ELAM-I and ICAM- 1, which are essential for leukocyte localization.
Growth factor-induced DNA synthesis and fibrobkst proiiferation
G Administration of glucocorticoids kads to protein catabolism which is a likely mechanism for their ability to resolve a keloid sw that has already been established.
+
Trertment
A wide variety of treatments have been applied to keloids with varying degrees of success. The
treatments can be arbitrarily divided into physical and phamiacological methods. The physical
treatments include surgical excision, radiation, laser, ultrasound, pressure occlusive dressings,
siticone gel sheets. and cryotherapy (Nemeth, 1993) (Datub-Brown 1990).
Phyakal Tmtmenb
(0 SWPrY
Surgical excision of the scar, witho~t any other treatment is associated with a high rate of
recurrence and, therefore, is almost always accompanied by some other form of treatment
(DaCosta, JC, 193 1 ).
(ii) Radiation
Radiation therapy mcludes the use of X-ray and strontium 90 beta rays. However, use of such
m e s can be potentially damaging due to the subsequent formation of rnalignant tumow
(Hofnaan 1982).
(iii) Laser Surgery
Lasa surgery of keloid and hypertrophic scars initially made use of a continuous wave laser
(argon, Nd:YAG, COI) which emits a constant bearn of iight. However, rwunences within two
y- were obscrved. Within the last decade, thc use of v~scular-specific 585 nm puiseâ dye
Lasa bas been successfbi in treating the erythematous component of hypertrophic and keloid
Oxyhemoglobin has a peak absorption of 585 nm. Pulses that are shorter than one ps are
selective for the destruction of small vessels. The vascular laser destroys capillaries trapped
within the keloid scar and increases the nurnber of mast celis. Through unknown mechanisms,
the vascular laser effects coiiagen turnover and synthesis (Alster. 1998).
The laser surgery also improved the scar texture, pliabiiity, thickness, and symptorns (Alster,
1998). Aister and Williams ( 1 995) propose that the selective destruction of capilliaries contained
within the scar tissue combined with an increase in pst-surgical mast cells appears to &ect
collagen turnover and deposition.
(iv) Ultrasound
The use of this technique is based upon the physical disnipion of the abnormal cohgen
structure in keloid scars (Datubo-Brown 1990).
(v) Pressure Dressings
Pressure dressings exert mechanical pressure upon a wound site. They can be eiastic garments,
springed clips, or clamps. These devices should exert at least 24 mm Hg upon the scar site. The
mechanism of action is unknown and there is no consensus among clinicians as to the duration
the drrssings sbould be wom. A bigh degree of patient cornpliance is required because the
g a n t s need to be wom for the majority of the day.
In the most successfbl clinical study using pressure dressings, Rauscher and KoLner (1 986)
corducted a study with 57 patients with recurrent earlobe keloids. FoUowing surgical excisions,
a steroid-impregnated tape was appiied to the surgical site and was held in place with a ciip-on
earring. M e r four y-, only 4 keloids were observed to recur. Whether these effects were the
resuh of the steroid or the pressure or the combination of the two is dificult to determine.
(vi) Silicone Gel Sheeting
Silicone gel sheet s are flexible polymers made tkom such compounds as polydimethyisiloxane
(Nemeth, 1993). nie use of silicone gel sheeting as a fiamework for wound repair has
experienced good success. Their mechanisrn of action is unknown, however research has show
that pressure, temperature, oxygen tension, or capillary occlusion are not factors (S proat, 1 992).
Advantages of the gel sheet include lack of steroid-associated toxicity and avoidance of painhl
injections. The gel sheets do not adhere very well to haky surfaces or large, irregular keloid
SCm
M a y of these physical treatments, such as laser surgery, uhiasound, and pressure dressings are
either very cost ly or highiy uncornfortable.
Pbarareo~ical Tratmeob
Whüe the physical mabods of tmthg keloids generaliy involved mechanical d h p t i o n or
ablation of the tissue, phannacologid methods target the processes involved m reforming the
tissue &er a wound. Processes such as the synthesis and breakdomi of collagen. In k t . if the
26
synthesis and breakdomi of coUagen can be controiîed, then it would be possible to prevent the
excess scarring that is associated with keloid scars h m ever occuring.
(i) Glucocorticoids
Tbe mainstay of phamiacological ûeatment of keloid scats is the use of synthetic glucocorticoids
and in particular, the use of triarncinolone acetonide. The success of these treatments is variable.
Gntnth et al., 1970, found that of 56 keloids treated with triamcinoIone only 5 recurred (in two
patients) over four years. These authors also reported that in a second series of patients with
keloids and hypertrophie scars ( 1 63 in 1 28 patients) treated with triamcinoIone, 90% displayed a
reduction in size of the scar and an improvement of the symptorns. However, another audy
(Kiü, 1977) reported that 52 patients who received triamcmolone had a recunence rate of 50%
after five years. The varying degrees of reported success highlight the individual variability in
the nature of the keloid scar.
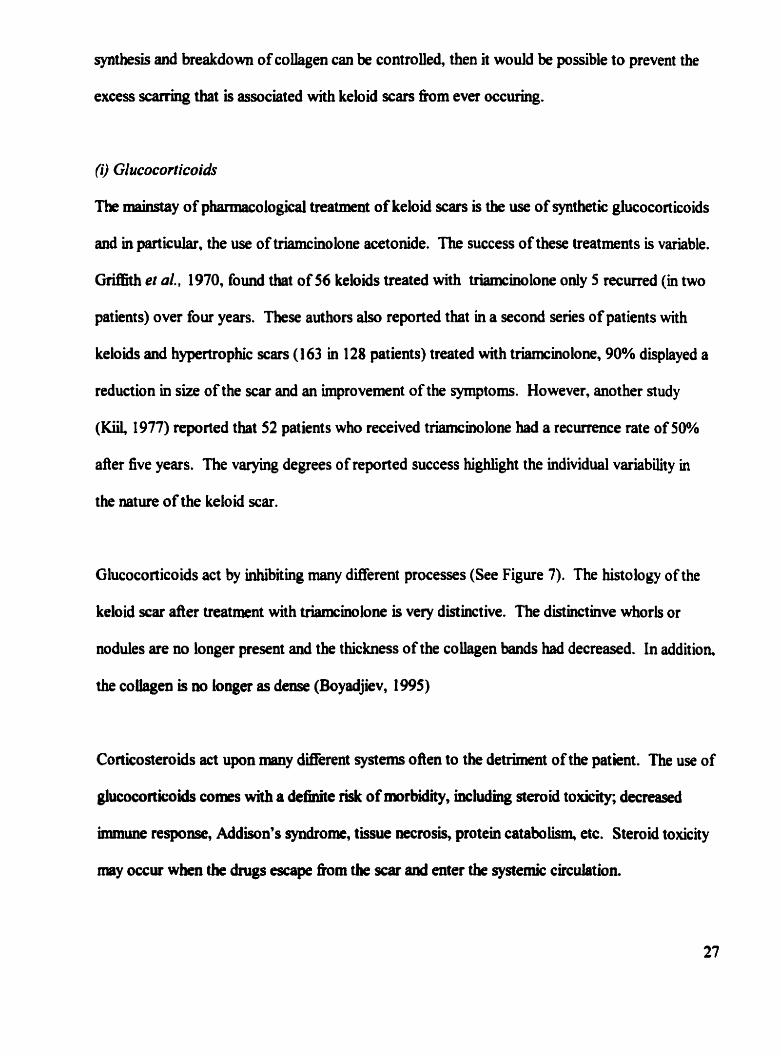
Glucocorticoids act by inhiiiting many difEerent processes (See Figure 7). The histology of the
keloid scar &er treatment with trismcinolone is very distinctive. The distinctmve whorls or
nodules are no longer present and the thickness of the cohgen bands had decreased. In addition,
the coüagen is no longer as dense (Boyadjiev, 1995)
Corticosteroids act upon many Werent systems ofken to the detriment of the patient . The use of
glucoeorticoids cornes with a dehite riBk of wrbidity, bcluâjng steroid toxicity; decreased
immune response, Addison's syndrome, tissue necrosis, protein catabolism. etc. Steroid toxkity
m y occur w k n the dmgs escape h m the ocar and enter the systemic circulation
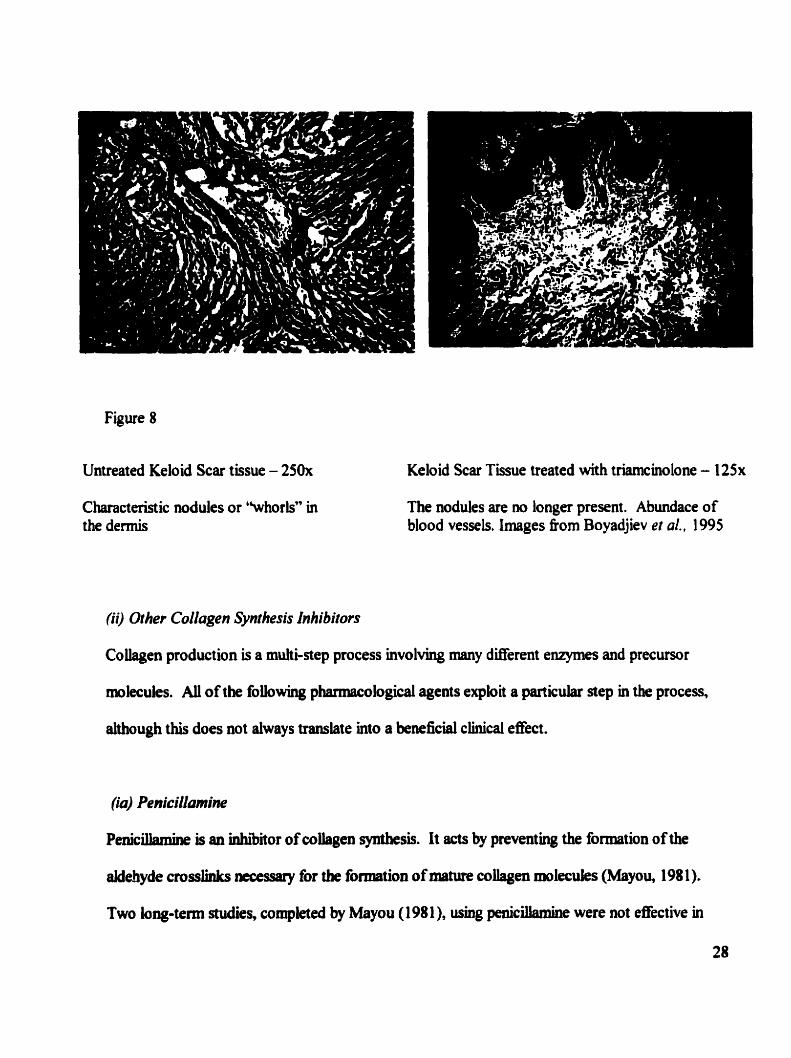
Figure 8
Untreated Keloid Scar tissue - 250x
Characteristic nodules or ''whorls" in the dermis
Keloid Scar Tissue treated with triamcinolone - l2Sx
The nodules are no longer present. Abundace of blood vessels. Images fiom Boyadjiev et al.. 1995
(ii) Other Collagen Synthesis Inhibitors
Coiiagen production is a muhi-step process involving many dEerent enzymes and precwsor
molecules. AU of the fobwing pharmacological agents exploit a piirticulat step in the process,
ahough this does not always translate into a beaeficial ciinical efect.
(io) Penicillamine
Peniciknhe is an inhior of cohgen synthesis. It acts by preventing the formation of the
aldehyde e s l i n k s accessary for the formation of mature coUagen molecules (Mayou, 1981).
Two long-terni studies, completed by Mayou (1 98 1 ), ushg peniciltamiae were not effective in
the treatment of keloids. The lack of e@cacy could have been the resdt of the low doses used to
treat the Iesions.
(iiu) Interferons (IFN)
IFNs inhibit the synthesis of collagen and stimulate the action of coUagenase resuling in an
antagonistic action towards TGF-P which sthulates the growth of coliagen AU three IFNs (a.
P, y) have been studied for their therapeutic effects on keloid s a i s and ciinicaily IFN-y has
shown the best resuhs (Low and Moy. 1992). The results of two studies testing the effects of
intdesional IFN-y (a double-blind placebo controiled study and a non-controlied study,
Granstein et al.. 1990 and Larrabee et al., 1990, respectively) demonstrated significant
reductions in the size of the keioid scars. IFNs do have adverse effects which include headaches,
myalgias, fever, CU. and fatigue (LOW and Moy, 1992).
Conflicthg reports exist for the eficacy of 1FN-a. Bernian and Duncan (1989) reponed a 4 1%
reduction of a progmsively enlarging keloid in one patient. However, Al-Kbawajah , 1 996,
compieted a more systematic study anâ deterrnined that IFN-a was not effective Ui reducing the
size of keloid scars. In an attempt to d u c e the expense of the cost ly IM treatments. the author
nduced the dose that had been used in previous studies which rnight haw aected the results
that & o bserved.
(iiio) Proline anulogues
Cis-hydroxyprob and azetidine carboxyiic acid are both analogues of proliw, which is a
crucial structural component of coilagen. Sufnfient quantities of the analogue in the procobgen
molecule can lead to destatiilization of the collagen tripk h e k The proline analogues have
k e n enective in decreasing the amount of cohgen deposition in cases of pulmonary fibrosis
and liver cnrhosis, but have yet to be tested for their efficacy aga& keloid scars (Low and Moy,
1992).
(iv) Miscellaneous
ûther drugs such as, retinoic acid, ûotretinoin, and dextran sulfate, have met with varying
degrees of success (Datubo-Brown, 1 990).
Despite their position as the first iine of treatment for kelo id scars, corticosteroids have a broad
spectrum of action and are thus an imprecise therapy because of their unwanted physiological
effects. Very kely the fiiture of keloid scar therapy (or treatment of any disorder resuhing fiom
excessive cellular proliferation) lies in the use of more precise phammicological agents that target
specific processes involved in the synthesis and production of collagen and the ECM, such as the
IFNs or 0 t h molecuk antagonists to TGF-B.
Adreaocortical Stemids and their Actions
Corticosteroids have widespread and varied effects on physiology (See Tables 1 J and Figure
10). Tbey are synthesized and secreted fiom the adred cortex in response to
adrenocorticotropic hormone (ACTH). ACTH is secreted fiom the anterior pituitary, which is
stimuiated by the presence of corticotropin releasing hormone (0. The hypothalaumus
secretes CRH. These h e e organs form the hypothalamic, anterior pituitary, adrenal cortex axis
(M'A). The HPA is responsible for maintainhg appropriate levels of glucocorticoids. The
levels of glucocorticoids fluctuate on a daily basis. The largest concentrations of glucocorticoids
occur in the monùng around eight a n Negative feedback is the primary mechankm that
regulates the proper levels of glucocort icoids. Stress can ovemde these regulatory controls and
result in large increases in the concentrations of glucocorticoids.
The steroids that are released fiom the adrenal glands can be divided into two categones;
glucocort icoids which broadly Sec t rnetabolism, and mheralocort icoids which affect water and
electrolyte balance. The adrenal cortex is separated into two distinctive fùnctioaal areas. The
outer mnae glomenilosa secretes the Mneralocorticoids and the inner mnae
fasciculata/reticularis wbich secretes glucocorticoids.
Mcchanism of Action
Glucocorticoids enter the cell and interact with the glucocorticoid receptor GR. The receptor is
conplexcd with kat-shock pmteins 70 and 90, as weii as with a d protein, 56 Da, cded
imumophillia Upon interaction between the receptor and steroid, a codonnational change
occurs which induces nuclear translocation. Once the cornplex has entered the nucleus, it
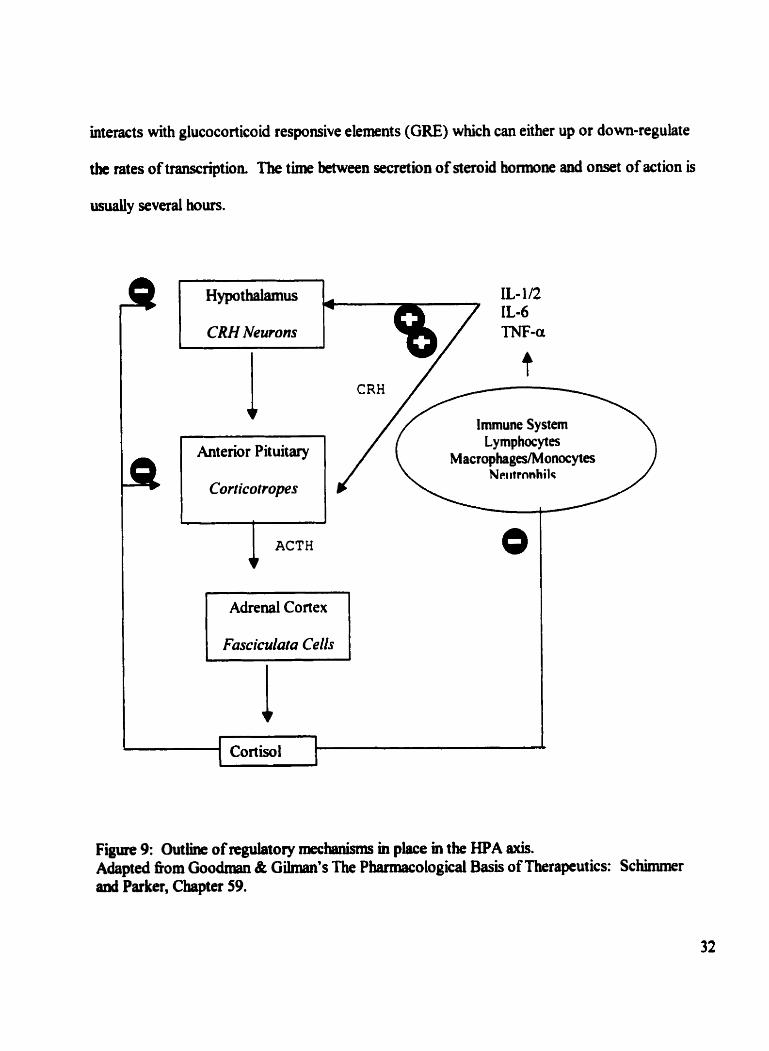
interacts with glucocorticoid responsive elements (GRE) which can either up or down-regulate
the rates of transcription. The t h e between secretion of steroid hormone and onset of action is
usually several hours.
IL- 1 /2 IL-6
CRH Newons TNF-a
I t Immune Sy stem
Lymphocytes Macrophages/Monocyta
N~iiitrnnhilc
1 Adrenal Cortex l
Cortisol I l
Figure 9: Outline of regdatory mec* m p k e m the HPA axis. Adapted nom Goodman & Gilman's The Pharmacological Basis of nierapeutics: Schmuner anû Parker, Chapter 59.
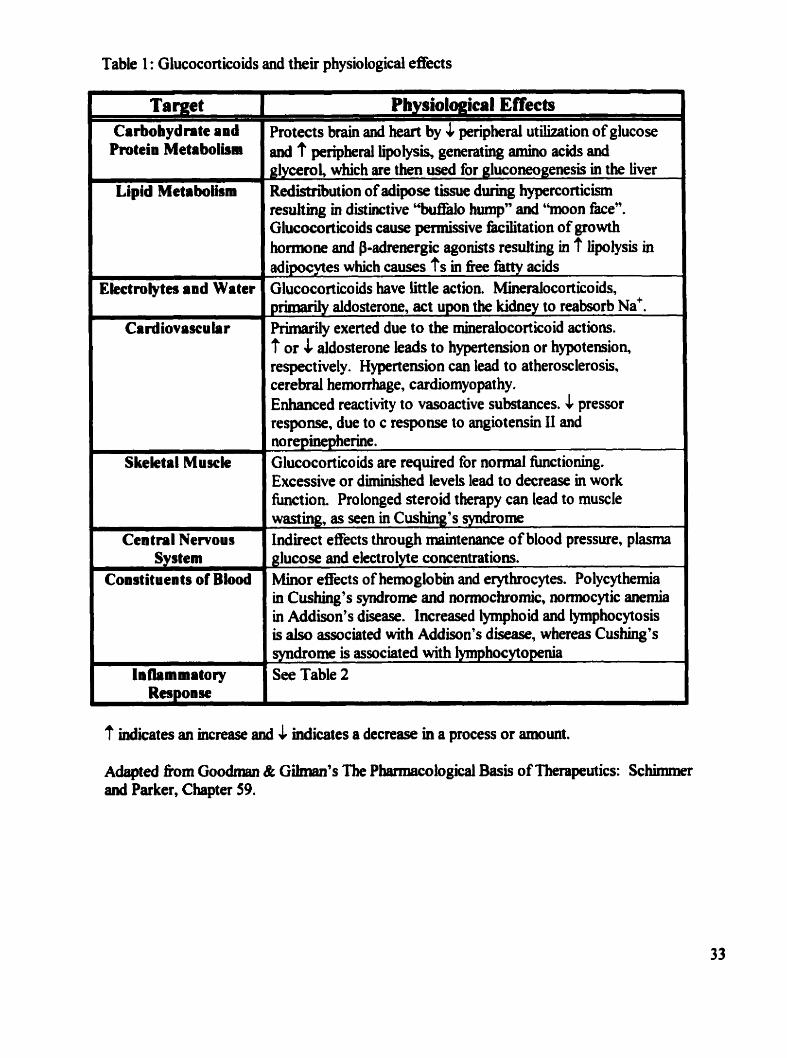
Table 1 : Glucocorticoids and their physiological effects
Carbohydrate and d
I Central Nervous 1
Pmtein Metaboliam
I
Lipid Metaboihm
Ekctrolytcs and Water
b J
Cardiovascular
J
Skeletal Muscle
System 1
Constituents of Blood
,
-
-
'
-
Protects brain and kart by & peripherai utilization of glucose and ? peripkral lipolysis, generating amino acids and glycerol, which an then used for gluconeogenesis in the liver
-- - -
Red'istnhution of adipose tissue during hypmorticism resulting in distinctive "buffao hump" and "moon face". Glucocorticoids cause permissive facilitation of growth honnone and P-adrenergic agonists nsulting in 7 lipolysis in adiaocvtes which causes ?'s in fke fàttv acids Glucocorticoids have Little action. Mineralocorticoids, primarily aldosterone, act upon the kidney to reabsorb ~ a ' . Rimanly exerted due to the mineraiocorticoid actions. ? or 1 aidosterme leads to hypertension or hypotension, respectively. Hypertension can lead to atherosclerosis, cerebial hemonhage, cardiomyopathy. Enhanced reactivity to vasoactive substances. & pressor response, due to c response to angiotensin LI and norepinepherine. Glucocortico ids are required for normal functioning . Excessive or diminished levels lead to decrease in work fimction. Prolonged steroid therapy cm lead to muscle wasting, as seen in Cushing's syndrome Indirect effects through maintenance of blood pressure, plasma glucose and electrolyte concentrations. Minor effects of hem globin and erythrocytes. Polycythemia in Cushing's syndrome and wrmochromic, normocytic anemia in Addison's disease. Increased lyrnphoid and lymphocytosis is also associated with Addison's disease, wbereas Cushing's syndrome is associated wit h lymphoc ytopenia See Table 2
'? indicates an increase and & Micates a decrease m a process or amount.
Aàapted âom Goodman & Gilman's fbe Phenaecologid Basis of Therapeutics: Scbimtner and Parker, Chapter 59.
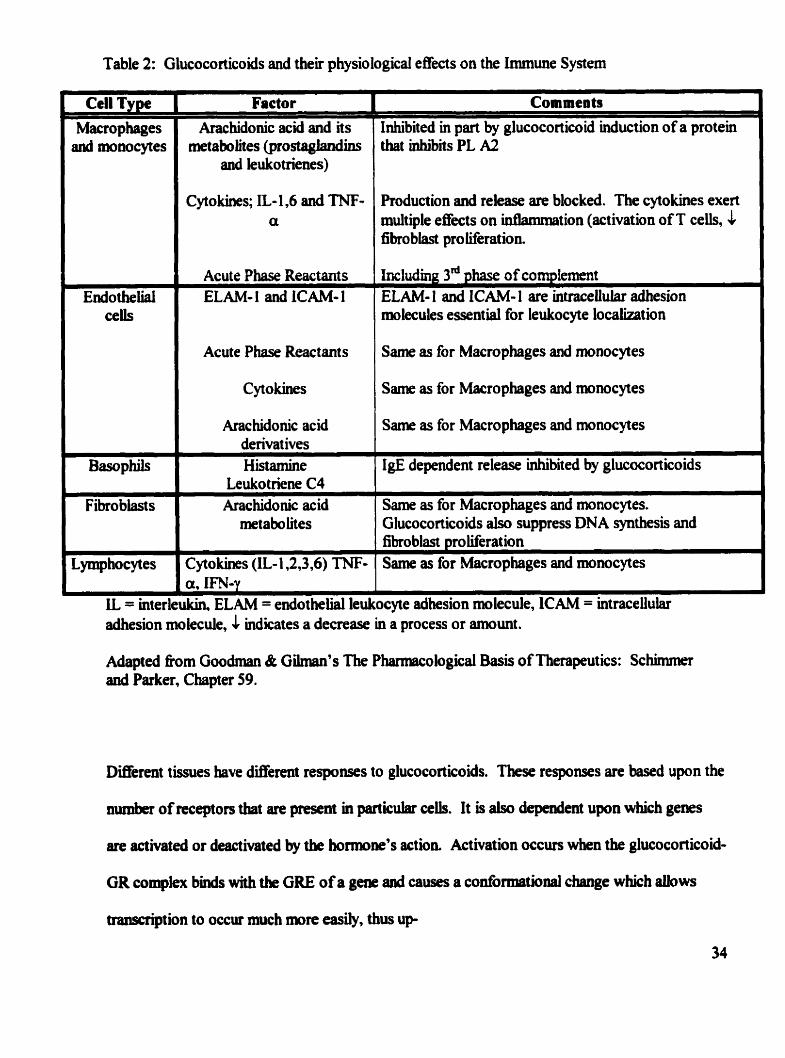
Table 2: GLucocorticoids and their physiological effects on the Immune Systern
Cell Type Macrophages and monocytes
E d o thelial cells
Factor
Arachidonic acid and its metaboiites (prostaglandins
and leukotrienes)
Cytokines; IL- 1.6 and TNF- a
Acute Pbase Reactants ELAM- 1 and ICAM- 1
Acute Phase Reactants
Cytokines
Arachidonic acid derivat ives Histamine
Leukotriene C4 Fibrobiasts Arac hidonic acid
metabohes
Lymphocytes Cytokines (IL- 1,2,3,6) TNF-
.- -- -- -
Comments
Inhibited in pari by glucocorticoid induction of a protein tbat inhibits PL A2
Production and rekase are blocked. The cytokines exert multiple effects on inûammation (activation of T cells, & fibro blast pro liferation.
hcluding 3" phase of coqlement ELAM- 1 and ICAM- 1 are intracellular adhesion molecules essential for leukocyte localization
Same as for Macrophages and monocytes
Same as for Macrophages and monocytes
Same as for Macrophages and monocytes
IgE dependent release inhibited by glucocorticoids - - - - - - -
Same as for Macrophages and monocytes. Glucoco rticoids also suppress DN A synt hesis and fibro blast proliferat ion Same as for Macrophages and monocytes
adhesion molecule, ICAM adhesion molecule, 1 indicates a decrease in a process or amount.
Adapted fiom Goodman & Güman's The Phamiacological Basis of Therapeutics: Schinrmer aad Parker, Chapter 59.
Dinerent tissues have different responses to glucocorticoids. These responses are based upon the
number of receptors that are ptesent in particular ceiis. It is also dependent upon whicb genes
are activatecl or deactivated by the hormone's action Activation occurs when the glucocorticoid-
GR compkx binds with tbe GRE of a gene and causes a conti>rniabnal cbange which albws
tmscription to occur much more easily, thus up
regulating the transcription of the gene. The transcription of the gene can be inhibited when the
glucocorticoid-GR complex binds to the GRE and caws a conformational change which makes
it dif6icult for the transcriptional machinery to associate with the DNA.
Abiorptioa
Hydrocortisone (including many of its congeners, and the synthetic analogues) are effectively
g k n by mouth Intramusculat injections of hydrocortisone, its congeners, and their esters can
result in prolonged effects. Glucocort ico ids are absorbed systemicaily fiom sites of local
adimnistration (either topical or injected), such as synovial spaces, the conjunctival sac, skin, and
respiratory tract .
Changes to the chernical structure can result in a great variety of changes with respect to rate of
absorption, rate of onset, and duration of action. Administration of synthetic glucocorticoids can
lead to sy stemic effects, such as suppression of the hypo thalamic- pituitary-adrenal axis (HPA).
Distribution, Metabolism, and Escretion
Corticosteroids are largely protein bound, up to 90%, in piasma. Only the unôound fiaction is
capable of exerting any physiological action. Two proteins account for the bmding;
corticosteroid bincüng protein (CBG) anâ aibumin, which are both pmduced by the iiver. The
former has a high aniniry for steroids, but a low total binding capacity, whereas the latter has a
b w afh i t y , but a high total bindiap capacity. At higber therapeutic doses, the binâmg
capacities of tbe proteins are overcome, and a higher percentage of unbound steroid exists in the
p h *
Generally, steroids are metaboiized by a series of oxidizations and reductions by the sequential
additions of oxygen and hydrogen, respectively, foilo wed by conjugat ion with water-soluble
derivatives. These &te esters and giucuronide derivatives are primarily excreted in the urine.
The biotransformation of corticosteroids occurs both at hepatic and extrahepatic sites.
Structure-Fraction Reîationships
Synthetic corticosteroids a h to separate the minerabcorticoid functioas fiom the glucocorticoid
actions. Certain h t i o n a l groups are required for glucocorticoid action. The keto group at C-3,
the double bond between C4 and CS and the three hydroxyl substitutions at C2 1, C 17a, and
C 1 1 P. The 1 1 P-OH group is essential for glucocorticoid act ivity. If this hydroxyl group is not
present, then the steroid will display only minerakorticoid activity. A keto group at Cl 1
contriiutes to glucocorticoid activity because it is metabolized to Cl 1 f3-OH. The 2 1 -OH is
essential for both mineralcorticoid and glucocorticoid activity. In some synthetic
glucocorticoids, the hydroxyl can be replaced by other functional groups such as Cl.
Further modifications can be made to increase the selectivity of the synthetic anaiogs for the
ghroconicoid receptors, such as introduction of double bonds between Cl and C2, or addition of
a flourine atom Thea structural changes also decrease biotransfomtion that the mlecules
experiences and this translates hto an increase in the haiClife of the glucocorticoid.
Tbc msjority of keloid scars are treated with syathetic corticosteroids. Triamn:inolone acetonide
is generally accepted as the corticosteroid of choice for the treatmmt of keloid scars (Murray,
1993). There is Little evidence that viamcinobne is mre effective thaa any of the other
synshetic d o g u e s . The case-controlied d i e s tbat examine either ttiamcinolone or other
glucocorticoids show highly variable results. Since there are glucocort ico ids that are more
potent and have longer durations of action, it is reasonable to examine the efficacy of these other
glucocorticoids in cornparison to triamcinolone. There are no known studies that compare
methylprednisolone or dexametbasone, with respect to their abi ies to treat keloid scars. The
former steroid shares the same potency and duration of action with triamcinolone and the latter is
both more potent and bas a longer duration of action (See Table 3). These are the two
glucocorticoids that will be used to determine if changes in structure, potency, and duration of
action have an improved effect on the growth of keloid scars when compared to triamcinolone.
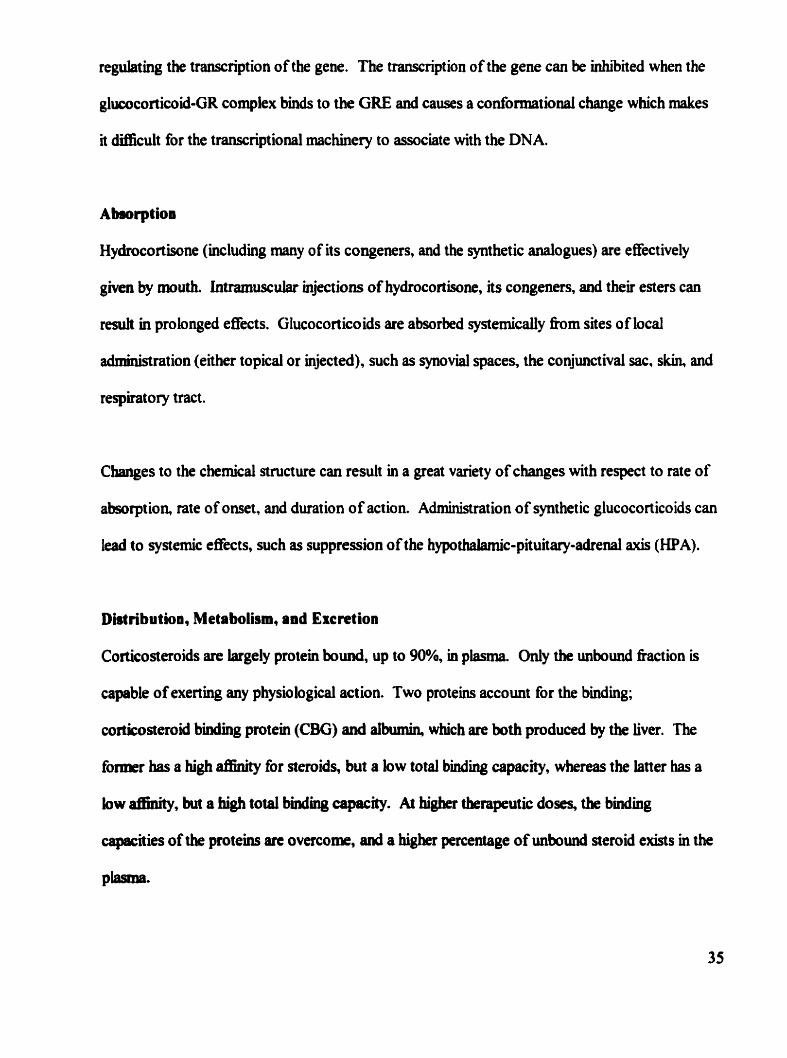
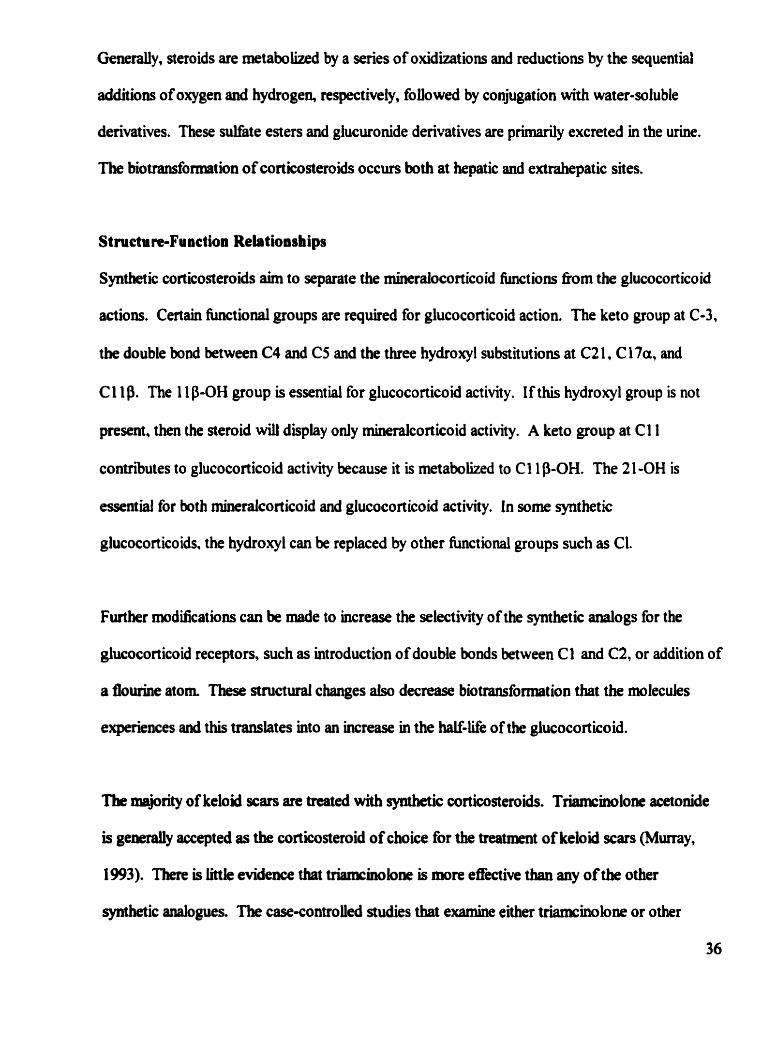
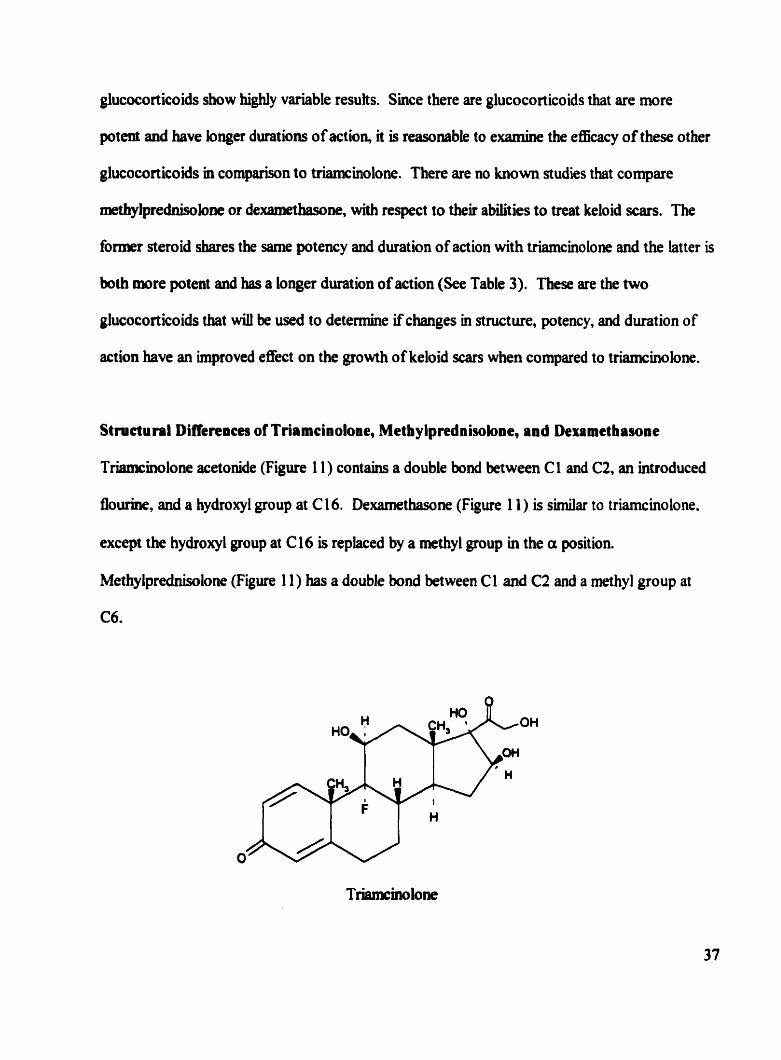
Structural Differeaces of Triamcinoloae, Metbylprednisolone, and Dexametbasoae
Triamcmolone acetonide (Figure 1 1) c o n t h a double bond between C 1 and C2, an introduced
flourine, and a hydroxyl group at C 1 6. Dexamethasone (Figure 1 1 ) is simüar to triamcinolone.
except the hydroxyl group at Cl6 is replaced by a methyl group in the a position.
Methylprednisolone (Figure 11) has a double bond between Cl and C2 and a methyl group at
C6.
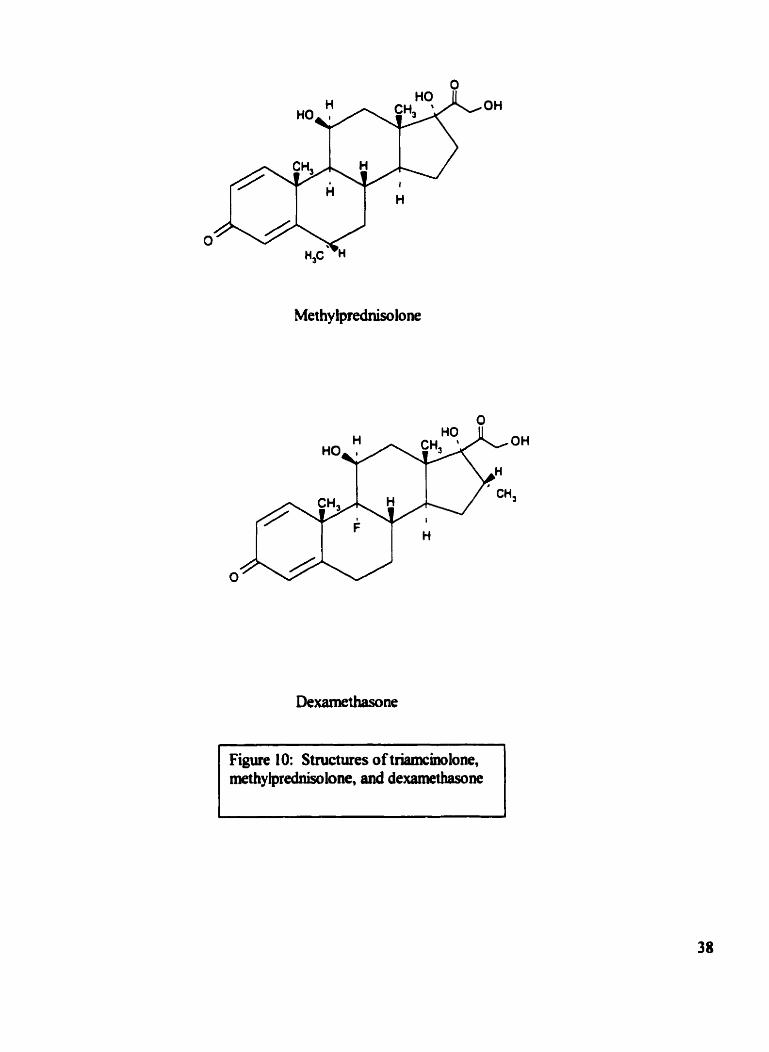
Figure 10: Structures of triamcblone, methylprednisolone, and dexamethasone
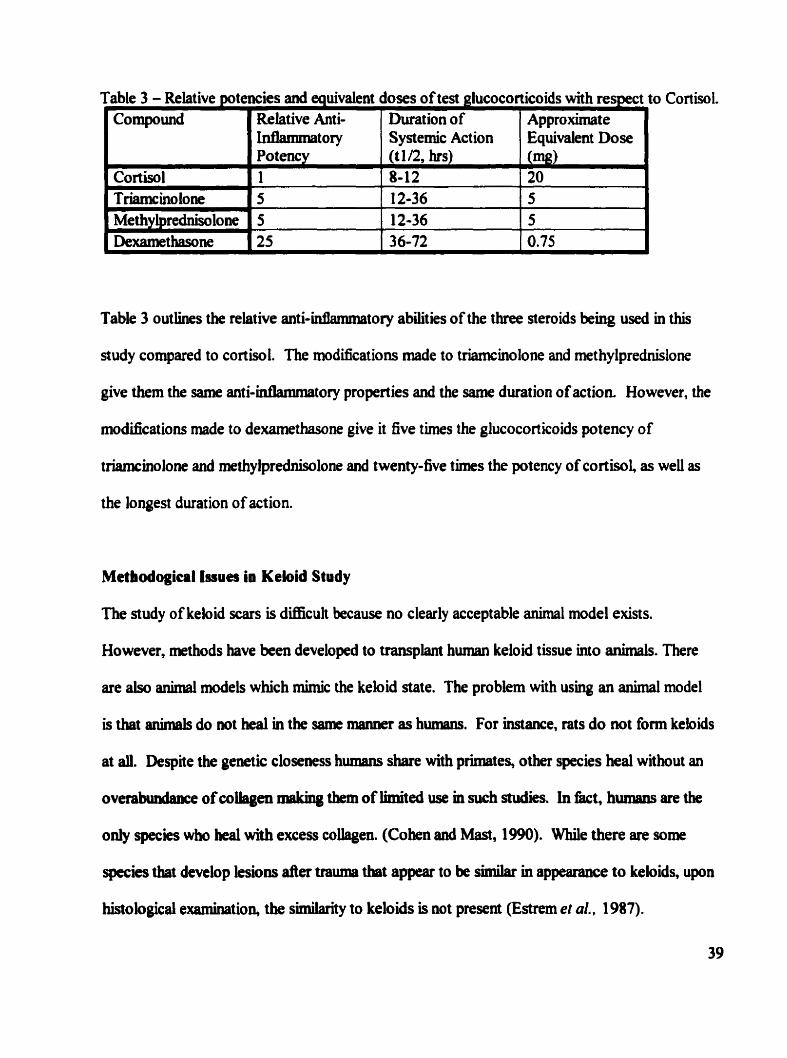
ro Cortisol. Table 3 - Relative potencies and equivalent doses of test glucocorticoids with respect I
Table 3 outlties the relative anti-iatlanmiatory abiüties of the three steroids being used in this
study compared to cortisol. The modifications made to triamcinolone and methylprednislone
give them the same anti-intlammatory properties and the same duration of action However, the
modifications made to dexamethasone give it five t h s the glucocorîicoids potency of
triamcinolone and methylprednisolone and twenty-five times the potency of cortisoi, as weU as
the longest duration of action.
Compound
Metbodogical Issues in Keloid Study
The study of keloid gars is ditncult because no cleariy acceptable animal model exists.
However, methods have b e n developed to transplant human keloid tissue into idmais. There
are also animal models which mimic the keloid state. The problem with using an animal model
is that animals do not heal in the same rrianner as humans. For instance, rats do not form keloids
at al. Despite the genetic closemss humens share with primates, other species heai without an
overabmhce of wlîagen niaking them of limited use m such stdies. In EBct, humaas are the
only species who heal with excess collagen. (Cohen and Mast, 1990). While there are some
species that develop lesions der trauma that appear to be smiilar in appeanuice to keloids, upon
histological examination, the similarity to keloids is not present (Estrem et al., 1 987).
Relative Anti- Inflaannatory
Dwation of Systernic Action
A p p r o h t e Equivalent Dose
The use of tissue culture is useful when wound heaiing processes are king studied because the
environment can be controlkd. Molecular biology dows for very specific experiments to be
done on individual molecules.
Whok Animal Studies
In order to overcome some of the problems, mentioned above, with developing an animal model
for kebid scars researchers have tried to generate states that mimic keloid scars by makuig
incisions and injecting animais with various compounds. Yet, the only histologicaliy and
biochemically faithful method to reproduce keloid scars in animals is to implant human keloid
tissue in athymic mice. Such animais cannot generate a signincant cell-rnediated h u n e
response to the foreign tisme (Reth, 1995).
Some animais, such as the horse, develop keloid-üke lesions after dermal trauma (Earem et al ...
1 987). However, upon histological examniation, resemblance to keloid scars was no longer
apparent. Abdulkader et al. ,1983, attempted to create keloid xars by injecting rabbits with
BCG. Yet, upon histological examination, the lesiow did not resemble keloid scars (Estrem, et
al., 1987) Autotransplantation of keloid scars in man has been shown to be possible, but the rate
success was only one in ten (Cahian and Copmbagen, 1967).
The only successful animal model that reproduces ail the characteristics of the keloid scar has
ùeen the athymic muse model pioneered by Sheltar et al. in 1985. These mvestigators
developed a mthod in which human keloid scar tissue was inserted into nude athymic mice,
which are mimunodeficient and as such are not capable of generating a significant immune
response. Estrem, et al. (1987) confimed that the uriplanted keloid tissue retained its distinctive
histology after surgical implant. Further studies by Kischer and Shetlar in 1 989 and 1 99 1,
respectively, showed that the histology and ~ÛE structural characteristics of the implanted keloid
tissue reiiyuned similar to pre-implant morphology for up to 246 days. Glycosaminoglycan
leveis remabmi, however, at pre-implant levels for approximately 60 days.
Kischer et al., 1989 performed vascularization studies to determine when the mouse began to
anastarnose the implanted keloid tissue. They observed that the athymic mouse would begin to
vascularize the peripheral tissues approximately 8 days pst-implantation and deeper
vascuhuization would begin sometirne befon 16 days.
Waki et al., 1991, demonstrated that the effects of phanriacologic agents could be tested using
the athymic mouse model. Mer implanting h m keloid tissue into athymic mice. they found
that lathyrogenic agents (compounds whic h irnpede coiiagen cross-linking) and triamcino lone
acetonide were effective in bnnging about some regression of the keloid implants.
Ath* nude mice are immunodeficient because they lack a thymus, which means that T-ceUs
are unabie tu mature into fùnctional T lymphocytes anâ are thus unable to participate m celî-
mediaSeci immune responses. Nude rnice are characterized by k i r Mless phenotype. These
mice k k a thymus because of an m o t tbst occurs duririg the developrnent process.
During normal developrnent, the central core of the thymus is fomied h m endodermal tissue.
On day 1 1, a unidentified signal is sent which results in ectoderrnai tissue surroundhg the
endodermai core resuiting in a functionai thymus. However, in nude mice the e c t o d e d sheath
never f o m because of hdty signal transmission or reception. The end result is that the
d o d d core collapses and never f o m a functional thymus. Nude mice do produce hair, but
it is w t dciently keratinized, leaving the hair too fiagile to emerge fiom the foilicle (Re*
1995). The lack of a significant immune response d e s the athymic muse an ideal candidate
for implantation of foreign tissues. The tissues will continue to fuaction normally which means
that they can undergo scientific experinientation within an in vivo system.
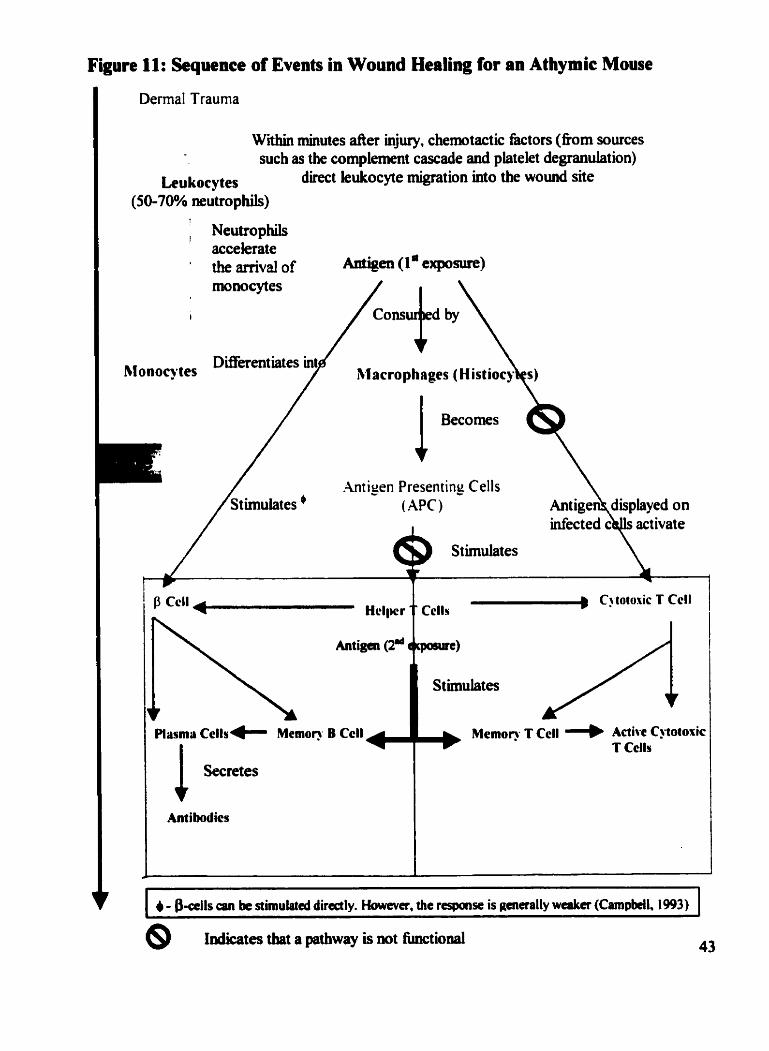
Figure 11: Scquence of Events in Wound Healing for an Athymic Mouse
Dermal Trauma
Within minutes d e r injury, chernotactic &tors (nom sources such as the cornplexnent cascade and platelet degrandation)
Lcukocytes direct kukocyte migration into the wound site (50-70% neutrophiis)
Neutrophiis 1
accelerate ' thearxivalof Antigen (1 * exposure)
monocytes
I
hlonocytes
.hti-,en Presentins Cells
Pluma ~ells- Mcmon B Ccll I + 1 Secretes
Ant i bodics
- --
Cj totoxic T Ccll Cclls
@ Indicates that a pathway is mt hctional 43
It is also possible to assess the efficacy of a compound using an animal model that does not
mvolve keloid scar tissue. Kubota et al. (1 985) induced the formation of granulation tissue using
cotton pellets md introducing surgical lesions in rats. Theu aim was to test the ability of a
wllagen prolyl hydroxylase inhiiitor, P- l894B, to reduce the amount of hydroxyproline. They
extrapolated the results they attained, in order to conclude that P-18948 wodd be a promising
agent for the treatment of keloid scars.
in 1992, Swawa et al, proposed a two-stage rat model in order to test the efficacy of tranilast
(an anti-intlammatory dnig) at treating keloid scars, as compared to triamcinolone. The
mvestigators induced granulation tissue in rats by delivering carrageenan through a surgicaliy
implanted osrnotic Mnipump. They detemiined that traiisilast was able to signiscant ly reduce
hydroxyproline levels in the carrageenan-induced granulation tissue, but the decrements were not
as significant as the decreases observed with trismcinolone.
Carrageenan is the name given to a M y of hear sulfated food grade polysaccharides obtained
h m the rad seaweeds which have the unique abiiity to fonn an almost Uifinite variety of gels at
room temperature. Carrageenan is widely used throughout the food industry. Yet, when
carrageenan is placed into a wound, it acts as an Mant and causes an incmsed inflawiiatory
response. (De Leve, 1980)
In the secoid stage of investigation, S w w a and colieagues implanted hunian keloid tissue in
athymic mice. They showed that aanüast, an anti-aliergic dmg, significantly decreased the
amount of cobgen and giycosaminogiycan synthesis in keloid tissue, however extraordiiiarily
doses of tranilast were us&.
The injection of carrageenan into the footpads of rodents is a standard test for efficacy of anti-
inflammatory drugs (De Leve et d.. 1 980). The effkcts of corticosteroids and theu anti-
inûammatory actions are weil known which means that a model designed to show the eEects of
corticosteroids on inflammation will not produce any new information. The value of the
carrageem-inflammatory model combined with the athymic m o u model is its potential to
predict the efficacy of drugs to prevent or reduce keloid scars. This model could be used as a
screen for new compounds thought to have efficacy against keloid scars. If the compound
cannot pass the first stage of the rreen, then it is unlikely that it will have any efficacy against
keloids. Since rats are less costly when compared to athymic mice (approximately ten times),
the model also makes economic sense because only compounds that are Likely to prevent or
reduce carrageenan induced keloid-like state will get to the second stage of the screen.
Tissue Culture
Tissue or ceil culture, in general, provides a very precise method for the investigator to control
the enwonment of the cells. This system is particuhrly uscful when studying a specific
metabolite or the activity of an enzyme, such as collagenase or prolyl hydoxylase. The downside
to using such a method is thai the in vitro environment in which the cells are living is often very
different fiom the in vivo environment.
Koch et al., 1996, repoited a mtbod cmpioying a kebid fïbroblast tissue culture without having
to use blood serum. The culture displayed the same growth kinetics and histology as previous
kebid c u b e s that required senim. However, for the purpose of the p m n t study, tissue
culture was not considered to be a suitable experimental method. The primary goal of treatments
45
employed in this project is to prevent the keloid fiom forming in the first place. Therefore, a
model in which a keloid scar couid be induced would be ideal. A tissue culture would consist of
keloid fibroblasts and it would be possible to assess the rate of prolifieration or regression of the
keloid. It would not, however, be possible to ascertain the prophyhctic characteristics of a given
treatment. An intact animal model is required for such detenninations.
The experimental strategy of the project to be descnid will k to assess the effectiveness of
thm dflerent glucocorticoids in preventing and reducing the severity of keloid scars in two
Mirent anunal models. The first rnodel involves hducing a hyperintlaMnatory state in male
Wistar rats using carrageenan implanted in a surgical wound site. The second model tarpts
humaa keloid tissue irnplanted into nude athymic mice.
The goal of this study is to use two difEerent animal models to evaluate keloid scar therapy using
dexamethasone, methylprednisolone, and triamcinolone. Aithough other giucocorticoids, such
as hydrocortisone, rnethylprednisolone, and dexamethasone have ken used to treat keloid scars
m man, triamcinolone remains the prDnary choice among clinicians to treat these lesions. There
has not ken a reported systematic, comparative study of the keloid-treatment effects of the other
synthetic glucocorticoids bemg used in this siudy. The efficacy of the three conicosteroids will
k compareù by their ability to reduce and/or prevent keloid scan.
hotber goal of this M y is to develop a potential scrrenpig tool for other keloid therapies. The
us of the cimageenan-induced idhmation rnodel would be a more potential mthod to
YlcntiS, potentially compounâs with possibüity to prevent or reduce keloid s&g relative to
the athymic muse model because of lowered expense and kreesed ease of working with rats
ratber than athymic mice. Any compound that reduces or prevent infiammation effectively could
be considered as a potentially effective because of the relationship that exists between
inflammation and wound healing . If the severity of the inflammatory response can be controlied.
then the subsequent ECM deposition and remodeling can be controlled as well. In the case of a
keloid scar, a prolonged intlaMnatory state is present. This results in the recruitment and
migration of many different mflammatory growih frictors and cytokines, such as TGF-P. The
role of these cytokines is to promote the regeneration of the ECM. However, the prolonged
inflammatory response results in too many of these cytokines being recruited into the wound site.
The end result is too much collagen deposition and not enough coliagen resorption, which
accounts for the exuberant growth of keloid scars.
This is not to rule out the possibility of other therapies, such as non-steroidal anti-dammatory
drugs (NSAiDs). For example, Acetasalicylic acid (ASA) is an NSAID that cm interfin with
platelet aggregation and can reduce the number of platekts present in the blood. Given the
important role that platelets play in the pathogenesis of keloid scars it is reasonabk to extrapolate
to a use for antiplatelet medications such as ASA or other NSAIDs in the treatment of keloids.
Materials and Methods
Animals
Male Wistar rats (1 5 1-1 75g, ) and male nude mice (28-42 days, approximately 15-20 g) (BALB I
cAnNCrl-nuBR nuhu) were obained fiom Chles Riwr, Quebec, Canada.
Approval for the use of animais was obtained fiom the Animal Research Ethics Board (AREB)
of McMaster University before any animal experirnentation began.
AU animais were housed at the Central Animal Facility (CAF) at McMaster University. The
Wiar rats were housed one to a cage in rooms open to the general environment at the CAF.
Each cage was equipped with a hepa filter bonnet. Rat chow (Lab Diet) and water were provided
ad libitum.
The nude mice, however, required sterile conditions at a higher level to minimize the occurrence
of bacterial infections. Sterilized m o w chow (Lab Diet) and water were provided ad libitum.
Upon entering an antwoom, personnel were required to Wear sterilized surgical gomis, surgical
bonnets, gloves, and booties before entering a subsequent room isolated fiom the general
enwonment at the CAF. This room was home to other hairless and furry colonies of mice. The
mice were housed one to a cage.
Cages, water bottles, bedding materials, and plastic cylinder (in which the rnice played) were ail
pre-sterilized. h y t h the nude mice were handled, the cage was brought underneath the
laminar flow hood.
AU animals were housed for at least four days before any procedures were carried out.
Supplies
A k t minipumps (mode1 2002,200pL capacity, 0.5 p L h for 1 4 days), Alza Corporation, Pa10 Aho, California, USA
Wound clips, 9 mm, Becton-Dickinson, Frankiin Lakes, New Jersey. USA
Wound Clip Applier and Remover, Becton-Dickinson, Frankh Lakes, New Jersey, USA
Tubercuiin (lcc) syringe, 25G5/8 needle, Becton Dickinson, Franklin Lakes, New Jersey, USA
3cc syringe, 21G112 needle, Becton Dickinson, Franklin Lakes, New Jersey, USA
Biopsy Purifh, 4mm, Accu-Punch, Fort Lauderdaie, Florida, USA
Triemcinolone acetonide 40 mg/ml USP (Kenalog@), Sabex Inc. Boucherville, Quebec, Canada
Methylptednisolone succinate 40 aiglrnl USP (Solu-Medrol@), Upjohn Company of Canda, Don Mills, Ontario, Cansda
Dexsmetbasone sodium phosphate10 mg/d USP (Hexadrol@), Organon Teknika, Toronto, Ontario, Canada
Carnageeuan Iota (gelath, vegctable; Irish Moss) Type V; fiom Eucheuma spinosu, Sigma Chenricals, St. Louis, Missouri, USA
Halothme, M C Phannaceutâals, Cambridge, O n e , Canada
Isoflurme, A b t Laboratorïes, Saint-Laurent, Quebec, Canada
Bupivacaine HCl USP, 0.25 mg/mL, (Seasoricaine@), Astra Phannsceuticals Inc. Mississauga, Ontario, Canada
Buprenorphine HCl USP, 0.3 n@mL, (Temgesicdb), Reckin and Colman, Hu& England
Sulhmethoxazole 40 mg/ml- Trimethoprim 8 mglmL (SeptraQB), B. W. Inc.
Sterile Salm USP, 0.9% NaCl, Baxter Corporation, Toronto, Ontario, Canada
ColdsporeO (1 0% glutaraldehyde, 0.5% O-pheny lphenol0.1% p-tert -amylpheno 1), Metrex Researcb, Monisburg, Ontario, Canada
Surgical Iodine (7.5% povidone-iodine), Rougier Inc., Chambix, Quebec, Canada
Histology witb Hematoxylin and Eosin
The fixing and aaining of tissues was performed according to the protocols established at the
pathology laboratory at St. Joseph's Hospitai, Hamihon, Canada.
Ail images of histological slides were captured using a Sony CCD digital camera.
In order to assess the efficacy of the different glucocorticoids in preventing or reducing either
chronic inflainnation (Study 1) or reducing the extent of keloid scar tissue (Study 3), a series of
categories were created and scores were assigned for each. The criteria for each score is Iisted
below. DiBerent criteria were used for each study because different phenornena were king
measured. The scoring was carrkd out in a blinded-Won by Dr. S. Salama.
The foiiowirig scak which assesses the ea6cacies of the glucocorticoids is largely subjective.
The preseace or absence of a structure or process was chosen instead of a numerical d e , in
order to remove any b i i by the observer and remove ambiguities chat a numerical sale might
give rise to. The presence of a deria was scored as a plus and the absence was scored as a
minus.
Criteria for Histological Scoriag
Stidy la2 - Iaduced chroiic inlbmmatioo in rats
The presence or absence of granulation tissue was assessed in the tissue samples. The formation
of granulation tissue is one of the first observabie processes to occur aller a wound has occuned
and is one of the first steps towards the formation of fibrous tissue which matures into scar
tissue. Granuiation tissue has a characteristic appeanuice in rat tissue samples stained with H&E
(See Figure 1 5 ) .
The œxt characteristic was the presence or absence of granulornatous foreign body reaction.
This is an immune response where histiocytes migrate towards foreign bodies and attempt to
digest them Granulomatous areas are identified by the presence of multinucleated giant cek
and a characteristic dark blue cobur after king stained with H&E (See Figure 20).
One way to measurc the extent of the chronic inflammation is to assess whether or not the
damage has extended beyond the subcutaneous tissues into the dermis. The presence or absence
of this activity was also scored.
The final marker that was assessed in the rat tissue samples was the presence or absence of
fibrous tissue. Granulation tissue giws rise to nbrous tissue, whkh m tum is the precursor to
scar tissue. Fibrous tissue is evident in tissue samples stained with H&E by observing orange
cobured coikgen in the background of granulation tissue. Certain samples had mature scar
tissue in the de*, but these were all related to the incision site used to insert the pump.
Study 3 - Keloid imphnts in athymic mice
The first marker that was assessed was acute inflammation. If neutrophils were observed then
the sample was scored positive for the presence of acute mflainmation Neutropbh are
identified by their muhi-lobed nucleus (See Figure 22)
As in tbe rat tissue samples, the presence or absence of granulation tissue and grandomatous
foreign body teaction were scored.
Many of the keloid tissue samples had calcium deposits. The severity of these deposits was
graded on a scale of zero to two. where zero indicated no calcium deposits; one indicated rniid
deposits; and two indicated marked deposits which consumed more than half of the keloid tissue.
Scoring sheets were created for each slide and the results were recorded. See Appendices C and
D for the inchidual scoring Eheets for rat tissue a d for keloid tissue.
Gram Stain
Para* sections were rrmoved fiom tissue bbcks and depamfhkd as a h . Slides were
covered mth aystai violet for 60 seconds and then washed with water for 5 seconds. Slides were
then f l d e d with ioâ i i solution for 60 seconds and tben rinsed with water for 5 seconds.
Ethanol was added to the skies drop wise until blue-violet was no longer being released 60m
52
the specimea As in previous steps, sarnples were rinsed with water for 5 seconds. Slides were
covered with safianin and dowed to amd for approhtely one minute. Samples were rinsed
with water for 5 seconds to remove any excess dye (See Figure 30)
Surgical Procedures
Carrageenan-Induced lnaammation Studies I & 2 with Male Wistar rats
Rats were anesthetized ushg either halothme or isoflurane. Using sterile surgical technique a
dorsal incision, approxirnately 1-2 cm, was made between the scapulae and to the level of the
panniculus muscle . Using a hernostat, a small pocket was fomed by spreading the
subcutaneous comective tissue. An osmotic minipump (Aizet Mode1 2002) was placed into the
pocket.
The mini-pump contains an intemai reservoir with a capacity of 200 pL that must be filled with
the appropriate solution. The mass of the mini-pump was taken before and after filhg to ensure
that the reservoir was completely Wed. Once the mini-pump was placed inside a physiological
environment, it began to absorb fluid and to discharge the contents of the mervou at a rate of
0.5 pL/hr for 14 days.
An appropriate carrageenen solution (0.5%, 1.00/o, or 2.096 w/v) was preparcd in sterik saline
solution. The mullpump was then îïlied according to the procedure above.
Approxhately 0.31111 of bupivacaine HCl(0.25 @mL) was bjected into the wound site. A
subcutaneous injection of approximately 0.3 mi, of buprenorphine, 1 : 10 dilut ion, was given to
provide pst-surgical analgesia. The incisions were closed using 9mm wound clips. The rats 53
were allowed to regain consciousness and recover fiom the surgery before king returned to their
cages. The wound clips were remved approximately ten days afier surgery.
Tissue biopsies were made using a 4mm skin punch. Tissue samples were placed in 10%
foddehyde for histological examination and immunostainhg or &ozen for hydroxy-probe
assays.
Studyl Detemination of Optimum Experimental Conditions
The experimental strategy for Study 1 and 2 involves using experimental animais ( Wistar rats) to
establish a predictive mode1 for assessing the efficacy of potential keloid scar therapies.
In order to approximate the keloid state, a hyper-inflannnatory condition must be produced. The
purpose of study 1 was to detemime the amount of carrageenan required to cause an approximate
keioid-like state. The conditions that were deterrnined moa effective in Study 1 were
subsequently used in Study 2 which involved treatment attempting to prevent or ameliorate the
hyper- -tory condit ion wit h synthet ic glucocort icoids.
The dulation of the control experiment was two weeks. Tissue sarnples were taken at one and
two weeks.
Eight d e Wistar rats were divided e q d y into 4 dBerent groups;
+ sham surgery (no minipump, oc@ a dorsal incision - 2 rats)
4 blank pump (rninipump containing physiological saline - 2 rats)
+ 2% carrageenan (1 week - 2 rats)
+ 2% carrageenan (2 weeks - 2 rats)
The two rats in the sham mrgery and blank pump groups were designated as either one or two
weeks and tissue samples were taken at these t h e points.
At the end of the experimentai period, either one or two weeks, the anmials were sacrificed using
a CO? chamber. A small portion of dorsal tissue (approximately 3x3cm) around the area of
incision or pump insertion was removed. The tissue sample was either fixed in 1 0%
formaldehyde or fiozen for later hydroxy-probe assay . Ail fiozen sarnples were stored at -
At the request of the staffvetennarian at the CAF, a second control experiment was carried out
using ten rats and 0.5% and 1% carrageenan. The purpose of the second experimmt was to
determine the optimum carrageenan concentration that would elicit the required amount of
mflammation wbile minimiPng any discornfion that high concentrations of carrageenan might
have caused the animais.
Ten male Wistar rats were divided equally into the following groups;
4 0.5% carrageenan (1 week - 2 rats)
+ 0.5% carrageenan (2 weeks - 2 rats)
4 1 % camigeenan ( I week - 2 rats)
4 1 % carrageenan (2 weeks - 2 rats)
+ saline (1 week - 1 rat)
4 saline (2 weeks - 1 rat)
A concentration of 2.0?40 for carrageenan was chosen for d further experiments because it was
capable of generating the hyper-inflanunatory state requued to approximate a keloid scar and did
not appear to cause signincant discodort to experirnental animals.
Study 2 The use of corticos~eroids tu prevent carrageenan-induced inflammation in rats
The goal of Study 2 was to determine the efficacy of three dif5erent corticosteroids in reducing or
preventing the inflammation caused by carrageenan in rats. Study 2 utilized the optimum
corditions for carrageenan concentrations (2%) detemimed in Study 1.
Thirty-two male Wistar rats were divided into four groups;
4 corn01 - no injections (saline pump)
+ 1 week-2 rats
+ 2 weeks - 2 rats
+ 3 weeks-2 rats
+ 4 weeks - 2 rats
+ 2% carrageenan - hiamciwlone acetonide, 4Omplmi (O. l ml weekly)
4 1 week-2 rats
+ 2 weeks - 2 rats
O 3 weeks - 2 rats
4 weeks-2 rats
+ 2% carrageenan - methylprednisolone succinate, 40mg/ml (O. 1 mi weekly)
1 week - 2 rats
2 weeks - 2 rats
+ 3 weeks - 2 rats
4 weeks - 2 rats
+ 2% carrageenan - dexamet hasone sodium phosphate, 8mg/ml(O. 1 mi weekly )
1 week - 2 rats
+ 2 weeks - 2 rats
3 weeks-2 rats
+ 4 weeks - 2 rats
The reiative anti--tory potency of triamcinolone acetonide and methylprednisolone
succinate are both 5, with respect to cortisol whereas the dexamthasone sodium phosphate has
a relative potcacy of 25. In order for al1 tbree corticosteroid solutions to have the same relative
potency, the concentration of coxnmercially available dexa~llethasone sodium phosphate was
düuted nom 10 rnglml to 8 mglm1 using sterüe saline.
Surgical insertion of the mUiipumps was carried out as descriid above. The first intralesional
dose of conicosteroid was given at the thne of surgery. A total of O. 1 ml (approximately 27
mgkg triamcinolone acetonide and methylprednisolone, and 5.34 mgkg dexamethasone for a
1 SOg rat) of each glucoconicoid was injected into four sites equally spaced dong the incision.
At the time of surgery, two biopsies using the 4mm skin punch were perfiormed on a dorsal area
between the hind legs of the animal, an a m that did not interfere with the surgical site. The
tissue samples were either used for histology or fiozen for later biochemical assays.
Subseqwnt intralesional injections (O. 1 ml) occuned at weekly intervals. The rats were
sacrificed at either 1,2, 3, or 4 weeks. Tissue samples sunounding the pump insertion site were
removed and either h e d in forrnaldehyde or fiozen.
Study 3
Imphting human keloid tissue in nude athymic mice (BALB / cAnNCrl-nuBR nuhu)
Male nude mice (BALB 1 cAnNCrl-nuBR ndnu) were housed in presterilized cages (one per
cage) m a sterile environment. Theu diet consisted of sterilized mouse chow ad libitum and
sterilUwd water. The mice were housed for at least four days before any procedures are
perfomd.
Human keloid tissue was obtained fiom patients who had elected to have their scar tissue
surgicaîly removed. Sampüng was carried out in accordance with a hurnan experimentation
protocol approved by the Research and Ethics Cornmittee at St. Joseph's Hospital. Hamilton,
Ontario. M e r the scar had been removed by a plastic surgeon, the tissue was placed Ui a
rehigerated aerile Petri dish between gauze bandages moistened with sahe. Surgical implants
of tbe keloid tissue to an athymic mouse host occurred within four hours of king excked fkom
the patient. Before impîantation, representative !amples were taken for biochemical and
morphological anaîysis.
AU sutgeries took place using aseptic technique, in a laminar flow hood. The mke were
anesthetized w h g isoflurane. A section of keloid approximately 2xZx2mtn was deepithehked
and p k e d through a 1 cm dorsal incision subjacent to the subcutaneous muscle located in the
miche, caudal to the scapulae. A second incision in the midline m the lumbar area between the
hind legs was made and a section of keloid tissue was pleced subjacent to the subcutaneous
musek. The incisions were closed usmg 9mm skin clips. Each mouse was weighed prior to and
after the experimental period. The skin clips of the mice remaining in the study were removed
&et two weeks.
Halfof the keloid irnplants fiom each treatment gmup were removed at 15 days. If there were
mice thst only had one implant removed leaving one intact, the resuhing wound was closed
again, while the rnouse was under anesthesia, using skin clips. If both implants had been
removed fiom a mouse, then the mouse was subsequentJy sacdiced. AU remaining implants
were rernoved at 30 days.
The Research Cornmittee at St. Joseph's Hospital in Hamilton reviewed the need for human
invohrernent with this project and gave their approval before any excised keloid tissue was used
experimentally. lnformed consent was given by each patient, prior to the plastic surgery
procedure (See Appendix B)
Kebid sampk 1
The first human keloid tissue sample was obtained fiom an Afio-American female, aged 25.
This patient was seeking cosrnetic remval of a nodular keloid on her nght earlobe. The keloid
was approxhately 3 x 5 ~ 3 cm in size.
Twelve mice received two dorsai, subcutaaeous implants of this keloid.
4 Coatrol group (no treatment) - 3 mice
4 Methyfprednisolone group (40 mg/& 0.025 rdkeloid) - 3 mice
Dexamethasone group (8 mg/ml0.025 myke1oid) - 3 mice
Tiiamcinolone group (40mg/ml, 0.025mVkeloid) - 3 mice
Ghicocorticoids were delivered at the tirne of surgery and repeated at two weeks. The total
observation period was one month.
Kcbid sampk 2
The second keloid t issw sample was O btained from a North American Nat ive Indian male
SU-, aged 19. The patient was seeking cosmetic removal of a nodular keloid, approximately
2xMcm, fiom his lefl earlobe.
Eigbt mice received two dorsai, subcutaneous implants of this keloid.
Control group (no treatment) - 2 rnice
+ Methylprednisolone group (40 murni, 0.025 rnlkeloid) - 2 rnice
Dexamethasone group (8 mg/mi, 0.025 mykeloid) - 2 mice
+ Triamcblone group (40mglmlO.025mVkeloid) - 2 rnice
Ghrocorticoids were delivered at the time of surgery and repeated at two weeks. The total
obacrvation period was one month.
Kdoid sampk 3
The thitd keloid sample was obtained h m a black female subject, aged 29. The patient was
seekiPg wsmetic remval of a large nodular keloid, approximately 4x3x2cm. on the left side of
ber œck.
Four mice received two dorsal, subcutaneous implants of this keloid.
+ Control group (no treatment) - 1 muse
Methylprednisolone group (40 mghi, 0.025 ml/keloid) - 1 muse
Dexametbasone group (8 mghi, 0.025 mlkeloid) - 1 muse
Triamcinolone group (40mg/d, 0.02SmYkeloid) - 1 mouse
Glucocorticoids were delivered at the t h of surgery and repeated at two weeks. The total
observation period was one month.
Tbe number of anirnals in each subgroup in Study 3 varied b u s e of the size of the keloid
scar. ûriginaiiy, there were a total of 24 rnice which were to be implanted with kelo id xar tissue
fiom two different patients. However, keloid sample 2 could only be subdivided into 1 6
implants. This left four unused mice. A third patient agreed to participate in the study which
albwed for keloid sample 3 to be implanted into the four remaining Mce.
Each mouse received approximately 2 mg of methylprednisolone and triamcinolone
(approximatety 100 mg/Kg for a 20 g muse) and 0.4 mg of dexamethasoae (approximately 20
ingll<g for a 200 mouse).
Hydmxy-ProUne h y
Kebid tissue samples were lyophybd for 18 hours, in order to remave any water content.
DrYd sampks were hydrolyzed m 6M HCI with 1% phenol for 24 hours. FoUowing hydrolysis,
excess HCI was m v e d d e r vaccum. The sample was derivatized using a solution of

methano1:water:triethylamhe;phenylisothiocyanate (PITC) (7: 1 : 1 : 1). The derivatking solution
was removed under vacuum. Samples were dissolved in sample diluent and injected into an
HPLC using a Waters PICO-TAG column runaing on a Waters Pico-TAG gradient. The column
temperatw was 33OC and the amino acids were detected at 254nm.
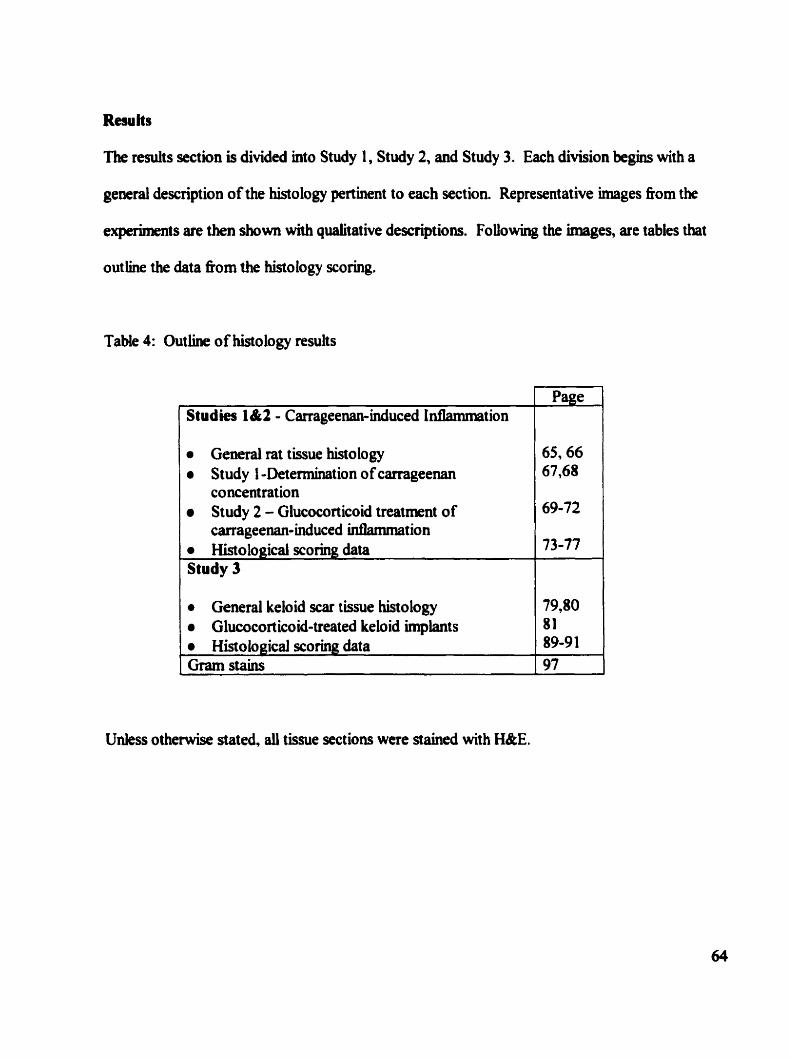
Results
The resuits section is divided mto Study 1, Study 2, and Study 3. Each division begins with a
geaeral description of the histology pertinent to each section Representative images fiom the
experiments are tben shown with quaiitative descriptions. Following the images, are tables that
out line the data fkom the histology scoring.
Table 4: Outline of histology results
General rat tissue histology a Study 1 -Determination of carrageenan
concentration Study 2 - Glucocorticoid treatment of
Studies 1&2 - Carrageenan-induced Infiammation
carrageenan-induced Uitlammation , Histological xoring data 73-77
Page
General keloid scar tissue histology a Glucocort icoid-treated keloid Unblant s ( 8?" 1
Unless otherwise stated, all tissue sections were stained with W E .
1
Histological scoring data Gram stains
89-9 1 97
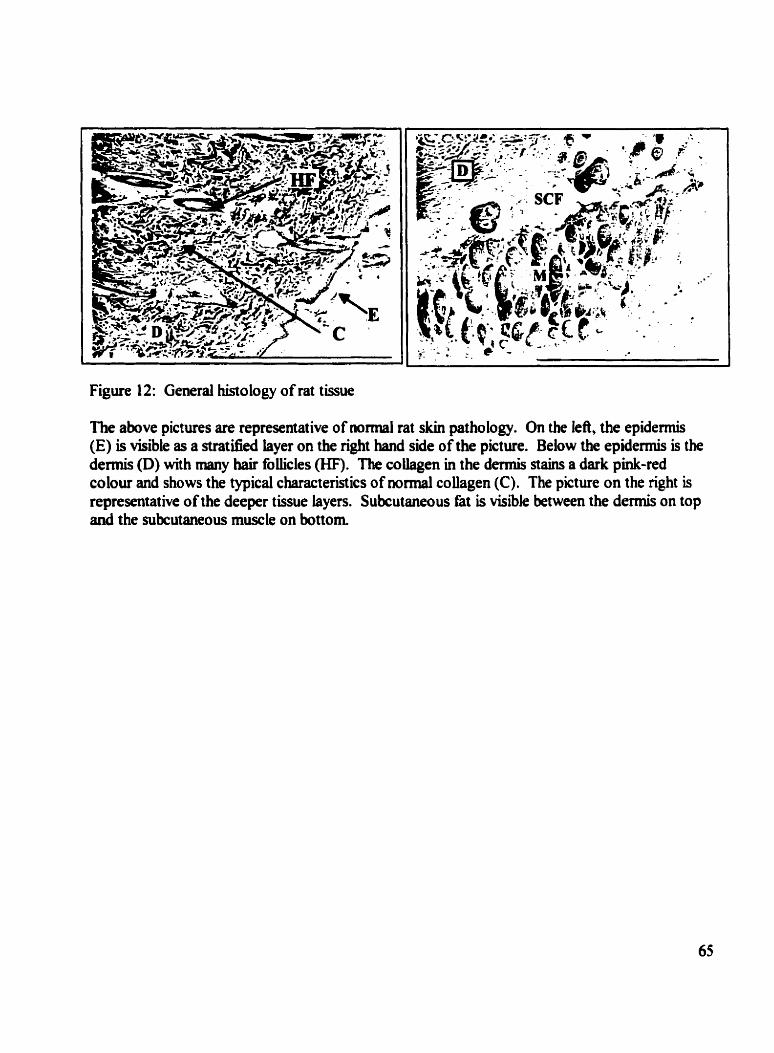
Figure 12: General histology of rat tissue
The above pictures are representative of nomial rat skin pathology. On the kft, the epidermis (E) is visible as a stratified layer on the nght hand side of the pictun. Below the epidemiis is the dermis (D) with many hair foliicles (HF). The coüagen in the dermis stains a dark pink-ted colour and shows the typical characteristics of nomial collagen (C). The picture on the right is representative of the deeper tissue layen. Subcutaneous fat is visible between the dermis on top and the subcutaneous muscle on bottom
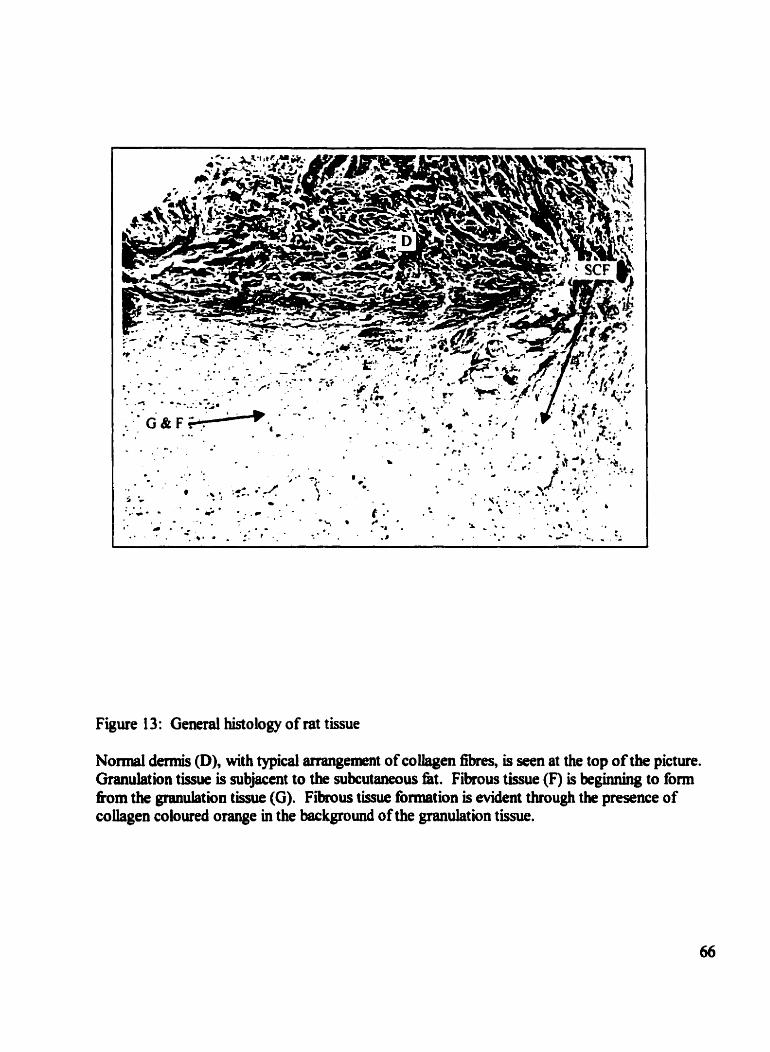
Figure 13: General histology of rat tissue
Normal dermis @), with typical arrangement of coiiagen fibres, is seen at the top of the picture. Granulation tissue is subjacent to the subcutaneous fat. Fibrous tissue (F) is beginning to fom îkom the granulation tissue (G). Fibrous tissue formation is evident through the presence of coiiagen coloured orange in the background of the granulation tissue.
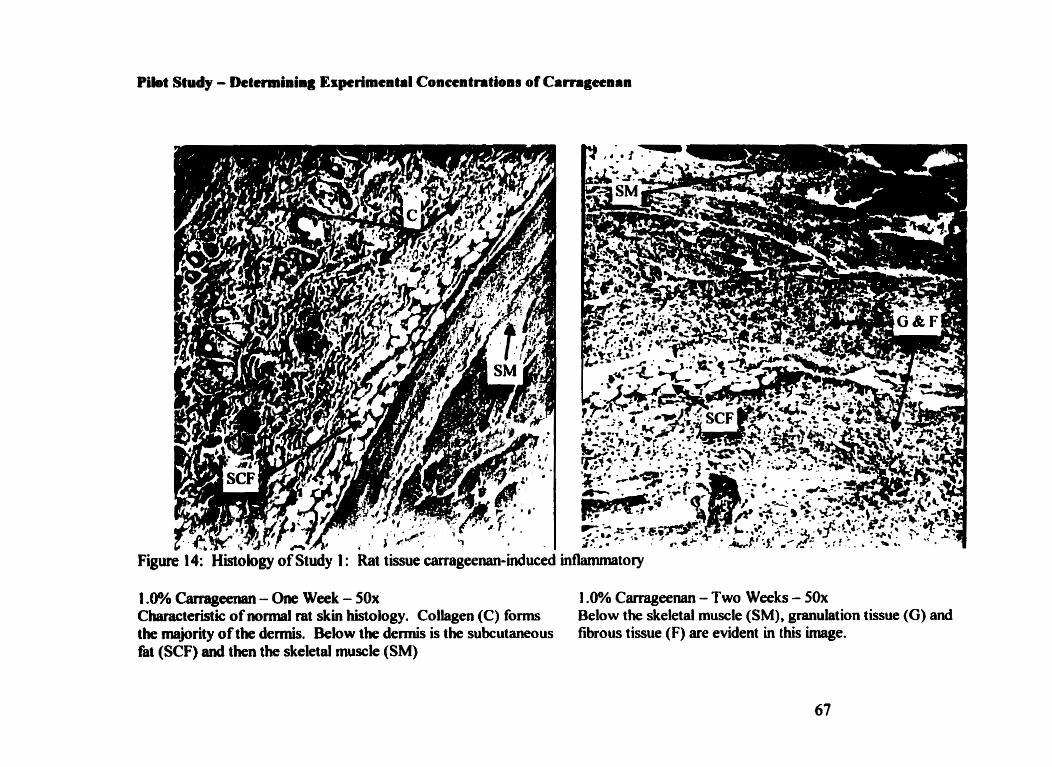
Piîot Study - Determiiiig Espcrimcatil Concentritions of Camgecnan
Figure 14: Hiscoiogy of Study 1 : Rat tissue carrageenan-induced inthnunatory
1 .û% Carrageenan - One Wbek - 50% 1 .O% Carrageenan - Two Weeks - 50x Characteristic of normal rat skin histology. Collagen (C) forms Below the skebtal mus& (SM), granulation tissue (G) and the mejority of the dermis. &low the dermis is the subcutaneous fibrous tissue (F) are evident in this image. fat (SCF) and then the skeletal muscle (SM)
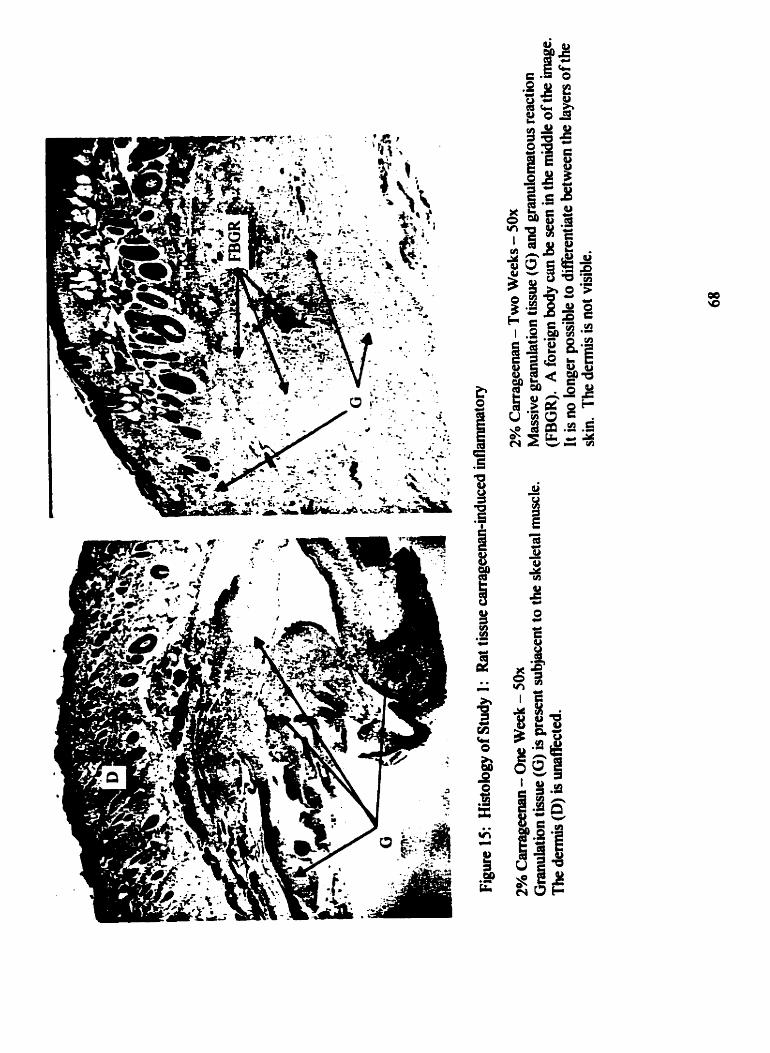
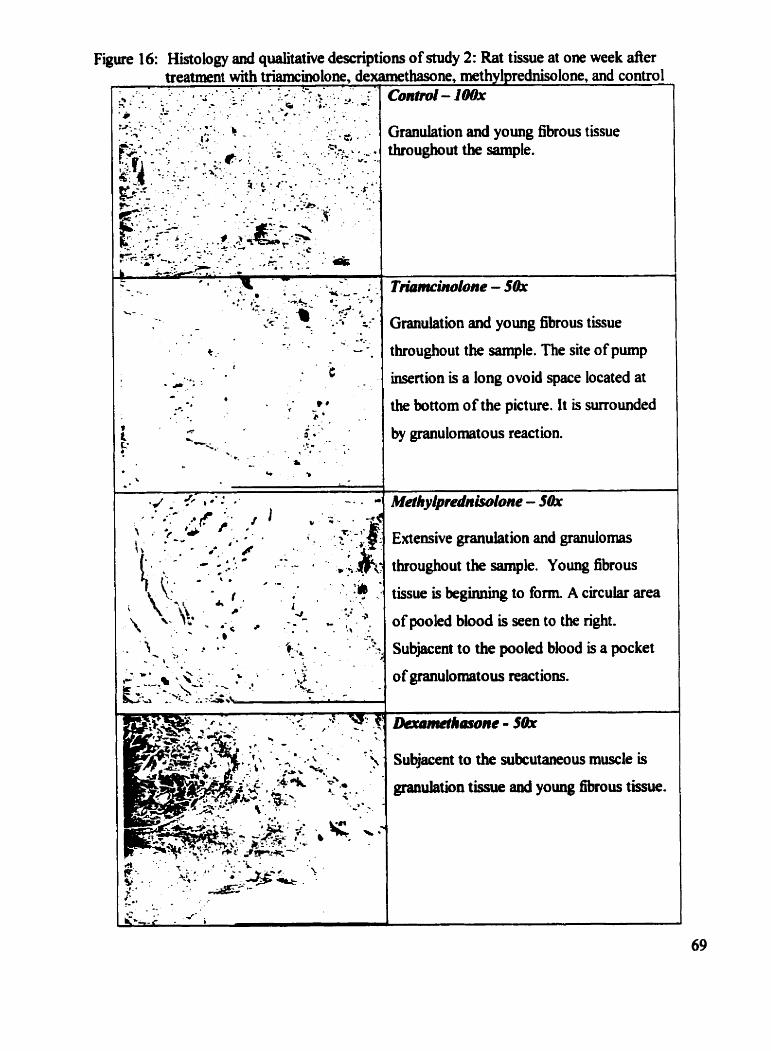
Figure 16: Histology and qualitative descriptions of study 2: Rat tissue at one week der treatment with triamcinolow, dexamethasone, methylprednisolone, and control
* 1 . . . ::.* ; - . . . . - 1 ., ' .8 : * .
: ". . :-7 : 2 - *.. - -, ,, - - . . *- . W . . . . - : + c o n t r d - l m
i.. "' .; 1- - .- . .. . . ' i .;- .. - . . *- . b:-. . .
l
t
. .
'. Y , . 1 .'.. 'c - . Fr' -. \ , . : .. 3 5 : " -;-..*-- . . .
. &A*- *
Granulation and young fibrous tissue throughout the sample.
Granulation and young fibrous tissue
throughout the sample. The site of pump
insertion is a long ovoid space located at
the bnom of the picture. It is mrrounded
by pulomatous reaction.
Extensive granulation and granulomas
throughout the sample. Young fibrous
tissue is beginning to form. A circula. area
of pooled blood is seen to the right.
Subjacent to the pooled blood is a pocket
of granulomatous reactions.
Subjacent to the subcutaneous muscle is
granulation tissue and young fibrous t h .
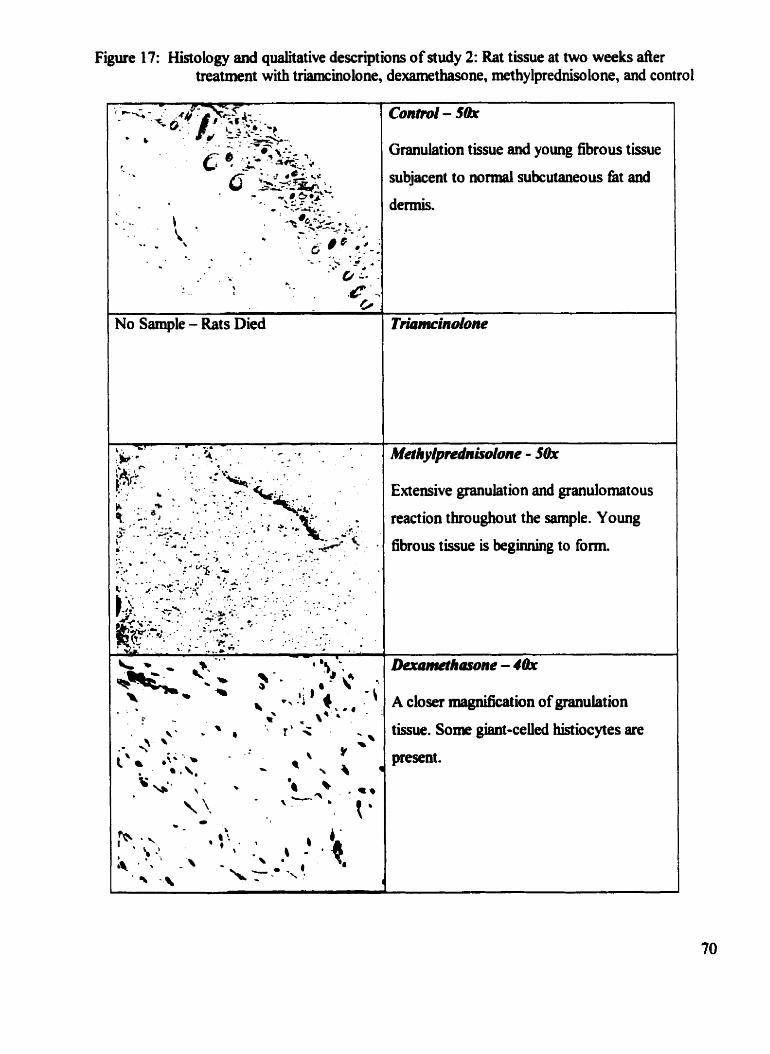
Figure 1 7: Histology and qualitative descript ions of study 2: Rat tissue at two weeks d e r treatment with triamcinolone, dexamethasone, methy lpredniso lone, and contro 1
No Sample - Rats Died
Granulation tissue and young fibrous tissue
subjacent to normal subcutaneous fkt and
dermis.
Extensive granulation and grandomatous
reaction throughout the sample. Young
fibrous tissue is beginning to fom
A closer magniocation of granulation
tissue. Som &nt-ceUd histiocytes are
present .
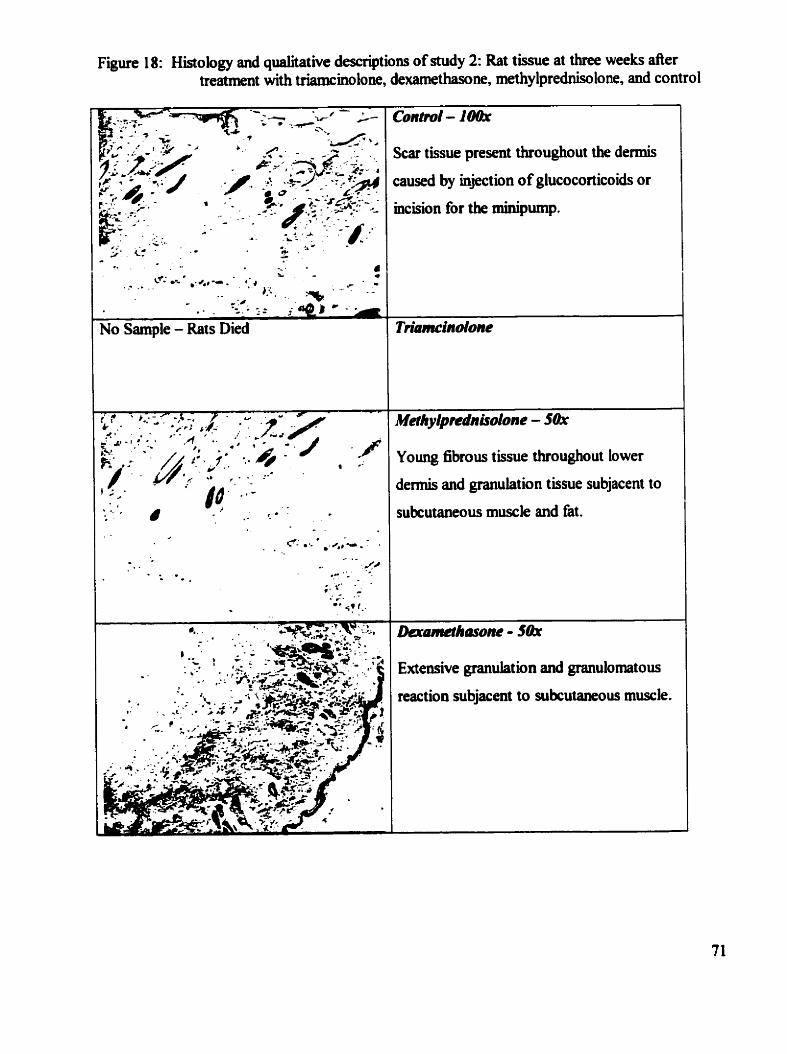
Figure 1 8: Histology and qualitative descriptions of study 2: Rat tissue at three weeks after treatment with triamcinolone, dexamethasone, methylprednisolone, and control
Zcar tissue present throughout the dennis
: a d by injection of glucocorticoids or
ncision for the xninipurnp.
Young fibrous tissue throughout lower
dermis and granulation tissue subjacent to
subcutaneous muscle and fat.
kamethasone - 5th Extensive gianuhtion and granulornatous
reaction subjacent to subcutaneous muscle.
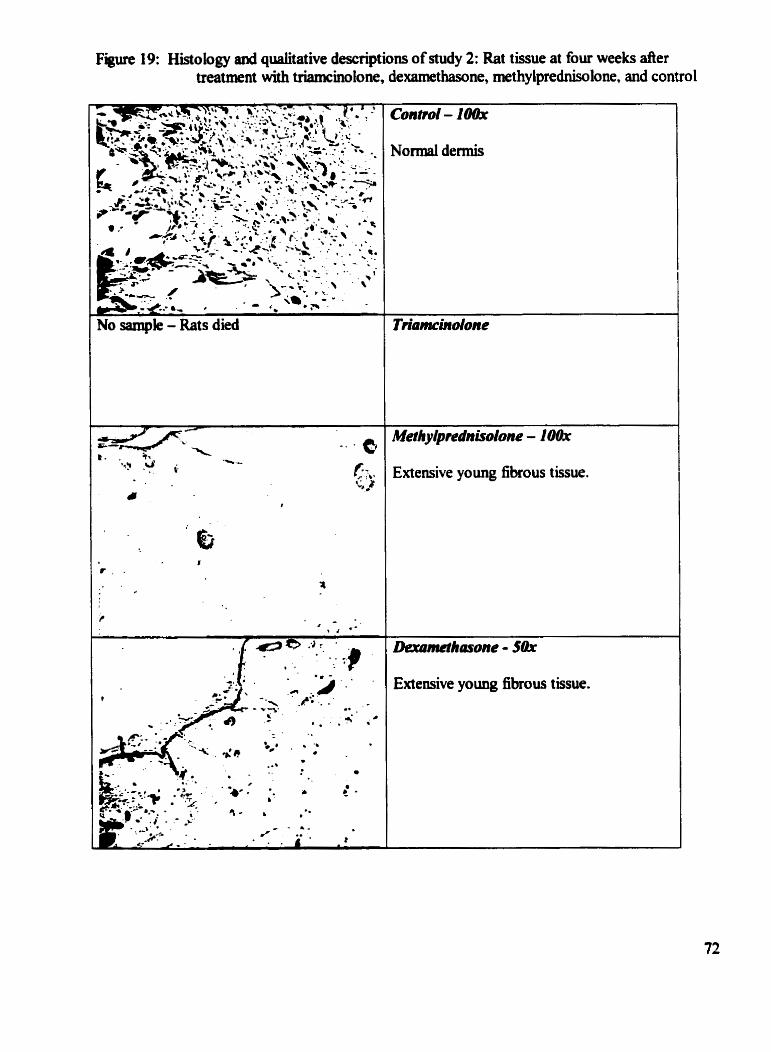
F i 19: Histology and qualitative descriptions of study 2: Rat tissue at four weeks d e r treatment with triamcinolone, dexamethasone, methy lprednisolom. and contro 1
go s e l e - Rats died
Meîhyipednisdone - 10th
Extensive yo ung fibrous tissue.
Extensive young fibrous tissue.
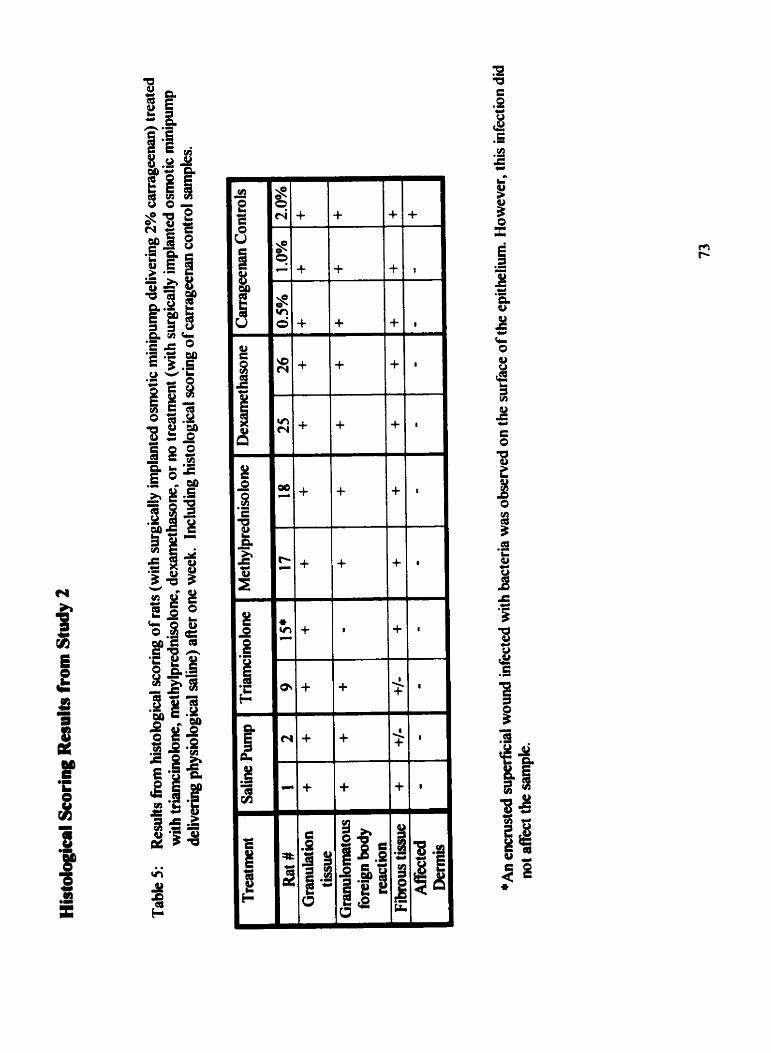
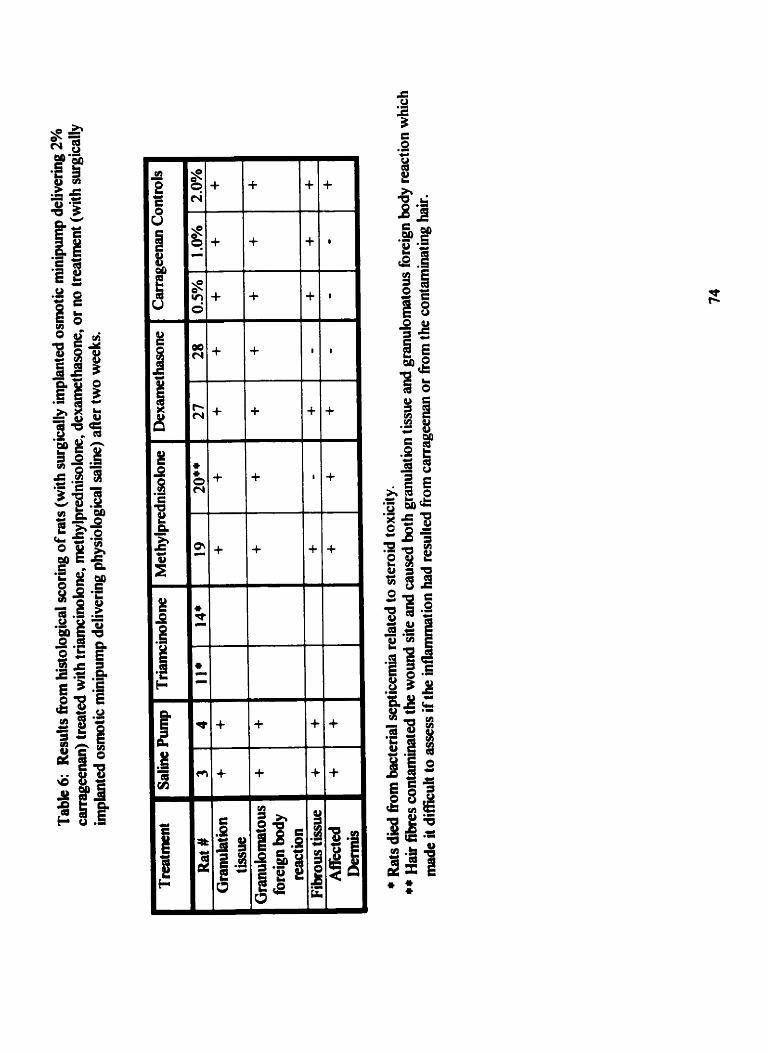
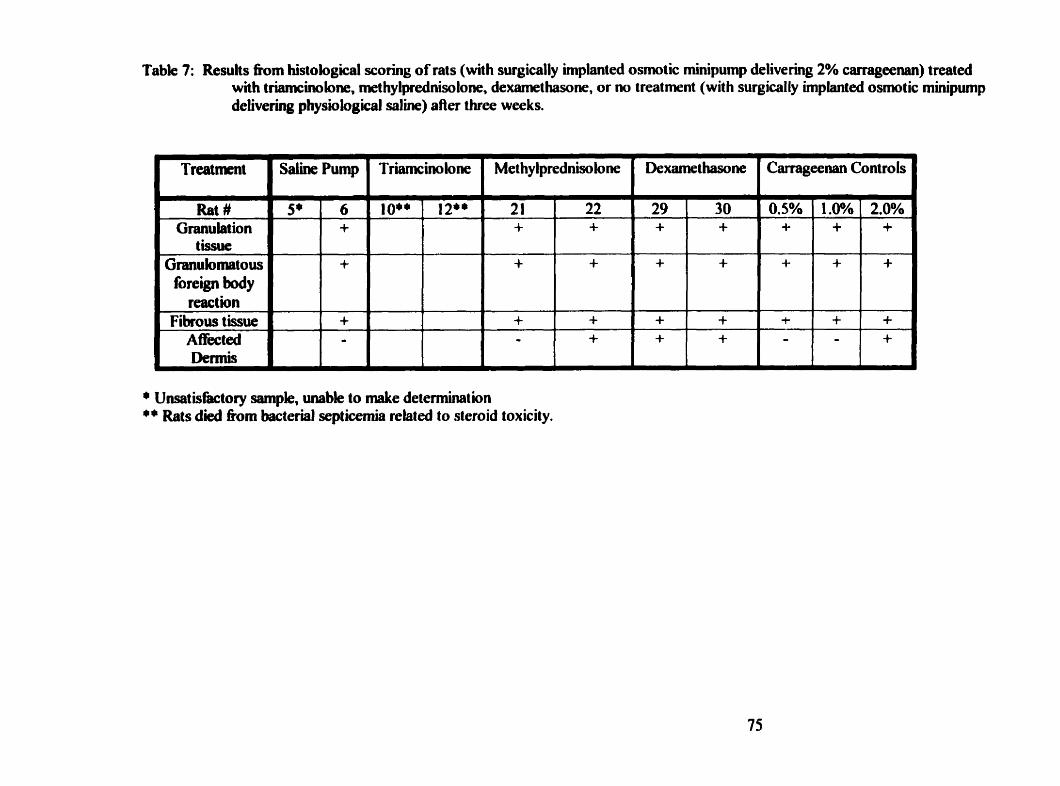
Tabk 7: Resuhs h m histological scoring of rats (with surgically implanted osmotic rninipump delivering 2% carrageenan) treated with triamcinolone, met hy lprednisolone, dexamethasone, or no treat ment (wit h surgically implanted osmot ic minipump delivering physiological saline) aAer three weeks.
Rat # Granulation
tissue Granulomatow foregn body
react ion Fibrous tissue
Affect4 Dennis
- Saline Pump TriamcinoIone Met hylprednisolone Dexamethasone ' Camgeenancontrols
* Unsatisbctory sarnple, unable to d e determination ** Rats died fiom bacterial septicemia rehed to steroid toxicity.
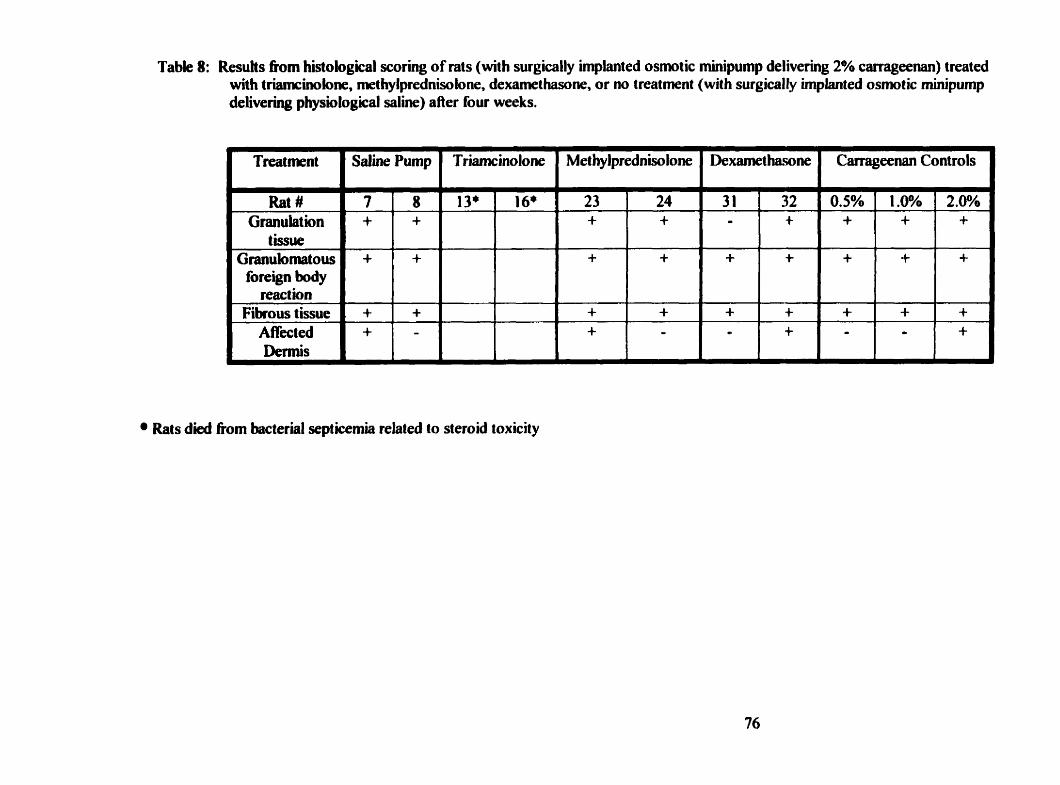
Table 8: Resuhs h m histological scoring of rats ( with surgically Unplanted osmot ic minipump delivering 2% carrageenan) treated with triamcinobne, methylprednisolone, dexamethasone, or no treatment (with surgically hplanted osmotic minipump delivering physio logical saline) a fier four weeks.
Rat # Granulation
tissue Granulomtous
foreign body reac t ion
Fibrous tissue Afiiected Dermis
Rais died fiom bacterial septicemia related to steroid toxicity
Histological mults one week after implratation of miaipumps for male Wistar nts
Table 5
Mer one week, the glucocorticoids were unable to prevent the formation of granulation tissue
or foreign body grimulomatous reactions. Nor were the treatments able to prevent the formation
of fibrous tissue. Many of the observations were scored as intermediete for the fibrous t h
because the early stages of fibrous tissue formation is difncult to dflerentiate fiom the histology
of granulation tissue.. The histology of the dennis was not dected in any of the treatment
groups.
The carrageenan controls, used to optimized the concentration of carrageenan, were positive for
ail the markers.
Histological mults two weeks i f ter implantation of miaipumps for male Wistar rats
Table 6
Mer one week, the remaining rats in the triamcinolone treatment groups had died. It was found
a h autopsy, that the rats had died fiom septicemia
The glucocorticoid treatments were unable to prevent the formation of granulation tissue or
foreign body grandomatous reactions. M e t two weeks the granulation tissue had begun to
affect the histology of the de* in all of the treatment groups.
The carrageenan controls were positive for ail the markers.
Hbtobgical resutts t h m week after implantation of minipumps for male Wistar rats
Table 7
The glucocorticoid treatments were mt able to prevent any of the observed markers &orn
occurring. The histology of the dermis was ody affected in the methylprednisolone and
dexamehsone treatment group and not the control group.
The carrageenan controls were positive for al1 the markers.
Histological mults four neeh ifter impiantatioa of minipumps for mak WLtar rats
Table 8
The glucocorticoid treatments were not able to prevent any of the observed markers from
occurring. The granulation tissue had afEected the histoiogy ofthe dermis in al of the treatment
groups.
The carrageenan controls were positive for al1 the markers.
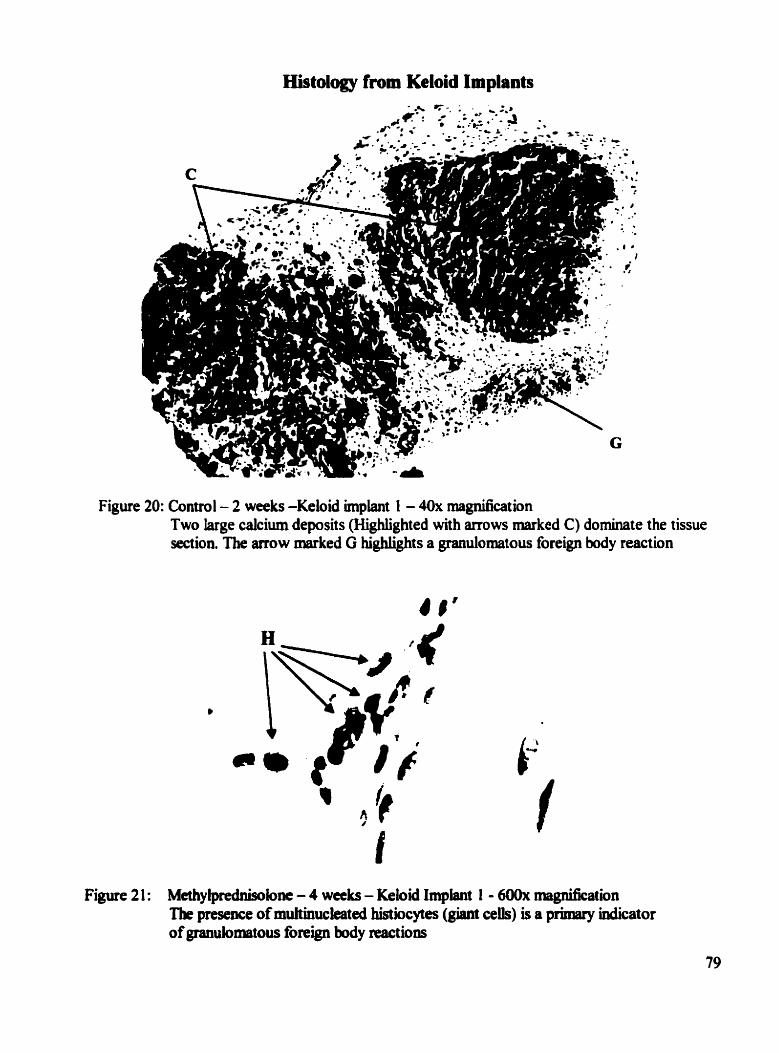
Histology from Keloid Implants
Figure 20: Contro 1 - 2 weeks -Keloid implant 1 - 40x rnagnification Two large calcium deposas (Kghlighted with arrows marked C) dominate the tissue section. The anow marked G highüghts a granulomatous foreign body reaction
Figure 2 1 : Methylprrdnisoloat - 4 weeks - Keloid Implant 1 - 6ûûx magnification The presence of muhinuckated histiocytes (giant cells) is a pniiary indicator of grandomatous foreign body mctions
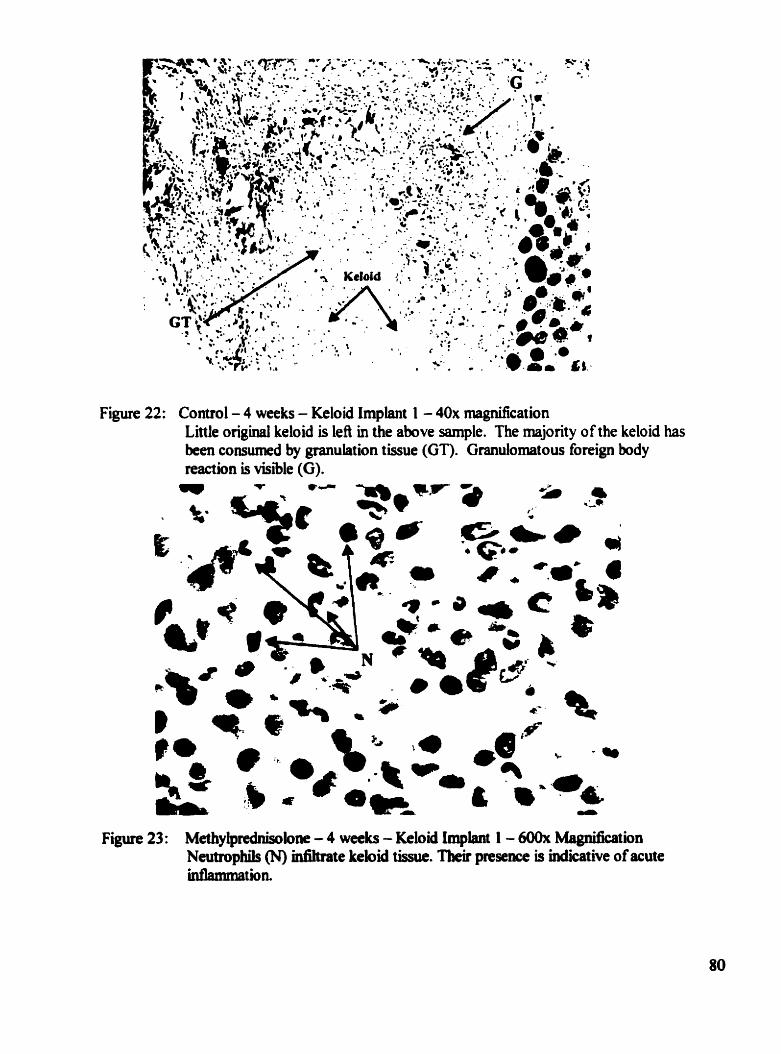
Figure 22: Control- 4 weeks - Keloid Implant 1 - 40x rnagnification Little original keloid is lefl in the above sample. The majority ofthe keloid has been consumed by granulation tissue (GT). Grnulornatous foreign body teaction is visible (G).
Figure 23: Methylprednisokne - 4 weeks - Keloid Implant 1 - 600x Magnification Neutrophils (N) mfihrate kebid tissue. Tbeir presence is indicative of acute inflammation.
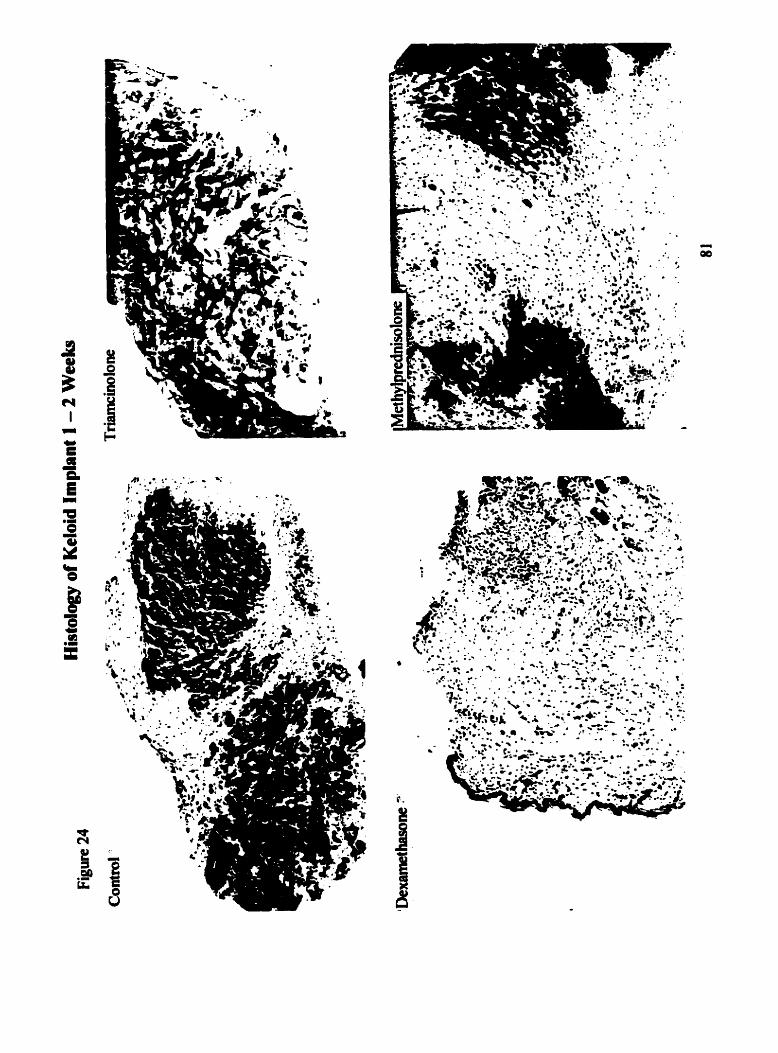
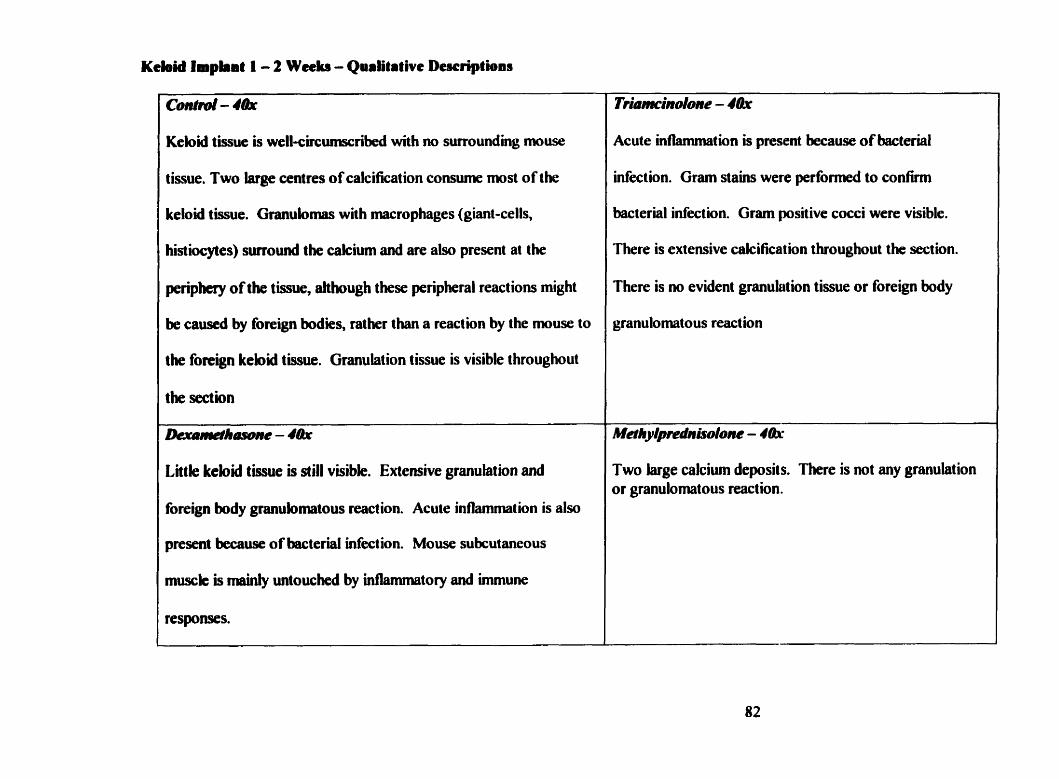
Kebid laphi t 1 - 2 Wcdu - Qualitative Descriptions
ConW - 4&
Keloid tissue is well-circumscdbed with m surroundhg muse
tissue. Two large centres of calcification consume most of the
keloid tissue. Granulomas with macrophages (giant-cells,
histiocytes) surround the cakium and are also present ai the
periphery of the tissue, ahhough these peripheral reactions might
be causd by foreign bodies, rather than a reaction by the muse to
the foreign kebid tissue. Granulation tissue is visible t hroughout
the section
h ~ h a w n e - 4tk
Little kebid tissue is still visible. Extensive granulation and
foreign body granulomatous reaction. Acute inflammation is a h
present because of bacterial infect ion. Mouse su bcutaneous
musck is mainiy untouched by intlannnatory and immune
responses.
TriamcinoIo~~e - 4 k
Acute inflammation is present because of bacterial
infection. Gram stains were performed to confimi
bacterial infection. Gram positive cocci were visible.
There is extensive calcification throughout the section.
There is no evident granulation tissue or foreign body
granulomatous reaction
Two large calcium deposit S. There is not any granulation or granulomatous reaction.
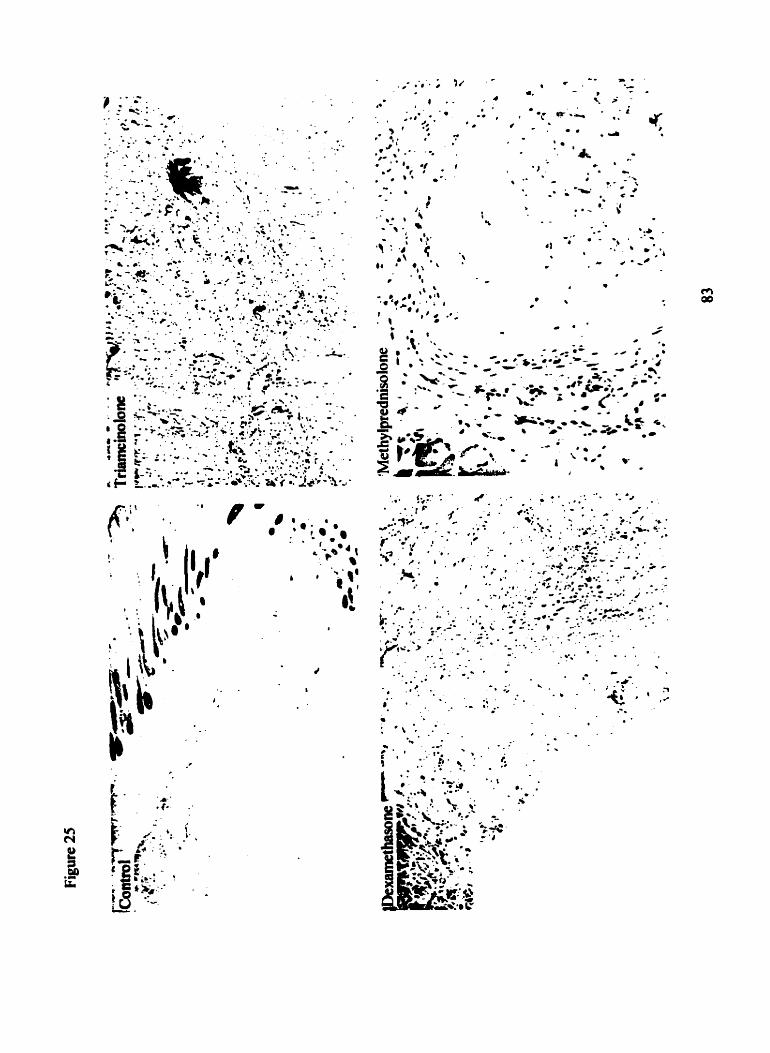
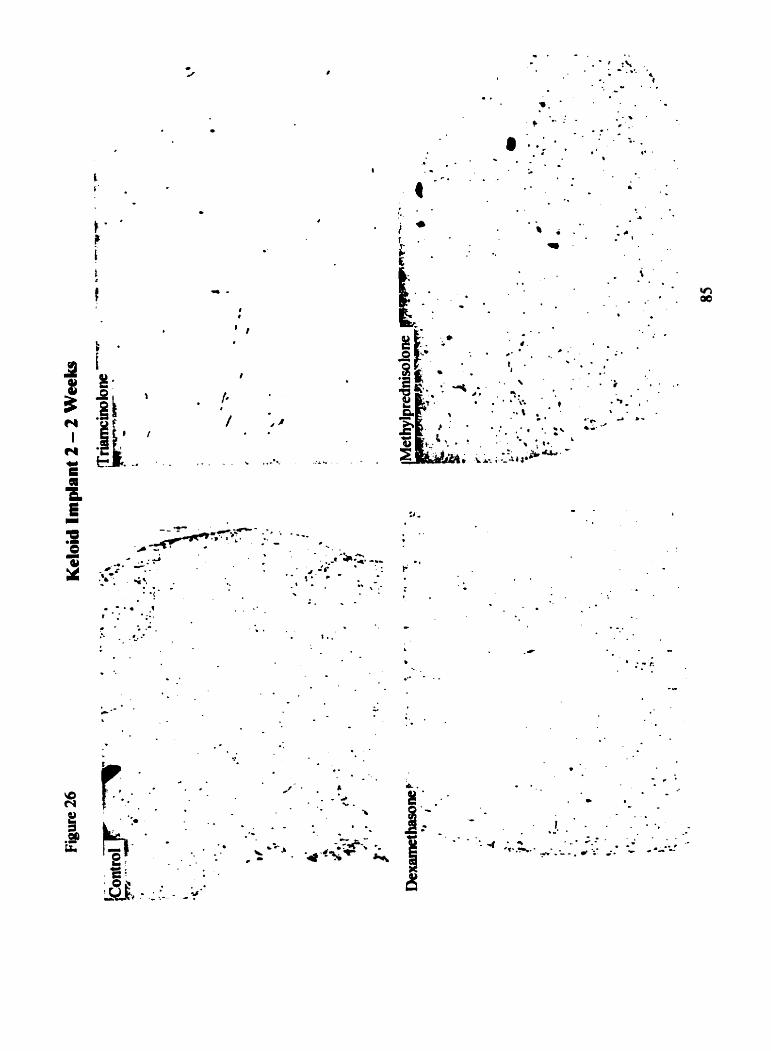
Conhrd- 4Qr
Keloid tissue with mild granulation and granulomas at the
periphery of the section.
~ - ' h ~ e - 4&
Very similat to triamchdone sampk, however both
granulation and granulomatous reactions have begun in
this section.
Triamciindone - lObr
Keloid tissue with no granulation or granulomas. Tissue appears
as it would if it had never been excised.
Methy@rednirsolo~~e - 48x
Granulation and granulomas sunound the keloid section.
Calcium deposits are visible throughout the section.
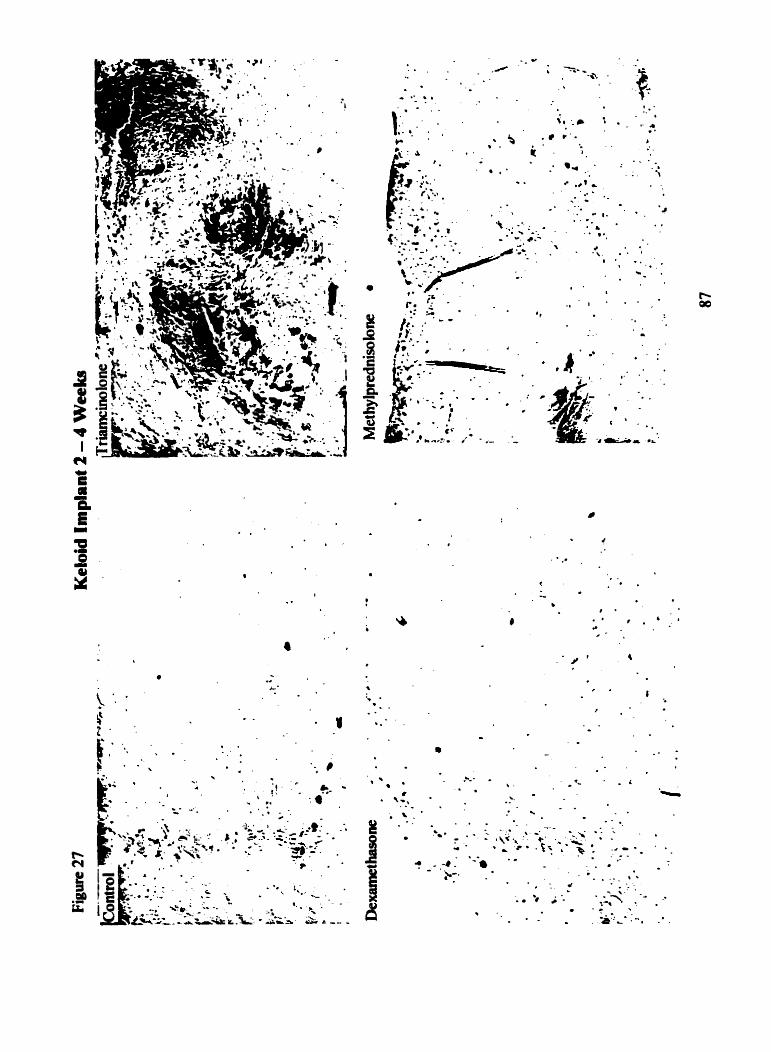
\;.: ;. . ; ..? . , r I . - 5 : . ' k p:- t h ? . . . . . a . . . . . . 4.
. S . & .= . . ' . \ d . - L n - 4. t e , Y.; ; ; - . . .*
' : - - - - . W. .- * - -,'" .*' Lm. . 9 --.-. ***; ' 9' : - . b
.. .... * *
8 .* ;
r ' . . . - . 1
: 9- ... i # t r : ' .
. < ._ .. - . - . * . . .. 0 1- .... . . ' & '. m.,
\ J - . \ . 8
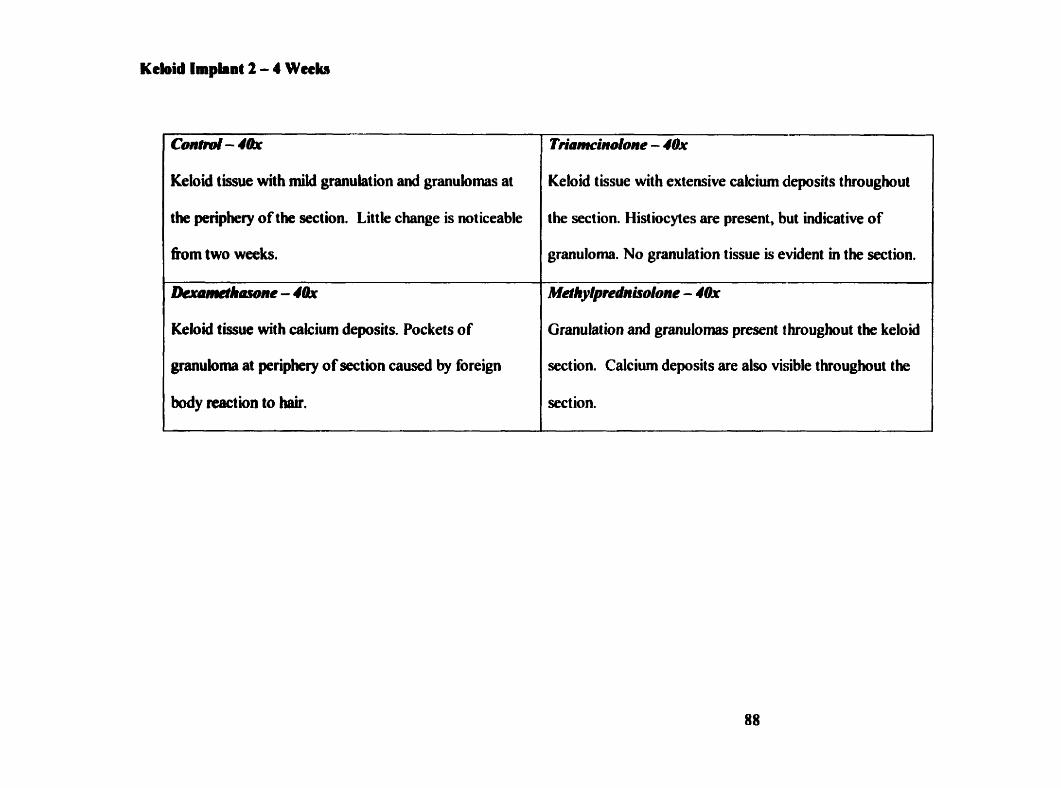
ConW - 4&
Keloid tissue with müd granulation and granulomas at
the periphery of the section. Little change is not iceable
fiom two weeks.
Lkwwîhawne - 4Q,
Keloid tissue with cakium deposits. Pockets of
granuloma at periphery of section caused by foreign
body reection to M.
Keloid tissue with extensive cakium deposits throughout
the section. Histiocytes are present, but indicative of
granuloma. No granulation tissue is evident in the section.
Granulation and grnulornas present t hroughout the keloid
section. Calcium deposits are also visible throughout the
section.
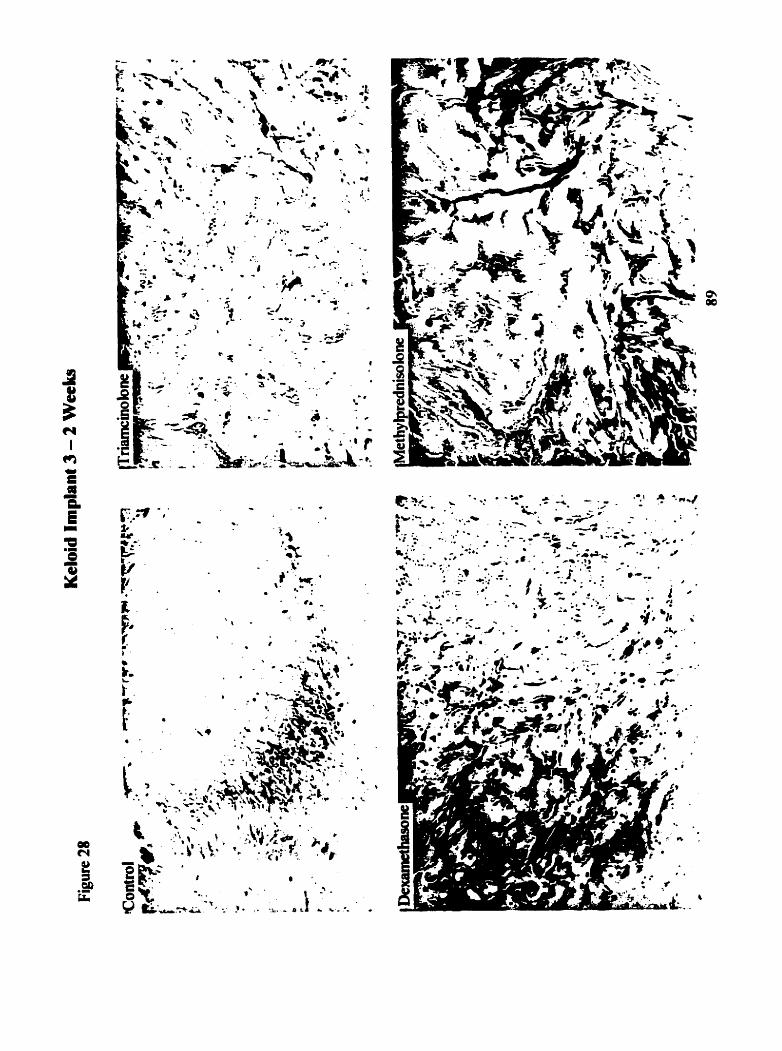
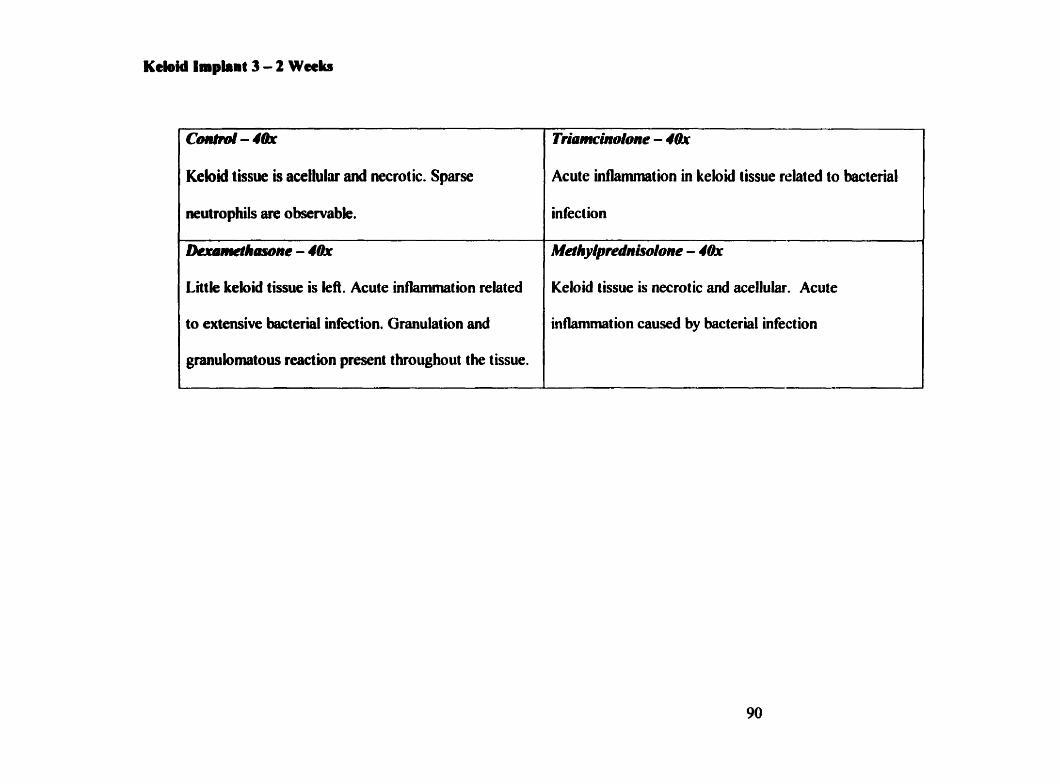
c m - 4th
Keloid tissue is acelluliu and necrotic. Sparse
neuttophils an observabk.
Dcrcomeîhasone - 4&
Little keloid tissue is lefi. Acute inflammation related
to extensive bacterial infection. Granulation and
granulomatous reaction present throughout the tissue.
Triamcinolone - 40x
Acute inilammation in keloid tissue related to bacterial
infect ion
MethyIprednisoIune - 4&
Keloid tissue is necrotic and acellular. Acute
in flamrnat ion caused by bacter id infect ion
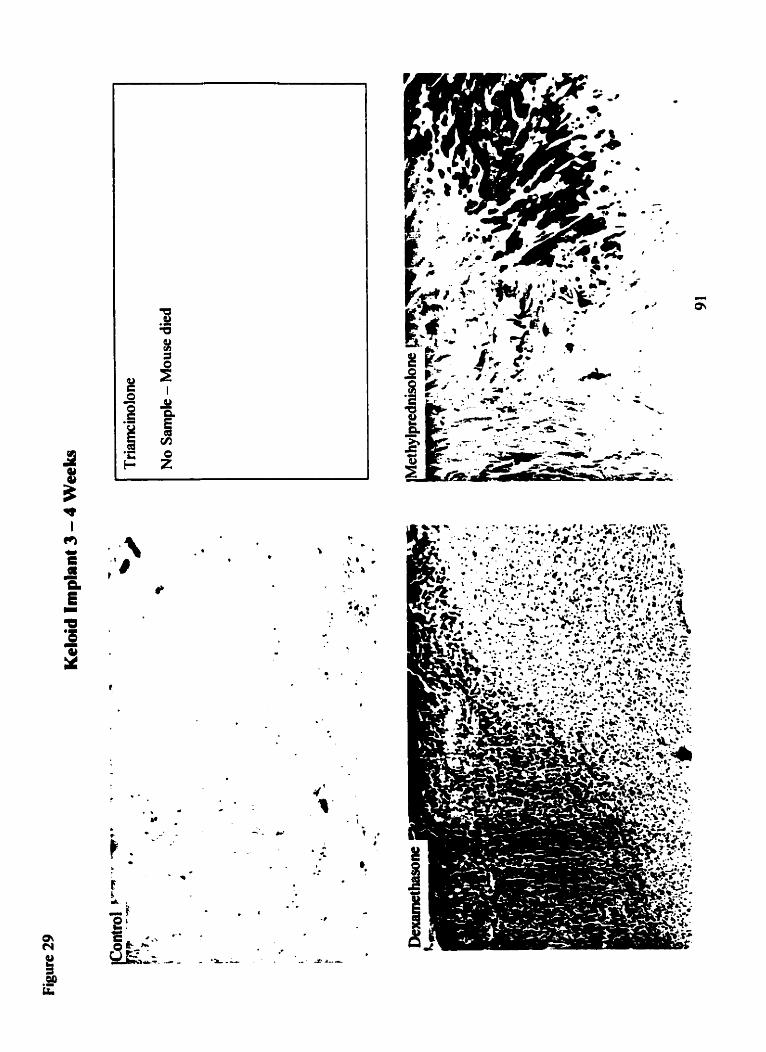
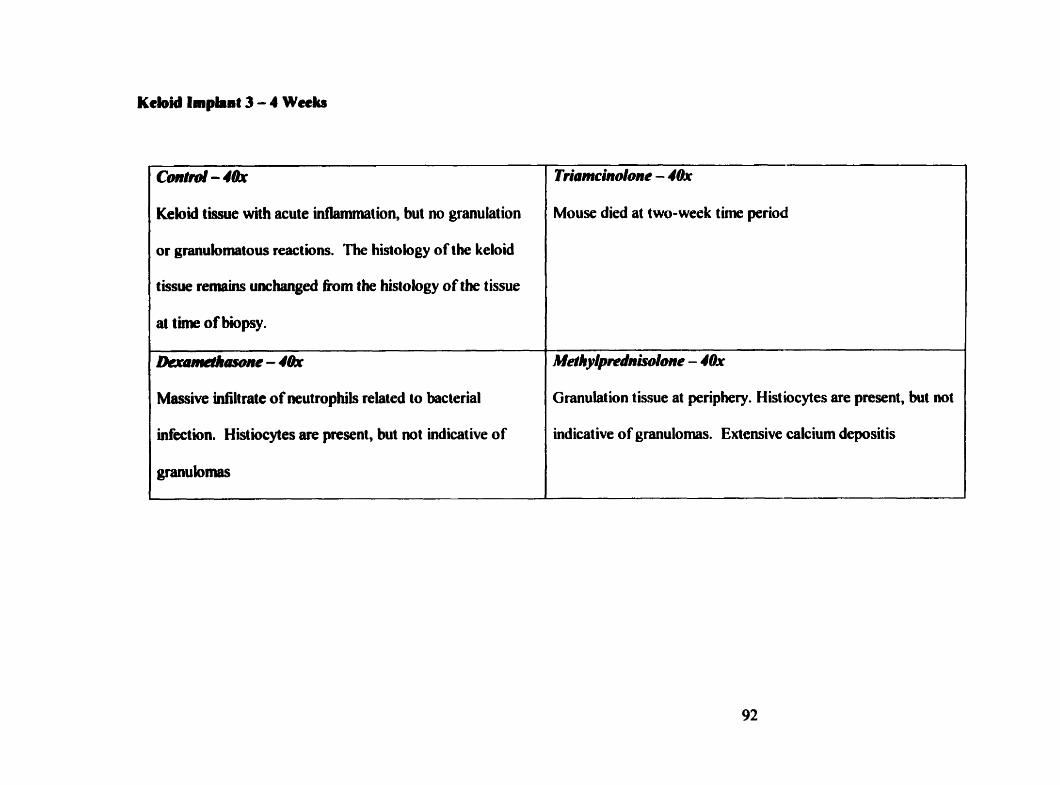
conhd - I&
Keloiâ tissue with acute Uitlamniation, but no granulation
or granulornatous reactions. The histology of the keloid
tissue remains unchangeû fiom the histology of the tissue
at time of biipsy.
JLrd-'"e - 4&
Massive infiltrate of neutrophils relaied to bacterial
infection. Histiocytes are present, but not indicative of
granulomas
Triomcindone - 4&
Mouse died at two-week t h e period
M e ~ h y ~ ~ d n ~ o n e - 4Ox
Granulation tissue ai periphery. Histiocytes are present, but not
indicative of granulomas. Extensive calcium depositis
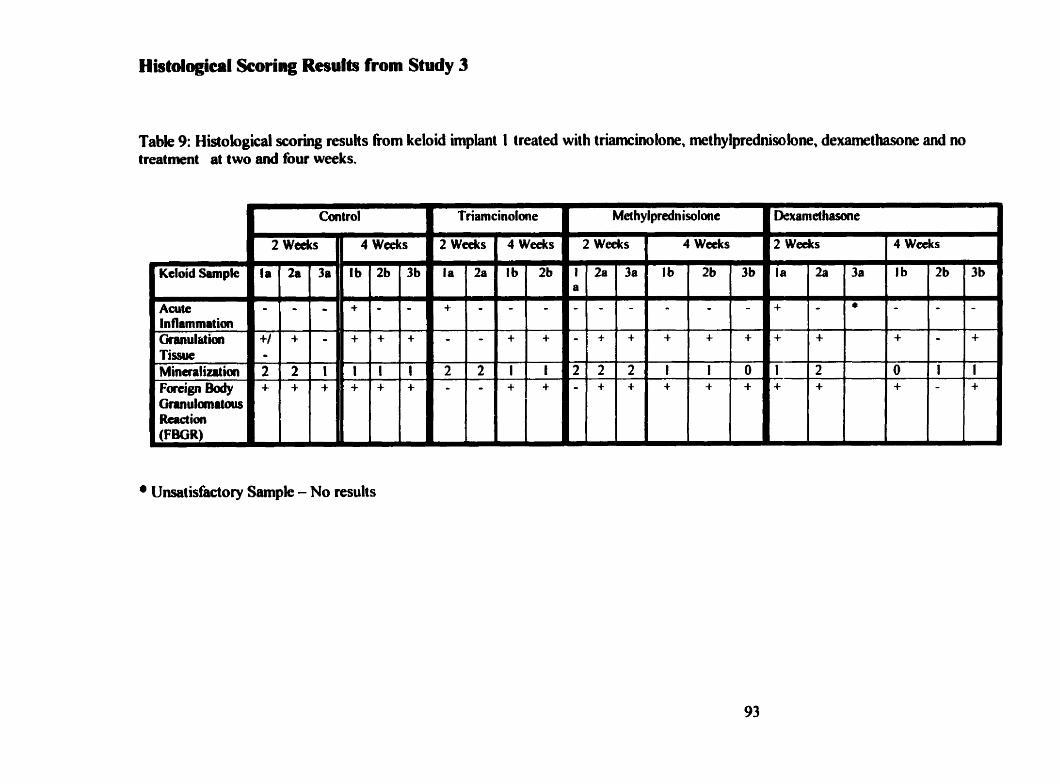
Histologica~l Scoring Rcsulb from Study 3
Table 9: Histological scoring resuls fiom keloid implant 1 treated wit h triamcinolone, methy lprednisolone, dexamethasone and no treatrnent at two and four weeks.
- 4 weeks
Ib 2b
+ +
l f + +
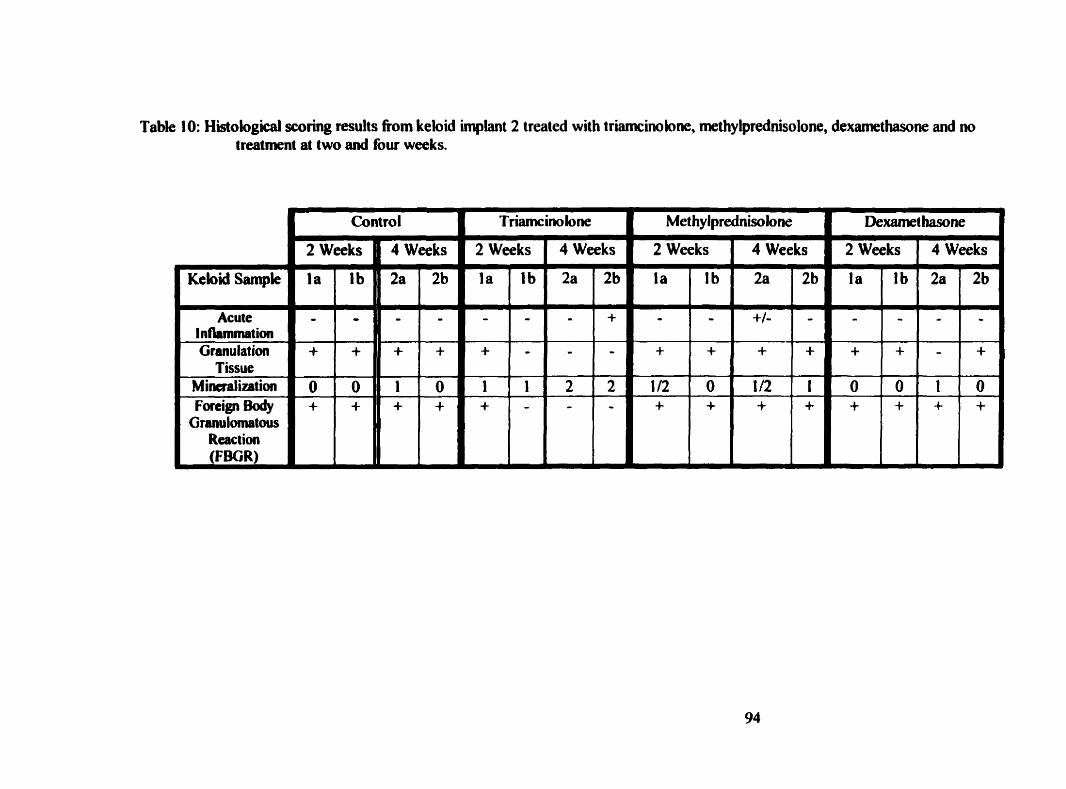
Table 10: Histological s c o ~ g results fiom keloid implant 2 treated with triamcinolone, methylprednisolone, dexamethasone and no treatment at two and four weeks,
4 Weeks 1 2 Weeks 4 Weeks ) 2 Weeks 4 Weeks
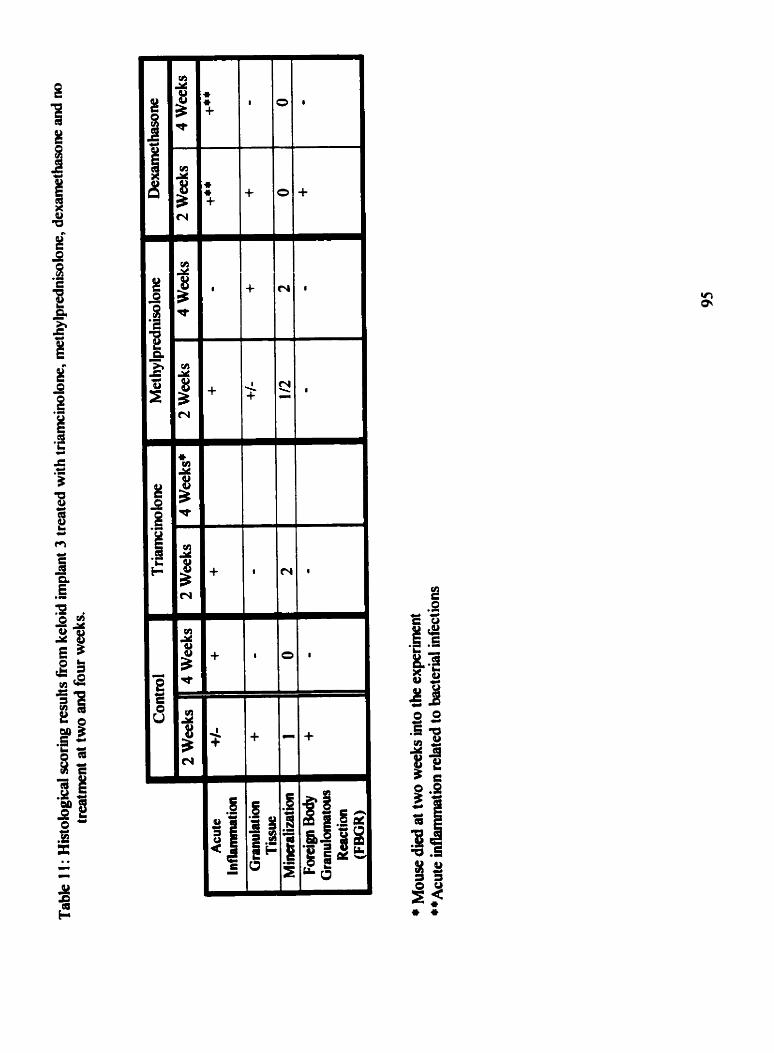
Histolgical Scoring Rnults of the keloid impiant 1, two and four weeks afier impbntation into an athymic mouse Table 9
There was not any observable pattem for the histological scoring in keloid implant 1 . No glucocorticoid
seemed to offer any advantage over one another. The anaiysis was more compiicated because of the
large calcium deposits a d bacteriai iafection observed in many of the samples.
Histological Scoring Results of tbe keloid implant 2, two and Cour wceks after implantation into an athymic mouse Table IO
niere was not any obsewable pattem for the histological scoring Li keloid implant 1 . No glucocorticoid
xemed to offer any advantage over one another. The analysis was more compkated because of the
large calcium deposits and bacterial infection observed in many of the samples.
Histological Scoring Results of the keloid impiant 3, two and four weeks ifter implantation iato an atbymic mouse Table 11
There was not any observable pattern for the histological scoring in keloid implant 1 . No glucocorticoid
seemed to offer any advantage over one another. The analysis was more complicated because of the
large calcium deposits and becterial mfeetion observed in many of the samples.
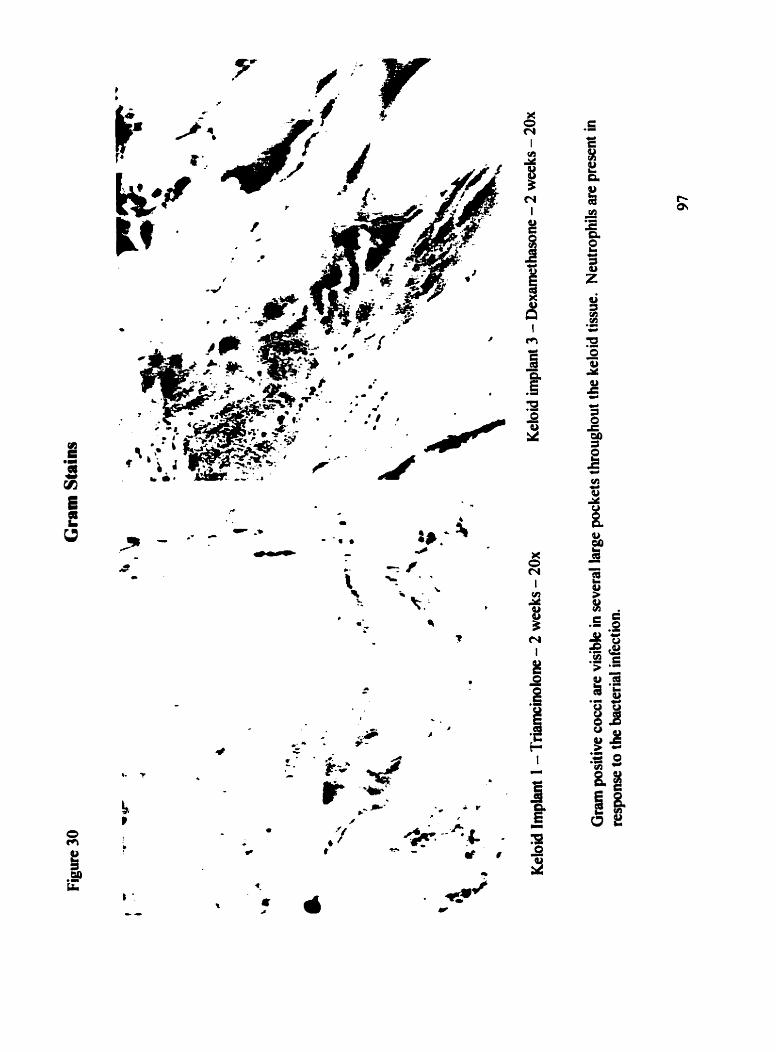
Many of the keloid samples stained with H&E appeared to be infiltrated with bacteria. In order
to d e t e d e the presence of bacteria, Gram stains were performed on al1 keloid tissue samples.
Figure 30 shows two representative Gram stains. On the left is a keloid samples treated with
aiamcblone for two weeks and on the right is a keloid q l e treated with dexamethasone for
two weeks. The purple stained areas throughout both samples indicate Gram- positive cocci.
The foilowing tables (1 2, 1 3, 1 4) tabulate the results of the Gram s t k and display which mouse
and which keloid sample were show to be infiltrated with bacteria aiter Gram staining .
The only treatment group not infected with bacteria was the control group probably indicating
that the glucocoxticoid treatment depressed the mice's h u n e response rendering them more
susceptible to bacterial infection.
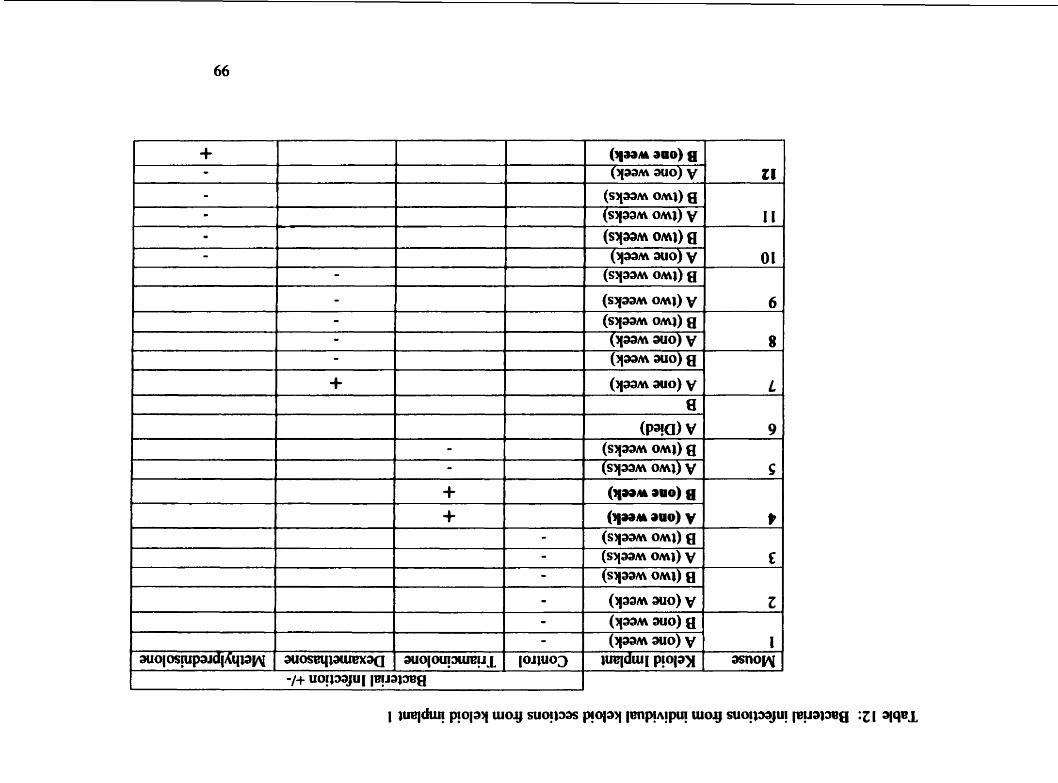
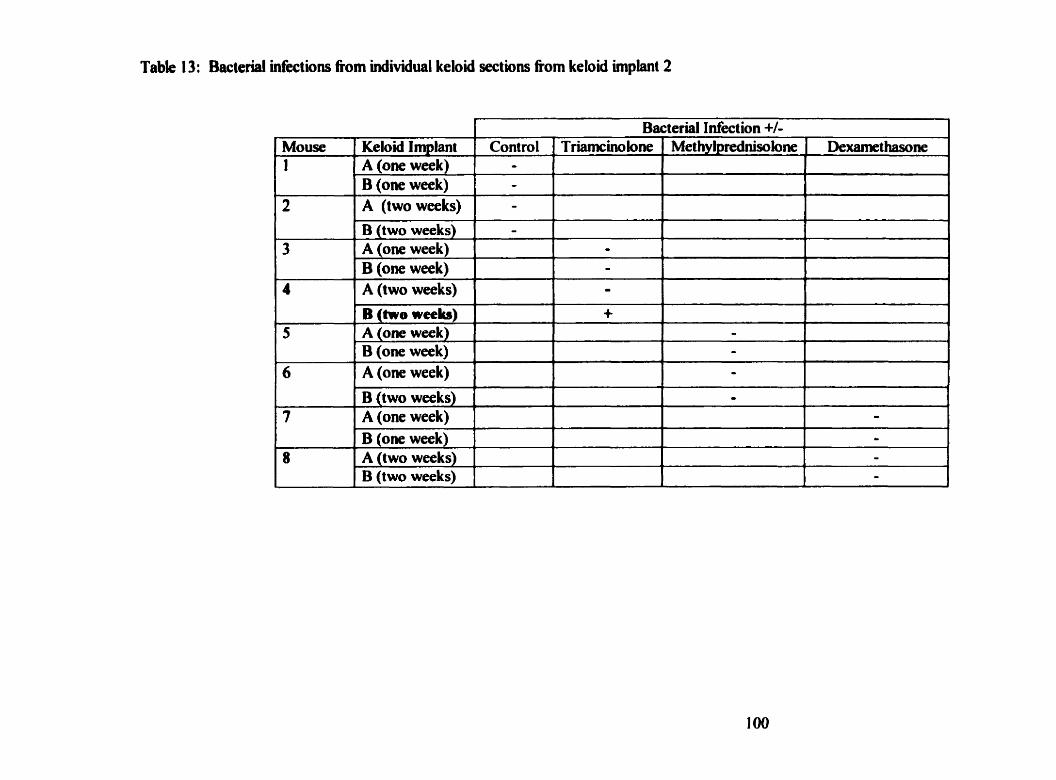
Table 13: Bacterial infections from individual keloid sections from keloid implant 2
1 Bacterial Infection +/-
5
6
7
Mouse 1
2
3
4
8
Methylprednisolone
-- B (Go-weeb) A (one week) B (one week) A (one week)
B (two weeks) A (one week)
D e x a m c h n e Keloidlmplant A (one week) B (one week) A (two weeks)
B (two weeks) A (one week) B (one week) A (two weeks)
B (one week) A (two weeks) B (two weeks)
+
Control [TriamcinoIone
L
- - - -
- - - O
- - -
O
- -
i
4
l -
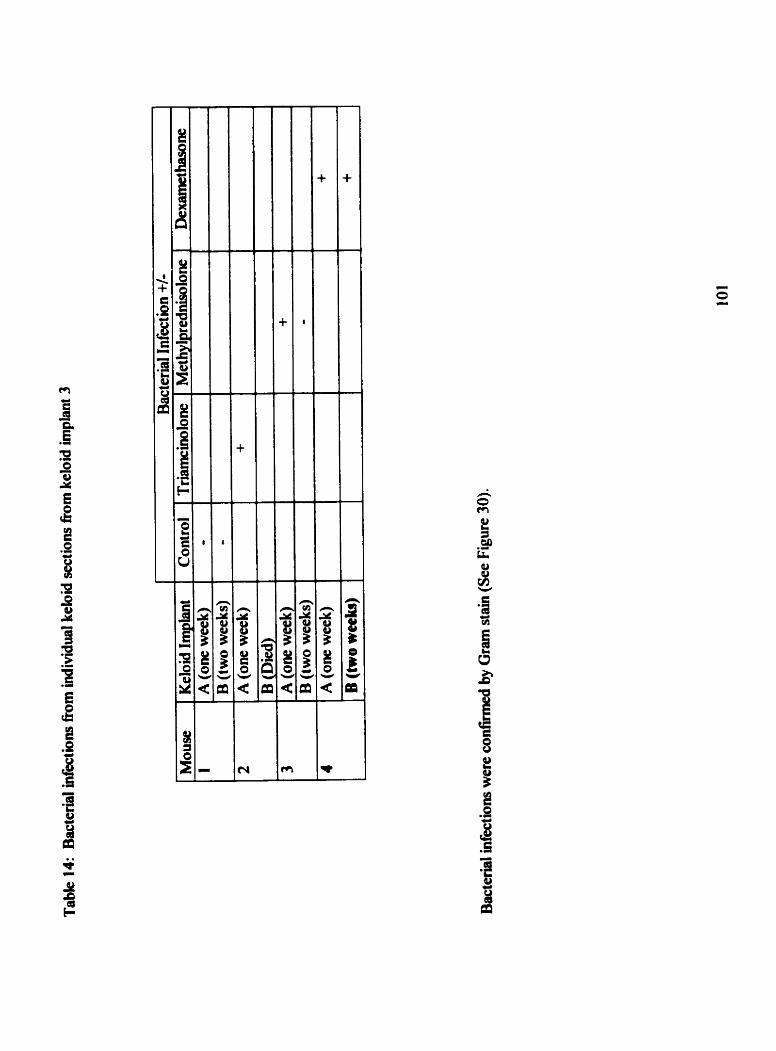
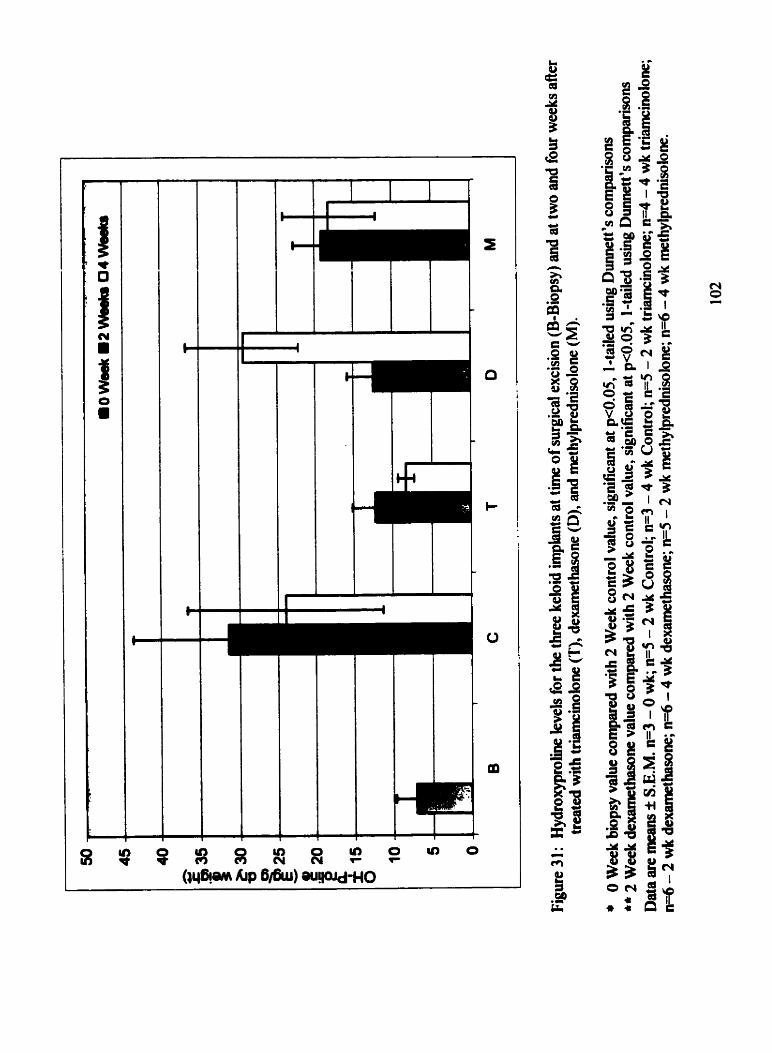
I I I
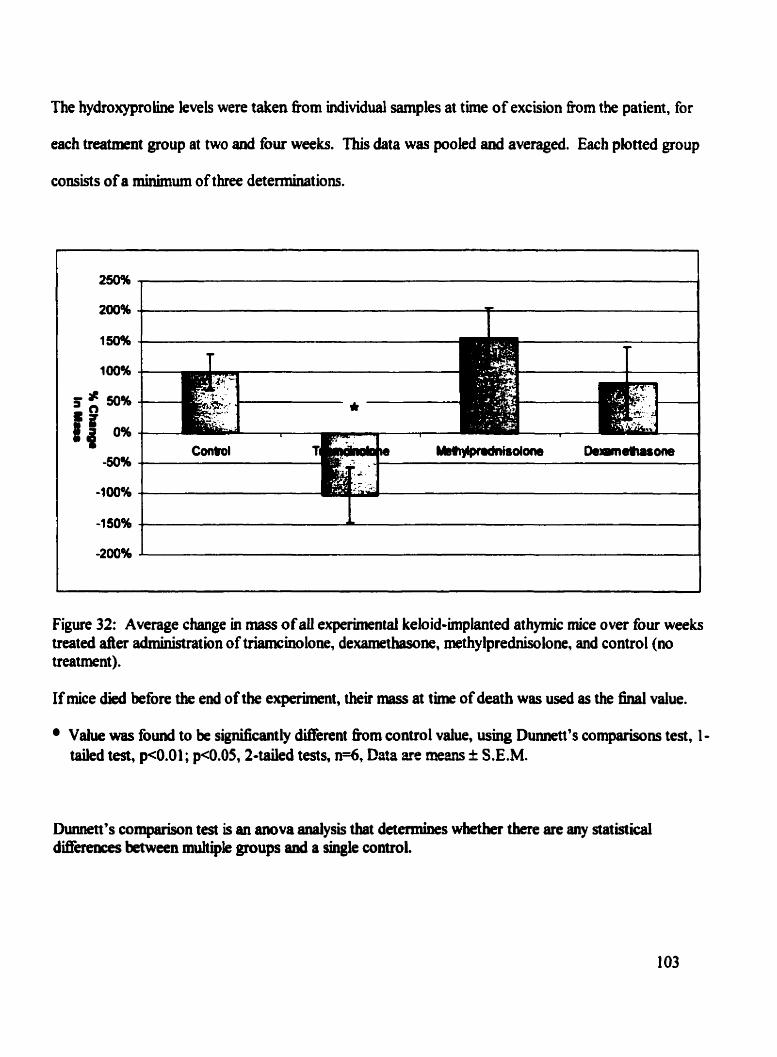
The hydroxyproiine levels were taken from individual samples at time of excision from the patient, for
each treatment group at two and four weeks. This data was pooled and averaged. Each plotted group
consists of a minimum of tbree determinations.
Figure 32: Average change in mas of a1 experirnentai keloid-implanted athyrnic mice over four weeks treated der administration of triamcinoIone, dexamethasone, w t h y lprednisolone, and control (no treatment ).
If Piice diod before the e d of the experirnent, theh m a s at time of death was used as the final value.
Vahw was found to be significantly different fiom control value, usmg Dunnett's compIuisons test, 1 - taiied test, pc0.01; p4).05,2-tded tests, n=6, Data are mem i S.E.M.
Dunnett's coqmison test is an anova Bnalysis that detemines whether there are any statisticai diffèrences between muhiple groups and a single control.
A. Observations following S r rge y Study 1
Tbree days d e r surgery, the rats kgan to scratch the area around the pump insertion resulting in
scarification. Their toenaüs were clipped to ieduce the darnage that they could inflict upon themselves.
A M e r precaution was taken by htroducing suIf'amethoxazole - trimethoprim (40-8 mg/mL, 4
mVSOOmL wter botîle) hto their drinking water, in order to prevent or elhinate ary x c o n d q
infections.
Study 2
Open superficial skin infections were observed on three rats in the control group. The lesions were
cleaned with peroxide and Vaseline@ was applied.
Four rats in the triamcinolone group showed signs of steroid toxicity. They displayed weight loss, paie
end fiagile skin, and an abnormal hunched posture. They were ail dehydrated; fluids were administered.
The teeth of one rat were clipped because abnorrnai growth was observed. Each of these rats received
acetaminophen (300 mg/Kg tid), daiiy for pain management.
Two of these rats were sacrificeci at the one-week intend and a third rat had to be sacdiced before the
second week interval had occurred. Each of the rats that died was examined by necropsy. Upon
autopsy, Ït was fourd the adrenal glards were normal, and the rats had died of secondary bacterid
infection.
The rats in the methylprednisolone group developed hernatomas around the pump insertion site, but
seemed otherwise beahhy. One rat developed diarrhea.
Study 3
At t k of removai, the keloid implants were located subjacent to the subcutaneous muscle. In many
experbental samples, the keloid was found to be overlaid by epidermal ukeration with superficial
crusting. The keloid itselfwas observed as an ovoid, firm, white, well-cucumscn'bed nodule located in
the midiine caudal to the scapulae and in the midline in the l u m k area between the hind legs. Prior to
implantation the keloid sample had been prepared by sectioning into d e r cuboid pieces using a
razor biade. When the keloid nodule was removed, it had assumed an ovoid appearance. However, the
keloid in all cases renïllned identical in appearance to the time of implantation.
Kebid sample 1
At 1 5 days, the athymic mice receiving triamcinolone were beginning to show signs of steroid toxicity,
hgile skin ami hunched posture. Therefore, the dose at each implant site was cut to 0.0125ml of
stemid. One mouse in the triamcinoloae group died on day 8. Therefore one m u s e was sacrificed at 15
deys aad both implants were rernoved. The remaining muse in the triamcinolone group was not given
a second dose because of its hg ik condition.
Keloid sampk 2
There were no mice fàtalities in this study group. AU of the treatment groups displayed a gain in mas,
except for the mice treated with triamcinolone.
Keloid siai pie 3
The triamcinolone muse died 17 days into the study. At tirne of death the mouse was fiail, weighing
17.0 g cornpared with 24.2g at thne of implant. The muse's skin was extremely fiagile.
The dexametharone mouse in this group showed an unusual loss of weight. AU of the other mice treated
with this corticosteroid experienced gains in mass. Although when all the mean changes in mass for all
of the treatment groups compared to control values were found to be not significant, except for
triamcino lone.
In addition, the four week dexamethasone keloid sample at the t h e of removal was a yellowish,
gelatinous iaass. This is inconsistent with other keloid samples, which were solid, white, weU-
circumscniid, ovoid masses. Due to the gelatinous nature of this sample, it was not possible to obtain
any histologicai data.
Discussion
Keloid scars are extremeiy difkult to prevent or treat effectively once established. No universally
accepted treatment for the revision of these scars exists (Nerneth, 1993). The range of treatment options
is diverse and no single approach offers an acceptably high fiequency of success (Urioste, 1999).
Treatment modahies vary among practitioners, partly because no matter which therapy is used a
relatively high degree of recurrence is o h e d and also because there is a lack of clinical evidence
coaclusively supporthg one method over another (Munay, 1994). The ditficulty of treating keloids led
Poiiack to conclude that "keloids are among the most perplexing of conditions treated by cutaneous
surgeons" (Shetlar et ai., 1 998)
Many studies have been performed exanMing different methods of treating keloids or preventing
keloids; fiom physical techniques such as radiation, lasers, or ultrasound to phamcological agents
ranging fiom corticosteroids to newer molecules such as interferon gamma (Berman and Flores, 1 998,
Granstein et al., 1990). However, there is no reported study to date that has presented a systematic
cornparison of tiamcinolone acetonide, a glucocorticoid that is the cornerstone of keloid treatment
(Urio ste, 1 999), with alternative glucorticoid treatments.
The need to study or to discover new treatments and prove the effectiveness of existing treatments is
important because of the high prevalence of keloid scars, especially out side of Europe and Nonh
America. Approximateiy 6-16% of the Atiican population form keloid SC= which means that there may
be 45 million people on the continent who will develop keloid scars at som point in their lives (Datub-
Brown, 1990). Amther study found an incidence of 4.5% and 16% in a predominantly black ard
hispanic population (Cosman et al, 1961). Alhady and Sivanantharajah, 1969, found an incidence ratio
between 5:l and 15: 1 when Blacks and Asians are compared with Caucasians. The devebpment of
keloid scars is essociated with cosmetic disfigurement, pniritus, contractures, and fiequently pain which
znakes audies hto the resolution or prophylaxis of this significant problem very important.
The lack of evidence for effective glucoconicoid treatment coupled with the epidemiological need for a
more effective treatment fomed the rationale for this study. There are three ways to approach the study
of keloid scars. The first method would be to compare potential therapies directly in a ciinical setting.
This is a costly and lengthy procedure. The resulting effects can then be monitored according to the
definitions of success that are outihed. Studies involving hunians can be ditncult with respect to
recniiting enough patients. ethics concems, drop-out rates, compensation to patients, and other logistical
concems. A further problem with this type of study is that it is ditncult to do any type of in vitro assay
during the study. N o d y , a biopsy would be taken and the tissue would be w d for the assay. This is
mt an option for people who have developed keloids because any M e r demial injury is ükely to
worsen the existing keloid scar or cause a new one to form Nonetheless, there are major advantages to
human d e s in that the scar is in its natural environment w b it has access to ail the endogenous
growth factors and processes that resulted in the generation of the scar tissue in the k s t place.
Tbe second mthod invoives using in vitro techniques such as tissue culture or test assays. Tbese
strate@ are excellent for examniing specific mechanistic questions and for oôserving the rates of
cbange of vatious biihemical pcesses in the keloid scar. Such assays are advantagrnus because the
108
experimental conditions cm easily be altered and new molecules added when necessary. However, the
goal of the present project mis to assess the efficacy of preventing and improving keloid scars. It would
be impossible to test for prophylaxis of keloid scars using tissue culture because the keloid scar already
exists. A prhmy &er of efficacy for this study was histological enamination of tissue sections
which would also be impossible with an in vitro study. If impediments could be overcome. an in vitro
assay would provide essential iosights into the clinical resolution of keloid scars.
Animai models are the third option to study keloid scars. Animais are an excellent choice because
experimental conditions can easily be rnanipuiated (not as easily as in vitro studies, but much more so
than in human studies). It is possible to house a number of animals for relatively little expense. Their
tissue ean be biopsied for histological and biochemical exarninat ion. It is potentially possible to test bo th
for the prophylaxis and reduction in severity of keloid scars using an animal model.
Ho-, the study of therapies directed at the prevention or amelioration of keloid scars in human or
a n i d models is challenging . The study of keloid scar formation in a labo ratory setting is very ditncuh
because only humans form keloid and hypertrophie scars (Urioste, 1999). There are certain animal
specks that form scars with simiiar outward appearance to keloids, but on rnicroscopic examination
these Lsioas tum out to be histologically d i s s i (Estrem et al., 1987). This leads to a dilemma; how
does OIE m a t e an animal mode1 of a biological process that only occun in humans. One solution as
descrbcd in this thesis is to meke use of an aMnal model that approximates the keloid scar as closely as
PO*.
A two-phase animal mode1 was chosen for this study . The goal of the fbst phase was to create an
enviromnt around an incision that would resernble the conditions that lead to the generation of keloid
tissue in hurnans. Keloid scars are the result of a disproportionate nbroblastic response to a dernial
wound (Tredgett, 1997). The basis of this i m b h c e lies in the idhmmatory stages of the wound
healiag response where macrophages and platelets release numerous cytokines that promote fibroblastic
and angiogenic activities resulting in a ptoüferative growth of the tissue surroundhg the wound site.
The uiicontrolled growth overwhelms the natural inhiiitory processes that normaily serve to terminate
the wound-beaiing process when mature scar tissue has been formed.
For unknown reasons. the wound environment is highly susceptible to the presence of TGF-P. This
could be occurring because there is more TGF-P than usual or because its receptors located on the celi
membnine of fibroblasts are present in larger numbers. It is important to note that it is not only the
presence of growth &tors that lead to keloid scaning, it also the inhiition or dom-regulation of the
mechsnisnis that usually couterbalance the pro liferat ive process.
The d e of TGF-P m the healing wound is muhidimensio~ but al1 of its actions have the sarne net
effect, which is the promotion of new tissue generation. TGF-p is released fiom two diierent sources;
mcmphages (de novo synthesis) and platelets (degranulation). Once released into the wound site, TGF-
f3 acts as a chemoattractant for leukocytes (neutrophils and monocytes) and fibroblasts.
TGF-p's prrsence is respomible for up-reguiating the synthesis of coüagen and other members of the
ECM, such as fibronectin. It also WVis the proteases capable of remodelüng the ECM. The resuhing
imbalance in the rate of formation of ECM proteins leads to the aggressive fibroproliferative growth that
is cbaracteristic of keloids. Essentially TGF-P prolongs the anabolic stage of tissue growth and prevents
the catabo tic stage of remdelling.
The expehmtal conditiotls of the first phase of this study attempted to create a long-lasting
carrageenan-induced hyper infhmmatory state that would approximate the characteristic conditions
Ieading to exuberant kebid growih
An osmotic rninipump containhg 2% carrageenan was inserted into a dorsal subcutaneous pouch of
male W ~ a r rats. Subcutaneous carrageenan causes locaiized subcutaneous Ulflammation
approximating the keloid state. The minipurnp released its contents in a h e m fashion over a period of
two weeks resuhing in a chronic state of infkmmation (See Figures 14 and 1 5).
A pilot-study was performed to determine the optimal concentrat ion of carrageenan to be delivered by
the minipump. Three concentrations up to two per cent were used (0.5, 1 .O, and 2.0%). Suuiwa et al.,
1992, used the same rnodel of idammation induced by carrageenan to mode1 keloid scars. They chose
a carrageem concentraiion of l.û%. However, it was f o d that 2.W carrageenan caused the kgest
maanmiatory respome h m the rats (See Figure 15). It was not possible to use any higher
concentrations because the carrageenan began to corn out of solution.
On histological exambition of tissue taken fiom rats at various time points over four weeks and with
vrinous glucocorticoid tttatments it was evident that carrageenan had exertecl Ïts effects on the healiag
wouad site. Grandation tissue, foreign body granukmatous reactions and fibrous tissue were observed.
111
These are all characteristic of a healing wound and they were alî observed in the dwerent tissue sectioas
(See Figures 1 6- 1 8). However, it was impossible to draw conclusions about the respect ive efncacies of
the three test glucocorticoids because there were no distinct differences among the treatment groups.
Pmblems with the experimental technique made the analysis even more cornpiicated. Many of the
grandomatous foreign body reactions were to hait shafis that had contaminated the wound site. Despite
steriie surgical technique, it was stili not possibk to remove al1 the hair fiom around the surgical incision
site and to prevent it fiom entering the operative site. A h , the injection site for the test glucocorticoids
ofien showed formation of fibrous tissue which made if diîiicult to interpret the resuhs.
The inabities to identify the source of fibrous tissue (whether it originated fiom glucocorticoid
injections or fiom the actions of carrageenan) and to keep contamhants out of the wound site rnake any
conclusions about the relative efficacies of the glucocorticoids impossible.
With better surgical technique this mode1 Mght prove more effective as a xreening tool for therapeutic
agents. Ultimately, however, this mode! wül never be able to be a tme predictor of a compound's
efficacy with respect to ameliorating or preventmg the formation of keloid scars because rats do not
form keioid scars. They hyper--tory state eventually matures into a typical scar which is
cbaracterized by thin, loose, psraUel, collagen bands and wt tbe thickened, chaotic histology seen in
keloid scars. This type of scar is sUnilar to the n o d scaning process in hunians. For this reason, the
carrageenan mflsnmietory mode1 is an Mffoctive tool for evaluating keloid scar îberapies.
Athymic Mousc as a Compromise
Nude athymic mire lack a thymus, which prevents them fiom producing mature T-ceh. T-ceils are
crucial cornponents to the immune response (See Figure 4) and without thern the mice lack the ability to
produce a ceil-mcdiated immune response. which means they lack cytotoxic Tcells. These cells are
potent d i a t o n of a full immune defence. Athymic mice are still able to produce neutrophils,
monocytes, macrophages (histiocytes), and antibodKs which are capable of locating and digesting
foreign matter. The humoral response produced by the plasma ceils and mediated by B ce* is aiil
present and capable of producing antibodies despite the lack of helper T-cek. Direct stimulation of the
humoral response is mediated through antigen-presenting tek. which are macrophages that have
eaBulfed foreign material. However, direct stimulation of B-ceUs results in an attenuated response when
compared to the response generated by the cell-rnediated pathway and helper T-ce& (Campbell, 1 993).
Since no animal is known to fonn a scar that bas morphological, histologicai, and biochemical
properties similar to the human keloid scat; an attractive option is to implant human keloid tissue into an
animal bost . The immunobgical deficiencies of the nude athymic muse make this species a suitable
candidate for implantation of foreign tissue.
Shetler et al, 1985, pioneered a method wbereby human keloid tissue was excsed and subsecpently
implanted mto a subcutaneous pocket in an athymic mouse. The founà the miplant retained histological
integr@ for 246 days, but that ECM proteins decreaseâ with the.
The viabiiity of Shetlar's mode1 for studying keloids has k e n indepedently c o h d by many studies
113
including those by Estreem, Kischer, and Waki. Shetlar et d ' s animai mode1 has k e n viewed as the
ody way to study keloid scars directly.
Erpcrirncnd Data
Phase One - Study Two
The goai of this study was to identify the most effective glucocorticoid for reducing the severity of
m8ammation. nie results fiom the histological scoring of the tissue sections fiom both phase one and
phase two are presented in tables, (See Tables 5-8). No real pattern is observable in the results fiom the
tissue sections taken from the experimental rats and it bas not been possible to draw any conclusions
fiom these results because empirically the glucocorticoids did not seem to have any consistent effect on
the severity of the inflammation.
The only definitive conclusion was that the dose of triamcinolone employed was too high because six of
the eight rats in that group died fiom steroid-related toxicity. The staff pathologist at the Central Animal
Facility at McMaster University performed autopsies (See Appendix E) and found that the rats had died
k m severe coccal pyelonephritis anâ skin rpsis resuhing in fatal septicemia.
The adrenal glands were removed fiom aii of the triamcinolone-treated rats and examined histologicaily
to asses wbethei the ghrocorticoYls had Bduced h n a l insufneiency. Ail the adtenai gleads
examid were fouad to be nonaal. The rats, had apparently died of severe septicemia probably related
to a d e p d immune system secondary to glucocorticoid admnistni . . tion.
Using carrageenan, it was possible to create severe inflammatory conditions leading to the formation of
granulation tissue, foreign body grariulomatous reaftions, and fibrous tissue (See Figures 16-19), yet it
was often dficult to determiw the precise ongin of these phenomena. For exarnple, in rnany tissue
sections granulomatous foreign body teactions were caused by bair s M s that had contaminated the
wound site. Also. in sorne tissue sections, nbrous tissue was created at injecion sites. These
observations compiicated any attempts to draw conclusions from the fint phase of this study and
c o n h e d the need for direct study of human keloid scar tissue as attempted in study three.
Phase two - Study T h - Human Kcloid Tissue
It was the goal of this phase of the study to identify which glucocorticoid was the most effective at
resohing the dense collagen fibrils of a keloid scar and establish whether there was any validity to the
predominant use of triamcinolone for treating keloid scar tissue in humans.
Excised keloid scar tissue was obtained fiom three separate patients varying in race, age, and gender
( M o American female, 25; North Amencan Aboriginal Male, 19; A6ro Amencan female, 29). Criteria
for histological scoring were defkd with the help of Dr. Sam Salama, a dermatopathologist at St.
Joseph's Hospital. The results fiom the histological scorhg can k seen in Tables 9-1 1. It was again
difficuh to dtew any conclusions h m these rrsuhs although sample numbers are d; there is no
apparent coasistency within a particular matment or a particular keloid Unplant. It is ûue that
individual keloids can Vary widely h m one another, with respect to their response to therspeutic agents
(one of the reasons making their effective clinical treatment more ditncuh). Since the three keloids
corne fiom varying locations and fiom patients with varying race, age, and gender it might be teasonable
to conclude that diffetences in histologicai scoring would exist between keloid samples. However, there
are inconsiPtencies for a particular treatment within the sarne keloid implant. Figures 24-26 show
representative pictures of histologicai slides fiorn the three différent keloid implants at two and four
weeks.
There are distinct histological diflierences observed with the admuustra . . tion of triarncinolone. Bo yadjiev
et al.. 1 995, teponed that keloid tissue treated wit h triamcinolone displayed a weil-de fined dermis wit h
fine collagenous fibrils and a lack of nodular collagen formations in the dermis. One of the
characteristic histological markers in keloid tissue is the appearance of coliagen ''whorls" or nodules and
the lack of a well-dehed dermis due to random and chaotic cohgen deposition.
The importance of sarnpüng cannot be emphasized enough when one of the markets of a study's success
is histological examination. When the keloid sections were removed îiom the mice they were ovoid.
Each section was split in halfand one haifwas used for histological examination. It is very possible that
this division could have obscured miportant nsuhs. It is ke iy that any pulomatous reaction or acute
idhmmation occuring in the kebid tissue would be present at the edges of the ovoid-shaped keloid
miplant. It is, therefore, possible k t the amount of obsmed grmuIoma aad acute mtlainmetion could
be unrepresentative of the acnial histological character of the tissue samples. The tissue was W e r
sectioned for staining and mountîng on a siide. Tbcse sources of experimentd e m r could have skewed
the results by overemphasizing ceriam instances of defbed histologicai markers becaw of poor
sampling or deernphasizing other markers because tbey were m v e d in the halfmained for
biochcm*cal testing. Any hterpretation of the resuhs must be made with these Eacts h mind.
The histological resuhs in the present study show that the muse model was not effective for
deteminhg optimal choice of giucocorticoid therapy. Previous studies have show the utility of this
model. Kischer et al. reportcd in 1989 that theh keloid implants showed histological similarity for 246
days after traiispiantation with no sigas of rejectioa They did, however, observe that keloid implants
10% more of their histologicai similarity over time than do hypertrophie scars.
Thc present study has found that athymic mice an still able to rnount a significant respoase to the
foreign keloid tissue, even though their total immune response is attenuated. The mice were still capable
of delivering numerous neurtophiles, macrophages (histiocytes) and plasma ce& to the foreign keloid
tissue. In sume samples, the original keloid was aimost completely destroyed by acute inflammation . granulation tissue, grandomatous foreign body reaction, or calcification (See Figures 22-26). Due to
the extensive reactions by the mice to the tissue in the present experiments, it was impossible to draw
any conclusions about the relative efficacy of the test glucocorticoids.
Hydroxyproline assays are usefùi markers of the rate of collagen synthesis. The levels of
hydroxyproiine were daermined for the keloid implant tissues. This amino acid is an integral structural
component of coiiagen. During translation, when Mividual coiiagen tibrils are king synthesid h m
messenger RNA, two-thirds of al the amino acids that maice up a complete collagen mlecule are
proline. Prolyl hydroxylase adds a hydroxyl group to the collagen chah duMg pst-translational
modification (Campbell, 1993). Collagen is the only manimaüan pmtem t h t contains significant
amounts of hydroxypmline. Therefore determination of hydroxyproiine can be used as a measufe of
collagen met8bolism (LeRoy, 1967). Using samples âom the s b ensures that dietary coiIagen wiil not
affect the resuhs (LeRoy, 1967).
Figure 31 shows the respective mean levels of hydroxyproline in the three keloid implants at tirne of
biopsy and at two weeks and at four weeks after king treated with triamcinolone, mthylprednisolone,
and dexamethasone.
The levels of hydroxyproliw m the biopsied tissue (O t b ) were found to be significantly different than
the two-week control values. The two week control values for hydroxyproline were also found to be
significantly dEerent fiom those O bserwd in the treatment group receiving dexamethasone. None of
the other treatment groups were found to be signincantly ditférent when compared to the control values
or to the levels of hydroxyproline found in the "zero" time samples. This lack of significance for the
other treatment groups and time periods could reflect a sample size which was not large enough to show
any statistical dinerences in hydroxyproline leveis after glucocorticoid treatment. It could also mean
that glucocorticoid treatment as employed here had no effect on the keloid tissue. Since there is a
volume of evidence that shows the effects of glucocorticoids on collagen turnover (Kauh et d , 1997,
McCoy et al., 1980) and confirms the clinical effects of glucocorticoids in resolving keloid scars
(Urioste et al., 1999), it would k reasonable to conclude that the sarnple size was too small.
Future studies rnight benefit fiom explorkg the use of animal models that not only have a diminished
immune response, such as athymic mice, but thet are also macrophage and kukocyte depleted. These
animais would be particularty sensitive to mfections and great caution would be required to prevent this.
It is desirable to create a murine model tbat bas a suitable microenvironment for the keloid scar. This
would enme that the scar was idependent of any of murine defence mechanisms or endogenous
biologicai products. The animai model with the least mterference h m host immune and wound-heaüng
mechanisms is probably the moa effective for studying keloid scars, but these deficiencies must be
taken mto account when interpreting resuhs because in humans it is these processes that are responsible
for the scar formation.
In a later paper, Shetlar et al. (1991) report that glycosaminoglycan levels remain at pre-implantation
levels for 80 days and, thus, conclude that this represents a window in which experirnental treatments
might prevail in the keloid tissue. However, the possibility exists that the immune response the athymic
mice were able to mount through monocytes, macrophages, neutrophils, and plasma ceUs could rnake
the study of any type of therapy uninterpretable despite the similar levels of ECM proteins in the implant
compared to a pre-irnplantat ion levels.
An interest h g pro blem that cornplicated interpretat ion of the histological resuhs was the cakincat ion of
many of the keloid tissue sections. A review of the Literat ure and personal communications with Dr. S.
Sakma, leads to the conclusion this is not known to hsppen in keloid Unplams in mice or in hunmuis
with keloid scan. Silbemiann has reported on glucocorticoid-induced enhancement and impairment of
mineralization of cartilige m mke (1 977 and 1978, respectively). It is possible that similar mec-
were at work in the keloid implant s. One of characteristic effects of cort icosteroids is l o s of bone mass
(Sc-, 19%). Perhaps the calcium was m o b i i towards the foreign keloià implant.
Glucocorticoids do exert eEects on the regulation of calcium homeostasis. Cakim uptake is d h p t e d
m the gut by unknown mchaaissns and there is incrrased excretion of calcium h m the kidney. Both of
these actions lead to decreased total stores of calcium and would m t be expected to cause d e d
calcification (Schimmer, 1996).
Several tissue sections bad extensive cakifkatioo. Some sections (See Figure 20) had more tban half of
the keloid tissue displaced by calcium de posit S. Generally , t here were granulomatous reactions around
the calcium deposits with maay muitinucleated giant cells (histiocytes). Since calcium seerns to act as
an attnictant for multinucleated giant ceiis, perhaps the mouse is experiencing a two-step process
resuhhg in the recniitment of histiocytes. If macrophages cannot be recruited mto the foreign matter by
any other rneans (vascularization or chernoattraction by cytokines) then it is possible that the calcium
deposits represent the oniy way that an Unmune response could be generated against the keloid tissue.
It has been observed by Kischer et al. (1989) that microvascuiar anastomosis occurs sometirne before 16
days post-implantation. Peripheral vascularization cm occur within 8 days of implantation. This rapid
vascularUation rnay help to explain the magnitude of the observed immune response.
Gluu~ronKoid Toxicity
A further problem with the nude mouse mode1 is that it is dif6cult to ensure that the injected
giucococticoid is actualiy king injected into the keloid tissw. Considering that many of the rnice (as
weli as the rats) showed signs of glucocorticoid toxicity (wasting, infections fkom decreased immune
mponse) it seems likely thai the inpcted stemid did escape fiom the keloiâ tissue and caused systemic
effects. This was, however, expected based on the human treatment. Patients have been reported to
sbow local tissue necrosis and the formation of telaageictasiae a r o d the injection site as a resuh of
injected steroiâ escaping fiom the keloid (Urioste et al., 1 999).
The rats and mke receivmg triamciroione were much more iikely to d e r from steroid toxicity, than
were the other two treatment groups. Loss of mass due to protein catabolism and loss of bone mass is a
baiimark of effects secondary to glucocorticoid treatment. Figure 32 shows that a significant loss of
body mass was observed when triamcinolone was administered to the mice. Other changes in rnass for
the different treatment groups were found to be insignificant.
Suppression of the immune system is another recognized effect secondary to glucocorticoid
. . adnmustration Tables 12, 13, and 14 show tbat many of the glucocorticoid-treated mice developed
sepsis. Berdicevsky and S i l b e m 1976, found that the rate of bacterial infection in rnice was
significantly higher than placebo or control groups when compared to the administration of
triamcinolone.
It was not anticipated that triamcinolone would be much worse with respect to its adverse effects than
the other two glucocorticoids. The doses were adjusted so that they were equal in anti-intlammatory
effect. Dexamethasone has a longer half-We in tissue than ttiamcinolom (Schimmer, 1996). The in
vitro half life of triamcinolone in liver homogenate fiorn athymic mice was found to be 2 1-34 minutes
compared with 1 3-68 minutes m human liver homogenates (Anderson et al., 1 982). This data wodd
mdicate that athymic mice should be able to metabolize triamcinolone at a frister rate than humans. I t
would sam that rodents react very poorly to the admmistra . . tion of triamcinolone for reasons that are not
Yet apparent-
in a pilot study performed by Waki et al. (1991), keloid tissue was implarited h o athyxnic mice for eight
weeks. The mice were then treated with a varkty of thempeutic agents inctudiag triamcinolone (0.05
ml, 40 mglmL every two weeks). Thcse mice eltpenenced an average weight gain of 1.7 g, whereas,
the other treatment groups were observed to have an average weight gain of 5.1 g (Control- no
treatment), 5.9 g (acetylcysteme, weekly intraiesional injections of 0.05 ml of a 20% solution), 5.3 g
(acetyic ysteine, daily intraperinoneal injections of O. 1 ml of a 20% solution), 6.6g (2 mg/ml
penicilliaminc in the mice's dniiking water), 6.40 (daily doses of colchicine, 0.005 mgll OOg of mouse
weight via intraperitoneal injection). In the study by Waki et al., mice treated with triamcinoIone died.
but kir death was not attniuted to steroid associated toxicity even though this seems a reasonable
pathogenic conclusion.
In an attempt to objectively quantfi the arnount of inflammation and scarring in a stained tissue section.
images of each slide were captured using a Sony CCD digital camera. Programs such as Signmiscan
(SPSS) can caliîrated to calculate the intensiiy of the stain and thus provide an arbitrary index of
inflanaation relative to some control. Unfominateiy, this rnethod proved impracticai because of the
sectioning and staining process. There was not any method to guarantee that the sections were taken
&om the same spatial location fkom anmial to animal, nor was it possible to control the amount of stain
that a particular section took up. Pathology remaias a discipline where a certain amount of human
intqmtation is stiil quired. The cornputer progranis, like Signiascan, are quite effective at
determiring the numbers of a particular cells, such as mast c e b or a leukocytes, but for an overall
daennination of the extent of SC- or idammation, the trained eye of a pathologist is still required.
The mechanisms, pathways, and key mediators in the pathogenesis of keloids stdl need to be elucidated
as a background to improved therapy. It is clear that TGF-p is a key contributor to the developrnent of
keloid scar tissue. It is, however, not clear by what mechanism TGF-B exerts its fibroproliferative
effects anâ why it is able to ovemhelm the inhibitory and degradative processes that are n o d y
responsible for remodelling a wound into mature scar tissue.
Except in the case of variceiia ernbyropathy, fetal tissue is known not to develop scar tissue after injury.
Researchers are begioning to study the mechanisms of this process. Comparative analyses are king
camed out to examine the dineremes between fetal and adult wound healing. If the questions of how
this is occwhg and why adults lose the ability to grow functional skin after an injury are answered,
then the problem of excess fibrosis might h d be sokd (Unoste et al.. 1999)
There is also reason to audy p53, a protein that has been cailed the "guardian of the genome". It is
associated with c e k that have undergone DNA damage and arrests these ceUs in Gi until DNA the
damage has been repaired. Mutated p53 has been Mplicated in approximately 50% of ail human
cancers. Mutated p53 may also be responsible for benign proliferative diseases, as well.
Saed, et al., 1998, found that p53 was mutated in seven of seven keloid tissue samples that were tested.
They postulate that the altered p53 predisposes fibmblast cek to hyperprolifemtion In another study by
Firestein et al., 1996, it was reported that mutations in p53 might have a causative role in the
developnmt of rheumatoid arthritis. They speculate that cells k g the joint becom activated and
begin to degrade the ECM. Further study of sinüat mutations and their roles Hi the formation of keloid
scars is needed.
124
The goal of this study was to determine whether dexametbasow or methylprednisolone were more or
less effective at reducing or preventing keloid scars than was triamcinoIone. The main rnarker of
efncacy for the present study was histological examination and scoring. In addition to the histology,
hydroxyproüne concent ratio w were detennined for the implanted keloid tissue. Due to confounding
variables present in the rat and keloid tissue, no definithe conclusions could bc made regarchg the
relative enicacies of the test glucocorticoids, with respect to one another. Unexpectedly, the
ghicocortiwids haâ little effect on the hydroxyproline levels
+ Use of the carrageenan-induced idammatory model to study keloids is imperfect
No dennite conclusions about efficacy of a particular drug can be made fiom the histology of the rat tissue
Keloids need to be studied directly to make definitive conclusions
+ Hydroxyproline concentrations + Significantly different at 2-week control samples vs. the biopsy values, indicating that coikgen
syntbesis continued d e r implantation 0 Significantly different for 2 week dexamethasone samples vs. 2 week control values, indicating
that only dexamethasone was able to d u c e the amount of collagen and only at the two week rnark.
4 The athymic mouse model has limitations 0 Immune respome to the foreign keloid tissue fiom the mouse hoa 4 Calcium deposits arising h m unknowu mechanisnis + Systemic effccts secondary to glucocortiwid treatment
+ Loss of- + Sepsis + Fatalities
+ Definitive conclusions fkom animai models are mt possible due to confounding variables + Ummticipated immune response in athymic mice + CoDtamination in operative site of rats with hair shafts + Urmnticipated calcium deposits + Unwanted fibrosis due to injections . . + Unwanted systemic effects fiom glucocort icoid administration
+ The best place to study clinicd solutions for keloid scars is iikely to be a ciinical setting
The fiiial conclusion of the present study is that the curent rnethods of studying cünical effects of keloid
therapy in an animal mode1 are unsatisnictory. This is particularly pertinent when triamcinolone is
utilized, because it has severe adverse effects associated with its administration (loss of body mass,
htalities releted to sepsis). With the developrnenî of mon sophisticated models, research studies (such
as the p m n t one) wül become more feasible and provide more definitive conclusions. However, until
such animal models are developed, the moa suitable way to test the efficacy of a keloid therapy is to
employ a cbca l trial with human subjects.
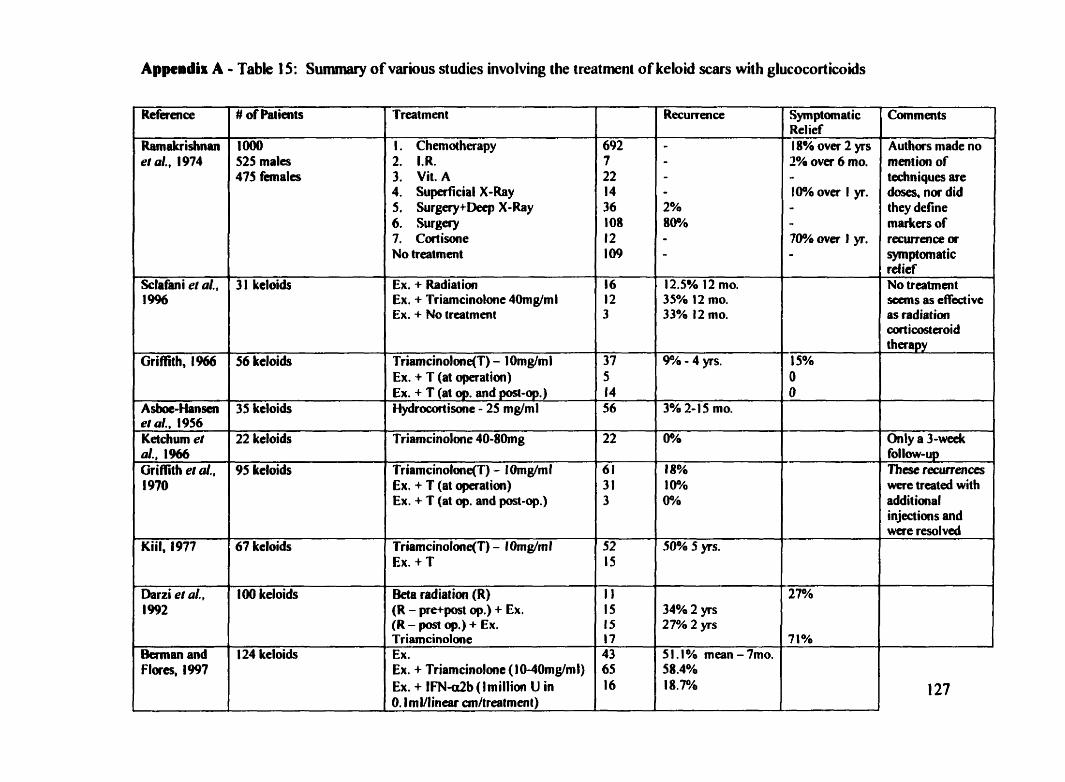
Appendis A - Table 15: Swnmary of various studies involving the treatment of keloid scars with glucocorticoids
Ramalrrishnan et al., 1974
Sclafani et al., 1 9%
Griffith, l%6
A stme-Nansen et al., 1956 Ketchum et al., 1966 Griffith el al., 1970
Darzi et al., 1 992
&man and Flores, 1997
# of Patients
Io00 525 males 475 fcmales
3 l keloids
56 keloids
35 kdoids
22 keloiâs
95 keloids
100 keloids
124 keloids
1. Chemotherapy 2. I.R. 3. Vit. A 4. Superficial X-Ray 5. Surgery+Deep X-Ray 6. Surgay 7. Cortisone No treatment
Ex. + Radiation Ex. + Triamcinolone 4Omg/ml Ex. -t No treatment
Ex. + T (at opefation) Ex, + T (at op. and post-op.) HydrOCOCfisone - 25 mglml
Triamcinolone 40-80mg
Triamcinolone(T) - 1 Orng/ml Ex. + T (at operatioci) Ex. + T (at op. and post-op.)
Triamcinolone(T) - IOmg/ml Ex. + T
Beîa radiation (R) (R - pre+post op.) + Ex. (R - p t op.) + Ex. ~ria&inolane Ex. Ex. + Triamcinolme (lMOmg/ml) Ex. + IFN-db (lmillim U in O. I rnl/linear crn/treatment)
12.5% 12 mo. 35% 12 mo. 33% 12 mo.
3% 2-15 mo.
Symptomatic Relief 18% over 2 yrs 2% over 6 mo, - 100h over I y. - - 76% over 1 y. -
Authors made no mention of techniques are doses, nor did they define markers of recwence or symptomatic ret ief No treatment
as radiation cort icostaoid therapy
Only a 3-week follow-up These fecurtences werc trcated with additional injections and were resolved
Appendix B
Informed Consent Form Keloid Scar Study
Background:
Keloid scars arise because the processes by which collagen is synthesized and degraded are altered to
mult in an overabundance of coüagen deposition. C o h e n is a structurai protein and is an integral
component of your sk in and comective tissue. Mer an injury to your skin, collagen plays a key role in
the formation of the scar. How these scars are formed is poorly understood and it is not yet known why
these scars form.
We are seeking permission to use your tissue in laboratory testmg. We are interested in how keloid tissue responds to dflerent dnigs with the hope of learning more about the biology of these scars, as weU as how they grow and mature.
The investigators are Dr. S.M. MacLeod, Dr. S. Salama, and A. Thorna of St. Joseph's Hospital.
If you agree to participate in this study, your keloid rar will be excised by a physician. Your participation in the study will not diect the procedure to remove your scar. The only difference wül occur after excision. Your tissue will be surgically Unplanted into a rnouse that lacks an immune system to prevent rejection of the implant.
The muse will then be treated with various corticosteroids to determine k i r effectiveness in shrlliking the keloid scar.
There will be no aidnffceb or r i s b amociated with the procedure.
AU of the cokted deta will be kept bcked m the laboratory and only accessible to the investigators who plan to publish the results without identifying any of the individuah who pariicipated. It is expected that thip research will k completed wahia 8 months. If you are interested, you m y feel fke to contact Dr. S.M. MacLeod at (905) 521-61 15 who wiii provide you with the resuits. The donation of your tissue not be comected to your mdical record m any way.
W e this study does not provide any specific bcmfits to you, we hope that the mfonnation h m this study wiü hclp us understand how keioid rrar tissue nsponds to Mirent dmgs and perhaps provide a new method of treatment in the fbture. 128
Your refusal to participate in this study will not afEect your fùtwe care at St. Joseph's hospital or affèct your rektionship with any of the investigators.
I have nad this consent fom and unâerstood its contents and have had the opportunity to ask questions of a member of the research team. 1 agree to assist with this research.
Signature of Patient
Signature of Witness Date
Signature of Investigator or Representative Date
If you have any questions or concerns about the study, you may contact Dr. S.M. MacLeod at (905) 521- 61 15.
Appendu C
Keloid Tissue Histology Scoring
+ Present - Absent
Scorer
SCOM~ Not Present - O Mild - 1 Matked - 2
I I Score I Acute Inflammation (PresentIAbsent)
l Grandat ion Tissue (PresenVAbsent )
Granulonïitous Foreign Body Reaction (Present/Absent)
Notes:
Appeadu D
Rat Tissue Histdogy Scoring
Scorer
Sample Code
Granulomatous Foreign Body Reaction (Present/Absent)
Granulation Tissue (PresentlAbsent)
Fibrous tissue (PresedAbsent)
Score
1 1s the dermis affected?
Notes:
Appeadix E
Figure 33: Necropsy Reports fiom the CAF
PATHO1.WY REPORT MclWSTER CMlVERSïrY CENTRAL AMMAL YAClLiTY
Appendix E - continued Figure 34: Necropsy report for an athymic mouse
faions rc aot ippumt in thc:
brnC2) N I m N
PATHOLOGY REPORT MCMASTER UNlVERSrrY CENTRAL ANtMAL FACiLITY
- -- . . - . - . -.
r r L i r N Y - N E. PUA I
c- ' - r rN O): Y *YIyrr:WIA -: NIA
R
Invd@œ. McIsod L
Mike fililbna
Crnpur m: Sr. Jmcph's
Enrnrk. 52141 15
RhQwi * SEPTlCEMIA. - A C V l E MEUMONITIS. - HEPAlUCELLUtAR DEGENEIUnON. - SPLENIC LYMPHOID AIROPHY. - PERIRENAL HEMORRHAGES. - RENAL C)JTERSTJTlAL EDEMA. - A T R O M OF EXOCRINE PANCUEAS.
N m duc: Jliiie 911 999
.bwircrnOUIl
IMI6
kr My 78199, 4-6 W.O.
9
alCAF99
Smti: 8dWNiidt
chdm M A
Wybt:
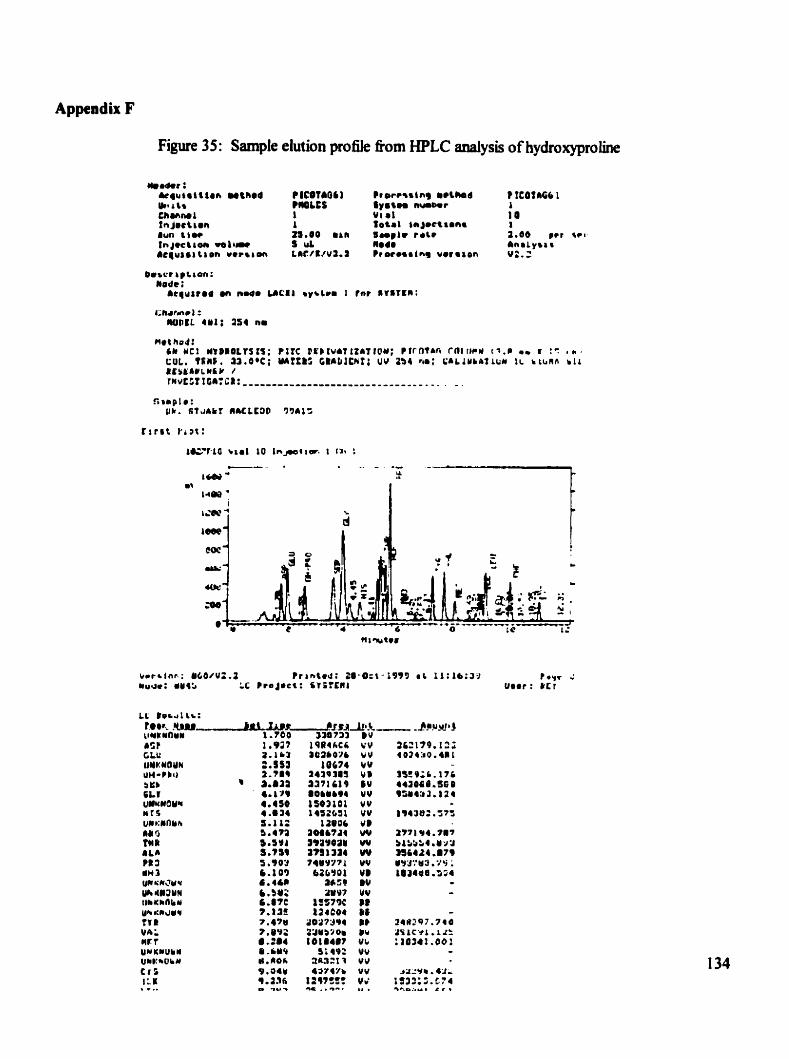
Appendix F
Figure 3 5 : Sample elut ion pro& &om HPLC analysis of hydroxyproline
as t C U UYKYQYN UH-Pb0 $Yb Q C t l umuouii wrs U I ~ Y h na 5 tn R a w ?1 3 iln3 yCi*'ujuu Urc l l3MN tlrwnlru Uh JUY TYR V A L mrt uurwuii* U*):*OIW Cr 5 1;a , ...
References
1. AMuatader, M., et al. 1983. Experimental Production of Keloids. Indian Journal of Cancer. 20: 27-3 1.
2. Abergel RP, Pissurro D, Meeker CA, et al. 1987. BiocheMcal composition of the connective tissue in keloids and analysis of collagen metaboüsm in keloid fibroblast cultures Journal of Investagative Dermutology. 88:727-736.
3. M y S.M. K Sivanantharajah. 1969. Keloids in various races: A review of 175 cases. PIastic and Reconstvuctive Surgery. 44: 564.
4. Al-Khawajah, Manvan M. 1996. Failure of Interferon-Alpha 2B In the Treatment of Mature Keloids. Intemational Jounui of Dermatology. JS:Sl5-Sl7.
5. Aster, Tina S. 1998. Review of Cutamous Lasers and Their Applications. Southern Medicul Journal. 91 : 806-8 14.
6. Andersson, Paul. Staffan Edsbacker, Ake Ryrfeldt, Christer von Bahr. 1982. In vitro biotransfonnat ion of glucocorticoids in üver and skm homogetiate fiact ion fiom man, rat, and hairless mouse. Journal of Steroid Biochernistry. 16:787-795.
7. Bettinger, David A. et al. 1 996. The effect of TGF-p on keloid fïbroblast pro Meration and collagen synthesis. Pfastic and Reconstructive Surgery. 98(5):827-833.
8. &mian, B. MR Dunkan. 1989. Short term keloid treatment in vivo with human interferon-aipha 2b. Resuhs in xlective and persisted mrmatUation of keloidd fibroblast coilagen glycosaminog lycan, and collagenase production in vitro. Jownal of the A merican Academy of Derma~oIogy. 2 1 :694-702.
9. Berman, Man. Francisco Fbrcs. 1998. The treatment of hypertrophie scars and keloids. Ewopean Journal of Denntatology . 8: 59 1-6.
10. Border, Wayne. A Erkki Ruoslahti. 1992. Transfomhg Growth Factor-P in Disease: The Dark Side of Tissue Repair. Journal of Clhical Imwtigation. 90: 1-7.
1 1. Boyadjiev, C. E. Popcbristova J. Mazgakva Histomorphologic 1995. Cbanges in Keloids Treated with Kenacort. The Journal of Trauma: Injury, Infection, and Critical Care. 38:299- 302.
12. Calnan, J.S. and H.J. Copenbagen.. l%7. Autotransplantation of Keioid m Man Brirish Journdof Surgery. S4:33030-3.
13. Co@ Keirnan I., and Bruce A* Mast. 1990. Models of Wound Healing. JoMMI of Trauma
1 4. Cosman B. G.F. Crikelair. D.M Ju. et al. 1 96 1 . The surgical treatment of keloids. Plastic and Recomîmctive Surgery. 44: 564
1 S. DaCosta, JC. Modem Surgery. Philadelphia. WB Saunders, 193 1.
1 6. Datubo-Brown, D.D. 1 990. Keloids: a review of the üterature. British Journal of Plasric Surgery. 43:70-77.
17. Dani, M. A. N. A. Chowdn. S.K. Kaul. M. Khan. 1992. Evaluation ofvarious methods of treating keloids and hypert~ophic scars: a 10 year folow-up study. British Journal of Plastic Surgery . 45:374-379.
18. De Leve L.D. M.$. Pa- P.R. Saxena. 1980. Redistribution of cardiac output during localized granulomatous inflammation and the effect of methysergide in anesthetized rats. Injc~rnmation. 4(4):359-69
19.EstremS. Impiantationofhumankeloidintoathymicmice. Laryngoscope. 1987. 97:1214-1218.
20. Gaspano, Francis. 1 998. Editorial: p5 3 in dermatology . Archives of Dermatology. 134: 102% 1032.
2 1. Glanze, Walter D. The Mosby Medical Encyclopedia. 1 992. Penguin Group. Toront0,Canada.
22. Granstein, Richard D. George F. Murphy. Randail J. Margolis. Michael H. Byrne. Edward P. Amento. 1987. Gamma-Interferon Inhibits Collagen S ynthesis In Vivo in the Mouse. Journal of ClinicaI Investigation. 79:1254-1258.
23. Granstein, Richard D. A Rook. TF Flotte, et ai. 1990. Controiied trial of intralesional recombinant interferon-y in the treatment of keloid s c h g . Archives of Dermatology. 126: 1295-302.
24. Hohan, S. 1982. Rsdiotherapy for keloids (letter). Annals of Plastic Surgery. 9:262.
25. Ignotz, IU, J. Massagw. 1986. Trdorming growth factor-g stimulates the expression of fibrone~fin and cohgen and theu incorporation into the extracelluiar mat& Jounrol of Biologicai Chemistry. 261 :4337-4345.
26. Ki& Jette. 1977 Kebids treated witb t o p a injections of triamcinolone acetonide (Kenalog): Imnediate and long term resuhs. S%an&navian Journai of Plastic Reconsîructive Surgery. 11: 169-172,
27. Kirsner, R o b S. William H. Eaglstein. 1993. The woud healing process. Dermatologie Clincs. 1 l(4):629-640
28. Kischer, Watd C., et al. 1989. Use of nude (athymic) rnice for the study of hypertrophic scars and keloids: Vascular continuity between mouse and miplant. Anatomical Record. 225: 189-196.
29. Kischer, C. W. and G.S. Brody. 1981. Structure of the coiiagen nodule tiom hypertrophic scars and keloids. Sconning EIectron Microscopy. part 3,371.
30. Kischer, Ward C., et al. 1989. Implants of hypertiophic scars and keloids into the nude (athyrnic) mouse: Viability and morphology. Journal of Trauma. 29(5):672-677.
3 1 . Koch, James et 01. 1997. Sem-fiee keloid fibroblast ceU cuhure: An in vitro mode1 for the study of aberrant wound healing. Plastic und Reconstrtrctive Surgery. 99(4): 1094- 1098.
32. Kubota, Y, K. Fujiwara, 1. Ogata, Y. Hori, H. Oka 1985. Collagen prolyl hydroxlyase inhibitor and reduced coilagen formation in Cotton pellet-induced granuloma and skin wound heaiing in rats. British JournuI of Dermatology. 1 13: 559-563.
33. Larrabee WF Jr. CA East. HS Jaffie. C Stephenson. KE Peterson. 1 990. Intralesional interferron gamma treatment for keloids and hypertro phic scars. Archives of Otoluryngology und Head and Neck Surgery. 116: 1159-62.
34. LeRoy, E. Carnile. The technique and signüicance of hydroxyproline rneasuement in man. In: Advances in Clinical Chernistry, V. 10. 1967. pp. 2 1 3-253.
35. Low Savina, Q. Ronald L. Moy. Scar Wars Strategies: Target Collagen. 1992. JoumaI of Dematological Surgery and Oncology. 18: 98 1-986
36. Mayou, Brian J. 1981. D-PenicillamM in the treatmnt of keloids. British Journal of Dennatology. 105:87-89.
38. Murray, John C. 1 994. Keloids and hypertrophic scars. Clinics in Dematology. 12:27-37
39. Murray, John Ce 1993. Scars and keloids. Dennotologic CIinics. 11 (4):697-708.
40. Mutsaers, Steven E. Ji E. Bisbop. Gus McGrouthst. Geoffery J. Laurent. 1997. Mechanisms of Tissue Repair: fiom Wound Healing to Fihosis. International Journal of Biochemistry and Cell Biology. 29:S-l7.
41. Nemeth, Albert J. 1993. Keloids and hypertrophic SC=. J o d of DermatoIogic Surgerycmd ûncology. 19:738-746. .
42. Oluwasanrni, J.O. 1 979. In Plastic Surgery in the Tropics. London and Basingstoke: The MacMillan Press Ltd.
43. Peltonen J., Hsiao U, Jaakkola S, Sollberg S, et al. 199 1 Activation of coUagen gene expression in keloids: CO-localization of type 1 and VI collagen and transforxning growth factor- Beta 1 mRNA. Journal of Investugational Dermatology. 97:240-8.
44. Roberts A.B. U.I. Heine. KC. Fianders. M.B. Spom. 1990. Transforming growth faftor-p. Major role in reguiation of extracellular matrix. A d of the New York Academy of Sciences. !580:225-232
45. Roberts A.B. M.B. Spom. 1993. Physiological actions and clinical applications of transforming growth factor-beta (TGF-P). Growth Factors. 8: 1-9.
46. Saed, Ghassan M. Daniel Ladin. J e d e r Olson. Xuefei Han. Zizheng Hou. David Fivenson. 1 998. Analysis of p53 gene mutations in keloids using polymerase chah reaction - based sing le-strand conformat ional po lymorphisms and DN A sequencing . Archives in Dermatology. 134:963-967.
47. Schirnmer, Bernard P. and Keith L. Parker. Chapter 59: Adrenocorticotropic Homne: Adrenocorticol Steroids and Their Synthetic Analogs; Inhibitors of the Synthesis and Actions of Adrenocortical Hormones. In Goodmn and Gillman. gh Edition. Edited by Joel G. Hardman, Lee E. Limbird, Perry B. Moiho& Raymond W. Ruddon. 1996. McGraw-HU. New York, New York.
48. Shah, Mamta. David M. Foreman Mark W.J. Ferguson. 1995. Neutraiization of TGF-P 1 and TGF-P2 or exongenous addition of TGF-P3 to cutaneous rat wounds reduces scarring . Journal of Cell Science. 108:98S-1002.
49. Shah, Marnta David M. Foreman. Mark W.J. Ferguson. 1992. Control of Scarring in Adult Wounds by Neutralising Antibody to Traasfomillig Growth P. Lancer. 339:213- 14.
50. Sheltar M, Shehar L, Kischer C. 1985. The use of athymic mice for the study of hwnan keloids. hoceedings of the Society For Experimentul Biology and Medicine. 179:549- 552.
51. Sheltar, M.R et al. 1990. Implants of keloid and hypertrophie scars mto the athymic nude muse: Changes m the glywsamiaoglycsna of the implants. Connective Tissue Reseurch. 26:23-36.
52. Shetlsr MR. Shalar DL Bloom RF. Shetlar CL. Margoiin SB. 1998. Involution of keloid implants in aihymic mice treated with pgfenidone or with triemciaolone. Joumuf of Laboratoty & Clinical Medicine. UZ(6): 49 1-6.
53. Silbe- M. T. Kedar. P. Kovat. 1977. Triamcinobne-induccd wasting disease in Y O W mke. Acta A nutomy. 97: 180-190.
138
54. Silbennann, Michael. Gila Maor. 1978. Mechanisms of glucocorticoid-induced growth retardation: Impairment of cartiiige mineralization. Acta Anatomy. 10 1 : 140-1 49.
55. Silbert11811~1, Michael. Zivia Toister. Dim Leuinson. 1977. Corticosteroid-induced enbaDced minerabation in neonatyl condylar cartiüge. Clinical &thopedic and Related Research. 129:293-298.
56. Sproat, Janet E. Arianna Dalcin. Nancy Weitauer. Robin S. Roberts. 1992. Hypertrophic Sternal Scars: Silicone Gel S&et versus Kenaiog Injection Treatment. Piastic and Rrcunstruc~iw Surgery. 90:988-992
57. Suzawa, Haruo. Kiyoshi Ichikaea, Shinji Kikuc hi, et al. 1 992. Folio P hurmacol. japon. Effect of transilast, an anti-akrgic h g , on canageenan-induced granulation and capillary permeability in rats. 99:241-246.
58. Suzawa, Hanio. Kiyoshi Ichikaea, Shinji Kikuchi, et al. 1 992. Folia Pharmacol. jupon. Effect of transiiast, an anti-dergic h g , on the human keloid tissues. 99:23l-239.
59. Treâget EE. 1994. The mokcular biology offibroproliferative disorders ofthe skin: Potential cytokine therapeutics. Annals of Plastic Surgery. 33: 152454.
60. Tredget EE, et ai. 1 997. Hypertrophic scars, keloids, and contractures. Surgical CIinics of North America. 77(3):701-730.
61. Urioae, Sandy S. Keweth A. Arndt. JeBey S. Dover. 1999. Keloids and hypertrophie scars; Review and treatrnent strategies. Seminars in Cutaneous Medicine and Surgery, 18(2): 159- 171.
62. Younai, Soheil. 1996. Role of growth factors in scar contraction: An in vitro analysis. Annals of Plastic Surgery. 35(5) : 495-50 1.





























