Embed Size (px)
Citation preview

Adisai Buakhamsri, MD Thammasat University Hospital
On-behalf of the writing committee of The 2018 Thai Guideline For Management of Heart Failure
Highlights of 2018 Thai Guidelines For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG20184
1. Taworn Suithichaiyakul, MD President of The Heart Association of Thailand2. Prasart Laothavorn, MD Advisory 3. Kriengkrai Hengrussamee, MD Advisory 4. Rungroj Krittayaphong, MD Chairman 5. Teerapat Yingchoncharoen, MD Secretary and Council Committee6. Smonporn Boonyarattavej, MD Council Committee 7. Rapeephon Kunjara Na Ayudhya, MD Council Committee 8. Sarinya Puwanant, MD Council Committee9. Aekarach Ariyachaipanich, MD Council Committee10. Kasem Rattanasumawong, MD Council Committee11. Rungsrit Kanjanavanich, MD Council Committee12. Arintaya Phrominthikul, MD Council Committee13. Adisai Buakhamsri, MD Council Committee14. Sopon Sanguanwong, MD Council Committee15. Thoranis Chantrarat, MD Council Committee 16. Pornwalee Porapakkham, MD Council Committee17. Satit Janwanishstaporn, MD Council Committee 18. Srisakul Chirakarnjanakorn, MD Council Committee 19. Pranya Sakiyalak, MD Council Committee20. Pat Ongcharit, MD Council Committee21. Norasak Suvachittanont, MD Council Committee
Committee for Renew Guideline HFCT 2018Writing committee of the new guidelines

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG20182
Table of Contents
Topics Slide Numbers
I: Guideline development 3
II: Introduction and guideline Implementation 7
III: Definition, diagnosis and evaluation of heart failure 16
IV: Pharmacological treatment of chronic heart failure 27
V: Acute heart failure 51
VI: Common comorbidities in heart failure 66
VII: Sudden cardiac death and device therapy in heart failure 82
VIII: End-stage heart failure 89
Sections of the new guidelines
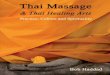
Class of recommendation Representative phrases/words COR
Evidence and/or general agreement: given treatment/procedure is beneficial, useful, effective
Recommended or indicated I
Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the given treatment or procedure: weight of evidence/opinion is in favor of its usefulness/efficacy
Should be considered IIa
Conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of the given treatment or procedure: usefulness/efficacy is less well established by evidence/opinion
May be considered IIb
Evidence and/or general agreement: given treatment or procedure is not useful/effective, and in some cases may be harmful
Not recommended III
The 2018 Thai Guideline For Management of Heart Failure

Level of evidence LOE
Data derived from multiple randomized clinical trials or metanalysis A
Data derived from a single randomized clinical trial or a large non-randomized studies
B
Consensus of opinion of the expert and/or small studies. Retrospective studies, registries
C
The 2018 Thai Guideline For Management of Heart Failure

Stages of HF and definition NYHA functional classification Symptom of HF
A At high risk for HF but without structural heart disease or symptoms of HF -
AbsentB Structural heart disease but without signs or symptoms of HF I No limitation of physical activity. Ordinary physical
activity does not cause symptoms of HF
CStructural heart disease
with prior or current symptoms of HF
I No limitation of physical activity. Ordinary physical activity does not cause symptoms of HF
IISlight limitation of physical activity.
Comfortable at rest, but ordinary physical activity results in symptoms of HF
PresentIII
Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity
results in symptoms of HF
IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest
D Refractory HF requiring specialized interventions IV Unable to carry on any physical activity without
symptoms of HF,or symptoms of HF at restThe 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
ACE inhibitors are recommended in all patients with asymptomatic LV systolic dysfunction regardless of etiology, in order to prevent or delay the onset of symptomatic HF unless contraindicated.
I A
ACE inhibitors are recommended in all patients with HFrEF and current or prior HF symptoms to reduce HF hospitalization and mortality.
I A
ACE inhibitors
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
ACE inhibitors should be initiated in clinically stable patients at a low dose and gradually uptitrated to the maximum tolerated dose.
I A
ACE inhibitors
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
ARBs are recommended in all patients with HFrEF with current or prior HF symptoms who are intolerant to ACE inhibitors, unless contraindicated, to reduce morbidity and mortality. Patients should also receive a beta-blocker and an MRA
I A
ARBs should be initiated in clinically stable patients at a low dose and gradually uptitrated to the maximum tolerated dose
I A
ARBs
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
ARBs are reasonable to reduce morbidity and mortality as alternative to ACE Inhibitors as first-line therapy for patients with HFrEF, especially for patients already taking ARBs for other indications,unless contraindicated
IIa A
Routine combined use of ACEI, ARB and MRA is harmful for patients with HFrEF.
III C
ARBs
The 2018 Thai Guideline For Management of Heart Failure
Recommendations COR LOE
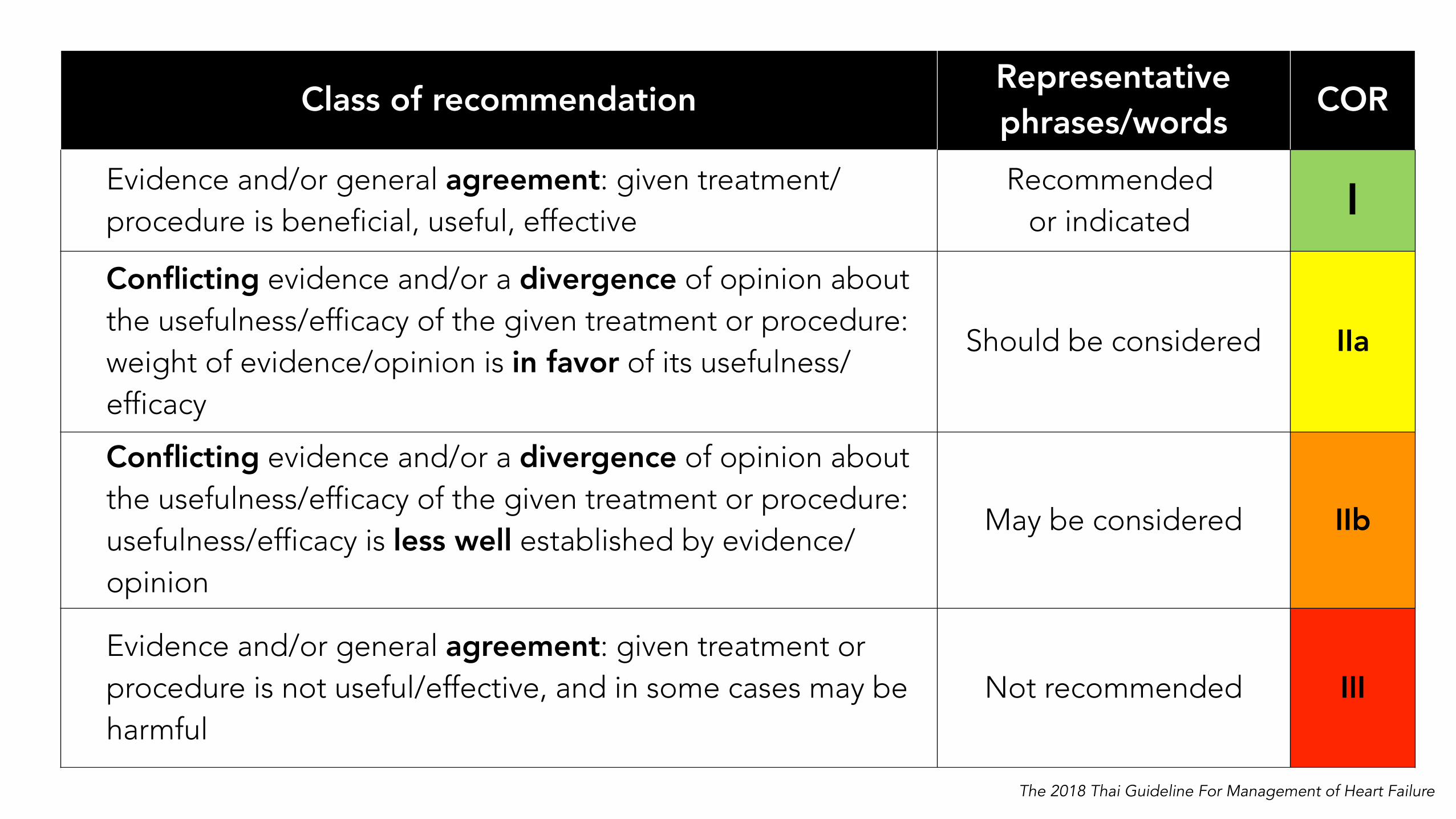
Beta-blockers are recommended in all patients with asymptomatic LV systolic dysfunction and a history of myocardial infarction in order to prevent or delay the onset of symptomatic HF and reduce mortality.
I B
Beta-blockers are recommended in all patients with asymptomatic LV systolic dysfunction, even they do not have a history of myocardial infarction, in order to prevent or delay the onset of symptomatic HF.
I C
Beta-blockers
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
A beta-blocker (bisoprolol, carvedilol, sustained-release metoprolol succinate and nebivolol ) is recommended, in addition to an ACEI, for all stable patients with current or prior symptoms of HFrEF to reduce the risk of HF hospitalization and death.
I A
Beta-blockers should be initiated in clinically stable patients at a low dose and gradually uptitrated to the maximum tolerated dose.
I A
Beta-blockers
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
Low-dose MRA ( spironolactone ) is recommended in symptomatic chronic HFrEF patients, unless contraindicated, preferably after treatment with ACE-I/ARB and BB, to further reduce HF hospitalization and mortality
I A
Routine combined use of ACEI, ARB and MRA is harmful for patient with HFREF
I A
MRA
The 2018 Thai Guideline For Management of Heart Failure

Drugs Drugs Initial dose (mg)
Target dose (mg)
Mean dose achieved in clinical trials
ACE inhibitors
Captopril 6.35 mg 3 times 50 mg 3 times 122.7 mg/d
Enalapril 2.5 mg twice 10-20 mg twice 16.6 mg/d
Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35 mg/d
Perindopril 2 mg once 8 to16 mg once n/a
Quinapril 5 mg twice 20 mg twice n/a
Ramipril 1.25 to 2.5 mg once 10 mg once n/a
ARBs
Candesartan 4 to 8 mg once 32 mg once 24 mg/d
Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d
Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d
Beta-blockers
Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d
Carvedilol 3.125 mg twice 25 mg twice 37 mg/d
Metorpolol succinate extended release
12.5 to 25 mg once 200 mg once 159 mg/d
Nebivolol 1.5 mg once 10 mg once 7.7 mg/dThe 2018 Thai Guideline For Management of Heart Failure

Drugs Drugs Initial dose (mg)
Target dose (mg)
Mean dose achieved in clinical trials
ACE inhibitors
Captopril 6.35 mg 3 times 50 mg 3 times 122.7 mg/d
Enalapril 2.5 mg twice 10-20 mg twice 16.6 mg/d
Lisinopril 2.5 to 5 mg once 20 to 40 mg once 32.5 to 35 mg/d
Perindopril 2 mg once 8 to16 mg once n/a
Quinapril 5 mg twice 20 mg twice n/a
Ramipril 1.25 to 2.5 mg once 10 mg once n/a
ARBs
Candesartan 4 to 8 mg once 32 mg once 24 mg/d
Losartan 25 to 50 mg once 50 to 150 mg once 129 mg/d
Valsartan 20 to 40 mg twice 160 mg twice 254 mg/d
Beta-blockers
Bisoprolol 1.25 mg once 10 mg once 8.6 mg/d
Carvedilol 3.125 mg twice 25 mg twice 37 mg/d
Metorpolol succinate extended release
12.5 to 25 mg once 200 mg once 159 mg/d
Nebivolol 1.5 mg once 10 mg once 7.7 mg/dThe 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure
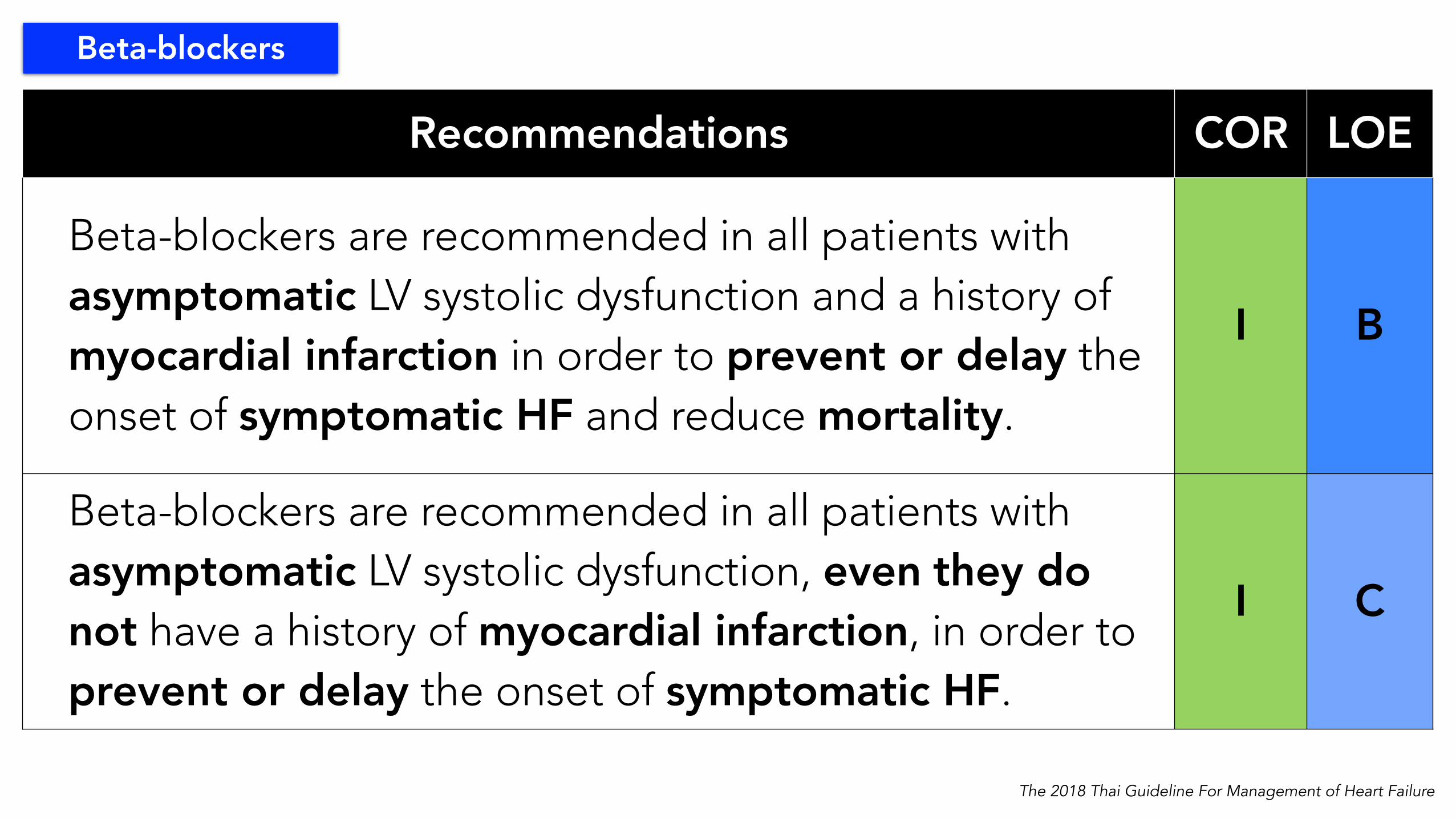
Recommendations COR LOE
Replacement of ACEI (or ARB) with ARNI (Sacubitril/valsartan) is recommended to further reduce the risk of HF hospitalization and mortality in patients with HFrEF who remain symptomatic despite optimal medical treatment with an ACEI (or ARB), a beta-blocker and an MRA.
I B
ARNI
The 2018 Thai Guideline For Management of Heart Failure
Recommendations COR LOE
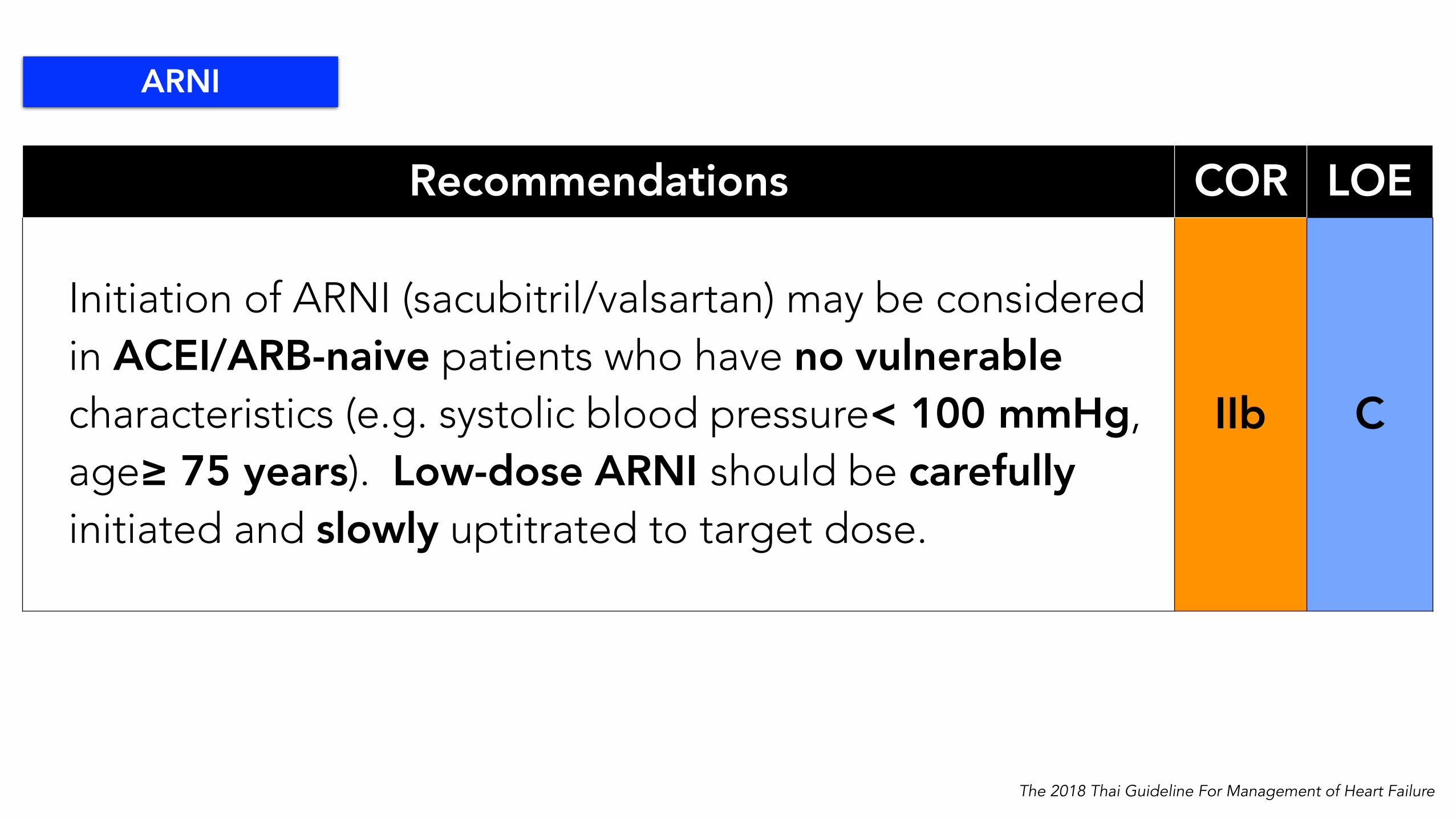
Initiation of ARNI (sacubitril/valsartan) may be considered in ACEI/ARB-naive patients who have no vulnerable characteristics (e.g. systolic blood pressure< 100 mmHg, age≥ 75 years). Low-dose ARNI should be carefully initiated and slowly uptitrated to target dose.
IIb C
ARNI
The 2018 Thai Guideline For Management of Heart Failure

• Avoid using ARNI in patients who has — hypotension (SBP < 90 mmHg)— eGFR <30 mL/min/1.73m2 — serum K+ > 5.2 mmol/L — history of angioedema — pregnancy
• ARNI must not be used concomitantly with an ACEI
• When switching from ACE-I to ARNI, stop ACE-I for at least 36 hours before starting ARNI, while no wash-out period is required when switching from ARB to ARNI
ARNI Precautions
The 2018 Thai Guideline For Management of Heart Failure
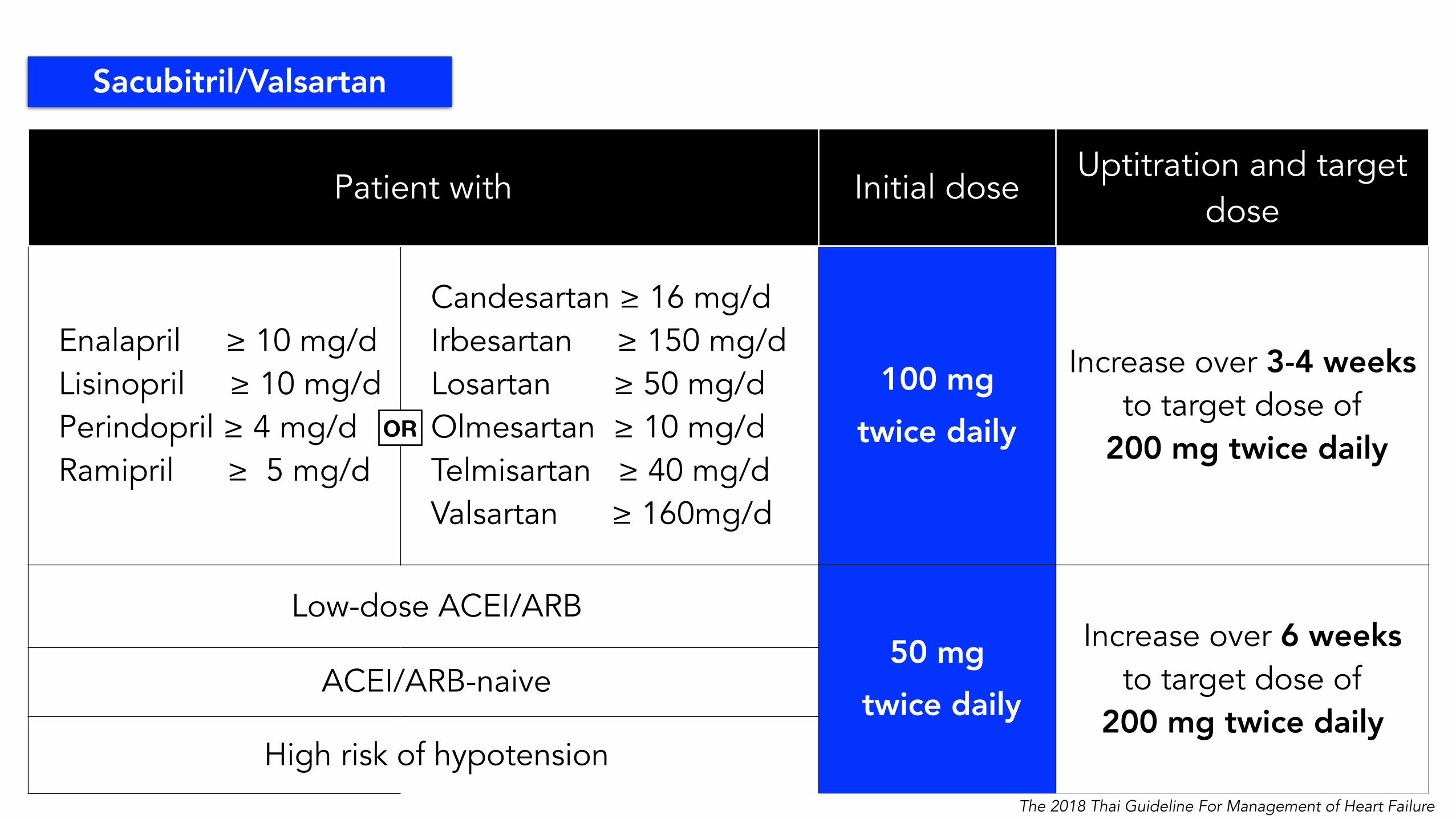
Patient with Initial doseUptitration and target
dose
Enalapril ≥ 10 mg/d Lisinopril ≥ 10 mg/d Perindopril ≥ 4 mg/d Ramipril ≥ 5 mg/d
Candesartan ≥ 16 mg/d Irbesartan ≥ 150 mg/d Losartan ≥ 50 mg/d Olmesartan ≥ 10 mg/d Telmisartan ≥ 40 mg/d Valsartan ≥ 160mg/d
100 mg twice daily
Increase over 3-4 weeks to target dose of
200 mg twice daily
Low-dose ACEI/ARB50 mg
twice daily
Increase over 6 weeks to target dose of
200 mg twice daily ACEI/ARB-naive
High risk of hypotension
OR
Sacubitril/Valsartan
The 2018 Thai Guideline For Management of Heart Failure
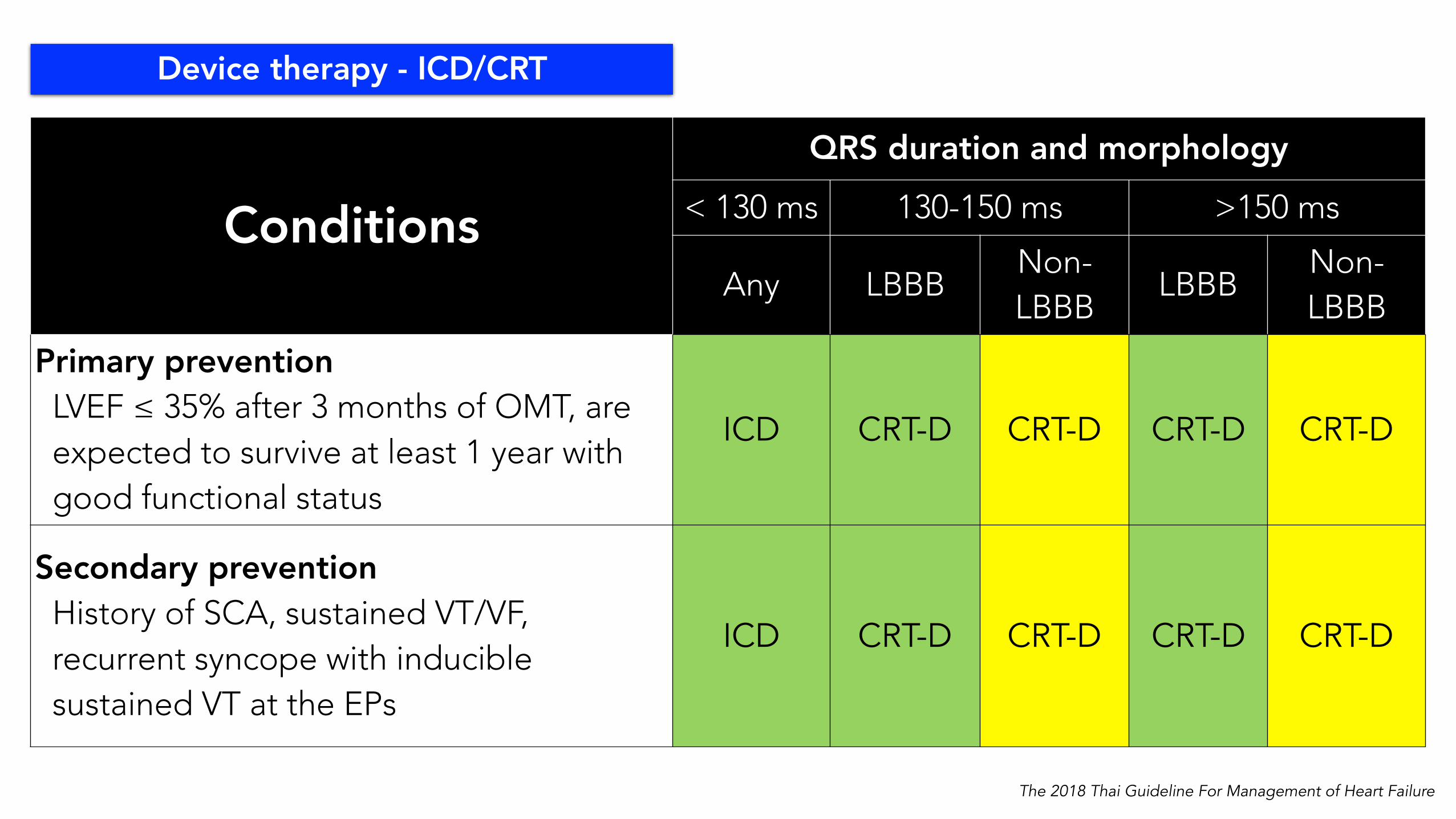
ConditionsQRS duration and morphology
< 130 ms 130-150 ms >150 ms
Any LBBBNon-LBBB
LBBBNon-LBBB
Primary prevention LVEF ≤ 35% after 3 months of OMT, are expected to survive at least 1 year with good functional status
ICD CRT-D CRT-D CRT-D CRT-D
Secondary prevention History of SCA, sustained VT/VF, recurrent syncope with inducible sustained VT at the EPs
ICD CRT-D CRT-D CRT-D CRT-D
Device therapy - ICD/CRT
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
Initiation of ivabradine should be considered to reduce the risk of HF hospitalization or cardiovascular death in symptomatic patients with LVEF ≤ 35%, in sinus rhythm and a resting heart rate ≥70 bpm despite optimal medical treatment, including maximum tolerated dose of beta-blocker, ACE Inhibitor (or ARB), and an MRA
IIa B
Ivabradine
Ivabradine should not be routinely used in patients with atrial fibrillation
The 2018 Thai Guideline For Management of Heart Failure
Recommendations COR LOE
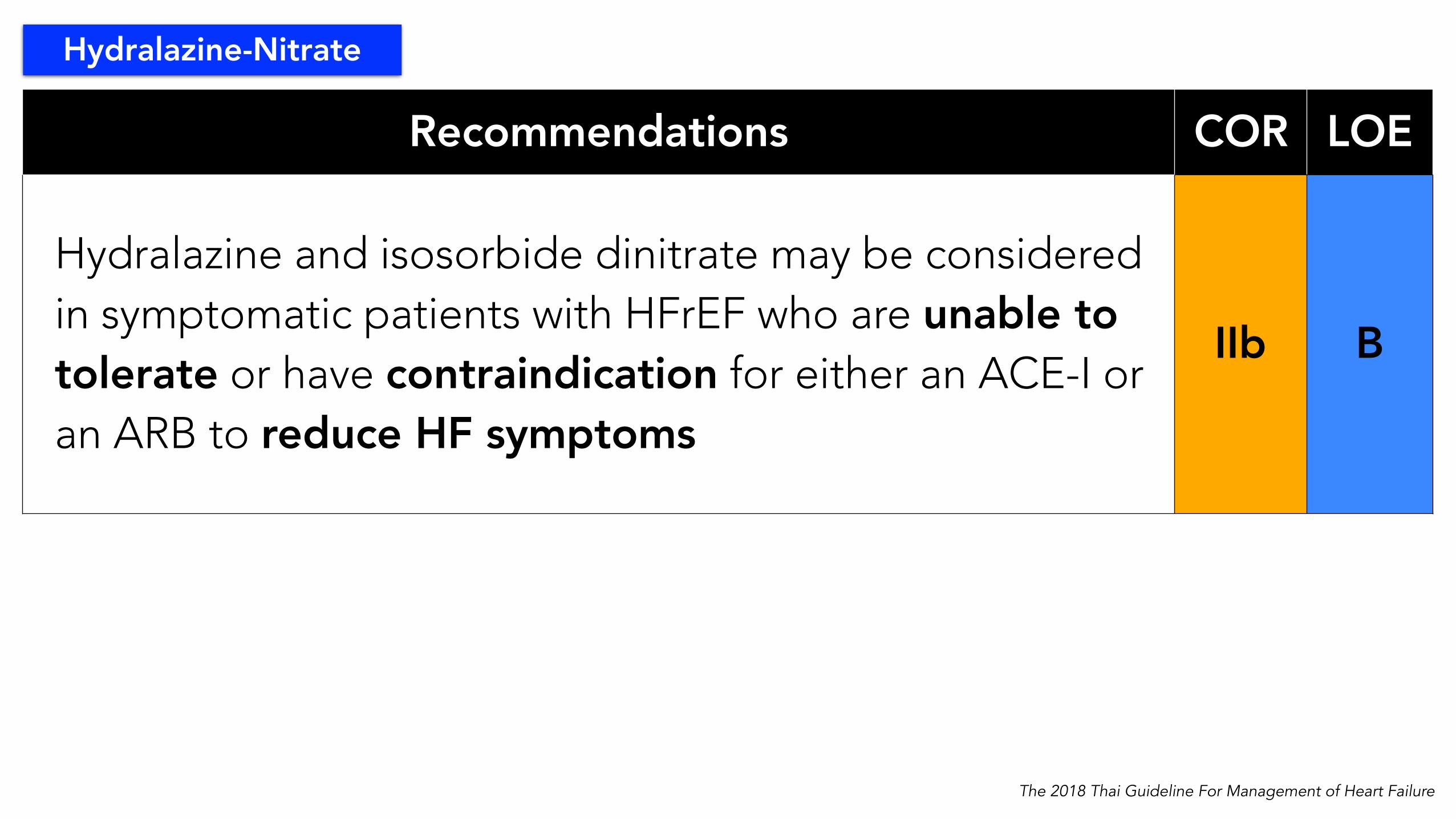
Hydralazine and isosorbide dinitrate may be considered in symptomatic patients with HFrEF who are unable to tolerate or have contraindication for either an ACE-I or an ARB to reduce HF symptoms
IIb B
Hydralazine-Nitrate
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
Recommendations COR LOEOptimal treatment of patients with hypertension with HFpEF is recommended in accordance with published clinical practice guidelines with a target systolic BP < 130 mmHg
I B
Diuretics are recommended in HFpEF patients who have evidence of volume overload to improve symptoms and reduce hospitalization. Care must be taken (in diuretics use) to avoid over-diuresis
I C
Cardiovascular and noncardiovascular comorbidities should be actively screened and optimally treated in all patients with HFpEF
I C
Concomitant coronary artery disease should be screened as a possible cause of exertional dyspnea and/or acute decompensation in HFpEF patients
IIa C
The 2018 Thai Guideline For Management of Heart Failure

Sleep disorder
Hypertension
AFDiabetes
Other; Depression
CKD PH etc.
Iron deficiency
& Anemia
Comorbidity
The 2018 Thai Guideline For Management of Heart Failure

Iron deficiency
& Anemia
Recommendations COR LOE
Assessment of anemia and iron deficiency should be performed in heart failure patients who remain symptomatic after optimizing guideline-directed medical therapy
IIa B
Intravenous iron should be considered to improve functional status and quality of life in symptomatic heart failure patients with NYHA functional class II and III and iron deficiency (serum ferritin <100 ng/mL, or serum ferritin 100-299 ng/mL and transferrin saturation <20%)
IIa B
Routine use of erythropoietin-stimulating agents to improve functional status and quality of life in heart failure patients with anemia is not recommended
III A
The 2018 Thai Guideline For Management of Heart Failure

Diabetes
Recommendations COR LOE
Metformin should be used as a first-line therapy in heart failure patients with diabetes, unless contraindicated
IIa C
SGLT-2 inhibitors should be considered in CVD patients with diabetes type 2 to reduce heart failure hospitalization
IIa B
Thiazolidinediones are not recommended in patients with heart failure because of an increased risk of worsening of heart failure and hospitalization
III A
The 2018 Thai Guideline For Management of Heart Failure
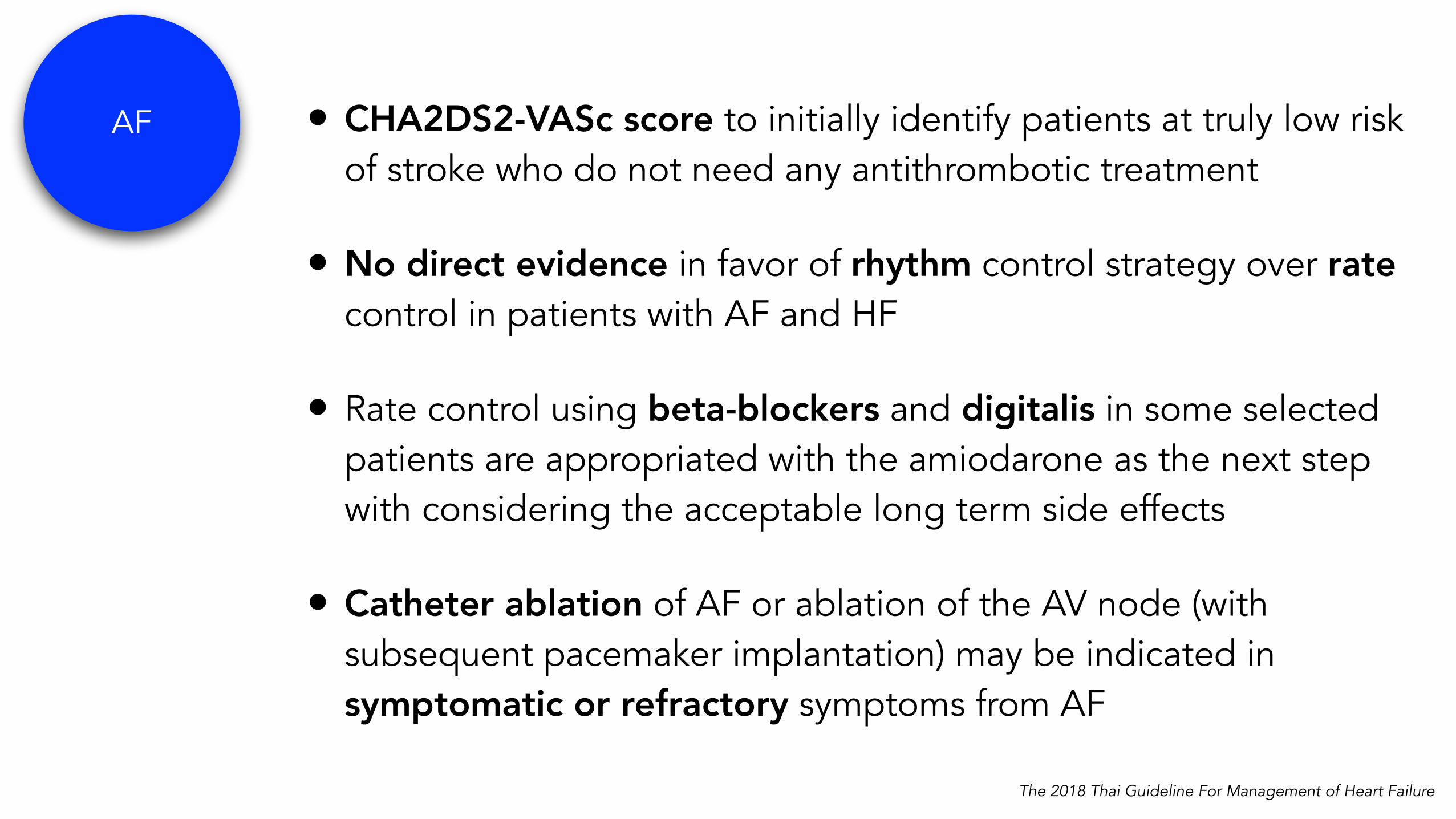
AF • CHA2DS2-VASc score to initially identify patients at truly low risk of stroke who do not need any antithrombotic treatment
• No direct evidence in favor of rhythm control strategy over rate control in patients with AF and HF
• Rate control using beta-blockers and digitalis in some selected patients are appropriated with the amiodarone as the next step with considering the acceptable long term side effects
• Catheter ablation of AF or ablation of the AV node (with subsequent pacemaker implantation) may be indicated in symptomatic or refractory symptoms from AF
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG2018
79
Comorbidities- Atrial fibrillation: Management
Patient with HF and AFPatient with HF and AF
Acute AFand acute HF
Acute AFand acute HF
Electrical cardioversionElectrical cardioversion
Significant heart failureUnstable v/s
Ongoing ischemia
anticoagulationanticoagulation
HR control < 110 bpmHR control < 110 bpm
Fluid balanceFluid balance
Mild HF
Pharmacologic cardioversion
Pharmacologic cardioversion
anticoagulationanticoagulation
Chronic AFand chronic HF
Chronic AFand chronic HF
EF ≥ 40digoxindigoxin
Diltiazem, verapamilDiltiazem, verapamil
diltiazemdiltiazem
betablockersbetablockers
digoxindigoxin
amiodaroneamiodarone
Atrioventricular node ablationAtrioventricular node ablation
amiodaroneamiodarone
Catheter ablationCatheter ablation
Rate control Rhythm control
EF < 40
unsuccess
Stroke prevention*Stroke prevention*
* See table
The 2018 Thai Guideline For Management of Heart Failure
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201880
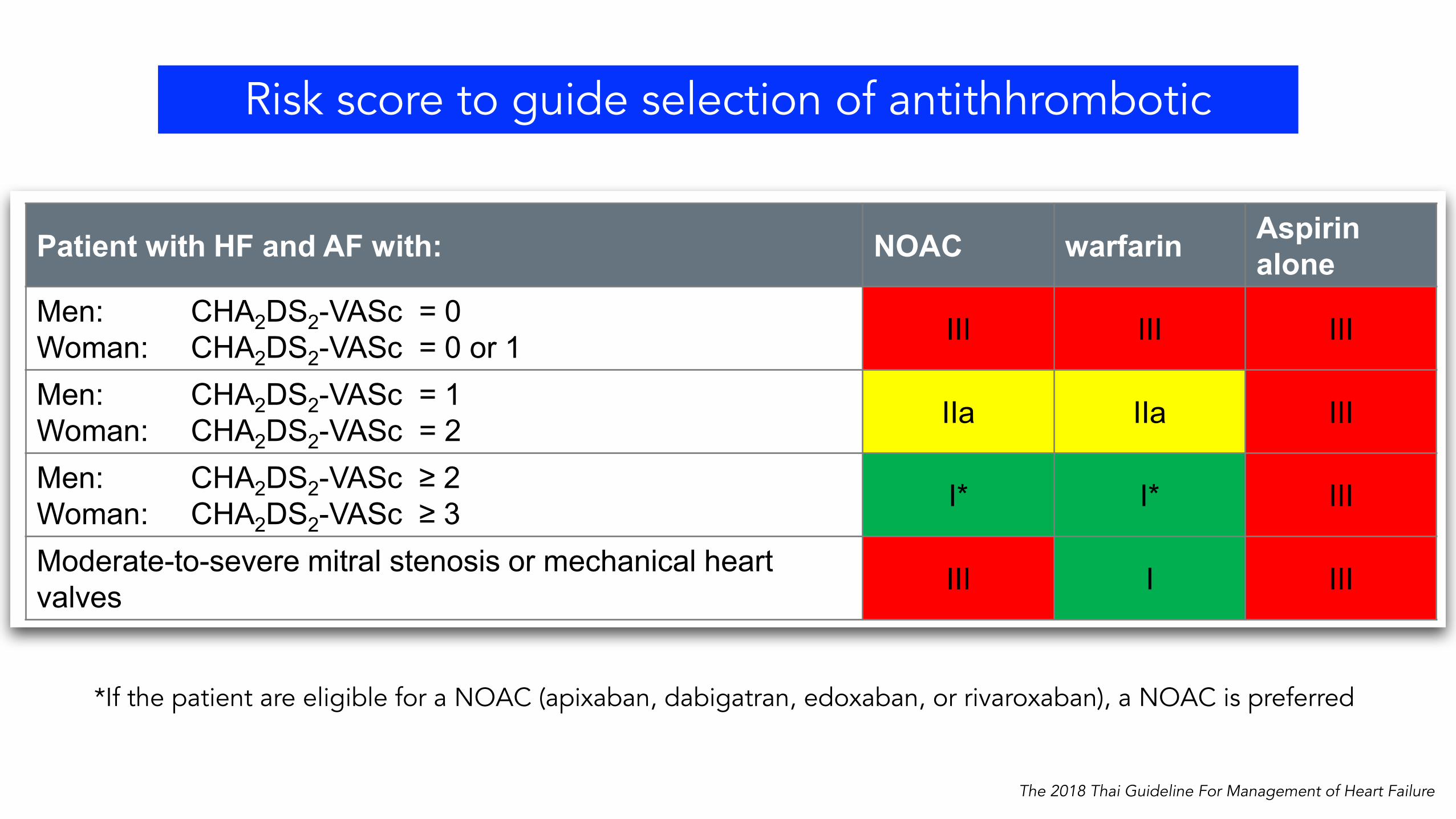
Patient with HF and AF with: NOAC warfarin Aspirin alone
Men: CHA2DS2-VASc = 0Woman: CHA2DS2-VASc = 0 or 1 III III III
Men: CHA2DS2-VASc = 1Woman: CHA2DS2-VASc = 2 IIa IIa III
Men: CHA2DS2-VASc ≥ 2Woman: CHA2DS2-VASc ≥ 3 I* I* III
Moderate-to-severe mitral stenosis or mechanical heart valves III I III
Comorbidities- Atrial fibrillation: Stroke Prevention in AF with HF
When oral anticoagulation is initiated, if the patient are eligible for a NOAC (apixaban, dabigatran, edoxaban, or rivaroxaban), a NOAC is preferred. If the patients are treated with a vitamin K antagonist, time in therapeutic range (TTR) should be kept as high as possible and closely monitored.
*If the patient are eligible for a NOAC (apixaban, dabigatran, edoxaban, or rivaroxaban), a NOAC is preferred
The 2018 Thai Guideline For Management of Heart Failure
Risk score to guide selection of antithhrombotic

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
Recommendations COR LOE
ARBs may be considered to decrease hospitalizations in HFpEF patients
IIb B
Low-dose MRA may be considered to decrease hospitalizations in HFpEF patients with elevated natriuretic peptides or history of recent HF hospitalization
IIb B
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
Annual influenza vaccine are recommended in all patients with HF I B
Combined pneumococcal vaccine and influenza vaccine are recommended in all patients with HF IIa B
Vaccination
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
Routine use of coenzyme Q10 is not recommended in patients with HFrEF due to insufficient data III B
Routine use of nitrates to improve functional capacity in HFpEF patients is not recommended
III B
Routine use of phosphodiesterase-5 inhibitors to improve symptoms in HFpEF is not recommended
III B
Other medications
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

\
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
Recommendations COR LOE
Management of patients with cardiogenic shock or respiratory failure in intensive care unit is recommended
I C
Identification of etiology and management of precipitating factors in AHF patients are recommended
I C
Intubation is recommended in patients with respiratory failure who cannot be managed non-invasively
I C
Non-invasive positive pressure ventilation (e.g. CPAP, BiPAP) should be considered in patients with respiratory distress (respiratory rate >25 breaths/min, SpO2 < 90%) who have SBP > 85 mmHg and normal consciousness
IIa B
Oxygen therapy is recommended in AHF patients with SpO2 < 90% or PaO2 < 60 mmHg to correct hypoxemia I C
Oxygen therapy is not routinely recommended III C
\
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
Recommendations COR LOE
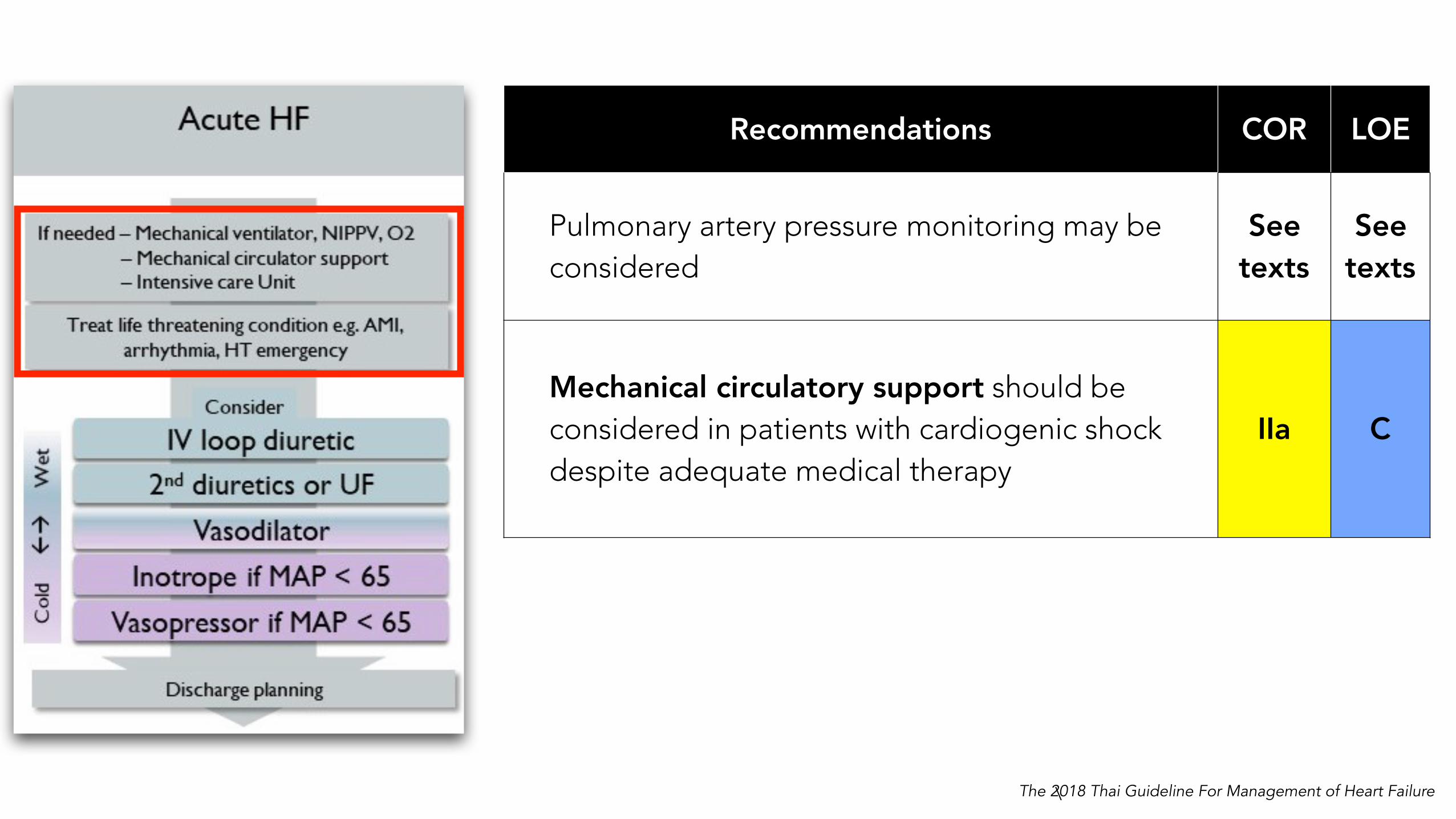
Pulmonary artery pressure monitoring may be considered
See texts
See texts
Mechanical circulatory support should be considered in patients with cardiogenic shock despite adequate medical therapy
IIa C
The 2018 Thai Guideline For Management of Heart Failure
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
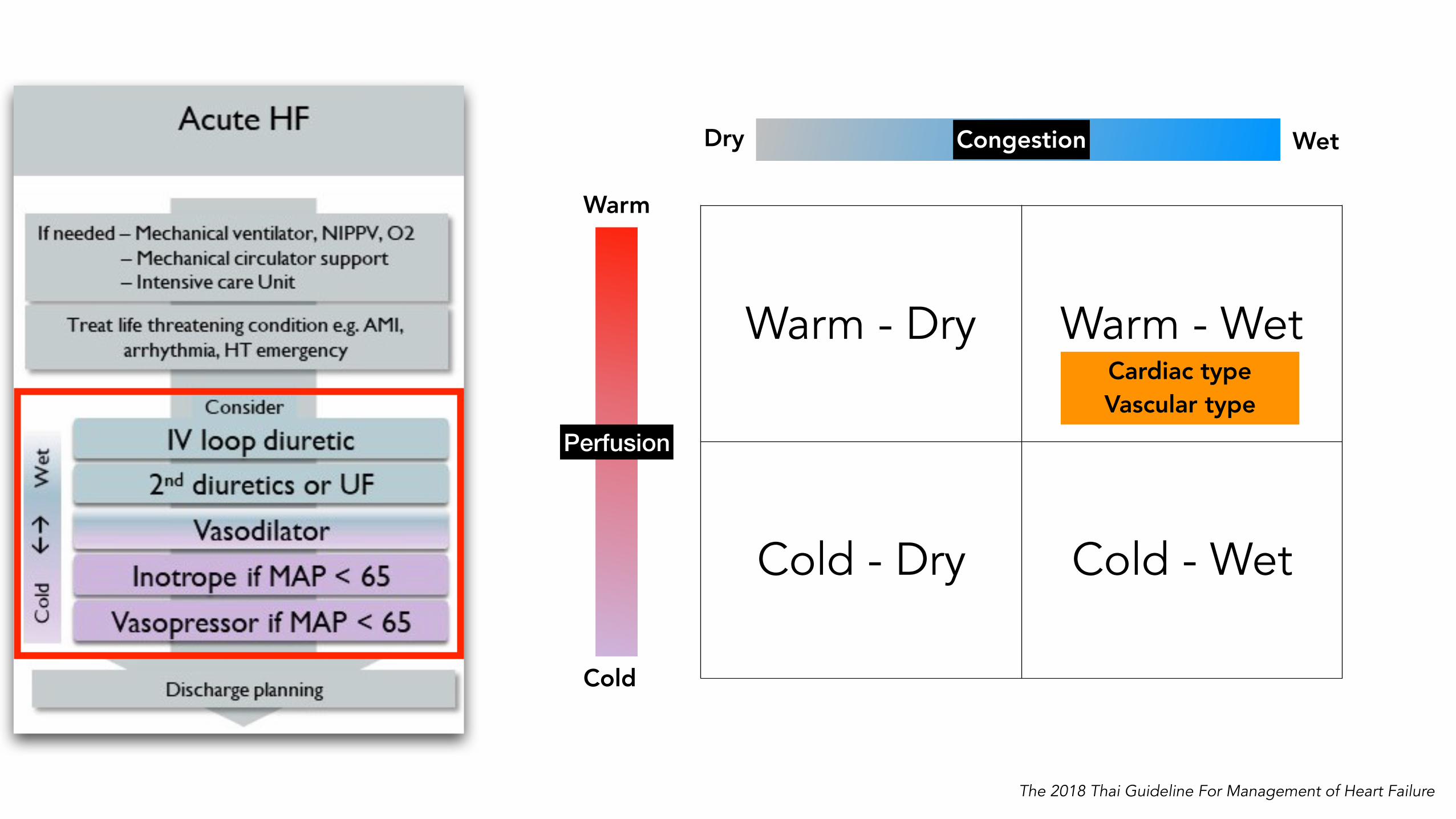
Warm - Dry Warm - Wet
Cold - Dry Cold - Wet
Cardiac type Vascular type
Dry Wet
Warm
Cold
Congestion
Perfusion
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
Loop diuretics are recommended to relieve signs and/or symptoms of congestion in heart failure patients
I B
Diuretics should be considered to reduce the risk of HF hospitalization in patients with signs and/or symptoms of congestion
IIa B
V2-selective vasopressin antagonist (tolvaptan) may be considered for adjunctive treatment in hospitalized heart failure patients with volume overload and inadequate response to diuretics with short-term use
IIb B
A V2-selective vasopressin antagonist (tolvaptan) may be considered for short-term use in hospitalized patients with symptomatic hyponatremia associated with hypervolumic state secondary to heart failure
IIb B
Decongestion
The 2018 Thai Guideline For Management of Heart Failure

Recommendations COR LOE
For warm and wet ( vascular type ), for congestive symptoms relief in patients with normal or elevated blood pressure (SBP>90 mmHg)
IIa B
Patients with signs/symptoms of hypoperfusion and congestion (cold and wet) with SBP > 90 mmHg, intravenous vasodilators should be considered with caution
IIa C
Cardiogenic shock I C
Signs/symptoms of hypoperfusion and/or end organ damage with hypotension (MAP < 65 mmHg) despite adequate filling status
I C
Intravenous infusion of milrinone or levosimendan may be considered to reverse the effects of beta blocker if beta blocker is considered as the cause of hypoperfusion
IIb C
Vasopressors (e.g. norepinephrine) may be considered in patients with cardiogenic shock, despite treatment with inotropic agents IIb B
IV Vasodilator
IV inotrope
IV vasopressor

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201811
Guideline implementation: Central illustration
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG2018
90
ACC/AHA 2009(stage D HF)
“Patients with truly refractory HF who might be eligible for specialized, advanced treatment strategies, such as mechanical circulatory support (MCS), procedures to facilitate fluid removal, continuous inotropic infusions, or cardiac transplantation or other innovative or experimental surgical procedures, or for end-of-life care, such as hospice.”
ACC/AHA 2013(stage D HF)
“A subset of patients with chronic HF will continue to progress and develop persistently severe symptoms despite maximum guideline-directed medical treatment (GDMT). Patients with marked HF symptoms at rest or recurrent hospitalizations despite GDMT.”
ESC 2007
1. Severe symptoms of HF with dyspnea and/or fatigue at rest or with minimal exertion (NYHA class III or IV).
2. Episodes of fluid retention (pulmonary and/or systemic congestion, peripheral edema) and/or reduced cardiac output at rest (peripheral hypoperfusion).
3. Objective evidence of severe cardiac dysfunction shown by at least 1 of the following:a. LVEF <30%b. Pseudonormal or restrictive mitral inflow patternc. Mean PCWP >16 mmHg and/or RAP >12 mmHg by PA catheterizationd. High BNP or NT-proBNP plasma levels in the absence of noncardiac causes
4. Severe impairment of functional capacity shown by 1 of the following:a. Inability to exerciseb. 6-Minute walk distance ≤300 md. Peak VO2 <12 to 14 mL/kg/min
5. History of ≥1 HF hospitalization in past 6 months.6. Presence of all the previous features despite “attempts to optimize” therapy, including diuretics
and GDMT, unless these are poorly tolerated or contraindicated, and CRT when indicated.
Definition of Advanced HF in Various Guidelines.Definition of advanced/end-staged heart failure
The 2018 Thai Guideline For Management of Heart Failure

• Relatively invasive and life-changing for all involved
• Allow patients to gain functional capacity and to improve so-called “quality of death” in inotrope-dependent patients
• Heart transplant as a gold standard treatment with new mechanical circulatory support systems (MCS)
• Palliative care — patient and family-centered QOL
Treatment in end-staged heart failure
The 2018 Thai Guideline For Management of Heart Failure

Clinical findings suggested of patients with advanced HF
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201891
Clinical findings suggested of patients with advanced HF
Persistent severe symptoms - NYHA class III, IV- Dyspnea with taking shower, eating, talking or at rest- Homebound≥ 2 HF Hospitalization within 6 months *Cannot tolerate the same doses of ACE/ARB, ARNI or BB that used to be able to tolerate Need high dose of diuretics (daily furosemide equivalent dose > 240 mg) and/or supplement with second diureticsEnd-organ failure- Cachexia (BMI <19)- CKD stage > 3, progressive worsening in BUN and/or Cr , hyponatremia- Cardiac cirrhosis, hypoalbuminemia- Pulmonary hypertension due to left heart diseaseMultiple ICD shocksUnresponsive to CRT treatmentDependence on intravenous inotropic medications * After a careful consideration of any reversible causes and optimization of treatment including HF self-care such as fluid and salt limitation, medication adherence, and medical and CRT/ICD therapy.
The 2018 Thai Guideline For Management of Heart Failure

HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201895
Recommendation COR LOEDiagnosisAn evaluation of prognosis is recommended in patients with persistent symptomatic HF. I C
It is recommended to investigate etiology of heart failure, patient compliance to treatment and alternative explanation for symptoms in patient with advanced HF. I C
ManagementSelection of treatments for advanced HF depends upon patient’s goal of care, prognosis and transplant candidacy. I C
Patient who is considered for heart transplant or MCS should be managed in conjunction with a referral center. I C
MedicationDigoxin may be considered in patient with advanced HF to improve symptoms and reduce HF hospitalization. IIb B
Continuous long-term use of intravenous inotropes such as dobutamine, milrinone, levosimendan or dopamine may be considered in patients with advanced HF with reduced EF to maintain end-organ performance and evaluating for appropriate treatment such as heart transplant, MCS , palliative care or other treatments
IIb B
Continuous long-term use of intravenous inotropes are not recommended in patients with life threatening arrhythmia, patients who have no hemodynamically response to these medications or patients with HFpEF.
III B
End-Staged Heart Failure- RecommendationRecommendations for end-staged heart failure
The 2018 Thai Guideline For Management of Heart Failure
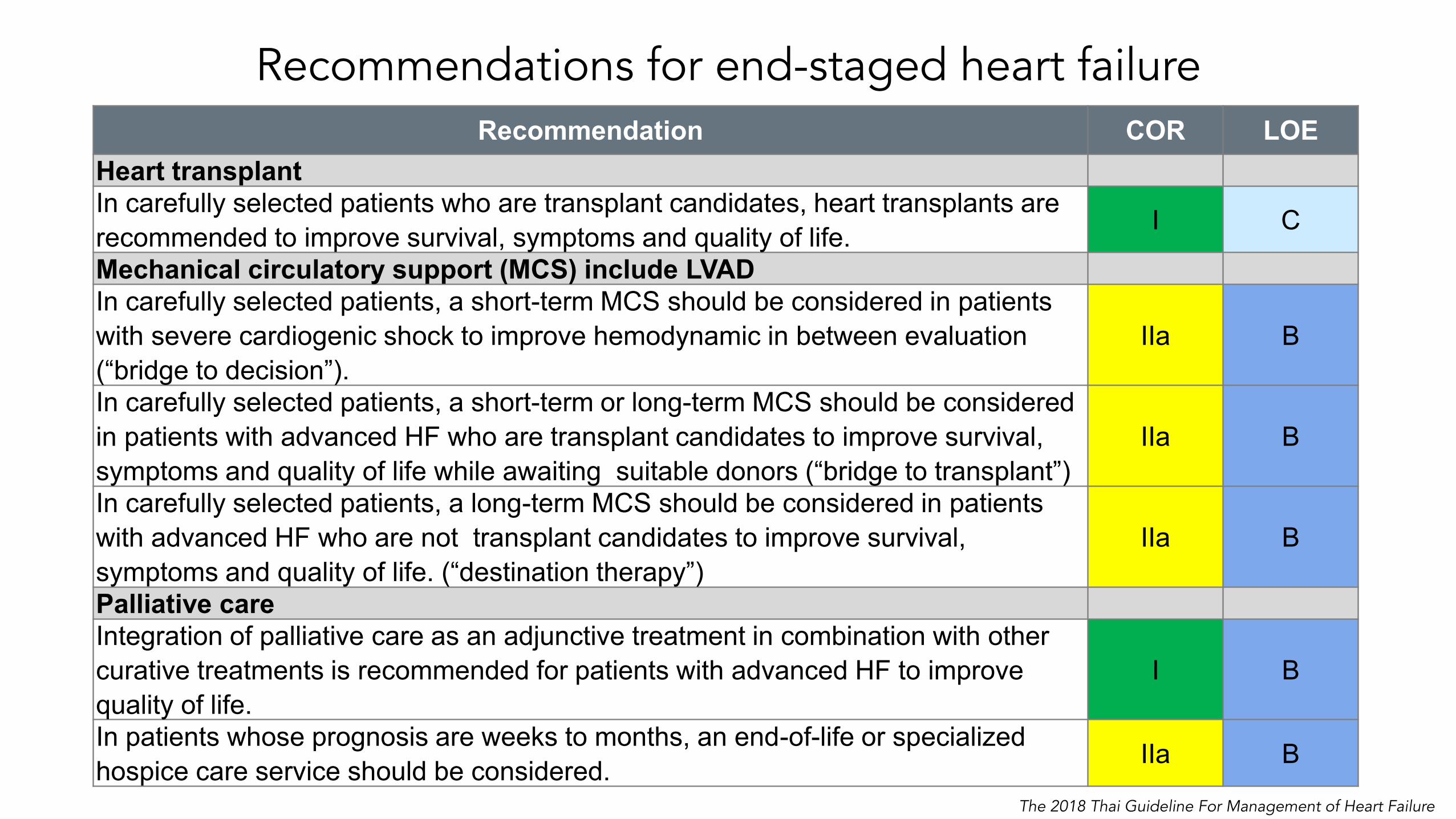
Recommendations for end-staged heart failure
HFCT/HAT 2018 Heart Failure Guideline_ Official Slide SetPreliminary_ver2.3_13AUG201896
Recommendation COR LOEHeart transplantIn carefully selected patients who are transplant candidates, heart transplants are recommended to improve survival, symptoms and quality of life. I C
Mechanical circulatory support (MCS) include LVADIn carefully selected patients, a short-term MCS should be considered in patients with severe cardiogenic shock to improve hemodynamic in between evaluation (“bridge to decision”).
IIa B
In carefully selected patients, a short-term or long-term MCS should be considered in patients with advanced HF who are transplant candidates to improve survival, symptoms and quality of life while awaiting suitable donors (“bridge to transplant”)
IIa B
In carefully selected patients, a long-term MCS should be considered in patients with advanced HF who are not transplant candidates to improve survival, symptoms and quality of life. (“destination therapy”)
IIa B
Palliative careIntegration of palliative care as an adjunctive treatment in combination with other curative treatments is recommended for patients with advanced HF to improve quality of life.
I B
In patients whose prognosis are weeks to months, an end-of-life or specialized hospice care service should be considered. IIa B
End-Staged Heart Failure- Recommendation
The 2018 Thai Guideline For Management of Heart Failure

Summary— 2018 Thai guidelines on heart failure
• Comprehensive review of evidences
• The recommendations span across spectrum of HF — more details on management of acute heart failure
• New recommendations have been added or updated on — ARNI in HFrEF— Iron deficiency and anemia — Diabetes (SGLT2-i)— MRA in HFpEF— AF, Device therapy, MCS/VADs— End-staged HF including cardiac transplant , palliative care
• Role of multidisciplinary approach

Adisai Buakhamsri, MD Thammasat University Hospital
On-behalf of the writing committee of The 2018 HAT Guideline For The Management of Heart Failure
Highlights of 2018 Thai Guidelines For The Management of Heart Failure






















![[Thai] FSI Thai Basic Course 1](https://img.pdfslide.us/doc/110x75/54e89b874a79599f4e8b497f/thai-fsi-thai-basic-course-1.jpg)