Embed Size (px)
Citation preview

731
HIGH DOSE METHYLPREDNISOLONE INCREASESPLASMA CYCLOSPORIN LEVELS IN RENAL
TRANSPLANT RECIPIENTS
SIR,-While monitoring plasma cyclosporin levels in renal
transplant patients we noticed striking increases after theintravenous administration of high doses of methylprednisolone foracute graft rejection. We have retrospectively analysed data fromthirty-three consecutive patients who received rejection treatment.At the time of rejection the maintenance immunosuppressionconsisted of oral cyclosporin and prednisolone, at daily doses of4-15 mg/kg and 10-40 mg, respectively. The rejection treatmentconsisted of intravenous bolus doses of methylprednisolone, 0,5 5 gon the first day and 0-25 g on the following 3-5 days. Thecyclosporin trough plasma levels were measured byradioimmunoassay.1 IIn eleven patients cyclosporin levels remained essentially
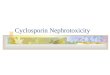
unchanged after methylprednisolone but in the remaining twenty-two they rose (figure), from 205±28 ng/ml (mean ±SEM, n=22)before methylprednisolone to peaks of482±61 ng/ml during orimmediately after such treatment (p<0 001). Six patients had theircyclosporin dose reduced because of high plasma levels and in twocyclosporin was discontinued because the grafts were deemed to beirreversibly damaged. In the fourteen patients whose cyclosporindose remained unchanged plasma levels returned to pre-rejectionvalues within 2 weeks, the mean being 210±21 ng/ml.The possibility that methylprednisolone might have affected the
assay was tested by adding methylprednisolone in vitro to plasmafrom patients on cyclosporin. The results were not affected.
Methylprednisolone metabolites were not tested.The reason for the increase in cyclosporin levels seen after high-’
dose methylprednisolone can dnly be speculated on. Since bothcyclosporin and prednisolone probably utilise hepatic microsomal
1. Donatsch P, Abisch E, Homberger M, et al. A radioimmunoassay to measurecyclosporin A in plasma and serum samples. J Immunoassay 1981; 2: 19-32.
Initiation of Methylprednisolone Treatment
Trough cyclosporin plasma levels before, during, and after rejectiontreatment with bolus doses of methylprednisolone in twenty-tworenal transplantrecipients. ,
In eleven other patients so treated the cyclosporin plasma levels remainedessentially unchanged. *Patients in whom the cyclosporin dose was reducedbecause of high cyclosporin levels. **Patients in whom cyclosporin wasdiscontinued.
enzymes for their metabolism" and since the rise and fall in
cyclosporin levels occurred rapidly one possible explanation couldbe that the steroid inhibits the metabolism of cyclosporin. Suchinhibition might be mutual. Dr Ost, at our institution, has foundthat the clearance of prednisolone is reduced in patients treated withcyclosporin (Feb 25, p 451).Our finding has clinical implications. An increase in cyclosporin
may cause side-effects, such as nephrotoxicity with an increase inserum-creatinine, and this in turn may make it difficult for theclinician to decide on the cause underlying the deterioration in therenal function. In a renal transplant recipient, a rise in serumcreatinine is usually assumed to be due to graft rejection unlessproved otherwise. Methylprednisolone is then promptly given. If,subsequent laboratory reports disclose a high cyclosporin level thismight lead to re-evaluation of the diagnosis: the clinician will say"this must be an episode of cyclosporin nephrotoxicity". In some ofour patients the cyclosporin dose was lowered because of such aconclusion; in others it was not. Further data are needed before thecorrect response in this situation can be defined.The question of whether oral prednisolone, given for
maintenance immunosuppression, also inhibits cyclosporinmetabolism and thereby potentiates the effect of any given dose ofcyclosporin cannot be answered on the basis of our data because allpatients were maintained on both drugs throughout.Departments of Transplantation Surgeryand Clinical Pharmacology,
Karolinska Institute,Huddinge Hospital,S-141 86 Huddinge, Sweden
GORAN KLINTMALM
JULIETTE SÄWE
AZOOSPERMIA INDUCED BY 19-NORTESTOSTERONE
SIR,-The use of the synthetic androgen 19-nortestosterone tobring about azoospermia, described by Dr Schurmeyer andcolleagues (Feb 25, p 417), may, in the long term, affect androgentarget organs and secondary sexual characteristics. This is because19-nortestosterone is a much weaker androgen than testosteronealthough it has equivalent myotrophic activity.3,4 The suppressionof gonadotropin release in man can also be achieved by treatmentwith 5 a -dihydrostestosterone,5 a potent androgen and a majortestosterone metabolite. However, the use of dihydrostestosteronealone as a contraceptive agent is precluded because it does notsupport sexual behaviour. Studies in animals suggest that malelibido may require the conversion of androgen to oestrogen(aromatisation) in the central nervous system and it is of note thattestosterone and 19-nortestosterone are aromatisable whereas
dihydrotestosterone is not. Evidence that the "aromatisation
hypothesis" of testosterone action may be applicable to man isprovided by a recent report where sexual function was maintainedin a castrated man given oestrogen and progesterone. An effectivemeans of providing an oestrogenic stimulus, without usingoestrogen itself or an aromatisable synthetic steroid such as
19-nortestosterone, might be to use the androgen/oestrogenintermediate 19-hydroxytestosterone. This hormone maintainssexual arousal in laboratory animals and, in combination withdihydrotestosterone, might provide effective fertility control.
Department of Behavioural Physiology,AFRC Institute of Animal Physiology,Babraham, Cambridge CB2 4AT R. F. PARROTT
2. Langhoff E, Madsen S. Rapid metabolism of cyclosporin and prednisone in kidneytransplant patient receiving tuberculostatic treatment. Lancet 1983; ii: 1031.
3. Herscheberger LG, Shipley EG, Meyer EK. Myotrophic activity of 19-nortestosteroneand other steroids determined by modified levator ani muscle method. Proc Soc ExpBiol Med 1953; 83: 175-80.
4. Segaloff A. Some biological and clinical aspects of the action of androgens andestrogens. Cancer Res 1963; 23: 1459-64.
5. Kuhn JM, Rieu M, Laudat MH, Forest MG, Pugeat M, Bricarie H, Luton JP. Effectsof 10 days administration of percutaneous dihydrotestosterone on the pituitary-testicular axis in normal men. J Clin Endocrinol Metab 1984; 58: 231-35.
6. McDonald P, Beyer C, Newton F, Brien B, Baker R, Tan HS, Sampson C, Kitching P,Greenhill R, Pritchard D. Failure of 5&agr;-dihydrostestosterone to initiate sexualbehaviour in the castrated male rat. Nature 1970; 227: 964-65.
7. Davidson JM, Camargo C, Smith ER, Kwan M. Maintenance of sexual function in acastrated man treated with ovarian steriods. Arch Sex Behav 1983; 12: 263-74.
8. Parrott RF. Effects of 17&bgr;-hydroxy-4-androsten-19-ol-3-one (19-hydroxytestosterone)and 5&agr;-androston-17&bgr;-ol-3-one (dihydrostestosterone) on aspects of sexualbehaviour in castrated male rats. J Endocrinol 1974; 61: 105-15.