Embed Size (px)
Citation preview

Lisa M. Brown, MD, MASAssistant Professor of Thoracic Surgery
University of California, Davis Health
Hiatal Hernia & GERD

• 45 year old woman with hiatal hernia discovered during workup for heartburn
• Her symptoms include heartburn increasing in severity over the past 5 years and occasional regurgitation
• She has no dysphagia
Case Study

Case Study: Psychosocial History• Cigarette Smoking
• Former Smoker, quit 10 years ago• 10 pack years
• Living Status• Lives alone
• Functional Status• Independent
• ECOG Score • 0

Symptoms
• Heartburn, regurgitation

Proton Pump Inhibitors (PPIs)
• Yes, Omeprazole • Partial relief

PPI Mechanism of Action
Gastrin
CCK2Receptor
PPI
AcetylcholineMuscarinic AntagonistsMuscarinic
M3 Receptor
Histamine H2Receptor Antagonists
Histamine
H2 Receptor
Parietal Cell
H+K+
ATPase
H+ K+
Acid
Gastric GlandLumen

Proton Pump Inhibitors (PPIs)• Omeprazole (Prilosec) (available OTC)• Esomeprazole (Nexium) (available OTC)• Lansoprazole (Prevacid)• Rabeprazole (AcipHex)• Pantoprazole (Protonix)• Zegrid (Omeprazole with sodium bicarbonate) (available OTC)

Case Study: EGD• Z-line at 40 cm from the incisors
• Biopsy without intestinal metaplasia• Hiatal hernia and normal mucosa in the stomach• The duodenal mucosa was normal

Kamal A, et al. Best Practice & Research Clinical Gastroenterology.2010;24(6):799-820

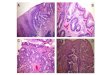
Barrett’s Esophagus• Premalignant condition
• Chronic injury from GERD• Mucus-secreting columnar cells replace reflux-damaged esophageal squamous
cells (metaplasia)• The only known precursor of esophageal adenocarcinoma• A small % of patients with BE will develop cancer
• More than 90% of patients with cancer have no prior history of BE• It is unclear why some patients with BE progress to cancer

Barrett’s Esophagus• At least 1 cm of salmon-colored mucosa proximal to the GEJ
• Biopsy confirmation of intestinal metaplasia
SquamousEpithelium
Columnar Epithelium(Intestinal Metaplasia)
Goblet CellGEJGEJ

Spechler SJ, Souza RF. NEJM 2014 Aug 28;371(9):836-45
Barrett’s Esophagus• Classification
• No dysplasia• Indefinite for dysplasia• Low-grade dysplasia• High-grade dysplasia

Barrett’s Esophagus

pH Testing

pH Testing
YesDeMeester score 58.4

Case Study: ManometryLower Esophageal Sphincter RegionLandmarksProximal LES (from nares/cm) 42.0LES length (cm) 4.0Esophageal length (LES-UES centers/cm) 23.3Intraabdominal LES length (cm) 0.0Hiatal hernia? Yes
LES PressuresPressure measurement method eSleeve, IRP
Basal (respiratory mean)(mmHg) 20 (13-43)
Residual (median)(mmHg) 6 (<15.0)
Esophageal MotilityNumber of swallow evaluated 12Chicago Classification% failed 0% weak 0% ineffective 0% panesophageal pressurization 0% premature contraction 0% fragmented 0% intact 100

Manometry
• Yes, Normal• LES resting pressure: 20 mmHg • % of failed swallows: 0%

Case Study: Imaging
Barium Swallow• No abnormality of the swallowing function• Configuration and motility of esophagus are
normal• Small sliding hiatal hernia
• Trace amount of elicited gastroesophageal reflux to the level of the mid-esophagus
• IMPRESSION• Small sliding-type hiatal hernia• Small volume gastroesophageal reflux
occurs with provocative maneuvers.

Imaging
• Yes• Type of imaging: Barium Swallow/Upper GI

Hiatal Hernia Type• Type I
• Sliding hiatal hernia• 95% of all HH
• Type II• Paraesophageal hernia
• Type III• Combination of Types I and II
• Type IV• Herniation of additional organs

Hiatal Hernia Size• Not always documented• May be documented in the following reports:
• Esophagogastroduodenoscopy (EGD)• Esophagram / Barium Swallow • Chest or Abdominal CT scan

Hiatal Hernia Size and Type
• Hiatal hernia size (cm): Missing Data
• Hiatal hernia type: I

Case Study: Operation
• Hernia repair status: Primary repair

Case Study: Procedure Approach
• Laparoscopic

Operative Details
• Fundoplication: Yes / Complete• Gastroplasty: No• Mesh: No• Relaxing Incision: No

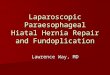
Fundoplication
Nissen(Complete)
Toupet(Partial)
Dor(Partial)
Normal Anatomy

Tension Free Hiatal Hernia Repair
Bradley DD et al. Surg Endosc 2015;29:796-804
• Axial Tension• Along the length of the
esophagus• Shortened Esophagus
• Intra-abdominal length <2cm
• Radial Tension• Between diaphragmatic
crura

Gastroplasty
• Shortened Esophagus• Most commonly from GERD• Inflammation
• Edema ----> Fibrosis• Can extend transmurally (full
thickness)• Repeated cycles of injury and repair• Contraction of collagen in scar
• Circumferential -> peptic stricture• Longitudinal -> short esophagus
Horvath KD et al. Ann Surg 2000;232(5):630-40

Gastroplasty (Collis)
Horvath KD et al. Ann Surg 2000;232(5):630-40

Mesh
Oelschlager BK et al. Ann Laparosc Endosc Surg 2017;2:50

Relaxing Incision: Right
Greene CL et al. Surg Endosc 2013;27:4532-38

Relaxing Incision: Left
Greene CL et al. Surg Endosc 2013;27:4532-38

Diagnosis

Primary Procedure


Case Study: Follow Up• Alive at 30 days• Postoperative course was unremarkable• Tolerating soft diet without dysphagia or heartburn
• Off of Omeprazole• No radiographic recurrence, symptom recurrence, endoscopic
intervention nor re-operation