Embed Size (px)
Citation preview
Volume 37, Number 1Patients First®
THE ALBERTA DOCTORS’
January/February 2012
Members help identify prioritiesin tracker surveyThe AMA is making progress in achieving fee equity.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07TD InSuRAnCE
MELOCHE MOnnEx/ AMA ScholArShiP
PRIMARY CARE
ALLIANCE
Finding Balance Campaign
Nominationsfor Achievement
Awards
TarrantScholarship
“Hey, AMA!”
Alberta Doctors’ Digest • January/February 20122
Are we too noisy?The health effects of all our noise on our cardiovascular systems and our nerves have been well documented, and everyone knows we’re ruining our ears. I’ve recently read a couple of good books on noise1,2 and have come to realize it’s something that people have been upset about for years. Mussolini, for example, declared war on noise in Italy in 1933, without much success.
Maybe there’s a hole in my hippocampus, or too much moisture in my frontal lobes. Maybe it’s age or maybe I’m just sensitive. But I think the world is getting noisier.
When I was a medical student half a century ago, I was lucky enough to spend time with a family doc in Mannville – and later in Vermilion – and experience the flavor of rural practice. Dr. Hasinoff – or “Dr. Dave,” as I called him – took me round his small hospital and would show me, for example, an old lady with pneumonia, a new mom with her baby, a child with croup and so on. I remember the time Dr. Dave showed me a new car he’d just gotten. It was a big, shiny brown Chrysler, a muscular car with fins and all the bells and whistles. All the bells and whistles except one, though: the car had no radio. Dr. Dave had had it removed. When I asked why, he smiled: “Peace and quiet.”
All these decades later, I know that Dr. Dave was prescient. We’re too noisy.
From The Editor
Dennis W. Jirsch, MD, PhD
EdiTor
the “Queen of Silence” by the press, was originally upset at the gratuitous night-time tooting of tugboats near her home in New York City. She was a force to be reckoned with and influenced public policy widely. Her efforts were largely responsible for our near-ubiquitous attempts to have quiet zones near public hospitals. Rice was a complicated lady, though, and so were her children, with one daughter a pilot and another the first woman in New York to speed around on a motorcycle.
There have been legal efforts worldwide to constrain noise – for example, I think locally we try to keep motorcycles muffled, but generally I think it’s pretty ineffectual stuff.
So I maintain we become noisier with each passing year. I have read about the extreme end of things, with noise used as weaponry and the car audio systems that have become so mammoth as to require extra storage space and even extra car batteries.
On a smaller scale there are the Walkman/MP3 devices plugged into ears on buses, in classrooms, gyms, pretty well everywhere. I’ve wondered about them mightily since on an evolutionary basis it would seem that the degree to which we have survived for millennia, probably
The health effects of all our
noise on our cardiovascular
systems and our nerves have
been well documented,
and everyone knows we’re
ruining our ears.
Even earlier in 1906, a woman called Julia Barnett Rice, along with an MD from the Women’s Medical College of the New York Infirmary, founded the Society for the Suppression of Unnecessary Noises. Rice, dubbed

Alberta Doctors’ Digest • January/February 2012 3
first as little tree-hugging creatures, surely depended on our ability to stay quiet, wary and listening in a world of more noisy predators. I realize our personal MP3-type noise may be a way of shutting things out, preventing unwanted stimuli. MP3 player users, I’m sure, would maintain that their noise devices add something to their lives, and I’ve heard Attention Deficit Disorder specialists say that some extraneous sounds can help sufferers, perhaps amplifying things or avoiding other distractions.
profundo of Leonard Cohen drives women crazy.
We’re perhaps just starting to recognize the salubrious qualities of quiet – silence is, after all, a big part of pretty well all the world’s religions. On this continent I gather there are long queues of people waiting to visit Trappist monasteries and the benefit of attending to quiet has long been especially recognized by Quakers, Buddhists and practitioners of silent meditation. Certainly silence offers space for reflection, but more than this it lets us “time out.” The damnable fact about our brains is that we live in a perpetual conundrum: we’re stuck in the here-and-now, but our brains have evolved to spool incessantly, either back in time or into the future, trying to solve – trying to re-solve or resolve – problems both real and imaginary. It’s hard to stop ourselves, but in quiet we can begin to do just that.
Prochnik1 has defined noise as sound that gets into your head and won’t go away. Conversely, silence is that mixture of sound and quiet that is eminently agreeable, that nourishes our powers of perception. When all is said and done we can’t find absolute silence; it’s like trying to get to Absolute Zero and there is a long list of people who have gone bonkers looking for total silence. Come close and you will start to hear your breath, fingers on your skin, or even the blood sloshing beneath your ears.
I’d say that, like many things, it’s a matter of balance. I’m in favor of developing lists of favorite sounds and their opposites, the noxious ones. My list of good stuff, for example, would include the sound – or lack
thereof – in my laneway late evening after a snowfall, the crunch of boots in snow on a sunny afternoon in January, and the riotous calls of bullfrogs in late spring.
My most noxious list is probably longer but would certainly include hard rock, certain strident voices, canned sit-com laughter and pretty well any store music. Retail sales experts talk about “sonic branding,” hence the peculiar, irritating tunes in stores and they well know that we drink and buy and eat more and faster when things are loud and the tempo is up.
I’d just as soon do without all of it. I long for the days when libraries were quiet places. It’s all situational of course, and I have to agree with Tom Waits4 who said: “The sound of a helicopter is really annoying, until you’re drowning and it’s there to rescue you. Then it sounds like music.”
And I think that Yogi Berra may have said it best: “You can hear a lot just by listening.”
I’m going to go and put some music on – perhaps Bach, or a little classical guitar. Or maybe I won’t. I’m pleased to know the choice is mine.
Thanks again, Dr. Dave, for taking out that radio.
References
1. In Pursuit of Silence: Listening for Meaning in a World of Noise, George Prochnik, Anchor Books, New York, 2010.
2. The Unwanted Sound of Everything We Want: A Book about Noise, Garret Keizer, Perseus Books Group, Philadelphia, 2010.
3. “A coachman who”: Lawrence Baron, “Noise and Degeneration: Theodor Lessing’s Crusade for Quiet,” Journal of Contemporary History 17, 1 (January 1982):165-78.
4. Tom Waits on his new album, “Bad as Me”.
We’re perhaps just starting
to recognize the salubrious
qualities of quiet — silence is,
after all, a big part of pretty well
all the world’s religions.
Philosopher Theodor Lessing3 noted 100 years or more ago that when people lack economic and social power, they often try to up their impact in the world by making noise. So it must be said that we make noise not only to communicate but sometimes to roar like lions, trying to secure our world with feigned bravado. Of course, there are harmonics and all the complexities of music too, and there’s the stuff about sound and gender. Low pitched – presumably male – voices may signal greater reproductive potential, and I reckon this is why the gravelly
3 Townhomes in old sTraThconaResidences @ 105 stReet
CUSTOM DESIGN YOUR HOME: The three residences are located in the heart of Strathcona on 87th Avenue between 105th and 106th Street. Each unit will be built with the highest standards for energy efficiency.
The sereniTyBrand new high-rise building on Jasper Avenue with 17 units left. Featuring 2 bedroom
and 2 bedroom + den units with hardwood flooring, granite, open floor plans, great views. 1,234 sq.ft. to 2,782 sq.ft. Convenient location, close to transportation, restaurants, coffee
shops, grocery stores, the Promenade, and the river valley. Starting at $465,000.
darlene sTrangYour Personal Realtor for Life
Condominium Specialist
[email protected] www.darlenestrang.com
For information on other properties, please visit my website at www.darlenestrang.comWhether you are buying or selling, I will be pleased to assist you.
Alberta Doctors’ Digest • January/February 2012 5
AMA Mission stAteMent
The AMA stands as an advocate for its physician members, providing leadership and support for their role in the provision of quality health care.
6 “Hey, AMA!” Members help identify priorities The AMA reports on another year of results from its member opinion tracker survey.
10 AMA seeks 2012 nominations to recognize outstanding achievements
Achievement Awards honor individuals who have contributed to improvement of the quality of health care in Alberta.
15 Tarrant Scholarship encourages students to practice in rural communities Help rural communities get the basic health care most Albertans take for granted.
18 Zumba anyone? Keeping active helps prevent seniors’ falls With arms waving, hips circling and the sound of belly-dancing scarves jingling, a group of seniors helped launch the fourth annual, AMA-sponsored Finding Balance public awareness and education campaign.
20 Introducing the Primary Care Alliance – a new representation structure for primary care The Alberta Medical Association’s primary care representative groups have reorganized to better serve the needs of their constituents and to better reflect the landscape of primary care in the province.
22 Apply for 2012 TD Insurance Meloche Monnex/ AMA Scholarship Picture it: $5,000 assistance for your additional training in a clinical area of recognized need in Alberta.
Patients First®
Patients First® is a registered trademark of the Alberta Medical Association.
The Alberta Doctors’ Digest is published six times annually by the Alberta Medical Association for its members.
Editor: Dennis W. Jirsch, MD, PhD
Co-Editor: Alexander H.G. Paterson, MB ChB, MD, FRCP, FACP
Editor-in-Chief: Marvin Polis
President: Linda M. Slocombe, MDCM, CCFP
President-Elect: R. Michael Giuffre, MD, MBA, FRCP, FRCPC, FACC, FAAC
Immediate Past President: Patrick J. (P.J.) White, MB, BCh, MRCPsych
Alberta Medical Association 12230 106 Ave NW Edmonton AB T5N 3Z1 T 780.482.2626 TF 1.800.272.9680 F 780.482.5445 [email protected] www.albertadoctors.org
March/April issue deadline: February 15
The opinions expressed in the Alberta Doctors’ Digest are those of the authors and do not necessarily reflect the opinions or positions of the Alberta Medical Association or its Board of Directors. The association reserves the right to edit all letters to the editor.
The Alberta Medical Association assumes no responsibility or liability for damages arising from any error or omission or from the use of any information or advice contained in the Alberta Doctors’ Digest. Advertisements included in the Alberta Doctors’ Digest are not necessarily endorsed by the Alberta Medical Association.
© 2012 by the Alberta Medical Association
Design by Sarah Tiemstra at Backstreet Communications
CONTENTSTABLE OF
FEATuRES
DEPARTMEnTS
Cert no. XXX-XXX-000
2 From the Editor
11 letters
12 insurance insights
14 health law Update
16 Mind Your own Business
23 residents' Page
24 PFSP Perspectives
26 Web-footed Md
29 in a different Vein
32 classified Advertisements
Alberta Doctors’ Digest • January/February 20126
c o V E r F E AT U r E
Members help AMA identify priorities:
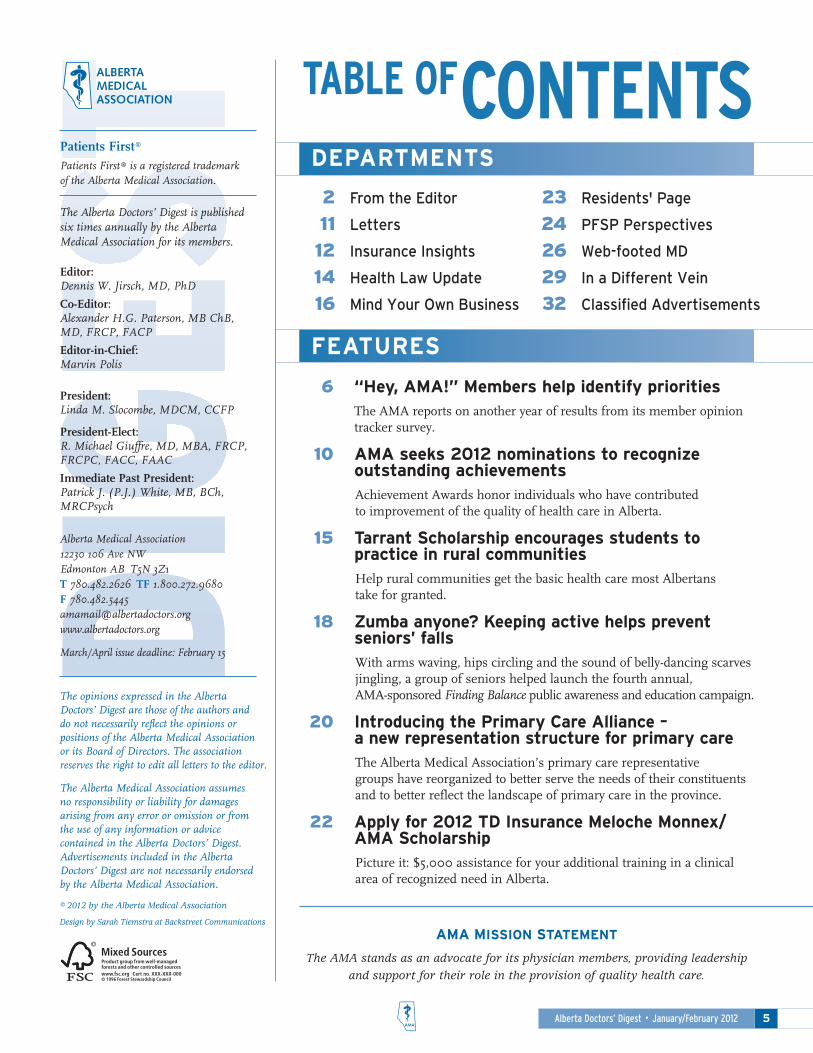
Year-end results from tracker surveyThe Alberta Medical Association (AMA) strives every day to identify issues that are important to its membership. One method is the tracker survey that is administered quarterly by Vancouver-based twisurveys. Anonymity of respondents is assured.
Every time you complete a survey, you are making your voice heard.
Collecting members’ views helps the Representative Forum, Board of Directors and senior staff identify priorities and develop the AMA’s annual business plan, strategies and activities. In addition, the association’s effectiveness in meeting members’ expectations and needs may be evaluated.
While reviewing an excerpt of the September 2011 survey below, consider that trends are analyzed, year over year since 2003 (or later for questions added at later dates).
With so many activities underway as we support members and pursue the mission of Patients First®, the perspectives physicians provide in the tracker survey are absolutely essential. The AMA extends sincere appreciation to all survey participants in 2011 and we look forward to continuing to engage with you via new tracker surveys in 2012.
The AMA is making progress in achieving fee equity.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
“Hey, AMA!”
Alberta Doctors’ Digest • January/February 2012 7
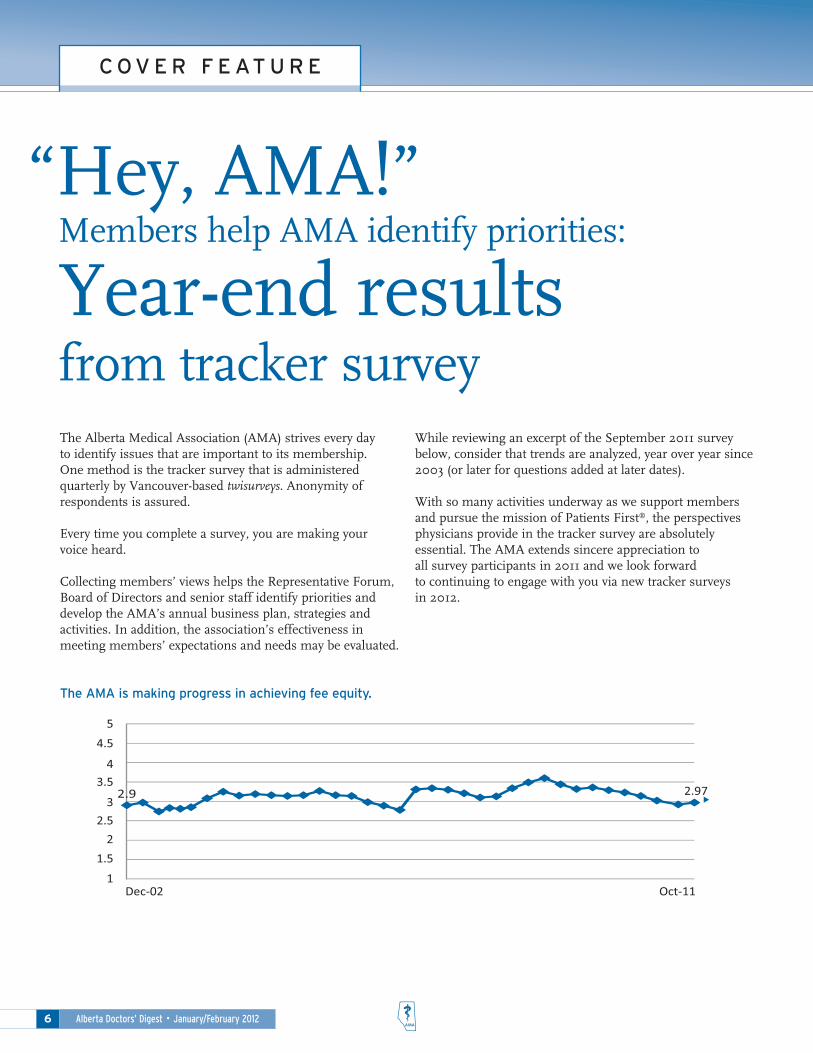
changes in the health care system during the past 12 months have improved my ability to meet the needs of my patients.
Funding of the Alberta health care system is keeping pace with the province's economic growth.
Whether or not i am compensated for it, i have a professional responsibility to provide on-call coverage for my patients.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
Primary care networks will help physicians to improve the delivery of care for our patients.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
Alberta Doctors’ Digest • January/February 20128
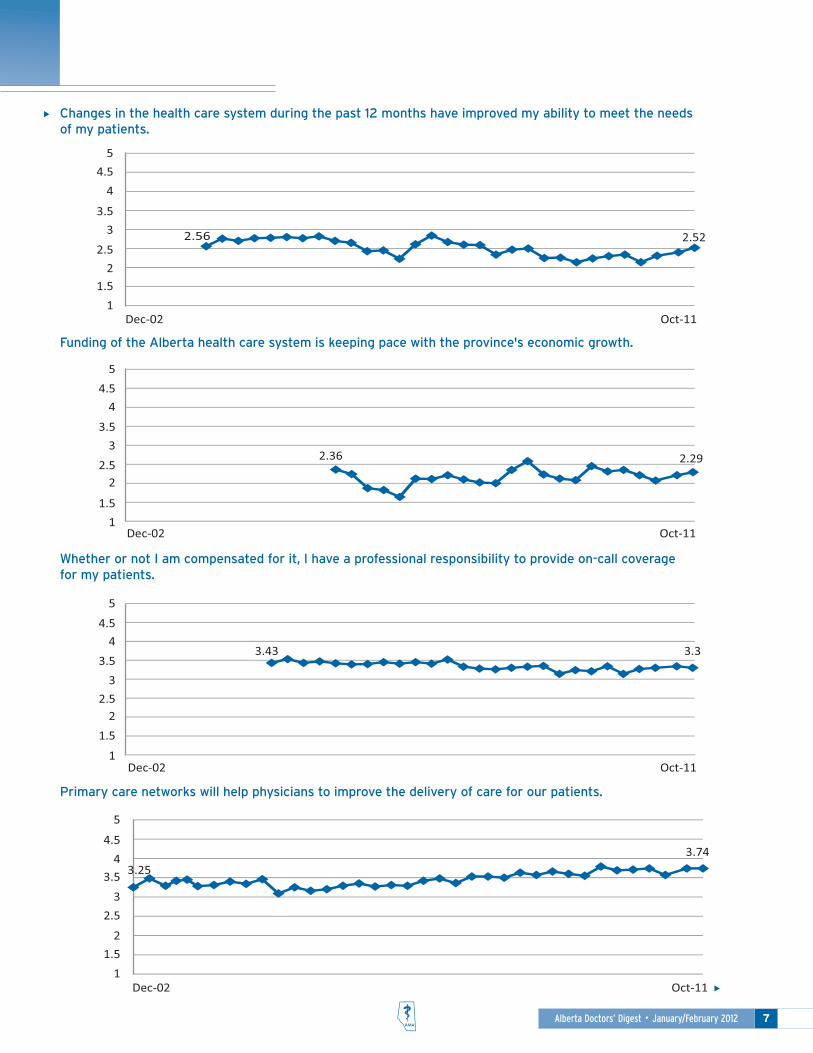
The physician's traditional role as manager and gatekeeper of the patient's record must be maintained in the design of electronic health and medical records.
in the past 12 months, i have taken steps to improve the balance between my professional life and my personal life.
Funding for computerized office systems should be independent from Alberta health Services.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07The development of a computerized health care system will improve the delivery of health care to my patients.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
Alberta Doctors’ Digest • January/February 2012 9
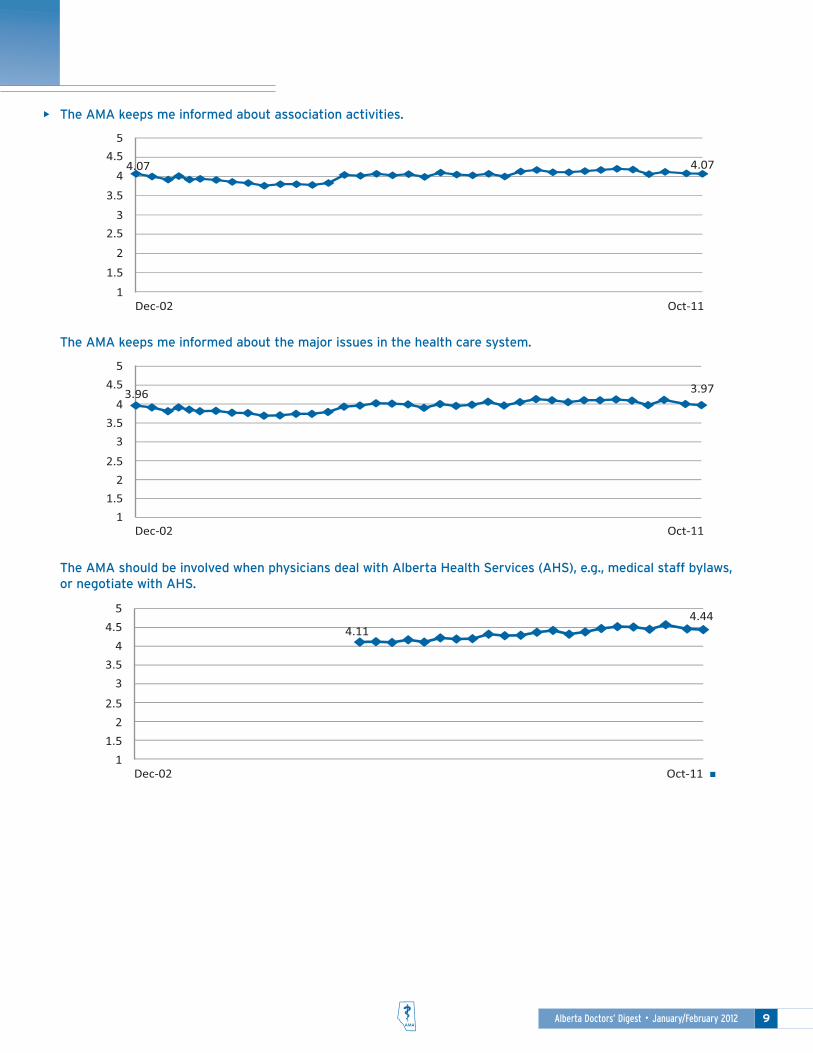
The AMA keeps me informed about the major issues in the health care system.
The AMA keeps me informed about association activities.
The AMA should be involved when physicians deal with Alberta health Services (AhS), e.g., medical staff bylaws, or negotiate with AhS.
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
2.97
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
2.56 2.52
1
1.52
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
2.36 2.29
1
1.5
22.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.43 3.3
1
1.5
22.5
3
3.5
44.5
5
Dec-02 Oct-11
2.9
3.74
1
1.5
2
2.5
3
3.54
4.5
5
Dec-02 Oct-11
3.87
11.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.18 4.25
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.963.58
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.34 3.46
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.97
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
4.114.44
1
1.5
2
2.5
3
3.5
4
4.5
5
Dec-02 Oct-11
3.25
3.86
3.96
4.07 4.07
Alberta Doctors’ Digest • January/February 201210
F E AT U r E
The Alberta Medical Association (AMA) is calling for Achievement Awards nominations for individuals who have contributed to improvement of the quality of health care in Alberta.
The Medal for Distinguished Service is given to a physician(s) who has made an outstanding personal contribution to medicine and to the people of Alberta, and in the process has contributed to the art and science of medicine while raising the standards of medical practice.
The Medal of Honor is awarded to a non-physician(s) who has raised the standards of health care and contributed to the advancement of medical research, medical education, health care organization, health
education and/or health promotion to the public.
In 2011, three physicians were recognized with Medals for Distinguished Service.
• Dr. April S. Elliott, Calgary
• Dr. Anthony L. Fields, Edmonton
• Dr. Thomas G. Salopek, Edmonton
In 2011, two individuals were recognized with Medals of Honor.
• Tanny Nadon, Sherwood Park
• Gail O’Brien, Calgary
Nominations for 2012 must be submitted by April 30. The awards will be presented at the AMA’s fall 2012 annual general meeting in Edmonton.
To request a nomination form for these awards, please contact: Janice Meredith, Administrative Assistant, Public Affairs, AMA: [email protected], 780.482.2626, ext. 291, toll-free 1.800.272.9680, ext. 291 or visit the AMA website (www.albertadoctors.org).
AMA seeks 2012 nominations to
recognize outstanding achievements in health care
Locums needed. Short-term & weekends. Family physicians & specialists.
Experience:
• Flexibility – Practice to fit your lifestyle.
• Variety – Experience different Alberta practice styles.
• Provide relief – Support rural colleagues and rural Albertans.
• Travel costs, honoraria, accommodation and income guarantee provided.
AMA Physician Locum Services®
CONTACT:
Barry Brayshaw, Director
AMA Physician Locum Services®
T 780.732.3366
TF 1.800.272.9680, ext. 366
www.albertadoctors.org/
AMAPhysician/Locum

Alberta Doctors’ Digest • January/February 2012 11
Alberta Medical Association
Board of Directors 2011-12
September/October 2011 was a great edition of Alberta Doctors’ Digest, which is always good, but this time excelled!
It’s good to see that Dr. Vincent Hanlon who I worked with in Fort McMurray – he was an emergency physician at that time – is now a contributor. “See personal and professional reality more clearly” was a good article under PFSP Perspectives.
The editor (Dr. Jirsch) and co-editor (Dr. Paterson) also deserve congratulations on their articles and Jonathan P. Rossall’s article on who owns patient information was very, very helpful at this time.
Please keep up the good work! The whole edition of the Digest was full of gems!
Back row, left to right: Dr. Alison M. Clarke; Dr. Padraic E. Carr; Dr. Paul E. Boucher; Dr. Sarah L. Bates; Michael A. Gormley, Executive Director; Dr. Pauline Alakija; Dr. Daniel J. Barer; Dr. Khalil Jivraj, PARA observer; Dr. Kathryn L. Andrusky; Dr. Christine P. Molnar; Matthew S. Karpman, MSA observer
Front row, left to right: Dr. Fredrykka D. Rinaldi; Dr. E. Sandra Corbett; Dr. Linda M. Slocombe, President; Dr. R. Michael Giuffre, President-Elect; Dr. Patrick J. White, Immediate Past President; Christine A. Fleck, Executive Assistant
Sincerely,
George Horner, MD FRCPC, General Pathology (Retired)Clarenville NL
The Alberta Medical Association (AMA) welcomes comments about Digest articles and suggestions for future topics. Please contact Communications Assistant, Daphne C. Andrychuk, [email protected], or write her c/o Public Affairs, Alberta Medical Association, 12230 106 Ave NW, Edmonton AB T5N 3Z1. The association reserves the right to edit all letters.
Letters
Alberta Doctors’ Digest • January/February 201212
The retirement landscape today is vastly different than what it was even just a generation
ago. With life expectancies increasing, people can expect a retirement period that lasts for 30 years or more. Accordingly, one of the greatest risks people now face in retirement is outliving their savings.
Fortunately, there are steps you can take now that will help you protect your nest-egg and also save you money during your retirement years, when your income is likely to be reduced.
Maintain adequate disability insurance and office overhead expense insurance
If you have to take time off to recover from an illness or injury, disability insurance provides a monthly income replacement benefit, while office overhead expense insurance helps cover fixed costs (e.g., rent, utilities, payroll, etc.) of running your practice.
For professionals in the late career stage, it’s especially important to
Insurance Insights
Glenn McAthey, CFP, CLu, CHS
dirEcTor/SEnior
inSUrAncE AdViSor,
AdiUM inSUrAncE
SErVicES inc.
Take steps now to protect your retirement incomeInsurance planning advice for medical professionals in pre-retirement
maintain maximum coverage amounts for both of these types of insurance. Why? If you had to withdraw from your retirement savings to finance your recovery period (given that you have a limited number of earning years ahead), it would be difficult not only to replace these savings, but also recoup the lost returns on your investment growth.
time of conversion and the type of policy you purchase.
Protect your retirement income with long term care insurance
Many of us take for granted the ability to do things like bathing, getting dressed and eating. But now that we are living longer than ever, and with constant new life-saving medical advances, studies show that we have a significant likelihood of needing extended care at some point, whether at home or in a facility.
Long term care insurance (LTC) provides a weekly benefit should you require help with at least two activities of daily living, or suffer a cognitive impairment that requires constant supervision. This type of protection is vital to have in retirement, especially since you will no longer qualify for disability insurance.
Like permanent life insurance, LTC has numerous plan design choices. Along with vital financial assistance, it also helps you get the care you need without placing this burden on your spouse or partner, children, or other family members and friends.
As an example, Dr. G. was an established family physician who loved his work and had planned to keep practicing for many years to come. But at age 53, he began experiencing symptoms of back strain, followed by weakness in his left quadricep. Although initial testing
There are steps you can take now
that will help you protect your
nest-egg and also save you money
during your retirement years.
Consider permanent life insurance protection
While term life insurance is a good option at younger ages to cover temporary risks like a mortgage or to pay for children’s education, the mid-to-late career stage is a good time to start thinking about permanent life insurance as a key part of your estate plan. As the name implies, this type of insurance provides lifetime coverage.
If you carry term life insurance, you usually have the option to convert to lifetime permanent coverage without medical evidence at any time before you reach a certain age (e.g., 70). Rates are based on your age at the

Alberta Doctors’ Digest • January/February 2012 13
Now that we are living longer
than ever, and with constant new
life-saving medical advances,
studies show that we have a
significant likelihood of needing
extended care at some point.
for Amyotrophic Lateral Sclerosis was negative, he was eventually diagnosed with the disease.
As his Amyotrophic Lateral Sclerosis progressed, Dr. G. reluctantly cut back to working part-time and began using a wheelchair due to increasing weakness in his arms and legs. Eventually, he had to give up his practice entirely. In just three years since diagnosis, his condition had deteriorated to the point where he relied on in-home care for four hours per day, seven days per week, to help him with activities like bathing and dressing. The cost of this care was fully covered by his monthly long term care insurance benefit.
to qualify for coverage at older ages. This type of protection provides a lump sum benefit payout if you are diagnosed with one of the conditions covered under the plan.
As you age, your expenses for dental care, medication and vision care often increase. Extended health care and dental insurance helps reduce your out-of-pocket costs for these services, along with emergency medical care. For self-employed or incorporated physicians, premiums for these plans are tax-deductible. There is no maximum age to apply for coverage under the Alberta Medical Association’s plan (AMA Health Benefits Trust Fund) but an annual enrolment period applies.
Advice for your pre-planning needs
As an AMA member, you have access to a wide range of valuable solutions that will help you create an effective protection plan for your retirement years at an affordable cost.
For help finding the right insurance solutions for your needs, contact your non-commissioned insurance advisor at ADIUM Insurance Services:
Toll-free: 1.800.272.9680, ext. 692 Email: [email protected] Website: www.albertadoctors.org/AdiumInsurance/Index
ADIUM Insurance Services Inc. is a wholly owned subsidiary of the Alberta Medical Association. ADIUM administers the group Disability, Office Overhead Expense, Term Life, Critical Illness, Accidental Death & Dismemberment, AMA Health Benefits Trust Fund, Student Disability Insurance and PARA Disability and Life Insurance plans.
ADIUM also has access to individual insurance products to help meet special risk or other unique insurance requirements that members may have.
PHYSICIAN(S) REQUIRED FT/PT
MILLWOODS EDMONTON
Also locums required
Phone: Clinic Manager (780) 953-6733 Dr. Paul Arnold (780) 970-2070
ALL-WELLPRIMARY CARE CENTRES
Dr. G. is especially grateful for the way long term care insurance helped his wife. He hopes she will, at only age 51, have a long and healthy life ahead. He is relieved to know she will not have to compromise her retirement lifestyle because of costs related to his illness. But perhaps more importantly, he is thankful she can spend their remaining time together as his wife, not as his caregiver.
Other important health insurance solutions
If you don’t already have critical illness insurance, it is still possible
Alberta Doctors’ Digest • January/February 201214
In the law business, the concept of “know your client” is all the rage. The underlying premise is to avoid fraud or money-laundering
by ensuring full client details are available and are cross-referenced to the sources of money being deposited. A recent medical-legal decision out of Quebec, however, may give rise to a similar concept – “know your patient” – but for very different reasons.
The case involved a complaint heard by a Discipline Committee early in 2011. The facts are these: the complainant presented at the emergency ward of the hospital in November 2009 with respiratory difficulties. He was transferred to an isolation room (212), as it appeared that he was suffering from H1N1 symptoms. He was seen by Dr. L.
The next day, he was transferred from room 212 to room 215 and another patient was admitted to room 212. Over the course of the next three days, Dr. L. continued to visit room 212, not realizing that the complainant
Health Law update
Jonathan P. Rossall, QC, LLM
PArTnEr, MclEnnAn
roSS llP
Know your patient….had been transferred and that he was actually seeing the wrong patient.
The practice in the hospital at the time was to place each patient’s name above the bed along with a color-code to identify the treating physician. When a patient was moved, a nurse would make note of the transfer in the patient’s medical notes, the prescription notes and the nurse’s observation notes. This had all been performed for the complainant. The nurse was also responsible for changing the sign with the patient’s name above the bed.
that his patient was actually in room 215. Prior to discharge a week or so later, the patient filed a complaint. Not unexpectedly, after a thorough investigation, the Disciplinary Committee found that Dr. L. had been negligent by not using the available tools to ascertain the identity of the patient.
While at first blush this case of mistaken identity may appear to be an anomaly, it is likely not as rare as one might think. Physicians see many, many patients in a given day or week and not all of the names or faces are necessarily familiar. And, the very fact that the practices regarding patient identification had been put in place suggests that this accidental mis-identification has happened before.
Given the complexity of procedures and the pace at which medicine is practiced, many safeguards are built into the health care system to prevent errors such as missed or mixed medications, or surgeries on the wrong limbs. But no matter how many safeguards and fail-safes are in place, health care practitioners (including physicians) are still human and prone to occasional mistakes. “Know your patient,” or perhaps more appropriately “remember your patient,” might be a useful addition to the lexicon.
While at first blush this case of
mistaken identity may appear to
be an anomaly, it is likely not as
rare as one might think.
Notwithstanding that all these practices had been performed by the nursing staff, Dr. L. continued to write notes and prescriptions in the complainant’s chart over the course of the next three days. On November 12, 2009, after seeing Dr. L. enter room 212, a nurse informed him
Alberta Doctors’ Digest • January/February 2012 15
F E AT U r E
Think of the plight of a family in a rural community many kilometers from the nearest family physician. Scheduled appointments mean taking the day off work, packing up the car and kids just to get the basic health care most Albertans take for granted. Unfortunately, this scenario is not uncommon for many Albertans living in rural communities.
That’s why the Alberta Medical Association’s (AMA's) Section of Rural Medicine created the Tarrant Scholarship to encourage medical students interested in rural medicine to eventually set up practice in smaller communities.
The Tarrant Scholarship is awarded each fall by the Section of Rural Medicine to third-year medical students at the University of Alberta (U of A) and the University of Calgary (U of C).
Since its inception in 2004 the Tarrant Scholarship has awarded almost $200,000 to 22 medical students. It is one of Alberta’s largest unrestricted medical school undergraduate awards and provides a full year’s tuition to its recipients.
Tarrant Scholarship encourages students to practice in rural communities
The scholarship is named in honor of the late Dr. Michael Tarrant, a Calgary family physician. Dr. Tarrant championed rural medical undergraduate education and helped establish ongoing rural roots for future physicians. The scholarship is presented to students who have demonstrated an interest in, and dedication to, rural medical issues during their undergraduate years.
A medical student is eligible to apply for the 2012 scholarship if he or she is:
• Entering third-year medical school at the U of A or the U of C this fall.
• Interested in a career in rural medicine in Alberta.
• Is demonstrating an interest in and dedication to rural medical issues in undergraduate work.
The Tarrant Scholarship application form is available on the AMA’s website at www.albertadoctors.org. The application deadline is May 7.
TAKE ADVANTAGE OF THE NEW ALBERTA RULES.Since the first book was published in 2004, there have been many changes that have a direct impact on your Professional Corporation. New rules and regulations in Alberta have created even more opportunities for professionals to keep more of what they make.The new version of Professional Corporations – The Secret to Success is larger, more in depth, and is the foremost resource for successful professionals.
“While Ottawa belatedly rejigsthe retirement income system, professionals are building their own security with Professional
Corporations. Tim Paziuk’s updated Professional
Corporations shows how business owners and
self-employed professionals can build their own
financial independence.”–Jonathan Chevreau,
Financial Post columnist &author of Findependence Day.
To purchase the updated version of Professional Corporations – The Secret to Success, please call our toll free number 1-888-315-0058or visit our website at http://www.tpcfinancial.com
Alberta Doctors’ Digest • January/February 201216
A salary grid establishes the minimum and maximum compensation for each staff person in your practice. Setting up and then maintaining a compensation
grid is one of the most difficult challenges that physicians face in managing staff and their performance.
Salary grids may have different numbers of steps or levels (often three to five), but typically they should reflect the fact that employees will have varying degrees of competence: entry level, mid level and fully competent.
Annually, the grid will be adjusted for inflation (cost of living adjustment or COLA) and likely should be reviewed every three to four years to ensure it is still competitive within the local job market. The easiest way to determine inflation is through the Consumer Price Index for Alberta (www40.statcan.gc.ca/l01/cst01/cpis02a-eng.htm).
It can be difficult telling staff that, once an employee has reached the highest step on the grid and the maximum rate for the position is achieved, the only increases will be for cost of living. Providing the grid to employees for their positions, however, helps them to understand what their earning potential in their positions is over time.
The next challenge is appropriately placing staff on the grid and setting guidelines for how they will move through the compensation grid during their employment.
The first step to placing employees on the grid is to determine their level of competence in relation to those set out in their position profiles. Ideally, profiles will include the responsibilities of the positions and the expected level
Getting your staff
“on the grid”of behavior in the areas of teamwork, health care business knowledge, judgment and decision making, patient focus, organization and personal effectiveness.
Employees are assessed to determine the level they are functioning at in relation to the competencies in their profiles. A new employee without significant experience or education will likely be placed on the first step (entry level) of the grid, whereas a new employee with significant experience and education may start at the top of the grid (fully competent). It is important to keep in mind that the grid is not linked directly to the length of employment.
Annually, through the performance review process, each employee’s competencies and performance are reviewed. It is expected that new employees will have developed their skills and will be functioning at a higher competency level than when they were first hired. They may still have some additional development needs in some areas and if this is the case, they would move to the mid-level competency step. If they have not progressed significantly they would remain at the entry level step. Employees who are fully competent remain at that step.
Examples for a three-step grid follow:
1. New employee in the early developmental stages. Placed on step one of the grid at the beginning of his/her employment. Through the annual review process, it is determined that the employee has developed skills and is demonstrating competency in most areas. Move to step two on the grid.
2. New employee in the early developmental stages. Placed on step one of the grid at the beginning of his/her employment. Through the annual review process, it is determined that the employee has yet to develop skills
Mind Your Own Business
PMP Staff
Alberta Doctors’ Digest • January/February 2012 17
and is only beginning to develop competencies expected of the position. Remain at step one of the grid.
3. An existing employee who is at the mid-competency level and step two of the grid has developed his/her skills completely and demonstrated the expected competencies in all areas. Move to step three on the grid.
4. An existing employee who is fully competent and is at step three on the grid continues to utilize his/her skills and demonstrate expected competencies. Remain at step three.
It is usually the last example that causes difficulty for physicians and their staff. Physicians generally want to reward their employees for work well done while their employees appreciate and expect recognition for their good
work. Ensuring that employees understand the grid and its use will help alleviate these difficult discussions during their annual performance reviews.
Physicians wishing to reward length of service may consider a one-time length of service recognition payment for their employees at five-year intervals. This approach provides recognition for the dedication of the employee without altering the salary grid which focuses on performance.
The Practice Management Program is able to support primary care physicians, either within or pursuing a primary care network, in developing human resource systems for their practices, including position profiles, performance management systems and compensation grids. For assistance, please contact Linda Ertman ([email protected]).
CHOOSE MED ACCESS EMR TO MEET YOUR NEEDS TODAY AND TOMORROW
ISO 13485FM 572891
REQUEST A DEMONSTRATION
The only vendor with funding eligible EMR software in all 4 Western provinces & Ontario.
True web-based EMR, resulting in greater speed, accessibility and reliability.
Highly configurable with robust functionality.
Complete set of intelligent reporting tools to improve care & practice management.
Alberta Doctors’ Digest • January/February 201218
F E AT U r E
Zumba anyone?
Keeping active helps prevent seniors’ fallsWith arms waving, hips circling and the sound of belly-dancing scarves jingling, a group of seniors helped launch the fourth annual Finding Balance public awareness and education campaign to prevent falls in seniors. The dancers – several over 90 years of age – performed a very energetic Zumba fitness demonstration to show that they walk (or dance) the talk when it comes to keeping active.
“Keep active” is one of several key messages of the Finding Balance campaign co-sponsored by the Alberta Medical Association (AMA). These residents of the Touchmark at Wedgewood, where the November 1, 2011 Edmonton launch event was held, clearly showed that people of any age can remain active to maintain their strength and balance.
Finding Balance was first launched in 2008 as an annual November campaign to raise awareness about the serious nature of falls among older adults, and the simple things they can do to reduce their risk of falling. It was initially developed as a partnership between the Alberta Centre for Injury Control and Research (ACICR) and the AMA.
The program has been recognized as a model for practitioners in Alberta and across Canada by the Public Health Agency of Canada.
Four key messages round out the educational component of the campaign:
• Keep active – exercise for strength and balance.
• Check your medications – tell your doctor or pharmacist about all the medications you are taking.
• Watch your step – wherever you are.
• Speak up about dizziness – tell your doctor and take action.
Speakers at the Edmonton launch addressed each of these issues. Dr. Kimberley P. Kelly, a family physician and member of AMA’s Health Issues Council, represented the
AMA at the event, speaking about some things that may help to prevent dizziness and advising when it is important to talk to a physician.
In addition, ACICR Associate Director Kathy Belton talked about falls-related statistics (one-in-three seniors will fall each year); physiotherapists Greg Cutforth and Cindy Grand spoke about and demonstrated “everyday exercises”; and Jennifer Fernandes, ACICR Education Coordinator, talked a senior attendee through a demonstration of how to get up from a fall.
A similar Finding Balance event, held simultaneously at the Calgary Greater Forest Lawn +55 Centre, featured seniors who performed a skit about the dangers of falling, and the Mop ‘N Glow choir who sang a tongue-in-cheek song about what happens to you when you do fall.
Calgary orthopedic surgeon and Health Issues Council member Dr. Linda A. Mrkonjic represented the AMA at the Calgary event, where she delivered the message about dizziness.
The Finding Balance program provides a number of resources including flyers, posters, bookmarks and magnetic picture frames. All feature the program’s key messages. A number of focus groups were held with seniors in the fall of 2011 to gather their impressions of the materials. Their feedback helped to hone the messages and the look of the flyers and posters, to better differentiate and help each individual message stand out.
Resources are available for order (at no charge) by physicians, health practitioners and various facilities (e.g., libraries, seniors’ centers, lodges, aboriginal centers, multicultural centers, etc.). This year saw the highest number of orders to date. As well, flyers were distributed to 1,018 pharmacies to hand out with prescription orders.
Dr. Linda A. Mrkonjic addresses seniors at a Calgary event.

Alberta Doctors’ Digest • January/February 2012 19
The program has an online presence through its website (www.findingbalancealberta.ca), and also connects with a Facebook page and ads, and a Twitter account. Print advertisements were carried in selected rural Alberta newspapers and ethnic publications. A program highlight this year was a front-page story in the Edmonton Journal.
At the end of November, the fourth annual Finding Balance campaign officially wrapped up for another year, although
Edmonton Finding Balance launch — Dr. Kimberley P. Kelly.Touchmark at Wedgewood residents — Zumba demonstration.
INTERNATIONAL MEDICAL TOUR
AN EXPLORATION OF HEALTH CARE AND CULTURE IN CUBA
The tropical island of Cuba is a unique mix of diverse people, rich culture and old customs. Cuba’s health care system is also unique, and thrives despite limited resources.
SAIT Polytechnic’s School of Health and Public Safety is offering a unique professional development opportunity to explore health care in another culture. Join our International Medical Tour to Cuba, April 21-28, 2012, to gain rsthand knowledge of Cuban culture and health care, and get insight on best practices and health care options.
Save $400 when you register by February 29, 2012.
Early bird: $4,599Regular: $4,999
FOR MORE INFORMATION, CALL 403.284.7341 OR VISIT SAIT.CA/MEDICALTOUR
the program may update falls prevention messages during the icy months of winter.
The key Finding Balance sponsors this year include: ACICR, Government of Alberta, AMA and Physiotherapy Alberta – College & Association. Others include Bayshore Home Health, Alberta Blue Cross, Alberta Therapeutic Recreation Association, College & Association of Registered Nurses of Alberta (CARNA), media sponsor Global Edmonton and print sponsor McCallum Printing Group Inc.
Alberta Doctors’ Digest • January/February 201220
F E AT U r E
Introducing the Primary Care Alliance – a new representation structure for primary care
The Alberta Medical Association’s (AMA’s) primary care representative groups have reorganized to better serve the needs of their constituents and to better reflect the landscape of primary care in the province. During the Fall Representative Forum (September 23-24, 2011), the Section of General Practice (SGP) launched the Primary Care Alliance (PCA).
The purpose of the PCA is to:
• Increase coordination and information between primary care groups.
• Promote policy and direction alignment for all primary care physicians.
• Develop and support physician leadership.
Although the PCA will focus on primary care, it will also encourage appropriate linkages with specialists. Because of the importance of all of this work, the AMA is providing transitional funding for the first three years of PCA operations.
The PCA was created through the hard work of the General Practice Representation Governance Working Group, which includes representatives from the Section of General Practice, Section of Rural Medicine, Primary Care Network (PCN) Physician Leads Executive Committee and Alberta College of Family Physicians.
The Primary Care Alliance will be comprised of two different groups – the PCA Forum and PCA Board.
The Primary Care Alliance held its first two board meetings October 21 and December 14, 2011. Topics discussed included:
• Special interest groups – The board evaluated some identified special interest groups and will invite them to present issues to ensure representation of these groups and their issues.
• Strategic Clinical Networks – The board received an update from AMA senior staff on Strategic Clinical Networks. Alberta Health Services (AHS) is in the process of restructuring the Clinical Networks into Strategic Clinical Networks. More information will soon follow.
• Health Pathways in Alberta – The board reviewed a paper by Dr. D. Rod Elford, Medical Director, Health Link Alberta, AHS, about Clinical Pathways (a concept developed in New Zealand). The Clinical Pathways contain very detailed and practical information on how to manage dozens of the most common acute and chronic health problems that usually require general practitioners (GPs) to refer to specialists. GPs and specialists initiate the Clinical Pathways development
process and bring in other health professionals, etc., as required to complete it. The pathways are then made available online for easy and quick access. The project has received AHS support. The PCA Board will continue to monitor the status of this project.
• SGP Strategic Retreat priorities The retreat was held last November and key priorities were forwarded to the Primary Care Alliance for discussion at its December 2011 board meeting. The priorities are:
• Increase sections of General Practice and Rural Medicine membership through recruitment.
• Continue to provide input on family physician remuneration.
• Participate in family care clinics development and work with other allied health providers.
• Continue involvement in current and future Strategic Clinical Networks.
More information about Primary Care Alliance initiatives is available in Section News.
Alberta Doctors’ Digest • January/February 2012 21
PriMArY cArE AlliAncE ForUM
The Primary Care Alliance Forum will meet twice annually to:
• Set PCA’s strategic direction.
• Ensure alignment and coordination between primary care groups.
• Increase information sharing between primary care groups.
• Act as leadership for committees and members.
Membership includes:
• Four Section of General Practice representatives.
• Two Section of Rural Medicine representatives.
• Three PCN Physician Leads Executive representatives.
• One Alberta College of Family Physicians representative.
• Two Academic Family Medicine representatives. (University of Alberta and University of Calgary).
• Two residents (Edmonton and Calgary).
• Five Zone Advisory Forums members.
• Other organized primary care special interest groups (e.g., hospitalists).
PriMArY cArE AlliAncE BoArd
The Primary Care Alliance Board will meet four to six times (or as required) per year to:
• Conduct strategic planning.
• Ensure policy and direction are aligned for all primary care providers.
• Provide advice and direction to the constituents’ groups.
• Promote the economic stability of the primary care practitioner.
• Communicate with members and external stakeholder groups.
• Develop and support physician leadership.
Board members include:
• Section of General Practice president.
• Section of Rural Medicine president.
• PCN Physician Leads Executive Committee chair.
• Alberta College of Family Physicians president.
• Two members-at-large (elected from PCA Forum).
[email protected] • phone: 780.571.1505 • cell: 780.819.4301
www.nexstepgroup.ca
Want Better Business Organization?Want Increased Revenue?Want Improved Patient Care?
We provide streamlined patient care solutions by providing Offsite administrative services to physicians, medical clinics, specialists and dentists.
Pam Osatiuk, RNBScN President
go offsite!
Transcription • Alberta Health & Wellness InitiativesNew & Existing Business Models • Patient Coordination Insurance Coordination • Recruitment • Recall Lists
Offsite Medical Services

Alberta Doctors’ Digest • January/February 201222
F E AT U r E
Picture it: $5,000 assistance for additional training in a clinical area of recognized need in Alberta. If that fits your situation, apply for the TD Insurance Meloche Monnex/Alberta Medical Association (AMA) Scholarship by March 30.
Scholarship applicants must be seeking additional training in a clinical area of recognized need in Alberta, be an AMA member, plus be enrolled and accepted in a clinical program of at least three months’ duration in a recognized educational facility.
The proposed program must be supplementary to completion of a Royal College of Physicians and Surgeons of Canada or College of Family Physicians of Canada certification program, or the physician may be in an established practice and wishing supplemental training.
Scholarship recipients of the last three years were:
Calling for 2012 TD Insurance Meloche Monnex/AMA Scholarship applicants
• 2011 – Dr. Sayeh Zielke, Calgary (fellowship in Echocardiography and Adult Congenital Heart Disease).
• 2010 – Dr. Michael W. Aucoin, Calgary (working with the underserved).
• 2009 – Dr. Janette A. Hurley, Calgary (addressing the health needs of the underserved).
Visit the AMA website (www.albertadoctors.org) to see the names of recipients going back to 1991, when the first scholarship was awarded.
To request a 2012 scholarship application form, please contact Janice Meredith, Administrative Assistant, Public Affairs, AMA: [email protected], 780.482.2626, ext. 291, toll-free 1.800.272.9680, ext. 291 or visit the AMA website (www.albertadoctors.org).
Are you looking to lease or purchase a new or pre-owned vehicle?
– Factory incentive programs.– Top price paid for your trade. – All makes offered.
– No hassles.– No shopping dealership to dealership.– Delivery available to your hometown.
“Let my 40 years of Auto Experience and Fleet Connections work for you. I will save you time and provide a no pressure quote on any vehicle.”
David Baker spouse of Dr. Karen Bailey knows first hand that a physician’s time is valuable. He has helped many physicians in
Alberta obtain their vehicle of choice without any hassle.
Call: 1.888.311.3832 or 403.262.2222Email: [email protected]: www.southdeerfootsuzuki.comMANY REfERENCEs AVAilABlE
Alberta Doctors’ Digest • January/February 2012 23
Feedback: A powerful two-edged sword
Residents' Page
Dr. naomi J. Fridhandler
oBSTETricS And
GYnEcoloGY
rESidEnT
PhYSiciAn
Like most resident physicians, I spent the years prior to medical school in an educational system that tracked my performance based on examinations and marks. As such, transitioning into medical school involved quite the paradigm shift.
No longer does it matter whether I get an 83 versus a 90% – or a 97% on a multiple choice exam; it really has very little external validity when looking at the clinical world of medicine. Determining how well I am performing has become much more difficult and relies far more on self-evaluation. Feedback and in-training evaluation by preceptors is critical to this process, especially when judging my ability to provide effective care to patients.
“Feedback is a gift,” according to Hilary Delver of the University of Calgary Office of Faculty Assessment and Development. I completely agree with her. In fact, as a resident physician, I crave it.
When delivered properly, feedback lets me know what I am doing well and what I need to work on; it gives shape
and validity to my self-evaluation. A simple pat on the back or word of encouragement helps me get through a difficult call shift. A brief comment on my strengths or where I have improved motivates me and makes me excited to come to work the next day. Suggestions for improvement may sting at first, but they provide objectives for me to work on. I appreciate tips on how to improve. Resident physicians want to impress their preceptors, but they need to know how they can do better and be given the opportunity to show improvement.
Clinical clerks and resident physicians are early in their careers and are vulnerable to poorly considered feedback and evaluations. The negative impact may be profound and include long-lasting loss of confidence and emotional distress. Sadly, I have seen passionate and hardworking learners become very discouraged because of misdirected evaluations. The negative consequences do not stop at the resident physician; they impact colleagues, friends, families and, ultimately, patients.
As medical professionals, we are trained to move past initial emotional reactions and use logical reasoning, objectivity and compassion when working with our patients. This philosophy should also be applied to medical education. Effective preceptors take a moment to reflect and try to frame feedback in terms of performance rather than perceived qualities of the learner.
In emotionally charged situations, a “cooling-down” period allows for more objective assessment on all sides. Differences in personality that compromise interactions, outside stressors in the learner’s life that may be influencing performance, and the consequences of a negative evaluation need to be considered, especially if this evaluation is included in a learner’s permanent record.
Feedback is a powerful tool that can promote positive and meaningful change. Feedback can also stunt learning if misdirected. Preceptors of medical students and resident physicians are responsible for providing feedback that will motivate learners and not discourage them. Burnt-out learners risk becoming ineffective physicians, but motivated ones will change the future of our medical profession for the better.
When delivered properly,
feedback lets me know what I
am doing well and what I need
to work on; it gives shape and
validity to my self-evaluation.
In acknowledging the crucial role of feedback, I remain conscious of the damage it may cause when delivered poorly. It is easy to understand how a preceptor may become irritated or upset with a learner and respond with quick judgments. Unfortunately, such judgments can sometimes be directed at the learner rather than the learner’s performance.
Alberta Doctors’ Digest • January/February 201224
The music of Christmas and the holiday season has been consigned to the cloud for another year. Try to imagine the year-end festivities sans music. No Handel’s Messiah. No Muzak in the malls. No Kermit and Darth Vader duet of Auld Lang Syne. A succession of silent nights and days in late December would be as emotionally distressing for music lovers as the complete consumers’ Christmas would be without Black Friday or the Boxing Day frenzy. A bleak mid-winter indeed.
What is it about music that adds pleasure to our life, not simply during the holiday season but throughout the year? Music is an ubiquitous aural presence. We can hear and enjoy listening to music at weddings and funerals, births and BBQs, sporting events, in cars, cafes and airplanes, at the dentist, or just walking the sunny side of the street singing to ourselves or doing our variation of the ear-bud, urban two-step.
Loewy and Spingte3 (2011), in an issue of Music and Medicine, report:
Positron emission tomography (PET) imaging studies have illustrated that ‘‘intensely pleasurable’’ responses to music correlate with activity in the brain regions implicated in reward, emotion, or pain, including ventral striatum, dorsomedial mid-brain
The Power of Music(PAG or pedunculopontine tegmental nucleus), amygdala, orbitofrontal cortex, the anterior cingulate cortex, and insula (p. 70).
We know that music can contribute mightily to our emotional well-being and to that of our patients. But, what is it that makes much (but not all) music a recurring pleasurable activity of daily life – in effect, a resource for daily living?
PFSP Perspectives
Vincent M. Hanlon, MD
PFSP ASSESSMEnT
PhYSiciAn
musical experience. In the Laboratory for Musical Perception, Cognition, and Expertise at McGill University, Levitin (2006) researches how the human brain responds to music, and how diverse, interconnected parts of our brain recognize, organize and create music. He also draws on extensive knowledge acquired during his former career as music producer. He is familiar with a host of musical genres – skate punk, baroque, bebop, death metal, fado – and refers to many of them as he shows “… how music affects our brains, our minds, our thoughts and our spirit” (p. 14).
To heighten the pleasure associated with Levitin’s book, read it with access to the iTunes store so you can listen to some of the music he discusses. I especially liked the section where he traces the evolutionary development of the reptilian brain, emotional processing in the amygdala and the neuroanatomical links that impel humans to dance to the music. He presents a compelling thesis to explain why your normally restrained brother-in-law, under the influence of a song like Dancing Queen, will get up at the family wedding and startle everyone with a Jacksonian sequence of loose-limbed dance moves.
Loewy and Aldridge (2009), in the lead editorial of the premier issue of Music and Medicine,2 describe a burgeoning interest among biomedical and social scientists in the interconnectedness of music and medicine:
In the past decade, we have witnessed a surge in the number of studies that have integrated the
We know that music can
contribute mightily to our
emotional well-being and to that
of our patients.
Daniel Levitin1 (2006), a neuroscientist and former record producer and session musician, addresses this and related questions in his book, This is Your Brain on Music: The Science of a Human Obsession. Your brain on music, he says, quoting Francis Crick, “is all about connections” (p. 192). He echoes Loewy and Spingte in his conclusion that: “Musical activity involves nearly every region of the brain that we know about, and nearly every neural subsystem” (p. 85-86).
Levitin begins the book by defining music and reviewing what the various musical elements – melody, rhythm, tempo, timbre, harmony and loudness – contribute to the

Alberta Doctors’ Digest • January/February 2012 25
science of medicine with the art of music, and the art of medicine with the science of music. Indeed, we will be attempting to integrate two pillars of modern culture, music and medicine. How these relate dynamically to each other in practice remains to be seen (p. 5-7).
Neurologist Oliver Sacks has written extensively about music and medicine. Sacks, like Levitin, is an amateur musicologist. In his book, Musicophilia,4 Sacks presents many case studies illustrating the significance music plays in many of his patients’ lives, often as one unusual facet in a common neurological illness.
In a story that will appeal to the would-be performer in some of us, Sacks (2007) recounts how one of his patients, an orthopedic surgeon, was struck by lightning in a phone booth. In the aftermath of his near-death and out-of-body experiences, the man develops a passion for listening to and composing music. At the age of 42 he becomes an accomplished pianist all the while continuing his surgical practice. Although unable to come up with a neuropathological basis for his patient’s new-found musicophilia, Sacks is left marvelling at the “lucky strike” (p. 17).
I still hear in my mind’s ear the baritone voice of a singing surgeon as we made early morning rounds when I was a family practice resident. That particular morning he did a credible a cappella cover of the Hall & Oates’ classic 1980s pop song, Maneater. It was only on the second morning I, but not he, was struck by the irony of the lyrics, “Watch out boys, she’ll chew you up, she’s a maneater,” as we moved from bed to bed, checking on the patients, most of whom were recovering from GI cancer surgery. Irony apart, the tune lightened his step while its upbeat energy radiated over our patients.
That musical memory is in contrast to one of a middle-aged man with angina that I once saw in the emergency department. Lack of hospital beds kept him in the emergency department for what turned out to be the final night of his life. Imagine the ambient noises and speech sounds that are part of the emergency soundscape. Not what I would request for my last night on earth. I expect we’ll soon see, and perhaps should encourage, more and more patients choosing their preferred musical accompaniments for extended visits to hospitals and clinics.
Music can be a form of sustenance and celebration, a vehicle for relaxation or a powerful source of energy, and a doorway to deeper emotional meaning for all of us. The stages of a life provide shifting opportunities to expand our enjoyment of music. In these days of rapid technological innovation, how and where we listen to music, and how we collect and share it, are parts of a fascinating human preoccupation.
Some readers may recall a collection of essays by pathologist Dr. Lewis Thomas (1983) entitled Late Night Thoughts on Listening to Mahler’s Ninth Symphony5. In the title essay he describes in elegiac style how his relationship with that piece of orchestral music changed during the years of the cold war, as mankind confronted the threat of nuclear annihilation:
I cannot listen to Mahler’s Ninth Symphony with anything like the old melancholy mixed with the high pleasure I used to take from this music (p. 164).
Former high pleasure now remembered with a sense of loss and a touch of melancholy describe my new relationship with Canada’s national broadcaster in the aftermath of major programming changes a few years ago. A friend helped me get over some of my auditory disappointment by introducing me to what has become one of my favorite iPhone apps: TuneIn Radio™. The 50,000 stations available feature diverse musical genres, broadcast from Antarctica to Azerbaijan, and are hosted in the language of your choice.
The tune lightened his step
while its upbeat energy radiated
over our patients.
We are all musical experts.
We may not be accomplished
players or singers but we are
expert listeners.
While reading Sacks, one begins to see ways physicians can tap the power of music as a force for healing and the restoration of well-being in their own and their patients’ lives.
Daniel Levitin makes the point that we are all musical experts. We may not be accomplished players or singers but we are expert listeners – most of us have listened to thousands of hours of music. Perhaps it’s time for some of us to join a choir, dust off the djembe, or sit down again at the keyboard. Whether as listeners or performers, some salutary musical moments await us in 2012 – even without the lightning bolt.
References
1. Levitin, D.J. (2006). This is Your Brain on Music: The Science of a Human Obsession. New York: Penguin.
2. Loewy, J.V., & Aldridge, D. (2009). Prelude to music and medicine. Music and Medicine, 1(1), 5-8. http://mmd.sagepub.com
3. Loewy, J.V., & Spingte, R. (2011). Music soothes the savage breast. Music and Medicine, 3(2), 69-71. http://mmd.sagepub.com
4. Sacks, O. (2007). Musicophilia. New York: Alfred A. Knopf.
5. Thomas, L. (1983). Late Night Thoughts on Listening to Mahler’s Ninth Symphony. New York: Viking.

Alberta Doctors’ Digest • January/February 201226
J. Barrie McCombs, MD, FCFP
This unique website has been designed by the University of Ottawa to help physicians cope with the stresses of their professional and personal lives. It provides a useful
supplement to the services provided by the Alberta Medical Association’s (AMA’s) Physician and Family Support Program. I wish these services had been available 25 years ago when a full-time family practice plus emergency shifts took a toll on my personal life. Since the new year is a time for reflection, I encourage every AMA member to visit this website for a “lifestyle checkup.”
Welcome page
www.ephysicianhealth.com
The initial welcome page contains a video that describes how to use the website. On later visits, the orange navigation button at the bottom of the screen will take you directly to the program menu page. Use these navigation buttons, rather than those of your browser program. You can return to the welcome page by clicking on the ePhysicianHealth logo on any page.
Web-footed MD
Program menu page
There are currently 14 modules available. A pop-up icon draws attention to the tiny help buttons at the bottom of the screen. Each module is organized under the headings of Focus, Reality, Strategy, Next Steps and Resources. The “download e-Book version” tab on each Resource page provides a useful summary in PDF format that can be downloaded to a computer or e-Book reader for reading or printing.
Videos
Depending on the speed of your computer and Internet connection, the Flash videos may be interrupted while the computer downloads the next section (a process called “buffering”). A pop-up message will sometimes appear giving you the option to download the entire video to your computer, which may make it easier to view without interruption.
Carpe diem - resilient physicians
This 24-minute video is an overview of physician resiliency. It was the most prone to the interruptions mentioned above.
Substance use disorders
It is estimated that 10-15% of health care professionals will abuse drugs or alcohol at some time in their career.
Weight, nutrition and fitness
As physicians, we often preach sermons on these subjects, but do we practice them ourselves? My partner, Carole, is a great cook, so I made sure that I reviewed the section about maintaining a healthy weight. Since I’ve retired, I’ve taken up square dancing, which is a great “low impact” form of exercise.
Depression, burnout and suicide
Will you recognize the signs and symptoms in yourself and your colleagues?
Anxiety
Be sure to read the table that lists the characteristics that make one a caring physician but can also lead to difficulties in our personal lives.
Resilience
This section uses the acronym “BASICS” (Body, Affect, Social, Intellectual, Community and Spiritual) as a way of looking at lifestyles. I enjoyed the section on “community,” since my local square dance club has become my new-found community.
Relationship with self
“Compassion fatigue” is an important topic discussed here. I now realize this was the main reason I gave up office practice back in the 1980s.
ePhysicianHealth
Alberta Doctors’ Digest • January/February 2012 27
Your comments and suggestions
are welcome.
Please contact me:
T 403.289.4227
Boundaries
The “slippery slope” is a unique way of discussing doctor-patient boundaries. I wonder if it is still okay to accept small gifts from patients? Those home-baked cookies always helped staff morale in our office.
Primary care
Must we “stop thinking like a doctor” in order to become a patient? My own family physician has also retired, so I will have to get used to being treated by someone from a different generation.
Disruptive behavior (five modules)
Dealing with disruptive behavior is discussed from the perspective of
physician leaders, practicing physicians, residents, medical students and health care teams. The goal is to prevent such behavior from interfering with quality health care delivery. I enjoyed the discussions of myths and what actually constitutes disruptive behavior.
About ePhysicianHealth
http://about.ephysicianhealth.com
The “Why Visit ePhysicianHealth” video on this related page provides a shorter introduction than the one on the main page.
The bottom line
I would recommend this website to any physician who is interested in maintaining a healthy lifestyle.
Please call PFSP toll-free at 1.877.SOS.4MDS (1.877.767.4637),
24 hours a day, 7 days a week, 365 days a year.
Physician and Family Support Program
Alberta Doctors’ Digest • January/February 201228
Below MarketLease Rates!
PurchaseOpportunities Available
new
-Medical Zoning approved-Abundant Parking-Custom Built Space-Available Immediately-Excellent Location-Low operating costs
DOUGLASDALE SOUTH HEALTH CENTRE
11420 27 Street SE
Calgary’s newestmedical facility!

Alberta Doctors’ Digest • January/February 2012 29
The plump Mexican Customs Officer stamped our boat’s papers. She looked at our passports and shrugged her
shoulders – no “touristico” forms. “Talvez… Cabo San Lucas” she said.
She sat under a tent at a table near the band where skimpily clad women holding bottles of beer danced with elderly males. We bought beers and offered her one. “Gracias, Senor. Mas tarde,” she said.
She smiled gracefully as photographs were taken. This was Bahia Santa Maria, our second anchorage in Mexico. The party went on for a couple of hours in the afternoon sun. It was the ultimate, painless Customs and Immigration, one that might rival the entrance to paradise.
The contrast returning via Houston was stark: “Stand behind the red line, buddy. Wait till you’re called.” I shuffled back – and was then immediately called: “Next.” I gave the humble smile, looking him full in the eyes, then down, signaling submission.
“Only in Mexico three days, huh? Whadaya doin’ takin’ a Canadian boat down thar? What line a business ya in?” he said, scowling at his computer.
The Ship Surgeon’s Chest
In A Different Vein
Alexander H.G. Paterson, MB ChB, MD, FRCP, FACP
co-EdiTor
The sail from San Diego on the annual race to Cabo San Lucas is not an arduous ocean passage – you can anchor and rest on the way and one is rarely out of sight of land, but these dust-and-rust fishing villages don’t have much.
In contrast, the sail from Vancouver to California can be a rough affair and a serious medical event prompted us to review the contents of the “surgeon’s chest” because next year we sail from Mexico to the Marquesas in the South Seas and beyond.
reflect the specialty of the physician choosing them. Hence the catheter recommendation must have come originally from a sailing urologist. Pediatric anesthetists with veterinary backgrounds like ketamine and lots of morphine; orthopods load the boat with plaster bandages and fibreglass casts which are useful for repairing the hull when the boat hits a reef; surgeons bring an assortment of scalpels which can also be used in the galley. I tested Peter’s theory on a gastroenterologist friend. He insisted that a generous supply of Pepto-Bismol would be essential.
As an oncologist, I believe nausea and vomiting (common sea-sickness) to be the major ailment on a voyage. That ominous feeling of increased salivation, too frequent swallowing, a bit of yawning, the fluttering sensitivity in the lower chest and upper abdomen and the unpleasant knowledge that you are no longer interested in dinner – these must be tackled promptly. But it can be hard because early diagnosis in an all male crew requires keen observation. Men do not like to admit to anything, including feeling queasy, seeing it as an expression of weakness, like admitting to light-headedness at
My friend and fellow sailing doc,
Peter Farran, believes that the
contents of a boat’s medical
chest reflect the specialty of the
physician choosing them.
One of the fun things the medical officer may have to do on an ocean passage is to pass a urinary catheter on an older crew member reporting inability to pass urine. Depending on how helpful the crew member has been to you, you may also need a local anesthetic gel. I’ve never had to do this at sea, but I do look forward to it. For this reason we carry a French-16 Foley catheter in the boat’s medical kit.
My friend and fellow sailing doc, Peter Farran, believes that the contents of a boat’s medical chest A warm welcome at Mexican customs. ( supplied by Dr. Paterson)
Alberta Doctors’ Digest • January/February 201230
Getting an honest medical
history from the crew is just as
hard. Assume they are all lying
until proven otherwise.
the sight of blood. It is not a sign of weakness, but often treatment must be given only after an acute attack has occurred.
Getting an honest medical history from the crew is just as hard. Assume they are all lying until proven otherwise.
yawn, as the Australians say. Then all cried Ruth.
Sudden severe sea-sickness can make the will to live recede into irrelevance. The idea of dying has no sting and in fact may be temporarily welcomed. Decision making becomes warped with chronic nausea and fatigue.
Our boat, Caledonia II, is a famous boat. You may have read about her in the papers in October 2006. She was abandoned in the Atlantic Ocean during a severe storm between Bermuda and Boston. The crew had become nauseated and exhausted. They had not accessed the medical kit – no physician was on board. An emergency was declared and the US Coast Guard took them off – ironically just as the storm was abating.
OK – we all know you never abandon a boat unless it’s sinking but when you have an exhausted nauseated crew, good decision making is difficult. If the crew had been properly treated for sea-sickness I doubt this abandonment would have occurred.
We carry intramuscular metoclopramide for acute vomiting. Don’t mess around; draw up 20 milligrams and stab it into the buttock – or 10 milligrams on each side if you want. The victim will be grateful for the pain which momentarily relieves the mind of the intensity of the nausea.You can then use an oral agent: meclizine, prochlorperazine or ondansetron. We also carry scopolamine pills and compounded triple suppositories of dimenhydrinate (Gravol) prochlorperazine (Stemetil) and metoclopramide (Maxeran) but for some reason they have never been used and remain lying in the chest as a threat that things can always get worse. A bag of saline, IV needles and lines for unrelenting vomiting completes the over-enthusiastically stocked N&V section of the kit. Oh, and loperamide (Imodium) of course, and laxatives.
An assortment of scalpels can also be useful in the galley. ( supplied by Dr. Paterson)
Getting an honest medical history from the crew is hard. Assume they are all lying until proven otherwise. ( supplied by Dr. Paterson)
Caledonia II is a famous boat. ( supplied by Dr. Paterson)
The most effective preventative approach to impending sea-sickness is to stick on a “transderm scop” patch containing 1.5 milligrams scopolamine on the skin overlying the mastoid process and post the victim on deck in a light breeze where he or she can see the horizon. The scopolamine blocks cholinergic stimuli from the vestibular nuclei to higher centres.
Once vomiting has started, it is harder to control. I once had the experience 150 nautical miles off Vancouver Island while on the wheel at 3 a.m. in a sudden gale. The crew attended to the urgent reefing of the sails. As we rocked up and down, all four became nauseated, and after we had reefed to a handkerchief, in the dim cockpit lights they looked like ghosts with their heads in their hands.
The skipper (who had not shown for this emergency) appeared in the companionway, lurched into the cockpit, threw himself into the scuppers and chucked up over the side. No wasting of time attaching himself to the safety jack-lines. He just “cried Ruth” and had a tartan
Alberta Doctors’ Digest • January/February 2012 31
Some carry a wrist band with a metal disc which you rub over the anterior of the wrist. This may work as a placebo for preventing nausea in light seas but when you’re heeling over at 40 degrees with the side-rails in the water and rocking up and down and wondering why in hell’s name you ever came out here, I would not waste time rubbing a disc of metal on your wrist.
We have thermometers, splints, assorted bandages, gauze, syringes, needles, packets of gastrolyte, eye-patches (useful as fancy pirate dress-up gear), an oro-pharyngeal airway, a pack of plaster of Paris, a suture kit (artery forceps, scissors, 3 and 4 silk and absorbable sutures, and rubber gloves) and local anesthetic (0.1% xylocaine) for serious cuts.
Those adhesive strips that come in different sizes (“Steri-strips”) are great for smaller cuts. Povidone-iodine (Betadene) for maximum antisepsis, sterility, pain and discomfort are important – and may also be used for acne in a younger crew member.
My ship-mate, Peter, also says – and this is important: “There are some things that can’t wait for a helicopter – I always carry a suture with a straight needle for arterial bleeds from lacerations, Ventolin for asthma attacks and injectable adrenaline for anaphylaxis.”
So we have those in the Surgeon’s Chest.
The ship surgeon’s duties may also include dispatching and filleting the tuna or mahi-mahi caught off the back. For dispatching, I prefer a whack with the “priest” and a teaspoon of cheap gin down the gills but more brutish crew prefer pulling out the gills and spilling blood all over the cockpit. Delegate the filleting, if possible.
Skippers often do like to take charge of the cooking, largely because it gets them out of doing the unpleasant task of washing up. So when they burn their hand on the stove we have Flamazine 1% (silver sulfadiazine 1%) and non-stick Telfa dressings of all sizes to cover it. A sizeable burn gets anyone off washing up duties.
best not mentioned to Customs agents unless you have all the papers in order. We have morphine and tramadol, a narcotic which, if discovered in your bag in Customs, can be explained away with a stunned expression: “I did not realize, Officer, that this was a banned substance.”
You may be able to argue that it is an anti-inflammatory, something not worthy of his attention. The name, tramadol, is helpful in that way, sounding innocuous like “panadol” which in the UK is the name for Tylenol.
At sea everyone believes themselves to be a budding medico and has much advice to give, free and without the requirement of knowledge, experience or responsibility. Do not argue back. Say nothing. Perhaps nod wisely. The waffling will fade quickly.
At our Mexican Customs and Immigration party, one young woman passed out in a heap in the sand holding an empty beer bottle. An excitable crowd gathered round. But the diagnosis here was obvious and need not concern the ship’s surgeon. Management of this kind of ailment can reliably be left to the surgeon’s mates, of whom there are many at sea.
The ship surgeon’s duties may
also include dispatching and
filleting the tuna or mahi-mahi
caught off the back.
We have antibiotics: ciprofloxacin, cephalosporin and doxycycline – the doxy useful for malaria, gastroenteritis and venereal disease. The last of these ailments is mentioned only for traditional nautical reasons and rarely occurs (except in the real Navy), but as the boy scouts say: be prepared. And a well-stocked chest should take all eventualities into account.
Pain control is a tricky issue since bringing narcotics over borders is
Ann DawrantAnn Dawrant
Websitewww.anndawrant.com
• Consistentlyintop5%ofEdmontonrealtors
• PrestigiousRE/MAXPlatinumClub
• 26yearsasasuccessfulresidentialrealtorspecializinginwestandsouthwestEdmonton
• BornandraisedinBuenosAiresandhaslivedinEdmontonsince1967
• BilingualinEnglishandSpanish
RE/MAXRealEstateCentre
(780) 438-7000
“Please call me to
experience the dedicated,
knowledgeable, and
caring service that I provide
to all my clients.”

Alberta Doctors’ Digest • January/February 201232
EDMONTON AB
Dr. Lal is looking for a full-time physician to join his busy family practice at 3504A 137 Avenue. Clareview Medical Clinic is in a residential area with high-patient volume. The complete clinic was recently renovated and is next to a pharmacy. This is a fee-for-service opportunity offering a 70/30 split. Additional starting incentives are available such as guaranteed monthly income. Hospital privileges preferred.
Office hours are 9 a.m. to 6 p.m., Monday to Friday and 9 a.m. to 4 p.m. on Saturday. Extended hours are a possibility; walk-ins welcome.
Contact: Dave GalonT 306.536.4642 orAileen JangT 780.232.9297
FORT MACLEOD AB
The Fort Macleod Family Medical Clinic requires an enthusiastic general practitioner or family physician to join our small, but vibrant, clinic located within the community’s health center. It is supported by numerous allied health care professionals as well as periodic visits from a general surgeon, internist, mental health worker and geriatrician. We receive the bulk of our earnings through a clinical Alternate Relationship Plan (ARP), liberating us from the encumbrances of the fee-for-service model allowing us to focus our time and energy toward the provision of superb primary care. Our participation in the Chinook Primary Care Network finances further initiatives toward this end.
In addition to clinic work, a full-time equivalent (FTE) will also work on-call, one-in-five in the emergency room and make bimonthly visits to the long-term care facility. No obstetrics or acute inpatient duties. A 1.0 FTE will work 40 hours per week, receive six weeks paid vacation and can expect to earn, through the ARP and other revenue streams,
sees 50-75 patients per day. This is a full-service clinic with extended hours with a family practice and walk-in component. We feature full computerization with labs and X-ray online. This is a fully supported practice with RN/LPN, reception, booking clerk, transcription and computer support on site. Complete administration and billing services provided with transcription and/or paperless option. High income potential with a large practice base and patient volume provide a superior opportunity. Hours worked and holidays easily accommodated as per individual needs.
Contact: Denise DrakeT [email protected]
CALGARY AB
Med+Stop Medical Clinics Ltd. has immediate openings for part-time physicians in our four Calgary locations. Our family practice medical centres offer pleasant working conditions in well-equipped modern facilities, high income, low overhead, no investment, no administrative burdens and a quality of lifestyle not available in most medical practices.
Contact: Marion BarrettMed+Stop Medical Clinics Ltd.290-5255 Richmond Rd SWCalgary AB T3E 7C4T 403.240.1752F [email protected]
EDMONTON AB
Two positions available at the West End Medical Clinic for part- or full-time general practitioners. Walk-in and family practice clinic. Physicians will enjoy no hospital on-call, paperless clinic and friendly staff. Clinic is in a busy area of west Edmonton and has four physician offices and eight examination rooms.
Contact: Dr. GaasT [email protected]
Physician wanted
CALGARY AB
Well-established family physician office in northwest Calgary is seeking a third physician. Our spacious doctor-owned clinic offers several attractive features including low overhead (approximately $6,700 per month), friendly and stable staff, free parking for patients, two large examination rooms and a large central office per doctor. We are in a great location in a well-established community (Banff Trail) with easy access to the bus and C-Train. We are associated with a supportive and progressive Calgary Foothills Primary Care Network with several in-office multidisciplinary team members including a pharmacist, chronic disease nurse, asthma educator, diabetes educator, dietician and behavioral health consultant who work in the clinic downstairs.
We have recently implemented Practice Solutions electronic medical records. We are looking for a physician who shares our passion for exceptional patient care. Our clinic is a friendly, supportive environment that nurtures personal growth and development.
Email resume to: [email protected]
CALGARY AB
Westbrook Medical Clinic is recruiting part- and full-time physicians for a busy clinic in southwest Calgary. The clinic is computerized but willing to accommodate doctors who are computer shy, 70/30 split.
Contact: Dr. LotaT 403.246.0877 (office) [email protected]
CALGARY AB
Properties Medical Clinic has an opportunity for a full-time physician in family practice. The position would be replacing a current physician who
Classified Advertisements

Alberta Doctors’ Digest • January/February 2012 33
Physician and/or locum wanted
SHERWOOD PARK AB
Synergy Medical Clinic, Women’s Wellness Centre and Medical Plus are looking to recruit part-time, full-time and locum general practitioners and specialists to join our state-of-the-art facility. We are excited to be part of the brand-new Synergy Wellness Centre in Sherwood Park, home to 18 health-related clinics with on-site services including radiology, laboratory, physiotherapy, dermatology, psychology, dentistry, sleep laboratory and cardio-pulmonary clinic. We offer a competitive fee split, fantastic staff, full electronic medical records and flexible hours.
Contact: [email protected] www.synergymedical.ca
SLAVE LAKE AB
Slave Lake Family Medical Clinic is urgently looking for a full-time family physician to work clinic and on-call hospital schedule. Paperless clinic, Netcare available. Urgently need locums to work Monday to Friday, 8:30 a.m. to 4:30 p.m.
Contact: Daniel PayneT 780.849.2860 (office)780.849.4009 (home)[email protected]
Space available
CALGARY AB
Office space available in the spring for a third family physician to join two established family doctors. Two full-time examination rooms per doctor available in recently renovated office. Very pleasant and conscientious staff. Central location with underground parking, pharmacy, physiotherapy, X-ray, cafe and restaurant in the building. Very reasonable overhead, stable and very desirable environment.
Contact: [email protected]
[email protected] orDr. Maureen McCall, RecruitmentT 403.346.2057F [email protected]
SHERWOOD PARK AB
Alberta Health Services is inviting applications from family physicians interested in providing after-hours coverage at Health First Strathcona.
Health First Strathcona is an urgent-care centre and has unique hours between 5:30 p.m. and 1 a.m. daily, year round. Care is provided in a multidisciplinary team environment. Clinical presentations range from uncomplicated cases to acute illness and sport injuries. Laboratory and X-ray are available for the full shift. Applicants must hold an MD or equivalent, be eligible for a license to practice medicine in Alberta and have completed a fellowship in family medicine. Current ACLS is also a requirement.
Applications will begin to be considered as of March 15, however, they will be reviewed continuously thereafter until all shifts are filled.
Interested physicians are invited to send their resumes to:
Contact: Dr. Lorraine Mann HosfordMedical Lead Health [email protected]
SLAVE LAKE AB
Congenial, extremely busy practice urgently requires a full-time family physician with interest in obstetrics. Good on-call schedule.
Contact: Merylin Hodge T 780.805.0746 orDr. John KeavenyT 780.849.4155F [email protected]
approximately $375,000 per year with very reasonable overhead expenses. No buy-in required.
Fort Macleod is a scenic rural community 25 minutes west of Lethbridge with a full spectrum of schools, recreational facilities, shopping, churches, etc. Fort Macleod is a wonderful family-centered community and a tremendous area in which to work and raise a family.
Contact: Dr. Robert SimpsonFort Macleod Family Medical ClinicPO Box 1239Fort Macleod AB T0L 0Z0T 403.553.0066, ext. 125F [email protected]
RED DEER AB
Associate Medical Group (AMG) is looking to recruit part- and/or full-time physicians to join a well-established, busy family practice with a long-term presence in Red Deer. Red Deer, population 90,000, offers many recreational and educational opportunities. Laboratory and X-ray services and hospital are in close proximity. AMG offers excellent staff, supportive colleagues and full electronic medical records. An interest in obstetrics is welcome. Good earning potential and the blend of practice can be tailored to your interests.
Contact: Diane Klassen, ManagerT 403.346.2057F [email protected]
RED DEER AB
Associate Medical Group walk-in requires part- and/or full-time physician(s). The clinic is near a pharmacy and has good access to laboratory and X-ray services, and the hospital. Fully integrated electronic health records, excellent support team, supportive colleagues and working closely with the Red Deer Primary Care Network. Good potential for excellent remuneration.
Contact: Diane Klassen, ManagerT 403.346.2057F 403.347.2989
Alberta Doctors’ Digest • January/February 201234
November 17-December 1 Focus: Rheumatology and palliative care Ship: Celebrity Equinox
MEDITERRANEAN CME CRUISEMay 18-30 Focus: Diabetes management update Ship: Celebrity Silhouette
July 22-August 3 Focus: Aesthetic medicine Ship: Celebrity Solstice
August 11-18 Focus: Hospitalist medicine Ship: Mariner of the Seas
BALTIC AND RUSSIA May 20-June 1 Focus: Cognitive behavioral therapy Ship: Celebrity Constellation
ALASKA CME CRUISEJuly 15-22 Focus: Women’s health and endocrinology Ship: Celebrity Century
RUSSIA RIVER CME CRUISEAugust 10-22 Focus: Cardiology, dermatology and oncology Ship: Uniworld Victoria
BRITISH ISLESSeptember 6-16 Focus: Internal medicine Ship: Regent Seven Seas Voyager
CANADA AND NEW ENGLANDSeptember 29-October 6 Focus: Psychiatry and the law Ship: Veendam
ISTANBUL TO LUXOR CME CRUISEOctober 31-November 14 Focus: Cardiology and lipidology Ship: Regent Seven Seas Voyager
Contact: Sea Courses Cruises TF 1.888.647.7327 [email protected] www.seacourses.com
CME AT SEA
CARIBBEAN CME CRUISEFebruary 26-March 4 CPA’s 15th International CPD Conference Celebrity Cruises – Celebrity Solstice
southwest prestigious Terwillegar/Riverbend neighborhoods. Space includes six rooms, waiting/reception area, built-in high-speed networking, phone and security system. Main floor is handicap accessible, ample parking and offered at below-market rate. Excellent tenant mix with pharmacy and allied professionals nearby.
Contact: Brian HunterRe/Max Real Estate CentreT 780.438.7000
HIGH RIVER AB
Approximately 2,000 sq. ft. available in an updated facility in High River, three-minute drive to the High River Hospital and 25-minute drive to Calgary. Clinic currently has a full-time obstetrician/gynecologist and is suitable for up-to-three family doctors or alternatively a specialist. Reasonable rent or will provide complete practice support with staff.
Contact: David Baker T [email protected]
Space wanted
CALGARY AB
Two well-established family doctors are looking to possibly relocate in order to share office space and expenses. Currently in central-southwest with lease expiring in April.
Contact: [email protected]
Courses
SEA COURSES CME CRUISES
Companion cruises FREE.
CARIBBEAN CME CRUISEMarch 11-18 Focus: Women’s health, dermatology and infectious diseases Ship: Freedom of the Seas
March 18-25 Focus: Endocrinology and cardiology Ship: Freedom of the Seas
CALGARY AB
Evergreen Professional Medical Building, 4015 17 Avenue SE, has space for lease. Building has existing long-term tenants, family practice/walk-in medical centre, pharmacy, dental clinic, denture clinic, physiotherapy/rehabilitation, Bank of Montreal and ATM centre. Building is well-maintained/newly renovated, minutes from Peter Lougheed Hospital, Alberta laboratory services centre and imaging centre. Minutes from downtown, easy airport access, excellent parking ratio and high-traffic 17 Avenue SE with terrific street signage.
Contact:T 403.606.1411 [email protected]
CALGARY AB
New medical office space for lease or purchase. Close to South Health Campus, the development will consist of six office/medical condos covering 24,000 sq. ft. on three floors. Constructed of concrete, steel and stucco and is zoned for commercial office and medical usage. Excellent access to Macleod Trail, Highway 22X, Deerfoot Trail and just minutes from the new South Calgary Hospital. Turn-key interior packages available at competitive pricing.
Contact: Bart HribarCity Core CommercialT [email protected]
EDMONTON AB
Medical practice space to share or sublet in a prime location office building in south Edmonton. Large area (3,000 sq. ft.), professionally designed with four treatment/examination rooms. Five-year lease with option to renew. Excellent opportunity for general practitioners and specialists.
Contact: T 780.938.2581
EDMONTON AB
Medical/professional office space available for lease in Edmonton’s
Alberta Doctors’ Digest • January/February 2012 35
Canada Post Publications Mail Agreement No. 40070054Return Undeliverable Canadian Addresses to
Alberta Medical Association, 12230 106 Ave NW, Edmonton AB T5N 3Z1
Display or ClassifieD aDs
To Place or renew, conTacT:
Daphne C. Andrychuk
Communications Assistant, Public Affairs
Alberta Medical Association
T 780.482.2626, ext. 275
TF 1.800.272.9680, ext. 275
F 780.482.5445
Seven-nights, round trip Ft. Lauderdale Up to 18 CPD credits Companion travels FREE
Contact:TF 1.888.523.3732 www.cruise-connections.com/cme
CARIBBEAN CME CRUISEMarch 11-18 Pain Management Update 2012 Celebrity Cruises – Celebrity Solstice Seven-nights, round trip Ft. Lauderdale Up to 18 CME hours Companion travels FREE
Contact: TF 1.888.523.3732www.cmeatsea.org
ALASKA CME CRUISEJuly 22-29 SOGC presents ALARM at SEA Celebrity Cruises – Celebrity Century Seven-nights, round trip Vancouver 16 RCPSC credits and up to 20 CFPC credits Companion travels FREE
Contact:TF 1.888.523.3732www.cruise-connections.com/cme
ALASKA CME CRUISEAugust 18-25 Internal Medicine Update 2012 Holland America Line – Ms Zuiderdam Seven-nights, round trip Vancouver Up to 18 CME hours Companion travels FREE
Contact: TF 1.888.523.3732www.cmeatsea.org
MEDITERRANEAN CME CRUISESeptember 8-20 Diabetes and Obesity Update 2012 Celebrity Cruises – Celebrity Solstice 12-nights, round trip Barcelona Up to 28 CME hours Companion travels FREE
Contact: TF 1.888.523.3732www.cmeatsea.org
ROMANTIC EUROPE CME CRUISE
September 19-October 1 Women’s Health Update 2012 Celebrity Cruises – Celebrity
Constellation 12-nights, round trip Southampton, England Up to 28 CME hours Companion travels FREE
Contact: TF 1.888.523.3732www.cmeatsea.org
TAHITI CME CRUISEJanuary 23-February 2, 2013 Cardiology Update 2013 Paul Gauguin Cruises 11-nights, Tahiti – round trip Papeete Up to 28 CME hours Companion travels and flies free
Contact: TF 1.888.523.3732www.cmeatsea.org
For sale
EDMONTON AB
For sale by owner, 3,000 sq. ft., condominium townhouse in Westridge, near the Misericordia Community Hospital. Asking $649,000.
Contact: 780.487.1834
EDMONTON AB
Two-storey house for sale in Grandview Heights, near the University of Alberta and southside health centres. The house has five bedrooms, 3.5 bathrooms, fireplace, atrium, living room, dining room, den, detached double garage, large lot and south-facing backyard (lots of sun).
Contact:[email protected]
Services
ACCOUNTING AND CONSULTING SERVICES EDMONTON AB
Independent consultant, specializing in managing medical and dental professional accounts, to incorporating PCs, full accounting, including payroll and taxes, using own computer and
software. Pick up and drop off for Edmonton and area, other convenient options for rest of Alberta.
Contact: N. Ali Amiri, MBAFinancial and Management ConsultantSeek Value Inc.T 780.909.0900F [email protected]
DOCUDAVIT MEDICAL SOLUTIONS
Retiring, moving or closing your family or general practice, physician’s estate? DOCUdavit Medical Solutions provides free storage for your paper or electronic patient records with no hidden costs. We also provide great rates for closing specialists.
Contact: Sid Soil DOCUdavit Solutions TF 1.888.781.9083, ext. [email protected]
RECORD STORAGE & RETRIEVAL SERVICES INC.
RSRS is Canada’s leader in medical records storage and scanning services since 1997. Free services for closing primary care practices. Physician-managed and compliant.
TF 1.888.563.3732, ext. 221www.recordsolutions.ca

![Hey, hey, hey! Welcome, welcome, everyone! · Hey, hey, hey! Welcome, welcome, everyone! • It’s me, your friend, [Host’s name], with you, and I am so glad you guys are here](https://img.pdfslide.us/doc/110x75/5fbe51e50602d61619707374/hey-hey-hey-welcome-welcome-everyone-hey-hey-hey-welcome-welcome-everyone.jpg)