Embed Size (px)
Citation preview

Poster Design & Printing by Genigraphics® - 800.790.4001
Herpes Zoster of the Larynx
John M. Carter, MD1; David Cai, BS1; Brian A. Moore, MD, FACS2 1Tulane University School of Medicine, 2Ochsner Clinic Foundation
Introduction Discussion Discussion
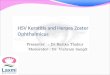
Figure 1 . Flexible fiberoptic laryngoscopy demonstrating vesicular lesions of the hemilarynx, a
paralyzed right vocal fold and pooling of secretions.
Abstract
Varicella Zoster is a systemic
disease process that rarely
occurs in the larynx. A 97
year old gentleman
encountered in the clinic and
then the hospital setting
presented with severe
dysphagia, odynophagia and
hoarseness. This case report
includes endoscopic images
of the larynx that reveal
mucosal vesicles of the
hemilarynx, pooling of
secretions and a unilateral
vocal cord paralysis. Varicella
zoster antibody titers for IGG
were positive. The gentleman
improved with systemic
antiviral medication, with
marked improvement of both
subjective and objective
findings.
Herpes zoster of the larynx may present in a variety of
ways. The patient may have one or more cranial nerve
palsies, painful mucosal vesicles, or pain without visible
herpetic lesions. Cranial nerves IX, X, and XI are most
often involved but CN VII and VIII may be affected in
more extensive cases.1 Patients may or may not have
concurrent skin involvement.
Varicella zoster in the head and neck affects various
cranial nerves in a locoregional distribution. The larynx
is supplied by the vagus nerve, namely the superior
laryngeal and recurrent laryngeal nerves. The superior
laryngeal nerve provides sensory innervation to the
supraglottic structures and vocal folds through its
internal branch, while the external branch provides
motor innervation to the cricothyroid muscle. The
recurrent laryngeal nerve innervates the remainder of
the motor function of the laryngeal muscles and sensory
innervation for the subglottis.7
Mucosal lesions of zoster of the head and neck are not
typically limited to one nerve distribution and do not
necessarily stem from one ganglion.1,2 In our case
disease was confined to the distribution of the superior
and recurrent branches of cranial nerve X. Lin et al.
described the only 11 previously reported cases of
varicella zoster infection that presented as cranial nerve
palsies with mucosal lesions that lacked skin
manifestations or evidence of herpes zoster oticus.
Four of these cases involved only the hemilarynx and
cranial nerve X, as in our presentation.1
Laboratory testing is supplemental to clinical
presentation and endoscopic findings. Useful tests
are varicella antibodies (IGM and IGG) and PCR
testing for viral genome detection. IGG may appear
as soon as 4 days after mucosal lesions, whereas
IGM typically rises 8-10 days afterwards.1,9 The
patient in this case was seropositive for varicella
antibody IGG, while IGM antibodies were negative.
It has been shown that not all cases present with a
positive IGM. The sensitivity of serum antibody IGM
ranges from 50-84%.1,6 A two-fold increase in IGG
has also been shown to be more useful in the
detection of herpes zoster reactivation than IGM.8
When the diagnosis in question, PCR has been
shown to have a sensitivity that approaches 100%.5
However, obtaining a bedside cotton swab for PCR
diagnosis may not be easily achievable or
comfortable for the patient.
Evidence for the treatment of these lesions is
lacking and largely based on treatment of herpes
zoster oticus. Despite definitive evidence, one can
justify attempting medical therapy with anti-viral
medications and steroids with the intention of
hastening the course of vesicle resolution and
perhaps return of nerve function.9 As in this case,
supportive measures such as gastrostomy tubes
may be required.
Herpes zoster is a rare but uncommon cause of
neuropathy in the head and neck and should be
considered whenever vesicular mucosal lesions are
present. Diagnosis is largely established through
clinical exam and confirmed through laboratory
testing. Treatment with anti-viral medications and
steroids lacks convincing evidence but may be used
to hasten recovery.
Varicella Zoster is a common systemic disease that
rarely affects the larynx.1-4 The virus is known to
establish a latent infection in the spinal cord or
cranial nerve ganglia that reactivates secondary to
various stressors. It has often been described in
head and neck as Ramsay Hunt Syndrome type II,
stemming from the geniculate ganglion. Patients
suffering from herpes zoster present with vesicular
eruptions, acute pain and nerve paralysis in the
distribution of the affected nerves. Herpes zoster of
the larynx is uncommon and often presents with
multiple cranial neuropathies.1-3 Furthermore, its
vesicular appearance may be confused with a
laryngeal neoplasm.
Herpes zoster of the larynx may manifest with
unilateral vocal fold paralysis, mucosal vesicles of
the hemilarynx, dysphagia and odynophagia. The
diagnosis of this disease process is largely clinical
and may be supplemented by viral antibody assays
and polymerase chain reaction (PCR).1,3,5,6
1. Lin YY. Kao CH. Wang CH. Varicella zoster virus infection of the pharynx
and larynx with multiple cranial neuropathies. Laryngoscope 2011;121:1627-
30.
2. Pinto JA, Pinto HC, Ramalho Jda R. Laryngeal herpes: a case report. J
Voice 2002;16:560–563.
3. Chitose S-I, Umeno H, Hamakawa S, Nakashima T, Shoji H. Unilateral
associated laryngeal paralysis due to varicella-zoster virus: virus antibody
testing and videofluoroscopic findings. J Laryngol Otol 2008;122:170-6.
4. Watelet JB, Evrard AS, Lawson G, et al. Herpes zoster laryngitis: case
report and serological profile. Eur Arch Otorhinolaryngol 2007;264:505–7.
5. Beards G, Graham C, Pillay D. Investigation of vesicular rashes for HSV
and VZV by PCR. J Med Virol 1998;54(3):155-7.
6. Van Loon AM, van der Logt JT, Heessen FW, Heeren MC, Zoll J. Antibody-
capture enzyme-linked immunosorbent assays that use enzymelabelled
antigen for detection of virus-specific immunoglobulin M, A and G in patients
with varicella or herpes zoster. Epidemiol Infect 1992;108:165–174.
7. Yoshida Y, Tanaka Y, Hirano M, Nakashima T. Sensory innervation of the
pharynx and larynx. Am J Med 2000;108:51S–61S.
8. Kawaguchi K. Inamura H. Abe Y. Koshu H. Takashita E. Muraki Y.
Matsuzaki Y. Nishimura H. Ishikawa H. Fukao A. Hongo S. Aoyagi M.
Reactivation of herpes simplex virus type 1 and varicella-zoster virus and
therapeutic effects of combination therapy with prednisolone and valacyclovir
in patients with Bell's palsy. Laryngoscope 2007;117:147-56.
9. Uscategui T. Doree C. Chamberlain IJ. Burton MJ. Antiviral therapy for
Ramsay Hunt Syndrome (herpes zoster oticus with facial palsy) in adults
Cochrane Database Syst Rev. 2008 Oct 8;(4):CD006851.
Conclusions
References
John M. Carter, MD
Tulane University School of Medicine
Email: [email protected]
Phone: 504-988-5454
Contact
Figure 2. Flexible fiberoptic laryngoscopy
demonstrating complete resolution of lesions.
A 97 year old male presented with one week of
worsening dysphagia, odynophagia and a mild
hoarseness. The patient was still able to tolerate a
normal diet. During flexible fiberoptic laryngoscopy
the patient did not have a vocal fold paralysis but
did have a small ulcer of the right aryepiglottic fold.
Two days later his dysphagia worsened and he was
no longer able to tolerate liquids.
Esophagogastroduodenoscopy was performed and
the only abnormality was a Schatzski ring at the
gastroesophageal junction. Secondary to his
severe dysphagia and a modified barium swallow
study that showed aspiration and hypopharyngeal
pooling of contrast, a gastrostomy tube was placed.
Contrast enhanced computed tomography of the
neck did not reveal any abnormality. The following
day flexible fiberoptic laryngoscopy was repeated,
revealing ulcerations of the right hemilarynx, pooling
of secretions and a complete right vocal fold
paralysis (Figure 1). The left hemilarynx was
unaffected. Laboratory testing was significant for
Varicella zoster IGG antibody titers that were five
times normal limits, 5.06 (NL= 0.0-0.9). Varicella
IGM antibody testing was negative.
The patient was started on intravenous valacyclovir
and prednisone. The following day his subjective
dysphagia began to improve. Laryngoscopy
revealed a reduction in the quality of the erythema
and ulcerations. Finally, two weeks after treatment,
the patient had a complete resolution of the vesicles
(Figure 2). The previously paralyzed right cord
demonstrated improved, but not yet normal mobility.
Case Presentation