Embed Size (px)
Citation preview

10/20/2015
1
South Carolina ChapterAmerican College of Physicians Scientific
Meeting 2015:Inpatient Management of Diabetes
Kathie L. Hermayer, MD, MS, FACE
Professor of Medicine
Division of Endocrinology, Diabetes and Medical Genetics
Medical University of South Carolina
October 30, 2015
Disclosure Verification for:
Name: Kathie L. Hermayer, MD
The presenter listed above:
___ Does not have any significant financial relationships to disclose
_X_ Has disclosed the following relationships:
NovoNordisk
_X Research Grants __Speakers Bureau Patent holder
__Consultant for fee
__Stock/Ownership Employment Partnership
__Advisory Committee/Board ___Other
_X_ Has disclosed this activity will not include discussion ofunapproved/investigational uses of products or devices
__ Has disclosed this activity will include discussion of unapproved/investigational uses of products or devices
Was this activity Supported by an educational grant or received in‐kind support?
__ Yes Name of Company: _X No
Learning Objectives
1. Recognize the pathophysiological changes of patients with stress hyperglycemia and diabetes in the hospital.
2. Discuss several studies which relate to the implications of hyperglycemia in the hospital regarding critically ill and medical‐surgical patients.
3. Discuss the current blood glucose guidelines for critically ill and medical‐surgical patients in the hospital.

10/20/2015
2
Hospital Cost of Diabetes in USA
• Total estimated cost of diagnosed diabetes in 2012 is
• $245 billion• $176 billion in direct medical costs• $69 billion in reduced productivity
• Components of medical expenditures
• Hospital inpatient care (43%)• Prescription meds to Rx complications of DM (18%)
• Antidiabetic agents and diabetes supplies (12%)• Physician office visits (9%)• Nursing/residential facility stays (8%)
• 41% increase from previous estimate of $174 billion (in 2007 dollars)
ADA, Diabetes Care. 2013. 36 (4): 1033‐1046.
Stress Hyperglycemia Exacerbates Illness
5
Stress Hormonescortisol, epinephrine Glucose Production
Lipolysis
FFAs
FFAs
+
Glucose Uptake
Glucose Fatty Acids
Hemodynamic
insult
Electrolyte losses
Oxidative stress
Myocardial injury
Hypercoagulability
Altered immunity
Wound healing
Inflammation
Endothelial
function
Illness
Clement S, et al. Diabetes Care. 27:553–591, 2004.
Hyperglycemia and Poor Hospital Outcome
Metabolic stress response
stress hormones and peptides
Glucose
InsulinImmune dysfunction
Infection dissemination
Cellular injury/apoptosisInflammation
Tissue damageAltered tissue wound repair
Prolonged hospital stayDisability / Death
FFA Ketones Lactate
Reactive O2 species
Transcription factors
Secondary mediators
Clement S, et al. Diabetes Care. 27:553–591, 2004.

10/20/2015
3
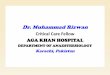
Insulin Requirements in Health and Illness
0
20
40
60
80
100
120
140
Correction
Nutritional
Prandial
Basal
Relative Proportion of
Insulin Requirement
(%)* *Estimations for illustrative purposes: requirements may vary widely.
Clement S, et al. Diabetes Care. 27:553–591, 2004.
Illness-Related
Healthy Sick/Eating Sick/NPO
Critically Ill Patients
Mortality Rate (%
)
Mean Glucose Value (mg/dL)N=1826 ICU patients.Krinsley JS. Mayo Clin Proc. 2003;78:1471‐1478.
0
5
10
15
20
25
30
35
40
45
80‐99 100‐119120‐139140‐159160‐179180‐199200‐249250‐299 >3000
5
10
15
20
25
30
35
40
45
0
5
10
15
20
25
30
35
40
45
Hyperglycemia and Mortalityin the Medical Intensive Care Unit
9
9.6%
42.5%
Diabetes present 22.4% population
~2x~3x
~4x
Note: modest increase BG after ICU admissionwas associated with substantial increase in hospital mortality

10/20/2015
4
Reference: Mean BG 100‐110 mg/dL
Reference: Mean BG 100‐110 mg/dL
Kosiborod M, et al. Circulation 2008:117:1018.
Mean Glucose & In‐Hospital MortalityIn 16,871 Patients with Acute MI
Mean Glucose & In‐Hospital MortalityIn 16,871 Patients with Acute MI
Intensive Insulin Therapy in Critically Ill Surgical Patients: The Leuven Study
Randomized controlled trial: 1,548 pts admitted to a surgical ICU. Pts were assigned to receive either:
• Conventional therapy: IV insulin if BG > 215 mg/dL•Target BG levels: 180‐200 mg/dL
•Mean daily BG: 153 mg/dL
• Intensive therapy: IV insulin if BG > 110 mg/dL
•Target BG levels : 80‐110 mg/dL
•Mean daily BG: 103 mg/dL
Van‐Den Berge et al, NEJM 345:1359, 2001
0 50
Prolonged (> 14 d) ICU Stay
Dialysis
Prolonged (>14 d) ventilation
Prolonged (>10 d) antibiotics
Bacteremia
Mortality 42%
41%
Intensive Insulin Therapy in Critically Ill Patients
*
*
*
*
*
*
* P < 0.01
Van‐Den Berge et al, NEJM 345:1359, 2001 Relative Risk reduction (%)
46
36%
38%
28%

10/20/2015
5
Survival Increased due to IIT (including
non diabetic patients) for Patients with a BG goal
of 80‐110 mg/dL who remained in ICU > 5 days
Van den Berghe. NEJM. 2001; 345: 1359‐1367
ICU Hospital floor
IIT reduced in‐hospital mortality by 34%
Intensive Insulin Therapy: Normoglycemia in Intensive Care Evaluation‐Survival Using Glucose Algorithm Regulation (NICE‐SUGAR) 2009
• Randomized, controlled trial in Australia, New Zealand, Canada, US
• 6104 adult medical and surgical patients admitted to the ICU
• Intensive– IV insulin started if BS > 108: goal 81‐108• Conventional– IV insulin started only if BS > 180: goal 144‐180
• 20% of patients were diabetic
• Primary endpoint: all‐cause 90‐day mortality
The NICE‐SUGAR Study Investigators. NEJM. 2009;360:1283‐97
Intensive Insulin Therapy: NICE‐SUGAR (2009)
• Intensive group• Actual glucose: 115 +/‐ 18 mg/dL
• Patients with BS < 40: 6.8%
• Conventional group• Actual glucose: 144 +/‐ 23 mg/dL
• Patients with BS < 40: 0.5%
The Nice‐Sugar Study Investigators. NEJM. 2009; 360: 1283‐1297

10/20/2015
6
Intensive Insulin Therapy: NICE‐SUGAR (2009)
The Nice‐Sugar Study Investigators. NEJM. 2009; 360: 1283‐1297
Mortality:Intensive: n=829 (27.5%)Conventional: n=751 (24.9%)P=0.03
Intensive Insulin Therapy: NICE‐SUGAR (2009)
• Discussion:• “In this large, international, randomized trial, we found that
intensive glucose control increased mortality among adults in the ICU: a blood glucose target of 180 mg/dL or less resulted in lower mortality than did a target of 81 to 108 mg/dL.”
The Nice‐Sugar Study Investigators. NEJM. 2009; 360: 1283‐1297
Why were the results of the Leuven SICU not reproduced?
• Single center vs multicenter studies
• Variability in duration of hyperglycemia before the start of the insulin protocol
• Variability in the type of insulin protocol
• Parenteral hyperalimentation the rule in Leuven study and enteral nutrition the rule in NICE SUGAR

10/20/2015
7
Pooled Meta‐analysis of 26 trials:Relative Risk of Death with Intensive Insulin Therapy
Griesdale DE, et al. CMAJ. 2009;180:821‐827.
The pooled relativerisk of death with IIT was 0.93 comparedwith conventional therapy(95% CI 0.83‐1.04).
Griesdale DE, et al. CMAJ. 2009;180:821‐827.
Severe Hypoglycemia in ICU Is More Likely With Intensive Insulin Therapy Than Conventional Glycemic Control: A Meta‐analysis
Overall severe hypoglycemia
RR 5.99(4.47‐8.03)
14 trials
Summary of Most Current Professional Societies’ Guidelines for Glycemic Control
Qaseem A., et. Al. Am. J. Med. Quality. 2014. 29 (2): 95‐98.Evans AS, et. Al. Minerva Endocrinologica. 2014; 39: 261‐273Standards Medical Care. Diabetes Care. 2015. 38 (Suppl 1): S80‐S85.

10/20/2015
8
Point of Care Testing Blood Glucose in Critical Illness
Factors to Consider When Using Devices in ICU Glucose Measurement
• Accuracy
• Speed of results
• Cost per test
• Sample volumes
Huong, T, et al. Journal of Diabetes Science and Technology. 2013 7(2): 489‐499. Hermayer, et. Al. Current Diabetes Reports, 2015; 15:10
Arterial, Capillary or Venous Blood
• Arterial blood has higher glucose levels compared with venous• 5‐10 mg/dL higher than capillary and venous concentrations
Huong, T, et al. Journal of Diabetes Science and Technology. 2013 7(2): 489‐499. Hermayer, et. Al. Current Diabetes Reports, 2015; 15:10

10/20/2015
9
Patient Conditions that Increase Risk of Errors
• CKD results in greater risk of hypoglycemia and anemia
• Hct <20% (may falsely raise BG in POC BG meters that do not detect Hct)
• End‐stage liver disease and malnutrition add to glycemic instability
• Sepsis heightens risk of hypoglycemia
Hermayer, Loftley, Reddy, Narla, Epps, Zhu. Current Diabetes Reports. 2015; 15:10.www.nursingcriticalcare.com. 2015. Accessed 6/30/15.
Inferences and Limitations of POC Devices: Clinical
• Interference from endogenous substances• Triglycerides, bilirubin, uric acid
• Conditions: Dehydration, hypoxia, DKA/HHS, hypotension, shock, capillary hypo‐perfusion, heart failure, finger edema
• Hematocrit outside range: ~ <10% or > 60%
• Interference from other sugars: maltose‐containing infusions• Glucose dehydrogenase pyrroloquinoline quinone (GDH‐PQQ) reagents
Hermayer, Loftley, Reddy, Narla, Epps, Zhu. Current Diabetes Reports. 2015; 15:10.www.nursingcriticalcare.com. 2015. Accessed 6/30/15.
Point of Care Devices
• International Organization for Standardization guideline (ISO 15197, 2003)
• BG > 75 mg/dL, 95% need to be within + 20% of the “reference” value (lab analyzed BG)
• BG < 75 mg/dL, 95% need to be within + 15 mg/dL• 1 out of 20 tests may have poor accuracy
• meter will be approved
Huong, T, et al. Journal of Diabetes Science and Technology. 2013 7(2): 489‐499. Hermayer, et. Al. Current Diabetes Reports, 2015; 15:10www.nursingcriticalcare.com. 2015. Accessed 6/30/15

10/20/2015
10
Point of Care Devices
• International Organization for Standardization guideline: 2014 FDA Draft• BG > 70 mg/dL, 99% need to be within + 10% of the “reference” value (lab analyzed BG)
• The other 1% must not exceed + 20%
• BG < 70 mg/dL, 99% need to be within + 7 mg/dL• The other 1% cannot exceed + 15 mg/dL
www.nursingcriticalcare.com. 2015. Accessed 6/30/15.
FDA Draft Recommendations for Hospital POC BG Meters
www.nursingcriticalcare.com. 2015. Accessed 6/30/15.
Wired vs Wireless POC Glucose Meters
Hermayer, Loftley, Reddy, Narla, Epps, Zhu. Current Diabetes Reports. 2015; 15:10.

10/20/2015
11
Non‐Critically Ill Patient Population
Glycemic Targets in Non‐Critical Care Setting
1. Premeal BG target of <140 mg/dl (7.8 mmol/L) and random BG <180 mg/dl (10 mmol/L) for the majority of patients.
2. Glycemic targets be modified according to clinical status.
• ‐ Patients with terminal illness, a higher target range
(BG <180‐200 mg/dl) may be reasonable.
3. For avoidance of hypoglycemia, diabetic therapy be reassessed when BG<100 mg/dl (5.5 mmol/L).
Umpierrez et al. J Clin Endocrinol Metabol. 97(1):16‐38, 2012
American College of Physicians recommended a BG target < 200 mg/dl (11.1 mmol/L), Ann Intern Med. 2012
Use of Oral Diabetes Agents in Hospitalized Patients
• 3 primary categories of oral agents:• Secretagogues: sulfonylureas and meglitinides
• Long action and predisposition to hypoglycemia
• Biguanides• Lactic acidosis (rare), however hospitalized pts at risk for hypoxia, hypoperfusion and renal insufficieny
• Side effects: nausea, diarrhea and decreased appetite
• Thiazolidinediones• Increase intravascular volume, concern for CHF and hemodynamic changes
• OHA have significant limitations for inpatient use
• OHA provide little flexibility for titration • Insulin when used properly may have many advantages in the hospital setting
Clement et al. Diabetes Care. 2004; 27: 553‐591

10/20/2015
12
DPP‐4 Therapy in Hospitalized Patients
Study Type: Multicenter, prospective, open‐label randomized clinical trial
Patient Population: Patients with T2D admitted to general medicine and surgery services at 3 hospitals: Emory University, Grady, and University of Michigan
Treatment Groups* Group 1. Sitagliptin once daily (n=30)Group 2. Sitagliptin plus glargine insulin once daily (n=30) Group 3. Basal bolus regimen with glargine once daily
and lispro before meals (n=30)
* All groups received supplemental doses of lispro for BG > 140 mg/dl before meals
Umpierrez et al. Diabetes Care. 2013 Nov;36(11):3430-5.
Randomization
Mean Daily BG During Treatment
Umpierrez et al. Diabetes Care. 2013 Nov;36(11):3430‐5.
Mean BG before Meals and at Bedtime during Treatment
Data is mean ± SE
P=0.22 P=0.15 P=0.52 P=0.57

10/20/2015
13
Randomization Blood Glucose (<180 mg/dl and >180 mg/dl) and Mean Daily Glucose
Concentration
Mean Daily Blood Glucose (mg/dL)
p= 0.91
p= 0.08
Umpierrez et al. Diabetes Care. 2013 Nov;36(11):3430‐5.
Conclusions
• Treatment with sitagliptin alone or in combination with basal insulin is safe and effective for the management of hyperglycemia in general medicine and surgery patients with T2DM.
Umpierrez GE, et. Al. Diabetes Care. 2013. 36: 3430‐3435.
Exenatide for Hyperglycemia in CICU
• Prospective, single‐center, open‐label, nonrandomized pilot study
• 40 patients admitted to the CICU with BG 140‐400 mg/dL
• All patients received IV exenatide as a bolus followed by a fixed dose infusion for up to 48 hours
• Exenatide effectiveness benchmarked to two historical insulin infusion cohorts, one (INT) with BG target 90‐119 mg/dL (n=84) and the other (MOD) with a target of 100‐140 mg/dL (n=71)
Abuannadi M, et. Al., Endocrine Practice. 2013. 19 (1): 81‐90.

10/20/2015
14
Median Glucose Values over Time
Target glucose levels were 100‐140 mg/dL for both the exenatide and modified control (MOD) arms, and 90‐119 mg/dL for the intensive control group (INT)
Abuannadi M, et. Al. Endocrine Practice. 2013. 19 (1): 81‐90.
Conclusions
• Steady state glucose values were similar between the exenatide(132 mg/dL) and the MOD groups (127 mg/dL), but lower in the INT group (105 mg/dL).
• Median time to steady state was 2.0 hrs in the exenatide group compared to 12.0 hours in the MOD group and 3.0 hours in the INT group.
• No episodes of severe hypoglycemia (<50 mg/dL) occurred in patients who received exenatide.
• Nausea was reported by 16 patients and vomiting by 2 patients.
• Summary: IV exenatide is effective in lowering glucose levels in CICU patients, but its use may be limited by nausea.
Abuannadi M, et. Al. Endocrine Practice. 2013. 19 (1): 81‐90.
Treatment Groups:
Insulin glargine once daily + supplemental insulin glulisine (n=65) N= 130
Sliding scale regular insulin four-times daily (n=65)
Study Type: Prospective, randomized, open‐label trial
Patient Population: 130 subjects with DM2 Oral hypoglycemic agents or diet therapy, insulin naive
Study Sites: Grady Memorial Hospital, AtlantaJackson Memorial Hospital, Miami
Randomized Basal Bolus versus Sliding Scale Regular Insulin Therapy in Patients with Type 2 Diabetes (RABBIT‐2 Trial)
Umpierrez et al, Diabetes Care. 30:2181–2186, 2007

10/20/2015
15
Rabbit 2 Trial: Changes in Glucose Levels with Basal‐Bolus vs. Sliding Scale Insulin
Umpierrez GE, et al. Diabetes Care. 2007;30(9):2181‐2186.
Days of Therapy
BG
, mg/
dL
100
120
140
160
180
200
220
240
Admit 1
Sliding‐scale
Basal‐bolus
bP<.05.
aa a
b bb
b
2 3 4 5 6 7 8 9 10
aP<.05.
• Sliding scale regular insulin (SSRI) was given 4 times daily • Basal‐bolus regimen: glargine was given once daily; glulisine was given before meals.
0.4 U/kg/d x BG between 140‐200 mg/dL
0.5 U/kg/d x BG between 201‐400 mg/dL
Basal–Bolus Insulin Regimen inNon‐critically Ill Patients
Rabbit‐2: Conclusion
• Basal/bolus insulin regimen with glargine once daily and glulisine before meals is a better insulin regimen than SSRI in the management of type 2 diabetics in the non‐ICU setting
• SSRI as a single insulin regimen should not be used for the management of patients with type 2 diabetes
Umpierrez et al. Diabetes Care. 30:2181–2186, 2007.

10/20/2015
16
• Study Type: Multi‐center, prospective, open‐label randomized clinical trial
• Patient Population: Patients with known T2DM admitted to general surgery services
• Study Sites: Grady Memorial Hospital, Veterans Affairs Medical Center and Emory University Hospital, Atlanta, GA
• Treatment Groups:
– Group 1: basal bolus regimen (n=104)
– Group 2: sliding scale regular insulin (n= 107)
Rabbit Surgery (Randomized Study of Basal Bolus Insulin Therapy in the Inpatient Management of Patients with T2DM Undergoing General Surgery):
Research Design and Methods
Umpierrez, et. Al. Rabbit Surgery. Diabetes Care. 2011; 34: 256‐261.
Duration of Treatment (days)
Blo
od G
luco
se (
mg/
dl)
120
140
160
180
200
220
SSRIBasal Bolus
* p: <0.001† p: 0.01ŧ p: 0.02
*
*
††
ŧ
ŧ
Randomi-zation
1 2 3 4 5 6 7 8 9
Glucose Levels During Basal Bolus and SSI Therapy
Postoperative Complications
P=0.003
P=NS
P=0.05 P=0.10
P=0.24
Glargine+Glulisine
Sliding Scale Insulin
Umpierrez et al. Diabetes Care. 34 (2):1–6, 2011.
* Composite of hospital complications: wound infection, pneumonia, respiratory failure, acute renal failure, and bacteremia.

10/20/2015
17
DEAN Trial: Changes in Mean Daily Blood Glucose Concentration
BG
, mg/
dL
Duration of Therapy, d
Data are means SEM.
Detemir + aspart
NPH + regular
Basal-bolus regimen: detemir was given once daily; aspart was given before meals.NPH/regular regimen: NPH and regular insulin were given twice daily, two thirds in AM, one third in PM.
Umpierrez GE, et al. J Clin Endocrinol Metab. 2009;94(2):564‐569.
P=NS
100
120
140
160
180
200
220
240
Pre-RxBG
0 1 2 3 4 5 6-10
NPH/Regular BG < 40 mg/dl: 1.6% BG < 60 mg/dl: 25.4%
Detemir/Aspart BG < 40 mg/dl: 4.5% BG < 40 mg/dl: 32.8%
DEAN Trial: Hypoglycemia
Emory University, Atlanta, GAMedical University of South Carolina, Charleston, SCTulane University, New Orleans, LA
Basal Plus Trial:Basal + Correction vs. Basal Bolus
Basal plus supplementsStarting glargine*: 0.25 units/kg Correction with glulisinefor BG >140 mg/dl per sliding scale
Basal Bolus Regimen
Starting TDD*: 0.5 U/kg
Glargine: 0.25 U/kg
Glulisine: 0.25 U/kg before meals
Correction with glulisinefor BG >140 mg/dl per sliding scale
* Reduce TDD to 0.15 U/kg in patients ≥70 yrs and/or serum creatinine ≥ 2.0 mg/dL
* Reduce TDD to 0.3 U/kg in patients ≥70 yrs and/or serum creatinine ≥ 2.0 mg/dL
Umpierrez et al. Diabetes Care. 2013 Aug;36(8): 2169‐74.

10/20/2015
18
Basal‐PLUS vs Basal Bolus: 375 Medical & Surgical Non‐ICU Patients
Patients treated with diet, oral agents or with low‐dose insulin ≤ 0.4 U/Kg/Day
Basal Plus:glargine once daily0.25 U/kg plus glulisine supplements
Basal Bolus:TDD: 0.5 U/kg/dGlargine 50%glulisine 50%
Umpierrez et al. Diabetes Care. 2013 Aug;36(8): 2169‐74.
A1C < 7%
Re‐start outpatient treatment regimen
(OAD and/or insulin)
A1C 7%‐9%
Re‐start outpatient oral agents and D/C on glargine once daily at 50% of hospital dose
A1C >9%
D/C on basal bolus at same hospital dose.
Alternative: re‐start oral agents and D/C on glargine once daily at 80% of hospital dose
Discharge Insulin Algorithm
Discharge Treatment
Umpierrez et al. Diabetes Care. 2014 Nov;37(11):2934‐9.
6.5
7
7.5
8
8.5
9
HbA1c
8.67±2.5
7.86±1.7
7.26±1.5
Hemoglobin A1c, %
Change in HbA1C after Discharge
Data are mean ±SD* p<0.001 from admission
Admission 4 Weeks 12 Weeks
*
*
Umpierrez et al. Diabetes Care. 2014 Nov;37(11):2934‐9.

10/20/2015
19
Conclusion
Measurement of HbA1c is a useful tool to assess metabolic control and to design treatment regimen at the time of hospital discharge.
The proposed HbA1c‐based hospital discharge algorithm is an effective and safe regimen for the management of general medicine and surgical patients with T2DM.
This study included frequent contacts not common for all post‐discharge patients, thus future randomized trials are need to confirm the efficacy of the proposed HbA1c based discharge algorithm in general medicine and surgery with type 2 diabetes.
Accessed 9/19/15
MUSC JC‐ADA Certifications
Carbohydrate Counting Diet

10/20/2015
20
Discharge Planning
• Be proactive! Start early (2‐3 days before)
• What can this patient handle at home, assisted living, rehabilitation, or skilled nursing facilities
• Consider side effects, drug intolerances,
comorbidities, costs
• Rx’s, supplies, appointments
• Medication reconciliation
• “Survival skills”
• Outpatient follow up with primary care provider, endocrinologist or diabetes educator within 1 month of discharge is key for all patients having hyperglycemia in the hospital
ADA. Diabetes Care. Standards of Medical Care in Diabetes. 2015. 38 (1): S83.
Overcoming the Barriers to Optimal GlycemicControl in the Hospital
• Achievable goals
• Teamwork
• Optimal glycemic control

10/20/2015
21
Thank you