Embed Size (px)
Citation preview

J. clin. Path. (1961), 14, 615
Hereditary elliptocytic anaemiaR. J. L. DAVIDSON AND W. T. STRAUSS
From the Departments ofPathology and Medicine, Queen's College, Dundee
SYNOPSIS A sibship with four cases of hereditary elliptocytic anaemia is described. The conditionin this family may have arisen as a mutation in the mother of the sibship; affected members were
unable to taste phenylthiocarbamide while normal members were tasters.Experiments with 32P-orthophosphate in vitro did not show any evidence of biochemical upset as
found in hereditary spherocytosis; thus a combination of congenital spherocytosis and elliptocytosiscannot be supported as the cause of the haemolytic state. Clinical evidence of haemolytic diseasewas accompanied by a tendency to excessive lysis in vitro.
Infection may play a part in the precipitationhaemolytic anaemias.
Elliptical erythrocytes occur as a well recognizedhereditary anomaly in man. The first record ofelliptical human red corpuscles is usually creditedto Dresbach (1904) but Lambrecht (1938) statesthat the anomaly was observed in 1860 by Goltz.Its inheritance as a regular autosomal dominant hasbeen confirmed in many studies since its nature wasfirst established as familial by Bishop (1914) and ashereditary by Hunter and Adams (1929). Now it isknown that in some families at least the elliptocytictrait shows genetic linkage with the rhesus bloodgroups (Goodall, Hendry, Lawler, and Stephen,1953; Marshall, Bird, Bailey, and Beckner, 1954;Morton, 1956; Clarke, Donohoe, Finn, McConnell,Sheppard and Nicol, 1960).
Hereditary elliptocytosis is not usually associatedwith anaemia. Thus, until 1943, only 12% of recordedcases showed a significant anaemia of haemolytictype (Penfold and Lipscomb, 1943). This hereditaryanomaly has to be differentiated from the ellipto-cytosis occurring in other types of anaemia, notablypernicious anaemia, hypochromic microcyticanaemia, and the anaemias of myelosclerosis andlymphoid neoplasms.The purpose of this paper is to report a six-year
study of the clinical course and haematologicalinvestigations of a sibship of seven, four of whomhave elliptocytosis with a significant haemolyticanaemia and splenomegaly. One member requiredcholecystectomy for pigment stones; another derivedbenefit from splenectomy.
Received for publication 21 March 1961
of anaemic crises in this as in other hereditary
CLINICAL DETAILS
The propositus, patient II 3 (Fig. 1), a 49-year-old farm-worker was admitted to hospital with a five-day historyof upper abdominal pain, nausea, vomiting, and slightjaundice. One similar attack two years previously hadresolved with conservative treatment. Examinationshowed epigastric tenderness, slight enlargement of theliver, a palpable tender spleen, and mild conjunctivalicterus. His urine contained a trace of bile and excessurobilinogen. Radiological examination of the chest,barium meal examination, and cholecystography revealed
I 2
1 ~~~2
I7E1 2 / 3 4 51 6 7
III 01 2
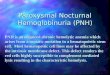
effl Dead J00 No Elliptocytosis. Non-taster
L13® No Elllptocytos*s. Taster No Elliptocytsosi_t.at.e
FIG. 1. The pedigree of the affected family.615
I
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

R. J. L. Davidson and W. T. Strauss
TABLE IHAEMATOLOGICAL FINDINGS IN THE SIBSHIP
Hb R.B.C. P.C.V.(g./100 ml.) (ml./ (Y/.)100% = c.mm.)148 g.)
M.C.H.C. M.C. V. Reticulo- W.B.C. Direct Alkaline(%) (cM) cytes (cellsl Coombs Phos-
(%) c.mm.) Test phatase(K.-A.units)
30/ 5/57 14-0818/10/59 13 66/ 6/56 13-12
22/ 5/60 12-32Pre-splenectomy25/5/59 9 0428/5/59 10-413/7/59 10-88Splenectomy 12/8/59Post-splenectomy20/ 8/59 13 4410/12/59 15 685/ 7/60 14-56
24/9/59 12-1629/2/60 11-5224/10/54 13-718/10/59 14 5624/10/55 15-0418/10/60 14-4
4-064-24-24-1
37363735
38373535
3-8 - -
3 9 34 383-63 33 33
(I pint blood transfused)
4-45065-13-443-864254-824-8465
394342323437414340
34-43634373437353536
91868885
8790
8582948887858986
7-26-45-69-2
4-361
099-270*5070-60-8
Neg. 14Neg. 12Neg. 8Neg. 9
2,8002,8003,200
4,0006,1004,800
091.52-0
04050-8
1-32.02-8
Neg. 8 1-0 0-4 1-4Neg. 9 14 0-6 2-0
Neg.Neg.Neg.Neg.Neg.Neg.Neg.Neg.
98 596
151299
0-80-61 41 3
0-320440-60-4
no abnormality. There was a mild normochromic anaemiawith 90% elliptocytes, occasional microelliptocytes andspherocytes, and a reticulocytosis of 7%. Haemolyticelliptocytic anaemia was diagnosed in this patient andhis siblings (Tables I to III). Tests of hepatic functionshowed raised serum bilirubin, thymol turbidity, andcephalin-flocculation values. The patient responded toconservative treatment but on discharge three weekslater the thymol turbidity and cephalin-flocculation levelswere still rather high and it was concluded that slight,chronic hepatic damage was present. This was laterverified by biopsy. No other sibling has similar hepaticdamage.
In January 1957 he suffered a further haemolytic crisispreceded by an attack of bronchitis.
In February 1957 a posterior gastro-jejunostomy wasperformed for a large posterior duodenal ulcer. Atoperation it was noted that the gall bladder was normaland contained no calculi, and that the spleen wasapproximately three times normal size. Liver biopsyshqwed chronic inflammatory thickening of the capsule,a fibrous scar with round cell infiltration, and a focus ofbile-duct hyperplasia. After gastro-jejunostomy hisdyspepsia was relieved and he has had no furtherhaemolytic episodes.
PATIENT II 2 This 56-year-old brother had a haemolyticepisode at the age of 34. He was seen by his family doctorwho diagnosed 'pernicious anaemia', but he made aspontaneous recovery without specific treatment. Fiveyears later, he had biliary colic for which cholecystectomywas performed at another hospital. The gall bladdercontained numerous small pigment stones. He has acompensated haemolytic anaemia (Table I) with slightconjunctival icterus and a palpable spleen.
1-141 022-01 7
03
0-2
PATIENT ii 4 This 48-year-old brother appears to havethe most labile haematological state of the affectedmembers as he has suffered from recurrent nausea,vomiting, weakness, anaemia, and jaundice since child-hood.
In May 1959 he was admitted to hospital with pyrexia,epigastric pain, nausea, vomiting, and a cough productiveof mucopurulent sputum (Table I). Repeated sputumculture revealed normal flora. Crepitations were heard atthe base of the right lung and radiological examinationshowed slight opacification at the right costophrenicangle. There was no hepatomegaly but the spleen wasenlarged and tender. His urine contained no bile, buturobilinogen was detected at a 1: 25 dilution by Ehrlich'stest. He responded to a course of antibiotics but re-current crises and anaemia with resultant incapacity forwork seemed to warrant splenectomy. After investigationthis was performed in August 1959 during a phase ofremission (Mr. G. M. Sturrock). At operation the gallbladder appeared normal; in particular it contained nocalculi. Liver biopsy revealed no histological abnormality.Marrow biopsy showed a hyperplastic, normoblasticreaction. The normoblasts were round, as were themajority of the polychromatic corpuscles.The enlarged spleen (500 g.) was uniformly congested
but showed no focal lesion. Imprints from freshly cutsurfaces showed only occasional erythrophages. Histo-logical examination confirmed the congestion and showedhyperplasia of the reticuloendothelial cells of the redpulp with diffuse haemosiderosis.
Since discharge in September 1959 the patient hasreturned to full work. His haematological state hasremained stable and satisfactory. Details and comparisonof studies performed before and after splenectomy areshown in tables.
616
Patient and Dateof Samples
Serum Bilirubin(mg./100 ml.)
Indirect Direct Total
II 2
II 3
II 4
II 5
II 6
II 7
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

Hereditary elliptocytic anaemia
PATIENT u 5 This 47-year-old sister has a life-longhistory of anaemia, but does not admit to having beenjaundiced. At one time she was treated elsewhere withfolic acid for a macrocytic anaemia not associated witha histamine-fast achlorhydria. Since coming underobservation she has had a fairly well compensatedhaemolytic state with no crises.
PATIENTS II 6 AND II 7 These sisters of the propositusare symptom-free and have normal blood. They havevery kindly acted as normal controls in various investi-gations.
PATIENT 11 I This brother, who died at the age of 19from 'spinal trouble', had no history of anaemia orjaundice.
GENETIC STUDIES
Both parents of the affected sibship are dead (Fig. 1),but it is known that the mother had anaemia, gall-stones, and intermittent jaundice.
In order to investigate the possibility of ellipto-cytosis in collaterals, all living paternal and maternalsiblings, i.e., brothers and sisters of I 1 and I 2, alltheir living offspring, and all living offspring ofdeceased siblings were examined by one of us(R.J.L.D.). Screen tests, made on finger-pricksamples, including Hb estimation (as oxyhae-moglobin in an EEL photoelectric colorimeter),reticulocyte count (Brecher's method), and examina-tion of Leishman-stained films. In preparing thefilms care was taken to spread them lightly to givea relatively thick smear, as the elliptical shape maybe lost by thin, hard spreading. Any member withan abnormal screen test or history of anaemia wasmore fully investigated, the further investigationsincluding tests of osmotic fragility and auto-haemolysis. In all, 27 paternal and 29 maternalrelatives were examined. None was shown to havesignificant anaemia or any familial anomaly of theerythrocytes. As the maternal history is compatiblewith a haemolytic anaemia and such a condition ispresent only in her offspring, we think it is likelythat this familial elliptocytosis arose as a mutationin the mother of the affected sibship.A link between the elliptocytosis and the rhesus
blood groups was sought, but because of thesimilarity of the Rh genotype of the affected andnormal members it could not be established. Data onthe ABO, MN, and P systems were similarly un-informative. On the other hand, a study of theirability to taste phenylthiocarbamide (P.T.C.) showedthe four affected members to be non-tasters and thenormal members to be tasters. The numbers, how-ever, are so small that linkage could not be estab-lished. Among other elliptocytic families, families
3 and 4 of Goodall et al. (1953 and 1954) and family5 of Lawler and Sandler (1954) have been similarlytested (Lawler, personal communication). The datawere such that no conclusions could be reached infamilies 3 and 4, but there appeared to be indepen-dence of tasting and elliptocytosis in family 5.The findings in this family suggest that futurestudies of families with hereditary elliptocytosisshould include ability to taste phenylthiocarbamide,particularly if there is no evidence of Rh linkage orif there is a consistently associated haemolyticanaemia.
HAEMATOLOGICAL INVESTIGATIONS
MORPHOLOGY All members of the sibship have hadat least four complete haematological investigationsduring the period of study, but only the resultsrelevant to the subsequent text are given below.The affected members all showed a similar red
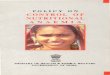
cell morphology with approximately 90% ellipto-cytes, occasional microelliptocytes, spherocytes, andcells which tended to crenate even in fresh samples.A variable reticulocytosis was always present.After splenectomy in patient II 4 (Fig. 2) thenumber of microelliptocytes and spherocytes wassignificantly increased, as has been noted in severalpreviously reported cases (Dacie, Mollison, Richard-son, Selwyn, and Shapiro, 1953; Lipton, 1955;Letman, 1955; Wilson and Long, 1955).The presence of microelliptocytes and sphero-
cytes in the peripheral blood, the splenomegaly, andthe haemolytic anaemia in all the affected memberssuggested the possible coexistence of congenitalspherocytosis and elliptocytosis, and the followinginvestigations were undertaken to see if this com-bination really existed.
RADIOCHEMICAL INVESTIGATION in vitro The rate ofexchange of 32P-orthophosphate between plasmaand erythrocytes in cases of congenital sphero-cytosis has been found to be normal (Prankerd,Altman, and Young, 1954, 1955) but it was laterfound by Tabechian, Altman, and Young (1956)that in the presence of sodium fluoride spherocytesbehaved differently from normal red cells. Thuswhen NaF (10-3M) is added to normal blood thereis little or no alteration in the rate of 32P-ortho-phosphate uptake by the erythrocytes, but withcongenitally spherocytic cells the exchange processceases after about one hour and may even be reversed.Two cases of congenital spherocytosis were examinedby us and showed the fluoride inhibition but bloodfrom the four siblings with elliptocytosis as well asfrom their unaffected sisters behaved normally.Patient II 4 gave similar results before and after
617
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

R. J. L. Davidson and W. T. Strauss
FIG. 2. Blood films (a) before splenectomy and (b) after splenectomy x 1,200.
splenectomy. Thus, from the results of this radio-chemical test, we have no reason to believe thateither the spherocytosis or the anaemia in ourelliptocytic cases was due to a coexistent con-genital spherocytic anaemia. Three other cases offamilial elliptocytosis with no anaemia and sixnormal controls likewise showed no inhibition ofexchange on addition of NaF. Studies on the32P-orthophosphate exchange in hereditary ellipto-cytosis have not been previously reported and detailsof these findings are to be published elsewhere.
OTHER CHEMICAL INVESTIGATIONS Haemoglobinfrom the affected siblings showed a normal electro-phoretic behaviour and virtually no alkali resistance.Liver function tests (including quantitative esti-mation of plasma proteins by both precipitation andelectrophoresis) were normal except in patient II 3,who showed increased cephalin-flocculation andthymol turbidity levels.
FRAGILITY AND AUTOHAEMOLYSIS TESTS Salineosmotic fragility (fresh and incubated) and auto-haemolysis tests were carried out according toDacie (1960a), except that heparinized blood wasused for all tests. The normal values quoted arederived from studies by one of us (R.J.L.D.) on34 normal men and 30 normal women.The splenic venous sample from patient IL 4 was
obtained at the time of operation, after the splenicartery had been ligated. The Hb level on this samplewas 11-5 g. per 100 ml.; haematocrit 38%. The
results of these tests are recorded in Tables II andIII. The total bilirubin content of the splenicvenous sample was 3-2 mg. per 100 ml., whereas
Patient
II 2II 3II 4
TABLE IIOSMOTIC FRAGILITY
Median Cell Fragility (% NaCI.)
Fresh Blood After SterileIncubation for24 Hours
Pre-splenectomySplenic venous bloodPost-splenectomy
II 5II 6II 7Normal range
0-4480-4320440480-4660-460-4204
0-384 to 0-464
0 5760-6160-600-720-660-5680540-5480-492 to 0-60
TABLE IIIAUTOHAEMOLYSIS% HaemolysisPatient
24 Hours
No GlucoseGlucose AddedAdded
II 2 1-2 0-3II 3 0-8 04II 4 Pre-splenectomy 0-6 0-3
Post-splenectomy 1-3 0-8II 5 1-0 05II 6 0 011 7 0 0Normal range 0 0-0 5 0 0-0 3
48 Hours
No GlucoseGlucose AddedAdded
9.5506-0170100091-50-5-5 0
1-21-31-24 12-3030-20-1-0-5
618
I
i
W:F..'
mdw.
7- 1
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

Hereditary elliptocytic anaemia
that of a peripheral venous sample was I1 mg. per100 ml.; this marked difference suggests that in thispatient the spleen was exerting an excessive haemo-lytic action on the abnormal erythrocytes.
DISCUSSION
THE ELLIPTICAL SHAPE In hereditary elliptocytosisthe factors determining the unusual shape of theerythrocytes are unknown. As in other such cases,Hb electrophoresis and alkali denaturation in thisfamily revealed no abnormal haemoglobins. It hasbeen shown, however, by Breuer, De Vries, Peket,and Matoth (1958) that special moving-boundaryelectrophoretic techniques reveal minor differencesbetween normal adult haemoglobin and haemo-globins from patients with elliptocytosis and otherhereditary anaemias; these observers postulate aweakness of the bonds that link the subunits of thehaemoglobin molecule and thus the internalstructure of these abnormal erythrocytes. The onlyreport of significantly high levels of foetal haemo-globin in adult elliptocytic cases is that of Ducla-Soares and Parreira (1958). A structural or enzymicdefect of the stroma or cell membrane is a possiblebut yet unproven explanation of the elliptical shape,and in our cases with haemolytic anaemia at least,such a defect seems probable in view of the abnormalhaemolysis in vitro.
OSMOTIC FRAGILITY in vitro The osmotic fragilityvalues of all the affected members in this familywere significantly higher than those of the un-affected members and were at or above maximumnormal levels. This supports the view that thepresence of bizarre-shaped cells, microelliptocytes,and spherocytes is likely to be associated withhyperhaemolysis.
After splenectomy, in patient II 4 there was asignificant increase in the osmotic fragility of bothfresh and incubated samples, explicable no doubt bythe increase of microelliptocytes and spherocytes inthe peripheral blood. An increase in fragility inelliptocytosis is generally accepted as occurringafter splenectomy, but in only a few cases has acomparison been made with pre-splenectomy valuesin the same patient, and in these cases the changesvaried from a marked increase (Letman, 1955) to noincrease at all (Blackburn, Jordan, Lytle, Swan, andTudhope, 1958). Similarly, in congenital sphero-cytosis, Young, Izzo, and Platzer (1951) and Dacie(1960b) conclude that there is a further increase inosmotic fragility following splenectomy, particularlyas measured on incubated samples.
Study of venous blood from the splenic vein itselfhas been thus far reported only once in relation to
elliptocytosis, no significant differences being notedin the red cell morphology or osmotic fragility rangein samples from the splenic vein and artery (Lipton,1955). In contrast, we found a considerable increasein the osmotic fragility of splenic venous blood inpatient 11 4 compared with that of peripheral venoussamples, and since this could not be explained byany difference in the packed cell volume of thesamples it may reflect a splenic action on the cellspromoting lysis in a way comparable with that seenin congenital spherocytosis (Emerson, Shen, Ham,Fleming, and Castle, 1956).
AUTOHAEMOLYSIS Reports on autohaemolysis inhereditary elliptocytosis are few and the resultsinconclusive. In this family the results are similarto those obtained by Dacie (1960c) in his familiesC, D, and G, namely, that increased levels were foundon sterile incubation for both 24 and 48 hours andthe addition of glucose greatly reduced the haemo-lysis but not to normal levels.
After splenectomy our patient II 4 showed afurther increase of autohaemolysis. The case D.Hiof family B described by Dacie (1960d) also showedan abnormally high level but had not been studiedbefore splenectomy. The rise in our case and thehigh level in Dacie's case contrast with the situationin congenital spherocytosis where post-splenectomyautohaemolysis levels tend to be lower than thoserecorded before splenectomy (Selwyn and Dacie,1954).
THE HAEMOLYTIC ANAEMIA Most cases of hereditaryelliptocytosis have neither clinical nor laboratoryevidence of haemolytic anaemia. A minority, how-ever, show various degrees of hyperhaemolysis butthe factors determining these grades of severity areonly partly understood. The homozygous state,which is so important in the haemoglobinopathies,has only twice been found responsible for severehaemolytic, elliptocytic anaemia (Wyandt, Bancroft,and Winship, 1941; Lipton, 1955).The presence of spherocytes in the blood of heter-
ozygous subjects with elliptocytic anaemia has ledobservers in the past to suggest the possibility of acombination of congenital spherocytosis and ellipto-cytosis as the basis for the anaemia but neitherHolst-Larsen (1947) nor subsequent workers haveoffered any proof of this idea, and certainly theresults of our genetic and radiochemical studies areagainst such a combination. A possible, and, to us,a reasonable explanation of the presenceof themicro-spherocytes and microelliptocytes is that thesesmall forms are the result of red cell fragmentation(Motulsky, Singer, Crosby, and Smith, 1954).The rare combination of the elliptocytic trait with
619
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

R. J. L. Davidson and W. T. Strauss
a haemoglobinopathy is not of any help in theelucidation of the usual type of hereditary ellipto-cytic anaemia, and, in the known examples of com-bination with Hb S (Vandepitte and Louis, 1955)and Hb C (Avery, 1956), the abnormal haemoglobindid not appear to potentiate the pathogenicity of theelliptocytosis.
It has been suggested that anaemia may becaused by the combination of the gene(s) for ellipto-cytosis with another gene which of itself does notcause any detectable change in the blood. Such apossibility was raised by the cases of Mason (1938)and Lendval (1949), where there was a history of anundetermined type of anaemia on the side of theparent not bearing the elliptocytic trait. In sum, thereis no convincing proof that the anaemia of hereditaryelliptocytosis is due to combination with othergenetically determined abnormalities.
INFECTION AND HAEMOLYSIS OR HAEMOPOIETIC DE-PRESSION In the congenital haemolytic anaemiasit is still uncertain whether the relationship of acasual infection to a clinical exacerbation of thehaematological state is an intensification of thehaemolysis or a suppression of haemopoiesis,although the observations of Owren (1948),Dameshek and Bloom (1948), and Gasser (1950,1951) all point to temporary marrow failure as themore important precipitating factor.
All the affected members in our elliptocyticfamily gave a history of episodes of fever, weakness,and anaemia associated with abdominal pain orrespiratory symptoms. Patient II 4 on his firstadmission to hospital had such an episode with aproductive cough but culture of the sputum yieldedno pathogenic organisms; the finding of leucopeniain the presence of a mild respiratory infection,anaemia, and a reticulocyte count well below his'compensated' level certainly suggested that theanaemia was due to a sudden haemopoietic insuf-ficiency. Unfortunately, confirmatory marrow aspira-tion was not carried out. Campanacci, Torlontano,Tonietti, and Conti (1960) suggested that their twoelliptocytic anaemic patients had hypoplastic erythro-poiesis, and although no other comparable reportsare available, infection seems to have unmasked thepresence of previously unsuspected hereditaryelliptocytosis by precipitating a severe anaemia inDacie's (1954) case and that reported by Blackburnet al. (1958).
MEGALOBLASTIC CHANGES The reputedly megalo-blastic relapse in Cases II 2 and II 5 were diagnosedelsewhere but not documented precisely enough tobe cited as indubitable. We have seen two othercases of elliptocytic anaemia mistakenly diagnosed
on the blood film as megaloblastic anaemias.Megaloblastic change is known to occur rarely incases of congenital spherocytosis and other haemo-lytic anaemias, particularly in pregnancy, but noadequately proven case has been recorded in a personwith hereditary elliptocytosis.
HAEMOLYTIC ROLE OF THE SPLEEN The spleen isusually enlarged and palpable in patients withelliptocytic haemolytic anaemia, but in thosepatients with merely the trait the spleen is notpalpable, and, therefore, probably not enlarged.The haemolytic activity of the spleen has beendemonstrated in patient II 4 by bilirubin estimationand osmotic fragility tests on splenic venous blood.As in congenital spherocytosis, the cause of thesplenic congestion and the mechanisms leading todestruction of the abnormal erythrocytes are largelyunexplained. The available evidence suggests, how-ever, that the lytic role of the spleen is secondary tothe genetically determined defect of the erythrocytes.
TREATMENT Although the factors responsible forthe elliptical shape of the erthrocytes and the patho-genesis of the occasionally associated haemolyticanaemia are far from being adequately understood,there seems little doubt that in the anaemic casessplenectomy alleviates the haemolytic state andimproves the physical well-being of the patient.The results of splenectomy are reviewed by Dacie(1960e) and we merely add that in our Case II 4 theoperation was of definite benefit.
We thank Professor 1. G. W. Hill and Mr. G. M. Sturrockfor permission to investigate patients under their care,Professor A. C. Lendrum, Dr. K. G. Lowe, and Dr.Sylvia D. Lawler for reviewing the manuscript, Dr. H.B. Goodall for encouragement and advice, Dr. F.Hutchison for help with the radioactive investigation, andMr. R. Smith and Mr. J. Corkhill for special technicalassistance.
REFERENCES
Avery, M. E. (1956). Bull. Johns Hopk. Hosp., 98, 184.Bishop, F. W. (1914). Arch. intern. Med., 14, 388.Blackburn, E. K., Jordan, A., Lytle, W. J., Swan, H. T., and Tudhope,
G. R. (1958). J. clin. Path., 11, 316.Breuer, M., De Vries, A., Peket, L., and Matoth, Y. (1958). Proc.
6th int. Congr. int. Soc. Hematology, Boston, 1956, p. 749.Grune and Stratton, New York.
Campanacci, L., Torlontano, G., Tonietti, G., and Conti, C. (1960).Minerva. nucleare (Torino), 4, 18.
Clarke, C. A., Donohoe, W. T. A., Finn, R., McConnell, R. B.,Sheppard, P. M., and Nicol, D. S. H. (1960). Ann. hum.Genet., 24, 283.
Dacie, J. V. (1954). The Haemolytic Anaemias, Congenital and Acquired.Churchill, London.
(1960a, b, c, d, e). Ibid, 2nd ed. Pt 1. Churchill, London.Mollison, P. L., Richardson, N., Selwyn, J. G., and Shapiro, L.(1953). Quart. J. Med., 22, 79.
620
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from

Hereditary elliptocytic anaemia
Dameshek, W., and Bloom, M. L. (1948). Blood, 3, 1381.Dresbach, M. (1904). Science, 19, 469.Ducla-Soares, A., and Parreira, F. (1958). Sang., 29, 33.Emerson, C. P. Jr., Shen, S. C., Ham, T. H., Fleming, E. M., and
Castle, W. B. (1956). A.M.A. Arch. intern. Med., 97, 1.Gasser, C. (1950). Sang, 21, 237.
(1951). Die hwnolytischen Syndrome im Kindesalter, p. 214.Thieme, Stuttgart.
Goodall, H. B., Hendry, D. W., Lawler, S. D., and Stephen, S. A.(1953). Ann. Eugen. (Lond.), 17, 272.__, -,- (1954). Ibid, 18, 325.
Holst-Larsen, T. (1947). Nord. Med., 34, 925.Hunter, W. C., and Adams, R. B. (1929). Ann. intern. Med., 2, 1162.Lambrecht, K. (1938). Ergebn. inn. Med. Kinderheilk., 55, 295.Lawler, S. D., and Sandler, M. (1954). Ann. Eugen. (Lond.), 18, 328.Lendval, J. (1949). Lancet, 1, 582.Letman, H. (1955). Acta med. scand., 151, 41.Lipton, E. L. (1955). Pediatrics, 15, 67.Marshall, R. A., Bird, R. M., Bailey, H. K., and Beckner, E. (1954).
J. clin. Invest., 33, 790.
Mason, V. R. (1938). In Handbook of Hematology, Vol. 3, ed. H.Downey, p. 2351. Hoeber, New York.
Morton, N. E. (1956). Amer. J. hum. Genet., 8, 80.Motulsky, A. G., Singer, K., Crosby, W. H., and Smith, V. (1954).
Blood, 9, 57.Owren, P. A. (1948). Ibid, 3, 231.Penfold, J. B., and Lipscomb, J. M. (1943). Quart. J. Med., n.s. 12,
157.Prankerd, T. A. J., Altman, K. I., and Young, L. E. (1954). J. clin.
Invest., 33, 957.(1955). Ibid, 34, 1268.
Selwyn, J. G., and Dacie, J. V. (1954). Blood, 9, 414.Tabechian, H., Altman, K. I., and Young, L. E. (1956). Proc. Soc.
exp. Biol. (N.Y.), 92, 712.Vandepitte, J., and Louis, L. (1955). Rev. Hemat., 10, 19.Wilson, H. E., and Long, M. J. (1955). A.M.A. Arch. intern. Med.,
95, 438.Wyandt, H., Bancroft, P. M., and Winship, T. 0. (1941). Arc/.
intern. Med., 68, 1043.Young, L. E., Izzo, M. J., and Platzer, R. F. (1951). Blood, 6, 1073.
Broadsheets prepared by the Association of Clinical PathologistsThe following broadsheets (new series) are published by the Association of Clinical Pathologists. They may be obtainedfrom Dr. R. B. H. Tierney, Pathological Laboratory, Boutport Street, Barnstaple, N. Devon. The prices include postage,
but air mail will be charged extra.
3 The Detection of Barbiturates in Blood, Cerebro-spinal Fluid, Urine, and Stomach Contents. 1953.L. C. NICKOLLS. IS.
4 The Estimation of Carbon Monoxide in Blood.1953. D. A. STANLEY. IS.
5 The Identification of Reducing Substances in Urineby Partition Chromatography on Paper. 1953.G. B. MANNING. is.
6 The Paul-Bunnell Test. 1954. R. H. A. SWAIN. Is.
7 The Papanicolaou Technique for the Detection ofMalignant Cells in Sputum. 1955. F. HAMPSON. Is.
10 Mycological Techniques: (1) Collection of Speci-mens. 1956. R. W. RIDDELL. IS.
11 Mycological Techniques: (2) Cultural Isolation.1956. R. W. RIDDELL. Is.
12 Techniques for Demonstrating L.E. Cells. 1956.J. V. DACIE and L. S. SACKER. Is.
13 The Identification of Serotypes of Escherichia coliAssociated with Infantile Gastro-enteritis. 1956.JOAN TAYLOR. Is.
14 The Determination of Serum Iron and SerumUnsaturated Iron-binding Capacity. 1956. ARTHURJORDAN. I S.
16 Preservation of Pathological Museum Specimens.1957. L. W. PROGER. 1s.
17 Cultural Diagnosis of Whooping-cough. 1957.B. W. LACEY. Is.
18 The Rose-Waaler Test. 1957. C. L. GREENBURY. Is.
19 The Laboratory Diagnosis of Fibrinogen Deficiency.1958. R. M. HARDISTY. IS.
20 Investigation of Porphyrin/Porphyria. 1958. c.RIMINGTON. 1 S.
21 Quantitative Determination of Porphobilinogen andPorphyrins in Urine and Faeces. 1958. C. RIMINGTON.ls.
22 Investigation of Haemolytic Anaemia. 1959. J. G.SELWYN. 1 S.
23 The Dried Disc Technique for Bacterial SensitivityTests. 1959. R. W. FAIRBROTHER and J. C. SHERRIS. IS.
24 Safe Handling of Radioactive Tissues in theLaboratory and Post-mortem Room. 1959. R. C.CURRAN. Is.
26 The Periodic Acid-Schiff Reaction. 1959. A. G. E.PEARSE I S.
28 Daily Fatty Acid Excretion. 1960. A. C. FRAZER. 2s.
29 The Preparation of Bone for Diagnostic Histology.1960. D. H. COLLINS. 2s.
31 Investigation of Haemorrhagic States with SpecialReference to Defects of Coagulation of the Blood.1961. E. K. BLACKBURN. 4s.
32 Detection of Resistance to Streptomycin, P.A.S., andIsoniazid in Tubercle Bacilli. 1961. R. CRUICK-SHANK and s. M. STEWART. 2s.
34 Titration of Antistreptolysin 0. 1961. H. GOODERand R. E. 0. WILLIAMS. 2s.
35 The Estimation of Faecal 'Urobilinogen.' 1961.C. H. GRAY. 2s.
621
on May 14, 2020 by guest. P
rotected by copyright.http://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.14.6.615 on 1 Novem
ber 1961. Dow
nloaded from