Embed Size (px)
Citation preview

Hepatitis D & E
Azizah Azhar

Content
• Introduction• Epidemiology• Mode of Transmission• Features• Prevention and control


Introduction
• Hepatitis Delta Virus• Recognized in 1977 – co existent with HBV
infection• A defective RNA virus than need hepadnavirus
(HBV) to replicate• 1980 – noticed the dependency of HDV to HBV
(need HBsAg to as virion coat)• Associated with most severe form of acute and
chronic HBsAg +

Epidemiology of Hepatitis D
• Spread worldwide– Highest in Russia, Romania, Southern Italy,
Mediterranean countries, Africa, South America– Low in China, Taiwan, India– Latest trends
• New foci in Okinawa, certain area of China, India, Albania
• Decreasing trend in Mediterranean


Mode of Transmission
• Spread– Percutaneous and sexually and through body
fluid/blood– Potentially infectious in whole phase
• People at risk– HBV carrier, HBV unvaccinated person
• IVDU• Unprotected sex• Exposed to unscreen blood, body fluid• People receiving blood, blood product

Hepatitis D Features
• IP – 5 to 64 days• Super-infection* or co-infection with HBV• Diagnosis
– Liver biopsy – Serology – anti HDV, Ig M*, RNA*
• Lead to fulminant acute hepatitis, severe chronic active hepatitis – cirrhosis, hepatocellular carcinoma

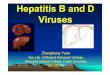
Serologic Course

Serologic Course

Prevention and Control
• Hep B vaccination*• Reduce risk behaviour• May improve with α-interferon• Epidemic measures
– Surveillance– Screening– Cases with common exposure – active case
detection, investigate source and do appropriate action


Introduction
• was not recognized as a distinct human disease until 1980
• non-enveloped, positive-sense, single-stranded RNA virus.
• antibodies to HEV or closely related viruses have been detected in primates and several other animal species.

Epidemiology of Hepatitis E
• Central and South-East Asia, North and West Africa, and in Mexico
• Common in hot climate area• sporadic cases of hepatitis E - south-east and
central Asia, the Middle East, northern and western Africa, and North America

www.ncdc.gov

Mode of Transmission
• Spread– faecal-oral route– Food and waterborne disease– possibility of zoonotic
• Risk factor– poor sanitation

Hepatitis E Features
• IP - 15 to 60 days• self-limiting viral infection • prolonged viraemia or faecal shedding are unusual
and chronic infection does not occur.• Fulminant hepatitis rarely occur (mortality 0.5-4%)• Higher in pregnant woman (mortality rate 20% in
3rd trimester)• Diagnosis
– serology - hepatitis E antibody by RT-PCR


Prevention and Control
• Surveillance and control procedures should include• provision of safe drinking water and proper disposal of sanitary waste• monitoring disease incidence• determination of source of infection and mode of transmission by epidemiologic investigation• detection of outbreaks• spread containment
• good personal hygiene, high quality standards for public water supplies and proper disposal of sanitary waste

References
• WHO. (2001). WHO Department of Communicable Disease Surveillance & Response
Available: http:/www.who.int/emc• Microbiology and Immunology Online, University of
South Carolina• Available:
http://pathmicro.med.sc.edu/virol/hepatitis-disease.htm• US CDC, Atlanta
Available: http://www.cdc.gov/ncidod/diseases/hepatitis/slideset