Embed Size (px)
Citation preview
HEMATOLOGY QUALITY CONTROL REVIEW
American Society for Clinical Laboratory Science Region III Triennial Meeting
November 18, 2016
Marquita D. Robinson, MPA, MLS(ASCP)CM
Technical Specialist, Core Laboratory
Children's of Alabama
No financial interests/relationships to disclose.
Overview
• Define Quality Control and its purpose as applicable to Automated Hematology analyzers
• Discuss how to establish quality control target ranges
• Review corrective action for out of control values
Definitions
• Quality Control (QC) – the set of procedures based on measurement of a stable material that is similar to the intended patient specimen, to monitor the ongoing performance of a measurement procedure and detect change in that performance relative to stable baseline analytical performance. QC includes testing QC materials, charting the results and analyzing them to identify sources of error, and evaluating and documenting any remedial action taken as a result of this analysis.
Definitions
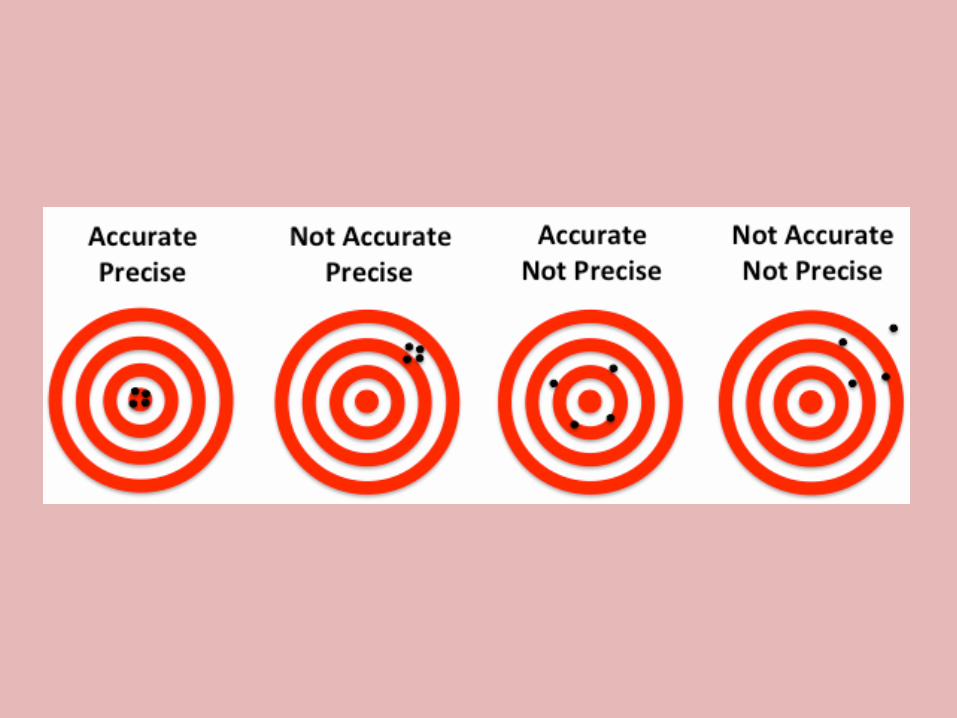
• Accuracy – closeness of agreement between a measured quantity value and a true quantity value
• Precision – closeness of agreement between indications or measured quantity values obtained by replicate measurements on the same or similar objects under specified conditions
Definitions
• Bias – estimate of a systematic measurement error; difference between the expectation of the test results
• Calibration – the process of testing and adjustment of an instrument, kit, or test system to provide a known relationship between the measurement response and the value of the substance being measured by the test procedure
• Reliability - able to maintain accuracy and precision
Calibration
• Commercial
– Stabilized human and/or animal blood
– Assigned value
– Stable
• Whole Blood
Purpose of Quality Control
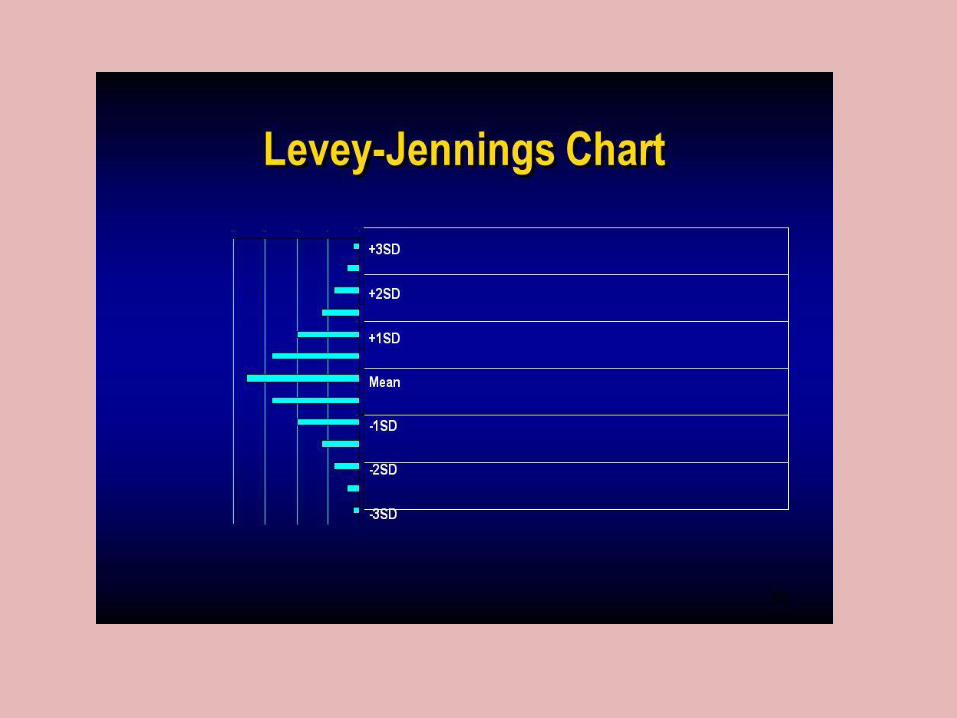
• “QA of clinical laboratory examination numeric results is not simply the processing of liquid commercial controls, generation of Levey-Jennings control charts, and multirule analysis. Rather, it includes preexamination, examination, and postexamination activities. A laboratory’s first concern is patient safety.”
Purpose of Quality Control
• Reduce the risk of harm to a patient due to an erroneous result
• Will an erroneous laboratory result cause an inappropriate medical decision?
• Detect changes in analyzer status
• Discover opportunities for improving analyzer performance

Performing Quality Control
Select Appropriate Quality Control
• Manufacturer’s recommendations
• Analyzer performance
• Frequency
• Price
• Peer Group Data
Control Requirements
• For laboratories subject to CLIA-88, at least two different controls must be assayed and evaluated every 24 hours.
Control Requirements
• CAP requirements The College of American Pathologists (CAP) Hematology Survey checklist states the following:
• For laboratories subject to CLIA-88, at least two different controls must be assayed and evaluated every 24 hours. For each QC procedure employed, the laboratory must have appropriate QC ranges. For example, expected recovery ranges for commercial control materials are NOT the same as between run SD ranges and are probably too wide for daily QC of a single instrument. The laboratory should calculate its own imprecision statistics for each instrument.
• HEM.25870 Phase II If commercially ASSAYED controls are used for CBC instruments, control values correspond to the methodology and have target values (mean and QC ranges) are verified or established by the laboratory. – NOTE: Most commercial controls have expected recovery ranges for each parameter, provided
by the manufacturer. The mean of such ranges may not be the exact target value in a given laboratory. Each laboratory should assign its own initial target value, based on initial analysis of the material; this target value should fall within the recovery range supplied by the manufacturer, but need not exactly match the package insert mean. The laboratory should establish specific recovery ranges that accommodate known changes in product attributes, assuming that calibration status has not changed.
Establish Control Means and SD
1. Analyze the control a minimum of 20 times. 2. Take the average of these runs. 3. The average should be within the range stated on the assay sheet. 4. If the average is within range, it will be considered as the “new
mean.” 5. Calculate the two Standard Deviation range from your results. 6. Incorporate this SD range around your mean and monitor
throughout the dating of the product. 7. The mean and SD values should be periodically recalculated
during the life of the new lot. 8. Mode to Mode Comparisons
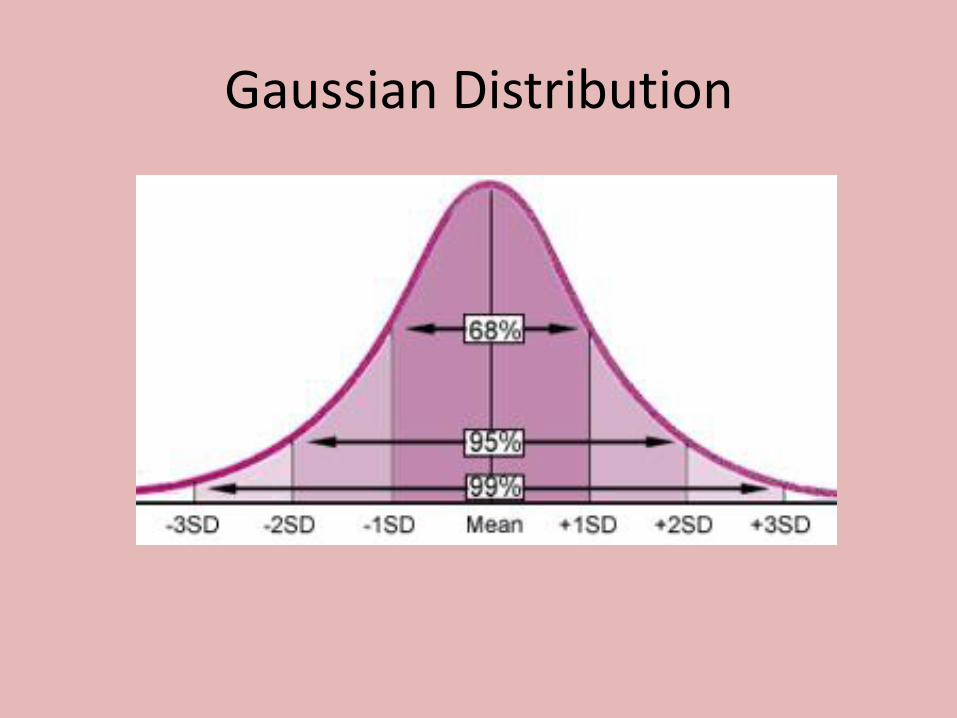
Gaussian Distribution
Lot to Lot
1. Analyze the control parallel to the current lot.
2. Take the average of these runs.
3. This average should be within the range stated on the assay sheet.
4. Use your historical established laboratory SD and CV% to set recovery ranges.
Laboratory Quality Assurance Program
• Preexamination – Operator Training/Competency – Specimen Collection – Specimen Mixing
• Examination – Calibration/Controls – Acceptable Performance, Limitations
• Postexamination – Delta Checks – Moving Averages – External Quality Assurance – Proficiency Testing
• Preexamination
– Operator Training/Competency
– Specimen Integrity
• Collection
• Specimen Mixing
Laboratory Quality Assurance Program
• Examination
– Calibration/Controls
– Acceptable Performance, Limitations
Laboratory Quality Assurance Program
• Postexamination
– Delta Checks
– Moving Averages
– External Quality Assurance
– Proficiency Testing
Delta Checks
• Compares the result from sample analysis with result from a previous analysis on same patient.
• Laboratory defined limits
• Instrument, middleware, or LIS performs calculations
Delta Checks
• WBC ± 35% 1440 min, RBC ± 20% in 1440 min, and MCV ± 4% in 1440 min. • We use delta checks for HGB, MCV, AND PLTS. • Don’t need both H&H and no need for diff parameters, WBC fluctuations
are daily. So we always ignored them anyway-but had a rule if 2 deltas-must explain- either post op, post transfusion, post IV fluids, etc…”
• We only use delta checks for MCH?!?! Where I use to work we did H&H, PLT, MCV, WBC. Always thru LIS. MCV/MCH are big ones that need a reason or redraw.”
• We use the flagging off the instrument for values we set, but we also have deltas on WBC, MCV, MCHC, HGB, all diff parameters and PLTs through LIS. We have the deltas to detect misdraws or pathological changes (usually misdraws or poor draws are the culprit).”
• Delta checks for HGB, HCT, MCV, AND PLT. And then we utilize all the rules/flags from the Sysmex plus more we built for when scan and man diffs are necessary.”
Moving Averages
• Allows continuous monitoring of instrument performance and used in combination with commercial QC
• Detects calibration drifts
• RBC indices: MCV, MCH, MCHC
• Performed if analyze ≥ 100 samples daily or ≥ 400 daily
Moving Averages Targets
• Start with Bull’s MCV=89.5 ; MCH=30.5; and MCHC=34.0
• Run ~ 400-500 samples. Determine mean (target), SD, CV%.
• Mean of batch results are compared to the target.
• Should remain constant unless patient population changes
Differentials
• Combination:
– Commercial Control
– Automated Hematology System flag and codes
– Manual counts
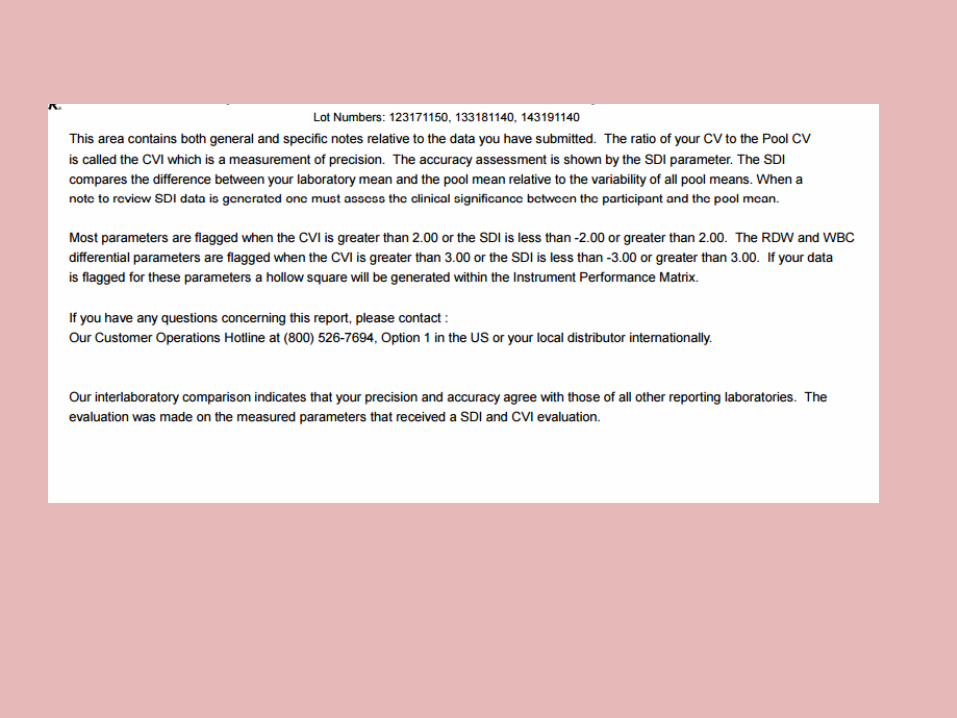
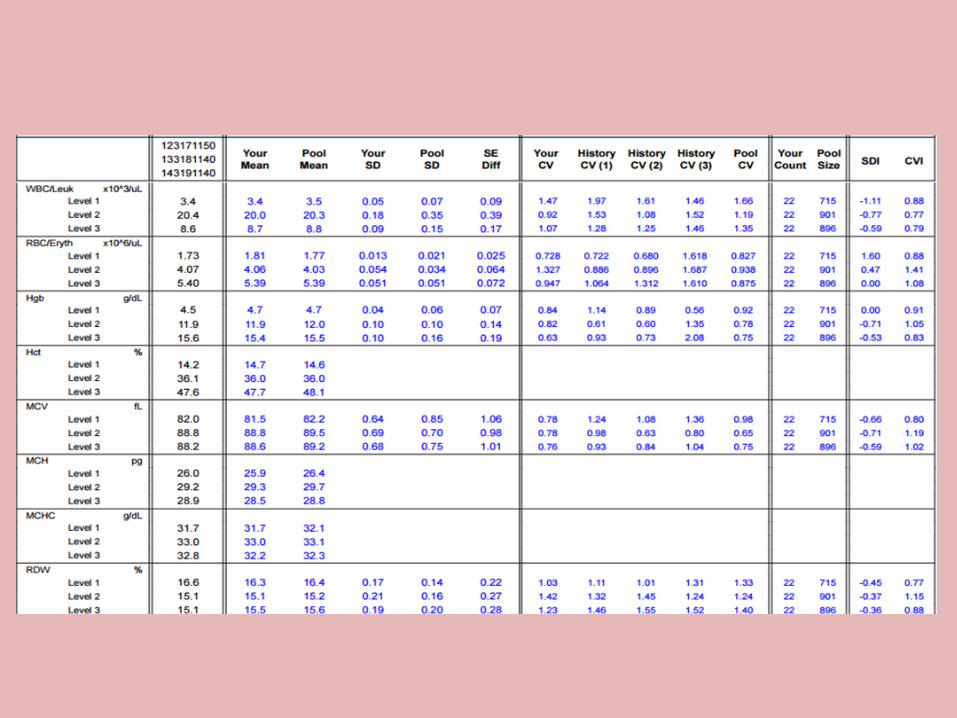
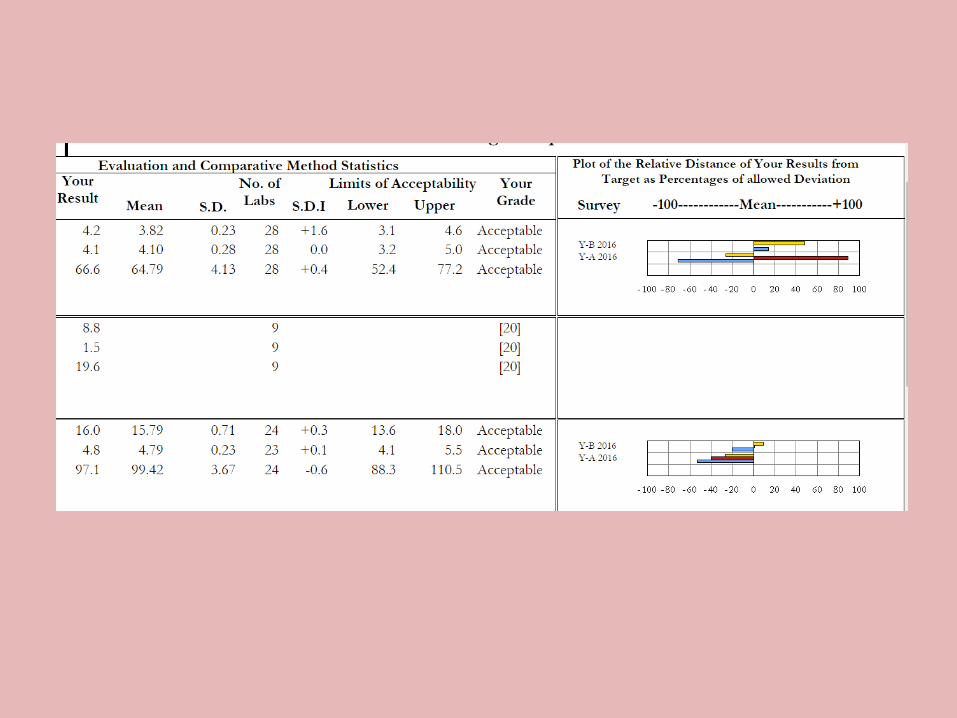
External Quality Control
• Monitors performance in comparison to other labs using the same instrument, method, or reagents.
• Accuracy and Bias
• SDI and CVI
Troubleshooting Out of Control Values
• Have a plan.
– Policies and Procedures
• Troubleshooting
• Contingency Plan
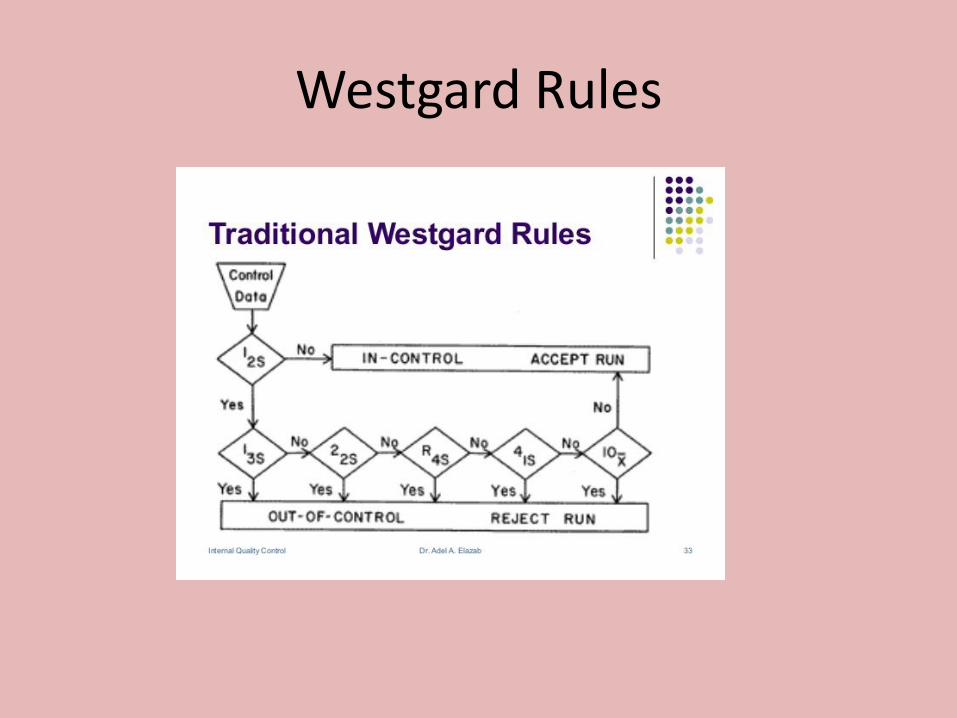
Westgard Rules
Westgard Rules
• 12s : this rule is used as a warning rule to trigger careful inspection of the control data by the following rejection rules.
• 13s: A run is rejected when a single control measurement exceeds the mean plus 3s or the mean minus 3s control limit.
• 22s: reject when 2 consecutive control measurements exceed the same mean plus 2s or the same mean minus 2s control limit.
• R4s: reject when 1 control measurement in a group exceeds the mean plus 2s and another exceeds the mean minus 2s.
• 41s: reject when 4 consecutive control measurements exceed the same mean plus 1s or the same mean minus 1s control limit.
• 10x: reject when 10 consecutive control measurements fall on one side of the mean.
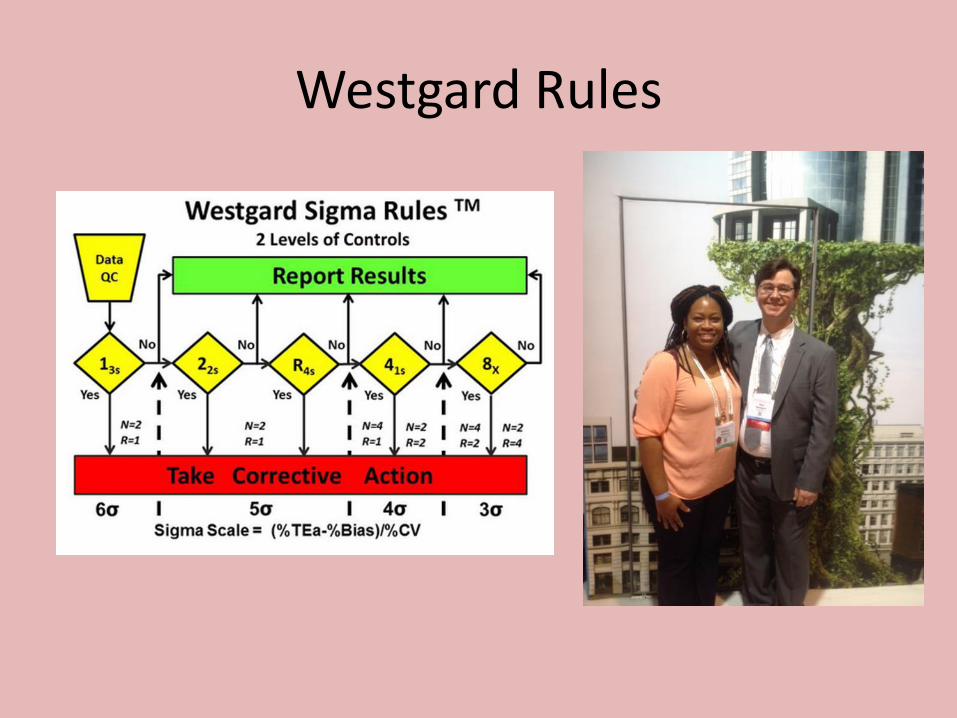
Westgard Rules
Problem Solving
• Bad Habits
• Distrusting our QC:
1. Simply repeat the control.
2. Try a new control.
• Good Habits
• Trust the QC, trust your skills, and have the right attitude.
1. Inspect the control charts or rules violated to determine type of error.
2. Relate the type of error to potential causes.
Problem Solving
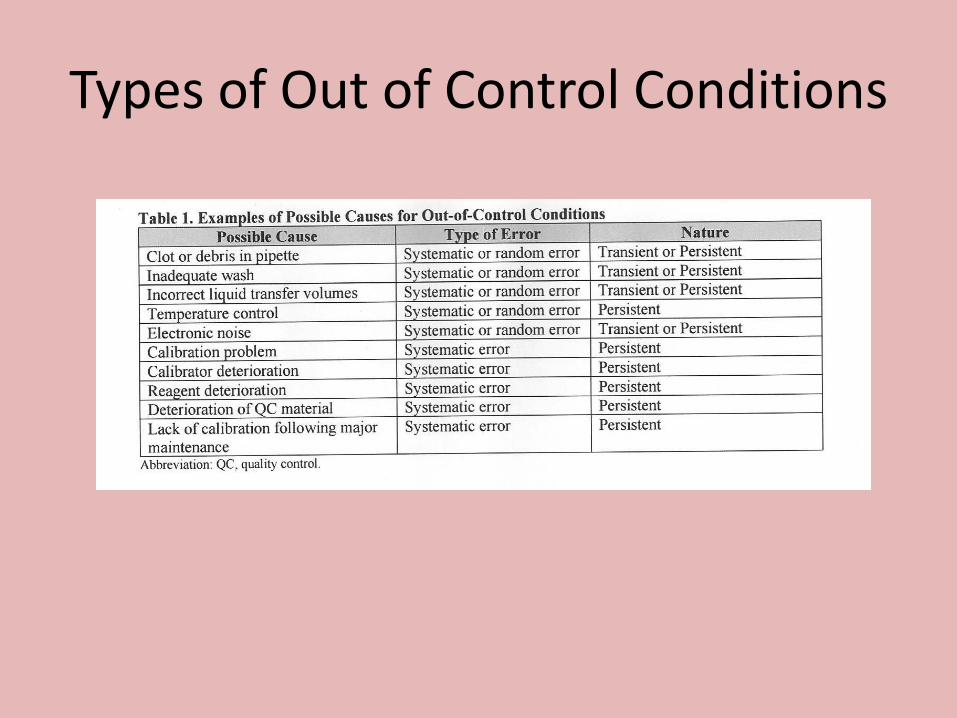
Types of Out of Control Conditions
• Good Habits
• Trust the QC, trust your skills, and have the right attitude. 1. Inspect the control charts or rules violated to
determine type of error.
2. Relate the type of error to potential causes.
3. Consider common factors in multitest systems.
4. Relate causes to changes or “events”
5. Verify the solution and document the remedy
Problem Solving
Trouble-shooting 6. Adopt a systematic troubleshooting approach
• QC Material – Correct material, lot number level? – Correctly prepared? – Levels interchanged? – Within stated expiration date/stability after preparation? – Correctly stored?
• Reagents – Correct material , lot number? – Correctly prepared? – Correctly loaded and used? – Within stated expiration date? – Correctly stored?
• Calibrator – Correct material , lot number? – Correctly prepared and used? – Correct number and order? – Correct calculations and settings? – Within stated expiration date?
• Analyzer – Correct maintenance? – Any recent changes? – Materials within stated on-board stability? – Visual inspection for problems?
• Environment – Proper water system? – Waste disposable functioning properly? – Temperature and humidity at proper levels?
7. Develop trouble-shooting guides.
Trouble-shooting
Documentation
• HEM.18691
QC Corrective Action - Waived Tests Phase II
There is evidence of corrective action when control results exceed defined acceptability limits.
Documentation
• HEM.20070 Precision Statistics Phase I The laboratory has an action protocol when data from precision statistics change significantly from previous data. NOTE: As an example, if the laboratory's normal-level commercial control usually yields a monthly CV of 2% for WBC, but the most recent month shows a 4% CV, then something has caused increased imprecision, and investigation with records is required. Similarly, if the monthly SD for MCV by moving averages is typically around 1.8 fL, but now is at 3.1 fL, the laboratory must find a cause for this shift and take action, if indicated. Finally, if commercially sponsored interlaboratory QC data for the same control lot and instrument model show SD/CV values markedly smaller or larger than the peer group, an explanation is required. Evidence of Compliance: ✓ Written procedure for investigation and corrective action should a significant change in precision statistics occur AND ✓ Records of investigation and corrective actions taken
References
• Quality Control (QC) Information and Troubleshooting Guide – Hematology – Beckman Coulter
• Establishing Quality Control Means and Standard Deviation for Hematology Instrument, Streck
• CLSI. Statistical Quality Control for Quantitative Measurement Procedures: Principles and Definitions.4th ed. CLSI guideline C24. Wayne, PA: Clinical and Laboratory Standards Institute; 2016.
• CLSI. Validation, Verification, and Quality Assurance of Automated Hematology Analyzers; Approved Standard-Second Edition. CLSI document H26.A2. Wayne, PA: Clinical and Laboratory Standards Institute; 2010.
• CAP Accreditation Checklists, Hematology and Coagulation, Nonwaived Tests 8-17-16.
• Westgard, James O., Ph.D. Basic QC Practices. 4th ed. Madison: Westgard QC, 2016. Print.
• Rodak, Bernadette F., MS, CLSpH(NCA), MT(ASCP)SH. Hematology Clinical Principles and Applications. 2nd ed. Philadelphia: Saunders, 2002. Print.






























