Embed Size (px)
Citation preview
Treatment of Iron Overload inMyelodysplastic Syndrome
Guest Editor: Alan F. List, MD
HEMATOLOGY/ONCOLOGY CLINICSNovember 2006 • Volume 20 • Supplement 1
Supported by an educational grantfrom Novartis Pharma AG
This activity has been jointly sponsored by the Elsevier Office of Continuing Medical Education and Excerpta Medica, Inc.
Inde
xed
in
Inde
x Med
icus®
MED
LINE
UP TO 1 FREE AMA PRA CATEGORY 1 CREDIT™

W.B. SAUNDERS COMPANY
A Division of Elsevier Inc.
1600 John F. Kennedy Boulevard, Suite 1800, Philadelphia, PA 19103-2899
http://www.theclinics.com
HEMATOLOGY/ONCOLOGY CLINICS OF NORTH AMERICA Volume 20, Supplement 1November 2006 ISSN 0889-8588Editor: Kerry Holland
Copyright: Copyright © 2006 Elsevier Inc. All rights reserved. No part of this publication may be reproducedor transmitted in any form or by any means, electronic, mechanical, including photocopy, recording, or anyinformation retrieval system, without written permission from the Publisher.
Opinions: Opinions expressed in Hematology/Oncology Clinics are those of the authors and do not necessarily reflect those of the Publisher. The Publisher does not assume responsibility for any injury and/ordamage to persons or property arising out of or related to any use of the material contained in this periodical.
Subscriptions: 6277 Sea Harbor Drive, Orlando, Florida 32887- 4800. Customer Service: 1-800-654-2452 (US).From outside the US, call 407-345-4000. E-mail: [email protected].
Reprints/Translations/Permissions: All inquiries, reprint orders, translations, and permission requests mustbe directed to Gail M. Gallo, Reprints Manager, in our Bridgewater, New Jersey, office. Contact: telephone(908) 547-2069, fax (908) 547-2204. E-mail: [email protected]
The Hematology/Oncology Clinics is covered in Index Medicus/MEDLINE, EMBASE/Excerpta Medica, andBIOSIS.
Printed in the United States of America.
Hematology/Oncology Clinics • Supplement 1

Hematology/Oncology Clinics • Supplement 1
TREATMENT OF IRON OVERLOAD INMYELODYSPLASTIC SYNDROME
Alan F. List, MDH. Lee Moffitt Cancer Center
and Research Institute12902 Magnolia Drive, SRB-4Tampa, Florida 33612-9497
Hematology/Oncology Clinics • Supplement 1
TREATMENT OF IRON OVERLOAD INMYELODYSPLASTIC SYNDROME
CONTENTS4
CME Information
6Preface
Alan F. List, MD
7Identifying best practices in the monitoring and
treatment of iron overload in myelodysplastic syndromeAlan F. List, MD
15Commentary
Alan F. List, MD
19CME Test Questions
21CME Test Answer Sheet and Evaluation Form

4 Hematology/Oncology Clinics • Supplement 1
ACCREDITATION STATEMENTThis activity has been planned and implemented in accordance with the Essential Areas and Policies of theAccreditation Council for Continuing Medical Education (ACCME) through the joint sponsorship of the ElsevierOffice of Continuing Medical Education (EOCME) and Excerpta Medica, Inc. The EOCME is accredited by theACCME to provide continuing medical education (CME) for physicians.
CME CREDIT STATEMENTThe EOCME designates this educational activity for a maximum of 1 AMA PRA Category 1 Credit(s)™. Physiciansshould only claim credit commensurate with their participation in the activity.
FACULTY DISCLOSURESAs a sponsor accredited by the ACCME, it is the policy of the EOCME to require the disclosure of anyone who is ina position to control the content of an educational activity. All relevant financial relationships with any commercialinterests and/or manufacturers must be disclosed to participants at the beginning of each activity. The faculty of thiseducational activity discloses the following.
Faculty Member Corporation/Manufacturer Relationship
Alan F. List, MD Scios Inc. Grant/Research Support
Celgene Corporation; ConsultantPharmion Corporation;Scios Inc.
Celgene Corporation; Speakers BureauPharmion Corporation
Kanisa Inc.; Advisory Board MemberSchering Corporation
Ronald K. Miller, PhD None None
RESOLUTION OF CONFLICT OF INTERESTThe EOCME has implemented a process to resolve conflict of interest for each CME activity. In order to help ensurecontent objectivity, independence, and fair balance, and to ensure that the content is aligned with the interest of thepublic, the EOCME has resolved the conflict by external content review.
UNAPPROVED/OFF-LABEL USE DISCLOSUREThe EOCME requires CME faculty to disclose to the participants:1. When products or procedures being discussed are off-label, unlabeled, experimental, and/or investigational (not
US Food and Drug Administration [FDA] approved); and2. Any limitations on the information that is presented, such as data that are preliminary or that represent ongoing
research; interim analyses; and/or unsupported opinion. Faculty may discuss information about pharmaceutical agents that are outside of FDA-approved labeling. This infor-mation is intended solely for CME and is not intended to promote off-label use of these medications. If you have ques-tions, contact the medical affairs department of the manufacturer for the most recent prescribing information.
INTENDED AUDIENCEThis activity has been developed for hematologists and oncologists who provide care to patients diagnosed withmyelodysplastic syndrome (MDS).
CME InformationTREATMENT OF IRON OVERLOAD IN
MYELODYSPLASTIC SYNDROME

Hematology/Oncology Clinics • Supplement 1 5
PROGRAM GOALTo increase awareness of clinical considerations in monitoring and treating iron overload in patients with MDS.
EDUCATIONAL OBJECTIVESAfter reading this Supplement to Hematology/Oncology Clinics and taking the test, participants should be able to: ● Describe the usefulness of applying the International Prognostic Scoring System to patients with MDS.● Identify key factors in considering donor stem cell transplant for patients with MDS.● Identify the advantages and disadvantages of iron chelating agents.● Describe study findings regarding the association between transfusion-dependent patients with MDS and survival rates.
FINANCIAL SUPPORTThis CME activity is supported by an educational grant from Novartis Pharma AG.
CONTENT DEVELOPMENT COMMITTEEAlan F. List, MD, Guest Editor
Jennifer DiBenedettoCindy Jablonowski, MA
Sherrilyn A. Chiu
SPECIAL NEEDSWe encourage participation by all individuals. If you have any special needs, please contact Sherrilyn Chiu at (908) 547-2086 or [email protected] for assistance.
CME InformationTREATMENT OF IRON OVERLOAD IN
MYELODYSPLASTIC SYNDROME

For patients with transfusion-dependent myelodys-plastic syndrome (MDS), regular blood transfusions mayimprove both symptoms and quality of life; however,long-term use of blood transfusions may also lead to ironoverload. This is especially true for patients at lower riskfor whom survival is expected to be prolonged, as theywill likely be receiving blood transfusions for an extend-ed period. Additionally, older patients with MDS whohave comorbid cardiac and hepatic conditions may like-ly suffer from morbidity and mortality associated withiron overload. Although supportive interventions andchelation therapy have been considered the standard ofcare for patients with MDS and iron overload, patientsand clinicians may be reluctant to initiate chelation ther-apy, as many are uninformed about the need for and thelong-term benefits of this treatment option. Althoughthere are drawbacks inherent to chelation therapy, maxi-
mum benefit may be seen when treatment is initiatedearly in the course of the disease.
This article addresses the characteristics of MDS; cur-rent treatment options, including 2 new pharmacologicagents; and the clinical impact of iron overload and chela-tion therapy in patients with transfusion-dependent MDS.Best practices in treating iron overload in MDS based onthe National Comprehensive Cancer Network guidelinesfor supportive care are summarized. In addition, the char-acteristics of patients with MDS who are most likely tobenefit from chelation therapy are reviewed.
Alan F. List, MDH. Lee Moffitt Cancer Center
and Research Institute12902 Magnolia Drive, SRB-4
Tampa, Florida 33612-9497E-mail address: [email protected]
Preface
Identifying best practices in the monitoring and treatment of iron overload in myelodysplastic syndrome

The myelodysplastic syndrome (MDS) comprises adiverse group of hematopoietic stem cell disorders thatare characterized by ineffective blood production withconsequent cytopenias, cytologic dysplasia, and variablerisk for leukemia transformation [1,2]. Although affectedindividuals with lower-risk disease may survive foryears, most patients eventually succumb either to infec-tious complications, complications from blood cell defi-ciencies, or acute leukemia [3,4].
In this article we review the characteristics and treat-ment of MDS, and discuss the clinical impact of ironoverload and chelation therapy in patients with transfusion-dependent MDS. Best practices in treating iron overloadin MDS are summarized based on current NationalComprehensive Cancer Network (NCCN) guidelines forsupportive care of patients with MDS [5]. Finally, wehighlight the characteristics of patients with MDS whoare most likely to benefit from chelation therapy, andbriefly discuss treatment-related factors that might influ-ence clinicians and patients to forego chelation therapyduring treatment of transfusion-dependent MDS.
Incidence and epidemiology of myelodysplastic syndrome
MDS is a relatively common hematologic malignancy.The annual incidence rate in all age groups is estimated at3 to 4 per 100,000 people [6,7]; however, these patientsare typically elderly with a male predominance, and amedian age at onset of 65 years. The rising incidence ofMDS in recent years is probably not due to changes in etio-logic factors, but rather may reflect increased awarenesson the part of clinicians and more extended use of diag-nostic procedures in elderly patients [6,7].
Morphologic categorization of myelodysplastic syndrome subtypes
MDS is currently described and categorized accordingto the World Health Organization (WHO) classification(Table 1) [8].
The French-American-British (FAB) criteria identifiedthe following 5 subtypes of MDS: refractory anemia (RA);refractory anemia with ringed sideroblasts (RARS);refractory anemia with excess blasts (RAEB); RAEB intransformation (RAEB-T); and chronic myelomonocyticleukemia (CMML) [9].
The current WHO classification differs from the FABsystem in that blood or bone marrow threshold for acutemyeloid leukemia (AML) is reduced to 20% blast cells,thereby eliminating the FAB category of RAEB-T [8].This newer classification also refines the definitions ofRA and RARS to refer to erythroid-limited dysplasia,and introduces the category of refractory cytopenia withmultilineage dysplasia. Furthermore, the RAEB categoryis divided into 2 subgroups, RAEB-1 and RAEB-2, de-pending on the number of blast cells present in blood andbone marrow [8].
A new MDS subtype in the WHO classification ischaracterized by a specific cytogenetic abnormality,MDS with deletion 5q [8]. Although deletions of chro-mosome 5q represent the most common chromosomeabnormality in MDS [10], this category is defined nar-rowly as de novo MDS with the presence of an isolat-ed cytogenetic deletion involving band q31 of chromo-some 5, abundant atypical marrow megakaryocyteswith a normal or elevated platelet count, and a lowblast percentage [8].
Finally, in the WHO classification [8], CMML is elim-inated from the category of MDS and placed in a separategroup of disorders with features of both myelodysplasiaand myeloproliferative diseases.
As a result of these changes in classification, the WHOcriteria delineate 8 subtypes of MDS, in contrast to the 5 subtypes characterized in the FAB classification [8,9].
Pharmacologic treatment of myelodysplastic syndrome
Until recently, supportive interventions have been theaccepted standard of care for patients with MDS. Two
Identifying best practices in the monitoring and treatmentof iron overload in myelodysplastic syndrome
Alan F. List, MDH. Lee Moffitt Cancer Center and Research Institute, 12902 Magnolia Drive, SRB-4,
Tampa, Florida 33612-9497

8 Hematology/Oncology Clinics • Supplement 1
pharmacologic agents now show promise for patientswith this condition.
Azacitidine (Vidaza®, Pharmion Corporation, Boulder,Colorado) is the first agent approved for the treatment ofMDS by the US Food and Drug Administration (FDA)[11]. This agent is approved for the treatment of all 5 sub-types of MDS, as originally categorized by the FAB classi-fication criteria, and is appropriate for treatment of both
low- and high-risk patients. Azacitidine is believed to exertantineoplastic effects through hypomethylation of DNAand direct cytotoxicity to the myelodysplastic clone [11].Azacitidine is administered by daily SC injection for aminimum of 4 treatment cycles, each cycle consisting of adaily dose for 7 days every 4 weeks.
The second agent to receive FDA approval in MDS islenalidomide (Revlimid®, Celgene Corporation, Summit,
Table 1World Health Organization classification and criteria for myelodysplastic syndrome
Disease Blood findings Bone marrow findings
Refractory anemia (RA) Anemia Erythroid dysplasia onlyNo or rare blasts <5% blasts– <15% ringed sideroblasts
Refractory anemia with ringed sideroblasts (RARS) Anemia Erythroid dysplasia onlyNo blasts <5% blasts– ≥15% ringed sideroblasts
Refractory cytopenia with multilineage dysplasia Cytopenias (bicytopenia Dysplasia in ≥10% of cells(RCMD) or pancytopenia) in ≥2 myeloid cell lines
No or rare blasts <5% blastsNo Auer rods No Auer rods<1 � 109/L monocytes <15% ringed sideroblasts
Refractory cytopenia with multilineage dysplasia Cytopenias (bicytopenia Dysplasia in ≥10% of cells and ringed sideroblasts (RCMD-RS) or pancytopenia) in ≥2 myeloid cell lines
No or rare blasts <5% blastsNo Auer rods No Auer rods<1 � 109/L monocytes ≥15% ringed sideroblasts
Refractory anemia with excess blasts-1 (RAEB-1) Cytopenias Unilineage or multilineage dysplasia<5% blasts 5% to 9% blastsNo Auer rods No Auer rods <1 � 109/L monocytes –
Refractory anemia with excess blasts-2 (RAEB-2) Cytopenias Unilineage or multilineage dysplasia5% to 19% blasts 10% to 19% blastsAuer rods ± Auer rods ±<1 � 109/L monocytes –
Myelodysplastic syndrome, unclassified (MDS-U) Cytopenias Unilineage dysplasia in granulocytesNo or rare blasts or megakaryocytes No Auer rods <5% blasts
No Auer rods
MDS associated with isolated del (5q) Anemia Normal to increased megakaryocytes<5% blasts with hypolobated nucleiPlatelets normal <5% blastsor increased No Auer rods– Isolated del (5q)
(Reprinted from Vardiman HW et al. The World Health Organization [WHO] classification of the myeloid neoplasms. Blood2002;100[7]:2292–302; with permission.)
Hematology/Oncology Clinics • Supplement 1 9
New Jersey), an immunomodulatory agent that is struc-turally related to thalidomide. This agent has significanterythropoietic and cytogenetic remitting activity inMDS with the chromosome 5q deletion [12], the preciseindication for which FDA approval was granted. In aPhase II study of 148 patients with confirmed transfusion-dependent MDS and 5q deletion [13], 99 (67%) of patientsachieved red blood cell transfusion independence aftertreatment with lenalidomide, and 73% of respondersexperienced a cytogenetic response. Nearly half (45%)of responders had a complete cytogenetic response, andmore than a third (36%) of evaluable patients achievedcomplete pathologic response. Responses were durableand the median duration of transfusion independence hadnot been reached after a mean follow-up of 24 months(range, <8.6 to >89 weeks). Moderate to severe myelo-suppression was the most common adverse event, necessi-tating close laboratory monitoring during the initial 8 weeksof clonal suppression.
Recombinant human erythropoietin has assumed a pri-mary role in the initial management of anemia in MDSpatients with inappropriately low endogenous erythropoietinlevels and infrequent transfusion requirements [5,14]. Otheragents—including antithymocyte globulin, darbepoetinalpha, cyclosporine, sirolimus, and a tumor necrosis factorreceptor inhibitor—have recently demonstrated encourag-ing results in preliminary clinical trials [15–19].
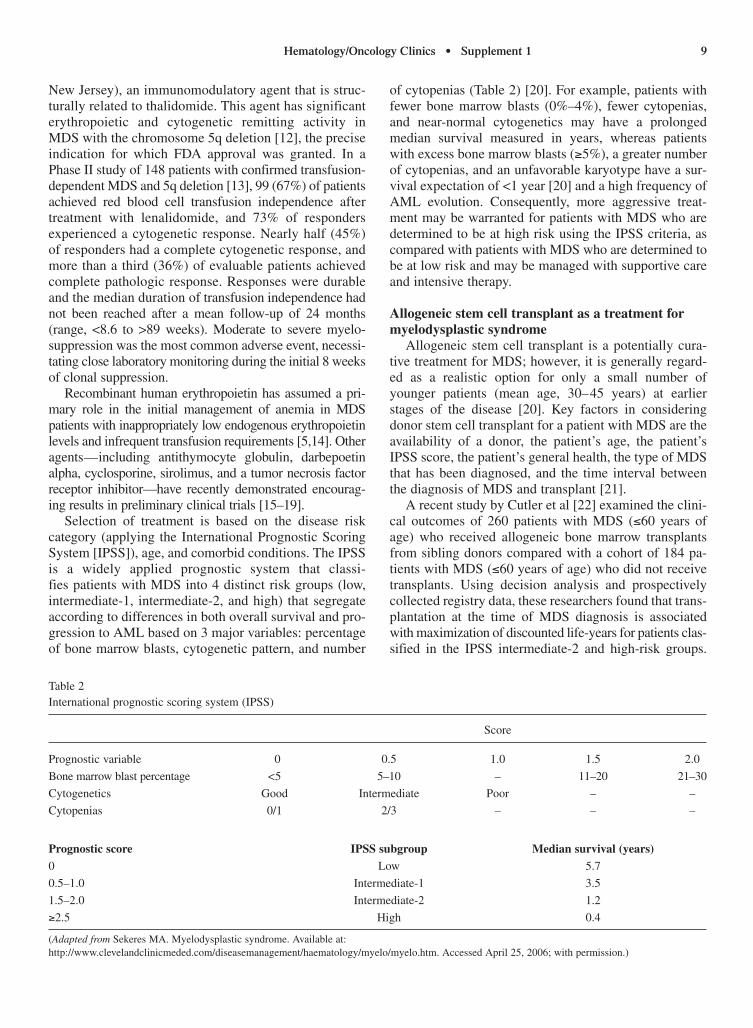
Selection of treatment is based on the disease risk category (applying the International Prognostic ScoringSystem [IPSS]), age, and comorbid conditions. The IPSSis a widely applied prognostic system that classi-fies patients with MDS into 4 distinct risk groups (low, intermediate-1, intermediate-2, and high) that segregateaccording to differences in both overall survival and pro-gression to AML based on 3 major variables: percentageof bone marrow blasts, cytogenetic pattern, and number
of cytopenias (Table 2) [20]. For example, patients withfewer bone marrow blasts (0%–4%), fewer cytopenias,and near-normal cytogenetics may have a prolongedmedian survival measured in years, whereas patientswith excess bone marrow blasts (≥5%), a greater numberof cytopenias, and an unfavorable karyotype have a sur-vival expectation of <1 year [20] and a high frequency ofAML evolution. Consequently, more aggressive treat-ment may be warranted for patients with MDS who aredetermined to be at high risk using the IPSS criteria, ascompared with patients with MDS who are determined tobe at low risk and may be managed with supportive careand intensive therapy.
Allogeneic stem cell transplant as a treatment formyelodysplastic syndrome
Allogeneic stem cell transplant is a potentially cura-tive treatment for MDS; however, it is generally regard-ed as a realistic option for only a small number ofyounger patients (mean age, 30–45 years) at earlierstages of the disease [20]. Key factors in consideringdonor stem cell transplant for a patient with MDS are theavailability of a donor, the patient’s age, the patient’sIPSS score, the patient’s general health, the type of MDSthat has been diagnosed, and the time interval betweenthe diagnosis of MDS and transplant [21].
A recent study by Cutler et al [22] examined the clini-cal outcomes of 260 patients with MDS (≤60 years ofage) who received allogeneic bone marrow transplantsfrom sibling donors compared with a cohort of 184 pa-tients with MDS (≤60 years of age) who did not receivetransplants. Using decision analysis and prospectivelycollected registry data, these researchers found that trans-plantation at the time of MDS diagnosis is associatedwith maximization of discounted life-years for patients clas-sified in the IPSS intermediate-2 and high-risk groups.
Table 2International prognostic scoring system (IPSS)
Score
Prognostic variable 0 0.5 1.0 1.5 2.0
Bone marrow blast percentage <5 5–10 – 11–20 21–30
Cytogenetics Good Intermediate Poor – –
Cytopenias 0/1 2/3 – – –
Prognostic score IPSS subgroup Median survival (years)0 Low 5.7
0.5–1.0 Intermediate-1 3.5
1.5–2.0 Intermediate-2 1.2
≥2.5 High 0.4
(Adapted from Sekeres MA. Myelodysplastic syndrome. Available at:http://www.clevelandclinicmeded.com/diseasemanagement/haematology/myelo/myelo.htm. Accessed April 25, 2006; with permission.)

10 Hematology/Oncology Clinics • Supplement 1
For patients classified in the IPSS low-risk or intermediate-1 risk groups, however, delaying transplantation until fur-ther disease progression is associated with maximumand quality-adjusted discounted life-years [22].
Iron overload may complicate the outcome of allo-geneic hematopoietic stem cell transplantation. In onestudy of bone marrow transplant recipients [23], 67 (88%)of 76 1-year survivors were found to have iron overloadwith high ferritin levels and high liver iron content. Inanother study, 20 (91%) of 22 liver biopsies performed15 to 110 days posttransplant showed histologic evidenceof siderosis [24]. Blood transfusion, prolonged dyseryth-ropoiesis, and increased iron absorption also contributeto the accumulation of iron which predisposes to hepaticdysfunction [25]. Although further studies on the clinicalconsequences of iron overload and therapeutic irondepletion in transplant recipients are needed, iron accu-mulation may contribute to the development of chronicliver disease [26]. In some patients, phlebotomy therapyafter transplant or adequate chelation therapy can helpminimize these risks and improve liver function [27].
Iron overload in patients with myelodysplastic syndrome
For patients with transfusion-dependent MDS, regularblood transfusions ameliorate symptoms and possiblyimprove quality of life. Unfortunately, long-term use ofblood transfusions may eventually lead to iron overload,a problem that commonly affects lower-risk patients withMDS in whom prolonged survival is expected [28,29].
MDS patients and others with refractory anemiasrequiring long-term blood transfusions develop ironoverload at a rate of ~0.5 mg/kg of body weight per day[30]. This iron accumulation ultimately leads to organcomplications that affect the liver, endocrine glands, and,most importantly, the heart. Complications of the heartcause cardiac failure and arrhythmias that account for~70% of deaths among patients with iron overload due tothalassemia major [30].
Studies of transfusion-dependent patients with thal-assemia or MDS have revealed the pathophysiology andadverse effects of chronic iron overload on the hepatic,endocrine, and cardiac systems. Specifically, when plas-ma iron content exceeds the binding capacity of availableplasma transferrin levels, non–transferrin-bound ironcombines with oxygen to form hydroxyl and oxygen radi-cals, both of which are toxic to cells and tissues. Theresults are lipid peroxidation and damage to cell mem-branes, protein, DNA, and organs [5,31,32].
The survival of patients with MDS worsens with thedevelopment of transfusion dependency. A study byMalcovati et al [33] found that although most clinicalfeatures at diagnosis are similar between transfusion-dependent and transfusion-independent patients withindefined subgroups, the effect of cytogenetics may sug-
gest the severity of bone marrow failure. Furthermore,the development of secondary iron overload (defined asserum ferritin >1000 ng/mL) adversely affects survival: a30% increase in hazard was found for every 500 ng/mLincrease in serum ferritin above the threshold. The authorsconcluded that therapeutic approaches that reduce transfu-sion needs or mitigate iron loading may impact survival inlower-risk patients. Treatment with iron chelating agentssuch as deferoxamine can reduce total body iron load.With prolonged treatment, sporadic reports suggest thatchelation may improve hematopoiesis [34].
Despite the importance of iron chelation therapy inavoiding iron toxicity in transfusion-dependent patientswith MDS, several factors may discourage patients andclinicians from pursuing this option. Patients with MDSare typically elderly. Although many elderly patientswith MDS receive blood transfusions, only a relativelysmall percentage of these patients receive iron chelationtherapy. Unlike patients with thalassemia major—whoare younger and have demonstrated benefits from chelationtherapy—little, if any, data are available on the benefits ofiron chelation in this older MDS population.
In addition, iron overload is widely underrecognizedamong patients with MDS, partly because of the insidi-ous nature of iron overload in light of the potentially devastating long-term effects of MDS. Furthermore, ironchelation therapy may not be initiated by cliniciansbecause of the typically advanced age of many patientswith MDS; a reduced life expectancy and high rate ofmedical fragility may apply for many of these patients.Patients and clinicians also may be uninformed about theneed for chelation therapy, as well as the potential long-term benefits of this treatment.
Estimating and monitoring iron overloadSerum ferritin levels are often used for estimating iron
burden, because these markers rise as iron stores increaseand fall as iron stores decrease, providing a rough esti-mate of total body iron stores over time [35]. Monitoringserum ferritin concentration at the time of diagnosis andat least every 3 months in patients receiving regularblood transfusions is prudent to help monitor iron over-load [35]. However, such measurements should be eval-uated in the context of overall MDS progression, basedon the understanding that serum ferritin levels may fluc-tuate owing to many factors, including inflammation,infection, hepatitis, hemolysis, or vitamin C deficiency[35,36]. It is appropriate, therefore, to consider thresholdlevels of serum ferritin within a wide range to allow forshort-term fluctuations and to provide flexibility withrespect to a patient’s transfusional status, as it may be therate of infusion rather than the actual number of infu-sions that may be more relevant to the decision to initiatechelation therapy [35]. Depending on a patient’s transfu-sion rate, chelation therapy should be considered when
Hematology/Oncology Clinics • Supplement 1 11
serum ferritin levels reach 1000 to 2000 ng/mL andshould be ongoing as long as transfusions continue andiron overload remains a risk [35].
Magnetic resonance imaging (MRI) is a noninvasivemethod of estimating organ iron load. Although in prin-ciple MRI can be used to quantify iron stores whereverthey exist in the body, current variability in its quantita-tive accuracy limits its usefulness as a definitive diag-nostic test. Furthermore, lack of availability and pooraccessibility of MRI, as well as cost factors, can be bar-riers to the widespread use of MRI for patients withMDS. Nevertheless, MRI can be used to detect iron over-load and monitor iron chelation therapy. Other imagingmodalities that may become more available to assess ironoverload include computed tomography, nuclear reso-nance imaging, and the superconducting quantum inter-ference device (SQUID).
Encouraging best practices for chelation therapy ofiron overload in myelodysplastic syndrome
Chelation therapy is considered the standard of carefor patients with iron overload. In fact, current guidelinesfrom the NCCN regarding the care of patients with MDSrecommend iron chelation therapy for those who receive>20 units of packed red blood cells [5]. Barriers to chela-tion therapy remain, however, because of the drawbacksinherent in the chelation treatment options currentlyavailable in the United States. Those patients most likelyto suffer from morbidity and mortality related to MDSand problems associated with iron overload are the el-derly, who often have comorbid conditions such as heartdisease and liver damage. This vulnerable populationmay benefit from iron chelation therapy, despite its draw-backs, with maximum benefit occurring when treatmentis initiated early in the course of the disease.
NCCN guidelines on supportive care for patientswith myelodysplastic syndrome
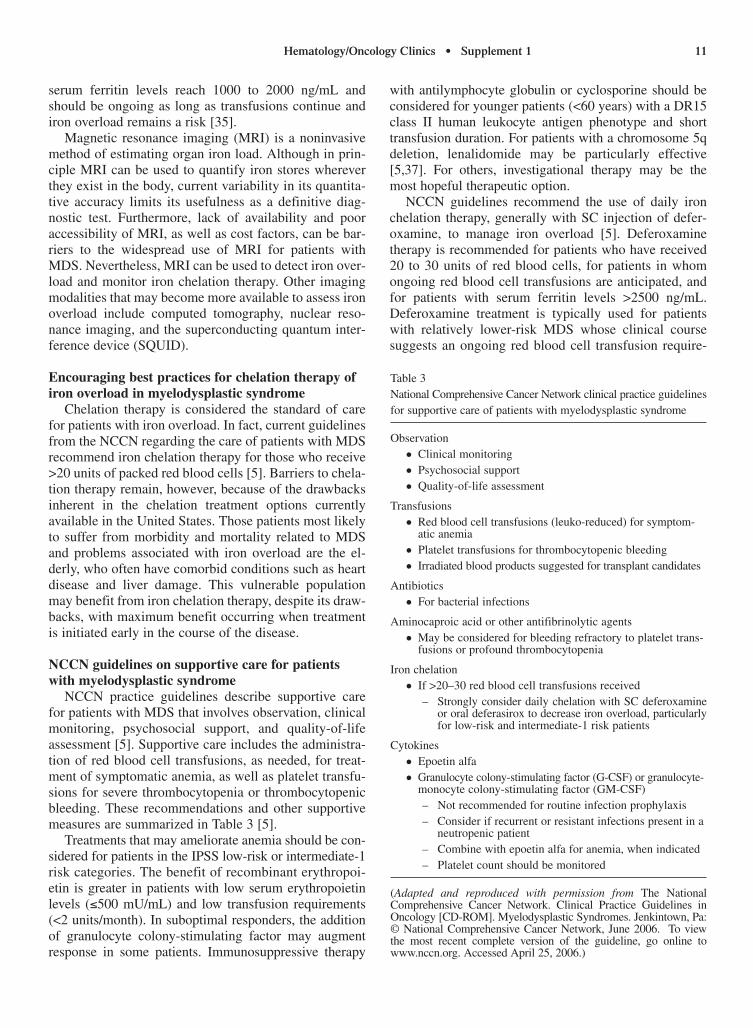
NCCN practice guidelines describe supportive carefor patients with MDS that involves observation, clinicalmonitoring, psychosocial support, and quality-of-lifeassessment [5]. Supportive care includes the administra-tion of red blood cell transfusions, as needed, for treat-ment of symptomatic anemia, as well as platelet transfu-sions for severe thrombocytopenia or thrombocytopenicbleeding. These recommendations and other supportivemeasures are summarized in Table 3 [5].
Treatments that may ameliorate anemia should be con-sidered for patients in the IPSS low-risk or intermediate-1risk categories. The benefit of recombinant erythropoi-etin is greater in patients with low serum erythropoietinlevels (≤500 mU/mL) and low transfusion requirements(<2 units/month). In suboptimal responders, the additionof granulocyte colony-stimulating factor may augmentresponse in some patients. Immunosuppressive therapy
with antilymphocyte globulin or cyclosporine should beconsidered for younger patients (<60 years) with a DR15class II human leukocyte antigen phenotype and shorttransfusion duration. For patients with a chromosome 5qdeletion, lenalidomide may be particularly effective[5,37]. For others, investigational therapy may be themost hopeful therapeutic option.
NCCN guidelines recommend the use of daily ironchelation therapy, generally with SC injection of defer-oxamine, to manage iron overload [5]. Deferoxaminetherapy is recommended for patients who have received20 to 30 units of red blood cells, for patients in whomongoing red blood cell transfusions are anticipated, andfor patients with serum ferritin levels >2500 ng/mL.Deferoxamine treatment is typically used for patientswith relatively lower-risk MDS whose clinical coursesuggests an ongoing red blood cell transfusion require-
Table 3 National Comprehensive Cancer Network clinical practice guidelinesfor supportive care of patients with myelodysplastic syndrome
Observation● Clinical monitoring● Psychosocial support● Quality-of-life assessment
Transfusions● Red blood cell transfusions (leuko-reduced) for symptom-
atic anemia● Platelet transfusions for thrombocytopenic bleeding● Irradiated blood products suggested for transplant candidates
Antibiotics● For bacterial infections
Aminocaproic acid or other antifibrinolytic agents● May be considered for bleeding refractory to platelet trans-
fusions or profound thrombocytopenia
Iron chelation● If >20–30 red blood cell transfusions received
– Strongly consider daily chelation with SC deferoxamineor oral deferasirox to decrease iron overload, particularlyfor low-risk and intermediate-1 risk patients
Cytokines ● Epoetin alfa● Granulocyte colony-stimulating factor (G-CSF) or granulocyte-
monocyte colony-stimulating factor (GM-CSF)– Not recommended for routine infection prophylaxis– Consider if recurrent or resistant infections present in a
neutropenic patient– Combine with epoetin alfa for anemia, when indicated– Platelet count should be monitored
(Adapted and reproduced with permission from The NationalComprehensive Cancer Network. Clinical Practice Guidelines inOncology [CD-ROM]. Myelodysplastic Syndromes. Jenkintown, Pa:© National Comprehensive Cancer Network, June 2006. To view the most recent complete version of the guideline, go online towww.nccn.org. Accessed April 25, 2006.)

12 Hematology/Oncology Clinics • Supplement 1
ment, and for those with cardiac or hepatic comorbidi-ties. For patients who require chronic red blood celltransfusions, ongoing assessments relating to the func-tion of the heart, liver, and pancreas should be made rou-tinely. Serum ferritin monitoring is also recommended,with target ferritin levels <1000 ng/mL. NCCN guide-lines recognize, however, that serum ferritin measure-ments are less precise than iron overload evaluationbased on SQUID or hepatic MRI evaluation of hepaticiron content.
Iron chelating agents: advantages and disadvantages Two iron chelating agents are currently approved by
the FDA for the treatment of iron overload: parenteraldeferoxamine (Desferal®, Novartis PharmaceuticalCorporation, East Hanover, New Jersey) [38] and oraldeferasirox (Exjade®, Novartis) [39]. A third agent, oraldeferiprone (Ferriprox™, ApoPharma, Piding, Germany)[40], is currently undergoing Phase III clinical trials inthe United States. The oral availability of these neweragents may offer greater compliance and better outcomesin the treatment of iron overload. Clinical trials in pa-tients with MDS are under way to determine the role ofdeferasirox and deferiprone, alone and in combinationwith deferoxamine, for treating iron overload.
Deferoxamine Deferoxamine (also known as desferrioxamine B) is
derived from ferrioxamine B, a sideramine isolated in1960 from Streptomyces pilosus. Whereas its high bindingaffinity for trivalent iron is clinically effective in removingexcess iron from blood and tissue [41], the mechanism ofaction of this agent is not fully understood [34].
The use of deferoxamine is supported by clinical evi-dence that optimal therapy with this agent can arrest pro-gression of iron overload and prevent early death fromthis condition [42–44]. However, deferoxamine treat-ment requires parenteral administration because of itslarge molecular size, poor oral bioavailability, and shortplasma half-life, making it necessary for patients toreceive lengthy infusions several times per week [38,45].According to NCCN guidelines [5], deferoxamine can beadministered in 1- to 2-g doses by overnight SC infusion5 to 7 nights per week, or as 1- to 2-g SC bolus infusionBID. This agent also may be given IM at intervals of 4 to 12 hours [38]. Careful monitoring of eye, ear, andrenal function is necessary during treatment with defer-oxamine. Toxicities associated with deferoxamine therapyinclude (1) retinal and optic nerve disturbances (risk maybe higher in patients with diabetes or other factors affect-ing the blood-retinal barrier); (2) high-frequency sen-sorineural hearing loss; (3) effects on growth and bone(including growth retardation and bone abnormalities);(4) localized reactions (such as skin reddening and sore-ness at the SC infusion site); and (5) increased risk of
infection (eg, Yersinia infection can occur in patients withiron overload who receive deferoxamine therapy) [46].When using deferoxamine therapy, ensure that doses donot exceed 40 mg/kg per day; be aware of concerns regard-ing the introduction of deferoxamine therapy to very youngpatients (<3 years of age); and follow guidelines to reducethe dose of deferoxamine as iron loading falls [46].
Because of the demanding regimen of parenteral infu-sions, many patients with iron overload succumb toorgan complications as a consequence of poor compli-ance with deferoxamine maintenance therapy [44].Furthermore, because of the practical difficulties ofrepeatedly administering lengthy SC infusions of defer-oxamine to MDS patients who generally are older andwho may have a variety of comorbidities, initiation ofparenteral chelation therapy is often delayed owing toreservations on the part of the patient and physician.Undertreatment of iron overload may occur due to thelack of therapeutic options that are determined to be tol-erable for a particular patient. Consequently, compliancewith parenteral deferoxamine regimens represents amajor clinical challenge.
Deferasirox Deferasirox is an oral iron chelator that is rapidly
absorbed and can be administered QD. It is a tridentateiron chelator, requiring 2 molecules to stabilize andchelate each molecule of iron [44]. In clinical trials, treat-ment with deferasirox achieved a negative iron balance inpatients with iron overload at rates comparable to thoseachieved in patients receiving deferoxamine [44,47].Investigations to date indicate that deferasirox is effectivein patients with various chronic anemias, including MDS,and its pharmacokinetic, tolerability, and safety profilesare suitable for long-term use [44,48–51]. This agent iswell tolerated in children as young as 2 years of age, withonly 3% of subjects in this age group withdrawing fromclinical studies due to adverse effects [52]. Deferasiroxwas recently approved by the FDA for the treatment ofall forms of iron overload. Given its safety and efficacyprofile, this agent is expected to offer greater compliancefor patients with lower-risk MDS and, as a consequence,possibly mitigate the adverse effect of transfusiondependence on survival expectations. Phase II studies are under way to evaluate the possible hematopoietic-promoting effect of deferasirox in patients with MDSwith prolonged daily administration.
Deferiprone Deferiprone is an orally active iron chelator licensed
in 43 countries for the treatment of iron overload inpatients for whom deferoxamine treatment has provedintolerant or inadequate. Deferiprone has a less efficientiron-binding profile than deferoxamine, with 3 mole-cules of deferiprone required to bind 1 molecule of triva-

Hematology/Oncology Clinics • Supplement 1 13
lent iron; therefore, relatively large doses are necessaryto achieve a negative iron balance in most patients [44].
Recent data suggest that this agent may be better thandeferoxamine in extracting iron from cardiac andendocrine tissue because of improved intracellular pene-tration that protects these tissues from toxicity related toiron overload [30]. Large, well-designed studies are need-ed to clarify the comparative utility of deferoxamine ver-sus deferiprone. Deferiprone may also prove useful incombination with deferasirox [30,44]. Patients receivingdeferiprone, especially those with diabetes, are atincreased risk for agranulocytosis and arthropathy, as wellas zinc deficiency [30]. These adverse effects may lead todiscontinuation of the drug in 5% to 10% of patients [30].
Conclusions Despite the ability of iron chelation therapy to lessen
or delay the complications of iron overload in transfusion-dependent patients with MDS, several factors have dis-couraged patients and clinicians from pursuing thisoption. Clinicians may not initiate iron chelation therapybecause of the advanced age and medical fragility ofmany of their MDS patients. Patients and clinicians alsomay be uninformed about the need for chelation therapyand the long-term benefits of this treatment. Other barri-ers relate to potential side effects and the practical draw-backs inherent in parenteral chelation treatment.
Because of the potential toxic effects of iron on theheart, liver, and other organs, the patients most likely tosuffer from the morbidity and mortality associated withiron overload in MDS are elderly patients with comorbidcardiac and hepatic conditions. This vulnerable popula-tion will benefit most from the development of new ironchelation agents that are safe, effective, and orally avail-able. The introduction of the oral chelators deferasirox inthe United States and deferiprone in Europe offers moreconvenient and effective iron chelation therapy. Clinicaltrials in MDS are under way to determine the role ofthese agents, alone and in combination with deferox-amine, for treating iron overload in MDS. Nonetheless,early intervention appears appropriate to maximize clin-ical benefit and mitigate the negative effects of iron over-load on survival expectation in lower-risk patients.
AcknowledgmentThe author wishes to thank Nathalie Smith, MSN, RN,
for her help in the preparation of this manuscript.
References[1] Miller KB, Kim K, Morrison FS, Winter JN, Bennett JM, Neiman RS,
et al. The evaluation of low-dose cytarabine in the treatment of
myelodysplastic syndromes: a phase-III intergroup study. Ann Hematol
1992;65:162-8. Erratum in: Ann Hematol 1993;66:164.
[2] Greenberg PL, Young NS, Gattermann N. Myelodysplastic syndromes.
Hematology January 2002:136–61.
[3] Mangi MH, Mufti GJ. Primary myelodysplastic syndromes: diagnos-
tic and prognostic significance of immunohistochemical assessment
of bone marrow biopsies. Blood 1992;79:198–205.
[4] List AF, Vardiman J, Issa JJ, DeWitte TM. Myelodysplastic syn-
dromes. Hematology 2004–American Society for Hematology
Education Program Booklet. 2004:297–317.
[5] National Comprehensive Cancer Network. Clinical Practice
Guidelines in Oncology—v.2.2006. Myelodysplastic syndromes.
Available at: http://www.nccn.org/professionals/physician_gls/PDF/
mds.pdf. Accessed April 25, 2006.
[6] Aul C, Gattermann N, Schneider W. Age-related incidence and other
epidemiological aspects of myelodysplastic syndromes. Br J Haematol
1992;82:358–67.
[7] Maynadie M, Verret C, Moskovtchenko P, Mugneret F, Petrella T,
Caillot D, et al. Epidemiological characteristics of myelodysplastic
syndrome in a well-defined French population. Br J Cancer 1996;
74:288–90.
[8] Vardiman JW, Harris NL, Brunning RD. The World Health
Organization (WHO) classification of the myeloid neoplasms. Blood
2002;100:2292–302.
[9] Bernstein SH, Burnetto VL, Davey FR, Wurster-Hill D, Mayer RJ,
Stone RM, et al. Acute myeloid leukemia-type chemotherapy for
newly diagnosed patients without antecedent cytopenias having
myelodysplastic syndrome as defined by French-American-British
criteria: a Cancer and Leukemia Group B study. J Clin Oncol 1996;
14:2486–94.
[10] Olney HJ, Le Beau MM. The cytogenetics and molecular biology of
myelodysplastic syndromes. In: Bennett JM, ed. The Myelodysplastic
Syndromes: Pathobiology and Clinical Management. New York, NY:
Marcel Dekker, Inc; 2002:89–120.
[11] Vidaza Prescribing Information. Boulder, Colo: Pharmion Corporation;
May 18, 2004. Available at: http://www.vidaza.com. Accessed
October 28, 2005.
[12] List A, Kurtin S, Roe DJ, Buresh A, Mahadevan D, Fuchs D, et al.
Efficacy of lenalidomide in myelodysplastic syndromes. N Engl J Med
2005;352:549–57.
[13] List AF, Dewald G, Bennet J, Giagounadis A, Raza A, Feldman E, et
al. Hematologic and cytogenetic (CTG) response to lenalidomide (CC-
5013) in patient transfusion-dependent (TD) myelodysplastic syndrome
(MDS) and chromosome 5 deletion: results of the multicenter MDS-
003 study. Paper presented at: American Society of Clinical Oncology
Annual Meeting; May 14–15, 2005; Orlando, Fla.
[14] Italian Cooperative Study Group for rHuEpo in Myelodysplastic
Syndromes. A randomized double-blind placebo-controlled study with
subcutaneous recombinant human erythropoietin in patients with low-
risk myelodysplastic syndromes. Br J Haematol 1998;103:1070–4.
[15] Molldrem JJ, Leifer E, Bahceci E, Saunthararajah Y, Rivera M,
Dunbar C, et al. Antithymocyte globulin for treatment of the bone
marrow failure associated with myelodysplastic syndromes. Ann
Intern Med 2002;137:156–63.
[16] Musto P, Lanza F, Balleari E, Grossi A, Falcone A, Sanpaolo G, et al.
Darbepoetin alpha for the treatment of anaemia in low–intermediate
risk myelodysplastic syndromes. Br J Haematol 2005;128:204–9.
[17] Ogata M, Ohtsuka E, Imamura T, Ikewaki J, Ogata Y, Kohno K, et al.
Response to cyclosporine therapy in patients with myelodysplastic
syndrome: a clinical study of 12 cases and literature review. Int J
Hematol 2004;80:35–42.
[18] Platzbecker U, Haase M, Herbst R, Hanel A, Voigtmann K, ThiedeCH, et al. Activity of sirolimus in patients with myelodysplastic syndrome—results of a pilot study. Br J Haematol 2005;128:625–30.
[19] Maciejewski JP, Risitano AM, Sloand EM, Wisch L, Geller N, BarrettJA, et al. A pilot study of the recombinant soluble human tumournecrosis factor receptor(p75)-Fc fusion protein in patients withmyelodysplastic syndrome. Br J Haematol 2002;117:119–26.Erratum in: Br J Haematol 2002;117:1002.
[20] Sekeres MA. Myelodysplastic syndrome. The Cleveland ClinicFoundation Web site. Available at: http://www.clevelandclinicmeded.com/diseasemanagement/hematology/myelo/myelo.htm. AccessedApril 25, 2006.
[21] Myelodysplastic syndromes. Leukemia Research Fund 2005.Available at: http://www.lrf.org/uk/en/2/infdispatmye.html. AccessedApril 25, 2006.
[22] Cutler CS, Lee SJ, Greenberg P, Deeg HJ, Perez WS, Anasetti C, etal. A decision analysis of allogeneic bone marrow transplantation forthe myelodysplastic syndromes: delayed transplantation for low-riskmyelodysplasia is associated with improved outcome. Blood 2004;104:579–85.
[23] McKay PJ, Murphy JA, Cameron S, Burnett AK, Campbell M,Tansey P, et al. Iron overload and liver dysfunction after allogeneic orautologous bone marrow transplantation. Bone Marrow Transplant1996;17:63–6.
[24] Iqbal M, Creger RJ, Fox RM, Cooper BW, Jacobs G, Stellato TA, et al. Laparoscopic liver biopsy to evaluate hepatic dysfunction inpatients with hematologic malignancies: a useful tool to effectchanges in management. Bone Marrow Transplant 1996;17:655–62.
[25] Tichelli A, Socie G. Considerations for adult cancer survivors.Hematology (American Society of Hematology Education Program)2005:516–22.
[26] Strasser SI, Sullivan KM, Myerson D, Spurgeon CL, Storer B, SchachHG, et al. Cirrhosis of the liver in long-term marrow transplant sur-vivors. Blood 1999;93:3259–66.
[27] Engelhardt R, Dürken M, Nielsen P, Newbauer F, Haberhausen M,Hiller J, et al. Biomagnetic liver susceptometry in long-term survivorsafter bone marrow or stem cell transplantation. Available at: http://biomag2000.hut.fi/papers/1015.pdf. Accessed January 20, 2006.
[28] Cortelezzi A, Cattaneo C, Cristiani S, Duca L, Sarina B, Deliliers GL,et al. Non-transferrin-bound iron in myelodysplastic syndromes: a marker of ineffective erythropoiesis? Hematol J 2000;1:153–8.
[29] Kwiatkowski JL, Cohen AR. Iron chelation therapy in sickle-cell dis-ease and other transfusion-dependent anemias. Hematol Oncol ClinNorth Am 2004;18:1355–77, ix.
[30] Hoffbrand AV. Deferiprone therapy for transfusional iron overload.Best Pract Res Clin Haematol 2005:18:299–317.
[31] Hershko C, Link G, Cabantchik I. Pathophysiology of iron overload.Ann N Y Acad Sci 1998;850:191.
[32] Farquhar MJ, Bowen DT. Oxidative stress and the myelodysplasticsyndromes. Int J Hematol 2003;77:342–50.
[33] Malcovati L, Port MG, Pascutto C, Invernizzi R, Boni M, Travaglino E,et al. Prognostic factors and life expectancy in myelodysplastic syn-dromes classified according to WHO criteria: a basis for clinical deci-sion making. J Clin Oncol 2005;23:7594–603.
[34] Jensen PD, Heickendorff L, Pedersen B, Bendix-Hausen K, JensenFT, Christensen T, et al. The effect of iron chelation on haemopoiesisin MDS patients with transfusional iron overload. Br J Haematol1996;94:288–99.
[35] Gattermann N, Porter J, Lopes LF, Seymour J. Iron overload inmyelodysplastic syndromes. Hematol/Oncol Clinics 2005:19(Suppl 1):1–25.
[36] Piga A. Monitoring of iron chelation and iron overload. The Institut furMedizinische Genetik Web site. EUMEDIS, Thalassemia, Monitoringiron overload. Available at: http://www.charite.de/ch/medgen/.Accessed April 27, 2006.
[37] Revlimid® (lenalidomide) Prescribing Information. Summit, NJ:Celgene Corporation.
[38] Desferal® (deferoxamine) Prescribing Information. East Hanover, NJ:Novartis Pharmaceuticals Corporation; 2002.
[39] Exjade® (deferasirox) Prescribing Information. East Hanover, NJ:Novartis Pharmaceuticals Corporation; 2005.
[40] Ferriprox® (deferiprone) Web site. Available at: http://www.ferriprox.com/Patient/aboutferriprox/UsingFerriprox.asp. AccessedApril 27, 2006.
[41] Keberle H. The biochemistry of deferoxamine and its relation to ironmetabolism. Ann N Y Acad Sci 1964;119:758–68.
[42] Olivieri NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGeeA, et al. Survival in medically treated patients with homozygous beta-thalassemia. N Engl J Med 1994;331:574–8.
[43] Olivieri NF, Brittenham GM. Iron-chelating therapy and the treatmentof thalassemia. Blood 1997;89:739–61.
[44] Cappellini MD. Iron-chelating therapy with the new oral agentICL670 (Exjade). Best Pract Res Clin Haematol 2005;18:289–98.
[45] Miskin H, Yaniv I, Berant M, Hershko C, Tamary H. Reversal of car-diac complications in thalassemia major by long-term intermittentdaily intensive iron chelation. Eur J Haematol 2003;70:398–403.
[46] Kushner JP, Porter JP, Olivieri NF. Secondary iron overload.Hematology 2001:47–61.
[47] Piga A, Galanello R, Cappellini MD, Forni G, Opitz H, Ford JM, et al.Phase II study of oral chelator ICL670 in thalassemia patients withtransfusional iron overload: efficacy, safety, pharmacokinetics (PK)and pharmacodynamics (PD) after 6 months of therapy. Blood 2002;100(Suppl 11):5a. Abstract 5.
[48] Piga A, Galanello R, Foschini ML, Zappu A, Bordone E, Longo F, etal. Once-daily treatment with the oral iron chelator ICL670: results of a phase II study in pediatric patients with β-thalassemia major.Presented at: American Society of Hematology 46th Annual Meeting;December 4–7, 2004; San Diego, Calif. Poster 3614.
[49] Galanello R, Piga A, Alberti D, Rouan MC, Bigler H, Sechaud R. Safety,tolerability, and pharmacokinetics of ICL670, a new orally active iron-chelating agent in patients with transfusion-dependent iron overload due to beta-thalassemia. J Clin Pharmacol 2003;43:565–72.
[50] Nisbet-Brown E, Olivieri NF, Giardina PJ, Grady RW, Neufeld EJ,Sechaud R, et al. Effectiveness and safety of ICL670 in iron-loadedpatients with thalassaemia: a randomised, double-blind, placebo-controlled, dose-escalation trial. Lancet 2003;361:1597–602.
[51] Porter J, Vichinsky E, Rose C, Piga A, Olivieri N, Gattermann N, etal. A phase II study with ICL670, a once-daily oral iron chelator, inpatients with various transfusion-dependent anemias and iron over-load. Presented at: American Society of Hematology 46th AnnualMeeting; December 4–7, 2004; San Diego, Calif. Poster 3193.
[52] Cappellini MD, Bejaoui M, Perrotta S, Agaoglu L, Kattamis A,Giardina P, et al. Phase III evaluation of once-daily, oral therapy withICL670 versus deferoxamine in patients with β-thalassemia and transfusional hemosiderosis. Presented at: American Society ofHematology 46th Annual Meeting; December 4–7, 2004; San Diego,Calif. Poster 3619.
Address correspondence to: Alan F. List, MD, H. Lee Moffitt Cancer Center and Research Institute, 12902 MagnoliaDrive, SRB-4, Tampa, FL 33612-9497.
14 Hematology/Oncology Clinics • Supplement 1

Iron overload is a serious concern in addressing the needs of patients with myelodysplastic syndrome (MDS).Although blood transfusions are an effective intervention that often restores some measure of function and improves thequality of life for many of these patients during the course of their care, multiple transfusions over time may lead to ironoverload. For some patients, iron overload can result in damage to the heart, endocrine glands, and/or liver, as well ascontribute to the morbidity and mortality of patients with MDS. Yet, iron overload is often underdiagnosed in clinicalpractice. Widespread awareness of the potential impact of iron overload in patients with MDS is clearly warranted.
Physicians around the globe face a number of challenges in determining “best practices” to assess and treat ironoverload in patients with MDS. A series of meetings with leading experts in the field and physicians who treat patientswith MDS was recently convened; one meeting held in Japan during May 2005 included participants from Europe,Latin America, and Asia-Pacific, and one meeting held in the United States during November 2005 included physi-cians from various health care facilities who collectively have provided care to thousands of patients with MDS overthe years. Participants’ opinions expressed during these meetings reflected a diversity of perspectives on many issues.This commentary attempts to highlight some of the key discussion points of these meetings, serving as a communica-tions tool to encourage further conversations in the physician community about the need to take a close look at clini-cal issues relating to iron overload in this population.
The primary focus of each meeting was to share information about various aspects relating to the diagnosis, monitor-ing, and management of iron overload in patients with MDS. Topics included discussion on the implications of iron overload in MDS; the use of chelation agents in the treatment of iron overload in patients with transfusion-dependentMDS; the basic criteria to determine how this patient population can benefit from chelation therapy; the utility ofapplying guidelines established by the National Comprehensive Cancer Network in clinical practice; and the needto raise awareness about the role of iron overload and chelation therapy among physicians who provide care topatients with MDS.
The following statements summarize the key discussion points generated from the meeting held in Japan [1].● The clinical consequences of untreated or inadequately managed iron overload in MDS are potential cardiac,
hepatic, and endocrine complications.● The goal of chelation therapy in MDS patients with iron overload is to prevent complications of iron overload
and to improve survival.● Chelation therapy is highly likely to be clinically important in a subgroup of patients with MDS.● Body iron stores should be assessed at diagnosis of MDS and at regular intervals thereafter, depending on
transfusion rate.● The tools used for diagnosis and monitoring of iron overload should be serum ferritin, transferrin saturation,
and liver magnetic resonance imaging (MRI).● Iron overload should be monitored at least every 3 months in patients receiving transfusions.● The initiation of chelation therapy should be considered in MDS patients when serum ferritin levels reach
1000 to 2000 ng/mL, depending on the transfusion rate.● Chelation therapy should continue as long as transfusion therapy continues and as long as iron overload
remains clinically relevant.● MDS patients likely to benefit most from treatment of iron overload include: transfusion-dependent
patients; patients with serum ferritin levels >1000 to 2000 ng/mL or other evidence of significant tissue ironoverload; patients with low-risk MDS (as defined by the International Prognostic Scoring System as low orintermediate-1 or as defined by the World Health Organization [WHO] classification system as refractory anemia,refractory anemia with ringed sideroblast, or 5q-syndrome [which is a cytogenetic abnormality that occurs in only
Commentary
Considerations in the care of patients with myelodysplastic syndrome who have iron overload
16 Hematology/Oncology Clinics • Supplement 1
a small proportion of the MDS patient population]); patients with documented stable MDS; patients free ofcomorbidities that severely limit prognosis; and candidates for allograft.
Participants also acknowledged that the current knowledge base about iron overload in MDS is inadequate. Furtherresearch using clinical trials and/or patient registries is needed to make advances in this area. Specific areas of researchwere identified to address a range of unanswered questions in the minds of these participants. These areas includeimproved methods for assessing iron burden in particular organs; objective evidence regarding the effect of iron over-load in MDS; and further clarification on the efficacy and safety of iron chelators in the MDS population, as well asstudies on the compatibility of iron chelation therapy with other therapies that are administered to patients with MDS.
Participants in the meeting held in the United States expressed a wide range of opinions on similar discussionpoints. As background, it is useful to point out that MDS affects between 12,000 and 20,000 people each year inthe United States, which translates to a rate of 22 to 45 people per 100,000 >70 years of age [2]. An estimated30,000 to 40,000 people are living with MDS in this country, with a majority of these patients determined to haveindolent MDS (which is generally defined as having <5% myeloblasts in the bone marrow) [2]. MDS is as preva-lent as other common hematologic malignancies of older adults, such as multiple myeloma and chronic lympho-cytic leukemia [3].
Discussion points among the participants in the US meeting included the need for objective data that clearly definethe role of chelation therapy in MDS. This group identified 4 treatment goals of chelation therapy in MDS patientswith iron overload: prevention of complications; treatment of complications; improvement of cytopenia; and improve-ment of survival. Potential cardiac, hepatic, and endocrine complications are regarded as the clinical consequences ofnot using iron chelation in MDS.
While noting the limitations of using serum ferritin measurements alone to make clinical decisions, many of theparticipants consider the need to assess serum ferritin in patients with MDS at the time of diagnosis and at follow-upvisits, as clinically indicated. Both serum ferritin testing and noninvasive imaging modalities (for example, T2-MRIwhen accessible) are identified as potentially useful in the diagnosis and monitoring of iron overload; tissue biopsyand serum ferritin testing are the most frequently used biomarkers in clinical practice among these physicians. Formany participants, the decision to start chelation therapy is based on the presence of organ dysfunction that is docu-mented as related to iron overload, with continuation of chelation therapy depending on how long iron overload con-tinues to be a clinical problem. Evidence of iron-related end-organ dysfunction is an important factor—along withother individualized considerations such as the perceived life expectancy—that helps these physicians determine thepotential benefits from chelation therapy for their patients with MDS.
A number of specific areas for further research of special interest to this US group were identified. More studies areneeded to provide objective evidence on the impact of iron chelation on MDS-related disease complications includingsurvival; the role of chelation before and after allogeneic transplant; the impact of iron overload on survival and qualityof life; and the impact of iron chelation on MDS-related cytopenias. In addition, further studies can provide a better under-standing of any potential impact when patients with MDS receive both iron chelation therapy and other concomitantlyadministered drugs, as well as more data on any adverse events relating to various combinations of therapies. Other areasof interest include optimal methods of assessing end-organ damage from iron overload; the role of additional agentsin optimizing iron mobilization; the impact of infectious complications; and the impact from concomitantly chelatedtrace elements.
Findings from 2 studies have been useful in addressing the need for additional information in caring for patientswith MDS who have iron overload. A study by Jensen et al [4] examined the long-term (defined as up to 60 months)follow-up data of 11 patients with MDS with transfusional iron overload (before and after iron chelation therapy); thisdata included an assessment of peripheral blood counts and hemoglobin requirements of these patients and includedthe morphological and cytogenetical bone marrow changes observed during iron chelation, as well as erythroid mar-row activity. Researchers concluded that iron chelation therapy in MDS patients with transfusional iron overload mayinduce blood transfusion independence if the patients are treated for a sufficiently long period of time.
An important study by Malcovati et al [5] was designed to evaluate the prognostic value of the new World HealthOrganization (WHO) classification system for MDS and assess the role of primary prognostic factors in MDS accord-ing to WHO subgroups, as well as estimate mortality and life expectancy in these groups of patients with MDS. In thisretrospective study, a total of 467 patients who were diagnosed with MDS between 1992 and 2002 were evaluated forclinical and hematologic features at time of diagnosis, overall survival, and progression to leukemia. Researchersfound that transfusion-dependent patients experienced a significantly shorter survival rate as compared with patientswho did not require transfusions (P < 0.001). Furthermore, researchers observed that the development of secondaryiron overload significantly worsened the survival of transfusion-dependent patients (P = 0.003). These findings suggest
Hematology/Oncology Clinics • Supplement 1 17
that efforts to reduce transfusion needs using various therapeutic approaches—as well as interventions that can helpprevent iron overload—may lead to improved outcomes in patients with MDS.
Clinical decision making among physicians who provide care for patients with MDS continues to be a dauntingchallenge. The availability of effective therapeutic modalities and the timing of specific interventions are critical fac-tors to consider. Complexities are inherent in caring for these patients, given the natural history of MDS that can rangefrom indolent conditions spanning over a number of years to forms that rapidly progress to leukemia. Widespreadawareness of the potential impact of iron overload in patients with MDS—in combination with more research in thisarea—will help physicians in clinical practice as they make decisions on an individualized basis.
References[1] Gottermann N, ed. Iron overload in myelodysplastic syndromes. Hematol/Oncol Clin 2005;19:18–25.
[2] Sekeres MA. Myelodysplastic syndrome. The Cleveland Clinic Foundation Web site. Available at: http://www.clevelandclinicmeded.com/diseasemanagement/hematology/myelo/myelo.htm. Accessed January 20, 2006.
[3] Greenberg P. Myelodysplastic syndrome. In: Hoffman R, Benz E, Shattil S, et al, eds. Hematology: Basic Principles andPractice 3rd Edition. New York, NY: Churchill Livingston; 2000.
[4] Jensen PD, Heickendorff L, Pedersen B, Bendix-Hansen K, Jensen FT, Christensen T, et al. The effect of iron chelation onhaemopoiesis in MDS patients with transfusional iron overload. Br J Haematol 1996;94(2):288–99.
[5] Malcovati L, Porta MG, Pascutto C, Invernizzi R, Boni M, Travaglino E, et al. Prognostic factors and life expectancy inmyelodysplastic syndromes classified according to WHO criteria: a basis for clinical decision making. J Clin Oncol2005;23(30):7594–603.

Hematology/Oncology Clinics • Supplement 1 19
1. The myelodysplastic syndrome (MDS) refers to agroup of hematologic stem cell disorders that arecharacterized by _______.a. ineffective blood production b. cytopenias and cytologic dysplasiac. variable risk for leukemia transformationd. both a and c e. all of the above
2. Most patients with MDS eventually develop whichof the following morbidities?a. Infectious complicationsb. Complications from blood cell deficienciesc. Cardiovascular diseased. Acute leukemiae. Either a, b, or d
3. The annual incidence rate of MDS for all agegroups is approximately _______ per 100,000 people.a. 1 to 2 b. 3 to 4c. 9 to 10 d. 14 to 15
4. The International Prognostic Scoring System(IPSS) classifies patients with MDS in risk groups for both overall survival and progression to acutemyeloid leukemia based on which of the followingvariable(s)? a. Percentage of bone marrow blastsb. Cytogenetic patternc. Number of cytopeniasd. Both a and ce. All of the above
5. What are the key factors in considering a donorstem cell transplant for patients with MDS?a. Availability of a donor and the time interval
between the diagnosis of MDS and transplantb. The patient’s age and general healthc. The patient’s IPSS scored. The type of MDS diagnosede. Only a, b, and cf. All of the above
6. Long-term use of blood transfusions may eventu-ally lead to iron overload.a. Trueb. False
7. Patients with MDS who receive regular bloodtransfusions should have their serum ferritin concen-tration monitored for iron overload how often?a. At time of diagnosis of MDS and at least every
3 monthsb. At time of diagnosis of MDS and every month if
serum ferritin concentration >1000 ng/mLc. At time of diagnosis of MDS and every 6 monthsd. At time of diagnosis of MDS and when serum
ferritin levels reach 1000 to 2000 ng/mL
8. MDS is as prevalent as other common hematolog-ic malignancies of older adults, such as multiplemyeloma and chronic lymphocytic leukemia.a. Trueb. False
9. Which of the following are potential clinical con-sequences of not using iron chelation in patients withMDS? a. Cardiac complicationsb. Hepatic complicationsc. Endocrine complicationsd. All of the above
10. A study by Malcovati et al on 467 patients whowere diagnosed with MDS between 1992 and 2002found that transfusion-dependent patients experi-enced a _______ survival rate as compared withpatients who did not require transfusions.a. longerb. shorter c. equal d. none of the above
CME Test QuestionsTREATMENT OF IRON OVERLOAD IN
MYELODYSPLASTIC SYNDROME


CME Test Answer Sheet and Evaluation Form forTREATMENT OF IRON OVERLOAD IN
MYELODYSPLASTIC SYNDROME
Hematology/Oncology Clinics • Supplement 1 21
Release Date of Activity: November 2006Expiration Date of Activity for AMA PRA Credit: November 30, 2008Estimated Time to Complete this Activity: 1 hourGet instant CME credit(s). Complete your test online and download your certificate now.Log on to: www.elseviercme.com/getcme/280009
Please Print
Name: ______________________________________________________ Specialty: ___________________________
Degree: ▫ MD ▫ DO ▫ PharmD ▫ RPh ▫ NP ▫ RN ▫ BS ▫ PA ▫ Other: _______________________________
Affiliation: ______________________________________________________________________________________
Street: _________________________________________________________________________________________
City: ______________________________________________ State: ____________________ Zip: _________________
Telephone: _________________________________________ Fax: _________________________________________
E-mail: ____________________________________________ Signature: _____________________________________
(All information is confidential.)
CME Credit VerificationI verify that I have spent ____ hour(s)/____ minutes of actual time working on this CME activity.
No more than 1 CME credit(s) will be issued for this activity.
PRETEST ASSESSMENT: Please rate your current knowledge of treatment of iron overload in myelodysplastic
syndrome on a scale of 1 to 5, with 1 being the lowest and 5 the highest. 1 2 3 4 5
CME TEST(Please circle correct answers.)
COURSE EVALUATION: Please evaluate the effectiveness of this activity by circling your choice on a scale of 1 to 5, with 1 being the lowest and 5 the highest.
1. Did the material adequately discuss the usefulness of applying the International Prognostic
Scoring System to patients with myelodysplastic syndrome (MDS)? 1 2 3 4 5
2. Did the material identify key factors in considering donor stem cell transplant
for patients with MDS? 1 2 3 4 5
3. How well did the article explain the advantages and disadvantages of iron chelating agents? 1 2 3 4 5
4. Did the article provide sufficient information on study findings regarding the association between transfusion-dependent patients with MDS and survival rates? 1 2 3 4 5✂
1. a b c d e
2. a b c d e
3. a b c d
4. a b c d e
5. a b c d e f
6. a b
7. a b c d
8. a b
9. a b c d
10. a b c d

22 Hematology/Oncology Clinics • Supplement 1
✂
5. How do you rate the overall quality of the activity? 1 2 3 4 5
6. How do you rate the educational content of the activity? 1 2 3 4 5
7. Was the material presented in this publication fair, objective, balanced, and free of bias in the discussion of any commercial product or service? ___Yes ___NoIf no, please comment: ___________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
8. Suggested topics for future activities:_______________________________________________________________________________________________________________________________________________________________________________________
9. Suggested authors for future activities:______________________________________________________________________________________________________________________________________________________________________________________________
10. After reading this publication, have you decided to change one or more aspects in the treatment of your patients? ___Yes ___No
If yes, what change(s) will you make?______________________________________________________________________________________________________________________________________________________________
If no, why not?_________________________________________________________________________________________________________________________________________________________________________________
11. Would you be willing to participate in postactivity follow-up surveys? ___Yes ___No
12. Would you be willing to participate in a phone, e-mail, or in-person discussion exploring ways to improve our CME activities? ___Yes ___No
The EOCME thanks you for your participation in this CME activity. All information provided improves the scope and purpose of our programs and your patients’ care.
Responses for AMA PRA Credit must be submitted by November 30, 2008.
CME INSTRUCTIONS
Log on to www.elseviercme.com/getcme /280009.This Supplement to Hematology/Oncology Clinics provides 1 free AMA PRA Category1 Credits™. Log on to the above URL to print your certificate now, or forward the TestAnswer Sheet and Evaluation Form to the address shown below.
Elsevier Office of Continuing Medical EducationDepartment 280009685 Route 202/206
Bridgewater, NJ 08807
Please allow 6 to 8 weeks for processing. A photocopy of this form is acceptable.(Refer to pages 4 and 5 for CME Information.)

1. e.MDS refers to a group of hematologic stem cell disordersthat are characterized by ineffective blood production,cytopenias and cytologic dysplasia, and variable risk forleukemia transformation.
2. e.Most patients with MDS eventually develop infectiouscomplications, complications from blood cell deficien-cies, or acute leukemia.
3. b.The annual incidence rate of MDS for all age groups isapproximately 3 to 4 per 100,000 people, typically foundin elderly men at a median age at onset of 65 years.
4. e.The IPSS classifies patients with MDS in risk groups forboth overall survival and progression to acute myeloidleukemia based on percentage of bone marrow blasts,cytogenetic pattern, and number of cytopenias.
5. f.Key factors in considering a donor stem cell transplantfor patients with MDS include availability of a donor, thetime interval between the diagnosis of MDS and trans-plant, the patient’s age, the patient’s general health, thepatient’s IPSS score, and the type of MDS diagnosed.
6. a.True. Long-term use of blood transfusions may eventu-ally lead to iron overload.
7. a.Patients with MDS who receive regular blood transfu-sions should have their serum ferritin concentration moni-tored for iron overload at time of diagnosis of MDS andat least every 3 months.
8. a.True. MDS is as prevalent as other common hematologicmalignancies of older adults, such as multiple myelomaand chronic lymphocytic leukemia.
9. d.Potential clinical consequences of not using iron chela-tion in patients with MDS include cardiac complications,hepatic complications, and endocrine complications.
10. b.A study by Malcovati et al on 467 patients who werediagnosed with MDS between 1992 and 2002 found thattransfusion-dependent patients experienced a significant-ly shorter survival rate as compared with patients whodid not require transfusions (P < 0.001).
Hematology/Oncology Clinics • Supplement 1 23
CME Test AnswersTREATMENT OF IRON OVERLOAD IN
MYELODYSPLASTIC SYNDROME

Excerpta Medica, an Elsevier business685 Route 202/206
Bridgewater, NJ 08807
hemonc.theclinics.comISSN 0889-8588
Treatment of Iron Overload inMyelodysplastic Syndrome