-
9/9/2015
1
& A Collaboration Between & A Collaboration Between
AbnormalAbn
& A Collaboration Between
Heat Attack Prevention
CAD kills more than 450,000 Americans annually (20% of all
deaths)
1,260,000 Americans will have MI this year- Nearly 40% will not
survive
CAD is Number 1 killer of women; more than next 7 causes
combined!
Primary care setting is ideal for identifying patients before
symptom onset or acute event
CAC scoring/CIMT testing ideal screening tests for CAD
Non-invasive, patient friendly, low cost
& A Collaboration Between
Percentage of Americans
whose First Symptom of
CAD is Myocardial
Infarction:
50%
& A Collaboration Between
Coronary Atherosclerosis
Long-standing association between arterial disease and
calcification.
Calcification ≈ atherosclerosis
20% of plaque volume is calcium
& A Collaboration Between
Multi- Slice CT Technology
6 second heart scan
.5mm slice thickness
Rotation speeds of .33
seconds
Up to 1500 slices per study
Excellent 3-D image quality
Reduced radiation
exposure
& A Collaboration Between
Calcium Scoring
Becomes the
Prevention
Paradigm:
The Heart
Mammogram or
Colonoscopy
Goal:
Leading Causes of
Death (United States) 1.Heart Disease
2.All Cancers
3.Stroke
4.Respiratory
5.Accidents
6.Diabetes
7.Alzheimer’s 8.Influenza & Pnuemonia
http://rds.yahoo.com/_ylt=A0WTefW4t6hLRFcAtKyjzbkF/SIG=12f1ifn77/EXP=1269434680/**http:/www.daviddarling.info/images/heart_attack_victim.jpg
-
9/9/2015
2
& A Collaboration Between
CCTA vs. Calcium Artery Calcium
CAC
CCTA: Symptomatic
CAC: Asymptomatic
& A Collaboration Between
Calcium Artery Calcium Score
Coronary calcium has been shown to independently
predict cardiovascular risk and…
New research indicates that calcified plaques are
intimately related to the unstable lesions
responsible for myocardial infarction
Carr JJ. Applied Radiology. December, 2005
& A Collaboration Between
Calcium Score Value
Current methods of identifying asymptomatic CAD
patients ineffective
Traditional risk assessment models identify only
60-65% of early CAD patients
Ca+ score plus Framingham adds incremental risk
prediction value
Ca+ linked to CAD, acute events, and mortality
5 minute test, no contrast, 1-2 mSv radiation
& A Collaboration Between
Radiation Exposure
Activity Radiation (mSV)__
CCTA 7-11
Nuclear Stress Test 15-20
Chest X-Ray .5
Catheter Angiography 5-8
PET CT 7-10
Mammography 1-2
Coronary Ca+ Score
-
9/9/2015
3
& A Collaboration Between
© 2007, CVI3 LLC & A Collaboration Between
Why Screen Asymptomatic
Individuals?
CAD may be silent
Current Framingham CV risk scoring fails many groups
Proven CV therapy is available to alter
natural history of an indolent disease
& A Collaboration Between SHAPE Task Force. Am J Cardiol.
2006;98:2-15
& A Collaboration Between
Brief Case:
Two prominent men:
Both smokers - #1 stopped, #2 continued
Both with limited exercise - #1 became an
avid runner, lost weight, became very fit,
#2 continued to be inactive and obese
Both #1 and #2 had family history of
premature death…
Assessing the VP Pyramid
& A Collaboration Between
Assessing the VP Pyramid Who was at greater risk for the
development
of heart disease?
Jim Fixx marathon runner, exercise advocate, author
-dead at 53 of a heart attack
Sir Winston Churchill broke every tenet of “healthy life style”
- dead at age 91 & A Collaboration Between
-
9/9/2015
4
& A Collaboration Between
“The best test for prediction of the risk of atherosclerosis is
the demonstration of
atherosclerosis”
Dr. Ernest Schaeffer, Editor-in-Chief of
Atherosclerosis
Common
Sense
& A Collaboration Between
ACCF/AHA CLINICAL EXPERT
CONSENSUS DOCUMENT
Consensus Document on Coronary Calcium Scoring
J Am Coll Card. 2007;49:378-402
& A Collaboration Between
Statement
Ca+ scoring has quality evidence supporting
its role in risk stratifying asymptomatic persons
Recent data supports coronary calcium is
predictive of CHD death or MI at 10-15 years
Ca+ is independently predictive of outcomes
over and above traditional risk measurements
Testing most beneficial in patients at
intermediate Framingham risk- least valuable
in low risk patients & A Collaboration Between
SHAPE TASK FORCE
GUIDELINES
National Screening for Heart Attack Prevention and Eradication
(SHAPE)
Am J Cardiol. 2006;98:2-15
& A Collaboration Between
SHAPE Recommendations
All asymptomatic males without known CAD
and between 45-75 should be screened for
CAD (Ca+ Score or IMT)
All asymptomatic females without known CAD
and between 55-75 should be screened for
CAD (Ca+ Score or IMT)
Younger adults having >2 CAD risk factors
Limited value for subjects having no risk factors
& A Collaboration Between
Atherosclerosis Test
Very Low Risk
Negative Test• CCS =0
• CIMT
-
9/9/2015
5
& A Collaboration Between
Patient Management Strategies Following
Heart Attack Prevention Sceening
& A Collaboration Between
CAC Score 0/CIMT
-
9/9/2015
6
& A Collaboration Between
CORONARY CALCIFICATION, RISK FACTORS
AND EVENTS : ST. FRANCIS HEART STUDY
Prospective, population-based primary prevention
study 5585 men and women aged 50 to 70
4.3 years follow-up
122 (0.6%/year) with ASCVD event:
Nonfatal MI/coronary death 43
CABG/PTCA 62
Non-hemorrhagic stroke 5
Peripheral vascular surgery 12
& A Collaboration Between
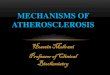
St. Francis Heart Study
Coronary outcomes* by calcium score
Calcium
Score
Event
Rate
Relative
Risk
95% CI
0 0.54 1 -
1-99 1.00 1.9 0.8-4.2
100-399 5.5 10.2 4.8-21.6
>400 14.0 26.2 12.6-53.7
*coronary death, nonfatal MI, CABG, and coronary angioplasty
Arad Y, Goodman KJ, Roth M et al. Coronary calcification,
coronary disease risk factors, c-reactive protein, and
atherosclerotic cardiovascular disease events. The St Francis
Heart Study. J Am Coll Cardiol 2005; 46: 158-165.
& A Collaboration Between
CAC Scores and CV Risk in “Low Risk” Women by FRS: The
Multi-Ethnic Study of Atherosclerosis (MESA)
Lagoski et al. 2007;167:2437-42
CAC scores
0 >0 1-99 100-299 >300
68% 32% 22% 6% 4%
2684 asymptomatic women 45-79
3.75 yr f/u
NIH sponsored prospective study;6,814 Asymptomatic pts: 3.75
year follow-up
& A Collaboration Between
Framingham Offspring Study
3529 subjects
All Intermediate risk
Ca+ score test
What percentage of
intermediate
Framingham subjects
would be reclassified as
high risk with “high” CAC
High CAC defined as 90th
or >100 Agatston
Results:
>90th percentile 22%
>100 score 39%
High-risk Reclassification:
61%
25% reclassified to low
risk with 0 CAC
Preis, et al. Am J Cardiol 2009;103:1710-1715.
& A Collaboration Between
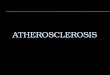
% Maintaining Statin Therapy at 3.6 Years by CAC Level
No CAC CAC 1-99 CAC 100-399 CAC>400
0
10
20
30
40
50
60
70
80
90
100
44
63
75
90
Visualizing Coronary Calcium is Associated with
Improvements in Adherence to Statin Therapy
Kalia et al. Atherosclerosis 2005
505 pts on statins
& A Collaboration Between
Case Study
Introduction:
47 year old female, in the primary care office with concerns
about family history for MI.
Clinical Background:
Medical History: Total cholesterol 230 with HDL 40
Family History: Both parents had MI
Physical Exam: Normal
Symptoms:
Asymptomatic
http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstrhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstrhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstrhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstrhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstrhttp://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=pubmed&dopt=Abstract&list_uids=19539080&itool=iconabstr
-
9/9/2015
7
& A Collaboration Between
Patient is concerned about significance of
family history of premature CAD
Don’t worry her; provide reassurance?
0-1 risk factors is low risk: 90% percentile)
CHD Risk Equivalent: CV Risk >20%
Advanced CAD Risk
Coronary Artery Scanning
u SEVERECALCIFICATION
& A Collaboration Between
When To Order
All males without known CAD and between 45-
75 should be screened for CAD (Ca+ or IMT)
All females without known Cad and between
55-75 should be screened for CAD (Ca+ or IMT)
Younger adults having >2 CAD Risk factors
Asymptomatic, apparently healthy population
Limited value for subjects having no risk factors
SHAPE Task Force. Am J Cardiol. 2006;98:2-15
& A Collaboration Between
CAC Scoring or CIMT
Into Prevention
Paradigm;
Mammography
PSA
Goal:
Leading Causes of
Death (United States) 1.Heart Disease
2.All Cancers
3.Stroke
4.Respiratory
5.Accidents
6.Diabetes
7.Alzheimer’s 8.Influenza & Pnuemonia
& A Collaboration Between
Therapy of Abnormal CACS
© 2007, CVI3 LLC
-
9/9/2015
8
& A Collaboration Between Int. J. Mol. Sci. 2015, 16,
8861-8883
© 2007, CVI3 LLC & A Collaboration Between
Changes in plaque burden over 1 y.
Matthew Budoff J. Nutr. 2006;136:741S-744S
©2006 by American Society for Nutrition
& A Collaboration Between
Coronary Artery Calcium Therapy
© 2007, CVI3 LLC & A Collaboration Between
The Potential Role of Vitamin K2
© 2007, CVI3 LLC
& A Collaboration Between
Omega 3 PUFA: A Possible Benefit
© 2007, CVI3 LLC
Randomized Comparison of High-Dose Oral Vitamins versus
Placebo
in the Trial to Assess Chelation Therapy (TACT)
Gervasio A. Lamas, MD, FACC
Professor of Clinical Medicine
Columbia University Division of Cardiology
Mount Sinai Medical Center
Miami Beach, FL
For the TACT Investigators
-
9/9/2015
9
0
0.1
0.2
0.3
0.4
0.5
0 6 12 18 24 30 36 42 48 54 60
Ev
en
t R
ate
Months since randomization
Placebo Infusions/Placebo Vitamins
Placebo Infusions/High-Dose Vitamins
EDTA Chelation/Placebo Vitamins
EDTA Chelation/High-Dose Vitamins
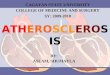
TACT Primary Endpoint: Factorial
Groups EDTA Chelation/High-dose Vitamins
vs. Placebo/Placebo
HR (95% CI): 0.74 (0.57, 0.95)
P = 0.016 Δ=8.3%
Subgroup Results for Vitamin Analyses
Participant Group N
Interaction
P-value HR 95% CI
All participants 1708 0.89 0.75, 1.07
Infusions 0.94
EDTA 839 0.89 0.68, 1.15
Placebo 869 0.90 0.7, 1.15
Gender 0.17
Male 1409 0.84 0.69, 1.03
Female 299 1.17 0.75, 1.83
Anterior MI 0.79
Yes 674 0.93 0.69, 1.26
No 1034 0.88 0.7, 1.09
Diabetes 0.72
Yes 538 0.84 0.62, 1.14
No 1170 0.90 0.72, 1.12
Statins at baseline 0.01
Yes 1248 1.03 0.84, 1.27
No 460 0.62 0.44, 0.87
CAM site 0.39
Yes 1089 0.84 0.67, 1.05
No 619 0.99 0.74, 1.33
4.0 1.0 0.25
High-Dose
Vitamins Better
Placebo
Better
2.0 0.5
& A Collaboration Between
Questions