Embed Size (px)
Citation preview

Heart Murmurs in Pediatric Patients:When Do You Refer?MICHAEL E. MCCONNELL, M.D., SAMUEL B. ADKINS III, M.D., and DAVID W. HAXNON, M.D.East Carolina University School of Medicine, Greenville, North Carolina
Many normal children have heart murmurs, but most children do not have heart dis-ease. An appropriate history and a properly conducted physical examination can iden-tify children at increased risk for significant heart disease. Pathologic causes of systolicmurmurs include atrial and ventricular septal defects, pulmonary or aortic outflow tractabnormalities, and patent ductus arteriosus. An atrial septal defect is often confusedwith a functional murmur, but the conditions can usually be differentiated based onspecific physical findings. Characteristics of pathologic murmurs include a sound levelof grade 3 or louder, a diastoMc murmur or an increase in intensity when the patient isstanding. Most children with any of these findings should be referred to a pediatric car-diologist. (Am Fam Physician 1999;60:558-65.)
O A patient infor-mation handout onheart murmurs in chil-dren, written by theauthors of this article,is provided on page565.
Primary care physicians frequentlyencounter children with heartmurmurs.' Most of these youngpatients do not have heart disease.One set of investigators^ found
that physicians were generally accurate indetermining whether a murmur was benign orpathologic. Nonetheless, 61 percent of the mur-murs referred for subspecialist evaluation werefound to be functional, or innocent, murmurs.The investigators hypothesized that increasededucation of health care providers and parentsmight be helpful in alleviating unnecessaryanxiety and reducing the number of patientswith innocent murmurs who are referred forfurther evaluation.-
Echocardiography is not always needed todiagnose pediatric murmurs. One study-*showed that direct referral for echocardiogra-phy was an expensive way to evaluate childrenwith heart murmurs. Pediatric cardiologyconsultation was significantiy less costly inthat many innocent murmurs were diagnosedwithout echocardiography. A recent stud/*found that pediatric echocardiograms per-
.ardidc pathology should be suspected In infants with a
history of poor feeding, failure to thrive, unexplained
respiratory symptoms or cyanosis.
formed in adult cardiology practices wereunnecessary in 30 percent of patients, were ofinadequate quality in 32 percent of patientsand resulted in an erroneous impression ofthe nature or presence of pathologic disease in32 percent of patients.
This article reviews the individual steps in thecardiac physical examination and the possibleinnocent or pathologic findings. The focus is onhelping physicians become even more confidentabout their ability to diagnose innocent mur-murs and to decide which patients might bene-fit from pediatric cardiology referral.
General Approach
Busy clinicians need an approach thatallows them to appropriately identify and referpatients with pathologic murmurs to a pedi-atric cardiologist. This approach should alsohelp them know when they can confidently re-assure the parents of a child with a functionalmurmur that referral is unnecessary.
In a busy office practice, time constraintsmake it difficult to perform a complete cardiacphysical examination on every patient. How-ever, this examination must be performed onany child who has a heart murmur or histori-cal features that indicate the presence of heartdisease or abnormal cardiac function. Fea-tures of concern in infants include feedingintolerance, failure to thrive, respiratorysymptoms or cyanosis. In older children, chest
558 AMF.RICAN FAMILY PHYSICIAN VOLUME 60, NUMBER 2 / AUGUST 1999

pain (especially with exercise), syncope, exer-cise intolerance or a family history of suddendeath in young people should prompt a com-plete examination.
The examination is conducted in a quietroom. An infant may lie quietly on the exam-ination table. However, it can be challengingto keep a one- to two-year-old child quietenough for a good examination to be per-formed. Having the child sit in the lap of aparent or other caregiver may be helpful.
Precordial Palpation
The cardiac examination begins with palpa-tion to assess precordial activity and femoralpulses. Increased precordial activity is com-monly felt in patients with increased right orleft ventricular stroke volume. Increased pre-cordial activity occurs in patients with anatrial septal defect, a moderate or large ven-tricular septal defect or significant patent duc-tus arteriosus. This increased activity shouldraise the possibility that the auscultatory find-ings may be pathologic. Other explanationsfor increased precordial activity includepatient anxiety, anemia and hyperthyroidism.
Once both brachial pulses have been pal-pated, the right brachial pulse should then bepalpated simultaneously with the femoralpulse. If the timing and intensity of the twopulses are equal and biood pressure in theright arm is normal, coarctation of the aorta isunlikely.
Precordial palpation is also necessary to feel"thrills," which are the palpable consequence ofblood flowing rapidly from high pressure tolower pressure. Some ventricular septal defectsresult in thrills at the lower left sternal border.Moderate to severe pulmonary valve stenosismay cause a thrill at the upper left sternal bor-der. A thrill resulting from aortic stenosis is fre-quently palpable in the suprasternal notch.
Auscultation of Firstand Second Heart Sounds
Precordial palpation is followed by auscul-tation. This part of the examination entails
Tihe sounds of a venous hum should disappear when the child
is in the supine position, when light pressure is applied over
the child's jugular vein or when the child's head is turned.
separate evaluation of each heart sound andeach phase of the cardiac cycle.'
FIRST HEART SOUND
Auscultation begins with listening for thefirst heart sound (S,) at the lower left borderof the sternum. The S, is caused by closure ofthe mitral and tricuspid valves and is normallya single sound. An inaudible S, indicates thatsome sound is obscuring the closure sound ofthese valves. The differential diagnosis formurmurs that obscure S, includes ventricularseptal defects, some murmurs caused by atri-oventricular valve regurgitation, patent ductusarteriosus and, occasionally, severe pulmonaryvalve stenosis in a young child. These S.-coin-cident murmurs are also known as "holosys-tolic" murmurs.
CLICKS
If SI is audible but appears to have two com-ponents at some spots in the precordium, thepatient has either a click or an asynchronousclosure of the mitral and tricuspid valves.Clicks may originate from any valve in theheart. Depending on their origin, clicks havedifferent identifying characteristics.
Ejection clicks originating from the pul-monic valve begin shortly after the atrioven-tricular valves close, vary with respirationand are best heard at the upper to middlearea of the left sternal border. Aortic valveejection clicks begin shortly after S, and arebest heard at the apex. They do not vary withrespiration.
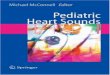
Systolic clicks originating from the mitralvalve are best heard at the apical area when thepatient is standing. Occasionally, the tissueclosing a ventricular septal defect can pop orclick early in systole (Figure I).
AUGUST 1999 / VOLUME 60, NUMBER 2 AMERICAN FAMILY PHYSICIAN 559

In patients with an atrial septa! defect, the features of
increased precordial activity, a widely split heart sound, a sys-
tolic murmur and a diastolic rumble are often present.
SECOND HEART SOUND
After auscultation for clicks throughoutthe four listening areas, the next step is toreturn to the upper left sternal border andlisten to the second heart sound (S;)- Thissound is caused by closure of the aortic andpulmonic valves.
The S2 should split into two componentswhen the patient inspires. The first compo-nent, aortic second sound (A,), is closure ofthe aortic valve. The second component, pul-monic second sound (P;), is caused by clo-
FIGURE 1. Listening areas for clicks: upper right sternal border (URSB) foraortic valve clicks; upper left sternal border (ULSB) for pulmonary valveclicks; lower left sternal border (LLSB), or the tricuspid area, for ventricu-lar septal defects; apex for aortic or mitral valve clicks.
sure of the pulmonary valve. The splitting ofS, occurs because inspiration brings moreblood into the right ventricle. Right ventricu-lar ejection is prolonged, and the pulmonaryvalve closes later. An awareness of this phe-nomenon is helpful in understanding thephysical examination features of the patientwith an atrial septal defect. A loud, single Sindicates either pulmonary hypertension orcongenital heart disease involving one of thesemilunar valves.
Murmurs
Systolic murmurs have only a few possiblecauses: blood flow across an outflow tract(pulmonary or aortic), a ventricular septaldefect; atrioventricular valve regurgitation, orpersistent patency of the arterial duct {ductusarteriosus). Systolic murmurs can also befunctional (benign).
GRADES
Systolic murmurs are graded on a six-pointscale. A grade 1 murmur is barely audible, agrade 2 murmur is louder and a grade 3 mur-mur is loud but not accompanied by a thrill. Agrade 4 murmur is loud and associated with apalpable thrill. A grade 5 murmur is associ-ated with a thrill, and the murmur can beheard with the stethoscope partially off thechest. Finally, the grade 6 murmur is audiblewithout a stethoscope. All murmurs louderthan grade 3 are pathologic.
TrMING
Systolic murmurs may be timed as early,middle or late systolic. They can also be timedas holosystolic.
VENOUS HUMS
Many children with functional murmurshave venous hums. These sounds are causedby the flow of venous blood from the headand neck into the thorax. They are heard con-tinuously when the child is sitting. The soundsshould disappear when light pressure isapplied over the jugular vein, when the child's
560 AMERICAN FAMILY PHYSICIAN Voi-UMK 60, NUMBER 2 / AUGUST 1999

Pediatric Heart Murmurs
head is turned or when the child is lyingsupine. Venous hums are common and arenot pathologic. Patients with venous hums donot require pediatric cardiology referral. Allother diastolic murmurs are pathologic andtherefore warrant referral.
DESCRIF»TION OF CHARACTER
The character, or tone, of a murmur mayaid in the diagnosis. Words such as "harsh,""whooping," "honking," "blowing," "musical"and "vibratory" may be useful, albeit some-what subjective, in describing murmurs.
A "harsh" murmur is consistent with high-velocity blood flow from a higher pressure toa lower pressure. "Harsh" is often appropriatefor describing the murmur in patients withsignificant semilunar valve stenosis or a ven-tricular septal defect.
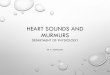
"Whooping" or "blowing" murmurs at theapex occur with mitral valve regurgitation. Theterm "flow murmur" is often used to describea crescendo/decrescendo murmur that isheard in patients with a functional murmur(Figure 2). However, similar systolic ejectionmurmurs may be heard in patients with atrialseptal defect, mild semilunar valve stenosis,subaortic obstruction, coarctation of the aortaor some very large ventricular septal defects.
Many functional or innocent murmurs are"vibratory" or "musical" in quality. Still's mur-mur is the innocent murmur most frequentlyencountered in children. This murmur is usu-ally vibratory or musical.
LOCATION OF HIGHEST INTENSITY
The location of the highest intensity of amurmur is also important (Table 1). A mur-mur caused by aortic stenosis is often bestheard at the upper sternal border, usually onthe right side. A murmur resulting from pul-monary stenosis is heard best at the upper leftsternal border. A murmur caused by a ventric-ular septal defect or tricuspid valve insuffi-ciency is heard at the lower left sternal border.A murmur resulting from mitral valve regur-gitation is best heard at the apex.
Functional Murmur
Exhalation Inspiration
Ventricular Septal Defect Atrial Septal Defect
\
Inspiration
tS, A, P,
Inspiration and exhalation
FIGURE 2. Graphic representation of common pediatric murmurs. Thediamond-shaped murmurs are crescendo/decrescendo. The murmur ofa ventricular septal defect obscures the closure sound of the mitral andtricuspid valves and is termed "holosystolic." (S, = first heart sound; P2= pulmonic second sound; A; = aortic second sound)
POSITION CHANGES IN THE DIFFERENTIATION
OF MURMURS
Position changes are very helpful in differ-entiating functional and pathologic murmurs.The vibratory functional murmur heard in ayoung child (Still's murmur) decreases inintensity when the patient stands.
TABLE 1
Listening Areas for Common Pediatric Heart Murmurs
Area Murmur
Upper right sternal border
Upper left sternal border
Lower left sternal border
Apex
Aortic stenosis, venous hum
Pulmonary stenosis, pulmonary flow murmurs,atrial septal defect, patent ductus arteriosus
Still's murmur, ventricular septal defect, tricuspidvalve regurgitation, hypertrophiccardiomyopathy, subaortic stenosis
Mitral valve regurgitation
AUGUST 1999 / VOI.UMF. 60, NUMBKR 2 AMERICAN FAMILY PHYSICIAN 561

TABLE 2
Physical Findings in Functional (Innocent) Heart Murmur and Atrial Septal Defect
Physical finding Innocent murmur Atrial septal defect
Precordial activity
First heart sound (S,)
Second heart sound (S )
Systolic murmur (supine)
Systolic murmur (standing)
Diastolic murmur
Normal
Normal
Splits and moves with
respiration
Crescendo/decrescendo
Possibly vibratory at lower
left sternal border
Decreases in intensity
Venous hum
Increased
Normal
Widely split and fixed (i.e., does not move
with inspiration)
C f escen do/decrescendo
"Flow" at upper left sternal border
Does not change
Inflow "rumble" across tricuspid valve area
Most pathologic murmurs do not changesignificantly with standing. An importantexception is the murmur of hypertrophic car-diomyopathy, a potentially life threateningcondition. This murmur increases in intensitywhen the patient stands. In the upright posi-tion, venous return to the heart is reduced,decreasing the left ventricular end diastolicvolume. As left ventricular size decreases, theleft ventricular outflow tract narrows, and thesystolic outflow obstruction increases. Thisnarrowing increases the intensity of the mur-
The Authors
MICHAEL E. MCCONNELL, M.D,, i5 associate professor of pediatrics at East CarolinaUniversity School of Medicine, Greenville, N.C, Dr. McConnell received his medicaldegree from the University of Alabama 5chool of Medicine, Birmingham. He com-pleted a pediatric residency at Children's Hospital, Birmingham, Ala., and a fellowshipin pediatric cardiology at Children's Hospital Medical Center. Cincinnati.
SAMUEL B, ADKINS III, M.D., is assistant residency director and director of primary caresports medicine for the family practice residency program at East Carolina UniversitySchool of Medicine. Dr. Adkins graduated from the University of Pittsburgh School ofMedicine and completed a residency in family practice at St. Margaret Memorial Hos-pital, Pittsburgh.
DAVID W. HANNON, M.D., is associate professor of pediatrics at East Carolina Uni-versity School of Medicine. Dr. Hannon received his medical degree from the Univer-sity of South Florida College of Medicine, Tampa, and completed a pediatric residencyand a cardiology fellowship at Children's Hospital Medical Center, Cincinnati.
Address correspondence to Michael E. McConnell, M.D., Division of Pediatric Cardiol-ogy, Brody Medical Sciences Building, East Carolina University School of Medicine,Greenville, NC 27858-4354. Reprints are not available from the authors.
mur. Overall, hypertrophic cardiomyopathy israre; however, it is one of the leading causes ofsudden death in athletes.''
AtrJal Septal DefectPerhaps the best way to decide whether a
patient needs to be referred to a pediatric car-diologist is to know confidently the clinicalfindings of the atrial septal defect. The abnor-mal findings in patients with atrial septaldefects are often quite subtle and thus are eas-ily confused with the physical findings inpatients with functional or innocent mur-murs (Table 2). Loud murmurs from ventric-ular septal defects or significant aortic or pul-monic stenosis are not subtle and are notoften confused with innocent murmurs.
The first step in the examination is palpa-tion for the precordial activity at the left ster-nal border, feeling for increased activity thatmay be present from right ventricular enlarge-ment. The examination is performed with thepatient in a supine position.
Auscultation at the lower left sternal bordershould reveal a normal, singie and easily audi-ble S|. Listening at the upper left sterna! bor-der for Sj should reveal variable splitting withrespiration. A widely split S2 that does notchange with respiration indicates either com-plete right bundle branch block or an atrialseptal defect.
562 AMERICAN FAMILY PHYSICIAN VOLUME 60, NUMBER 2 / AUGUST 1999

Pediatric Heart Murmurs
Because of the increased volume of bloodin the right ventricle in the patient with anatrial septai defect, the S, always sounds as ifthe patient has taken a deep breath. Thismeans that the volume of blood in the rightventricle Is increased and it takes longer forthe ventricle to eject its contents, thus leadingto a fixed, widely split S2.
Murmurs heard in patients with atrial sep-tal defects are often of low pitch and inten-sity. However, the intensity of the murmur isnot a reliable basis for the diagnosis. The sys-tolic murmur is caused by an increased vol-ume of blood coursing across the right ven-tricular outflow tract. If the murmur isaudible, it can be heard at the upper left ster-nal border.
Patients with atrial septal defects may alsohave a diastolic murmur. In this situation,increased diastolic blood flow across the tri-cuspid valve may cause a soft, often barelyaudible low-frequency "diastolic rumble."This sound is heard best with the bell of thestethoscope placed at the lower left sternalborder. Pushing down with the bell causes theskin beneath the stethoscope to act as a dia-phragm. Consequently, only the high-fre-quency sounds are heard. Releasing the ten-sion on the bell allows the low-frequencyrumbling sound to become audible at thelower left sternal border.
After the supine examination, the examina-tion should be repeated with the patientstanding. If the patient has an atrial septaldefect, the features of increased precordialactivity, a widely split Sj, a systolic murmur atthe upper left sternal border and a diastolicrumble should still be present when thepatient is standing. If the patient has an inno-cent or ftinctional murmur, the precordialactivity should be normal, the S, should splitand move with respiration, the systolic mur-mur should decrease in intensity and no dias-tolic murmur should be present in the tricus-pid valve area.
If no symptoms are present, the S, is nor-mal, the S2 splits and is of normal intensity,
and no clicks are heard, the differential diag-nosis of a grade 1 to grade 2 systolic murmuris frequently a choice between an atrial septaldefect and a functional murmur.
In young children, it can be difficult to con-fidently distinguish the respiratory variation ofS. splitting in the patient with a normal mur-mur ft-om the fixed S2 splitting in the patientwith an atrial septal defect. Because the patientwith an asymptomatic atrial septal defea willnot develop pulmonary hypertension or otherpermanent sequelae early in life, careful yearlyfollow-up examination by the primary carephysician can be recommended. By the time achild reaches preschool age, the normal orabnormal splitting of the S usually becomesclear (Table 3).
Follow-up or ReferralA patient who has a pathologic cardiac ex-
amination or who has cardiac symptoms andquestionable findings on the cardiac examina-tion should be referred to a pediatric cardiol-ogist. A child with a malformation syndromeassociated with congenital heart diseaseshould also be referred for additional evalua-tion. Conversely, an asymptomatic patientwhose physical findings on a conscientiouslyperformed cardiac examination indicate a lowprobability of cardiac pathology should be
TABLE 3
Features That Increase theLikelihood of Cardiac Pathology
Symptoms such as chest painFamily history of Marfan syndrome or sudden
death in young family membersMalformation syndrome (e.g., Down syndrome)Increased precordial activityDecreased femoral puisesAbnormai second heart soundCiicksLoud or harsh murmurIncreased intensity of murmur when patient stands
AUGUST 1999 / VOLUME 60, NUMBER 2 AMERICAN FAMILY PHYSICL\N 563

Pediatric Heart Murmurs
followed by the primary care physician. Refer-ral is indicated if possibly pathologic findingsemerge on serial examinations.'
Final CommentMany normal children have heart mur-
murs, but all of these children do not requirereferral to a pediatric cardiologist. Atrial septaldefect is the pathologic diagnosis that is fre-quently missed or easily confused with a func-tional murmur. It is important for familyphysicians to remember the physical examina-tion features that differentiate a functionalmurmur from a pathologic murmur. Beforereferring asymptomatic patients to a pediatriccardiologist, family physicians should attemptto rule out atrial septal defects by performinga complete, organized cardiac examination. Inthis way they can reduce the number of refer-rals for evaluations of functional murmurs
and at the same time increase their ability toconfidently reassure families when referral isunnecessary.
REFERENCES
Rosenthal A. How to distinguish between innocentand pathoiogic murmurs in chiidhood. Pediatr ClinNorth Am 1984:31:1229-40.McCrindle BW, Shaffer KM, Kan JS, Zahka <G,Rowe SA, Kidd L, Factors prompting referral for car-diology evaluation of heart murmurs in children [Let-ter]. Arch Pediatr Adolesc Med 1995:149:1277-9.Danford DA, Nasir A, Gumbiner C. Cost assess-ment of the evaluation of heart murmurs in chil-dren. Pediatrics 1993;9V365-8.HunA/itz RA, Caldwell RL, Should pediatric echocar-diography be performed in adult laboratories?[Abstract] Pediatrics 1998:102:390. Complete textat el 5 at: vwi'w.pediatrics.org.Peiech AN. The cardiac murmur: when to refer?Pediatr Ciin North Am 1998,45:107-22Maron BJ, Epstein SE, Roberts WC. Causes of sud-den death in competitive athletes. J Am Coll Car-diol 1986:7:204-14.
564 AMERICAN FAMILY PHYSICIAN VOLUME 60, NUMBER 2 / AUGUST 1999




















![[Int. med] heart murmurs from SIMS Lahore](https://img.pdfslide.us/doc/110x75/55d2cd1fbb61eb744e8b4581/int-med-heart-murmurs-from-sims-lahore.jpg)