Embed Size (px)
DESCRIPTION
Heart and Diabetes Baker IDI in the Centre. Professor Garry Jennings Director Baker IDI Heart and Diabetes Institute. Themes. Outcomes in diabetes Atherosclerosis and diabetes Coronary disease in the diabetic patient Diabetic heart Therapeutic aspects - PowerPoint PPT Presentation
Citation preview
Page 1: Baker IDI
Heart and DiabetesBaker IDI in the Centre
Professor Garry Jennings
Director
Baker IDI Heart and Diabetes Institute
Page 2: Baker IDI
Themes
• Outcomes in diabetes
• Atherosclerosis and diabetes
• Coronary disease in the diabetic patient
• Diabetic heart
• Therapeutic aspects
• What Baker IDI is doing relevant to indigenous health
Page 4: Baker IDI
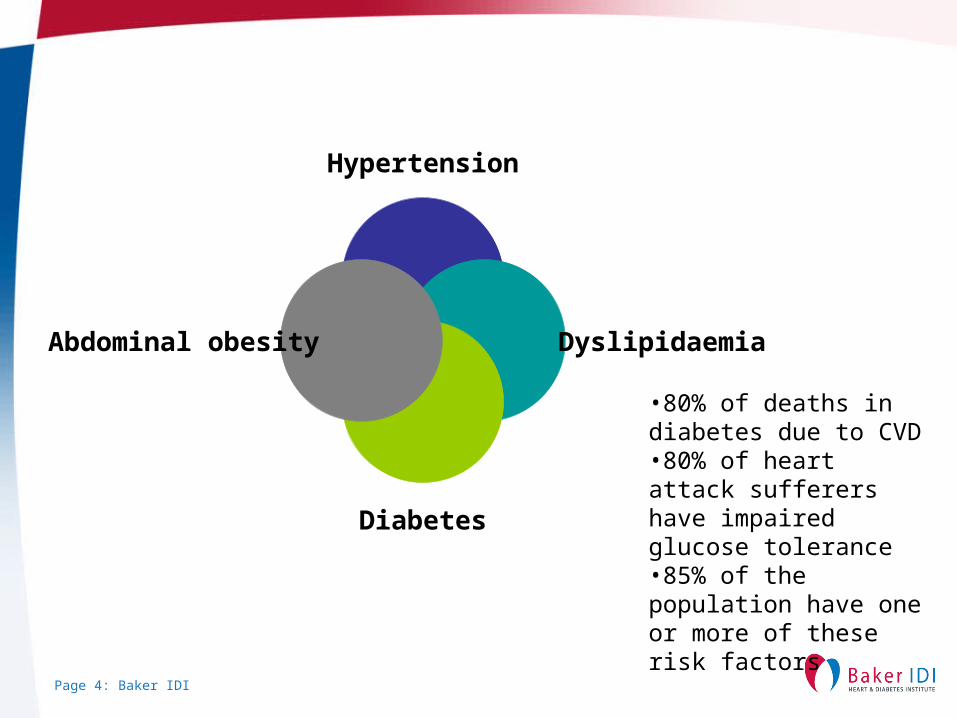
Hypertension
Dyslipidaemia
Diabetes
Abdominal obesity
•80% of deaths in diabetes due to CVD•80% of heart attack sufferers have impaired glucose tolerance•85% of the population have one or more of these risk factors
Page 5: Baker IDI
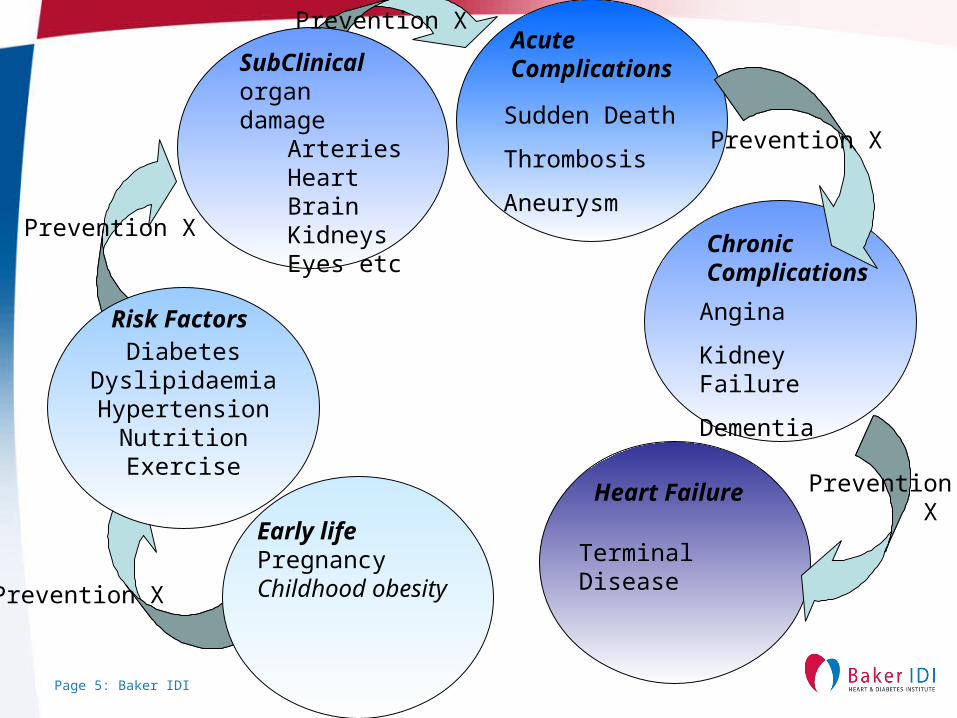
DiabetesDyslipidaemiaHypertension
NutritionExercise
Early lifePregnancy Childhood obesity
Risk Factors
SubClinicalorgan damage
ArteriesHeartBrain KidneysEyes etc
Acute Complications
Chronic Complications
Heart Failure
Terminal Disease
Angina
Kidney Failure
Dementia
Sudden Death
Thrombosis
Aneurysm
Prevention X
Prevention X
Prevention X
Prevention X
Prevention X
Page 6: Baker IDI
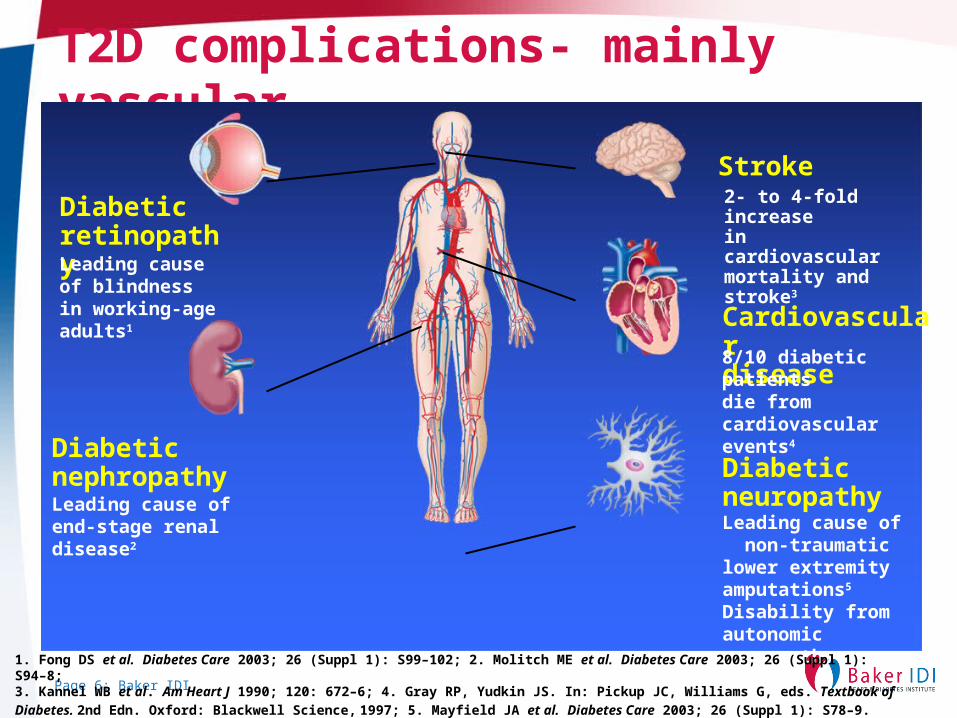
T2D complications- mainly vascular
DiabeticretinopathyLeading causeof blindnessin working-ageadults1
DiabeticnephropathyLeading cause of end-stage renaldisease2
Cardiovasculardisease
Stroke2- to 4-fold increasein cardiovascular mortality and stroke3
DiabeticneuropathyLeading cause of non-traumatic lower extremity amputations5
Disability from autonomic neuropathy
8/10 diabetic patients die from cardiovascular events4
1. Fong DS et al. Diabetes Care 2003; 26 (Suppl 1): S99–102; 2. Molitch ME et al. Diabetes Care 2003; 26 (Suppl 1): S94–8; 3. Kannel WB et al. Am Heart J 1990; 120: 672–6; 4. Gray RP, Yudkin JS. In: Pickup JC, Williams G, eds. Textbook of Diabetes. 2nd Edn.
Oxford: Blackwell Science, 1997; 5. Mayfield JA et al. Diabetes Care 2003; 26 (Suppl 1): S78–9.
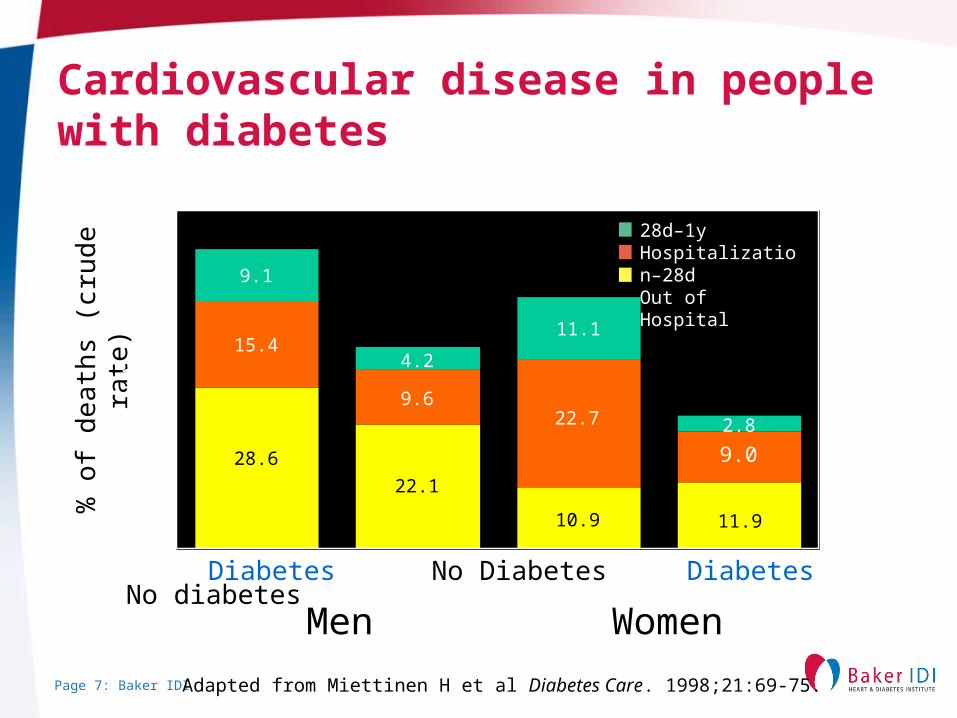
Page 7: Baker IDI Adapted from Miettinen H et al Diabetes Care. 1998;21:69-75.
Diabetes No Diabetes Diabetes No diabetes
% o
f de
ath
s (c
rude
ra
te)
60
40
30
20
10
0
Men
28.6
15.4
9.1
22.1
9.6
4.2
10.9
22.7
11.1
11.9
9.0
2.8
28d–1yHospitalization–28dOut of Hospital
Women
50
Cardiovascular disease in people with diabetes
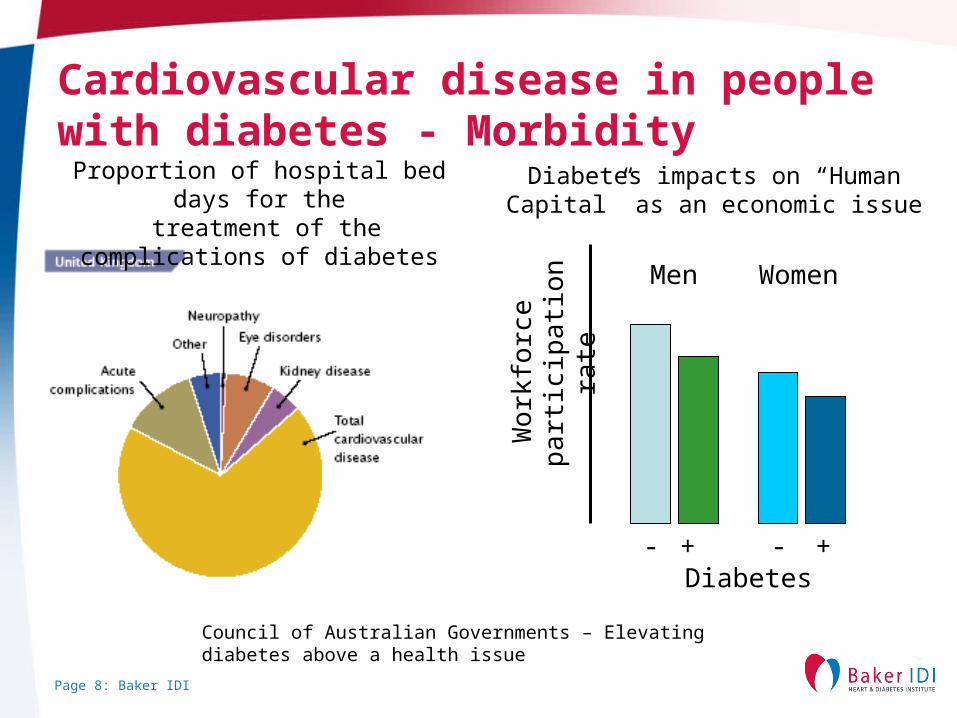
Page 8: Baker IDI
Proportion of hospital bed days for the treatment of the complications of
diabetes
Diabetes- - ++
Men Women
Wo
rkfo
rce
p
artic
ipat
ion
rate
Diabetes impacts on “Human Capital” as an economic issue
Council of Australian Governments – Elevating diabetes above a health issue
Cardiovascular disease in people with diabetes - Morbidity
Page 9: Baker IDI
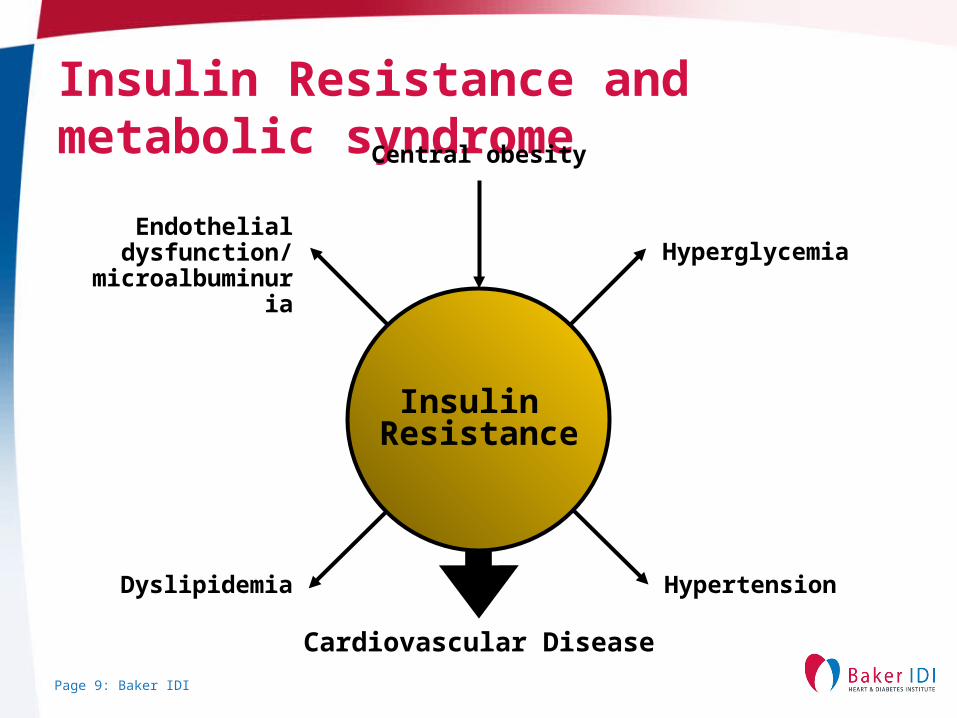
Insulin Resistance and metabolic syndromeCentral obesity
HyperglycemiaEndothelial
dysfunction/microalbuminuria
Cardiovascular Disease
HypertensionDyslipidemia
Insulin Resistance
Page 10: Baker IDI
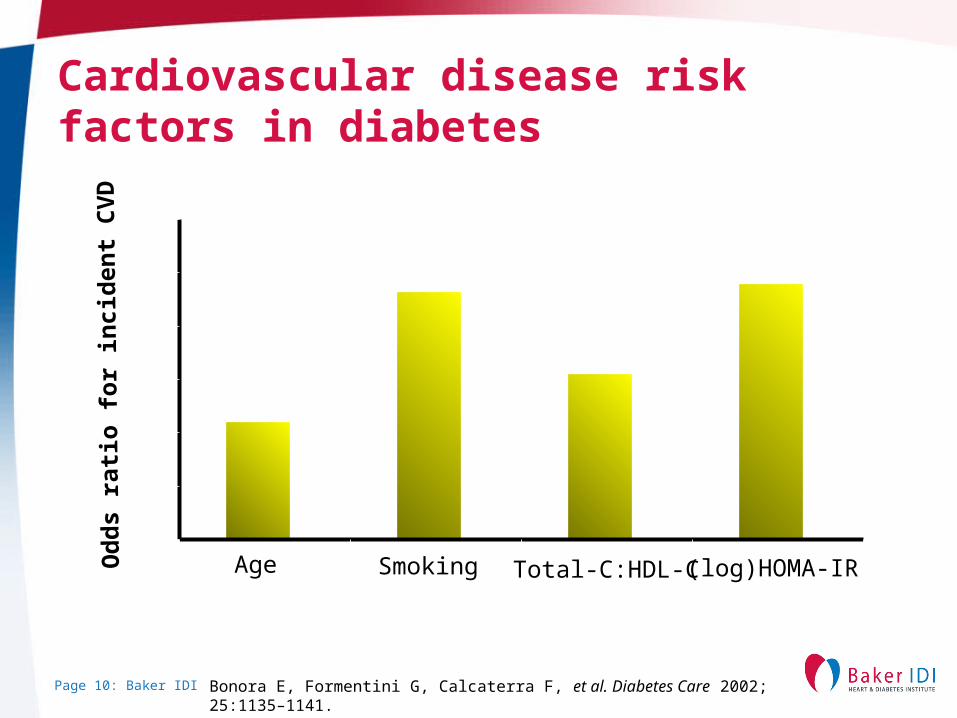
Cardiovascular disease risk factors in diabetes
0.6
0.8
1.0
1.2
1.4
1.6
1.8
Od
ds
rati
o f
or
inci
den
t C
VD
Age Smoking Total-C:HDL-C (log)HOMA-IR
Bonora E, Formentini G, Calcaterra F, et al. Diabetes Care 2002; 25:1135–1141.
Page 11: Baker IDI
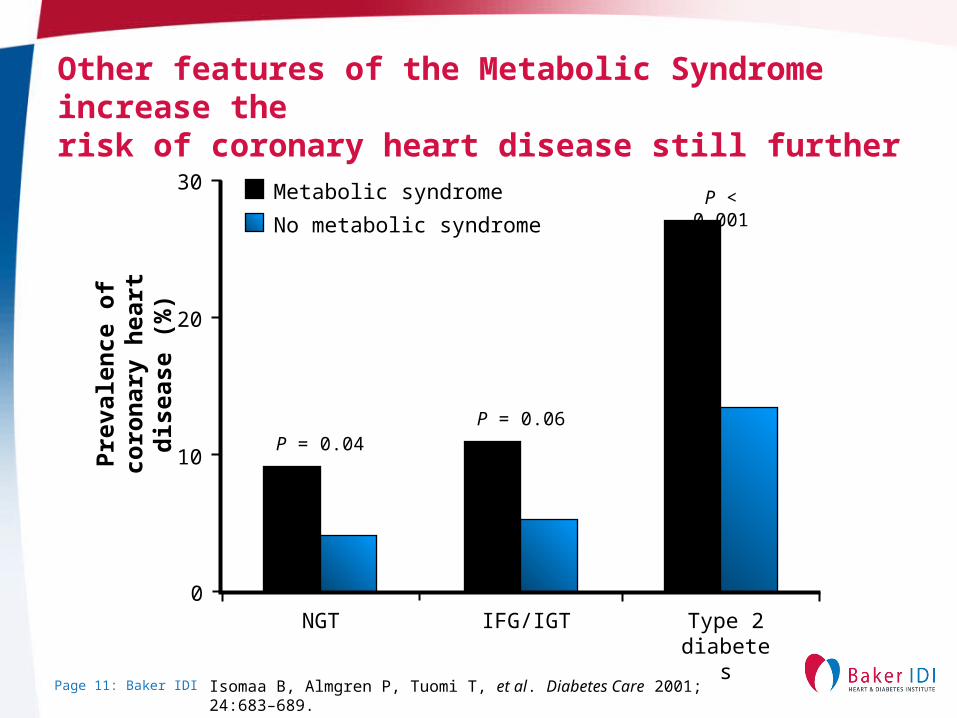
Other features of the Metabolic Syndrome increase the risk of coronary heart disease still further
Pre
vale
nce
of
coro
nar
y h
eart
dis
ease
(%
)
30
20
10
NGT IFG/IGT Type 2diabetes
No metabolic syndrome
Metabolic syndrome
P = 0.04P = 0.06
P < 0.001
0
Isomaa B, Almgren P, Tuomi T, et al. Diabetes Care 2001; 24:683–689.
Page 12: Baker IDI
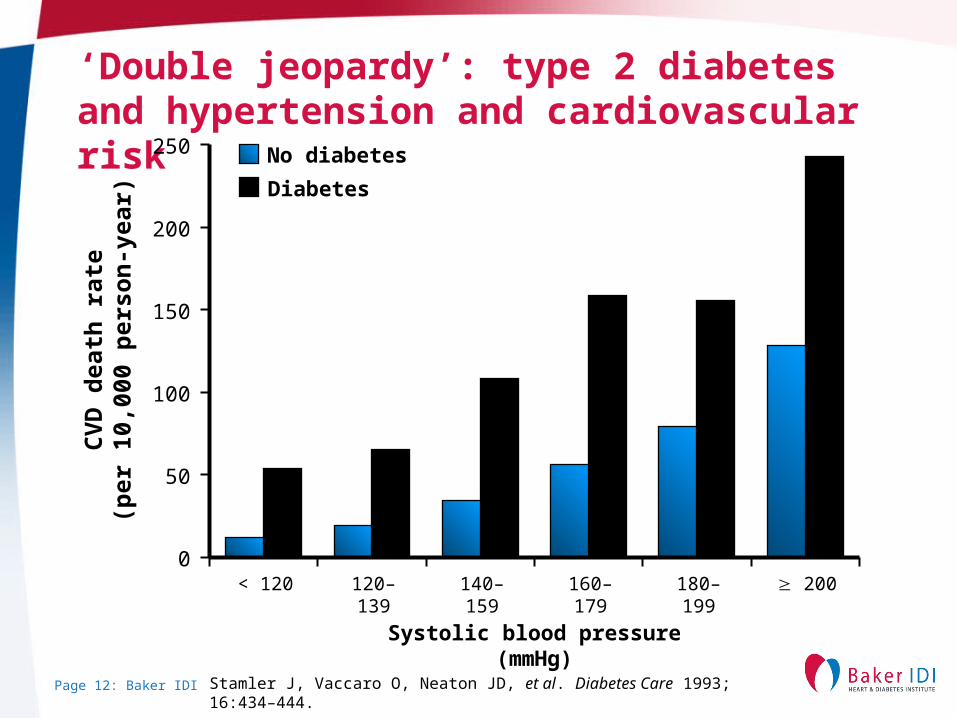
‘Double jeopardy’: type 2 diabetes and hypertension and cardiovascular risk
Diabetes
No diabetes
CV
D d
eath
rat
e(p
er 1
0,00
0 p
erso
n-y
ear)
250
0
200
150
100
50
Systolic blood pressure (mmHg)
< 120 120–139 140–159 160–179 180–199 200
Stamler J, Vaccaro O, Neaton JD, et al. Diabetes Care 1993; 16:434–444.
Page 13: Baker IDI
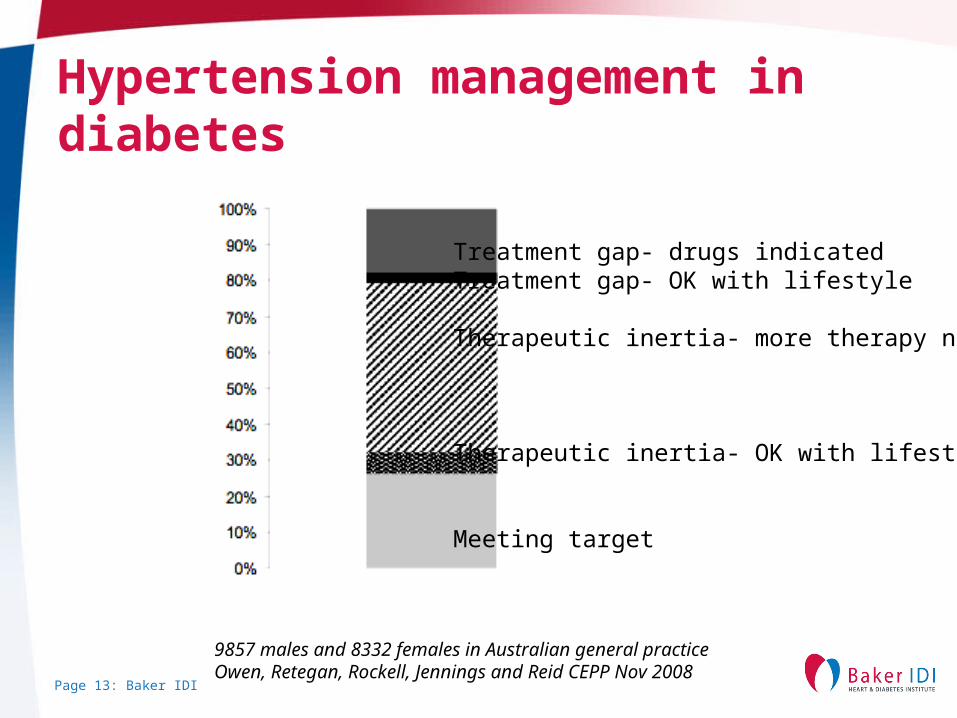
Hypertension management in diabetes
Treatment gap- drugs indicatedTreatment gap- OK with lifestyle
Therapeutic inertia- more therapy needed
Therapeutic inertia- OK with lifestyle
Meeting target
9857 males and 8332 females in Australian general practiceOwen, Retegan, Rockell, Jennings and Reid CEPP Nov 2008
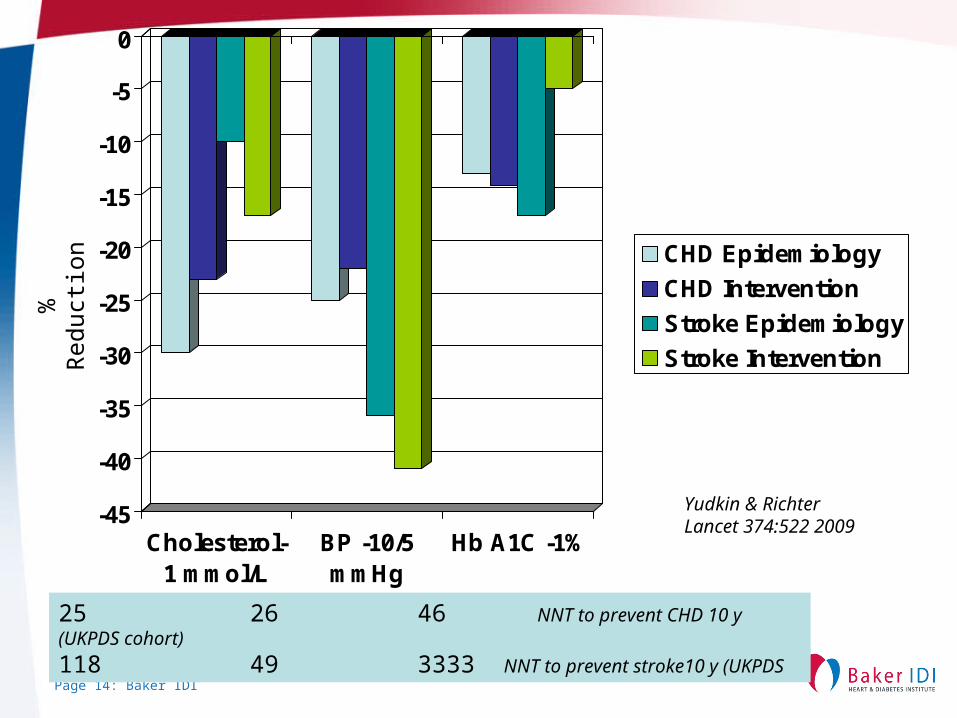
Page 14: Baker IDI
-45
-40
-35
-30
-25
-20
-15
-10
-5
0
Cholesterol-1 mmol/L
BP -10/5mmHg
Hb A1C -1%
CHD Epidemiology
CHD Intervention
Stroke Epidemiology
Stroke Intervention
25 26 46 NNT to prevent CHD 10 y (UKPDS cohort)
118 49 3333 NNT to prevent stroke10 y (UKPDS
%R
educ
tion
Yudkin & RichterLancet 374:522 2009
Page 15: Baker IDI
Atherosclerosis in the setting of diabetes
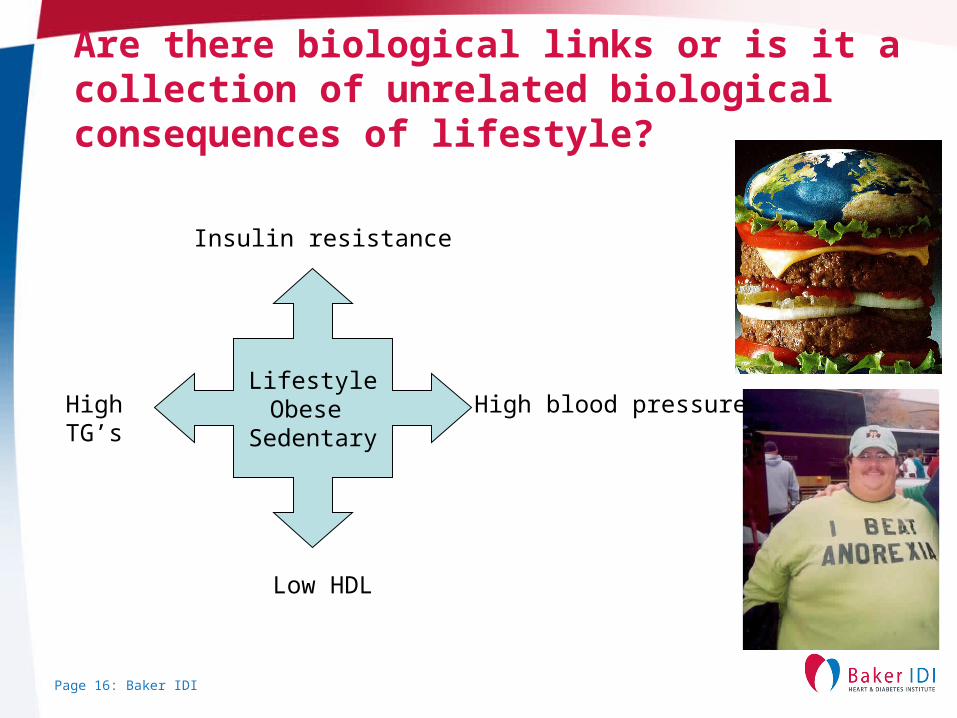
Page 16: Baker IDI
Are there biological links or is it a collection of unrelated biological consequences of lifestyle?
LifestyleObese
Sedentary
Insulin resistance
High blood pressure
Low HDL
HighTG’s
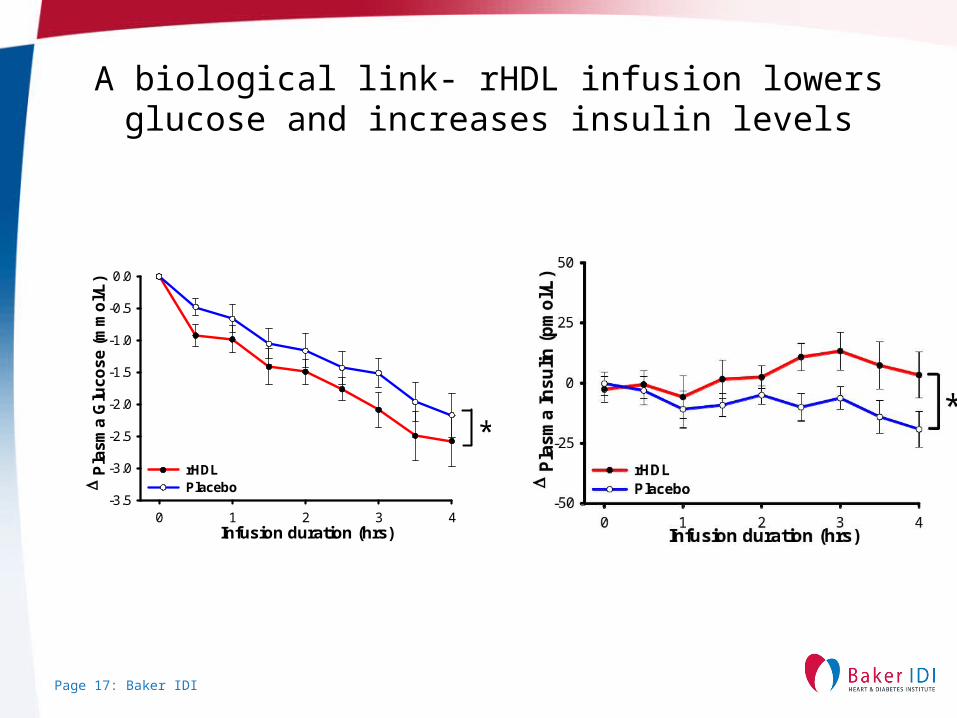
Page 17: Baker IDI
A biological link- rHDL infusion lowers glucose and increases insulin levels
Infusion duration (hrs)0 1 2 3 4
P
lasm
a G
luco
se (
mm
ol/
L)
-3.5
-3.0
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
rHDLPlacebo
*
Page 18: Baker IDI
Cellular and biochemical drivers of atherosclerosisAll atherosclerosis:
• Lipid retention by vascular matrix (proteoglycans) (Skalen et al., 2002)• “Inflammation” (Ross, 1999; Libby, 2006)• Oxidation (Witztum, 1994; Stocker and Keaney, 2004; Steinberg et al., 1989)• Endothelial injury/dysfunction (Ross, 1992; Davignon and Ganz, 2004)
Also in diabetes:
• Hyperglycaemia• Advanced glycation end products (AGEs and RAGEs)
(Brownlee, 2001, Forbes et al., 2004)• Hyperglycaemia/Oxidation/ROS
Page 19: Baker IDI
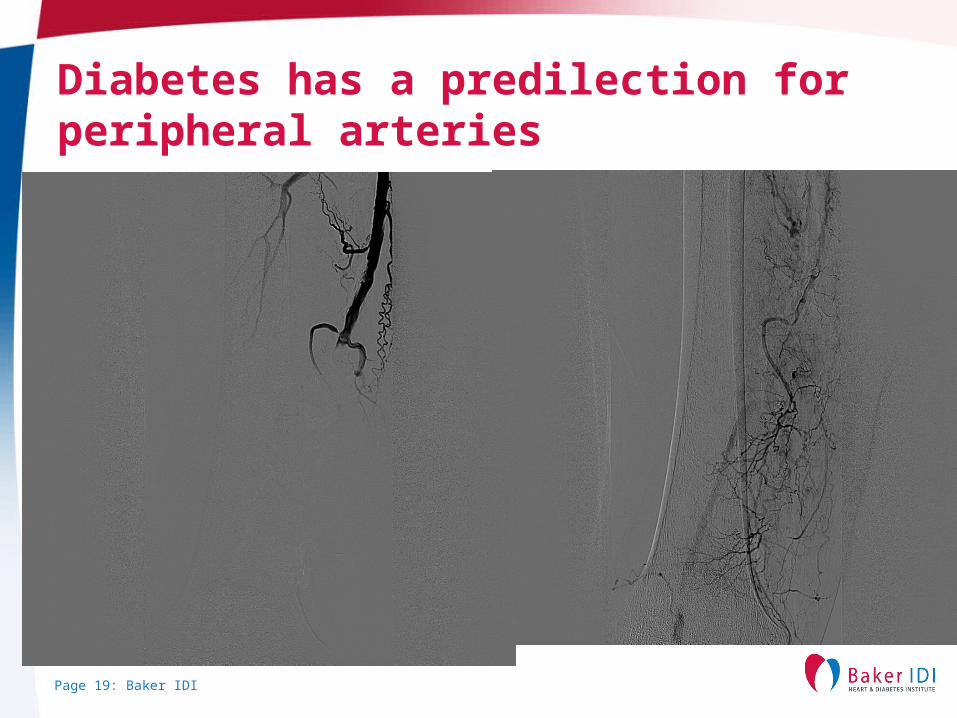
Diabetes has a predilection for peripheral arteries
Page 20: Baker IDI
Coronary disease in diabetes
More commonMore silent infarctsMore silent ischaemiaMore plaque instabilityMore sudden death
Page 21: Baker IDI
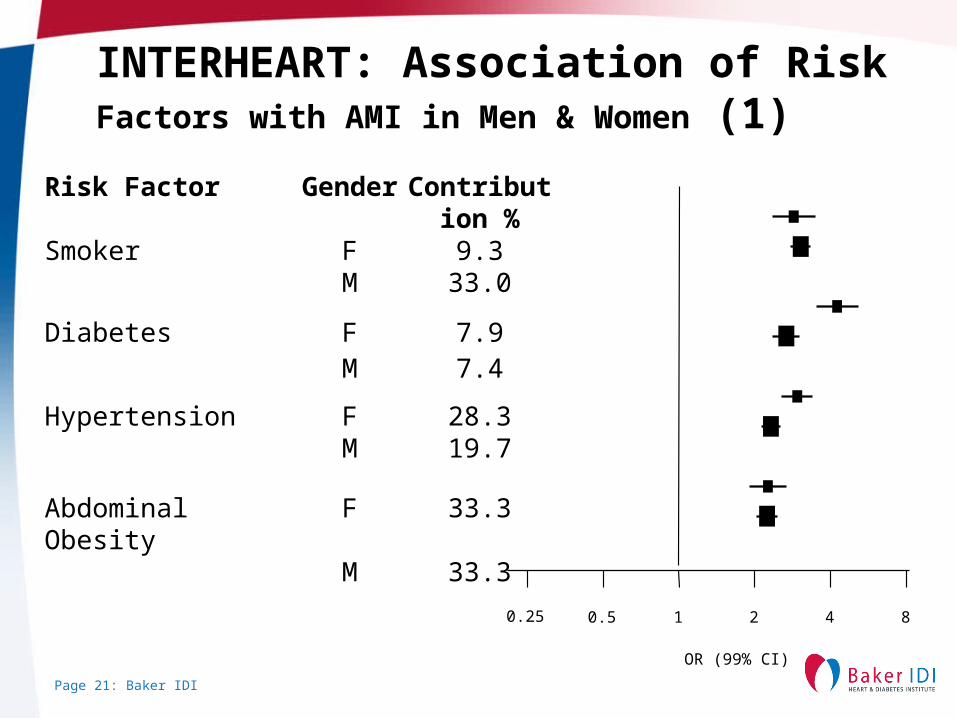
INTERHEART: Association of Risk Factors with AMI in Men & Women (1)
Risk Factor Gender Contribution %
Smoker F 9.3M 33.0
Diabetes F 7.9M 7.4
Hypertension F 28.3M 19.7
Abdominal Obesity F 33.3M 33.3
0.25 0.5 1 2 4 8
OR (99% CI)
Page 22: Baker IDI
Inci
den
ce o
f m
ult
ives
sel
dis
ease
(%
)
Single vessel disease is less common in diabetes
80
0
60
40
20
No diabetes Diabetes
n = 148
n = 923
Granger CB, Califf RM, Young S, et al. J Am Coll Cardiol 1993; 21:920–925.
Page 23: Baker IDI
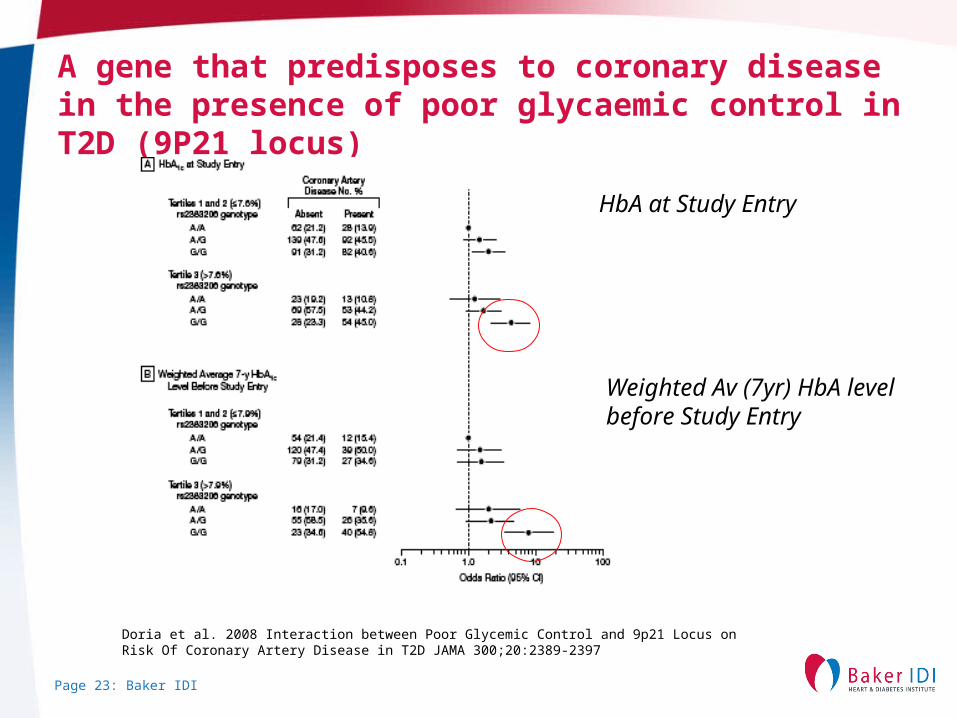
A gene that predisposes to coronary disease in the presence of poor glycaemic control in T2D (9P21 locus)
HbA at Study Entry
Weighted Av (7yr) HbA level before Study Entry
Doria et al. 2008 Interaction between Poor Glycemic Control and 9p21 Locus on Risk Of Coronary Artery Disease in T2D JAMA 300;20:2389-2397
Page 24: Baker IDI
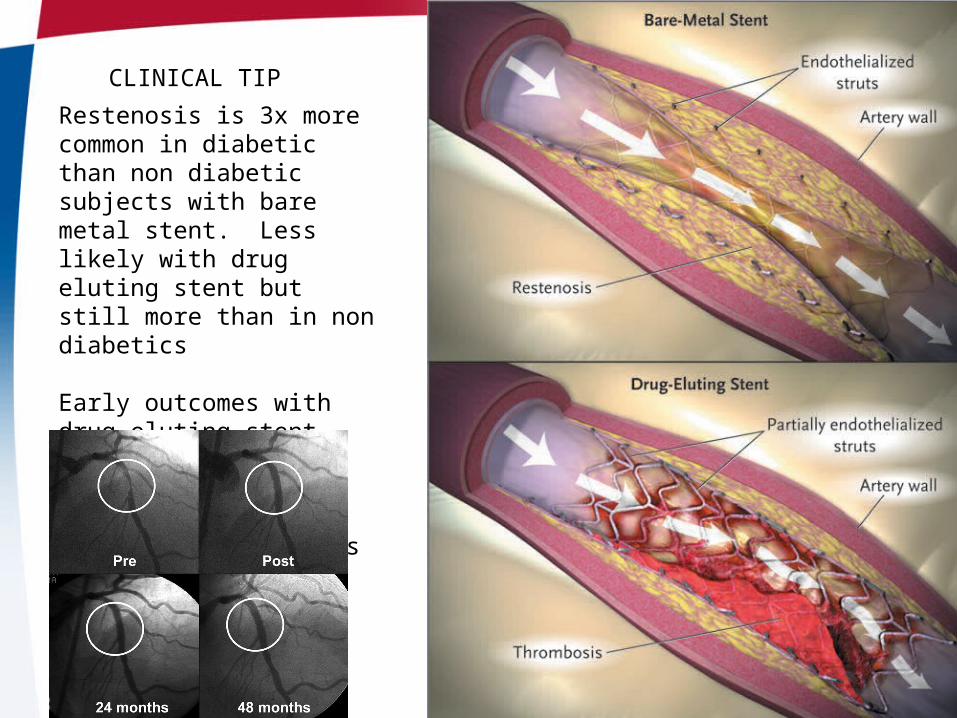
Restenosis is 3x more common in diabetic than non diabetic subjects with bare metal stent. Less likely with drug eluting stent but still more than in non diabetics
Early outcomes with drug eluting stent match CABG (NY registry) but confounding likely- await FREEDOM results
CLINICAL TIP
Page 25: Baker IDI
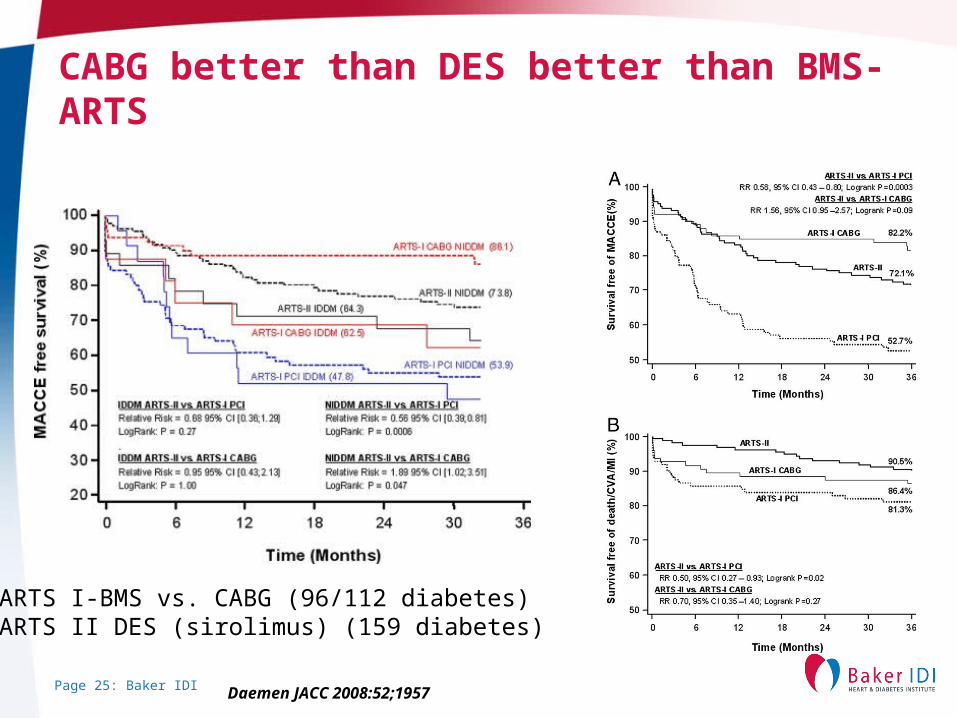
CABG better than DES better than BMS-ARTS
ARTS I-BMS vs. CABG (96/112 diabetes)ARTS II DES (sirolimus) (159 diabetes)
Daemen JACC 2008:52;1957
Page 26: Baker IDI
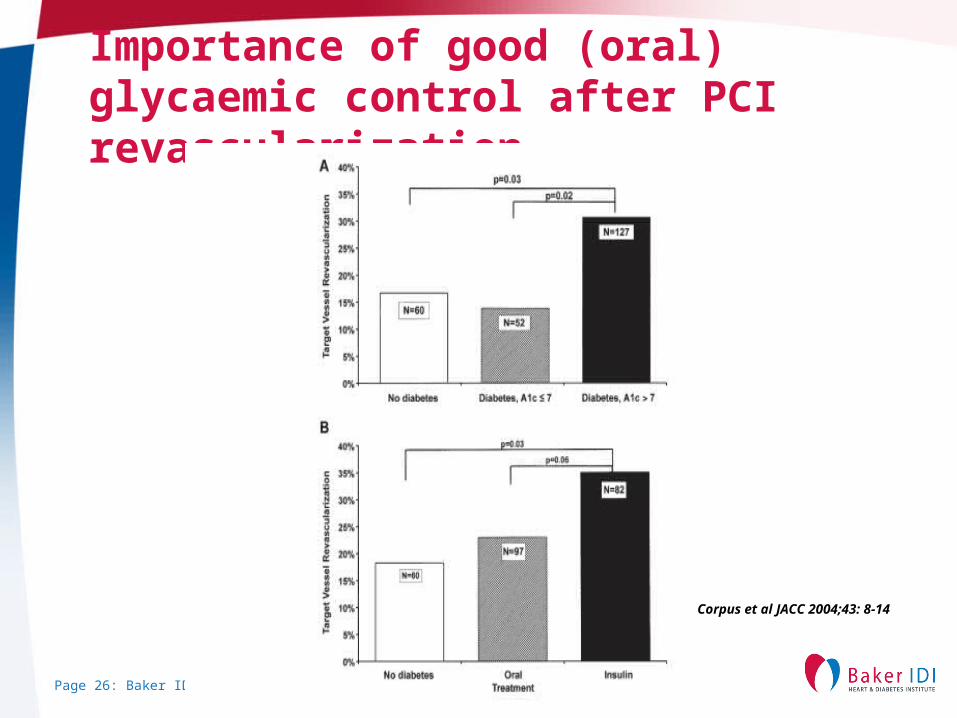
Importance of good (oral) glycaemic control after PCI revascularization
Corpus et al JACC 2004;43: 8-14
Page 27: Baker IDI
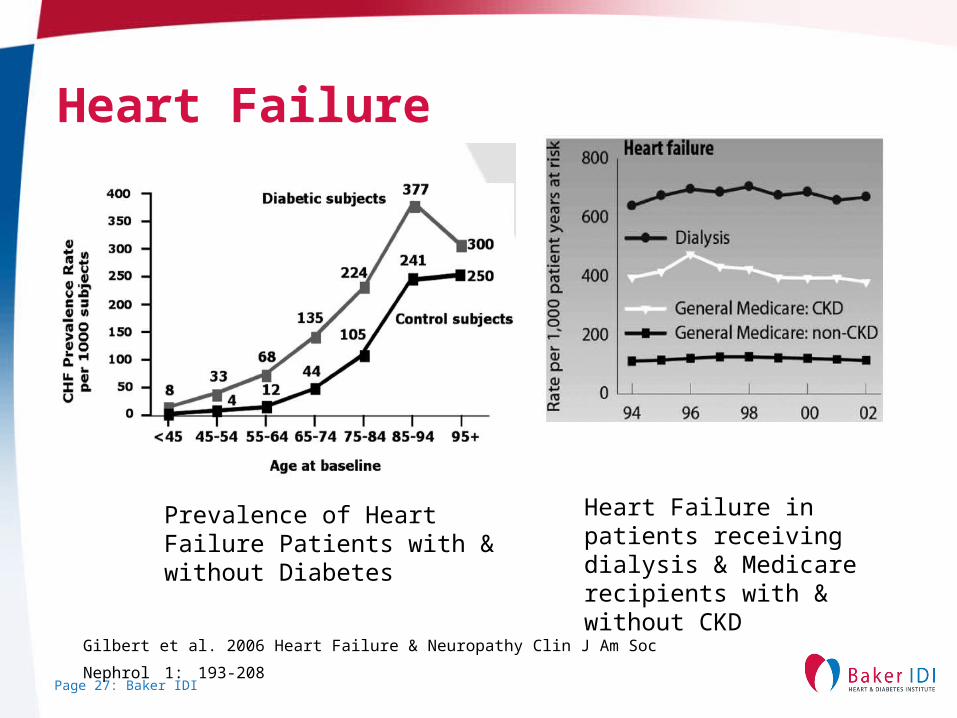
Heart Failure
Gilbert et al. 2006 Heart Failure & Neuropathy Clin J Am Soc Nephrol 1: 193-208
Prevalence of Heart Failure Patients with & without Diabetes
Heart Failure in patients receiving dialysis & Medicare recipients with & without CKD
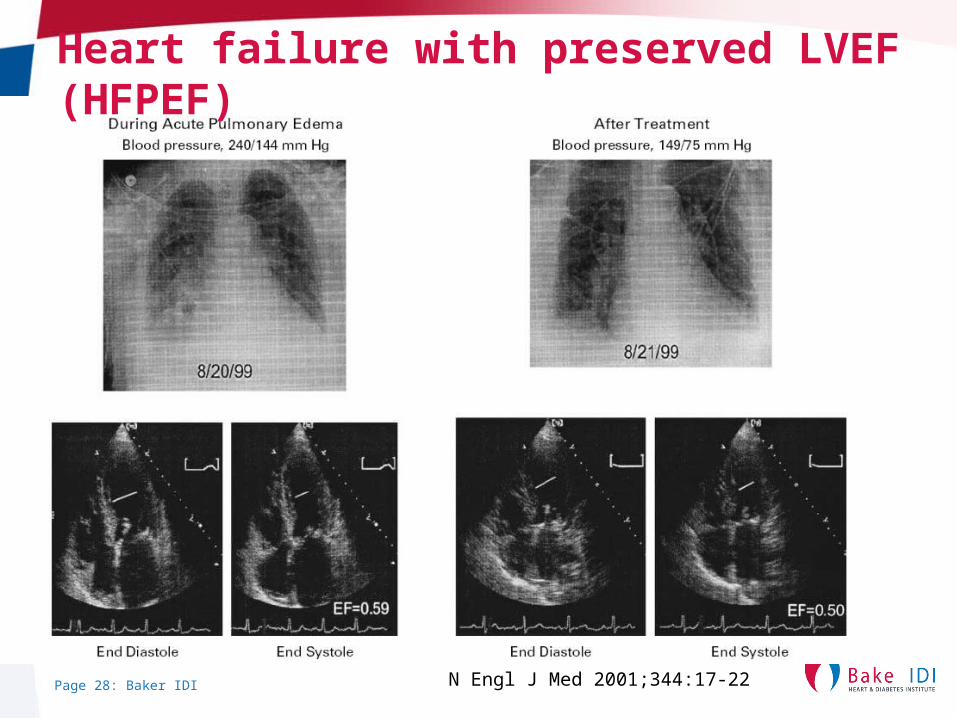
Page 28: Baker IDI N Engl J Med 2001;344:17-22
Heart failure with preserved LVEF (HFPEF)
Page 29: Baker IDI
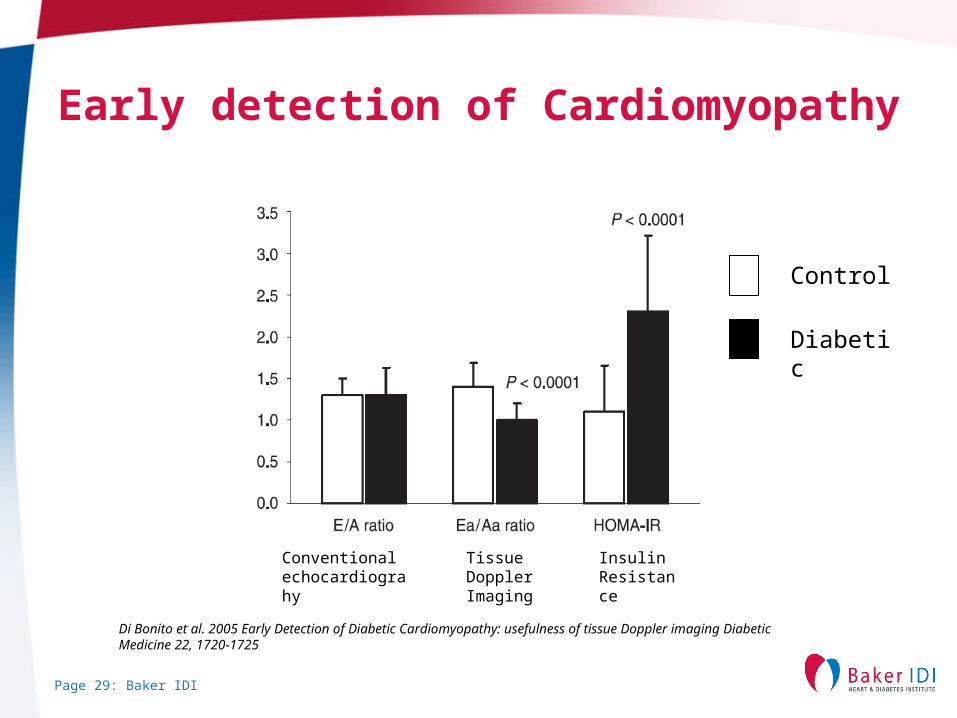
Early detection of Cardiomyopathy
Di Bonito et al. 2005 Early Detection of Diabetic Cardiomyopathy: usefulness of tissue Doppler imaging Diabetic Medicine 22, 1720-1725
Conventional echocardiograhy
Control
Diabetic
Tissue Doppler Imaging
Insulin Resistance
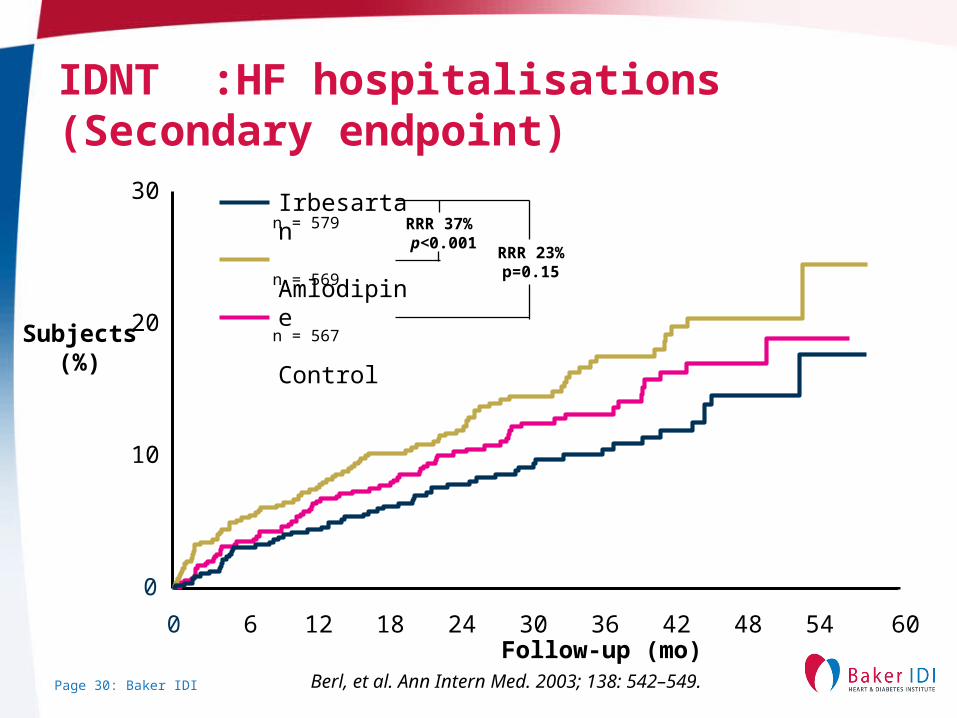
Page 30: Baker IDI
Subjects(%)
Irbesartan
Amlodipine
Control
RRR 37% p<0.001
RRR 23%p=0.15
0 6 12 18 24 30 36 42 48 54Follow-up (mo)
60
0
10
20
30
IDNT :HF hospitalisations(Secondary endpoint)
Berl, et al. Ann Intern Med. 2003; 138: 542–549.
n = 579
n = 569
n = 567
Page 31: Baker IDI
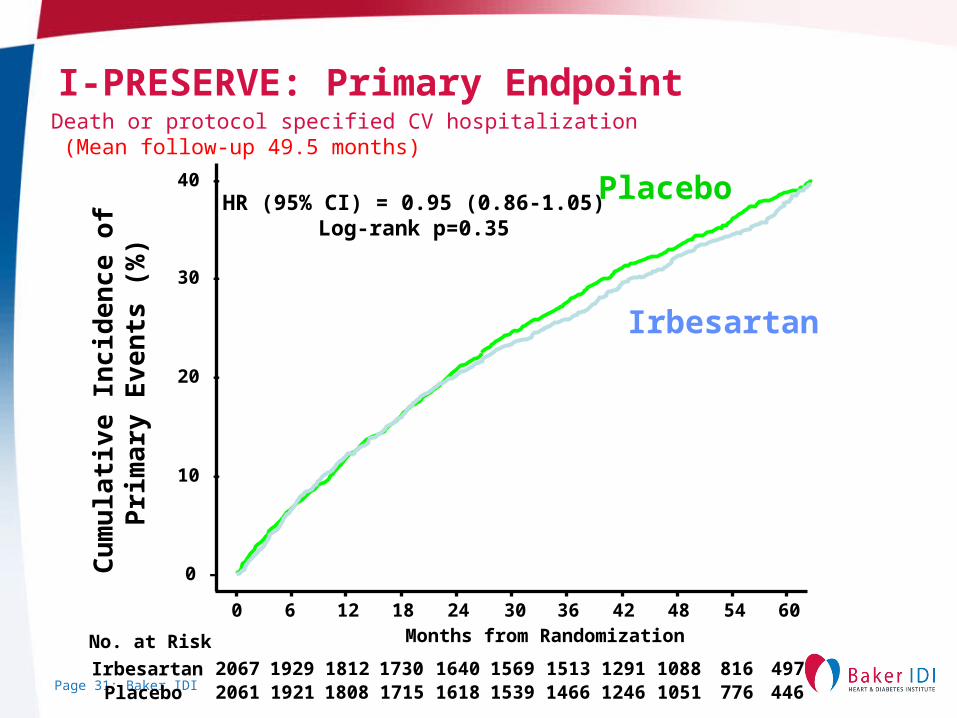
I-PRESERVE: Primary Endpoint
Months from Randomization
Cu
mu
lati
ve In
cid
enc
e o
f P
rim
ary
Eve
nts
(%
)
40 -
0 -
10 -
20 -
30 -
0 6 12 18 24 36 4230 48 6054
2067 1929 1812 1730 1640 1513 12911569 1088 4978162061 1921 1808 1715 1618 1466 12461539 1051 446776
No. at Risk
IrbesartanPlacebo
HR (95% CI) = 0.95 (0.86-1.05)Log-rank p=0.35
Placebo
Irbesartan
Death or protocol specified CV hospitalization (Mean follow-up 49.5 months)
Page 32: Baker IDI
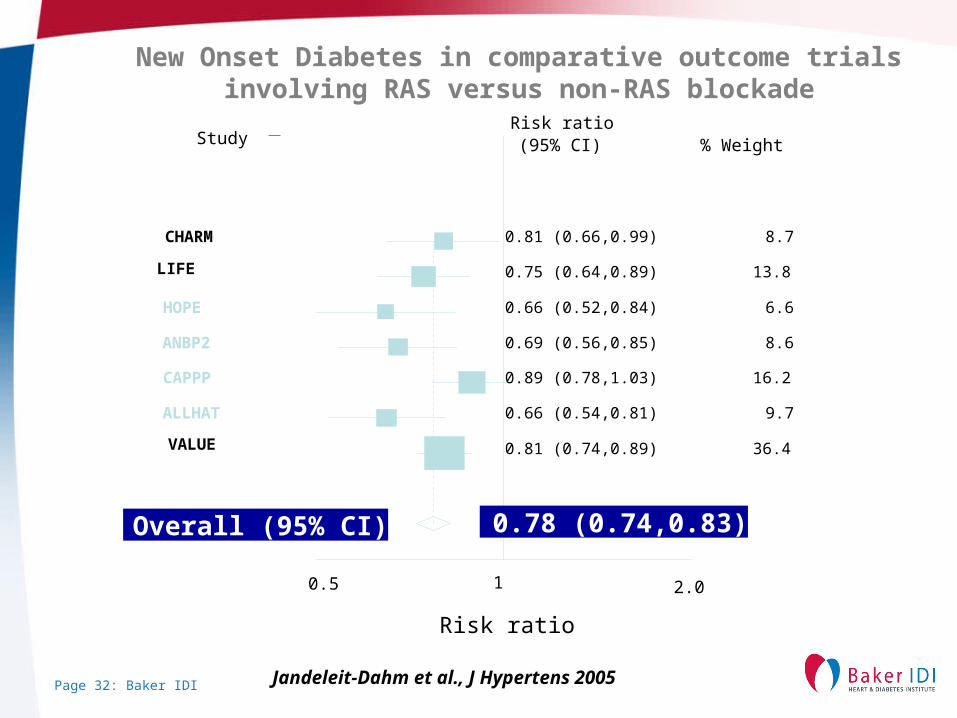
Risk ratio
0.5 1 2.0
Study % Weight Risk ratio (95% CI)
0.81 (0.66,0.99) CHARM 8.7
0.75 (0.64,0.89) LIFE 13.8
0.66 (0.52,0.84) HOPE 6.6
0.69 (0.56,0.85) ANBP2 8.6
0.89 (0.78,1.03) CAPPP 16.2
0.66 (0.54,0.81) ALLHAT 9.7
0.81 (0.74,0.89) VALUE 36.4
0.78 (0.74,0.83) Overall (95% CI)
New Onset Diabetes in comparative outcome trials involving RAS versus non-RAS blockade
Jandeleit-Dahm et al., J Hypertens 2005
Page 33: Baker IDI
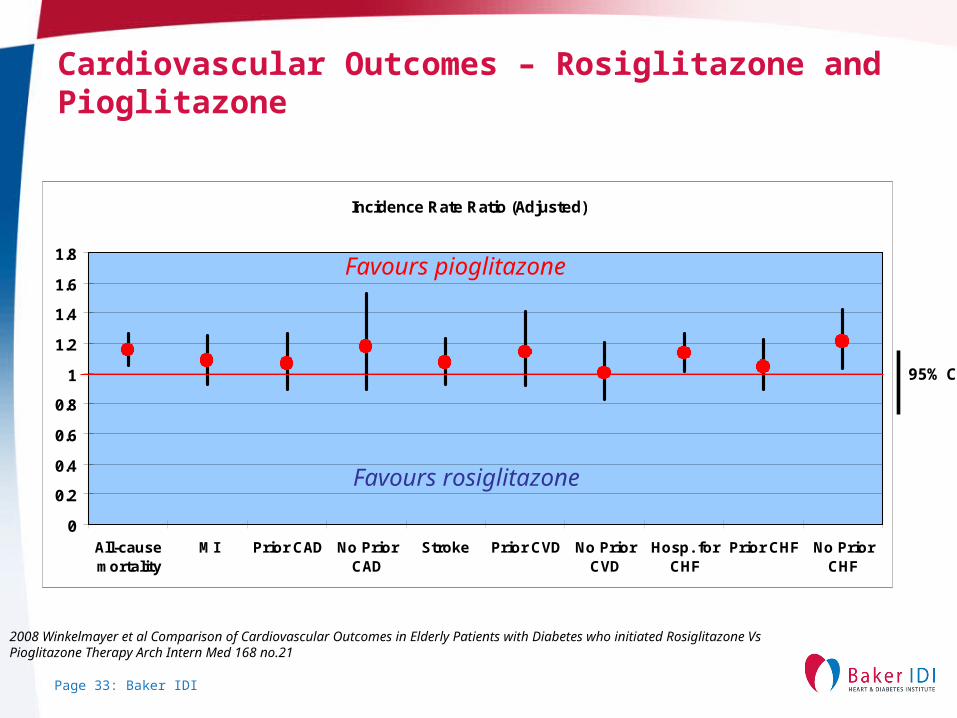
Cardiovascular Outcomes – Rosiglitazone and Pioglitazone
Incidence Rate Ratio (Adjusted)
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
All-causemortality
MI Prior CAD No PriorCAD
Stroke Prior CVD No PriorCVD
Hosp. forCHF
Prior CHF No PriorCHF
2008 Winkelmayer et al Comparison of Cardiovascular Outcomes in Elderly Patients with Diabetes who initiated Rosiglitazone Vs Pioglitazone Therapy Arch Intern Med 168 no.21
95% CI
Favours pioglitazone
Favours rosiglitazone
Page 34: Baker IDI
Most guidelines recommend aspirin as primary prevention in those with diabetes• Evidence is circumstantial
• Japanese aspirin trial in diabetics (2009)– Primary end point not met– 90% reduction in secondary end point- fatal
coronary disease and stroke
• Sub study of Nurse Health Study also supportive (2008)
Page 35: Baker IDI
WHAT CAN BAKER IDI BRING TO INDIGENOUS CVD AND DIABETES?
Page 36: Baker IDI
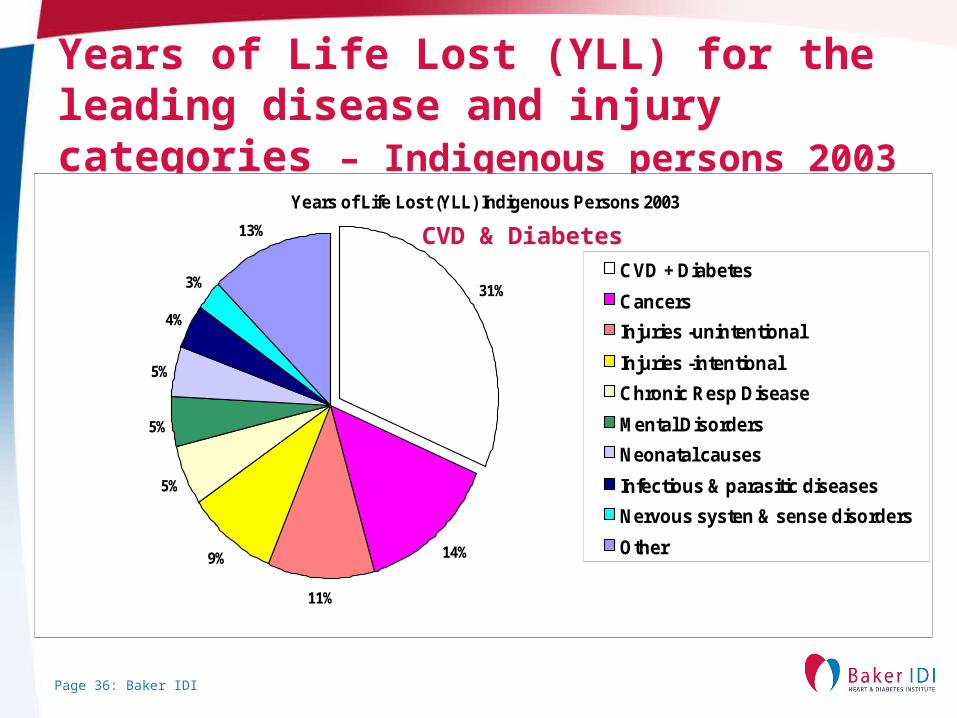
Years of Life Lost (YLL) for the leading disease and injury categories – Indigenous persons 2003
Years of Life Lost (YLL) Indigenous Persons 2003
31%
14%
11%
9%
5%
5%
5%
4%
3%
13%
CVD + Diabetes
Cancers
Injuries -unintentional
Injuries -intentional
Chronic Resp Disease
Mental Disorders
Neonatal causes
Infectious & parasitic diseases
Nervous systen & sense disorders
Other
CVD & Diabetes
Page 37: Baker IDI
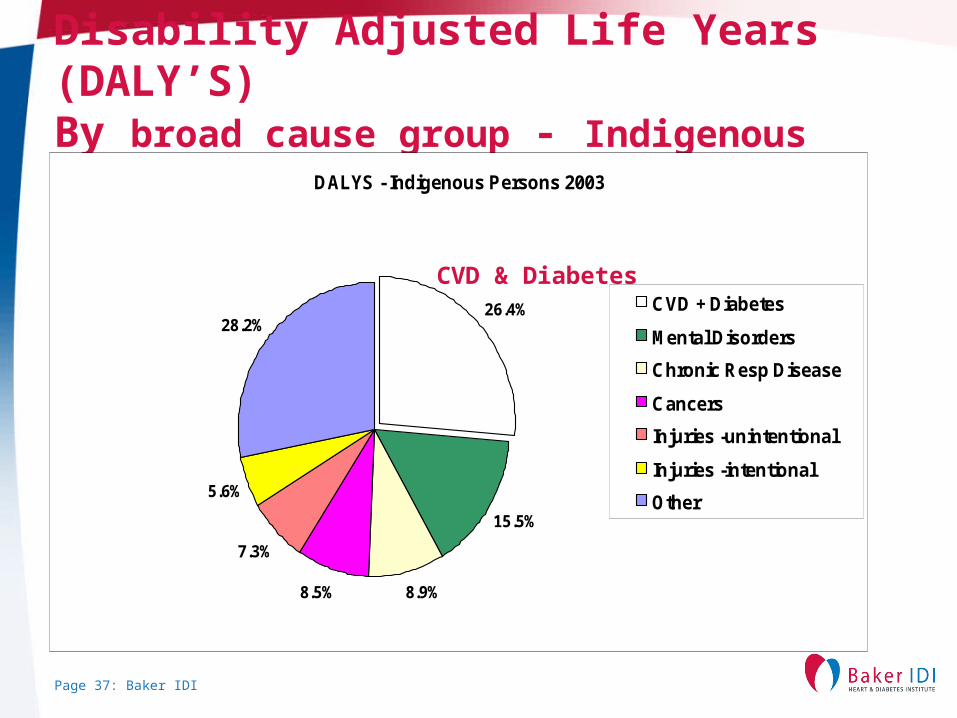
Disability Adjusted Life Years (DALY’S)By broad cause group - Indigenous Persons 2003 DALYS - Indigenous Persons 2003
8.9%8.5%
7.3%
5.6%
15.5%
28.2%26.4% CVD + Diabetes
Mental Disorders
Chronic Resp Disease
Cancers
Injuries -unintentional
Injuries -intentional
Other
CVD & Diabetes
Page 38: Baker IDI
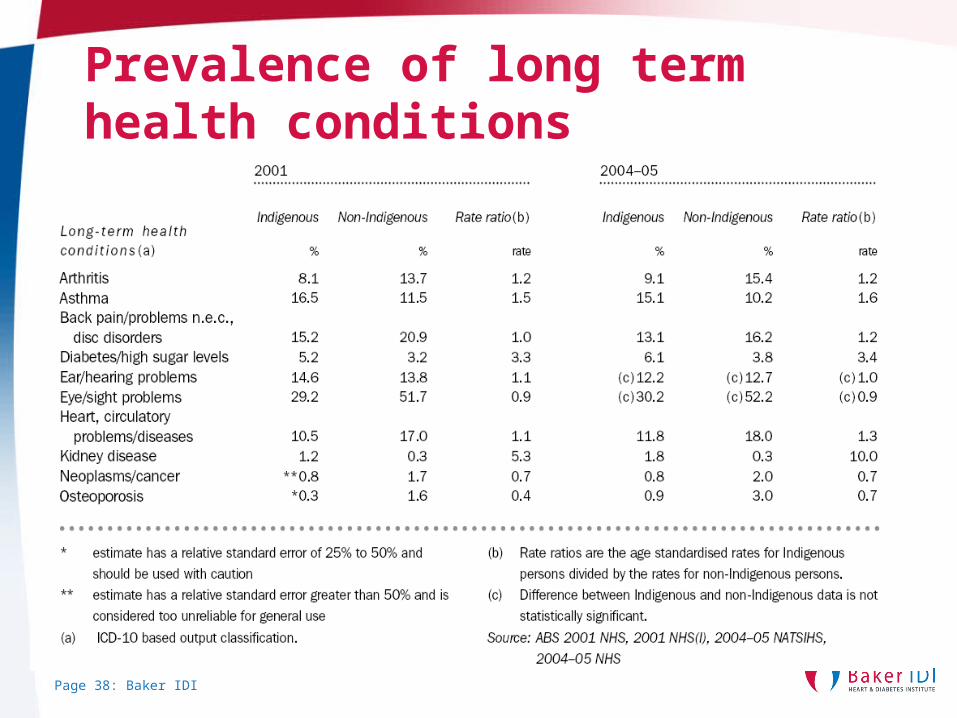
Prevalence of long term health conditions
Page 39: Baker IDI
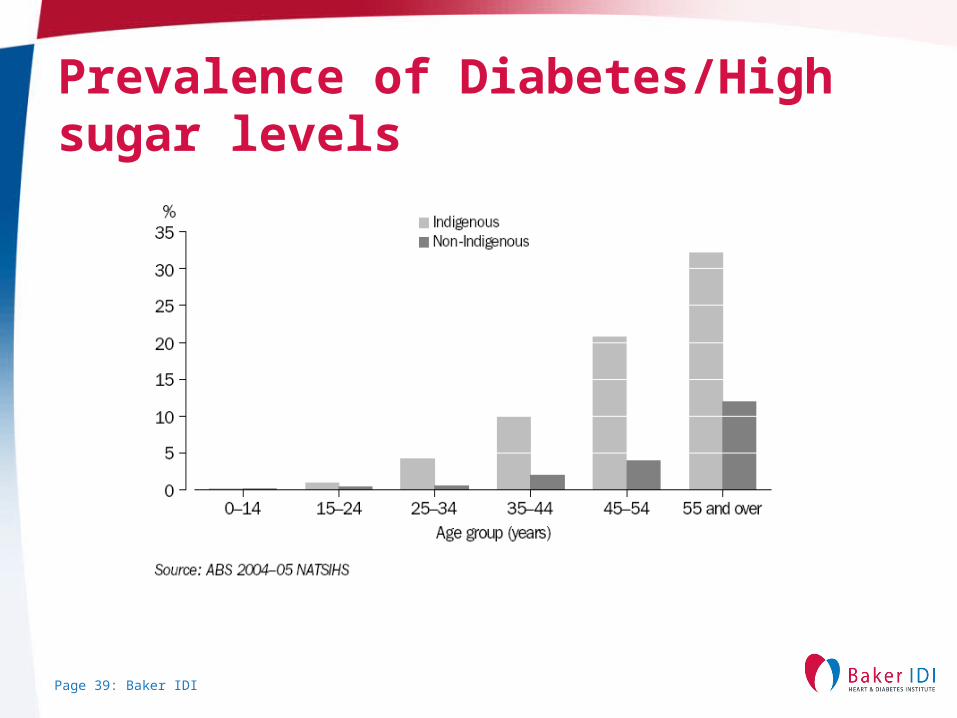
Prevalence of Diabetes/High sugar levels
Page 40: Baker IDI
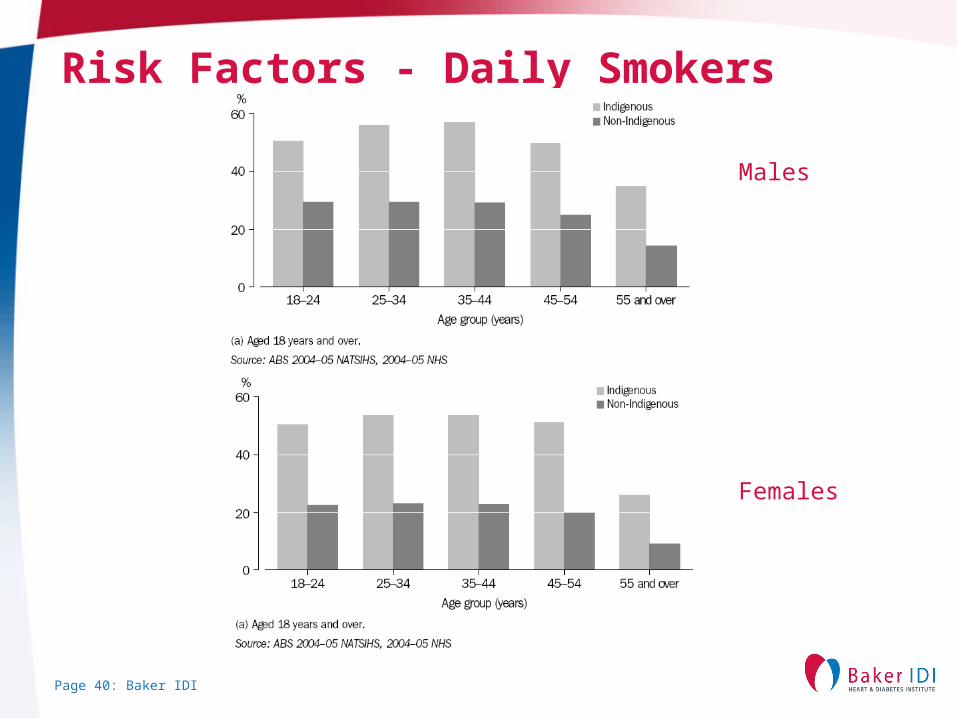
Risk Factors - Daily Smokers
Males
Females
Page 41: Baker IDI
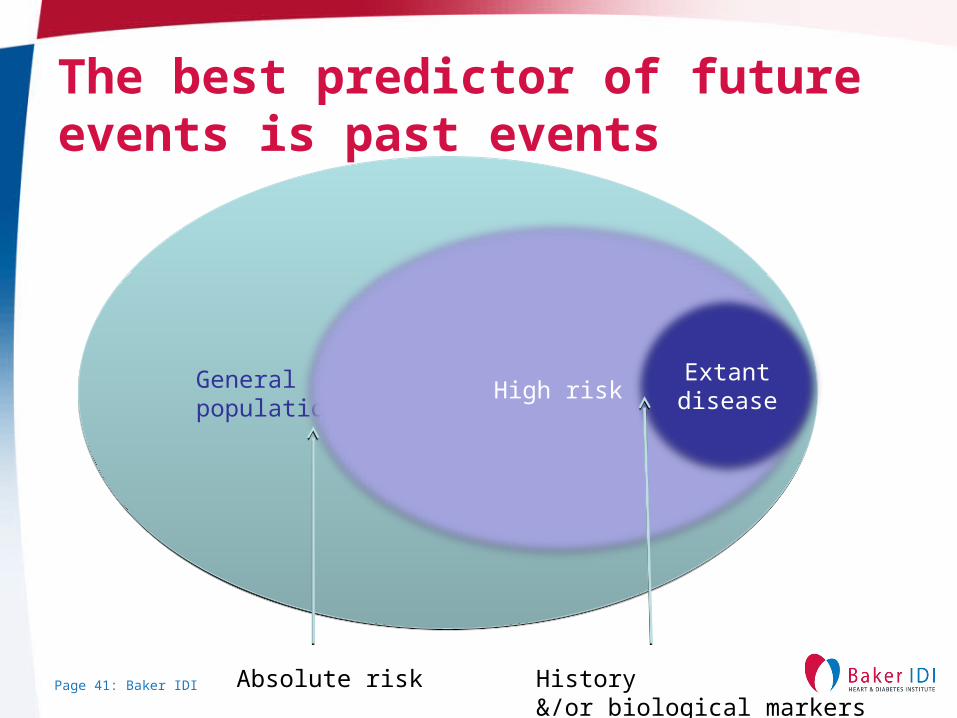
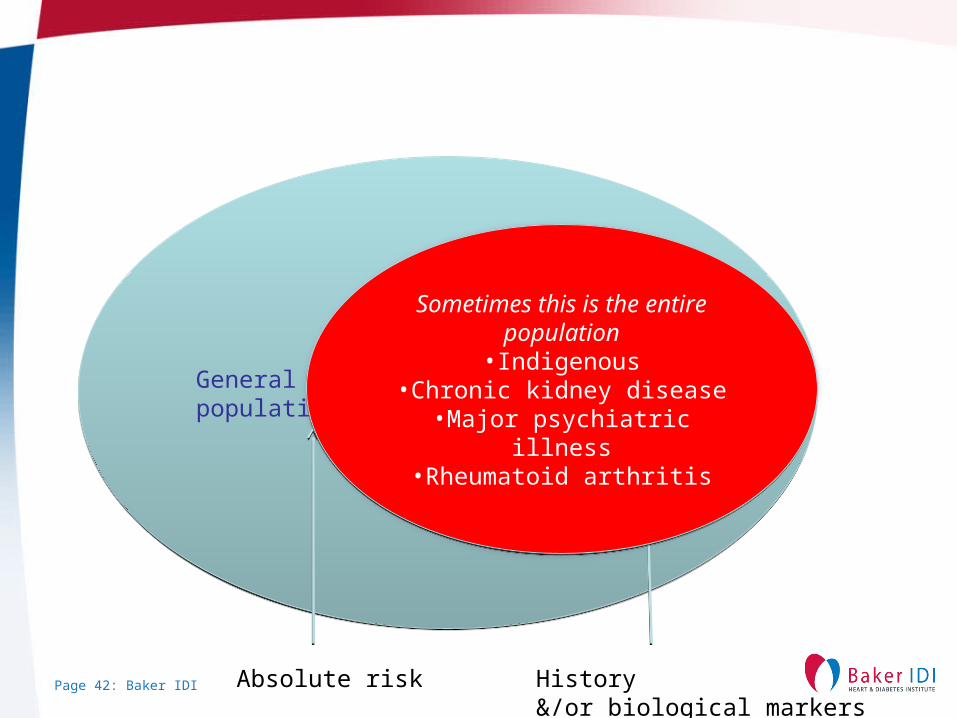
The best predictor of future events is past events
General populationGeneral population
High riskExtant
disease
Absolute risk History&/or biological markers
Page 42: Baker IDI
General populationGeneral population
High riskExtant
disease
Absolute risk History&/or biological markers
Sometimes this is the entire population
•Indigenous•Chronic kidney disease•Major psychiatric illness
•Rheumatoid arthritis
Sometimes this is the entire population
•Indigenous•Chronic kidney disease•Major psychiatric illness
•Rheumatoid arthritis
Page 43: Baker IDI
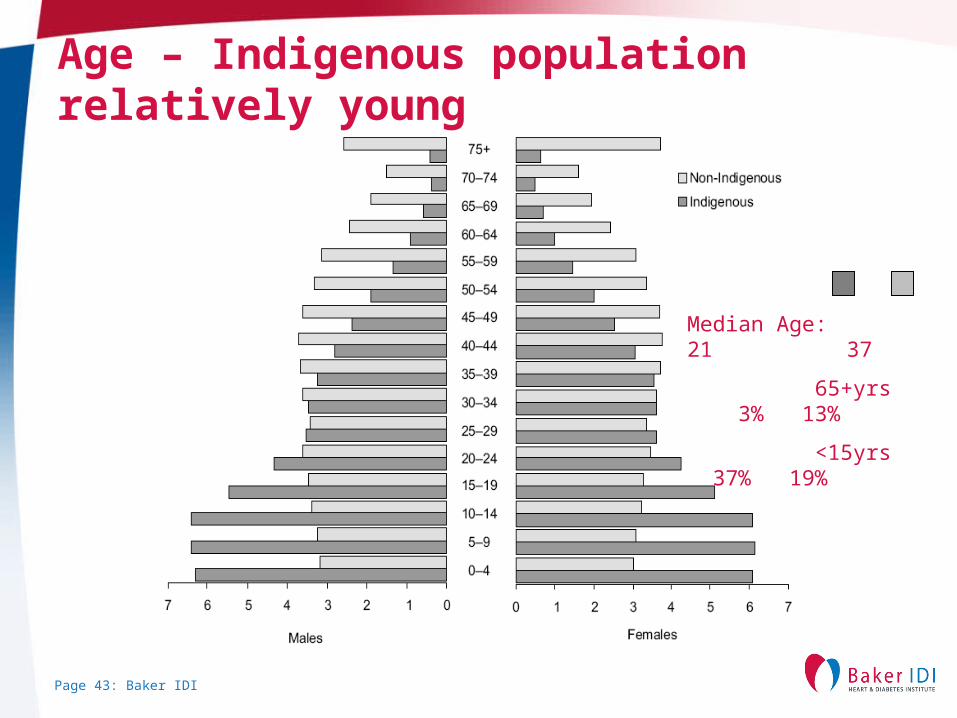
Age – Indigenous population relatively young
Median Age: 21 37
65+yrs 3% 13%
<15yrs 37% 19%
Page 44: Baker IDI
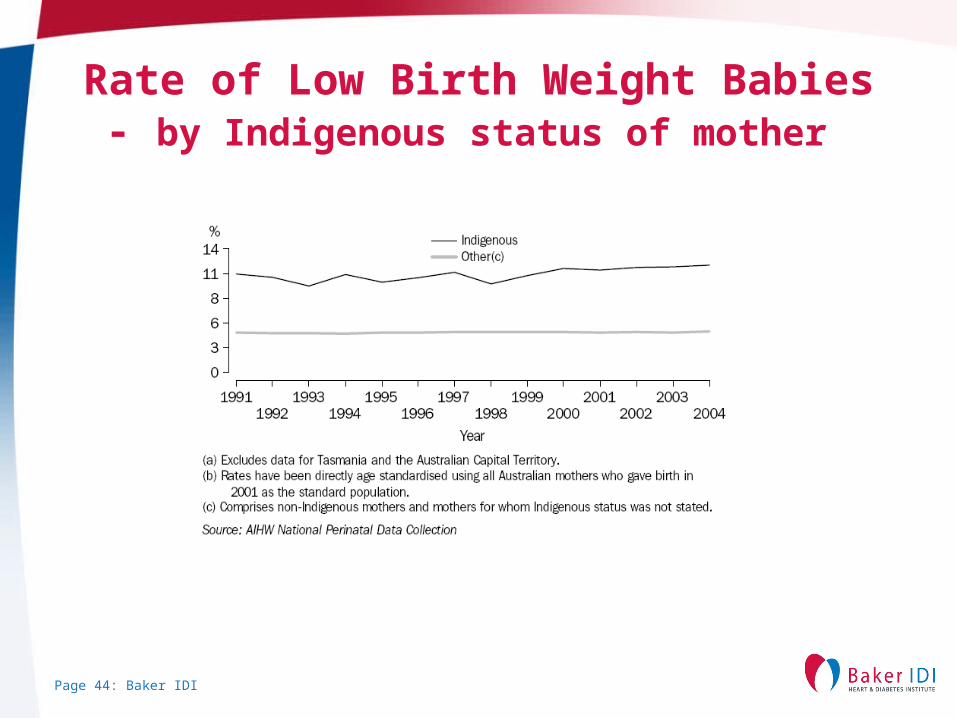
Rate of Low Birth Weight Babies- by Indigenous status of mother
Page 45: Baker IDI
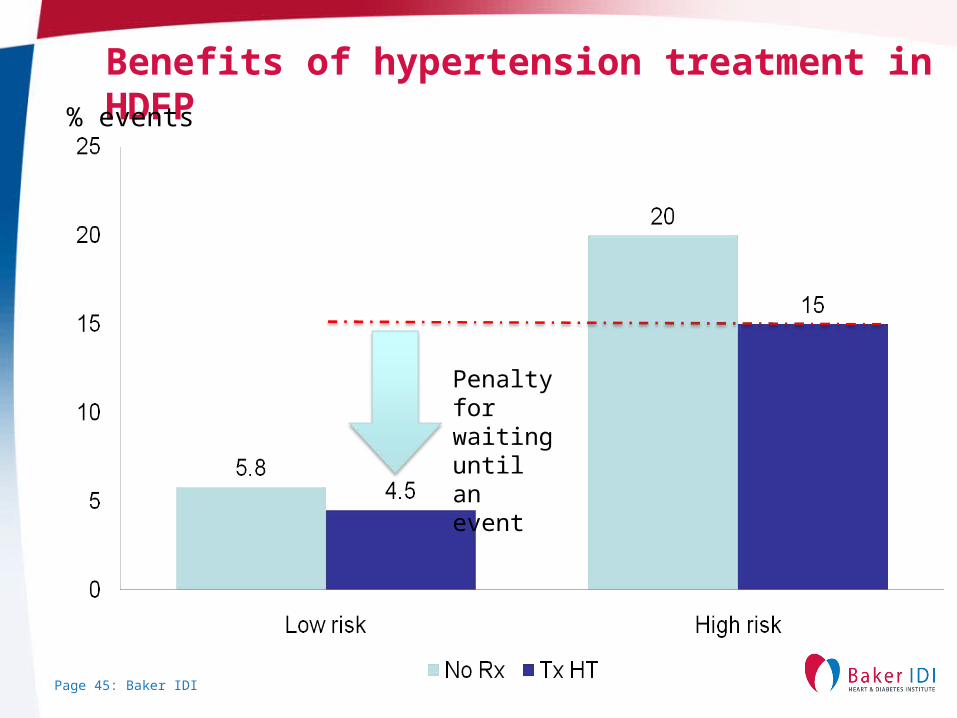
Benefits of hypertension treatment in HDFP% events
Penalty for waiting until an event
Page 46: Baker IDI
DiabetesDyslipidaemiaHypertension
NutritionExercise
Early lifePregnancy Childhood obesity
Risk Factors
SubClinicalorgan damage
ArteriesHeartBrain KidneysEyes etc
Acute Complications
Chronic Complications
Heart Failure
Terminal Disease
Angina
Kidney Failure
Dementia
Sudden Death
Thrombosis
Aneurysm
Prevention X
Prevention X
Prevention X
Prevention X
Prevention XBasic research on
metabolic memory (epigenetics)
Maternal interventionsGestational diabetes markers (proteomics)
Metabolic syndrome/obesity
Screening and intervention in rural and
remote communitiesNutritional interventions
PolypillResistant hypertension
Hearts and minds
Prevention of diabetes complications
LVHPAD treatment
Novel anti thromboticsCIN
Unstable plaque markers
Aneurysm treatment
Heart failure screeningDisease managementGene and stem cell
therapiesHFPEF
Page 47: Baker IDI
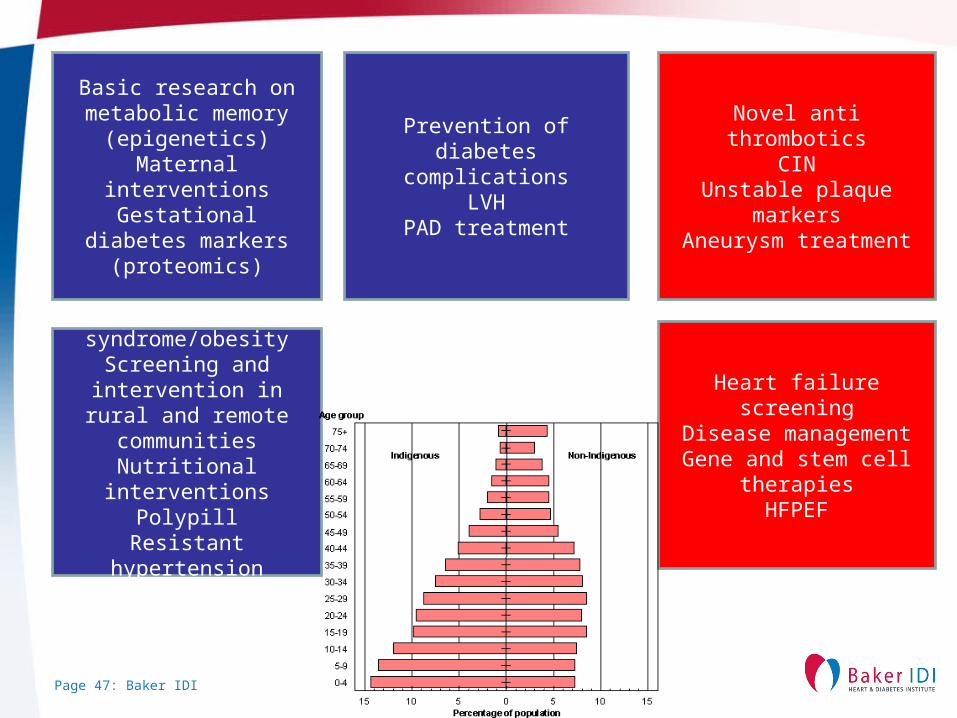
Basic research on metabolic memory
(epigenetics)Maternal interventionsGestational diabetes markers (proteomics)
Metabolic syndrome/obesity
Screening and intervention in rural and
remote communitiesNutritional interventions
PolypillResistant hypertension
Hearts and minds
Prevention of diabetes complications
LVHPAD treatment
Novel anti thromboticsCIN
Unstable plaque markersAneurysm treatment
Heart failure screeningDisease management
Gene and stem cell therapiesHFPEF
Page 48: Baker IDI
Conclusions
• The link between diabetes and CVD is strong but can be mitigated– Primary and ‘secondary’ prevention– Achieve blood pressure targets– Achieve glycaemia targets (?)– Special role for RAS inhibition?– Integrated care
Page 49: Baker IDI





























