Embed Size (px)
Citation preview
Page 1: Baker IDI
Update on therapies for type 2 diabetes
Page 2: Baker IDI
Treatment algorithms for type 2 diabetes
Page 3: Baker IDI
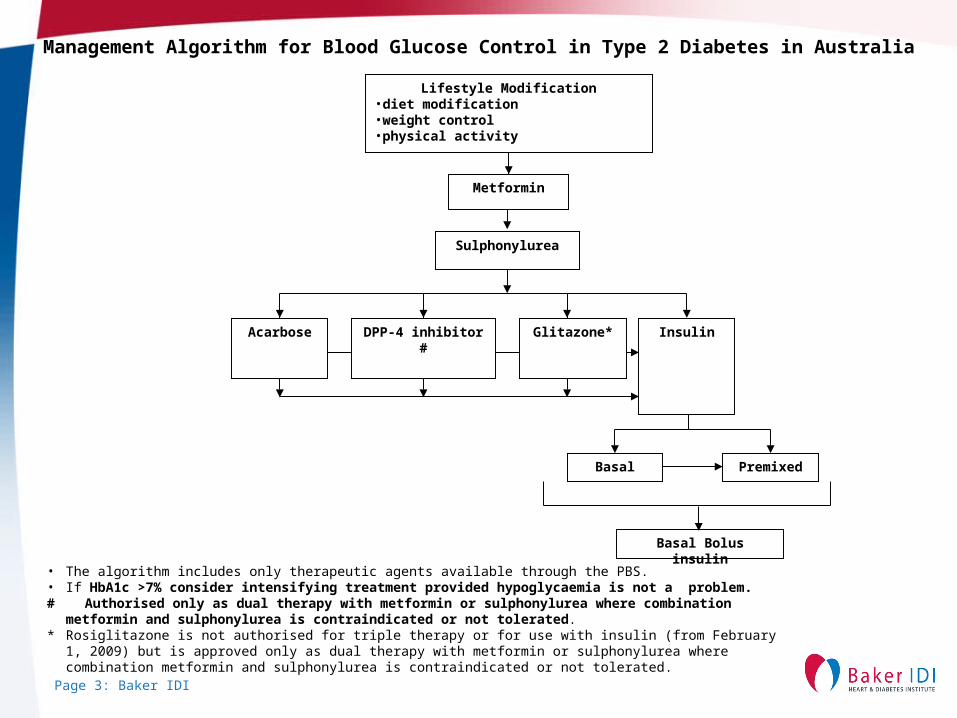
Basal Premixed
Basal Bolus insulin
Sulphonylurea
Acarbose DPP-4 inhibitor # Glitazone* Insulin
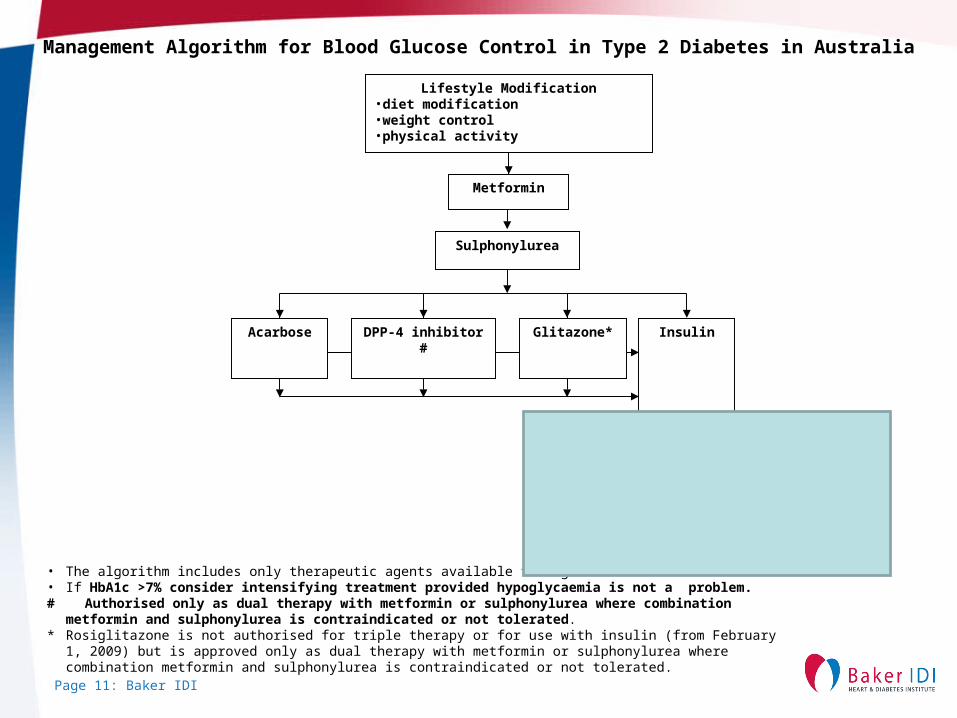
Lifestyle Modification•diet modification•weight control•physical activity
Metformin
Management Algorithm for Blood Glucose Control in Type 2 Diabetes in Australia
• The algorithm includes only therapeutic agents available through the PBS.• If HbA1c >7% consider intensifying treatment provided hypoglycaemia is not a problem.# Authorised only as dual therapy with metformin or sulphonylurea where combination metformin and sulphonylurea
is contraindicated or not tolerated.* Rosiglitazone is not authorised for triple therapy or for use with insulin (from February 1, 2009) but is approved only as dual
therapy with metformin or sulphonylurea where combination metformin and sulphonylurea is contraindicated or not tolerated.
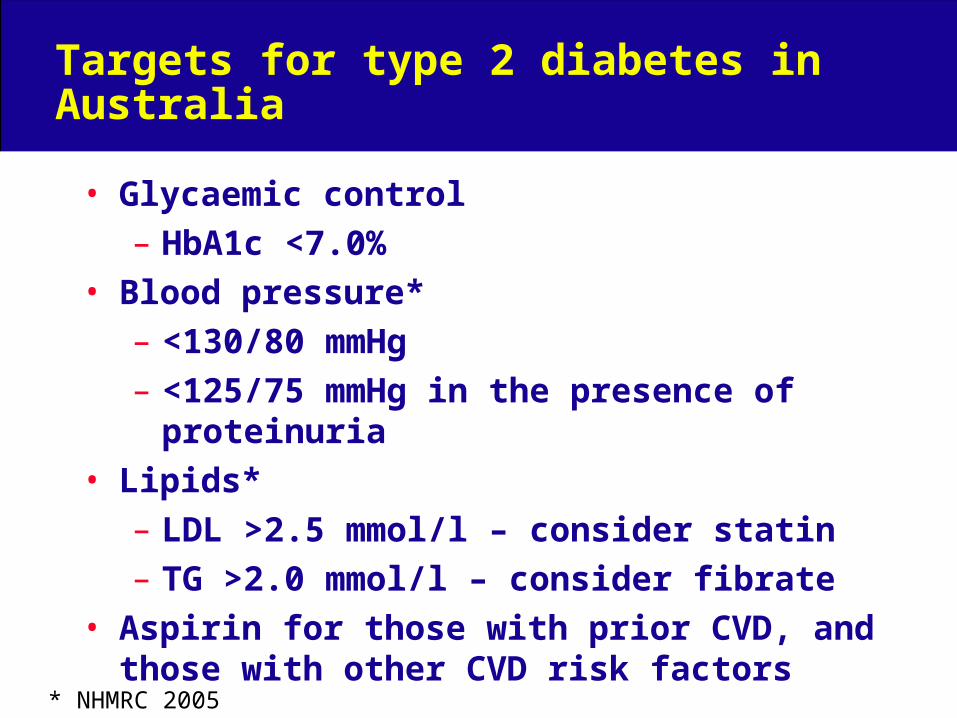
Targets for type 2 diabetes in Australia
• Glycaemic control
– HbA1c <7.0%
• Blood pressure*
– <130/80 mmHg
– <125/75 mmHg in the presence of proteinuria
• Lipids*
– LDL >2.5 mmol/l – consider statin
– TG >2.0 mmol/l – consider fibrate
• Aspirin for those with prior CVD, and those with other CVD risk factors
* NHMRC 2005
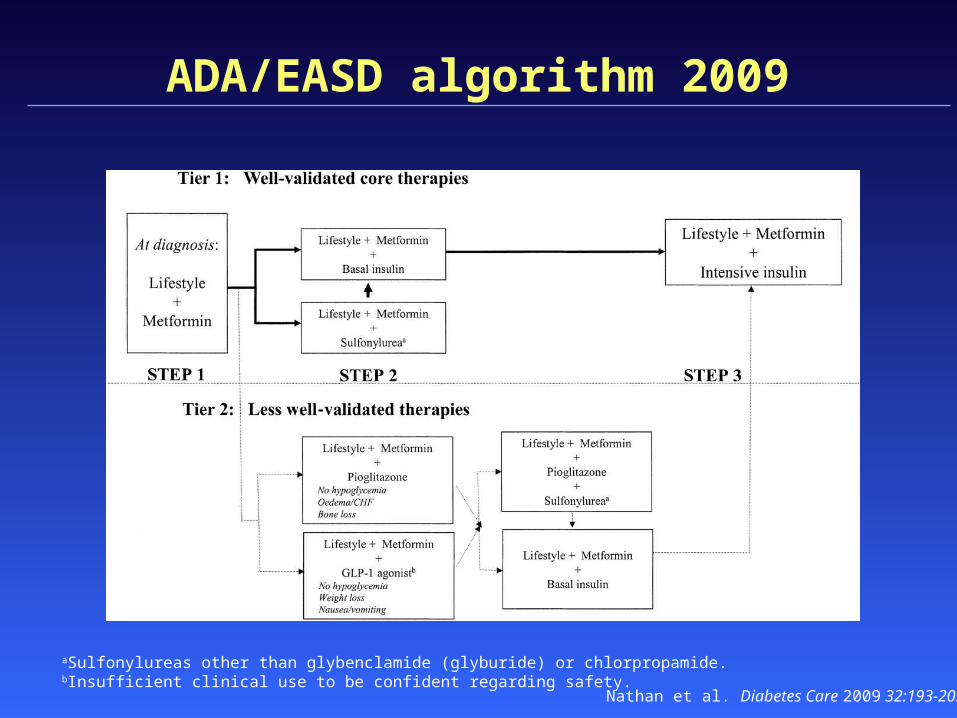
ADA/EASD algorithm 2009
aSulfonylureas other than glybenclamide (glyburide) or chlorpropamide.bInsufficient clinical use to be confident regarding safety.
Nathan et al. Diabetes Care 2009 32:193-203
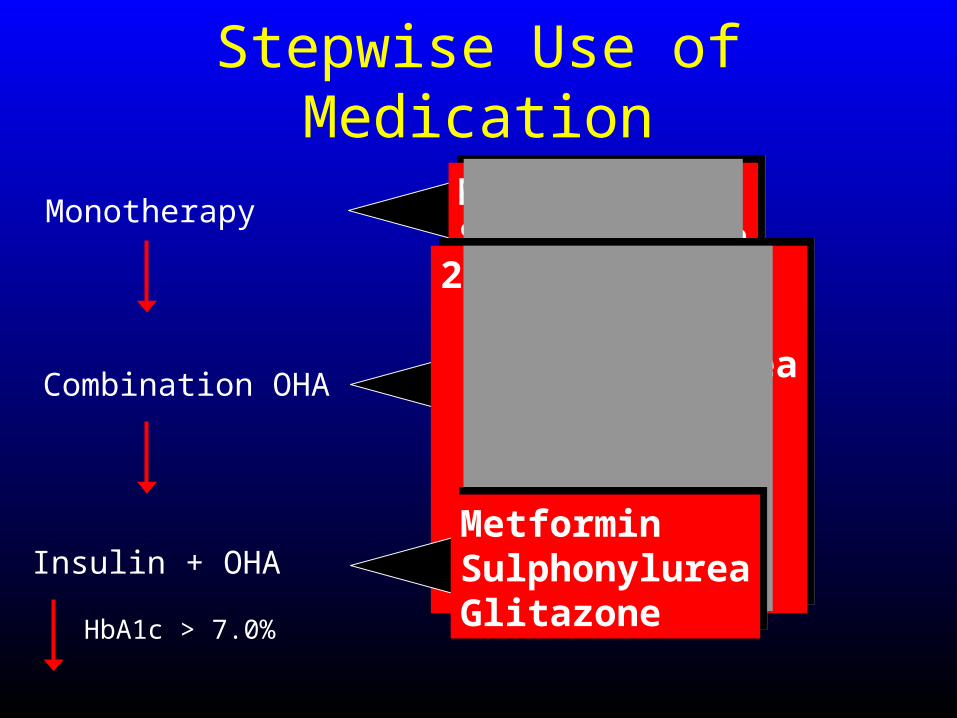
Stepwise Use of Medication
Monotherapy
Combination OHA
Insulin + OHA
HbA1c > 7.0%
MetforminSulphonylureaMetforminSulphonylurea2 or more of: Metformin Sulphonylurea Acarbose Glitazone Glinide GLP1 DPPIV
2 or more of: Metformin Sulphonylurea Acarbose Glitazone Glinide GLP1 DPPIV
MetforminSulphonylureaGlitazone
MetforminSulphonylureaGlitazone
Thiazoledinediones – Australian PBS restrictions
• Dual therapy, ie. rosiglitazone or pioglitazone, when SU or metformin contra-indicated or causes adverse event
• Triple oral therapy NOW pioglitazone only!
• Can be combined with insulin NOW pioglitazone only!
• HbA1c must be >7.0% at initiation• Precautions: fluid retention, bone loss, (?coronary
events with rosigltazone)

Page 8: Baker IDI
Insulin initiation in type 2 diabetes
2 4 6 8
Hours after Injection
0.5
2.5
0
Hours after injection
2 4 6 8
Insu
lin A
ctio
n
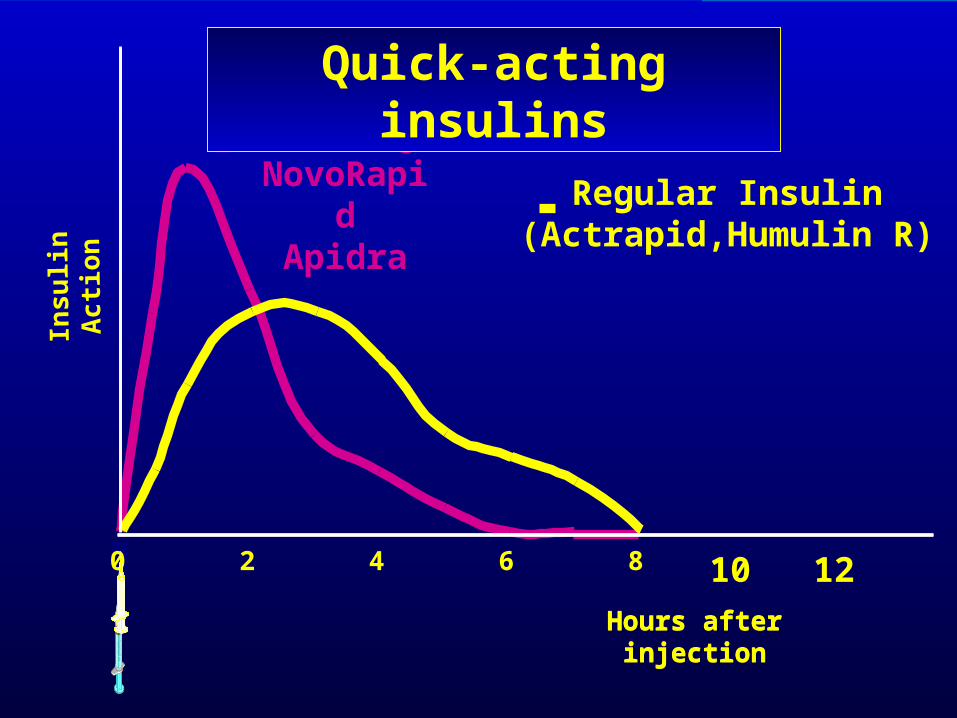
Regular Insulin(Actrapid,Humulin R)
HumalogNovoRapid
Apidra
0
Hours after injection
10 12
Quick-acting insulins
2 4 6 8
Hours after Injection
0.5
2.5B
lood
Insu
lin L
evel
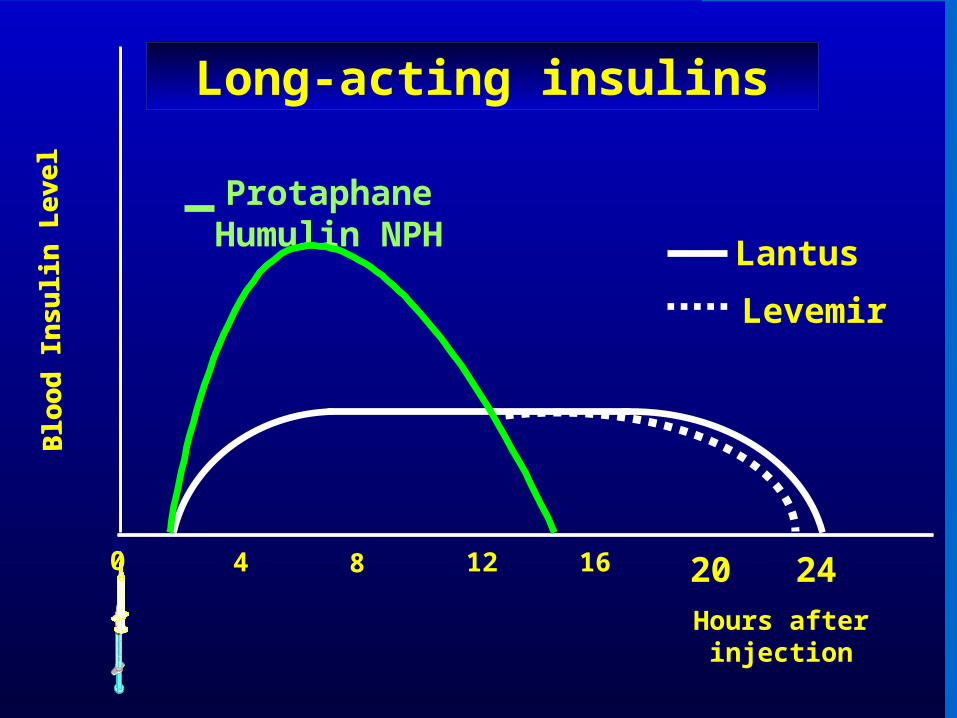
0 4 12 16
Hours after injection
8
Blo
od In
sulin
Lev
el
0 20 24
ProtaphaneHumulin NPH Lantus
Levemir
Long-acting insulins
Page 11: Baker IDI
Basal Premixed
Basal Bolus insulin
Sulphonylurea
Acarbose DPP-4 inhibitor # Glitazone* Insulin
Lifestyle Modification•diet modification•weight control•physical activity
Metformin
Management Algorithm for Blood Glucose Control in Type 2 Diabetes in Australia
• The algorithm includes only therapeutic agents available through the PBS.• If HbA1c >7% consider intensifying treatment provided hypoglycaemia is not a problem.# Authorised only as dual therapy with metformin or sulphonylurea where combination metformin and sulphonylurea
is contraindicated or not tolerated.* Rosiglitazone is not authorised for triple therapy or for use with insulin (from February 1, 2009) but is approved only as dual
therapy with metformin or sulphonylurea where combination metformin and sulphonylurea is contraindicated or not tolerated.
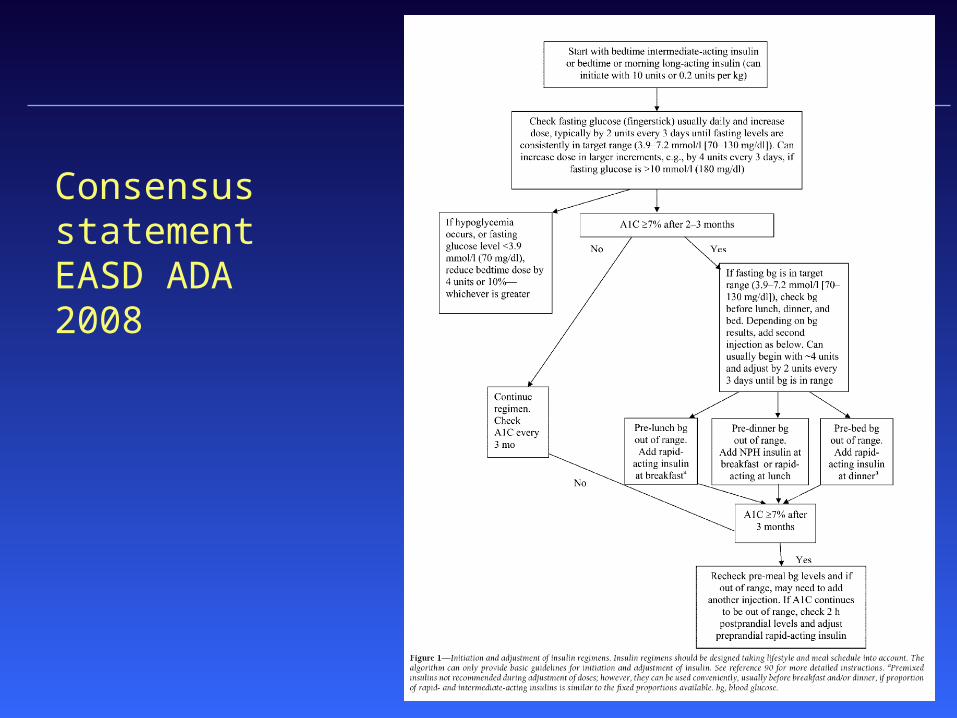
Consensus statement EASD ADA 2008
Page 13: Baker IDI
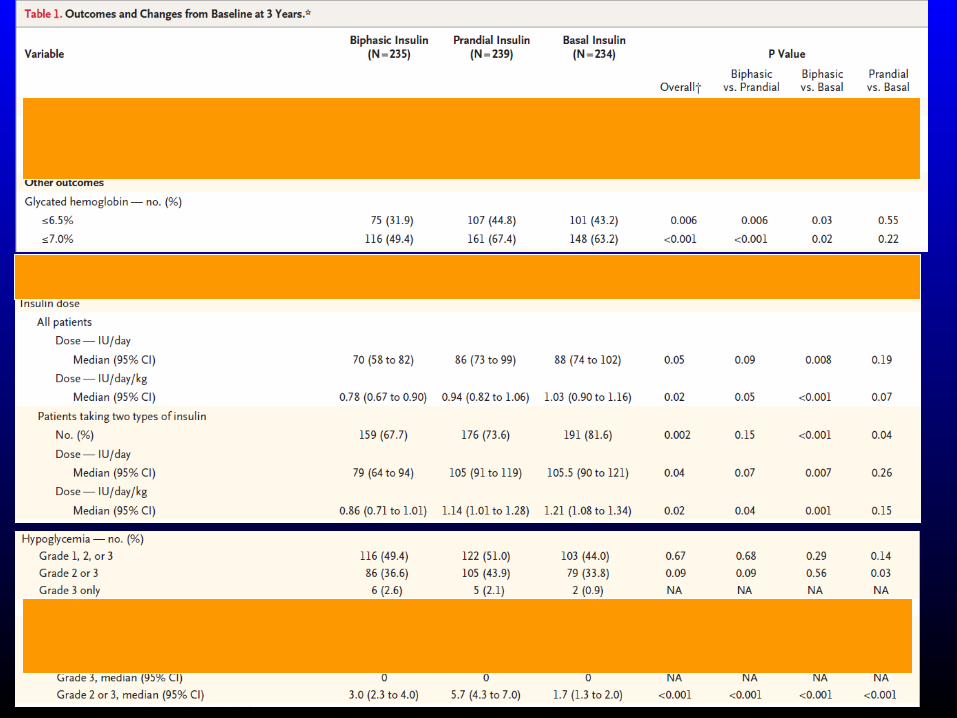
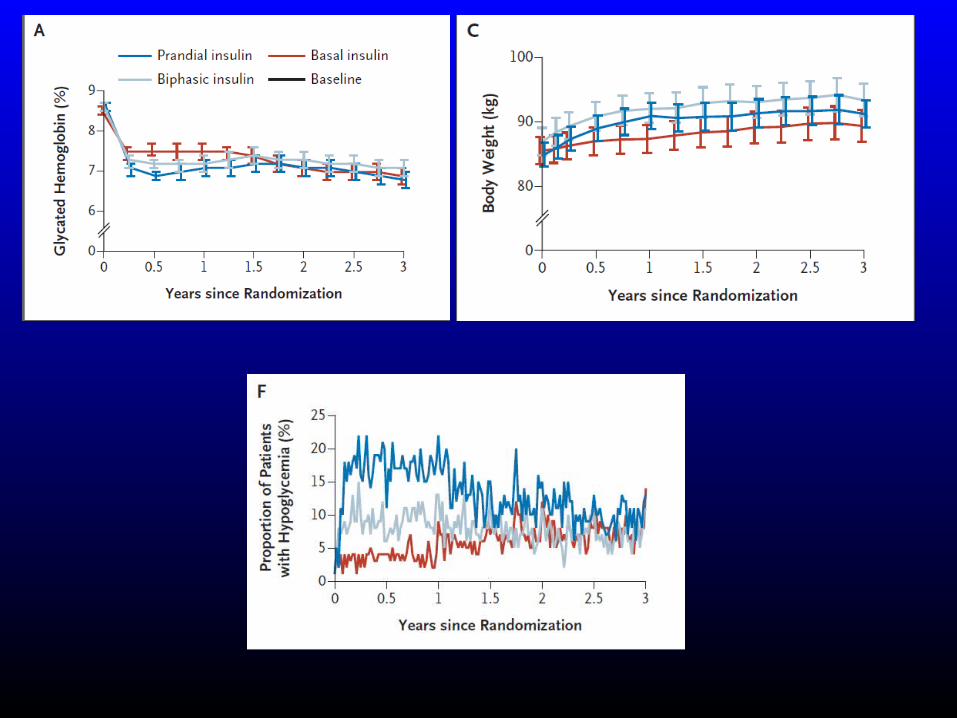
Insulin initiation trials
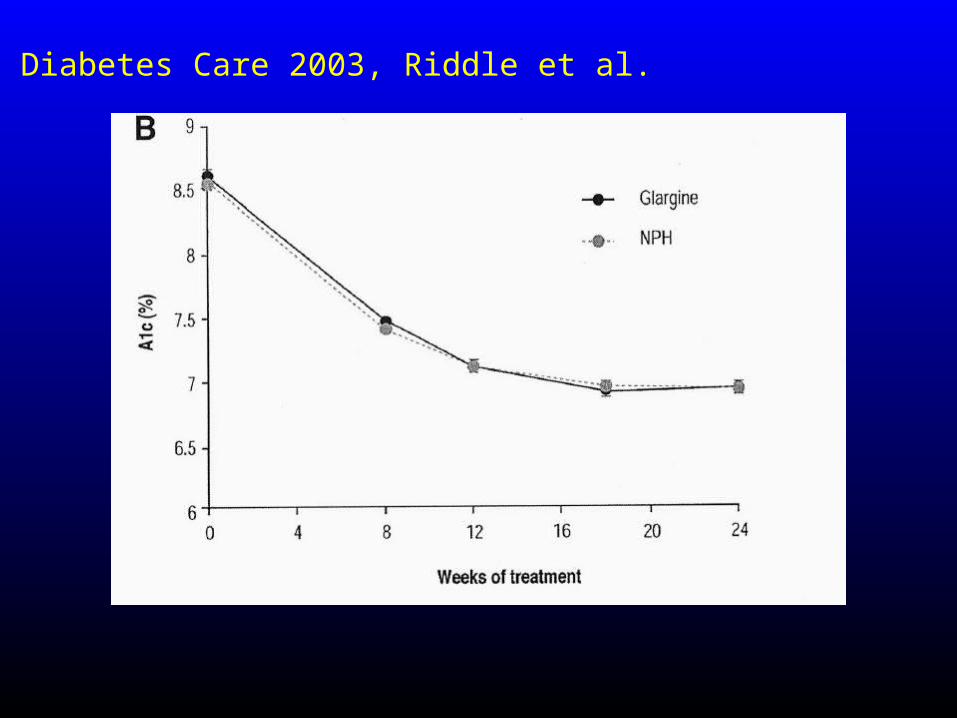
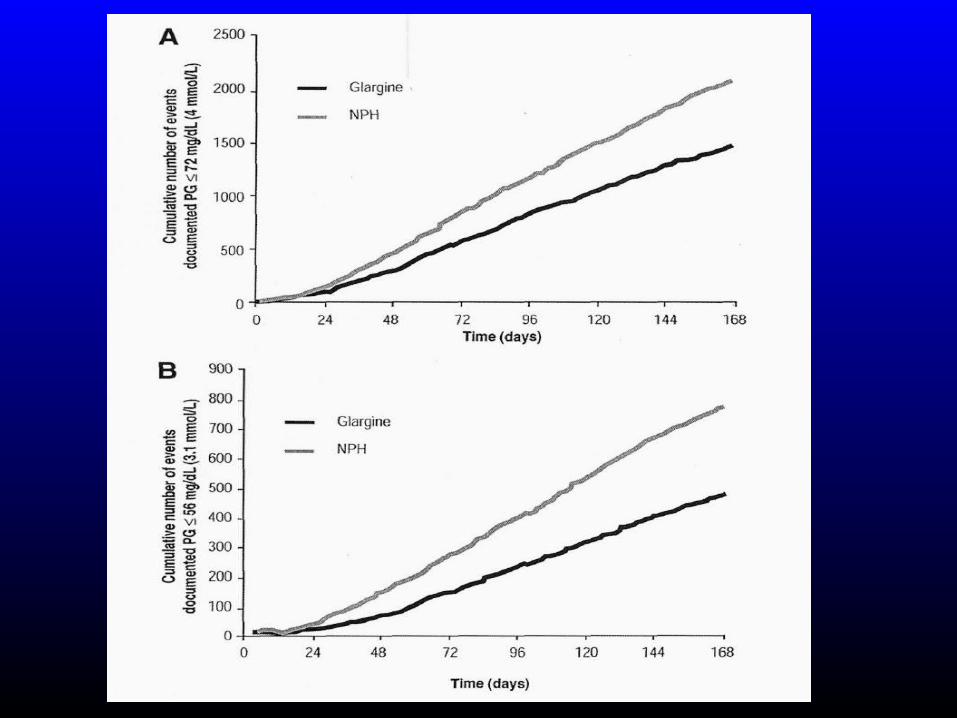
Diabetes Care 2003, Riddle et al.
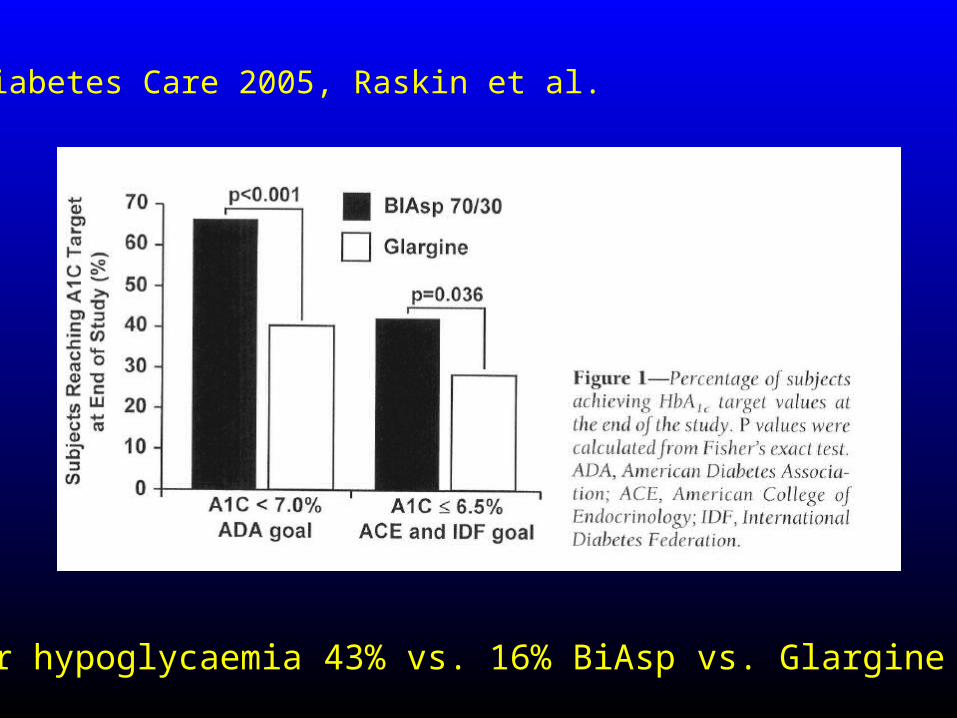
Minor hypoglycaemia 43% vs. 16% BiAsp vs. Glargine
Diabetes Care 2005, Raskin et al.
Page 21: Baker IDI
Why new treatments?
What’s wrong with the old treatments?
Page 22: Baker IDI
New treatments - why new treatments?
• Beta cell preservation– Prevent relentless progression of type 2 diabetes
• Hypoglycaemia ? harmful• CV morbidity and mortality
– ACCORD and other CV outcome trials– Glitazone controversies
• Weight loss as a priority – Recognized as a major factor in morbidity
Page 23: Baker IDI
Incretins
• GLP 1 analogues• Exenatide• Liraglutide• Once weekly GLP – 1 analogues
• DPP 4 inhibitors• Sitagliptin
Page 24: Baker IDI
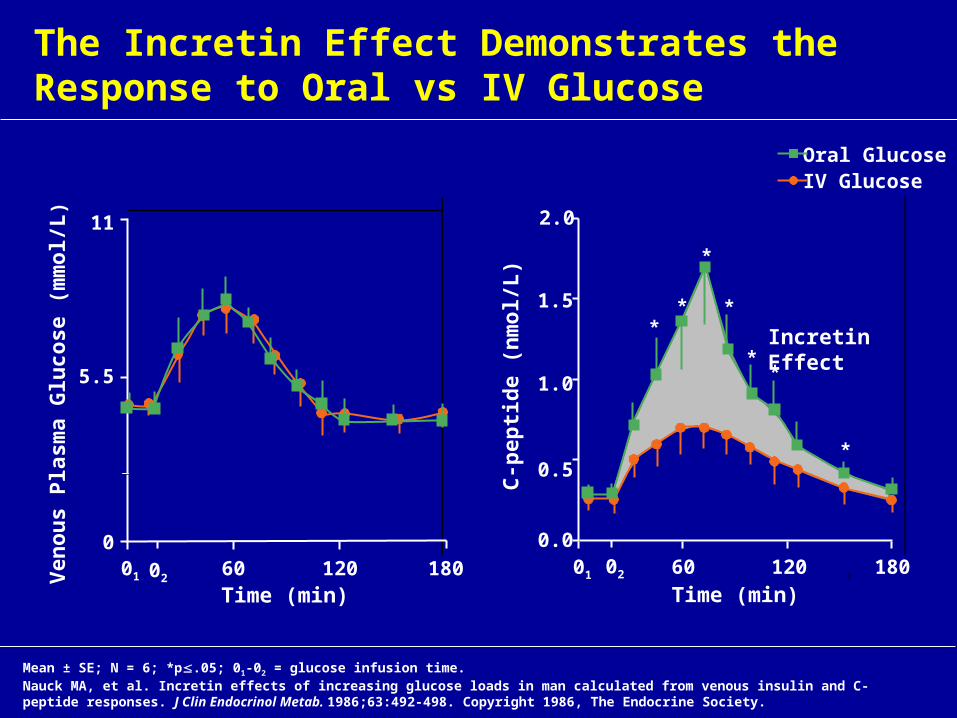
The Incretin Effect Demonstrates the Response to Oral vs IV Glucose
Mean ± SE; N = 6; *p.05; 01-02 = glucose infusion time.Nauck MA, et al. Incretin effects of increasing glucose loads in man calculated from venous insulin and C-peptide responses. J Clin Endocrinol Metab. 1986;63:492-498. Copyright 1986, The Endocrine Society.
Ven
ou
s P
lasm
a G
luco
se (
mm
ol/L
)
Time (min)
C-p
epti
de
(nm
ol/L
)
11
5.5
001 60 120 180 01 60 120 180
0.0
0.5
1.0
1.5
2.0
Time (min)02
02
Incretin Effect
Oral Glucose IV Glucose
**
*
*
**
*
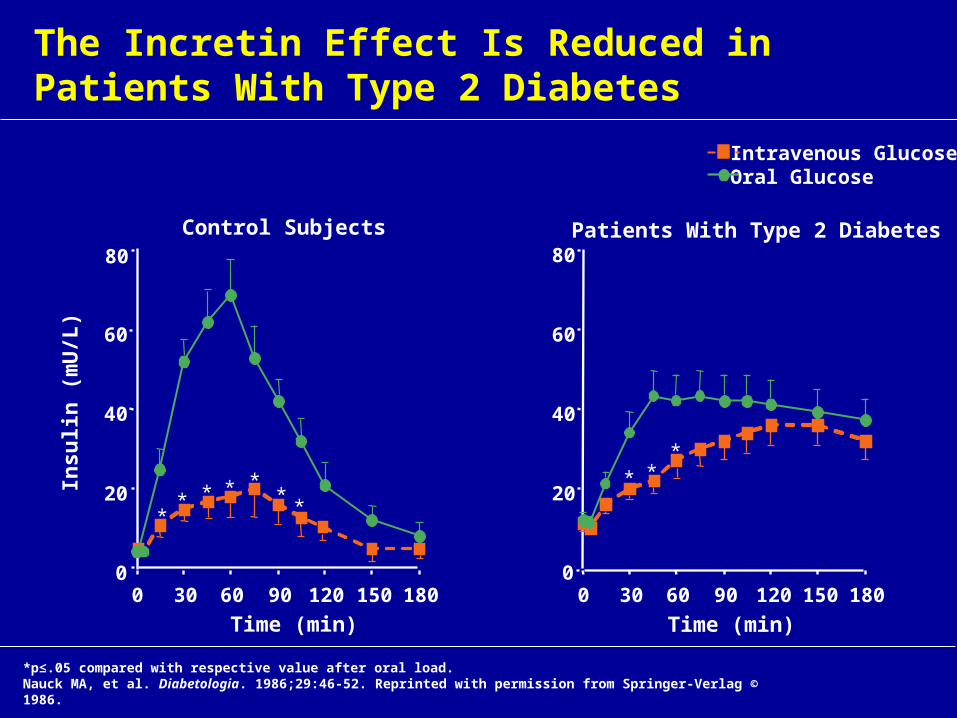
The Incretin Effect Is Reduced in Patients With Type 2 Diabetes
0
20
40
60
80
Insu
lin (
mU
/L)
0 30 60 90 120 150 180
Time (min)
** *
** **
0
20
40
60
80
0 30 60 90 120 150 180
Time (min)
**
*
*p≤.05 compared with respective value after oral load. Nauck MA, et al. Diabetologia. 1986;29:46-52. Reprinted with permission from Springer-Verlag © 1986.
Patients With Type 2 DiabetesControl Subjects
Intravenous GlucoseOral Glucose
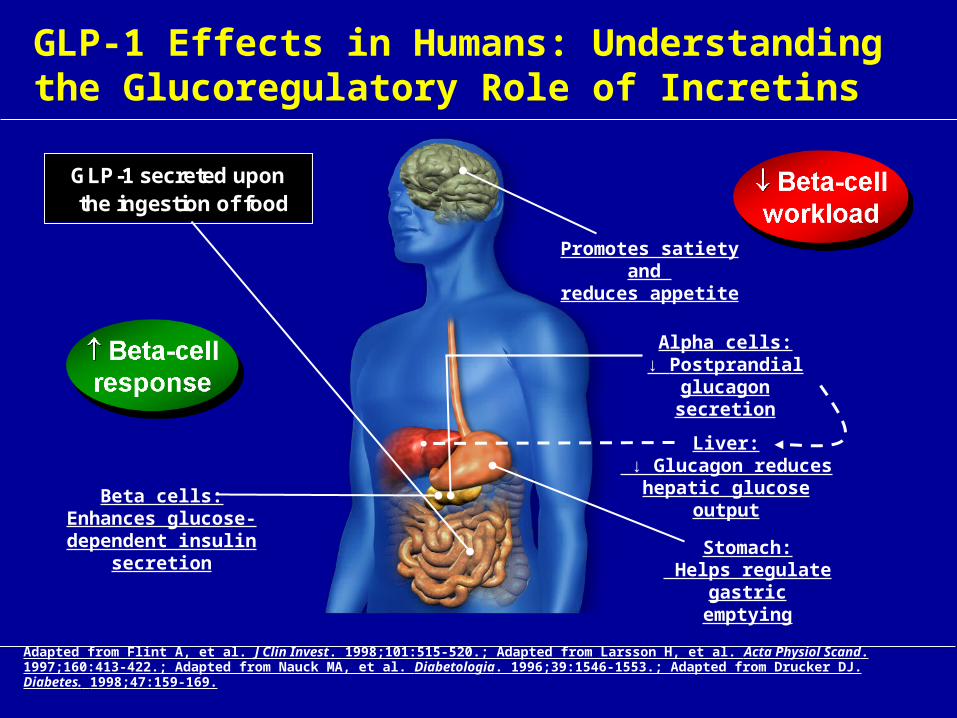
GLP-1 Effects in Humans: Understanding the Glucoregulatory Role of Incretins
Promotes satiety and reduces appetite
Beta cells:Enhances glucose-dependent insulin
secretion
Adapted from Flint A, et al. J Clin Invest. 1998;101:515-520.; Adapted from Larsson H, et al. Acta Physiol Scand. 1997;160:413-422.; Adapted from Nauck MA, et al. Diabetologia. 1996;39:1546-1553.; Adapted from Drucker DJ. Diabetes. 1998;47:159-169.
Liver: ↓ Glucagon reduces
hepatic glucose output
Alpha cells:↓ Postprandial
glucagon secretion
Stomach: Helps regulate
gastric emptying
GLP-1 secreted upon the ingestion of food
28
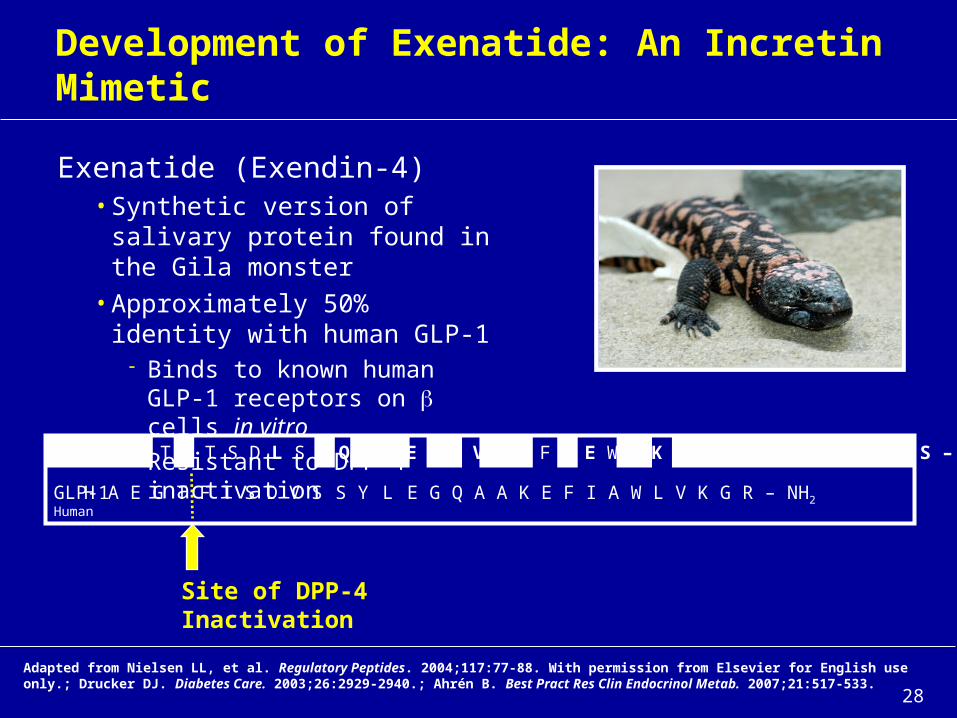
Exenatide (Exendin-4)• Synthetic version of salivary
protein found in the Gila monster• Approximately 50% identity with
human GLP-1 Binds to known human GLP-1
receptors on cells in vitro Resistant to DPP-4 inactivation
Development of Exenatide: An Incretin Mimetic
Adapted from Nielsen LL, et al. Regulatory Peptides. 2004;117:77-88. With permission from Elsevier for English use only.; Drucker DJ. Diabetes Care. 2003;26:2929-2940.; Ahrén B. Best Pract Res Clin Endocrinol Metab. 2007;21:517-533.
Site of DPP-4 Inactivation
H G E G T F T S D L S K Q M E E E A V R L F I E W L K N G G P S S G A P P P S – NH2
H A E G T F T S D V S S Y L E G Q A A K E F I A W L V K G R – NH2
Exenatide
GLP-1Human
Page 29: Baker IDI
Page 30: Baker IDI
Page 31: Baker IDI
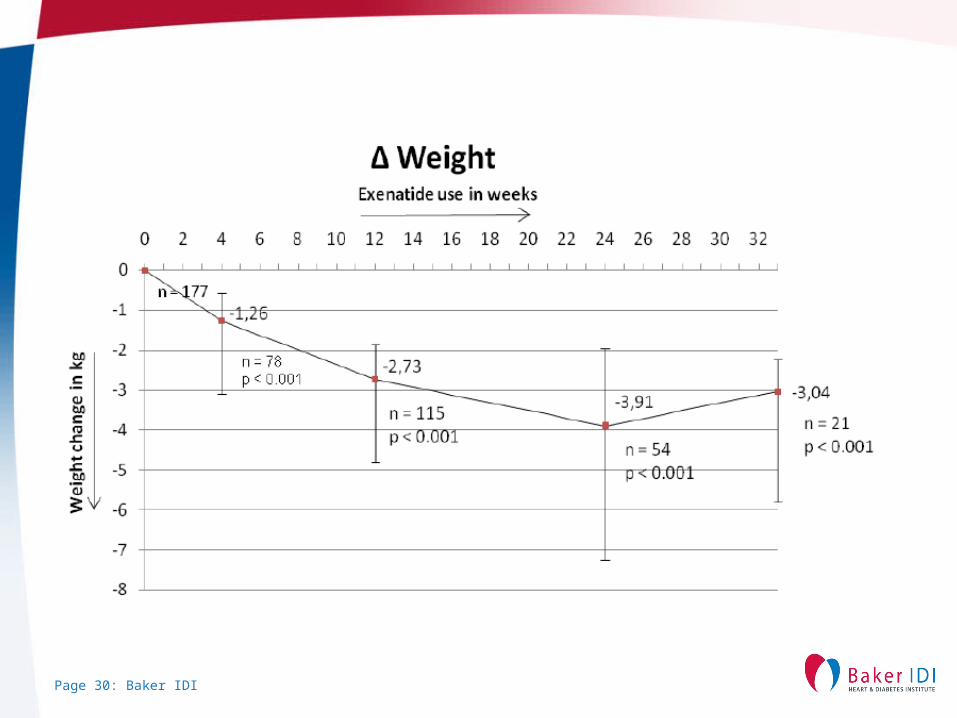
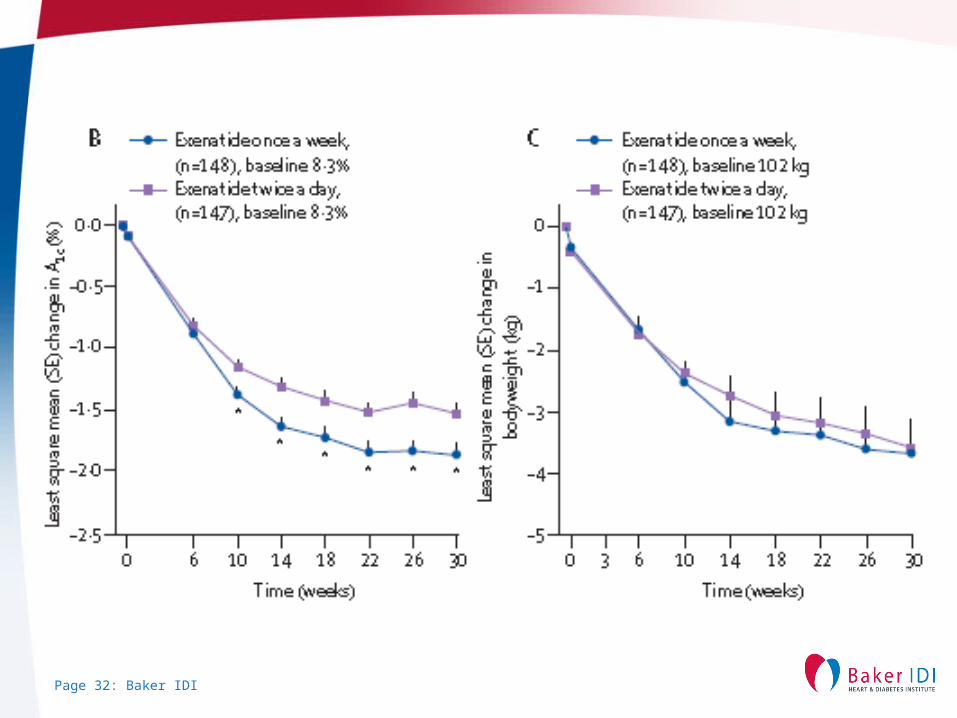
Exenatide once weekly
• Once weekly vs bd exenatide, 30 week study• Patients were drug naive or treated with 1 or more oral glucose-
lowering therapies (~15% diet/exercise, ~45% 1 OAD, ~40% 2 OADs).
• Starting HbA1c 8.3±1.0%• HbA1c decreased in both groups , 1.9%±0.08 vs 1.5%± 0.08
(P=0.002) in once weekly vs bd
• 22 week extension study LAR for all patients after first 30 weeks• At 52 weeks decrease HbA1c by 2.0% both groups, 4.1 kg wt loss ,
80% patients lost weight BP decreased 4-6 mmHg
Page 32: Baker IDI
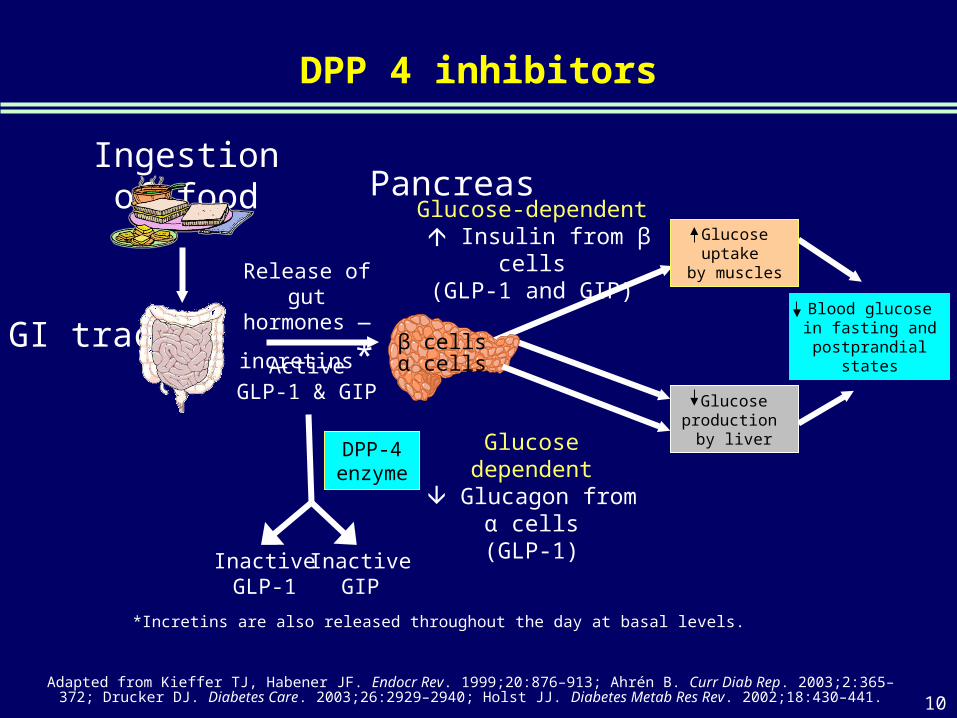
DPP 4 inhibitors
Adapted from Kieffer TJ, Habener JF. Endocr Rev. 1999;20:876–913; Ahrén B. Curr Diab Rep. 2003;2:365–372; Drucker DJ. Diabetes Care. 2003;26:2929–2940; Holst JJ. Diabetes Metab Res Rev. 2002;18:430–441.
Ingestion of food
β cellsα cells
Release of gut hormones —
incretins*
PancreasGlucose-dependent
Insulin from β cells(GLP-1 and GIP)
Glucose uptake by muscles
Glucose dependent Glucagon from
α cells(GLP-1)
GI tractActive
GLP-1 & GIP
DPP-4 enzyme
InactiveGIP
InactiveGLP-1
*Incretins are also released throughout the day at basal levels.
Glucose production
by liver
Blood glucose in fasting and postprandial states
10
Clinical experience with sitagliptin
• Effective for dual , triple therapy and with insulin
• Low side effect profile
• Weight neutral
• No hypoglycaemia in combination with metformin or
glitazone
• Safe and effective in older patients
Januvia -PBS restrictions in Australia
• Dual therapy for combination with metformin or a sulphonylurea agent
• HbA1c > 7.0% at initiation
• Treatment with metformin or sulphonylurea as a second agent is either contraindicated or not tolerated
• (private script $100 per month)
Page 36: Baker IDI
Other new agents
•SGLT 2 inhibitors•Glucokinase activators•Glucagon receptor antagonists





























