Embed Size (px)
Citation preview

European Journal of Internal Medicine xxx (2015) xxx–xxx
EJINME-02879; No of Pages 7
Contents lists available at ScienceDirect
European Journal of Internal Medicine
j ourna l homepage: www.e lsev ie r .com/ locate /e j im
Original Article
Health-related quality of life and multimorbidity in community-dwellingtelecare-assisted elders in the Basque Country
Edurne Alonso-Morán a,⁎, Roberto Nuño-Solinís a, Juan F. Orueta b, Begoña Fernandez-Ruanova c,Alfredo Alday-Jurado c, Enrique Gutiérrez-Fraile c
a O+berri, Basque Institute for Healthcare Innovation, Torre del BEC (Bilbao Exhibition Centre), Ronda de Azkue 1, 48902 Barakaldo, Spainb Osakidetza, Basque Health Service, Astrabudua Health Centre, Mezo 35, 48950 Erandio, Spainc Osatek S.A., Public Society of the Basque Government, Alameda de Urquijo 36, Edificio Plaza de Bizkaia, 48011 Bilbao, Spain
⁎ Corresponding author. Tel.: +34 650718526.E-mail address: [email protected] (E. Alonso-M
http://dx.doi.org/10.1016/j.ejim.2015.02.0130953-6205/© 2015 European Federation of Internal Medi
Please cite this article as: Alonso-Morán E, etin the Basque Country, Eur J Intern Med (20
a b s t r a c t
a r t i c l e i n f oAvailable online xxxx
Keywords:Chronic diseasesHealth-related quality of lifeMultimorbidityTelecare
Introduction: Multimorbidity is more common in the elderly population and negatively affects health-relatedquality of life (QoL). The aims of the study were to report the QoL of users of the Basque telecare public service(BTPS) and to establish its relationship with multimorbidity.Methods: The EuroQol questionnaire was administered to 1125 users of the service. Their sociodemographic andhealthcare characteristics were obtained from BTPS databases and the Basque healthcare service. Multipleregression analysis was performed on the overall questionnaire index to determine the effect of chronic diseases
and sociodemographic. Moreover, the effects of the different diseases on specific dimensions of the test wereexplored by logistic regression.Results: Of the users interviewed, 82% were women, 88%≥75 years and 66% lived alone. The average of chronicpathologies was higher among men (5.3 vs. 4.6), for the lower age range and among those not living alone(P b 0.001). For QoL, men and people aged over 84 obtained better scores (0.64 and 0.61, respectively). WorseQoL was associated with being a woman, multimorbidity, and living with one or more people. The existence ofmultimorbidity meant impaired QoL of 2.6 points for each additional disease over the overall score (P b 0.001).Conclusions: This study reveals that for the population covered by BTPS the impact of chronic pathologies,multimorbidity and their social context affects QoL very diversely. These diverse social and healthcare needs ofcommunity-dwelling elders allow the development and implementation of personalised services, such astelecare that facilitate them to remain at home.© 2015 European Federation of Internal Medicine. Published by Elsevier B.V. All rights reserved.
1. Introduction
As themain causes ofmorbidity andmortality in elderly societies arechronic diseases, there is a growing interest in cost-effective ways ofcaring for this population. Moreover, multimorbidity is turning into anincreasingly more common reality and is especially frequent in somegroups such as women, elderly people and those bearing moreunfavourable socio-economic conditions [1–3].
Some consequences of morbidity are already known: they are asso-ciated with worse healthcare outcomes in people, a high degree ofdisability, functional impairment and worse quality of life [2,4,5]. Inaddition, it has been broadly demonstrated that multimorbidity has anegative impact on healthcare-related quality of life (HRQoL) [2,6].However, understanding the effects of multimorbidity in detail is notan easy task. Individual chronic conditions may vary in regard to theirimpact on patients' daily quality of life and their function [7,8].
orán).
cine. Published by Elsevier B.V. All rig
al, Health-related quality of li15), http://dx.doi.org/10.1016
HRQoL offers a multidimensional perspective ranging from patients'physical, emotional and social function [9]. In general, patients withmore than one comorbid condition report a poorer score HRQoL [10],but some chronic diseases are more significantly associated with aworse HRQoL score than others. The severity of individual chronic con-ditions is also a factor that has an impact on this quality [10].
Moreover, it has a significant financial impact; therefore, for exam-ple 64% of the annual healthcare budget in the Basque Country isearmarked for caring for people with multimorbidity; this represents24% of the total population [11]. These figures are compatible to thosepublished by the public insurance system Medicare for those agedover 65 in the USA [12].
Being familiar with the sociodemographic and healthcare character-istics, in addition to their impact on quality of life variables is useful toprovide personalised care, especially when technology is involved.
The telecare service is increasingly popular for the provision ofservices to elderly populations in the OECD. In the Basque Country, theBasque government telecare public service (hereinafter BTPS) providesdomiciliary care to dependent and other populations and is connected
hts reserved.
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013

2 E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
in a coordinated manner with healthcare devices which enables thedevelopment of integrated social and healthcare provision models.One of the main aims of BTPS is to encourage users to remain in theirusual social setting.
The main aim of this study was to analyse the influence of demo-graphics', chronic healthcare problems, social characteristics andmultimorbidity on quality of life, recorded by means of the EuroQolquestionnaire, for users of a telecare service. The second aim was todetermine the relative impact of a predetermined number of “chronicconditions” on the specific dimensions of HRQoL in the same group.
2. Materials and methods
2.1. Ethics committee
The study protocol was approved by Euskadi Clinical Research EthicsCommittee (PI2014106). The teleoperators of BTPS's own servicerequested the user's informed consent prior to administration of thequestionnaire.
2.2. Study population: sample and procedures
In the Basque Country, the inhabitants over 65 years in 2012 were452,698 (20.0% of the total population) and 145,780 (8.2%) over80 years [13]. At 1 September 2012, the Basque government telecarepublic service responding to requests from 25,757 individual users(79.55% women).
The BTPS is the result of cooperation between the Department ofHealth and Department of Social Services. This service is part of a com-prehensive care model focused on the person, whose fundamentalaspect is to address the social and health needs of people in a coordinat-ed manner, both in preventive and in care aspect. Its connection withhealth care devices allows having information of systems which sharedata on health and social issues. This makes possible a characterizationof the target population and the development of integrated health andsocial care provision models. The socio-health coordination has beenturned into the adoption of various measures and it addresses objec-tives and actions for active ageing, coordination of socio-health space,adequate health care for the elderly, promotion of autonomy andrespect for personal wills, the new technologies for quality of life, wel-fare, promotion of volunteering, and personal and intergenerationalrelationships.
The inclusion criterion in BTPS is one of the following characteristics:a) persons aged over 75 who live alone, b) persons older than 65 whoare in a situation of recognised dependence or vulnerability recognisedby social services, c) persons with intellectual, physical or sensorialdisability and any degree of recognised dependence and d) personswho suffer from diagnosed mental disease and present a situation ofrecognised dependence or risk of social exclusion.
A representative sample of all BTPS users was selected by means ofstratified random sampling by historic areas, by applying the formulaalready reported by other authors [14]. A 95% confidence interval wasselected, that is z= 1.96, an error of 3%was considered and equal prob-abilities of p and q and equal to 0.5 were selected. A sample of 1125users of the services was subsequently estimated.
The study period was from 1 September 2012 to 31 August 2013. Atotal of 1554 interviews were performed, 14.7% of these intervieweesopted not to take part in the study and 8.6% of the interviews couldnot be fully completed, whereby they were excluded from the sample.Of the 1192 full interviews, 94.4% could be linked to healthcare data,whereby the final sample was 1125 users.
2.3. Sources of information
For this study, there was a combination of information in regard tosocial variables such as marital status and cohabitation unit, from the
Please cite this article as: Alonso-Morán E, et al, Health-related quality of liin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016
BTPS database, demographic variables and clinical variables from theelectronic clinical history and other computerised sources from theBasque Health Department (Osakidetza).
To detect the existence of chronic diseases, diagnosis and pres-cription data were reviewed during the last 6 years for each one of thepeople included and a methodology similar to that reported by otherauthors was adopted [15]. A list of 52 diseases was defined; specificcriteria for each one of them were agreed to be considered as active.For this study multimorbidity was considered as the coexistence oftwo or more diseases in the same person.
To obtain measurements on healthcare-related quality of life, theEuroQol 5D-3L telephone questionnaire was used. This is a multidimen-sional, self-administered scale with a total score in regard to the qualityof life perceived by the patient. It hasfive dimensions to evaluate qualityof life (mobility, self-care, usual activities, pain/discomfort and anxiety/depression) each with three possible answers (no problems, moderateproblems and severe problemswith the dimension at issue). The overallindex values are between 0 and 1 where 1 is the best health conditionpossible and 0 is the worst health condition possible.
2.4. Analysis
To analyse the effects of multimorbidity and individual conditionson HRQoL in general and on specific dimensions, multiple regressionof ordinary least squares (OLS) and multiple logistic regression wereused. All models were adjusted for demographic variables, taking malesex and youngest age range as a reference; the overall index was scaled(dependent variable) by 100.
For the first model, OLS regression was used to estimate the effect ofmultimorbidity, measured as the sum of chronic diseases, on the overallEuroQol index. In the secondmodel, OLS was used to estimate the effectof the different chronic pathologies on the overall index. Moreover, sev-eral logistic regression models were estimated to explore the effects ofthe individual condition in the five specific dimensions of the question-naire using dichotomous variables (0 for those who answered no prob-lems and 1 for those who answered moderate or severe problems) foreach dimension as a dependent variable. For the second OLS regressionmodel and logistics models they included those chronic pathologieswhose prevalence was greater than 1%.
Statistical calculations were performed using Stata, Data Analysisand Statistical Software, Release 12 (StataCorp, LP, College Station, TX,USA).
3. Results
3.1. Demographic, healthcare and social characteristics of thesurvey respondents
The survey sample was comprised of 82.13% women, 87.82%users aged over 74; almost half of the users were widows and66.22% lived alone. Both for men and women 92% of the users weremultimorbid. The average number of chronic pathologies was higherin men, for the lower age range (64–74) and for those who lived withat least one person. The total averagewas 4.7 chronic pathologies perperson (Table 1). It was verified by means of the ANOVA test that thedifferences in the average of chronic pathologies between sexes, ageranges, cohabitation unit and marital status were all statistically sig-nificant (P b 0.001).
The most prevalent chronic diseases for both sexes were hyperten-sion, anxiety, dyspepsia anddiabetes.Men added prostatic hypertrophy,atrial fibrillation, chronic obstructive pulmonary disease, cancer, strokeand ischaemic heart disease asmost prevalent; andwomen addedmus-culoskeletal degeneration, depression and osteoporosis (additional ma-terial A).
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013

Table 1Demographic features and average of chronic pathologies of BTPS users included in thestudy by sex, age ranges, cohabitation unit and marital status.
Characteristics N (%) Average ofchronicpathologies(SD)
Differences betweengroups: F-statistics(P value)
SexMales 201 (17.87) 5.32 (2.81) 13.4 (0.0003)Women 924 (82.13) 4.59 (2.53)
Age ranges65–74 137 (12.18) 5.10 (2.73) 4.70 (0.0029)75–79 304 (27.02) 4.92 (2.69)80–84 401 (35.64) 4.76 (2.49)85 or more 283 (25.16) 4.26 (2.51)
Cohabitation unitLives alone 745 (66.22) 4.43 (2.37) 6.75 (b0.0001)Lives with 1 person 319 (28.36) 5.13 (2.76)Lives with 2 people 38 (3.38) 6.16 (3.58)Lives with 3 or morepeople
23 (2.04) 6.00 (3.33)
Marital status. 363 (32.27) 5.58 (0.0002)Married 184 (16.36) 5.34 (2.90)Separated or divorced 15 (1.33) 4.67 (3.09)Single 44 (3.91) 3.80 (2.74)Widow 519 (46.13) 4.46 (2.31)Total average (SD) 1125 (100) 4.72 (2.59)
N represents the size of the subgroup, % the percentage represented by each subgroup ofthe sample, SD the standard deviation and "." no data available.
3E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
3.2. Results of the health-related quality of life survey (EQ-5D)
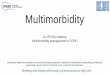
A total of 72% of users surveyed considered that they did not haveproblems for their self-care even when 61% had mobility problemsand 56% had their physical activity conditioned (13% severely). Pain ordiscomfort was present in 69% of cases; 19% with severe cases (seeFig. 1).
Stratified by age ranges and sex (Table 2) it was observed that menobtained better scores on health-related quality of life than women andelderly people. Observing by dimension, age had a special emphasis onmobility, self-care and activities of daily living (which is where higherscores were obtained). However, the eldest persons presented lesspain and discomfort and less anxiety and depression than youngerage groups. Men reported worse mobility and self-care values thanwomen. Consequently, women reported worse values for activities ofdaily living, pain or discomfort and anxiety or depression.
Bymeans of the ANOVA test statistically significant differences wereverified for the different dimensions of the EuroQol between sexes forpain/discomfort (P b 0.001) and between sexes and age range for anxi-ety/depression (both P b 0.001). Moreover, statistically significant dif-ferences were obtained between sexes for the overall questionnairescore (P b 0.01).
3.3. Effects of multimorbidity and chronic pathologies on the overallquestionnaire index
Table 3 reveals the association between quality-of-life andmultimorbidity. It was observed that female sex accounted for morenegative scores thanmen, 9.3 points less on the scale. The sumof chron-ic pathologies as a continuous variable had the effect of subtracting 2.57from the scale for each chronic disease suffered by the individual, that is,if an individual presented six chronic pathologies they would have atleast 15.6 points less on the total scale of 100 points. Age did not comeout significantly for the model. Cohabitation unit negatively affectedthe scale, the more members in the family unit the worse the valuesobtained.
Please cite this article as: Alonso-Morán E, et al, Health-related quality of liin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016
The prior analyseswere repeated by switching the number of chron-ic conditions for chronic diseases in themselves (Table 4). Sex was sig-nificant in the model; women reported worse results, up to 6 pointsless out of 100. Age groups were not statistically significant in themodel. The chronic diseases for which worse health-related quality oflow scores (statistically significant) were reported were: Parkinson'sdisease, muscular dystrophy or paralysis, peripheral vascular disease,and hepatopancreatic chronic diseases. Moreover, heart failure, ischae-mic heart disease, rheumatoid arthritis and others, musculoskeletaldegeneration, depression, dyspepsia and lumbago presented betweenfive and 10 points less than the overall index.
3.4. Effects of the chronic pathologies on each one of theEuroQol dimensions
Table 5 only presents those variables that were statistically signifi-cant in the model although the full table (B) is presented as additionalmaterial. In regard to themobility dimension, the risk of havingmoder-ate or severe problems was greater in people with Parkinson's diseaseor muscular dystrophy or paralysis, just as for the self-care dimension.For activities of daily living, the same pattern was repeated and periph-eral vascular disease was also added. In regard to pain, those who hadperipheral vascular disease presented a higher risk of moderate orsevere problems. Anxiety and depression are related to this dimension.
4. Discussion
The public telecare in the Basque Country serves an elderly agegroup that resides in their home and which is predominantly women.This study reveals that in this population there is a high prevalence ofchronic diseases and multimorbidity that has a negative impact ontheir HRQoL. Orueta et al. [16] revealed that this prevalence ofmultimorbidity is higher than the remaining Basque Country citizensof their same sex and age.
In our study, the prevalence of multimorbidity was 92% and theaverage for chronic pathologies was higher among men, in the lowerage ranges (65–74) and for those who lived with at least one person.Because of the method used to capture BTPS users, an increase in mor-bidity in regard to ageing was not observed.
In relation to answers given by BTPS users, although these revealedless problems for the self-care dimension, moderate or severe problemswere observed in regard to pain and/or discomfort, just as for the studyperformed by Brettschneider et al. [17].
Other authors that have used the EuroQol have also found thatmultimorbidity is negatively associated with HRQoL [17–21]. At thesame timewomen presented lower levels for quality of life which is con-sistent with other studies performed [20,22]. Similarly, people who donot live alone presented worse quality of life which may suggest thatthe existence of family carers enables keeping people with health prob-lems that significantly affect HRQoL in non-institutionalised settings.
The highest quality of life was among the oldest users, which op-poses most of the results from other studies where quality-of-life re-duces with age [17,20,23]. However, this result is in accordance withthe characteristics of the population which benefits from the telecareservice in the Basque Country, in which younger groups are peoplewith disability and related problems [15].
Parkinson's disease,muscular dystrophy or paralysis, peripheral vas-cular disease, hepato-pancreatic chronic diseases, heart failure, rheuma-toid arthritis and depression, in this order, were the chronic diseaseswhich most negatively affected quality of life. Other authors found anegative association between quality of life and Parkinson's disease[17,20], in addition to depression and arthritis [22]. However, moreeye-catching is the fact that pathologies such as stroke, malignant neo-plasia, schizophrenia and dementia are not statistically significant. Thismay be because in some of these pathologies the most serious casesare institutionalised and the cognitive impairment hinders giving an
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013

441, 39%
676, 60%
8, 1%MOBILITY
811, 72%
253, 23%
61, 5%
SELF-CARE
495, 44%484,
43%
146, 13%
USUAL ACTIVITIES
352, 31%
556, 50%
217, 19%
PAIN/DISCOMFORT
653, 58%
376, 33%
96, 9%
ANXIETY/DEPRESSIONNo problems
Moderate problems
Severe problems
Fig. 1. Distribution of user responses by dimension (number and percentage).
4 E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
answer to the questionnaire at issue. The results obtained for stroke andmalignant neoplasia differ from those of Hunger et al. [23] in which adeteriorated quality of life in these patients was revealed.
Comparing the results of a study on the association of chronicpathologies with each one of the specific dimensions of the EuroQolwith those of the study by Brettschneider et al. [17], it was observedthat they obtained similar odds ratios for the dimensions self-care andactivities of daily living for Parkinson's disease; and for the dimensionsmobility and activities of daily living for heart failure.
One of the strengths of this study compared with others on HRQoLlies in the fact that a list of 52 chronic pathologies was used whilst
Please cite this article as: Alonso-Morán E, et al, Health-related quality of liin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016
other authors considered a lower number: from 6 [23] to 42 [17] con-ditions. Conversely, the sources of information used connect social ser-vices and healthcare databases. This is because telecare in the BasqueCountry is a pioneering example of an integrated socio-healthcare ser-vice platform and has enabled having a wealth of information available.Subsequently, the coordination of these two services and telecare as aservice platform offers substantial opportunities for innovationin interventions on this BTPS user population. In addition, we haveanalysed a database containing information regarding primary, special-ized and ambulatory hospital care, as well as prescriptions. This is rele-vant given that other authors have established that the use of a single
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013

Table 2Average EuroQol scores by dimension and by overall index of the study population stratified by sexes and age ranges.
Mean (SD) by EuroQol dimensions
Characteristics Mobility Self-care Daily activities Pain/discomfort Anxiety/depression Overall index
SexMale 1.64 (0.51) 1.36 (0.61) 1.67 (0.69) 1.64 (0.68) 1.32 (0.53) 0.64 (0.25)Female 1.61 (0.50) 1.33 (0.57) 1.69 (0.69) 1.93 (0.70) 1.54 (0.67) 0.59 (0.25)
Age ranges65–74 1.61 (0.49) 1.33 (0.57) 1.67 (0.64) 1.97 (0.72) 1.67 (0.70) 0.57 (0.25)75–79 1.58 (0.51) 1.31 (0.55) 1.64 (0.67) 1.93 (0.68) 1.58 (0.67) 0.60 (0.25)80–84 1.62 (0.49) 1.33 (0.58) 1.69 (0.70) 1.86 (0.72) 1.46 (0.64) 0.60 (0.25)85 or more 1.65 (0.51) 1.36 (0.61) 1.75 (0.71) 1.81 (0.68) 1.42 (0.60) 0.61 (0.25)Total average (SD) 1.62 (0.50) 1.33 (0.58) 1.69 (0.69) 1.88 (0.70) 1.50 (0.65) 0.60 (0.25)
Table 4Linear regression on the overall index scaled by 100 adjusting by sex, age groups andchronic diseases with a prevalence higher than 1%.
Overall index Betacoefficient
Standarderror
[95% confidenceinterval]
SexMan (ref)Woman −6.15 2.33 −10.73 −1.57
Age ranges65–74 (ref)74–79 2.85 2.50 −2.05 7.7680–84 2.35 2.42 −2.39 7.09Over 84 0.54 2.55 −4.46 5.54
Chronic pathologiesParkinson's disease −13.42 3.17 −19.65 −7.19
5E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
sourcemay produce inaccurate results [24,25]whilst the complementa-ry use of various different sources helps to improve the description ofpeople's health problems [26].
The study has some limitations. First, the administrative databasesonly contain treated morbidity records, whereby information is exclud-ed on diseases and problems for which patients did not request care;this is a common situation for some chronic diseases. Second, we hadto consider them limitations inherent to questionnaires administeredby telephone to an elderly age group; it may be the case that peoplewith cognitive problems have answered the tests although the trainingof interviewers substantially limits this possibility.
Finally, although the purpose of the study is not an evaluation of thetelecare service, it is important to stress that authors such as Hirani et al.[27] have revealed that the telecare service potentially contributes tothe improvement in the reduction of HRQoL for users of a service ofthis nature.
Muscular dystrophy or paralysis −11.10 4.49 −19.91 −2.3Peripheral vascular disease −10.54 5.36 −21.06 −0.02Hepatopancreatic chronic diseases −10.11 5.00 −19.92 −0.30Heart failure −9.10 2.68 −14.36 −3.84Rheumatoid arthritis and others −8.90 3.18 −15.14 −2.66Depression −7.01 1.73 −10.4 −3.61Immunological diseases −6.84 5.76 −18.15 4.47Musculoskeletal degeneration −6.34 1.58 −9.43 −3.24Ischaemic heart disease −6.23 2.56 −11.25 −1.21Lower back pain −6.10 2.50 −11.02 −1.19Dyspepsia −5.39 1.62 −8.57 −2.21Stroke −4.14 2.11 −8.29 0.01Inflammatory bowel disease −4.02 6.78 −17.33 9.30
5. Conclusions
This study reveals that for a specific population covered by BTPS, theimpact of chronic pathologies andmultimorbidity is high. Although theresults of this study cannot be generalised due to specific characteristicsof the population covered, it provides several useful hints. Therefore, weconsider that to ascertain the sociodemographic, healthcare and qualityof life features of aged populations covered by telecare services is usefulto develop and implement personalised services and interventions.
Table 3Linear regression on the overall index scaled by 100 adjusting by sex, age groups, sum ofchronic diseases and cohabitation unit.
Characteristics Beta coefficient Standard error [95% confidenceinterval]
SexMan (ref)Woman −9.29 1.87 −12.96 −5.62Total of chronic pathologies −2.57 0.28 −3.12 −2.03
Age ranges65–74 (ref)74–79 3.60 2.43 −1.17 8.3780–84 3.32 2.34 −1.27 7.90Over 84 2.65 2.47 −2.20 7.49
Cohabitation unitLives alone (ref)Lives with 1 person −11.16 1.61 −14.31 −8.01Lives with 2 people −13.88 3.97 −21.67 −6.09Lives at least with 3 people −1.71 5.02 −11.56 8.15Intersection 80.45 2.94 74.67 86.22
Ref— reference group in the regression analysis.
Irritable bowel syndrome −3.82 6.07 −15.73 8.10Chronic heart failure, others −3.36 2.38 −8.03 1.30Anxiety −3.03 1.51 −6.00 −0.06Diverticulosis −2.45 2.66 −7.66 2.77Psoriasis or eczema −2.24 6.10 −14.21 9.74Deafness −1.82 2.56 −6.83 3.20Peripheral neuropathy −1.45 2.81 −6.97 4.07Chronic sight disorders −1.32 2.83 −6.88 4.24Prostatic hypertrophy −1.12 3.65 −8.29 6.05Emphysema, chronic bronchitis, COPD −0.97 2.56 −6.00 4.06Osteoporosis −0.94 1.90 −4.66 2.78Diabetes −0.88 1.71 −4.23 2.48Malignant neoplasia −0.81 2.33 −5.39 3.76Hypertension −0.43 1.87 −4.10 3.24Glaucoma −0.30 1.95 −4.12 3.53Chronic renal failure 0.03 2.57 −5.01 5.07Gout 0.51 4.00 −7.33 8.36Asthma (treated currently) 0.83 3.30 −5.64 7.30Hypothyroidism 1.77 2.27 −2.68 6.21Schizophrenia 1.88 6.21 −10.31 14.07Metabolism errors andchromosomopathies
2.14 5.40 −8.46 12.74
Atrial fibrillation 3.95 2.10 −0.17 8.08Dementia 5.36 2.64 0.18 10.53Chronic hematological diseases 8.92 7.08 −4.98 22.82Intersection 75.18 3.26 68.77 81.59
COPD — chronic obstructive pulmonary disease; ref — reference group in the regressionanalysis.
Please cite this article as: Alonso-Morán E, et al, Health-related quality of life andmultimorbidity in community-dwelling telecare-assisted eldersin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016/j.ejim.2015.02.013

Table 5Logistic regression on the overall index scaled by 100 adjusting by sex, age groups and chronic diseases with a prevalence higher than 1%. Only those statistically significant variables arerepresented (P b 0.05).
Mobility Self-care Activities of daily living Pain/discomfort Anxiety/depression
Characteristics OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI) OR (95% CI)
SexMan (ref)Woman 2.68 1.75 4.11 1.69 1.09 2.61
Age ranges65–74 (ref)80–84 0.53 0.34 0.82Over 84 0.52 0.33 0.83
Chronic pathologiesStroke 1.49 1.00 2.23Rheumatoid arthritis and others 1.90 1.07 3.38 2.36 1.14 4.87Anxiety 1.39 1.04 1.87 1.54 1.18 2.01Ischaemic heart disease 2.22 1.30 3.80Musculoskeletal degeneration 1.88 1.40 2.52 1.65 1.23 2.23 1.84 1.34 2.53Dementia 0.51 0.31 0.82 0.45 0.28 0.74Depression 1.67 1.20 2.31 1.75 1.28 2.39 2.77 2.03 3.76Dyspepsia 1.47 1.09 1.99 1.60 1.16 2.22Muscular dystrophy or paralysis 5.62 1.61 19.60 3.45 1.53 7.81 5.34 1.77 16.11Chronic heart failure, others 1.56 1.01 2.43Hepatopancreatic chronic diseases 2.47 1.02 5.98Peripheral vascular disease 3.33 1.05 10.63 5.53 1.42 21.62Heart failure 2.28 1.31 3.96 1.78 1.07 2.96 1.90 1.07 3.38Lower back pain 1.84 1.12 3.03 1.92 1.09 3.36Peripheral neuropathy 2.24 1.25 4.00 0.45 0.26 0.77Parkinson's disease 4.22 1.99 8.97 4.56 2.58 8.08 3.84 1.93 7.67 1.28 0.68 2.44 1.13 0.64 1.98Intersection 0.49 0.27 0.89 0.12 0.06 0.24 0.44 0.24 0.79 0.67 0.36 1.24 0.53 0.29 0.97
CI— confidence interval; COPD — chronic obstructive pulmonary disease; OR— odds ratio; ref — reference group in the regression analysis.
6 E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
Abbreviations
Basque Telecare Public Service BTPSHealthcare-related quality of life HRQoLMultiple regression of ordinary least squares OLS
Conflict of interest
The authors declare that they have no conflicts of interest associatedwith this manuscript.
Acknowledgements
The authors wish to acknowledge the team of teleoperators of BTPS,for calling andmaking all interviews to the users, as well as, those userswho took part in the study.
This paper arises from research conducted as part of the Joint Actionaddressing chronic conditions and healthy ageing across the life cycle(JA-CHRODIS), which has received funding from the European Union,under the framework of the Health Programme (2008–2013).
References
[1] Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA. Epidemiology and im-pact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract JR Coll Gen Pract 2011;61:e12–21. http://dx.doi.org/10.3399/bjgp11X548929.
[2] Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. Agingwith multimorbidity: a systematic review of the literature. Ageing Res Rev 2011;10:430–9. http://dx.doi.org/10.1016/j.arr.2011.03.003.
[3] Schäfer I, Hansen H, Schön G, Höfels S, Altiner A, Dahlhaus A, et al. The influence ofage, gender and socio-economic status on multimorbidity patterns in primary care.First results from the multicare cohort study. BMC Health Serv Res 2012;12:89.http://dx.doi.org/10.1186/1472-6963-12-89.
[4] Salive ME. Multimorbidity in older adults. Epidemiol Rev 2013. http://dx.doi.org/10.1093/epirev/mxs009.
[5] Gijsen R, Hoeymans N, Schellevis FG, Ruwaard D, Satariano WA, van den Bos GA.Causes and consequences of comorbidity: a review. J Clin Epidemiol 2001;54:661–74.
[6] Fortin M, Lapointe L, Hudon C, Vanasse A, Ntetu AL, Maltais D. Multimorbidity andquality of life in primary care: a systematic review. Health Qual Life Outcomes2004;2:51. http://dx.doi.org/10.1186/1477-7525-2-51.
Please cite this article as: Alonso-Morán E, et al, Health-related quality of liin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016
[7] Hodek J-M, Ruhe A-K, Greiner W. [Relationship between health-related quality of lifeandmultimorbidity]. Gesundheitswesen Bundesverb Ärzte Öffentl GesundheitsdienstesGer n.d.;72:455–65. http://dx.doi.org/10.1055/s-0029-1234121.
[8] Rijken M, van Kerkhof M, Dekker J, Schellevis FG. Comorbidity of chronic diseases:effects of disease pairs on physical and mental functioning. Qual Life Res Int J QualLife Asp Treat Care Rehabil 2005;14:45–55.
[9] Mcdowell I. Measuring health: a guide to rating scales 3rd ed. 2006.[10] Fortin M, Bravo G, Hudon C, Lapointe L, Almirall J, Dubois M-F, et al. Relationship be-
tween multimorbidity and health-related quality of life of patients in primary care.Qual Life Res Int J Qual Life Asp Treat Care Rehabil 2006;15:83–91. http://dx.doi.org/10.1007/s11136-005-8661-z.
[11] Orueta JF, García-Álvarez A, García-Goñi M, Paolucci F, Nuño-Solinís R. Prevalenceand costs of multimorbidity by deprivation levels in the Basque Country: a popula-tion based study using health administrative databases. PLoS One 2014;9:e89787.http://dx.doi.org/10.1371/journal.pone.0089787.
[12] Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications ofmultiple chronic conditions in the elderly. Arch Intern Med 2002;162:2269–76.
[13] Orueta JF, Nuño-Solinís R, García-Alvarez A, Alonso-Morán E. Prevalence ofmultimorbidity according to the deprivation level among the elderly in the BasqueCountry. BMC Public Health 2013;13:918. http://dx.doi.org/10.1186/1471-2458-13-918.
[14] Israel GD. Determining sample size. University of Florida Cooperative Extension Ser-vice, Institute of Food and Agriculture Sciences, EDIS. University of Florida Coopera-tive Extension Service, Institute of Food and Agriculture Sciences, EDIS; 1992.
[15] Orueta JF, García-Álvarez A, Alonso-Morán E, Vallejo-Torres L, Nuño-Solinis R. Socio-economic variation in the burden of chronic conditions and health careprovision—analyzing administrative individual level data from the Basque Country,Spain. BMC Public Health 2013;13:870. http://dx.doi.org/10.1186/1471-2458-13-870.
[16] Orueta JF, Alonso-Morán E, Nuño-Solinis R, Alday-Jurado A, Gutiérrez-Fraile E,García-Álvarez A. Prevalencia de cronicidad y multimorbilidad en la poblacióncubierta por el servicio público de teleasistencia de Euskadi: impacto en costes ycalidad de la atención. An Sist Sanit Navar 2013;36:429–40. http://dx.doi.org/10.4321/S1137-66272013000300008.
[17] Brettschneider C, Leicht H, Bickel H, Dahlhaus A, Fuchs A, Gensichen J, et al. Relativeimpact of multimorbid chronic conditions on health-related quality of life—resultsfrom the MultiCare Cohort Study. PLoS One 2013;8:e66742. http://dx.doi.org/10.1371/journal.pone.0066742.
[18] Vogel I, Miksch A, Goetz K, Ose D, Szecsenyi J, Freund T. The impact of perceived so-cial support and sense of coherence on health-related quality of life in multimorbidprimary care patients. Chronic Illn 2012;8:296–307. http://dx.doi.org/10.1177/1742395312445935.
[19] Heyworth ITM, Hazell ML, Linehan MF, Frank TL. How do common chronic condi-tions affect health-related quality of life? Br J Gen Pract J R Coll Gen Pract 2009;59:e353–8. http://dx.doi.org/10.3399/bjgp09X453990.
[20] Saarni SI, Härkänen T, Sintonen H, Suvisaari J, Koskinen S, Aromaa A, et al. The im-pact of 29 chronic conditions on health-related quality of life: a general population
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013

7E. Alonso-Morán et al. / European Journal of Internal Medicine xxx (2015) xxx–xxx
survey in Finland using 15D and EQ-5D. Qual Life Res Int J Qual Life Asp Treat CareRehabil 2006;15:1403–14. http://dx.doi.org/10.1007/s11136-006-0020-1.
[21] Agborsangaya CB, Lau D, Lahtinen M, Cooke T, Johnson JA. Health-related quality oflife and healthcare utilization in multimorbidity: results of a cross-sectional survey.Qual Life Res Int J Qual Life Asp Treat Care Rehabil 2013;22:791–9. http://dx.doi.org/10.1007/s11136-012-0214-7.
[22] Garin N, Olaya B, Moneta MV, Miret M, Lobo A, Ayuso-Mateos JL, et al. Impactof multimorbidity on disability and quality of life in the spanish older popula-tion. PLoS One 2014;9:e111498. http://dx.doi.org/10.1371/journal.pone.0111498.
[23] Hunger M, Thorand B, Schunk M, Döring A, Menn P, Peters A, et al. Multimorbidityand health-related quality of life in the older population: results from the GermanKORA-Age study. Health Qual Life Outcomes 2011;9:53. http://dx.doi.org/10.1186/1477-7525-9-53.
Please cite this article as: Alonso-Morán E, et al, Health-related quality of liin the Basque Country, Eur J Intern Med (2015), http://dx.doi.org/10.1016
[24] Aubé-Maurice J, Rochette L, Blais C. Divergent associations between incident hyper-tension and deprivation based on different sources of case identification. Chronic DisInj Can 2012;32:121–30.
[25] Van den Bussche H, Schäfer I, Wiese B, Dahlhaus A, Fuchs A, Gensichen J, et al. Acomparative study demonstrated that prevalence figures on multimorbidity requirecautious interpretation when drawn from a single database. J Clin Epidemiol 2013;66:209–17. http://dx.doi.org/10.1016/j.jclinepi.2012.07.019.
[26] Orueta JF, Urraca J, Berraondo I, Darpón J. Can primary care physicians use the ICD-9-MC? An evaluation of the quality of diagnosis coding in computerized medical re-cords. Gac Sanit 2006;20:194–201.
[27] Hirani SP, Beynon M, Cartwright M, Rixon L, Doll H, Henderson C, et al. The effect oftelecare on the quality of life and psychological well-being of elderly recipients of so-cial care over a 12-month period: the Whole Systems Demonstrator clusterrandomised trial. Age Ageing 2013:1–8. http://dx.doi.org/10.1093/ageing/aft185.
fe andmultimorbidity in community-dwelling telecare-assisted elders/j.ejim.2015.02.013