Embed Size (px)
Citation preview

Developing interventions for people with
complex multi-morbidities: general
principles
Carl May

Acknowledgements
Frances Mair,* Alison Richardson,** Victor M Montori,† David Eton,† Katie Gallacher,*
Katherine Hunt,** Anne Rogers,** Nathan Shippee‡
*University of Glasgow
**University of Southampton & NIHR CLAHRC Wessex
†Mayo Clinic
‡University of Minnesota
2

Presentation draws on three programmes of work
1. Understanding the processes through which work becomes embedded
in everyday practice, and to the problem of patient contributions to
illness related work (May et al; Mair et al).
2. Investigating interactions between the work delegated by healthcare
systems to patients, and the ways in which they negotiate capacity to
meet the demands of delegated work (Mair et al; Montori et al).
3. Exploring how demand, self-care, and social networks, social support,
influence the conduct and outcomes important practical work around
healthcare and self-care (Rogers et al).
3

• Multi-morbidity: presence of two or more clinically defined conditions. Examples:
– stroke + anxiety + osteoarthritis
– schizophrenia + diabetes
– Lowy body dementia + heart failure + glaucoma

• Multi-morbidity is a recently discovered, and perhaps previously hidden epidemic
– Creates complex and demanding work for patients
– (burden of symptoms + burden of treatment)
– Creates complex and demanding work for healthcare providers
– (specialisms not generalisms, disease specific guidelines and performance indicators)

• The NHS is in danger of
being overwhelmed
• Demand can’t be
controlled
• New services and skills
are needed
• Not clear who will
deliver them
General Principles for

• Patients and health care providers experience increased workload
• Complex consultations, multiple clinic appointments, administration, demand management
• Multimorbidity + Burden of symptoms + Burden of Treatment = complexity

Illness burden + treatment burden = Adverse
outcomes
Ageing population;
Multimorbidity
Polypharmacy;
Multiple appointment
s
Quality/safety concerns;
Fragmentation
Slide courtesy of David Blane/Frances Mair

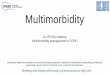
CapacityTreatment
BurdenTreatment
BurdenCapacity
Capacity/Workload ThresholdGallacher K, May CR, Montori V, Mair FS. Treatment Burden in Multimorbidity. In ABC of Multimorbidity. 2014

10

Minimally Disruptive Medicine
• Establish the weight of burden.
• Incentivise co-ordination in clinical practice.
• Acknowledge co-morbidity in clinical evidence.
• Prioritize from the patient perspective.

12
As workload increases
• Sense-making is threatened
• Participation declines
• Care is fragmented
• Monitoring is complicated


Attack Burden of Treatment (1)
• Build and strengthen networks around sick people, people, and equip them to to more effectively navigate navigate services and opportunities.
• Facilitate co-operation and and social capital, and that that compensate for deficiencies in functional performance.

Attack Burden of Treatment (2)
• Reduce the load of cognitive and practical tasks delegated to patients and their significant others.
• Maximize collective competence in enacting practical tasks, distributing help and exploiting local resources.

16

17

Thank you!
Picture credits: Cathy Chesham; BMJ Publications; Steve Galbraith