Embed Size (px)
Citation preview

10/25/2019
1
Health EquityVulnerable Populations
Haywood L. Brown, MD, FACOG
Past President ACOG (2017‐2018)
Professor Obstetrics Gynecology
Associate Dean, Diversity
University South Florida
Professor Emeritus Duke University
UNIVERSITY OF SOUTH FLORIDA
Objectives
At the conclusion of this presentation the participant will be able to:
• Discuss health equity and the impact on disparity in the context of maternal health
• Emphasize the impact of bias on maternal outcome for individuals from vulnerable populations at the clinical, operational and system levels
• Discuss health policy implications for support or lack there of on the quality of maternity child care in the US
UNIVERSITY OF SOUTH FLORIDA
Disclosure
• Merck • Manual
• Merck for Mother’s Global Advisory Board
• Up to Date• Contributor to publications
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
2
Definitions
• Disparity (Healthy People 2010)• the quantity that separates a group from a reference point on a particular measure of health that is expressed in terms of a rate, proportion, mean, or some other quantitative measure
• often measured from the most favorable group rate
• Health inequity (Boston Public Health Commission)• difference in health that is not only unnecessary and avoidable but, in addition, are considered unfair and unjust
• rooted in social injustices that make some population groups more vulnerable to poor health than other groups.
UNIVERSITY OF SOUTH FLORIDA
Health Disparities (Vulnerable populations)
Equality
• Giving everyone a shoeEquity
• Giving everyone a shoe that fits
Contributors to health and health care inequities
Patient-level factors•Beliefs and preferences•Race/ethnicity, culture, family•Education and resources•Biology
Clinical encounter•Provider communication•Cultural competence
Provider factors•Knowledge and attitudes•Competing demands•Implicit/explicit biases
Health system factors• Health services organization, financing, delivery• Health care organizational culture, QI
Structural factors• Poverty/wealth• Unemployment• Stability of housing• Food security• Racism
Adapted from Kilbourne et al,AJPH 2006
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
3
Contributors to health and health care inequities
Patient-level factors•Beliefs and preferences•Race/ethnicity, culture, family•Education and resources•Biology
Clinical encounter•Provider communication•Cultural competence
Provider factors•Knowledge and attitudes•Competing demands•Implicit/explicit biases
Health system factors• Health services organization, financing, delivery• Health care organizational culture, QI
Structural factors• Poverty/wealth• Unemployment• Stability of housing• Food security• Racism Adapted from Kilbourne et al,
AJPH 2006
Racial/ethnic disparities in Ob/GynAI/AN Asian Black Hispanic White
Disparities in health outcomes
Infertility in last 12 months
(% of women)
-- 10 12 9 7
Unintended pregnancy (%
of pregnancies)
-- -- 69 56 42
Preterm birth (% of LB) 14 10 17 12 11
Fetal death (/1,000 live
births+ fetal deaths)
-- -- 11 5 5
Maternal death (/100,000
live births)
-- 10 33 10 11
Gonorrhea (/100,000
population)
96 18 570 -- 24
Breast cancer deaths
(/100,000 population)
16 12 31 15 22
ACOG CO
#649
Research, Ethics and Health Care& Penicillin
TRUST, Research, Ethics and health disparities
• TUSKEGEE• US Public Health Service Tuskegee Untreated Syphilis Study in Negro Men
• Over 40 years lost to follow‐up only 17%
• 1100 paper published between 1934‐1974

10/25/2019
4
Trust gaps
• ETIOLOGY OF DISPARITIES IN MATERNAL MORTALITY
“When Landrum complained about how she was feeling more forcefully at the appointment, she recalls, her doctor told her to lie down — and calm down.”
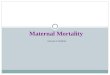
U.S. Maternal and Infant Mortality
U.S. has higher maternal and infant mortality rates than other wealthy countries:
• Ranks 19th of 20 in child mortality
• Ranks > 21th in maternal mortality
“Hidden causes” of maternal mortality
Koch, 2016

10/25/2019
5
Maternal Mortality is Preventable
Main et al. Obstet Gynecol 2015;125(4):938-947
UNIVERSITY OF SOUTH FLORIDA
Vulnerable populations• US has higher maternal mortality than Iran, Libya and Turkey
• US maternal mortality 2x greater than Canada
• Childbirth number 1 reason for hospitalization in the US
• For every maternal death 50‐100 near miss morbidities
• 60 maternal deaths postpartum
• Black women die at rate of 3 to 4 times that of white women in the US
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
6
Preterm Birth Report 2016
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
7
Rural Hospital Closures
• Many of those hospitals in the South in states that did not expand Medicaid as of January 2017.
• 82% of rural hospital closures (no Medicaid expansion)
• Rural Southeastern communities with measurable health disparities for chronic conditions
• Diabetes
• Hypertension
• obesity
UNIVERSITY OF SOUTH FLORIDA
Preventable Maternal Mortality
• Leading causes of maternal death for non‐Hispanic black women• Cardiomyopathy (14.0%)• Cardiovascular and coronary conditions (12.8%)• Preeclampsia/eclampsia (11.6%)• Hemorrhage (10.5%)• Embolism (9.3%)
• Deaths with the higher degree of preventability • Cardiovascular and coronary disease ( 68.2%)• Hemorrhage (70%)
• Metz TD, Obstet Gynecol 2018;132:1040‐5.
UNIVERSITY OF SOUTH FLORIDA
Maternal MortalityPostpartum
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
8
Fragmentation of Care
• 50% of all hospitals in US provide care for three or fewer deliveries a day
• Team training for readiness to manage preventable morbidity (i.e. limited blood supply)
• Tighten the partnership with health centers (clinics), hospital and all obstetrical care providers: obstetricians, family physicians, nurse practitioners, midwives)
• telemedicine
• Shortage and maldistribution of obstetricians in the US particularly in rural communities
• Specialty and subspecialty consultation
UNIVERSITY OF SOUTH FLORIDA
Rural vs Urban Care and Maternal Morbidity
• Lisonkova et al. CMAJ 2016• Results
• British Columbia, Canada comparing mortality and severe morbidity
• death and severe maternal morbidity ( OR‐1.15, Ci 1.03‐1.28) in rural vs urban
• Rural had Higher rate of eclampsia (OR‐2.70, Ci 1.79‐4.08), embolism (OR‐2.16, CI 1.14‐4.07), uterine rupture (OR‐1.96, CI 1.42‐2.72) than urban women
• Infants in rural more likely to have severe neonatal morbidity (OR‐ 1.14, CI 1.10‐1.19
• Conclusions• Providers in rural areas need to be aware of potential morbidities and mortality risk.
UNIVERSITY OF SOUTH FLORIDA
Understanding Racial Disparities:The Big Picture
Source: Elisabeth Howell, MD, MPP. Reduction of PeripartumDisparities Bundle. 2017.
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
9
Health Equity
• In an analysis of 23,692 women with Medicaid, predictors of not attending a postpartum visit included:
• Black race
• Alcohol or drug use
• Mental health disorder other than depression
• Living in a neighborhood where a high proportion of individuals >25 do not have a high school diploma
• Ensuring ALL women are engaged in the support they need following birth is an essential step in achieving health equity
Bennett et al (2014)http://www.ncbi.nlm.nih.gov/pubmed/24474651
Impact of lack of postpartum follow‐up
Early cessation of breastfeeding
Short interval pregnancy Undiagnosed postpartum depression / anxiety
Preterm birth and infant mortality
Levels of Maternal Care
UNIVERSITY OF SOUTH FLORIDA

10/25/2019
10
UNIVERSITY OF SOUTH FLORIDA
American Heart Association Guidelines for CVD Prevention
• Detailed history of pregnancy• Gestational diabetes• Preeclampsia
• Preterm birth
• Small infant
• Historically screening occurs later in life
• Identification during pregnancy maximizes opportunity for prevention
Circulation March 2011
UNIVERSITY OF SOUTH FLORIDA
Critical Factors
• System Leadership • Awareness and assess for risk of pregnancy complications without promoting fear
• Education of patient and providers and shared decision making in obstetrical care
• Awareness of institutional biases that impact obstetrical care at any level that might impact quality and safety
• Adopt and require adherence to best practice guidelines, protocols, and bundles to reduce risk for morbidity and mortality
• Adequate resources for safe and supportive obstetrical care• Team training, simulation drills for common obstetrical emergencies
• Accountability UNIVERSITY OF SOUTH FLORIDA

10/25/2019
11
Health Policy Implications
• Coverage beyond 6 weeks for women with pregnancy complications
• Seamless handover of care
• Disseminate to providers, public and payors
• Monitor and incentivize compliance
• Fund research to improve lifelong health in women
UNIVERSITY OF SOUTH FLORIDA
Health Policy (Human Rights)
Disparity
• Social inequality kills: • It deprives individuals and communities of a healthy start in life, increases their burden of disability and disease, and brings early death.
• Poverty and discrimination
• Inadequate medical care
• And violation of human rights
• “All act as powerful social determinants of who lives and who dies, at what age, and with what degree of suffering.”
• Nancy Krieger (2005). Healthy bodies and disparity. Boston Harvard school of Public Health

10/25/2019
12
Conclusions
• Racial/ethnic disparities and inequities in obstetrical health and health care are prevalent and persistent
• Movement beyond documentation of disparities and inequities in obstetrics is critical to their elimination
• Adoption of uniform care standards, recognizing our own biases and understanding of the contribution of social determinants of health (including systemic racism) have particular importance for care and outcomes of women in underserved communities
• We can and should advocate for codifying equity best practices, by legislative action, among others