Embed Size (px)
Citation preview
DOI: 10.1542/peds.2009-3592 published online Feb 14, 2011; Pediatrics
Sara M. Seifert, Judith L. Schaechter, Eugene R. Hershorin and Steven E. Lipshultz Health Effects of Energy Drinks on Children, Adolescents, and Young Adults
http://www.pediatrics.orglocated on the World Wide Web at:
The online version of this article, along with updated information and services, is
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275. Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by on February 15, 2011 www.pediatrics.orgDownloaded from

Health Effects of Energy Drinks on Children,Adolescents, and Young Adults
abstractOBJECTIVE: To review the effects, adverse consequences, and extent ofenergy-drink consumption among children, adolescents, and youngadults.
METHODS: We searched PubMed and Google using “energy drink,”“sports drink,” “guarana,” “caffeine,” “taurine,” “ADHD,” “diabetes,”“children,” “adolescents,” “insulin,” “eating disorders,” and “poisoncontrol center” to identify articles related to energy drinks. Manu-facturer Web sites were reviewed for product information.
RESULTS: According to self-report surveys, energy drinks are con-sumed by 30% to 50% of adolescents and young adults. Frequentlycontaining high and unregulated amounts of caffeine, these drinkshave been reported in association with serious adverse effects, espe-cially in children, adolescents, and young adults with seizures, diabe-tes, cardiac abnormalities, or mood and behavioral disorders orthose who take certain medications. Of the 5448 US caffeine over-doses reported in 2007, 46% occurred in those younger than 19years. Several countries and states have debated or restricted theirsales and advertising.
CONCLUSIONS: Energy drinks have no therapeutic benefit, and manyingredients are understudied and not regulated. The known and un-known pharmacology of agents included in such drinks, combinedwithreports of toxicity, raises concern for potentially serious adverse ef-fects in association with energy-drink use. In the short-term, pediatri-cians need to be aware of the possible effects of energy drinks invulnerable populations and screen for consumption to educate fami-lies. Long-term research should aim to understand the effects in at-riskpopulations. Toxicity surveillance should be improved, and regulationsof energy-drink sales and consumption should be based on appropri-ate research. Pediatrics 2011;127:511–528
AUTHORS: Sara M. Seifert, BS, Judith L. Schaechter, MD,Eugene R. Hershorin, MD, and Steven E. Lipshultz, MD
Department of Pediatrics and the Pediatric Integrative MedicineProgram, University of Miami, Leonard M. Miller School ofMedicine, Miami, Florida
KEY WORDSenergy drink, caffeine, taurine, children, adolescents, overdose
ABBREVIATIONSFDA—Food and Drug AdministrationADHD—attention-deficit/hyperactivity disorder
www.pediatrics.org/cgi/doi/10.1542/peds.2009-3592
doi:10.1542/peds.2009-3592
Accepted for publication Dec 3, 2010
Address correspondence to Steven E. Lipshultz, MD, Departmentof Pediatrics (D820), Leonard M. Miller School of Medicine,University of Miami, Medical Campus MCCD-D820, 1601 NW 12thAve, 9th Floor, PO Box 016820, Miami, FL 33101. E-mail:[email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they haveno financial relationships relevant to this article to disclose.
Funded by the National Institutes of Health (NIH).
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 511 by on February 15, 2011 www.pediatrics.orgDownloaded from

“Energy drinks” are beverages thatcontain caffeine, taurine, vitamins,herbal supplements, and sugar orsweeteners and are marketed to im-prove energy, weight loss, stamina,athletic performance, and concen-tration.1–3 Energy drinks are availablein �140 countries and are the fastestgrowing US beverage market; in 2011,sales are expected to top $9 billion.4–10
Half of the energy-drink market con-sists of children (�12 years old), ado-lescents (12–18 years old), and youngadults (19–25 years old).7–10
Although healthy people can toleratecaffeine in moderation, heavy caffeineconsumption, such as drinking energydrinks, has been associated with evenmore serious consequences such asseizures, mania, stroke, and suddendeath.6–8,12–14 Numerous reports existin the popular media, and there are ahandful of case reports in the litera-ture that associate such adverseevents with energy-drink consump-tion; it is prudent to investigate thevalidity of such claims (Appendix).Children, especially those with car-diovascular, renal, or liver disease,seizures, diabetes, mood and behav-ioral disorders, or hyperthyroidism orthose who take certain medications,may be at higher risk for adverseevents from energy-drink consump-tion.6–8,14–24 Although the US Food andDrug Administration (FDA) limits caf-feine content in soft drinks, which arecategorized as food, there is no suchregulation of energy drinks, which areclassified as dietary supplements.1–3
Despite the large, unregulated marketfor energy drinks and reports in theliterature and popular media of seri-ous adverse events associated withtheir consumption, research into theiruse and effects has been sparse.25
However, schools, states, and coun-tries increasingly are exploring con-tent and sales regulations of thesedrinks.1,8,13,26–35
Given the rapidly growing market andpopularity among youth, we re-viewed the literature to (1) deter-mine what energy drinks are, (2)compile consumption data of energydrinks by children, adolescents, andyoung adults, (3) compile caffeineand energy-drink overdose data, (4)examine the physiologic effects ofthe ingredients in energy drinks, (5)identify potential problems of energydrinks among children and adoles-cents, (6) assess the marketing ofenergy drinks, (7) report currentregulation of energy drinks, and (8)propose educational, research, andregulatory recommendations.
METHODS
We searched PubMed by using “energydrink,” “sports drink,” “guarana,” “caf-feine,” “taurine,” “ADHD” (attention-deficit/hyperactivity disorder), “diabe-tes,” “children,” “adolescents,” “insulin,”“eating disorders,” and “poison controlcenter” singly or in combination. We lim-ited searches to English-language andforeign-language articles with English-languageabstractsandselectedarticlesby relevance to energy-drink use in chil-dren and adolescents. We similarlysearched Google for print and trademe-dia. We reviewed articles and Internetsources by the above search throughJune 2010 and updated sections as newinformation became available throughJanuary 2011.
RESULTS
Two-thirds of the 121 references wefound on energy drinks were in the sci-entific literature, although reports bygovernment agencies and interestgroups also contained much useful in-formation (Table 1). Most informationcame from the United States, but Euro-pean, Canadian, Australian, New Zea-land, and Chinese sources are alsorepresented.
DISCUSSION
What Are Energy Drinks?
Energy drinks may contain caffeine,taurine, sugars and sweeteners,herbal supplements, and other ingre-dients (Table 2) and are distinct fromsports drinks and vitamin waters (Ta-ble 3).6,8 In 2008, the National Federa-tion of State High School Associations,while recommending water andsports drinks for rehydration, spe-cifically did not recommend energydrinks and cited potential risks, theabsence of benefit, and drug interac-tions (Table 4).36,37
Caffeine is the main active ingredientin energy drinks; many of them contain70 to 80 mg per 8-oz serving (�3 timesthe concentration in cola drinks) (Ta-ble 5).8,31 Caffeine content can benearly 5 times greater than that in 8 ozof cola drinks when packaged as “en-ergy shots” (0.8–3 oz) or as 16-ozdrinks.6,29,38
Energy drinks often contain additionalamounts of caffeine through additives,including guarana, kola nut, yerbamate, and cocoa.6,7,14,25 Guarana(Paullinia cupana) is a plant thatcontains caffeine, theobromine (achronotrope), and theophylline (aninotrope).39 Each gram of guaranacan contain 40 to 80 mg of caffeine,and it has a potentially longer half-life because of interactions withother plant compounds.7,14 Manufac-turers are not required to list thecaffeine content from these ingredi-ents.7,14 Thus, the actual caffeinedose in a single serving may exceedthat listed.9,29
Consumption of Energy Drinks byChildren, Adolescents, and YoungAdults
In the United States, adolescent caf-feine intake averages 60 to 70 mg/dayand ranges up to 800 mg/day.24,40 Mostcaffeine comes from soda; however,
512 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from
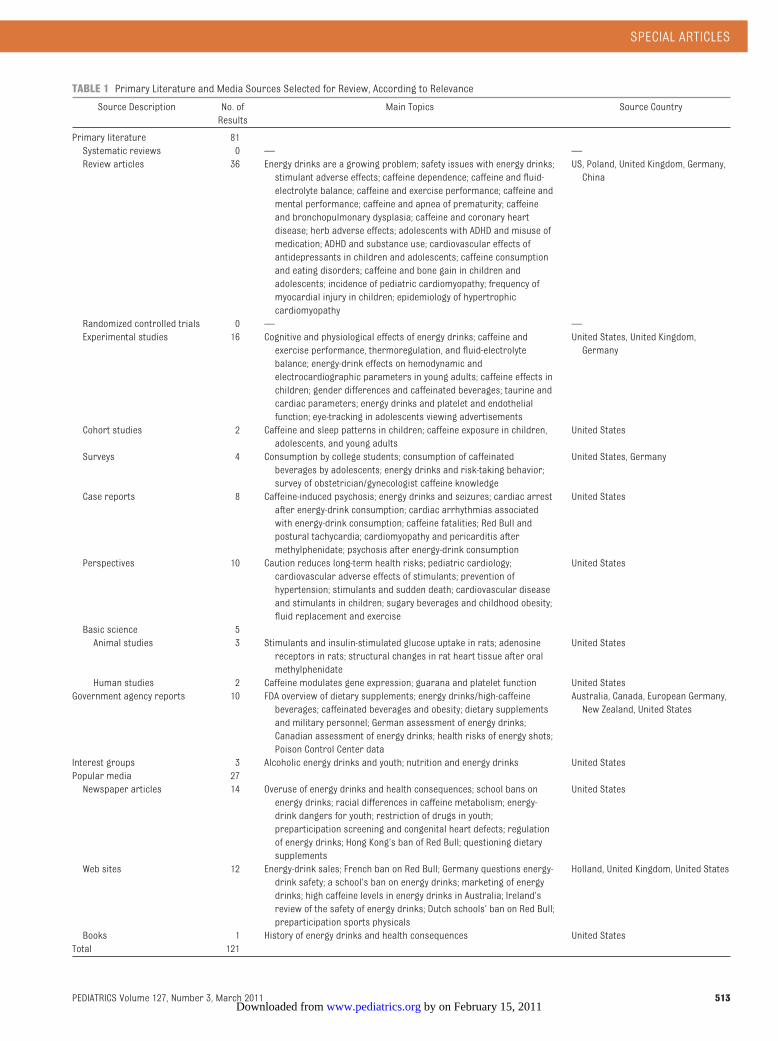
TABLE 1 Primary Literature and Media Sources Selected for Review, According to Relevance
Source Description No. ofResults
Main Topics Source Country
Primary literature 81Systematic reviews 0 — —Review articles 36 Energy drinks are a growing problem; safety issues with energy drinks;
stimulant adverse effects; caffeine dependence; caffeine and fluid-electrolyte balance; caffeine and exercise performance; caffeine andmental performance; caffeine and apnea of prematurity; caffeineand bronchopulmonary dysplasia; caffeine and coronary heartdisease; herb adverse effects; adolescents with ADHD and misuse ofmedication; ADHD and substance use; cardiovascular effects ofantidepressants in children and adolescents; caffeine consumptionand eating disorders; caffeine and bone gain in children andadolescents; incidence of pediatric cardiomyopathy; frequency ofmyocardial injury in children; epidemiology of hypertrophiccardiomyopathy
US, Poland, United Kingdom, Germany,China
Randomized controlled trials 0 — —Experimental studies 16 Cognitive and physiological effects of energy drinks; caffeine and
exercise performance, thermoregulation, and fluid-electrolytebalance; energy-drink effects on hemodynamic andelectrocardiographic parameters in young adults; caffeine effects inchildren; gender differences and caffeinated beverages; taurine andcardiac parameters; energy drinks and platelet and endothelialfunction; eye-tracking in adolescents viewing advertisements
United States, United Kingdom,Germany
Cohort studies 2 Caffeine and sleep patterns in children; caffeine exposure in children,adolescents, and young adults
United States
Surveys 4 Consumption by college students; consumption of caffeinatedbeverages by adolescents; energy drinks and risk-taking behavior;survey of obstetrician/gynecologist caffeine knowledge
United States, Germany
Case reports 8 Caffeine-induced psychosis; energy drinks and seizures; cardiac arrestafter energy-drink consumption; cardiac arrhythmias associatedwith energy-drink consumption; caffeine fatalities; Red Bull andpostural tachycardia; cardiomyopathy and pericarditis aftermethylphenidate; psychosis after energy-drink consumption
United States
Perspectives 10 Caution reduces long-term health risks; pediatric cardiology;cardiovascular adverse effects of stimulants; prevention ofhypertension; stimulants and sudden death; cardiovascular diseaseand stimulants in children; sugary beverages and childhood obesity;fluid replacement and exercise
United States
Basic science 5Animal studies 3 Stimulants and insulin-stimulated glucose uptake in rats; adenosine
receptors in rats; structural changes in rat heart tissue after oralmethylphenidate
United States
Human studies 2 Caffeine modulates gene expression; guarana and platelet function United StatesGovernment agency reports 10 FDA overview of dietary supplements; energy drinks/high-caffeine
beverages; caffeinated beverages and obesity; dietary supplementsand military personnel; German assessment of energy drinks;Canadian assessment of energy drinks; health risks of energy shots;Poison Control Center data
Australia, Canada, European Germany,New Zealand, United States
Interest groups 3 Alcoholic energy drinks and youth; nutrition and energy drinks United StatesPopular media 27Newspaper articles 14 Overuse of energy drinks and health consequences; school bans on
energy drinks; racial differences in caffeine metabolism; energy-drink dangers for youth; restriction of drugs in youth;preparticipation screening and congenital heart defects; regulationof energy drinks; Hong Kong’s ban of Red Bull; questioning dietarysupplements
United States
Web sites 12 Energy-drink sales; French ban on Red Bull; Germany questions energy-drink safety; a school’s ban on energy drinks; marketing of energydrinks; high caffeine levels in energy drinks in Australia; Ireland’sreview of the safety of energy drinks; Dutch schools’ ban on Red Bull;preparticipation sports physicals
Holland, United Kingdom, United States
Books 1 History of energy drinks and health consequences United StatesTotal 121
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 513 by on February 15, 2011 www.pediatrics.orgDownloaded from

energy drinks are becoming increas-ingly popular.7,24,41,42 The following self-report studies have examined energy-drink consumption by children,adolescents, and young adults.7,24,41,42
One study found that 28% of 12- to14-year-olds, 31% of 12- to 17-year
olds, and 34% of 18- to 24-year-oldsreported regularly consuming en-ergy drinks.5,43 Shortly after energydrinks were approved in Germany, astudy of 1265 adolescents found that94% were aware of energy drinks,53% had tried them, 23% drank �1
can per week, and 3% drank 1 to 7cans per week.44 Among 10- to 13-year-olds, 31% of girls and 50% ofboys had tried energy drinks, and 5%of girls and 23% of boys reporteddrinking them regularly but at a rateof �1 can per week.44 Most children
TABLE 2 Common Ingredients, Therapeutic Uses, and Adverse Effects of Energy-Drink Ingredients8,14,25,50,54,83,84
Ingredient Description Therapeutic Uses Purported Effect FromEnergy Drinks
Adverse Effects (due to Idiosyncratic orExcessive Dosage)
Caffeine An adenosine receptorantagonist: a centralnervous systemstimulant
As caffeine citrate, used to treat apneaand bronchopulmonary dysplasia inpremature infants
Increases exercise enduranceand improves cognition andmood when fatigued orsleep-deprived
Nervousness, irritability, anxiety, insomnia,tachycardia, palpitations, upsetstomach, vomiting, abdominal pain,rigidity, hypokalemia, alteredconsciousness, paralysis,hallucinations, increased intracranialpressure, cerebral edema, seizures,rhabdomyolysis, supraventricular andventricular tachyarrhythmias
Guarana A South American plantthat contains largeamounts of caffeine,theobromine, andtheophylline (achronotrope and aninotrope) and tannins
None known Stimulant, mainly through theeffects of caffeine, andweight loss
Generally considered safe by the FDACenter for Food Safety and AppliedNutrition
Taurine An abundant amino acid inthe central nervoussystem; acts in neuralgrowth and protection,cell metabolism,osmoregulation,antioxidation, andglycolysis; estimateddaily intake is 400 mg/d
Infant formula has been supplementedwith taurine since the 1980sbecause of evidence that itpromotes healthy development;used to treat alcohol withdrawal,congestive heart failure, cysticfibrosis, palpitations/dysrhythmias,hypertension, diabetes, seizuredisorders, hepatitis
Marketed to promote eye andbiliary health and toprevent congestive heartfailure by lowering bloodpressure while improvingcardiac contractility
Generally considered safe by the FDA
L-Carnitine An amino acid involved in�-oxidation of fattyacids
Used as a therapeutic supplement incongenital and acquired-deficiencystates, end-stage renal disease,valproate toxicity, and dementia;increases attention and decreaseshyperactivity in certain populationsof children; nonstimulant L-acetyl-carnitine is used to treat ADHD inboys with fragile X syndrome and, in1 study, children with typical ADHD;it may also protect against heartdisease
Added to promote fatmetabolism and increaseendurance
In high doses, can cause nausea, vomiting,abdominal pain, and diarrhea; has beenreported to cause seizures in patientswith no known disease and to increaseseizure frequency in patients withseizure disorder
Ginseng An East Asian herb Believed to improve memory, increasestamina, and stimulate immunefunction
Improve physical performance Reported symptoms of ginseng toxicityinclude diarrhea, vaginal bleeding,headache, vertigo, mania, hypertension,rashes, insomnia, irritability, Stevens-Johnson syndrome, andagranulocytosis; some of thesesymptoms may be related tocontaminants, such as phenylbutazoneand aminopyrine, used in its processing
Yohimbine An alkaloid found in theplants Pausinystaliayohimbe and Rauwolfiaserpentina
An herbal supplement believed to bean aphrodisiac and to relieve chestpain, diabetic complications,depression, and erectile dysfunction
Increase energy, metabolism,and stamina; promoteswell-being
Can cause hypertension at usual dosesand hypotension at high doses;tachycardia, death
514 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from
in the study consumed energy drinksin moderation, but a small groupconsumed extreme amounts.44
A survey of 496 college students foundthat 51% of those surveyed regularlyconsumed �1 energy drink per
month; the majority of them habituallydrank energy drinks several times perweek.9 Insufficient sleep (67%) and the
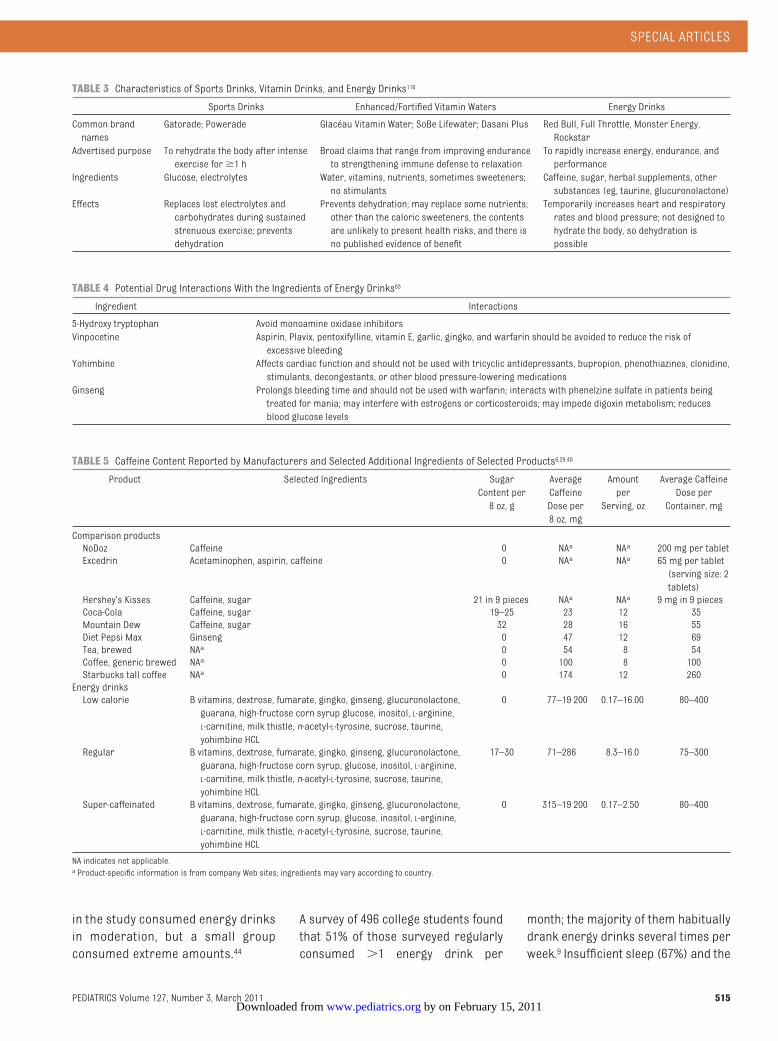
TABLE 3 Characteristics of Sports Drinks, Vitamin Drinks, and Energy Drinks116
Sports Drinks Enhanced/Fortified Vitamin Waters Energy Drinks
Common brandnames
Gatorade; Powerade Glacéau Vitamin Water; SoBe Lifewater; Dasani Plus Red Bull, Full Throttle, Monster Energy,Rockstar
Advertised purpose To rehydrate the body after intenseexercise for�1 h
Broad claims that range from improving enduranceto strengthening immune defense to relaxation
To rapidly increase energy, endurance, andperformance
Ingredients Glucose, electrolytes Water, vitamins, nutrients, sometimes sweeteners;no stimulants
Caffeine, sugar, herbal supplements, othersubstances (eg, taurine, glucuronolactone)
Effects Replaces lost electrolytes andcarbohydrates during sustainedstrenuous exercise; preventsdehydration
Prevents dehydration; may replace some nutrients;other than the caloric sweeteners, the contentsare unlikely to present health risks, and there isno published evidence of benefit
Temporarily increases heart and respiratoryrates and blood pressure; not designed tohydrate the body, so dehydration ispossible
TABLE 4 Potential Drug Interactions With the Ingredients of Energy Drinks83
Ingredient Interactions
5-Hydroxy tryptophan Avoid monoamine oxidase inhibitorsVinpocetine Aspirin, Plavix, pentoxifylline, vitamin E, garlic, gingko, and warfarin should be avoided to reduce the risk of
excessive bleedingYohimbine Affects cardiac function and should not be used with tricyclic antidepressants, bupropion, phenothiazines, clonidine,
stimulants, decongestants, or other blood pressure-lowering medicationsGinseng Prolongs bleeding time and should not be used with warfarin; interacts with phenelzine sulfate in patients being
treated for mania; may interfere with estrogens or corticosteroids; may impede digoxin metabolism; reducesblood glucose levels
TABLE 5 Caffeine Content Reported by Manufacturers and Selected Additional Ingredients of Selected Products6,29,46
Product Selected Ingredients SugarContent per8 oz, g
AverageCaffeineDose per8 oz, mg
Amountper
Serving, oz
Average CaffeineDose perContainer, mg
Comparison productsNoDoz Caffeine 0 NAa NAa 200 mg per tabletExcedrin Acetaminophen, aspirin, caffeine 0 NAa NAa 65 mg per tablet
(serving size: 2tablets)
Hershey’s Kisses Caffeine, sugar 21 in 9 pieces NAa NAa 9 mg in 9 piecesCoca-Cola Caffeine, sugar 19–25 23 12 35Mountain Dew Caffeine, sugar 32 28 16 55Diet Pepsi Max Ginseng 0 47 12 69Tea, brewed NAa 0 54 8 54Coffee, generic brewed NAa 0 100 8 100Starbucks tall coffee NAa 0 174 12 260Energy drinksLow calorie B vitamins, dextrose, fumarate, gingko, ginseng, glucuronolactone,
guarana, high-fructose corn syrup glucose, inositol, L-arginine,L-carnitine, milk thistle, n-acetyl-L-tyrosine, sucrose, taurine,yohimbine HCL
0 77–19 200 0.17–16.00 80–400
Regular B vitamins, dextrose, fumarate, gingko, ginseng, glucuronolactone,guarana, high-fructose corn syrup, glucose, inositol, L-arginine,L-carnitine, milk thistle, n-acetyl-L-tyrosine, sucrose, taurine,yohimbine HCL
17–30 71–286 8.3–16.0 75–300
Super-caffeinated B vitamins, dextrose, fumarate, gingko, ginseng, glucuronolactone,guarana, high-fructose corn syrup, glucose, inositol, L-arginine,L-carnitine, milk thistle, n-acetyl-L-tyrosine, sucrose, taurine,yohimbine HCL
0 315–19 200 0.17–2.50 80–400
NA indicates not applicable.a Product-specific information is from company Web sites; ingredients may vary according to country.
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 515 by on February 15, 2011 www.pediatrics.orgDownloaded from
desire to increase energy (65%) werethe most common reasons for use.9 Inthis study, 54% of the respondents re-ported mixing energy drinks with alco-hol, and 49% drank �3 of them whilepartying.9 Another study of 795 collegestudents found that 39% of the respon-dents had consumed an energy drinkin the previous month and that, on av-erage, men drank energy drinks 2.5days/month, whereas women drank1.2 days/month.45
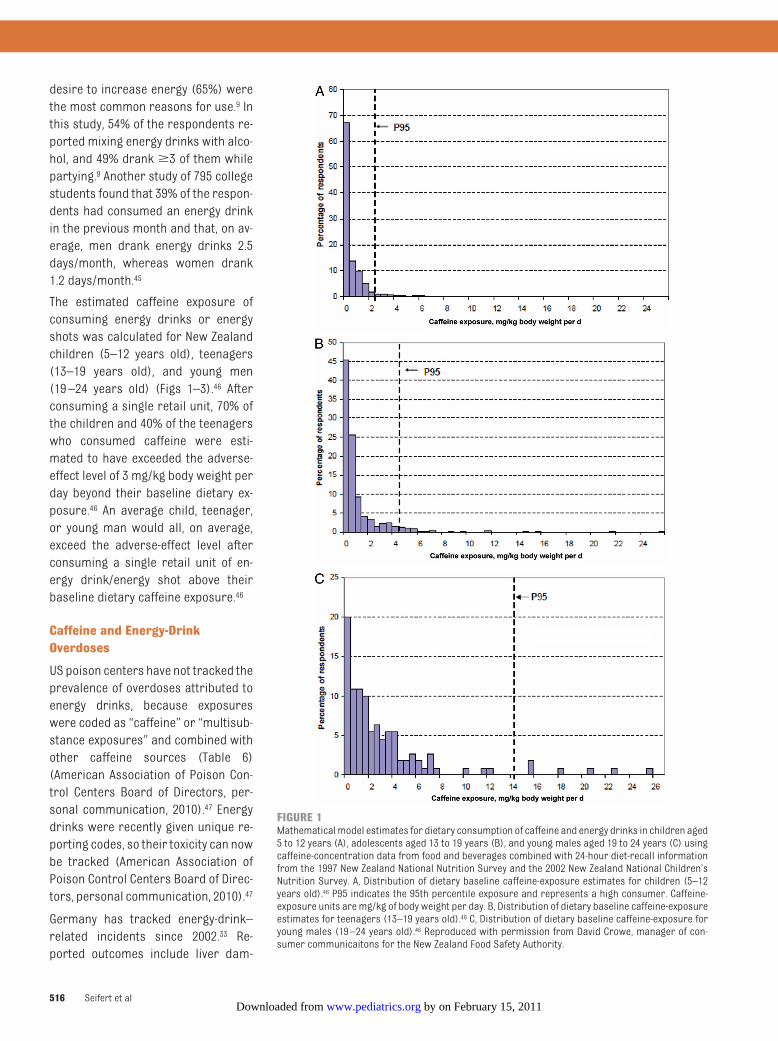
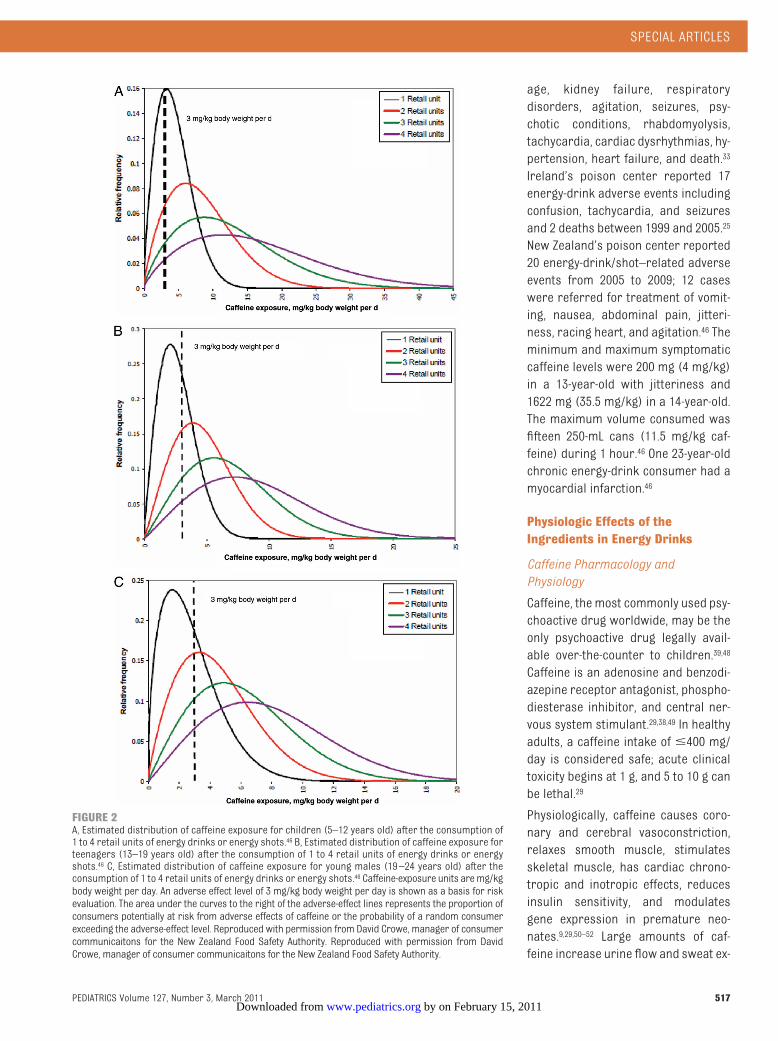
The estimated caffeine exposure ofconsuming energy drinks or energyshots was calculated for New Zealandchildren (5–12 years old), teenagers(13–19 years old), and young men(19–24 years old) (Figs 1–3).46 Afterconsuming a single retail unit, 70% ofthe children and 40% of the teenagerswho consumed caffeine were esti-mated to have exceeded the adverse-effect level of 3 mg/kg body weight perday beyond their baseline dietary ex-posure.46 An average child, teenager,or young man would all, on average,exceed the adverse-effect level afterconsuming a single retail unit of en-ergy drink/energy shot above theirbaseline dietary caffeine exposure.46
Caffeine and Energy-DrinkOverdoses
US poison centers have not tracked theprevalence of overdoses attributed toenergy drinks, because exposureswere coded as “caffeine” or “multisub-stance exposures” and combined withother caffeine sources (Table 6)(American Association of Poison Con-trol Centers Board of Directors, per-sonal communication, 2010).47 Energydrinks were recently given unique re-porting codes, so their toxicity can nowbe tracked (American Association ofPoison Control Centers Board of Direc-tors, personal communication, 2010).47
Germany has tracked energy-drink–related incidents since 2002.33 Re-ported outcomes include liver dam-
FIGURE 1Mathematicalmodel estimates for dietary consumption of caffeine and energy drinks in children aged5 to 12 years (A), adolescents aged 13 to 19 years (B), and young males aged 19 to 24 years (C) usingcaffeine-concentration data from food and beverages combined with 24-hour diet-recall informationfrom the 1997 New Zealand National Nutrition Survey and the 2002 New Zealand National Children’sNutrition Survey. A, Distribution of dietary baseline caffeine-exposure estimates for children (5–12years old).46 P95 indicates the 95th percentile exposure and represents a high consumer. Caffeine-exposure units aremg/kg of body weight per day. B, Distribution of dietary baseline caffeine-exposureestimates for teenagers (13–19 years old).46 C, Distribution of dietary baseline caffeine-exposure foryoung males (19–24 years old).46 Reproduced with permission from David Crowe, manager of con-sumer communicaitons for the New Zealand Food Safety Authority.
516 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from
age, kidney failure, respiratorydisorders, agitation, seizures, psy-chotic conditions, rhabdomyolysis,tachycardia, cardiac dysrhythmias, hy-pertension, heart failure, and death.33
Ireland’s poison center reported 17energy-drink adverse events includingconfusion, tachycardia, and seizuresand 2 deaths between 1999 and 2005.25
New Zealand’s poison center reported20 energy-drink/shot–related adverseevents from 2005 to 2009; 12 caseswere referred for treatment of vomit-ing, nausea, abdominal pain, jitteri-ness, racing heart, and agitation.46 Theminimum and maximum symptomaticcaffeine levels were 200 mg (4 mg/kg)in a 13-year-old with jitteriness and1622 mg (35.5 mg/kg) in a 14-year-old.The maximum volume consumed wasfifteen 250-mL cans (11.5 mg/kg caf-feine) during 1 hour.46 One 23-year-oldchronic energy-drink consumer had amyocardial infarction.46
Physiologic Effects of theIngredients in Energy Drinks
Caffeine Pharmacology andPhysiology
Caffeine, themost commonly used psy-choactive drug worldwide, may be theonly psychoactive drug legally avail-able over-the-counter to children.39,48
Caffeine is an adenosine and benzodi-azepine receptor antagonist, phospho-diesterase inhibitor, and central ner-vous system stimulant.29,38,49 In healthyadults, a caffeine intake of �400 mg/day is considered safe; acute clinicaltoxicity begins at 1 g, and 5 to 10 g canbe lethal.29
Physiologically, caffeine causes coro-nary and cerebral vasoconstriction,relaxes smooth muscle, stimulatesskeletal muscle, has cardiac chrono-tropic and inotropic effects, reducesinsulin sensitivity, and modulatesgene expression in premature neo-nates.9,29,50–52 Large amounts of caf-feine increase urine flow and sweat ex-
FIGURE 2A, Estimated distribution of caffeine exposure for children (5–12 years old) after the consumption of1 to 4 retail units of energy drinks or energy shots.46 B, Estimated distribution of caffeine exposure forteenagers (13–19 years old) after the consumption of 1 to 4 retail units of energy drinks or energyshots.46 C, Estimated distribution of caffeine exposure for young males (19–24 years old) after theconsumption of 1 to 4 retail units of energy drinks or energy shots.46 Caffeine-exposure units aremg/kgbody weight per day. An adverse effect level of 3 mg/kg body weight per day is shown as a basis for riskevaluation. The area under the curves to the right of the adverse-effect lines represents the proportion ofconsumers potentially at risk from adverse effects of caffeine or the probability of a random consumerexceeding the adverse-effect level. Reproduced with permission from David Crowe, manager of consumercommunicaitons for the New Zealand Food Safety Authority. Reproduced with permission from DavidCrowe, manager of consumer communicaitons for the New Zealand Food Safety Authority.
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 517 by on February 15, 2011 www.pediatrics.orgDownloaded from
cretion and alter blood electrolytelevels.11,53 Although caffeine is a milddiuretic, consumption of�500mg/daydoes not cause dehydration or chronicwater imbalance.54,55
Caffeine is a ventilatory stimulant withanti-inflammatory and bronchoprotec-tive effects.56 Caffeine has been linkedto dyspnea on exertion from centraland peripheral chemoreceptor stimu-lation.56 In addition, increased breath-ing work may divert blood flow awayfrom locomotor muscles and negateany ergogenic advantage.56 Caffeine’scardiovascular effects include de-creased heart rate from stimulation ofmedullary vagal nuclei and increasedblood pressure.24,57–61
Adults who consume low-to-moderateamounts of caffeine (1–3 mg/kg or12.5–100 mg/day) have improved exer-cise endurance, cognition, reactiontime, and mood with sleep depriva-tion.9,24,56,62 However, these studiestypically involve habitual caffeineconsumers, and results reflectwithdrawal-symptom reversal.58
Consuming 4 to 12 mg/kg of caffeinehas been associated with undesir-able symptoms, including anxietyand jitteriness.63 Headache and fa-tigue, common withdrawal symp-toms, can occur after short-term,high-dose use.64 Caffeine intoxicationis a clinical syndrome of nervous-ness, irritability, anxiety, insomnia,tremor, tachycardia, palpitations,and upset stomach.6,7,9,14,26,65 Addi-tional adverse effects includevomiting and abdominal pain, hypo-kalemia, hallucinations, increasedintracranial pressure, cerebraledema, stroke, paralysis, rhabdomy-olysis, altered consciousness, rigid-ity, seizures, arrhythmias, anddeath.1,2,8,29,48
Caffeine intakes of�300 mg/day havebeen associated with miscarriage andlow birth weight.38,66,67 Long-term caf-feine consumption relates to a lower
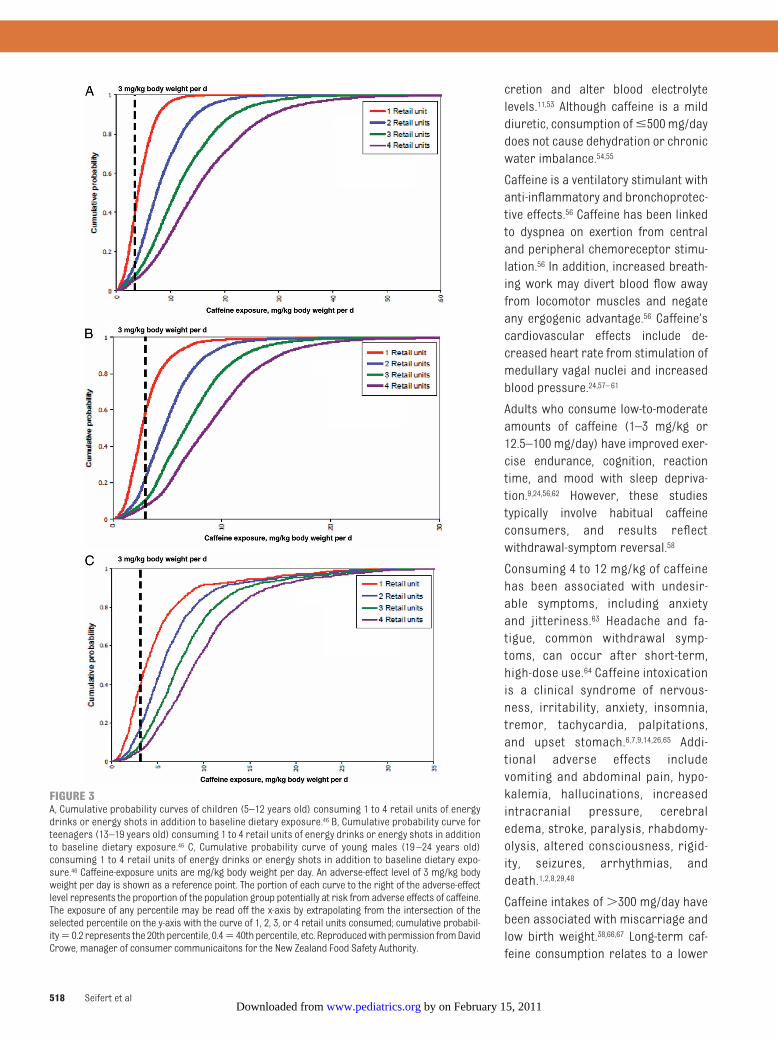
FIGURE 3A, Cumulative probability curves of children (5–12 years old) consuming 1 to 4 retail units of energydrinks or energy shots in addition to baseline dietary exposure.46 B, Cumulative probability curve forteenagers (13–19 years old) consuming 1 to 4 retail units of energy drinks or energy shots in additionto baseline dietary exposure.46 C, Cumulative probability curve of young males (19–24 years old)consuming 1 to 4 retail units of energy drinks or energy shots in addition to baseline dietary expo-sure.46 Caffeine-exposure units are mg/kg body weight per day. An adverse-effect level of 3 mg/kg bodyweight per day is shown as a reference point. The portion of each curve to the right of the adverse-effectlevel represents the proportion of the population group potentially at risk from adverse effects of caffeine.The exposure of any percentile may be read off the x-axis by extrapolating from the intersection of theselected percentile on the y-axis with the curve of 1, 2, 3, or 4 retail units consumed; cumulative probabil-ity�0.2 represents the 20thpercentile, 0.4�40thpercentile, etc. Reproducedwithpermission fromDavidCrowe, manager of consumer communicaitons for the New Zealand Food Safety Authority.
518 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from

risk of Parkinson disease and a slowerage-related cognitive decline.58
Effects of Caffeine in Children andAdolescents
Adolescent and child caffeine con-sumption should not exceed 100 mg/day and 2.5 mg/kg per day, respective-ly.7,38,63 For example, 8 oz of Red Bull(Fuschl am See, Austria) provides 77mg of caffeine, or 1.1 mg/kg for a 70-kgmale or 2.2 mg/kg for a 35-kg pre-teen.40 Whether the effects of caffeinein adults can be generalized to chil-dren remains unclear.63 In a study of 26boys and 26men, the same dose of caf-feine affected blood pressure simi-larly, but heart rate was significantlylowered in boys, whereas there was noeffect on heart rate in men.68 Boys alsoexhibited increased motor activity andspeech rates and decreased reactiontimes than did men.69
Caffeine can improve attention, butit also increases blood pressureand sleep disturbances in chil-dren.24,63,70,71 After cessation in chil-dren who habitually consume caf-feine, attention decreases andreaction time increases transient-ly.24,39 Similarly, reaction time hasbeen shown to decrease as the doseof caffeine in children increases.24
In a study of 9- to 11-year-olds withhabitual (mean intake: 109 mg/day)and low (mean intake: 12 mg/day)caffeine consumption given 50 mg ofcaffeine after overnight abstention,habitual caffeine users reportedwithdrawal-symptom (headache and
dulled cognition) reversal. The chil-dren who did not habitually consumecaffeine reported no markedchanges in cognitive performance,alertness, or headache.63
Caffeine may affect future food andbeverage preferences by acting on thedeveloping child’s brain reward-and-addiction center; this effect may begender specific.5 A study of 12- to 17-year-olds revealed that boys found caf-feinated soda more reinforcing thandid girls regardless of usual caffeineconsumption.72
Physiologic Effects of OtherIngredients in Energy Drinks andPotential Synergistic Effects
Popular media and case reports haveassociated adverse events withenergy-drink consumption (Appendix).Yet, few studies have examined thephysiologic effects of individual ingre-dients or potential synergistic effects;furthermore, results of experimentalstudies have been inconclusive and oc-casionally contradictory.24,25,59,73
Some studies of adults revealed im-proved mental alertness, reactiontimes, and concentration with energydrinks59,74; others revealed no improve-ment compared with caffeine or glu-cose alone.73 One study of 14 youngadults compared a complete energy-drink mixture to the glucose fraction,the caffeine fraction, and the herbalfraction.9,59 Although individual compo-nents did not enhance cognition, thecombined ingredients did.9,59 Caffeine
and taurine combined may synergisti-cally decrease heart rate initially; onestudy found that 70 minutes after con-sumption, heart rate returned to nor-mal and blood pressure increased.25,75
Taurine similarly produced a reflexbradycardia when injected into the ratcerebroventricular system.75 Anotherstudy of 15 healthy young adults in a7-day trial in which they consumed 500mL of an energy drink each day with160 mg of caffeine and 2000 mg of tau-rine, reported an average increase insystolic blood pressure of 9 to 10 mmHg and an average increased heartrate of 5 to 7 beats per minute 4 hoursafter consumption.25,38
Caffeine- and taurine-containing bev-erages increased left atrial contractil-ity in 13 athletes, thereby increasingleft ventricular end-diastolic volumeand stroke volume.76 The caffeine-onlygroup showed no changes in left ven-tricular function.76 Taurine may causethis increase in stroke volume by sup-pressing sympathetic nervous stimu-lation and influencing calcium storesin cardiac muscle.8 Results of humanand animal studies have suggestedthat long-term taurine exposure maycause hypoglycemia25 but a decreasedrisk of coronary heart disease.77 In an-imal experiments, taurine also hasshown anticonvulsive and epilepto-genic properties.25
Among 50 young adults who drank onesugar-free energy drink, hematologicand vascular effects included in-creased platelet aggregation and
TABLE 6 American Association of Poison Control Centers’ Data on Caffeine Toxicity, 2006–200847
Year Total callsto PCCs toReportCaffeineToxicity, n
Calls ThatReported
Caffeine Toxicityin Children�6 y
old, n(% of Total Calls)
Calls ThatReported
Caffeine Toxicityin 6- to-19-Year-Olds, n
(% of Total Calls)
Calls ThatReported
Caffeine Toxicityin Adults(�19 y old), n(% of Total Calls)
PatientsSubsequentlyTreated, n
(% of Total Calls)
Patients WithModeratelySevere
Symptoms, n(% of Total Calls)
Patients WithLife-ThreateningEffects, n
(% of Total Calls)
Deaths, n(% of Total Calls)
2008 4852 1208 (24.9) 1170 (24.1) 1090 (22.5) 1281 (26.4) 470 (9.7) 11 (0.2) 1 (0.02)2007 5448 1176 (21.6) 1328 (24.4) 1404 (25.8) 1561 (28.7) 544 (10.0) 16 (0.3) 1 (0.02)2006 5696 1247 (21.9) 1427 (25.1) 1427 (25.1) 1799 (31.6) 654 (11.5) 18 (0.3) 1 (0.02)
PCC indicates poison control center.
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 519 by on February 15, 2011 www.pediatrics.orgDownloaded from
mean arterial pressure and a de-crease in endothelial function.78 Guar-ana has antiplatelet aggregation prop-erties in vitro, but how it functionsphysiologically in energy drinks is un-known.79 A study of 20 healthy subjectsrevealed that caffeinated espressohad no effects on endothelial func-tion.80 Caffeine alone did not affectplatelet function.81
Ginseng, a common ingredient in manyenergy drinks, may lower blood glu-cose levels, but its actions in energydrinks are unclear.82
Potential Problems of EnergyDrinks Among Children andAdolescents
Cardiovascular Effects of EnergyDrinks on Children and Adolescents
High doses of caffeine may exacerbatecardiac conditions for which stimu-lants are contraindicated.17,18,84–86 Ofparticular concern are ion chan-nelopathies and hypertrophic cardio-myopathy, the most prevalent geneticcardiomyopathy in children and youngadults, because of the risk of hyperten-sion, syncope, arrhythmias, and sud-den death.11,86,87
Effects of Energy Drinks on Childrenand Adolescents With ADHD
ADHD occurs in 8% to 16% of US school-aged children and may be more preva-lent in children with heart disease.88,89
Some 2.5 million US children take stim-ulants for ADHD, which may increaseheart rate and blood pressure.89–91
Children with ADHD have higher ratesof substance abuse, including theabuse of caffeine, which blocks the A2Aadenosine receptors and thereby en-hances the dopamine effect at the D2dopamine receptor, similarly to theway guanfacine works for ADHD.92,93 Aswith the ADHD stimulants, the com-bined effects of energy drinks and an-tidepressants are unknown.94 For thesubpopulation with methylphenidate
cardiotoxicity, energy-drink use mayincrease cardiac events.95,96
Energy-Drink Use in Children andAdolescents With Eating Disorders
Children and adolescents with eatingdisorders, especially anorexia nervosa,may regularly consume high amounts ofcaffeine to counter caloric-restriction–associated fatigue, suppress appetite,and produce looser stools and some di-uresis.71–100 The risk of cardiac dys-rhythmias and intracardiac conduc-tion abnormalities from high-caffeineenergy drinks in children with eatingdisorders at higher risk for cardiac-related morbidity/mortality and electro-lyte abnormalities is disconcerting.91–99
Effects on Caloric Intake and Diabetes
Because obesity is epidemic, caloricincreases from energy-drink con-sumption become important. Addi-tional calories may increase bloodpressure, blood glucose levels, BMI,calcium deficiency, dental problems,depression, and low self-esteem.4,101,102
Sugar and caffeine may also synergis-tically increase postprandial hypergly-cemia, which is of concern for childrenwith diabetes.38,51,52
Effects on Bone Mineralization
Early adolescence is the time ofmaximalcalcium deposition in bone, and caffeineinterferes with intestinal calcium ab-sorption.103,104 It remains controversialwhether caffeine itself has the mostmarked effect on bone acquisition dur-ing adolescence or whether replace-ment ofmilk intake by caffeinated bever-ages is the leading contributor.103,104
Marketing of Energy Drinks
Youth-targeted marketing strategiesdate to 1987 when Red Bull was intro-duced in Austria.100 When it took 5years to get permission to export RedBull to Germany, rumors about its le-gality and dangerous effects helpedfuel its popularity, and it became
known as “speed in a can,” “liquid co-caine,” and a “legal drug.”100
Energy-drink marketing strategies in-clude sporting event and athlete spon-sorships, alcohol-alternative promo-tion, and product placement in media(including Facebook and video games)oriented to children, adolescents, andyoung adults.43,105 Newer alcoholic en-ergy drinks, the cans of which resem-ble the nonalcoholic counterparts, tar-get risk-taking youth.43
Contrasting with brand design is thevoluntary fine-print warning label onsome products, which state that theymay not be safe for children, thosewho are sensitive to caffeine, or forpregnant or nursing women.105–107
Regulation of Energy Drinks
The FDA imposes a limit of 71 mg ofcaffeine per 12 fl oz of soda.1,2 Energy-drink manufacturers may circumventthis limit by claiming that their drinksare “natural dietary supplements.”1,2
Thus, safety determinations of energydrinks are made solely by the manufac-turers, and there are no requirementsfor testing, warning labels, or restrictionagainst sales or consumption by mi-nors.1–3 In contrast, over-the-counterdedicated caffeine stimulants (eg, No-Doz [Novartis Consumer Health, Par-sippany, NJ]) must list the minimumage for purchase (12 years), adverseeffects, cautionary notes, recom-mended dose, and the total dailyrecommended dose of caffeine. In No-vember 2009, the FDA asked manufac-turers of alcoholic energy drinks toprove their safety.108 The US Senate isconsidering a bill that would requiresupplementmanufacturers to registerannually with the FDA and allow FDArecalls of supplements suspected ofbeing unsafe. Ingredients may also berestricted to those that have alreadybeen approved by the FDA.109
Regulatory controversies also extendinternationally (Table 7). When France
520 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from
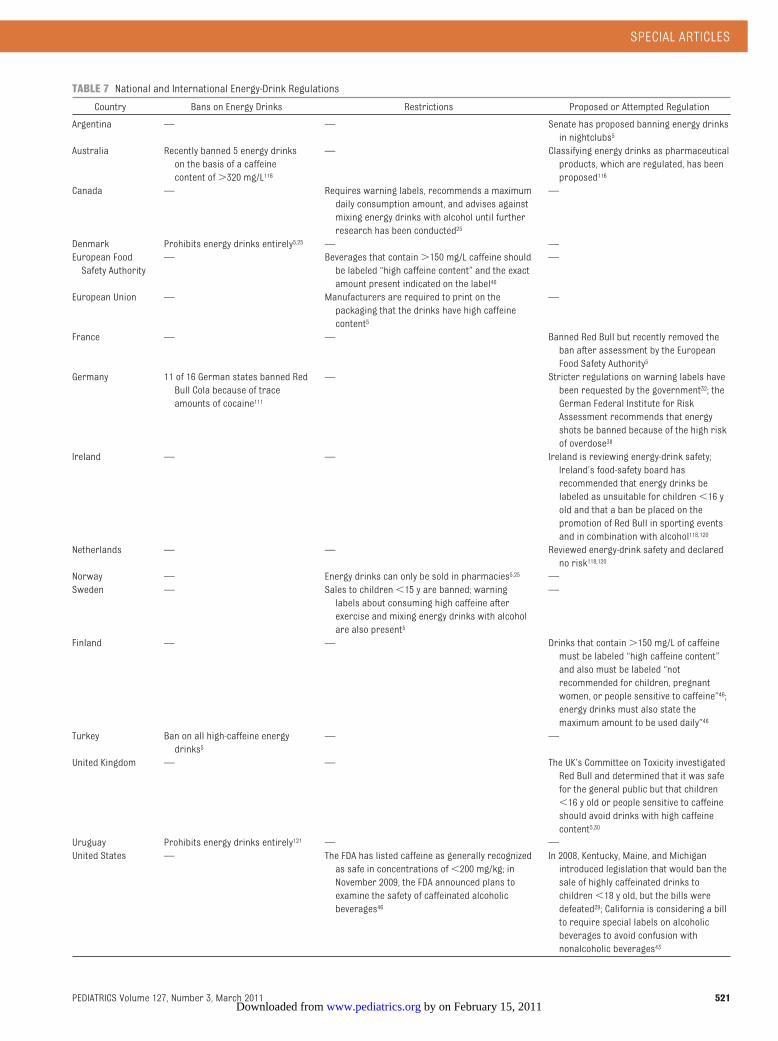
TABLE 7 National and International Energy-Drink Regulations
Country Bans on Energy Drinks Restrictions Proposed or Attempted Regulation
Argentina — — Senate has proposed banning energy drinksin nightclubs5
Australia Recently banned 5 energy drinkson the basis of a caffeinecontent of�320 mg/L116
— Classifying energy drinks as pharmaceuticalproducts, which are regulated, has beenproposed116
Canada — Requires warning labels, recommends a maximumdaily consumption amount, and advises againstmixing energy drinks with alcohol until furtherresearch has been conducted25
—
Denmark Prohibits energy drinks entirely5,25 — —European FoodSafety Authority
— Beverages that contain�150 mg/L caffeine shouldbe labeled “high caffeine content” and the exactamount present indicated on the label46
—
European Union — Manufacturers are required to print on thepackaging that the drinks have high caffeinecontent5
—
France — — Banned Red Bull but recently removed theban after assessment by the EuropeanFood Safety Authority5
Germany 11 of 16 German states banned RedBull Cola because of traceamounts of cocaine111
— Stricter regulations on warning labels havebeen requested by the government32; theGerman Federal Institute for RiskAssessment recommends that energyshots be banned because of the high riskof overdose38
Ireland — — Ireland is reviewing energy-drink safety;Ireland’s food-safety board hasrecommended that energy drinks belabeled as unsuitable for children�16 yold and that a ban be placed on thepromotion of Red Bull in sporting eventsand in combination with alcohol118,120
Netherlands — — Reviewed energy-drink safety and declaredno risk118,120
Norway — Energy drinks can only be sold in pharmacies5,25 —Sweden — Sales to children�15 y are banned; warning
labels about consuming high caffeine afterexercise and mixing energy drinks with alcoholare also present5
—
Finland — — Drinks that contain�150 mg/L of caffeinemust be labeled “high caffeine content”and also must be labeled “notrecommended for children, pregnantwomen, or people sensitive to caffeine”46;energy drinks must also state themaximum amount to be used daily”46
Turkey Ban on all high-caffeine energydrinks5
— —
United Kingdom — — The UK’s Committee on Toxicity investigatedRed Bull and determined that it was safefor the general public but that children�16 y old or people sensitive to caffeineshould avoid drinks with high caffeinecontent5,30
Uruguay Prohibits energy drinks entirely121 — —United States — The FDA has listed caffeine as generally recognized
as safe in concentrations of�200 mg/kg; inNovember 2009, the FDA announced plans toexamine the safety of caffeinated alcoholicbeverages46
In 2008, Kentucky, Maine, and Michiganintroduced legislation that would ban thesale of highly caffeinated drinks tochildren�18 y old, but the bills weredefeated29; California is considering a billto require special labels on alcoholicbeverages to avoid confusion withnonalcoholic beverages43
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 521 by on February 15, 2011 www.pediatrics.orgDownloaded from

banned Red Bull, the manufacturerschallenged the ban through the Euro-pean Commission, which determinedthat the caffeine and taurine concen-trations in energy drinks had not beenproven to be health risks and orderedFrance to lift the ban; the EuropeanFood Safety Authority has encouragedinternational data-pooling to better as-sess risks in children, adolescents,and young adults.33,110 In 2008, authori-ties in Germany, Hong Kong, and Tai-wan detected 0.13 �g per can of co-caine (average) in Red Bull Cola. RedBull manufacturers insisted that ac-tive cocaine was removed from thecoca leaf during processing and thatthe extract was used for flavoring.However, 11 of 16 German statesbanned the product.111
CONCLUSIONS
On the basis of this review, we con-clude that (1) energy drinks have notherapeutic benefit, and both theknown and unknown pharmacology ofvarious ingredients, combined with re-ports of toxicity, suggest that thesedrinks may put some children atrisk for serious adverse health ef-fects11,16,24,25,38; (2) typically, energydrinks contain high levels of caffeine,taurine, and guarana, which havestimulant properties and cardiac andhematologic activity,7,8,11 but manufac-turers claim that energy drinks are nu-tritional supplements, which shieldsthem from the caffeine limits imposedon sodas and the safety testing andlabeling required of pharmaceuti-cals7,8,11; (3) other ingredients vary, areunderstudied, and are not regulated;(4) youth-aimed marketing and risk-taking adolescent developmental ten-dencies combine to increase over-dose potential; (5) high consumptionis suggestedby self-report surveysbut is
underdocumented in children (deleteri-ous associations with energy-drinkconsumption have been reportedglobally in case reports and popularmedia7,8,11,25,31,38); and (6) interactionsbetween compounds, additive anddose-dependent effects, long-termconsequences, and dangers associ-ated with risky behavior in children re-main to be determined.5,14,25,38
EDUCATIONAL, RESEARCH, ANDREGULATORY RECOMMENDATIONS
In the short-term, pediatric healthcare providers need to be aware ofenergy-drink consumption by chil-dren, adolescents, and young adultsand the potentially dangerous conse-quences of inappropriate use.112 Dietand substance-use histories shouldinclude screening for episodic/chronicenergy-drink consumption, both aloneand with alcohol. Screening is espe-cially important for athletes, childrenwith high-risk behaviors, certainhealth conditions (eg, seizures, diabe-tes, hypertension, cardiac abnormali-ties), and children with behavioralchanges, anxiety, poor nutrition, orsleep disturbances.11
For most children, adolescents, andyoung adults, safe levels of consump-tion have not been established. Yet,heavy use may be harmful or interactwith medications and cause untowardadverse effects. Health care providersshould educate families and childrenat risk for the potential adverse effectsof energy drinks.
Routine high school athletic physicalsdo not identify everyone at risk forsudden cardiac death.11,113 Childrenwith cardiac conditions should becounseled regarding the risks ofcaffeine-containing products, includ-ing irregular heart rhythms, syncope,dysrhythmias, and sudden death.17,18,85
Community partners, including schools,athletic groups, and regulatory bodies,also need to promote risk aware-ness.113 The fourth edition of the“Preparticipation Physical Evaluation”monograph will feature a revampedhealth questionnaire focused on car-diac health problems that may be ex-acerbated by physical activity; thus,adding questions about stimulant use,including energy-drink consumption,becomes important.113
Long-term research objectives shouldaim to better define maximum safedoses, the effects of chronic use, andeffects in at-risk populations (eg,those with preexisting medical con-ditions, those who consume energydrinks during and after exercise, orthose who consume them in combi-nation with alcohol), and better doc-umentation and tracking of adversehealth effects.47 Unless research es-tablishes energy-drink safety in chil-dren and adolescents, regulation, aswith tobacco, alcohol, and prescrip-tion medications, is prudent.11
This approach is essential for reduc-ing morbidity and mortality, encourag-ing research, and supporting familiesof children and young adults at risk forenergy-drink overdose, behavioralchanges, and acute/chronic healthconsequences.
ACKNOWLEDGMENTSThisworkwas supported by National Insti-tutesofHealthgrantsHL072705, HL078522,HL053392, CA127642, CA068484, HD052104,AI50274, CA068484, HD052102, HL087708,HL079233, HL004537, HL087000, HL007188,HL094100, HL095127, and HD80002; HealthResources and Services Administrationgrant HCOF-C76HF15614; the Children’sCardiomyopathyFoundation;andtheWom-en’s Cancer Association.
522 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from

REFERENCES
1. Lee J. Energy drinks vs. sports drinks:know thy difference. Available at: http://speedendurance.com/2009/07/09/energy-drinks-vs-sports-drinks-know-thy-difference. Accessed January 17, 2011
2. McCarthy M. Overuse of energy drinksworries health pros. Available at: www.usatoday .com/sports/2009 -07 -01 -Drinks_N.htm. Accessed January 17,2011
3. US Food and Drug Administration. Over-view of dietary supplements. Available at:www.fda.gov/Food/DietarySupplements/ConsumerInformation/ucm110417.htm.Accessed January 17, 2011
4. Nitzke S, Tanumihardjo S, Salomon J,Coleman G. Energy drinks, sports drinks,and other functional/enhanced beveragesare often a waste of money. Available at:www.uwex.edu/ces/wnep/specialist/nfl/mmpdfs/0810.pdf#page�1. AccessedJanuary 17, 2011
5. Oddy WH, O’Sullivan TA. Energy drinks forchildren and adolescents, erring on theside of caution may reduce long termhealth risks. BMJ. 2009;339:b5268
6. Reissig CJ, Strain EC, Griffiths RR. Caffein-ated energy drinks: a growing problem.Drug Alcohol Depend. 2009;99(1–3):1–10
7. Babu KM, Church RJ, Lewander W. Energydrinks: the new eye-opener for adoles-cents. Clin Pediatr Emerg Med. 2008;9(1):35–42
8. Clauson KA, Shields KM, McQueen CE,Persad N. Safety issues associated withcommercially available energy drinks. JAm Pharm Assoc (Wash DC). 2008;48(3):e55–e63; quiz e64–e67
9. Malinauskas BM, Aeby VG, Overton RF,Carpenter-Aeby T, Barber-Heidal K. A sur-vey of energy drink consumption patternsamong college students. Nutr J. 2007;6:35. Available at: www.nutritionj.com/content/6/1/35. Accessed January 17,2011
10. Press Office. New report predicts energydrink sales in the U.S. to exceed $9 billionby 2011 [press release]. Available at: www.reportbuyer.com/press/new-report-predicts-energy-drink-sales-in-the-us-to-exceed-9-bi l l ion-by-2011. AccessedJanuary 17, 2011
11. Lipshultz S. High risk: Ban energy drinksfrom schools.Miami Herald. April 20, 2008:4L, L4
12. Broderick P, Benjamin AB. Caffeine andpsychiatric symptoms: a review. J OklaState Med Assoc. 2004;97(12):538–542
13. Hedges DW, Woon FL, Hoopes SP. Caffeine-induced psychosis. CNS Spectr. 2009;14(3):127–129
14. Heneman K, Zidenberg-Cherr S. Somefacts about energy drinks. Available at:http://nutrition.ucdavis.edu/content/infosheets/EnergyDrinks.pdf. AccessedJanuary 17, 2011
15. Brecher EJ. Study: caffeine in sodas riskyfor black kids. Miami Herald. May 18,2004:7E
16. Cohen H. Dangerous jolt: energy drink dan-gers for children. Miami Herald. April 1,2008:E10, 10E
17. Frassica JJ, Orav EJ, Walsh EP, LipshultzSE. Arrhythmias in children prenatally ex-posed to cocaine. Arch Pediatr AdolescMed. 1994;148(11):1163–1169
18. Lipshultz SE, Frassica JJ, Orav EJ. Cardio-vascular abnormalities in infants prena-tally exposed to cocaine. J Pediatr. 1991;118(1):44–51
19. Lipshultz SE. Ventricular dysfunction clini-cal research in infants, children and ado-lescents. Prog Pediatr Cardiol. 2000;12(1):1–28
20. Lipshultz SE, Wilkinson JD, Messiah SE,Miller TL. Clinical research directions inpediatric cardiology. Curr Opin Pediatr.2009;21(5):585–593
21. Lipshultz SE. Realizing optimal care forchildren with cardiovascular disease:funding challenges and research ap-proaches. Prog Pediatr Cardiol. 2005;20(1):71–90
22. Mone SM, Gillman MW, Miller TL, HermanEH, Lipshultz SE. Effects of environmentalexposures on the cardiovascular system:prenatal period through adolescence. Pe-diatrics. 2004;113(4 suppl):1058–1069
23. Chrissos J. Cold medicines taboo for kidsunder 4: further restricting the use of coldmedicines for young children, drug com-panies now say they shouldn’t be used inchildren younger than 4.Miami Herald. Oc-tober 8, 2008: Living-Health
24. Temple JL. Caffeine use in children: whatwe know, what we have left to learn, andwhy we should worry. Neurosci BiobehavRev. 2009;33(6):793–806
25. Federal Institute for Risk Assessment. Newhuman data on the assessment of energydrinks. Available at: www.bfr.bund.de/cm/245/new_human_data_on_the_assessment_of_energy_drinks.pdf. Ac-cessed January 17, 2011
26. Health Canada. Energy drinks safety andhealth effects. Available at : www.
enotalone.com/article/10272.html. Ac-cessed January 17, 2011
27. Iyadurai SJ, Chung SS. New-onset seizuresin adults: possible association with con-sumption of popular energy drinks. Epi-lepsy Behav. 2007;10(3):504–508
28. Berger AJ, Alford K. Cardiac arrest in ayoung man following excess consumptionof caffeinated “energy drinks.”Med J Aust.2009;190(1):41–43
29. Cannon ME, Cooke CT, McCarthy JS.Caffeine-induced cardiac arrhythmia: anunrecognised danger of healthfood prod-ucts. Med J Aust. 2001;174(10):520–521
30. Bestervelt L. Raising the red flag on someenergy drinks. Available at: www.nsf.org/media/enews/documents/energy_drinks.pdf. Accessed January 17, 2011
31. Nordqvist C. French ban on Red Bull(drink) upheld by European Court. Avail-able at: www.medicalnewstoday.com/articles/5753.php. Accessed January 17,2011
32. Parikh RK. Red alert on energy drinks. LosAngeles Times. September 1, 2008: Health
33. Starling S. Energy drinks safety ques-tioned by German agency. Available at:www.beveragedaily.com/content/view/print/166290. Accessed January 17, 2011
34. High school students warned about en-ergy drink: Smokey Hill student hospital-ized after drinking SPIKE. Available at:www.thedenverchannel .com/news/11070908/detail.html. Accessed January17, 2011
35. Quinones D. Sidelined college footballfreshman plans medical path. Miami Her-ald. July 30, 2009: Sports
36. National Federation of State High SchoolAssociations, Sports Medicine AdvisoryCommittee. Position statement and rec-ommendations for the use of energydrinks by young athletes. Available at:www.nfhs.org/search.aspx?searchtext�Energy%20Drinks. Accessed January 17,2011
37. National Federation of State High SchoolAssociations, Sports Medicine AdvisoryCommittee. Minimize the risk for dehydra-tion and heat illness. Available at: www.nfhs.org/search.aspx?searchtext�Energy%20Drinks. Accessed January 17,2011
38. Federal Institute for Risk Assessment.Health risks of excessive energy shot in-take. December 2, 2009. Available at: www.bfr.bund.de/cm/245/health_risks_of_
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 523 by on February 15, 2011 www.pediatrics.orgDownloaded from

excessive_energy_shot_intake.pdf.Accessed January 17, 2011
39. O’Connor E. A sip into dangerous territory.Monit Psychol. 2001;32(6). Available at:www.apa.org/monitor/jun01/dangersip.aspx. Accessed January 17, 2011
40. Pollak CP, Bright D. Caffeine consumptionand weekly sleep patterns in US seventh-,eighth-, and ninth-graders. Pediatrics.2003;111(1):42–46
41. Bernstein GA, Carroll ME, Thuras PD, Cos-grove KP, Roth ME. Caffeine dependence inteenagers. Drug Alcohol Depend. 2002;66(1):1–6
42. Strain EC, Mumford GK, Silverman K, Grif-fiths RR. Caffeine dependence syndrome:evidence from case histories and experi-mental evaluations. JAMA. 1994;272(13):1043–1048
43. Simon M, Mosher J. Alcohol, energydrinks, and youth: a dangerous mix. Avail-ab le at : www.marin inst i tute .org/alcopops/resources/EnergyDrinkReport.pdf. Accessed January 17, 2011
44. Viell B, Grabner L, Fruchel G, Boczek P. Newcaffeinated beverages: a pilot survey of fa-miliarity and consumption by adolescentsin north-Rhine Westphalia and Berlin andconsiderations of consumer protection [inGerman]. Z Ernahrungswiss. 1996;35(4):378–386
45. Miller KE. Wired: energy drinks, jock iden-tity, masculine norms, and risk taking. JAm Coll Health. 2008;56(5):481–489
46. Thomson B, Schiess S. Risk profile: caf-feine in energy drinks and energy shots.Available at: www.nzfsa.govt.nz/science/r isk -profi les/ fw10002 -ca f fe ine - in -beverages-risk-profile.pdf. Accessed Jan-uary 17, 2011
47. Bronstein AC, Spyker DA, Cantilena LR Jr,Green JL, Rumack BH, Heard SE; AmericanAssociation of Poison Control Centers.2007 Annual Report of the American Asso-ciation of Poison Control Centers’ NationalPoison Data System (NPDS): 25th AnnualReport. Clin Toxicol (Phila). 2008;46(10):927–1057
48. Holmgren P, Norden-Pettersson L, AhlnerJ. Caffeine fatalities: four case reports. Fo-rensic Sci Int. 2004;139(1):71–73
49. Greenwood MRC, Oria M. Use of dietarysupplements by military personnel. Avail-able at: www.nap.edu/catalog/12095.html.Accessed January 17, 2011
50. Connolly S, Kingsbury TJ. Caffeine modu-lates CREB-dependent gene expression indeveloping cortical neurons. Biochem Bio-phys Res Commun. 2010;397(2):152–156
51. Dworzanski W, Opielak G, Burdan F. Side
effects of caffeine [in Polish]. Pol MerkurLekarski. 2009;27(161):357–361
52. Kolnes AJ, Ingvaldsen A, Bolling A, et al.Caffeine and theophylline block insulin-stimulated glucose uptake and PKB phos-phorylation in rat skeletal muscles. ActaPhysiol (Oxf). 2010;200(1):65–74
53. Del Coso J, Estevez E, Mora-Rodriguez R.Caffeine during exercise in the heat: ther-moregulation and fluid-electrolyte bal-ance. Med Sci Sports Exerc. 2009;41(1):164–173
54. Armstrong LE. Caffeine, body fluid-electrolyte balance, and exercise perfor-mance. Int J Sport Nutr Exerc Metab. 2002;12(2):189–206
55. Armstrong LE, Pumerantz AC, Roti MW, etal. Fluid, electrolyte, and renal indices ofhydration during 11 days of controlled caf-feine consumption. Int J Sport Nutr ExercMetab. 2005;15(3):252–265
56. Chapman RF, Mickleborough TD. The ef-fects of caffeine on ventilation and pulmo-nary function during exercise: an often-overlooked response. Phys Sportsmed.2009;37(4):97–103
57. Rogers PJ, Dernoncourt C. Regular caf-feine consumption: a balance of adverseand beneficial effects for mood and psy-chomotor performance. Pharmacol Bio-chem Behav. 1998;59(4):1039–1045
58. Rogers PJ. Caffeine, mood andmental per-formance in everyday life. Br Nutr FoundNutr Bull. 2007;32(suppl l):84–89
59. Scholey AB, Kennedy DO. Cognitive andphysiological effects of an “energy drink”:an evaluation of the whole drink and ofglucose, caffeine and herbal flavouringfractions. Psychopharmacology (Berl).2004;176(3–4):320–330
60. Lipshultz SE. Vote for children’s health.Mi-ami Herald. October 25, 2008; Opinion-Other Views-Healthcare
61. Whelton PK, He J, Appel LJ, et al; NationalHigh Blood Pressure Education ProgramCoordinating Committee. Primary preven-tion of hypertension: clinical and publichealth advisory from the national highblood pressure education program. JAMA.2002;288(15):1882–1888
62. Burke LM. Caffeine and sports perfor-mance. Appl Physiol Nutr Metab. 2008;33(6):1319–1334
63. Heatherley SV, Hancock KM, Rogers PJ.Psychostimulant and other effects of caf-feine in 9- to 11-year-old children. J ChildPsychol Psychiatry. 2006;47(2):135–142
64. Griffiths RR, Woodson PP. Caffeine physicaldependence: a review of human and labo-
ratory animal studies. Psychopharmacol-ogy (Berl). 1988;94(4):437–451
65. Steinke L, Lanfear DE, Dhanapal V, KalusJS. Effect of “energy drink” consumptionon hemodynamic and electrocardio-graphic parameters in healthy youngadults. Ann Pharmacother. 2009;43(4):596–602
66. Hinds TS, West WL, Knight EM, Harland BF.The effect of caffeine on pregnancy out-come variables. Nutr Rev. 1996;54(7):203–207
67. Dlugosz L, Belanger K, Hellenbrand K, Hol-ford TR, Leaderer B, Bracken MB. Maternalcaffeine consumption and spontaneousabortion: a prospective cohort study. Epi-demiology. 1996;7(3):250–255
68. Turley KR, Desisso T, Gerst JW. Effects ofcaffeine on physiological responses toexercise: boys versus men. Pediatr ExercSci. 2007;19(4):481–492
69. Rapoport JL, Jensvold M, Elkins R, et al.Behavioral and cognitive effects of caf-feine in boys and adult males. J Nerv MentDis. 1981;169(11):726–732
70. Bancalari E. Caffeine for apnea of pre-maturity. N Engl J Med. 2006;354(20):2179–2181
71. Bancalari E. Caffeine reduces the rate ofbronchopulmonary dysplasia in very lowbirth weight infants. J Pediatr. 2006;149(5):727–728
72. Temple JL, Bulkley AM, Briatico L, DeweyAM. Sex differences in reinforcing value ofcaffeinated beverages in adolescents. Be-hav Pharmacol. 2009;20(8):731–741
73. Smit HJ, Cotton JR, Hughes SC, Rogers PJ.Mood and cognitive performance effectsof “energy” drink constituents: caffeine,glucose and carbonation. Nutr Neurosci.2004;7(3):127–139
74. Warburton DM, Bersellini E, Sweeney E. Anevaluation of a caffeinated taurine drinkon mood, memory and information pro-cessing in healthy volunteers without caf-feine abstinence. Psychopharmacology(Berl). 2001;158(3):322–328
75. Terlizzi R, Rocchi C, Serra M, Solieri L, Cor-telli P. Reversible postural tachycardiasyndrome due to inadvertent overuse ofred bull. Clin Auton Res. 2008;18(4):221–223
76. Baum M, Weiss M. The influence of a tau-rine containing drink on cardiac parame-ters before and after exercise measuredby echocardiography. Amino Acids. 2001;20(1):75–82
77. Wójcik OP, Koenig KL, Zeleniuch-JacquotteA, CostaM, Chen Y. The potential protective
524 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from

effects of taurine on coronary heart dis-ease. Atherosclerosis. 2010;208(1):19–25
78. Worthley MI, Prabhu A, De Sciscio P,Schultz C, Sanders P, Willoughby SR. Detri-mental effects of energy drink consump-tion on platelet and endothelial function.Am J Med. 2010;123(2):184–187
79. Subbiah MT, Yunker R. Studies on the na-ture of anti-platelet aggregatory factors inthe seeds of the Amazonian herb guarana(Paullinia cupana). Int J Vitam Nutr Res.2008;78(2):96–101
80. Buscemi S, Verga S, Batsis JA, et al. Acuteeffects of coffee on endothelial function inhealthy subjects. Eur J Clin Nutr. 2010;64(5):483–489
81. Natella F, Nardini M, Belelli F, et al. Effect ofcoffee drinking on platelets: inhibition ofaggregation and phenols incorporation.Br J Nutr. 2008;100(6):1276–1282
82. Hui H, Tang G, Go VL. Hypoglycemic herbsand their action mechanisms. Chin Med.2009;4:11
83. Dangerous supplements. Consum Rep.September 2010:16–20
84. Lipshultz SE, Wong JC, Lipsitz SR, et al. Fre-quency of clinically unsuspected myocar-dial injury at a children’s hospital. AmHeart J. 2006;151(4):916–922
85. Sokol KC, Armstrong FD, Rosenkranz ER, etal. Ethical issues in children withcardiomyopathy: making sense of ethicalchallenges in the clinical setting. Prog Pe-diatr Cardiol. 2007;23(1):81–87
86. Lipshultz SE, Sleeper LA, Towbin JA, et al.The incidence of pediatric cardiomyopathyin two regions of the united states. N Engl JMed. 2003;348(17):1647–1655
87. Colan SD, Lipshultz SE, Lowe AM, et al. Epi-demiology and cause-specific outcome ofhypertrophic cardiomyopathy in children:findings from the pediatric cardiomyopa-thy registry. Circulation. 2007;115(6):773–781
88. Barbaresi WJ, Katusic SK, Colligan RC, et al.How common is attent ion-deficit/hyperactivity disorder? Incidence in apopulation-based birth cohort in Roches-ter, Minn. Arch Pediatr Adolesc Med. 2002;156(3):217–224
89. Vetter VL, Elia J, Erickson C, et al; AmericanHeart Association, Council on Cardiovas-cular Disease in the Young Congenital Car-diac Defects Committee; American HeartAssociation, Council on CardiovascularNursing. Cardiovascular monitoring ofchildren and adolescents with heart dis-ease receiving stimulant drugs: a scien-tific statement from the American HeartAssociation Council on Cardiovascular Dis-
ease in the Young congenital cardiac de-fects committee and the council on cardio-vascular nursing [published correctionappears in Circulation. 2009;120(7):e55– e59]. Circulation. 2008;117(18):2407–2423
90. Wilens TE, Gignac M, Swezey A, MonuteauxMC, Biederman J. Characteristics of ado-lescents and young adults with ADHD whodivert or misuse their prescribed medica-tions. J Am Acad Child Adolesc Psychiatry.2006;45(4):408–414
91. Wilens TE, Prince JB, Spencer TJ, Bieder-man J. Stimulants and sudden death: whatis a physician to do? Pediatrics. 2006;118(3):1215–1219
92. Biederman J, Wilens T, Mick E, Spencer T,Faraone SV . Pharmacotherapy ofattention-deficit/hyperactivity disorder re-duces risk for substance use disorder. Pe-diatrics. 1999;104(2). Available at: www.pediatrics.org/cgi/content/full/104/2/e20.Accessed January 17, 2011
93. Fredholm BB, Svenningsson P. Striataladenosine A2A receptors: where are they?What do they do? Trends Pharmacol Sci.1998;19(2):46–48
94. Wilens TE, Biederman J, Baldessarini RJ, etal. Cardiovascular effects of therapeuticdoses of tricyclic antidepressants in chil-dren and adolescents. J Am Acad ChildAdo lesc Psych ia try . 1996 ;35(11) :1491–1501
95. Dadfarmay S, Dixon J. A case of acute car-diomyopathy and pericarditis associatedwith methylphenidate. Cardiovasc Toxicol.2009;9(1):49–52
96. Take G, BahceliogluM, OktemH, et al. Dose-dependent immunohistochemical and un-trastructural changes after oral methyl-phenidate administration in rat hearttissue. Anat Histol Embryol. 2008;37(4):303–308
97. Krahn DD, Hasse S, Ray A, Gosnell B,Drewnowski A. Caffeine consumption inpatients with eating disorders. Hosp Com-munity Psychiatry. 1991;42(3):313–315
98. Stock SL, Goldberg E, Corbett S, KatzmanDK. Substance use in female adolescentswith eating disorders. J Adolesc Health.2002;31(2):176–182
99. Striegel-Moore RH, Franko DL, ThompsonD, Barton B, Schreiber GB, Daniels SR. Caf-feine intake in eating disorders. Int J EatDisord. 2006;39(2):162–165
100. Popkin B. We are what we drink. InTheWorld Is Fat: The Fads, Trends, Policies,and Products That Are Fattening the Hu-man Race. New York, NY: Penguin Group;2002:43–65
101. Moreno MA, Furtner F, Frederick PR. Sug-ary drinks and childhood obesity. Arch Pe-diatr Adolesc Med. 2009;163(4):400
102. National Center for Chronic Disease Pre-vention and Health Promotion. Obesity:halting the epidemic bymaking health eas-ier. Available at: www.cdc.gov/nccdphp/publications/AAG/pdf/obesity.pdf. Ac-cessed January 17, 2011
103. Heaney RP. Effects of caffeine on bone andthe calcium economy. Food Chem Toxicol.2002;40(9):1263–1270
104. Lloyd T, Rollings NJ, Kieselhorst K, Eggli DF,Mauger E. Dietary caffeine intake is notcorrelated with adolescent bone gain. JAm Coll Nutr. 1998;17(5):454–457
105. Hein K. A bull’s market: the marketing ofRed Bull energy drink. Available at: http://findarticles.com/p/articles/mi_m0BDW/is_22_42/ai_75286777/?tag�content%3Bcol1. Accessed January 17, 2011
106. Thomsen SR, Fulton K. Adolescents’ atten-tion to responsibility messages in maga-zine alcohol advertisements: an eye-tracking approach. J Adolesc Health. 2007;41(1):27–34
107. Fischer PM, Richards JW Jr, Berman EJ,Krugman DM. Recall and eye trackingstudy of adolescents viewing tobacco ad-vertisements. JAMA. 1989;261(1):84–89
108. Weise E. Petition calls for FDA to regulateenergy drinks. USA Today. October 22,2008: News, Health & Behavior
109. Our view on pills and potions: do you reallyknow what’s in that dietary supplement?Available at: www.usatoday.com/news/opinion/editorials/2010-06-07-editorial07_ST_N.htm?loc�interstitialskip. Accessed January17, 2011
110. European Food Safety Authority. EFSAadopts opinion on two ingredients com-monly used in some energy drinks [pressrelease]. Available at: www.efsa.europa.eu/en/press/news/ans090212.htm. Ac-cessed January 17, 2011
111. Red Bull pulled from shelves in Hong Kong.Available at: http://content.usatoday.com/communities/ondeadline/post/2009/06/67549503/1. Accessed October 27, 2009
112. Anderson BL, Juliano LM, Schulkin J. Caf-feine’s implications for women’s healthand survey of obstetrician-gynecologists’caffeine knowledge and assessment prac-tices. J Womens Health (Larchmt). 2009;18(9):1457–1466
113. Pepine CJ. Panel endorses preparticipa-tion sports physicals for every child. Car-diol Today. 2010:13(6). Available at: www.cardiologytoday.com/print.aspx?rid�65042. Accessed January 17, 2011
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 525 by on February 15, 2011 www.pediatrics.orgDownloaded from

114. Cerimele JM, Stern AP, Jutras-Aswad D.Psychosis following excessive ingestion ofenergy drinks in a patient with schizophre-nia. Am J Psychiatry. 2010;167(3):353
115. Convertino VA, Armstrong LE, Coyle EF, et al.American college of sports medicine positionstand: exercise andfluid replacement.MedSciSports Exerc. 1996;28(1):i–vii
116. Bruce B. Energy drinks banned over caf-feine levels in Australia. Available at: www.foodbev .com/news/energy -dr inks -banned-over-caffeine-levels-in-australia.Accessed January 17, 2011
117. Neuman W. “Energy shots” stimulatepower drink sales. Available at: www.nytimes.com/2009/07/11/business/11energy.html. Accessed January 17,2011
118. Derbyshire D. Energy drinks “should havecaffeine health warning on cans.” Mail-Online. Available at: www.dailymail.co.uk/news/article-1060705/Energy-drinks-caffeine-health-warning-cans.html.Accessed January 17, 2011
119. Energy drinks’ caffeine buzz can land theunwary in the ER. REDORBIT News. 2005.
Available at: www.redorbit.com/news/display/?id�833954. Accessed January17, 2011
120. Nutra Ingredients.com. Ireland to reviewsafety of energy drinks. Available at: www.nutraingredients.com/Regulation/Ireland-to-review-safety-of-energy-drinks. Ac-cessed January 17, 2011
121. Red Bull banned in Dutch schools. DutchDa i l y N ews . A v a i l a b l e a t : www .dutchdailynews.com/red-bull-banned-in-dutch-schools. Accessed January 17,2011
526 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from
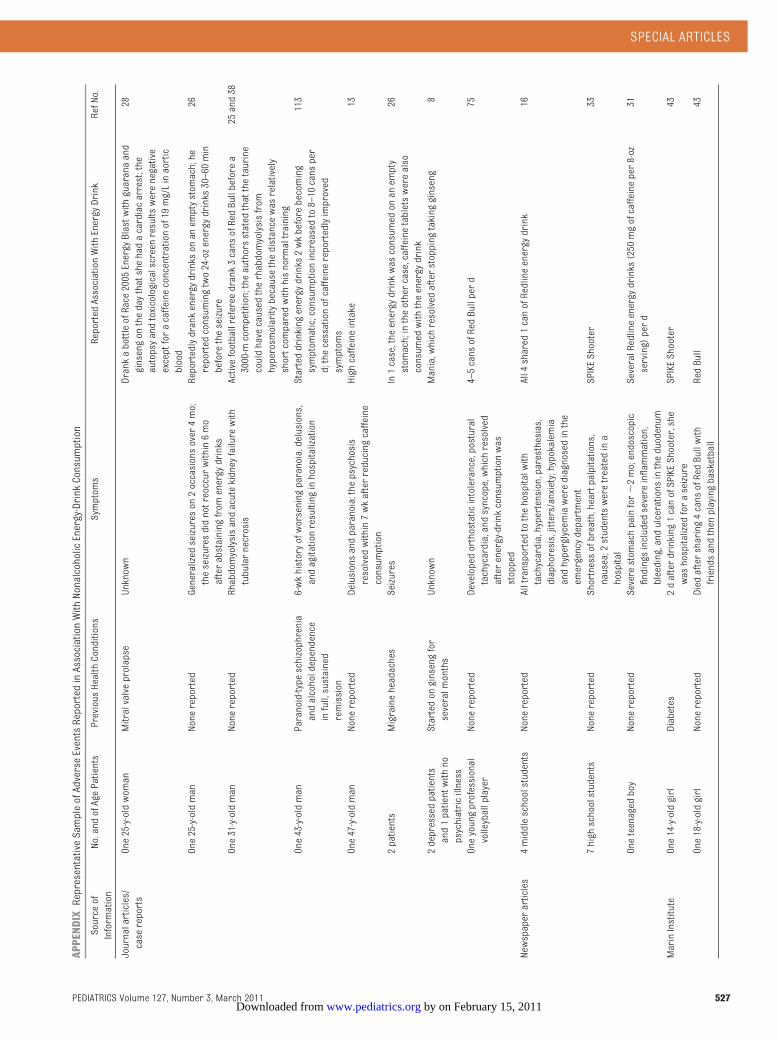
APPENDIXRepresentativeSampleofAdverseEventsReportedinAssociationWithNonalcoholicEnergy-DrinkConsumption
Sourceof
Information
No.andofAgePatients
PreviousHealthConditions
Symptoms
ReportedAssociationWithEnergyDrink
RefNo.
Journalarticles/
casereports
One25-y-oldwoman
Mitralvalveprolapse
Unknown
DrankabottleofRace2005EnergyBlastwithguaranaand
ginsengonthedaythatshehadacardiacarrest;the
autopsyandtoxicologicalscreenresultswerenegative
exceptforacaffeineconcentrationof19mg/Linaortic
blood
28
One25-y-oldman
Nonereported
Generalizedseizureson2occasionsover4mo;
theseizuresdidnotreoccurwithin6mo
afterabstainingfromenergydrinks
Reportedlydrankenergydrinksonanemptystomach;he
reportedconsumingtwo24-ozenergydrinks30–60min
beforetheseizure
26
One31-y-oldman
Nonereported
Rhabdomyolysisandacutekidneyfailurewith
tubularnecrosis
Activefootballrefereedrank3cansofRedBullbeforea
3000-mcompetition;theauthorsstatedthatthetaurine
couldhavecausedtherhabdomyolysisfrom
hyperosmolaritybecausethedistancewasrelatively
shortcomparedwithhisnormaltraining
25and38
One43-y-oldman
Paranoid-typeschizophrenia
andalcoholdependence
infull,sustained
remission
6-wkhistoryofworseningparanoia,delusions,
andagitationresultinginhospitalization
Starteddrinkingenergydrinks2wkbeforebecoming
symptomatic;consumptionincreasedto8–10cansper
d;thecessationofcaffeinereportedlyimproved
symptoms
113
One47-y-oldman
Nonereported
Delusionsandparanoia;thepsychosis
resolvedwithin7wkafterreducingcaffeine
consumption
Highcaffeineintake
13
2patients
Migraineheadaches
Seizures
In1case,theenergydrinkwasconsumedonanempty
stomach;intheothercase,caffeinetabletswerealso
consumedwiththeenergydrink
26
2depressedpatients
and1patientwithno
psychiatricillness
Startedonginsengfor
severalmonths
Unknown
Mania,whichresolvedafterstoppingtakingginseng
8
Oneyoungprofessional
volleyballplayer
Nonereported
Developedorthostaticintolerance,postural
tachycardia,andsyncope,whichresolved
afterenergy-drinkconsumptionwas
stopped
4–5cansofRedBullperd
75
Newspaperarticles
4middleschoolstudents
Nonereported
Alltransportedtothehospitalwith
tachycardia,hypertension,paresthesias,
diaphoresis,jitters/anxiety;hypokalemia
andhyperglycemiawerediagnosedinthe
emergencydepartment
All4shared1canofRedlineenergydrink
16
7highschoolstudents
Nonereported
Shortnessofbreath,heartpalpitations,
nausea;2studentsweretreatedina
hospital
SPIKEShooter
33
Oneteenagedboy
Nonereported
Severestomachpainfor
�2mo;endoscopic
findingsincludedsevereinflammation,
bleeding,andulcerationsintheduodenum
SeveralRedlineenergydrinks(250mgofcaffeineper8-oz
serving)perd
31
MarinInstitute
One14-y-oldgirl
Diabetes
2dafterdrinking1canofSPIKEShooter,she
washospitalizedforaseizure
SPIKEShooter
43
One18-y-oldgirl
Nonereported
Diedaftersharing4cansofRedBullwith
friendsandthenplayingbasketball
RedBull
43
SPECIAL ARTICLES
PEDIATRICS Volume 127, Number 3, March 2011 527 by on February 15, 2011 www.pediatrics.orgDownloaded from
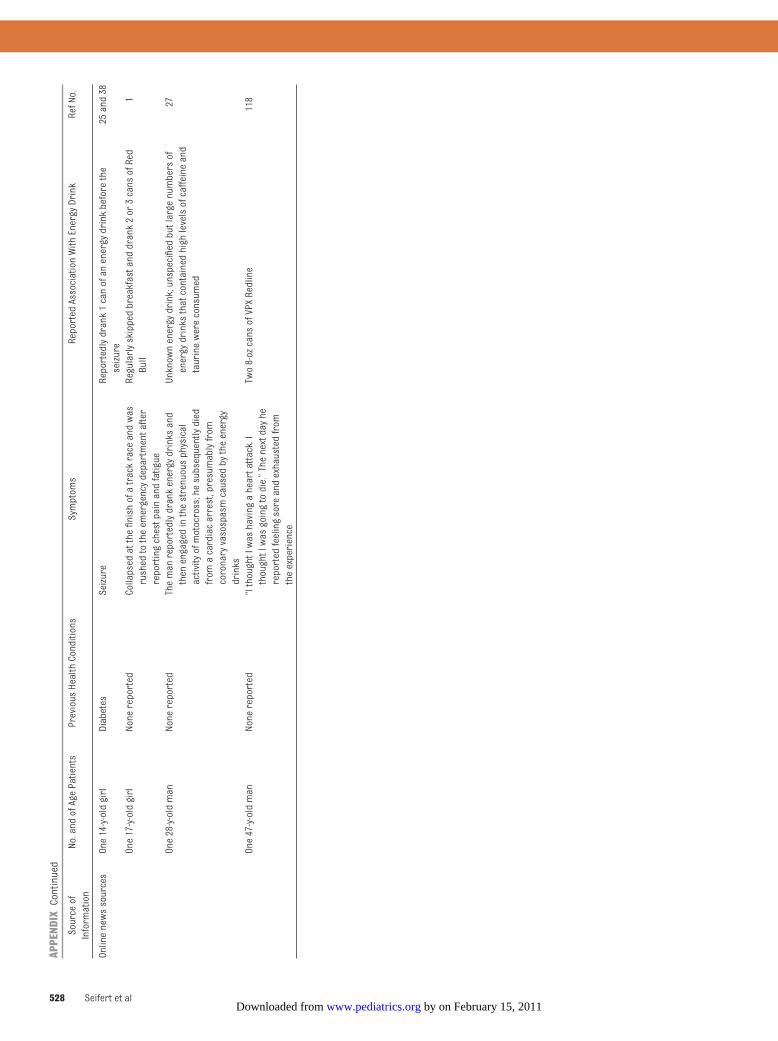
APPENDIXContinued
Sourceof
Information
No.andofAgePatients
PreviousHealthConditions
Symptoms
ReportedAssociationWithEnergyDrink
RefNo.
Onlinenewssources
One14-y-oldgirl
Diabetes
Seizure
Reportedlydrank1canofanenergydrinkbeforethe
seizure
25and38
One17-y-oldgirl
Nonereported
Collapsedatthefinishofatrackraceandwas
rushedtotheemergencydepartmentafter
reportingchestpainandfatigue
Regularlyskippedbreakfastanddrank2or3cansofRed
Bull
1
One28-y-oldman
Nonereported
Themanreportedlydrankenergydrinksand
thenengagedinthestrenuousphysical
activityofmotocross;hesubsequentlydied
fromacardiacarrest,presumablyfrom
coronaryvasospasmcausedbytheenergy
drinks
Unknownenergydrink;unspecifiedbutlargenumbersof
energydrinksthatcontainedhighlevelsofcaffeineand
taurinewereconsumed
27
One47-y-oldman
Nonereported
“IthoughtIwashavingaheartattack.I
thoughtIwasgoingtodie.”Thenextdayhe
reportedfeelingsoreandexhaustedfrom
theexperience
Two8-ozcansofVPXRedline
118
528 Seifert et al by on February 15, 2011 www.pediatrics.orgDownloaded from

DOI: 10.1542/peds.2009-3592 published online Feb 14, 2011; Pediatrics
Sara M. Seifert, Judith L. Schaechter, Eugene R. Hershorin and Steven E. Lipshultz Health Effects of Energy Drinks on Children, Adolescents, and Young Adults
& ServicesUpdated Information
http://www.pediatrics.orgincluding high-resolution figures, can be found at:
Permissions & Licensing
http://www.pediatrics.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://www.pediatrics.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by on February 15, 2011 www.pediatrics.orgDownloaded from





























