-
8/3/2019 Health Economics- Lecture Ch09
1/26
Consumer Choice and Demand
Dr. Katherine Sauer Metropolitan State College of Denver
Health Economics
-
8/3/2019 Health Economics- Lecture Ch09
2/26
O verview:
I. Consumer TheoryII. Issues in Measuring Health Care DemandIII.
Empirical Measurements of Demand ElasticitiesIV. Impacts of
Insurance on Aggregate ExpendituresV. O ther Variables Affecting
Demand
-
8/3/2019 Health Economics- Lecture Ch09
3/26
I. Consumer Theory
A. PreferencesConsumers have different preferences for medical
carewhen they are sick vs when they are well.
-
8/3/2019 Health Economics- Lecture Ch09
4/26
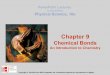
B . Deriving the Demand Curve
Initially, the price of an office visit is p1.
At that price and for a
given income andgiven set of
preferences, theconsumer chooses V1office visits.
-
8/3/2019 Health Economics- Lecture Ch09
5/26
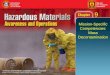
W hen the price falls toP2, the budget lineshifts out along the
Vaxis.
The optimal bundle isnow V2 visits.
W hen the price falls toP3, the optimal bundleis V3.
-
8/3/2019 Health Economics- Lecture Ch09
6/26
W hen incomeincreases, the entire
budget line shifts out.
The optimal number of visits is V3.
-
8/3/2019 Health Economics- Lecture Ch09
7/26
W e can use the price-quantity information to plot thisconsumers
demand curve:
W hen incomeincreased, the demandcurve shifted out.
W hat else could shiftdemand?
-
8/3/2019 Health Economics- Lecture Ch09
8/26
II. Issues in measuring health care demand
In this section, the focus is on variables of interest toscience
and public policy.
-
8/3/2019 Health Economics- Lecture Ch09
9/26
A. Individual and Market Demand Functions
Demand function for physician visits, V:V =f(P, r, t, P 0 , Y,
HS, AGE, ED,)
where P is price per visitr is the patients coinsurance ratet is
a time price
P 0 is the price of other goods
Y is a measure of income HS is the patients health status AGE
and ED reflect other need and taste factors
-
8/3/2019 Health Economics- Lecture Ch09
10/26
B . Measurement
Investigators often measure the quantity of services indollar
expenditures.
O ne problem is that expenditures reflect a complexcombination
of price of care, quantities of care, andqualities of care.
Alternative measures include quantity of visits, patientdays, or
cases treated, yet these do not necessarilymeasure the intensity of
care.
-
8/3/2019 Health Economics- Lecture Ch09
11/26
A related problem is to define the price of services.
Because of the prevalence of health insurance,most patients do
not pay the full price for their
treatments.
-
8/3/2019 Health Economics- Lecture Ch09
12/26
C. Differences in Study Populations
Different researchers, naturally, use different samplesor
populations.
Elasticities will differ between populations and evenwithin
populations at different points in time.
For example, many health economists believe thatincome
elasticities for health care have become smaller over the years in
the United States, presumably becauseof the effects of programs
like Medicare and Medicaid.
-
8/3/2019 Health Economics- Lecture Ch09
13/26
D. Data Sources
A common source of health care data is the insuranceclaim.
Claims data are limited to services covered by
insurance and used by the insured.
Claims data often lack detail on individualscharacteristics,
such as education and income.
In contrast, health interview survey data often incorporate
personal data, but their accuracy depends on the recallability of
the people being interviewed.
-
8/3/2019 Health Economics- Lecture Ch09
14/26
Experimental and Non-experimental Data
Much of health care demand research used non-experimental
data.
The researcher could not control the environmentor assure that
other extraneous variables were heldconstant.
A useful alternative involving the natural experiment
issometimes possible.
For example: a given area changes its healthinsurance plan
-
8/3/2019 Health Economics- Lecture Ch09
15/26
III. Empirical measurements of demand elasticities
A. Price Elasticities
-
8/3/2019 Health Economics- Lecture Ch09
16/26
B. Firm Specific Price Elasticities
-
8/3/2019 Health Economics- Lecture Ch09
17/26
C. Individual Income Elasticities
-
8/3/2019 Health Economics- Lecture Ch09
18/26
D. Income Elasticities Across Countries
Newhouse (1977) found elasticity estimates ranging from1.15 to
1.31.
Parkin et al (1987) found elasticities greater than 1.0.
Gerdtham et al. (1992) and Getzen and Poullier (1992)find
similar results.
-
8/3/2019 Health Economics- Lecture Ch09
19/26
E. Insurance Elasticities
-
8/3/2019 Health Economics- Lecture Ch09
20/26
IV. Impacts of insurance on aggregate expenditures
According to the RAND investigators, coinsurance andincome
accounted for about one-fifth of the total increasein real health
expenditures.
Subsequent research (Peden and Freeland, 1998)determined that
about half of the expenditure increasewas due to induced
technological innovation.
-
8/3/2019 Health Economics- Lecture Ch09
21/26
V. O ther variables affecting demand
A. Ethnicity and Gender
Many studies of demand examine the influence of race,and find
that blacks tend to consume less medical care
than the other large, self-identified groups when other factors
are held constant.
Females differ from males most clearly in their time
pattern of medical care usage.- childbearing years: women are
relatively heavyusers of health care- healthier in the long run
-
8/3/2019 Health Economics- Lecture Ch09
22/26
B . Rural vs Urban
Studies sometimes find differences in health care usagedue to
rural status.
If rural residents use less care, the reasons why are
notnecessarily clear.
Rural dwellers may differ culturally, and some analystsargue
that this factor is more important to ones
perception of life than ethnicity is.
-
8/3/2019 Health Economics- Lecture Ch09
23/26
C. Education
Education is strongly associated with better health.
If you are a college student, the odds are very good that
you are healthier than your noncollege counterparts.
As in the demand for health capital model, this may be because
you are a more efficient producer of health, you
are less likely to smoke, and you are more likely to eat
ahealthful diet.
-
8/3/2019 Health Economics- Lecture Ch09
24/26
D. Age, Health Status and Uncertainty
O lder people consume three to four times more healthcare than
the younger population.
W edig (1988) finds that the price elasticity of thedecision to
seek health care tends to be lower for thosewith poorer health
status.
W hen a consumer, uncertain about a future health risk,seeks
advice or preventive treatment, we call this a
precautionary demand (Picone, Uribe, and W ilson,1998).
-
8/3/2019 Health Economics- Lecture Ch09
25/26
Parting thought:
A good understanding of demand theory serves as therationale for
market-based, consumer-driven
approaches to health system reform.
In 2007, there were nearly 5 million enrollees
inconsumer-directed health plans (CDHPs), and their
numbers were increasing rapidly.
-
8/3/2019 Health Economics- Lecture Ch09
26/26
Discussion Questions:
W hy are firm-specific demand price elasticities higher than
elasticities for demand in general? W hy does a highelasticity
indicate a very competitive market?
The frequencies of health care visits are often used tomeasure
service demand. Many, however, criticize the useof this variable. W
hat are some pros and cons of using thisvariable?
In clinics that provide free care, price doesnt serve as
therationing mechanism. Explain how rationing might work.