Embed Size (px)
Citation preview
Health, Economic and Social Aspects of Ageing
Dr Virpi TimonenSchool of Social Work and Social Policy
Trinity College Dublin
Guest Lecture at the Royal College of Surgeons in Ireland19 December 2008

Key characteristics of ‘ageing’ as a research / study topic
� It is complex!
� Multi- / inter-disciplinary� Relatively new area of research, hence
much description, defining, conceptualising
� Tendency to problematise (aspects of) ageing, hence search for ‘solutions’ – and somewhat less for theories

Factors Influencing the Experience of Ageing
HappinessHappiness
HealthHealth WealthWealth
Quality of Life Quality of Life
Social networks (families), Social networks (families), leisure, care, housing, moraleleisure, care, housing, morale
ContributionsContributions mademadeby older peopleby older people
PhysicalPhysicalMental Mental
EnvironmentEnvironment
ExpectationsExpectations Experience,Experience,Life CourseLife Course
Work, PensionsGenesGenes
Key challenges
(1) How can one understand something as complex as ‘ageing’?
(2) Understanding ‘structure’ and ‘agency’: role of ‘actors’ vs. ‘the stage’
(3) Understanding ‘micro’ and ‘macro’ levels: how do individuals change & how do societies / policies change
Understanding ageing-related phenomena
The importance of the temporal aspect:
� Antecedents: Who? Why? � Processes: What? How?� Consequences: What? Why? How?
But: expense and demands of longitudinal studies

‘Tenets of gerontological imagination’(Ferraro 2006)� Ageing is not a cause of all age-related phenomena� Ageing involves biological, psychological and social
changes in individuals at varying rates� The imprint of genetics on development and ageing is
substantial� Age is positively associated with heterogeneity in a
population� Ageing is a life-long process and using a life-course
perspective helps advance the scientific study of ageing� Disadvantage accumulates over the life course� There is a propensity toward ageism in modern societies
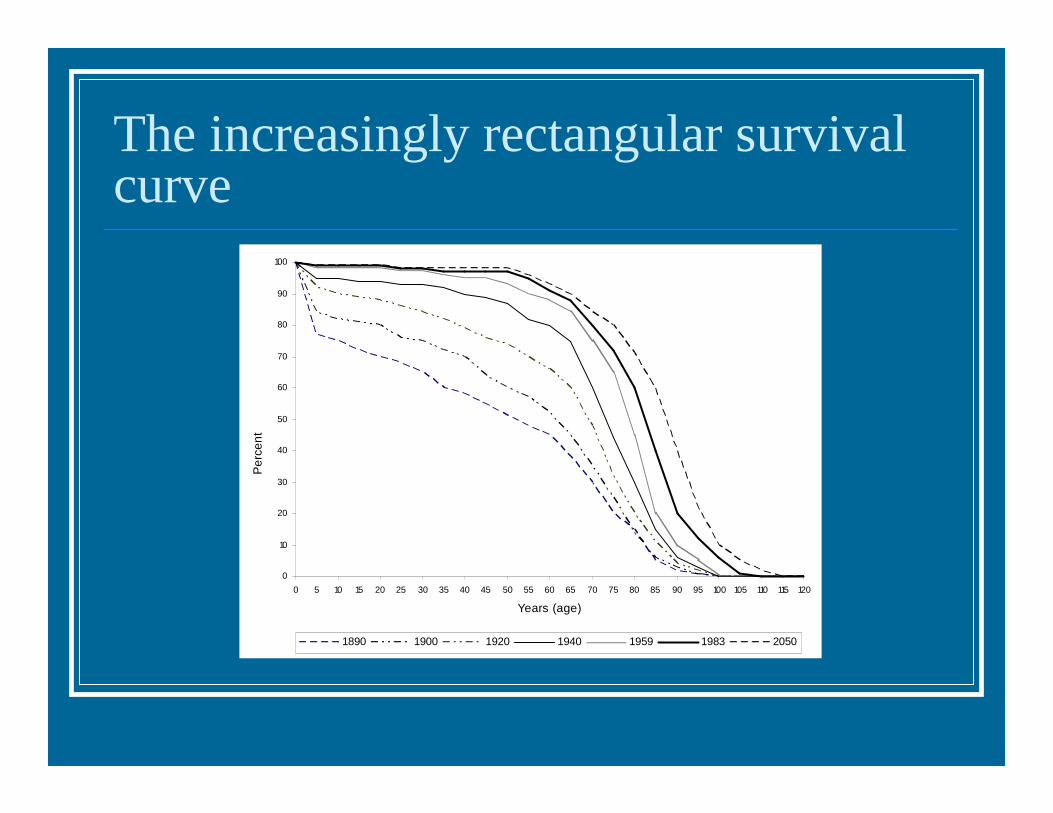
The increasingly rectangular survival curve
0
10
20
30
40
50
60
70
80
90
100
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90 95 100 105 110 115 120
Years (age)
Per
cen
t
1890 1900 1920 1940 1959 1983 2050

Global population will change markedly over the next 25 years

Programmes and projects > Highlights on health, Ireland 2004 > Burden of disease > Life expectancy and healthy life expectancy
Highlights on health, Ireland 2004
Home
Contents
Summary: findings and policy considerations
Selected demographic information
Burden of disease
Self-reported health
Health system
Contact us
LE and HALE© 2007 World Health OrganizationContact usPrivacy statement |Search ISO-88591 Life Expectancy & Healthy Life Expectancy 2000

Gait speed by wealth (ELSA)
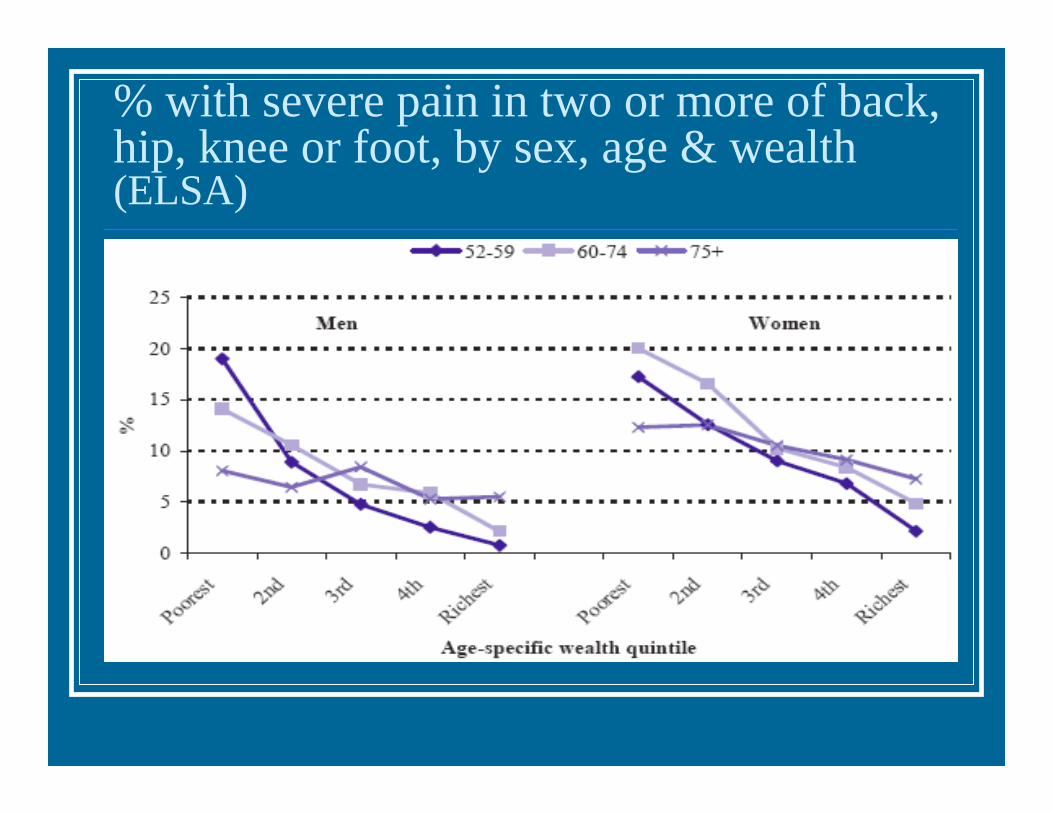
% with severe pain in two or more of back, hip, knee or foot, by sex, age & wealth (ELSA)
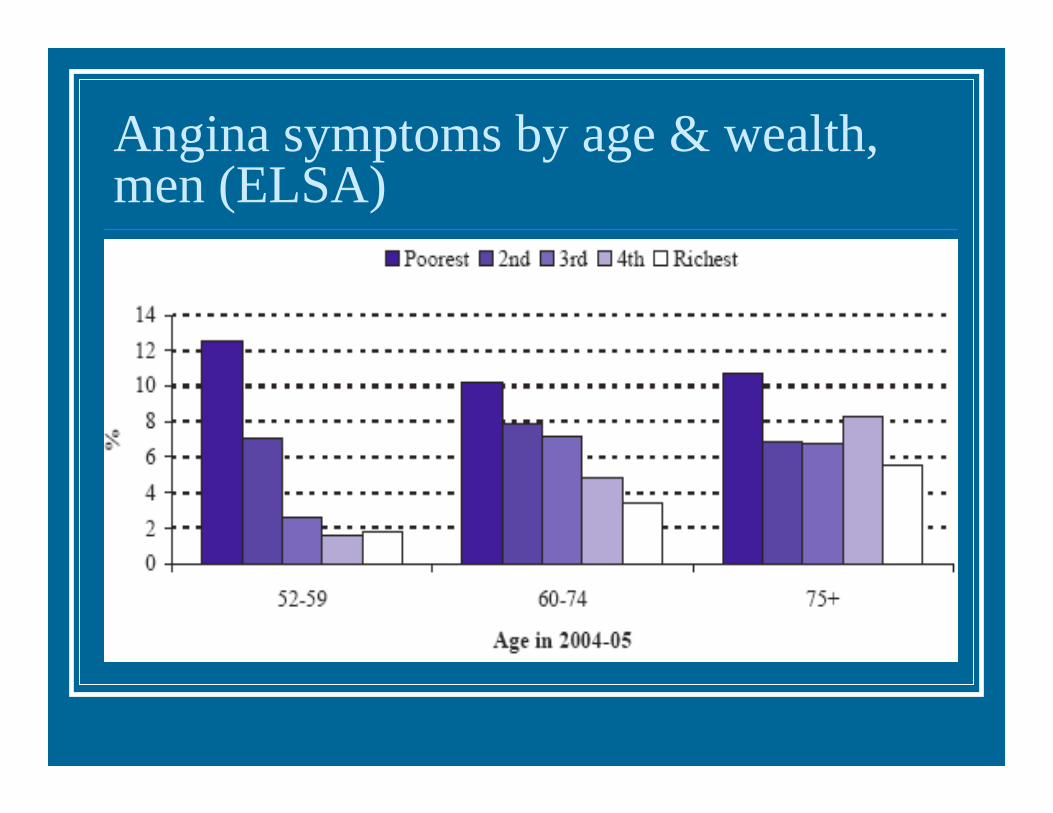
Angina symptoms by age & wealth, men (ELSA)

% with personal computer, by age and wealth (ELSA)

Feel isolated from other people by age & wealth (ELSA)

Survival by marital status, males (ELSA)

Survival by alcohol consumption, females (ELSA)

Health by education, SHARE - Irl
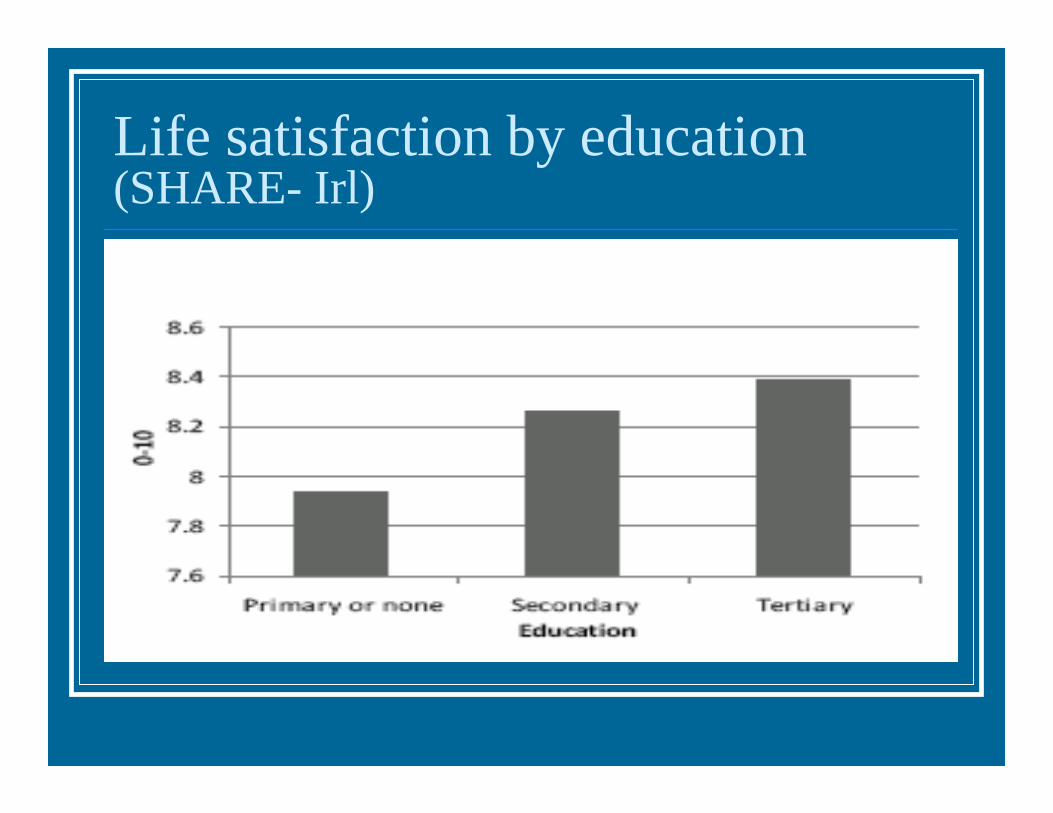
Life satisfaction by education (SHARE- Irl)

Need for care by age and sex (SHARE – Irl)
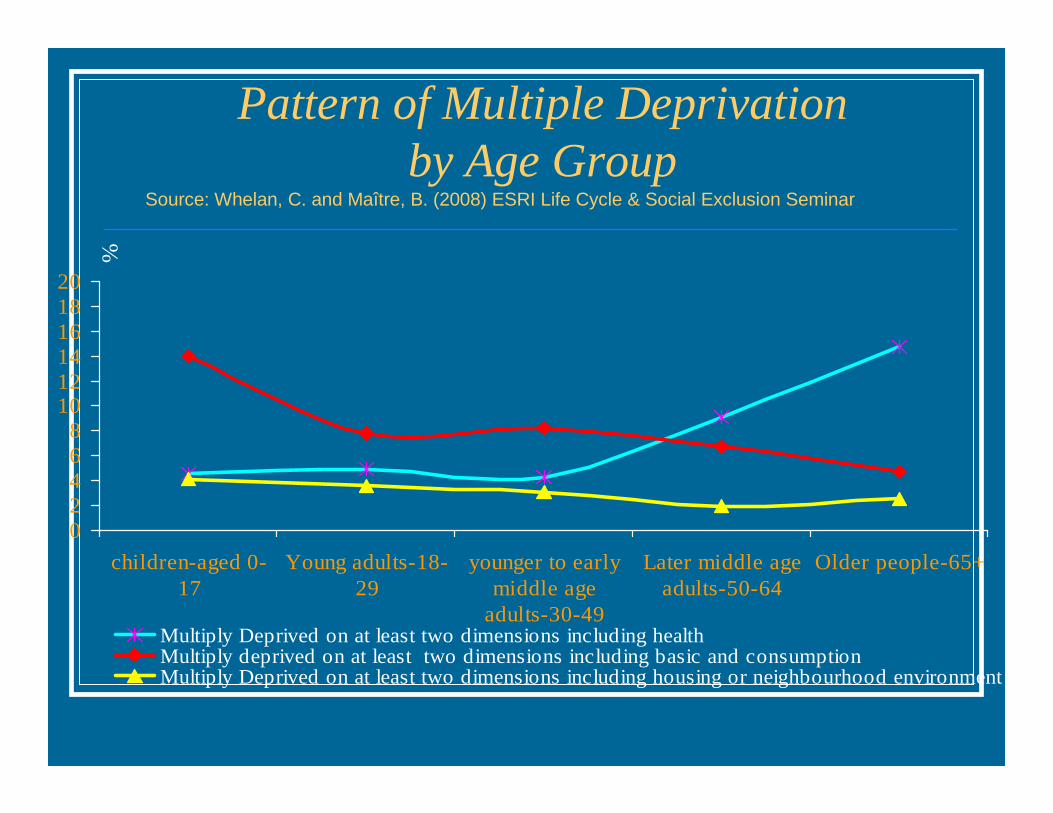
Pattern of Multiple Deprivation by Age Group
Source: Whelan, C. and Maître, B. (2008) ESRI Life Cycle & Social Exclusion Seminar
02468
101214161820
children-aged 0-17
Young adults-18-29
younger to earlymiddle age
adults-30-49
Later middle ageadults-50-64
Older people-65+
%
Multiply Deprived on at least two dimensions including healthMultiply deprived on at least two dimensions including basic and consumptionMultiply Deprived on at least two dimensions including housing or neighbourhood environment

At Risk of Poverty by Life Cycle Stage & HRP Educational Qualifications
Source: Whelan, C. and Maître, B. (2008) ESRI Life Cycle & Social Exclusion Seminar
0
10
20
30
40
50
60
Children Living withothers WA
Living togetherwith partner WA
Lone parent withchildren
Living togetherwith partner with
children
Living alone WA Older people
%
Inter level Leaving toTertiary level No qualifications
Percentage of respondents who reported having 3 or more close people they could count on if they had serious personal problems, by age, gender and social class, SLAN III

Understanding the Pathways from ‘Social’ to Health (and vice versa)Social – health
Social Engagement
• Social network• Social integration• Social support•Relationship quality
Health Outcomes
Physical Disease:• Disability•Osteoarthritis•CVD•Respiratory Disease
Psychiatric Disease:•Cognitive decline: Dementia, Alzheimer's Disease•Depression
Mortality
Survival after adverse health events
Pathways
Psychological processes:
• Loneliness• Anxiety• Hostility• Perceived stress• Depression• Positive affect
Behavioral processes:
• Smoking• Alcohol• Exercise• Sleep• Nutrition
BiomarkersStress hormones: Cortisol,, Adrenaline
Inflammatory markers: IL-6, CRP, Fibrinogen
Cardiovascular: General: BMI, WHRBlood pressureHeart rate variabilityPulse wave velocityBiomarkers: HbA1c, LipoA, Fasting lipids, Homocysteine
Socio-demographicCharacteristics
What is ‘successful ageing’?
‘Minimization of losses that occur as a result of a reduction in physical, cognitive and social reserves and a maximization of gains that result through adaptation, mastery and the use of wisdom.’
Baltes & Baltes, 1990
Ageing as Adaptation (1)� Process of adaptation at both individual
and societal levels� But some face greater challenges than
others! Those same individuals less well equipped to deal with these challenges
� In most countries, adaptation expected to happen primarily at the level of individuals / families

Ageing as Adaptation (2)� Locus of adaptation in all systems has
been gradually shifting towards older people themselves
� The ‘problem’ becomes the ‘solution’ (at a high cost to some groups)
� Increasing focus on ‘opportunities’ & ‘freedoms’ → apparent / real decline in ageism; age resistance / denial
To conclude…Points for discussion…
� Plentiful evidence of links between health, economic & social aspects of life in older age
� But ‘pathways’ (the why & the how) poorlyunderstood!
� ‘Good old age’ in fact guaranteed for some, denied to others, at a much younger age?
� What, if anything, should be done?