Embed Size (px)
Citation preview

The Royal Marsden
Head and neck cancer: what symptoms matter?
Professor Vinidh Paleri
Consultant Head and Neck Surgeon

87
Outline
2 week wait referral pathway
– Evidence base
– 2015 guidance
– “Tease” out relevant symptoms
– Clinical scenarios
– Neck exam and lumps
– Oral exam and lumps
Head and Neck Cancer referral from Primary Care

88 Head and Neck Cancer referral from Primary Care

Results 89
2012N=1809 Cancer diagnoses 6.3% to 14.6%Pooled detection rate: 11.1%
Head and Neck Cancer referral from Primary Care
2016N=4028Cancer diagnoses 2.2% to 14.6%Pooled detection rate: 8.8%Subgroup of later studies 6.6%

90
NICE HN cancer 2015 guidance
– June 2015: updated NICE HNC referral guidance
– Categorised by organ sites
– Positive predictive value (PPV) used to determine the high-risk symptoms for HNC.
– Used data from studies within a primary care setting
– The Guideline Development Group (GDG) included all symptoms with a PPV threshold of 3% or higher
Head and Neck Cancer referral from Primary Care

91 Head and Neck Cancer referral from Primary Care

Head and Neck Cancer referral from Primary Care92
Total dataset: n = 5,082 via the 2WW systemMissing data = 367 Prediction model = 4,715 M:F = 2,058: 2,657 Mean age: 59 years Patients with HNC = 397 (8.4%)
Multivariate binary logistic regressionIdentify of 2 and 3 way interactions Assess the performance of the current and previous NICE referral guidance

93 Head and Neck Cancer referral from Primary Care
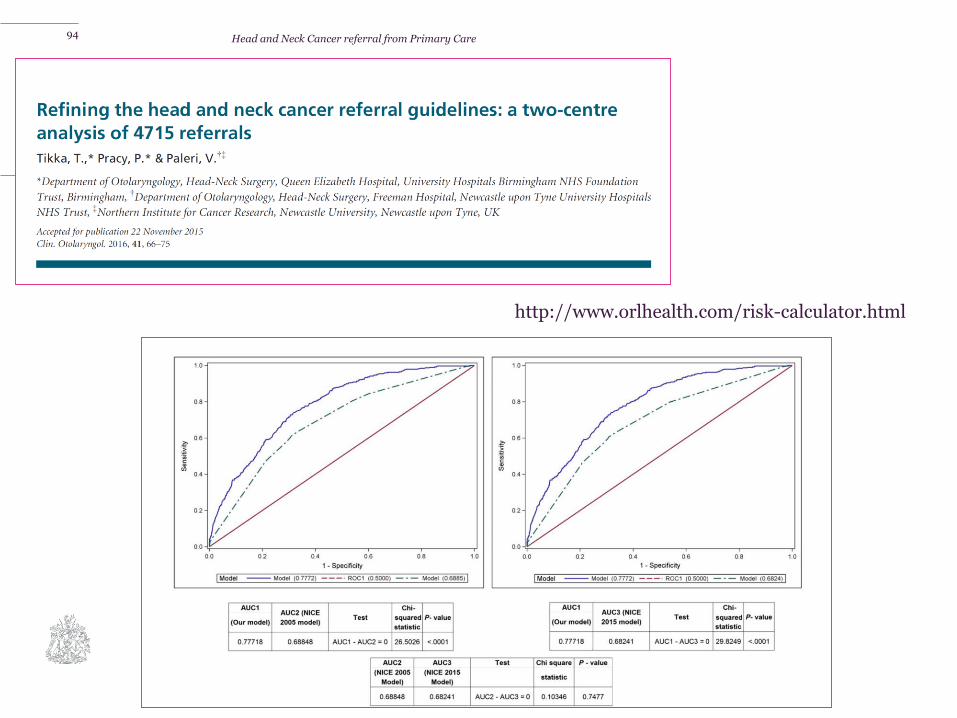
94
http://www.orlhealth.com/risk-calculator.html
Head and Neck Cancer referral from Primary Care

95
Referral symptoms and pick up rates
Symptom Frequency (%) PPV (%)
Persistent otalgia, normal otoscopy 0.9 18.2
Unexplained lump in neck >3 weeks 22.5 17
Dysphagia >3 weeks 4.7 13
Ulceration of oral mucosa >3 weeks 8.7 12.4
Hoarseness >3weeks 20.2 7.76
Persistent sore or painful throat 5.8 5.9
Red and white patches of oral mucosa 3.2 4
Sensation of lump in throat 7.1 1.5
Intermittent hoarseness 7.7 0.8

A different model
Persisting hoarseness > 3 weeks
Unexplained oral ulceration or mass > 3 weeks
Unexplained persistent swelling in the salivary gland >3 weeks
Unexplained neck mass >3 weeks or recently appeared neck mass
Dysphagia > 3 weeks
Odynophagia >3 weeks
Unexplained otalgia with normal otoscopy
Sensation of lump in throat AND presence of blood in mouth
Sensation of lump in throat AND unexplained otalgia and normal
otoscopy
96
http://www.orlhealth.com/risk-calculator.html

Head and neck cancer: what symptoms matter?
97

Symptom-based telephone triage for suspected head and neck cancer referrals in the UK: 6-month outcomes from a prospective national service evaluation during the initial peak of the COVID-19 pandemic.
- Supported by ENT UK, BAHNO and INTEGRATE
- 16 week period, between 23rd March and 13th July 2020
- Risk stratification with HaNC-RC-v2 http://orlhealth.com/
John Hardman
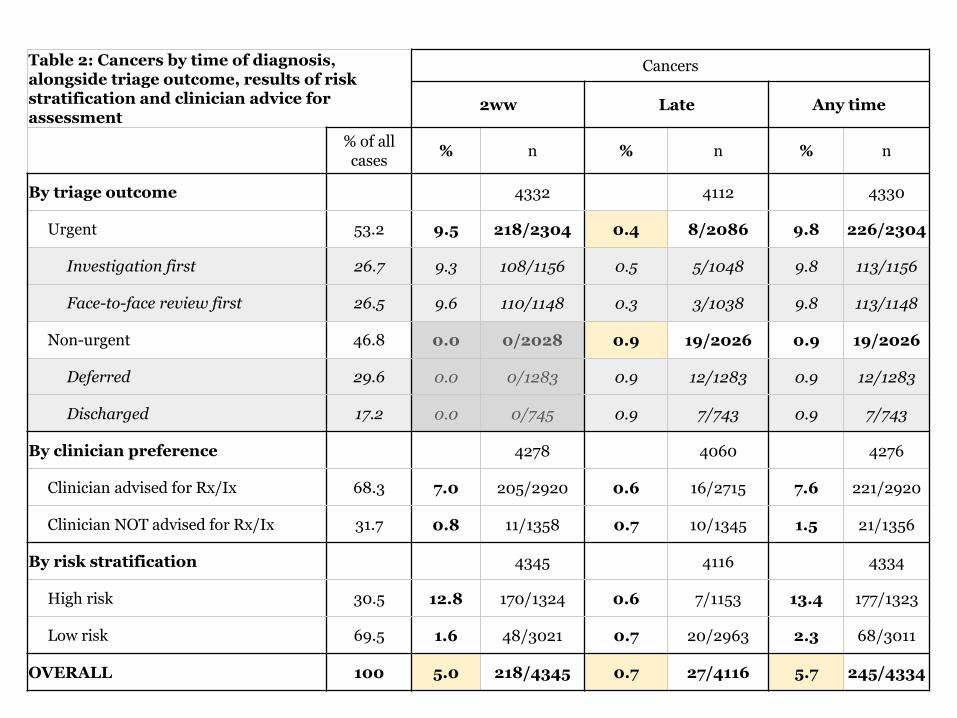
Table 2: Cancers by time of diagnosis, alongside triage outcome, results of risk stratification and clinician advice for assessment
Cancers
2ww Late Any time
% of all cases
% n % n % n
By triage outcome 4332 4112 4330
Urgent 53.2 9.5 218/2304 0.4 8/2086 9.8 226/2304
Investigation first 26.7 9.3 108/1156 0.5 5/1048 9.8 113/1156
Face-to-face review first 26.5 9.6 110/1148 0.3 3/1038 9.8 113/1148
Non-urgent 46.8 0.0 0/2028 0.9 19/2026 0.9 19/2026
Deferred 29.6 0.0 0/1283 0.9 12/1283 0.9 12/1283
Discharged 17.2 0.0 0/745 0.9 7/743 0.9 7/743
By clinician preference 4278 4060 4276
Clinician advised for Rx/Ix 68.3 7.0 205/2920 0.6 16/2715 7.6 221/2920
Clinician NOT advised for Rx/Ix 31.7 0.8 11/1358 0.7 10/1345 1.5 21/1356
By risk stratification 4345 4116 4334
High risk 30.5 12.8 170/1324 0.6 7/1153 13.4 177/1323
Low risk 69.5 1.6 48/3021 0.7 20/2963 2.3 68/3011
OVERALL 100 5.0 218/4345 0.7 27/4116 5.7 245/4334

OUTER:PPV of symptom
INNER:How commonly that symptom is reported
0.0 1.3
2.9
3.5
3.7
3.7
3.7
4.4
5.0
5.9
6.67.8
7.9
8.1
8.3
9.1
9.6
10.1
10.2
10.5
13.9
14.717.1
2.1 12.1
25.3
5.3
11.1
32.6
3.1
5.2
9.7
28.01.7
10.711.116.5
5.8
10.4
1.2
9.8
9.5
6.1
6.0
21.9 0.9
Ho
ars
e
(
pers
., e
xp
lain
ed
)
Th
roat
pain
(
int. b
ilat.
/mid
.)Hoa
rse
(
int.)
Throat p
ain
(
int.
unilat.)
Dysphagia
(int.)
FOSIT
Mouth ulcer
Neck lump
(fluct./reduc.)
Throat pain
(pers. bilat./mid.)
Ex−
smoker
Strid
or
Ota
lgia
Ho
ars
e
(
pers
.)Curr
ent
smoke
r
Mouth
sw
ellin
gOdynophagia
Ex−excess
alcohol
Weight loss
Heavy alcohol
Throat pain
(pers. unilat.)
Dysphag
ia
(pers.)
Neck lu
mp
(pers
.)
Sk
in le
sio
n

OUTER:Straight to Ix
INNER:Straight to discharge
15.015.6
16.6
17.6
21.5
22.8
22.9
23.0
23.6
24.2
24.425.428.5
28.9
29.9
30.1
31.5
35.7
38.5
38.7
40.4
44.858.0
20.724.0
3.5
31.9
8.1
17.3
16.7
16.7
13.5
11.12.4
7.99.71.3
4.9
11.8
11.3
1.1
9.6
6.1
16.7
1.2 2.2
Th
roa
t p
ain
(in
t. b
ila
t./m
id.)
Ho
ars
e
(
int.
)H
oar
se
(
per
s.)
Hoarse
(
pers.,
explain
ed)
Mouth ulcer
FOSIT
Ex−smoker
Heavy alcohol Throat pain
(int. unilat.)
Thro
at p
ain
(pers
. bila
t./mid
.)
Skin
lesio
n
Mo
uth
sw
ellin
g
Ota
lgiaStr
idor
Odyn
ophagia
Dysphagia
(in
t.)
Current
smoker
Throat pain (pers. unilat.)
Ex−excessalcohol
Weight loss
Neck lu
mp
(fluct./red
uc.)
Dysp
hag
ia
(pers
.)
Ne
ck
lum
p
(pe
rs.)

Key points- Reporting outcomes from a prospective multicentre national
study of telephone triage of 4,345 suspected head and neck
cancer referrals in 40 centres with minimum follow-up of 6
months.
- Over a quarter of patients were triaged directly to an
investigation and 1 in 6 were discharged directly from the
telephone consultation.
- The overall cancer rate in this population was 5.7% after 6
months minimum follow-up, similar to non-pandemic rates.
- The rate of late cancer diagnosis leading to harm was 0.2% in
patients seen and/or investigated urgently and 0.4% in those
triaged as non-urgent who were deferred or discharged.
- If performing telephone triage, clinicians should be mindful
that nasal cavity/nasopharygeal, oesophageal and lung cancers
were the highest incidence in the late cancer group.

103
The neck lump

Midlinethyroidlarynx
104
Laterallymph nodes salivary glands
Non- cancer Cancer
Neck lump
Rapid increase in sizeHardSkin invasionNon-inflamedRegional symptomsSystemic symptoms
InflammatoryDevelopmentalBenign neoplasm

Source: National Cancer Information Service

269 papers, 19,000 + patients

Branchial Cyst (A dangerous diagnosis >35 years)
– Presentation
– Management

Current recommendation
Comprehensive ENT
examination±NBI
Fine needle cytology
18FDG-PET/CT
Panendoscopy, bilateral
tonsillectomy and tongue base
mucosectomy
“True” unknown primaries 15%
US guided core biopsy


Beware
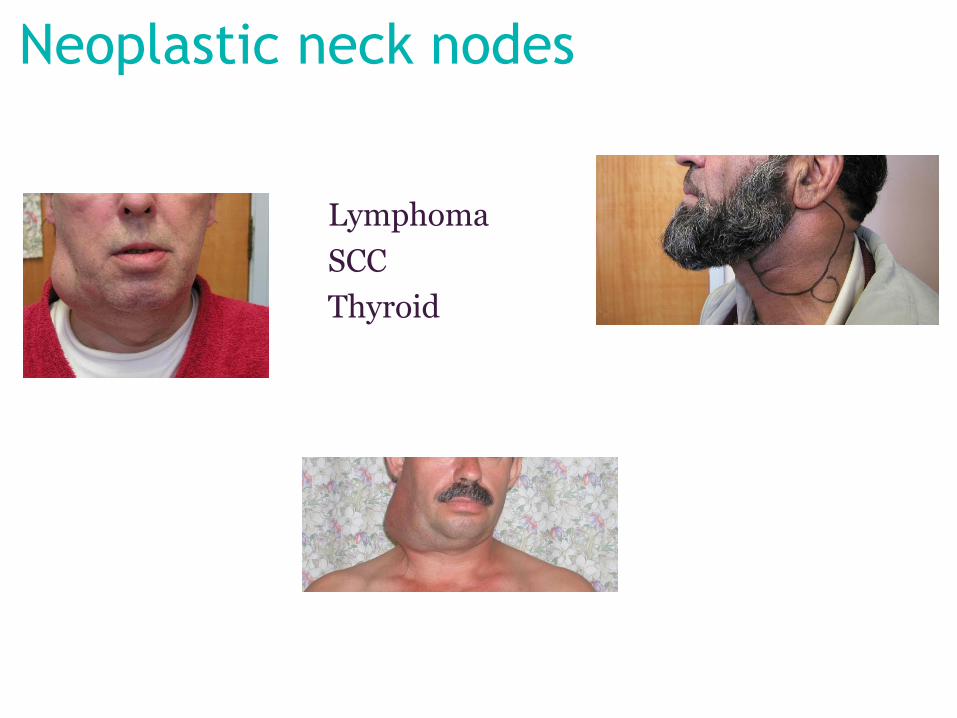
Neoplastic neck nodes
Lymphoma
SCC
Thyroid

A lesson learnt

A lesson learnt

Cervical lymphadenopathy
– Infective– Specific
– Non specific
Glandular fever
Toxoplasmosis
TB
Atypical TB
Kawasaki disease
CMV
Etc….

Thyroid Lumps
– History– Toxic symptoms
– Hypofunction
– Examination– Eye signs
– Tremor
– Reflexes
– Swallowing
US guided FNA and/or core biopsy

Thyroglossal cysts
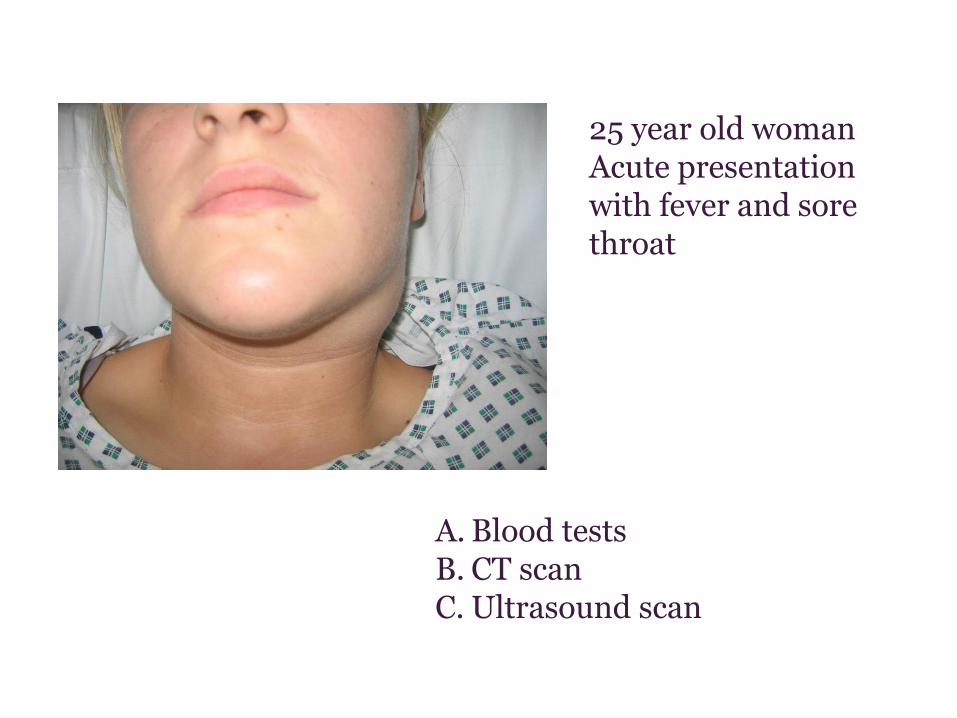
25 year old womanAcute presentation with fever and sore throat
A. Blood testsB. CT scanC. Ultrasound scan

64 year old manWorsening swelling for 4 weeksNo systemic symptomsExamination reveals a brawny swelling, relatively superficial, fluctuant at sitesWeeping wound
A. Parotid MalignancyB. Organised parotid abscessC. Sebaceous cyst

34 year old manWorsening swelling for 6 weeksNo systemic symptomsDental work prior to onset of swellingExamination reveals a fluctuant swelling
A. Submandibular salivary gland malignancy
B. Actinomyces C. Sebaceous cyst

1 year old Lump present for 3 months
A. 1st branchial arch cystB. Parotid abscessC. Atypical TB

What will clinch the diagnosis? A. Clinical examinationB. Ultrasound scanC. CT scan
30 year old manSwelling for 9 monthsNo systemic symptoms

14 year old Lump present for 2 yearsIntermittent infection
14 year old Wetness noticed with intermittent inflammation


124
The oral cavity

Oral cavity
Oral cavity exam

Features that may reduce suspicionRecurrent ulceration that heals inbetween episodesMultiple synchronous ulcers Clustering of ulcersOccurrence in association with systemic diseasesBlister formationAssociated sore and bleeding gumsIdentifiable local causes (for example, sharp tooth)
126
Features that should raise suspicion Non-healing painless ulcer present for >3 weeksInduration and lack of inflammation surrounding ulcerUlcer with rolled thickened edgeSmoking and alcohol useAge (85% of cases at age >50 years)Male sex (2:1)Previously diagnosed premalignant lesion No history of previous ulcerationNo local factors of ulcerationNo systemic factors of ulcerationHistory of oral squamous cell carcinoma

Non-cancer lesions
Lichen planus
Lichenoid reactions
Lupus erythematosus
Graft versus host disease
Lichen sclerosis et atrophicus
Lichenoid & granulomatous stomatitis




Oral Premalignant Lesions
Leukoplakia
Erythroplasia
Lichen planus
Oral submucous fibrosis
Syphilitic leukoplakia
Chronic hyperplastic candidosis
Actinic keratosis
Discoid lupus erythematosus
Sideropenic dysphagia
Immunosuppression






Aphthous ulcers



Common oral infections

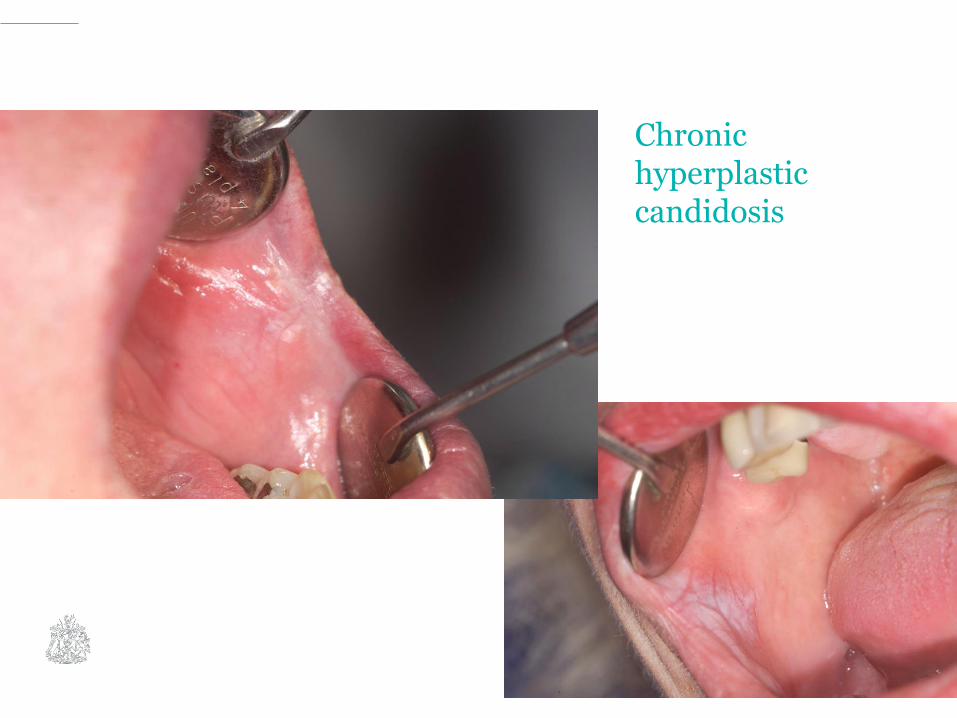
Chronic hyperplastic candidosis

Denture stomatitis


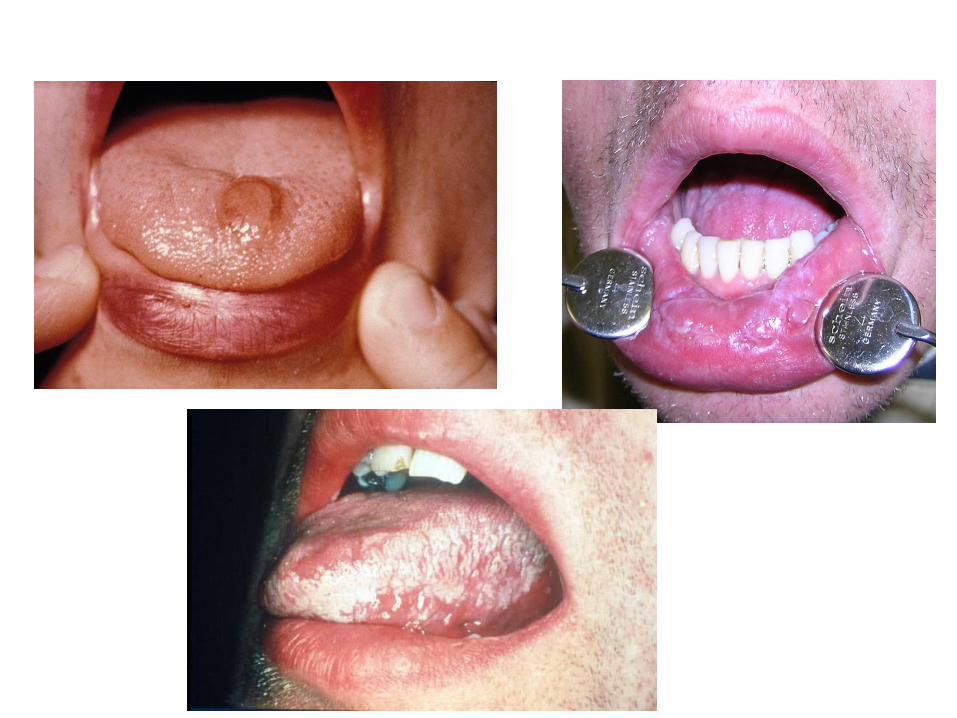




Drug induced ulcers
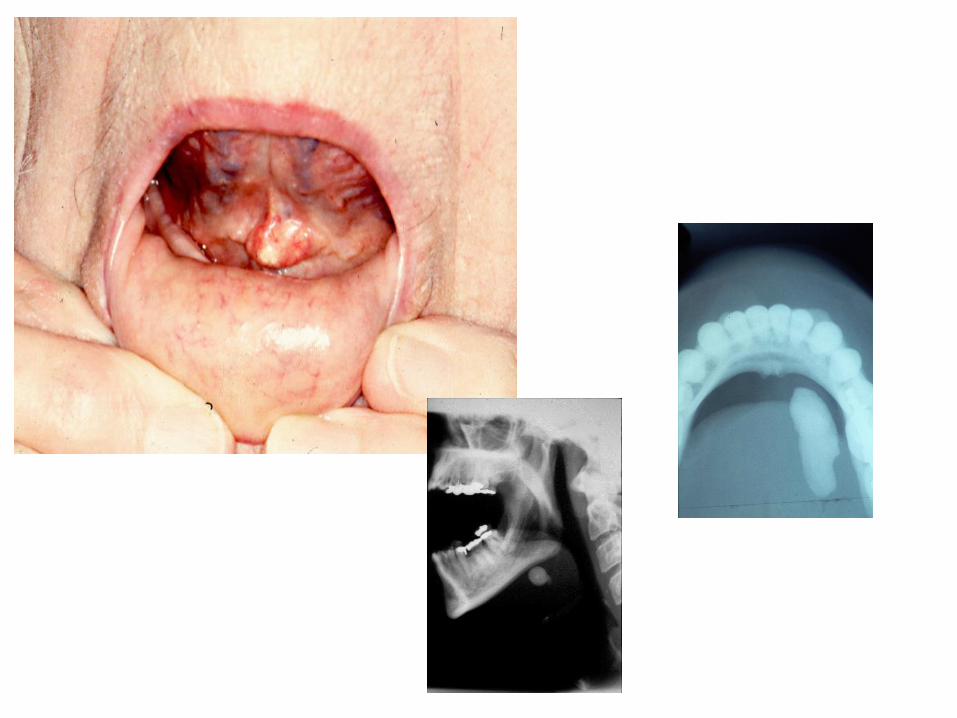
Oral lumps

Submandibular gland

155

156

Conclusions - Adopt a systematic approach to neck and oral cavity
examination
- Examine UADT mucosa for all patients presenting with neck lumps
- Treat all neck lumps in patients >35 as cancer unless proven otherwise
- Unexplained otalgia is a red flag symptom with high PPV
- Flat, non-indurated oral ulcers have a multitude of causes, many self limiting
- Treat all non-bony oral lumps as cancers unless proven otherwise
- A more evidence based approach to HN cancer referral is awaited
158