Embed Size (px)
Citation preview
Panel: George Bovis, MD Philip Gorelick, MD, MPH Thomas Grobelny, MD Barbara Parilla, MD Susan Rubin, MD
Moderator: Wayne Rubinstein, MD
Case Discussion Stroke Risk in Women: Hot Topics
Objectives • Discuss the clinical practice of stroke in women
– evaluation of acute neurologic presentations
– consideration of atypical stroke mechanisms
– immediate and ongoing management
– assessment of recurrence risk
– recommendations for secondary stroke prevention
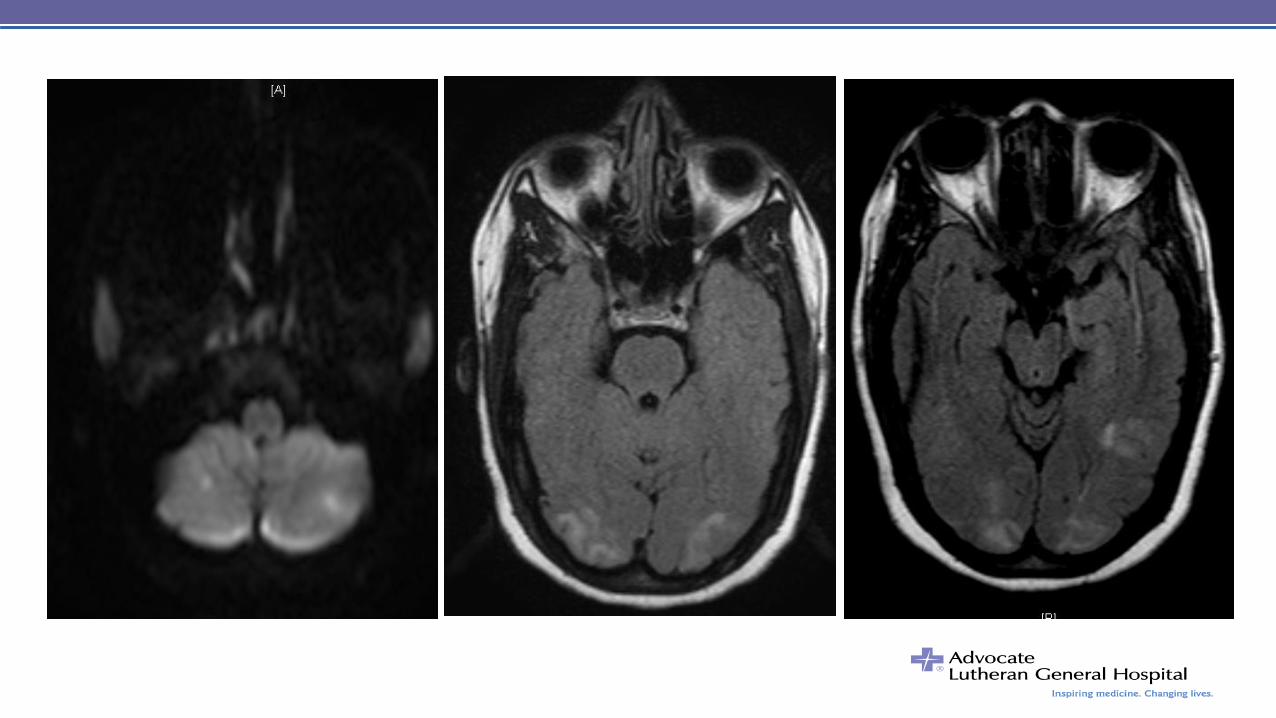
Case #1 • 35 y/o RH woman, 1 week after NSVD and PPTL,
presenting with three days of severe headache
• Transiently responsive to sumatriptan
• Distinct from prior migraine: bilateral, throbbing, neck pain,
photophobia, no focal neurological symptoms
• Time course of onset not specified
• 140/90, 72, 37o, normal neurologic exam
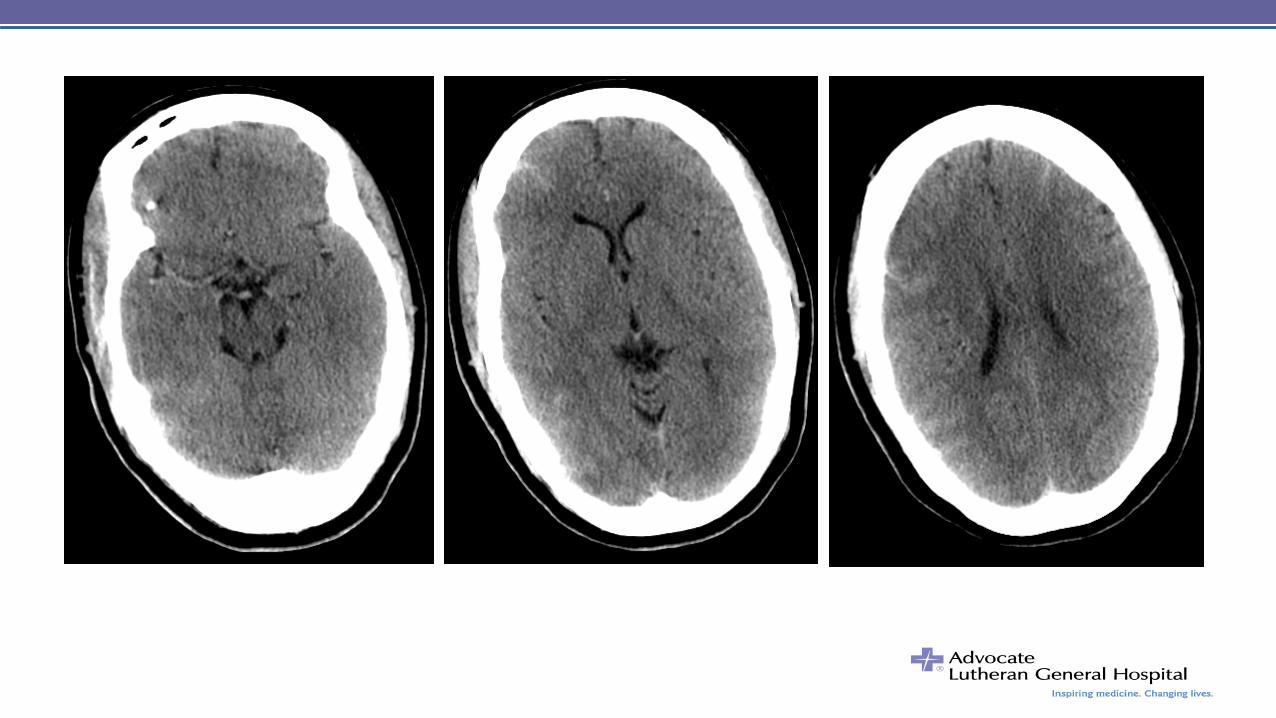
• Non contrast head CT unremarkable
Case #1 • No positional component apparent
• CBC, CMP, INR, normal
• CSF: no cells, protein 7.4, glucose 46
– ? ̶
• Tentative diagnosis of status migranosis
• DHE protocol initiated
• Methylprednisolone IV
• HD-2: unresponsive appearing post ictal, 180/90
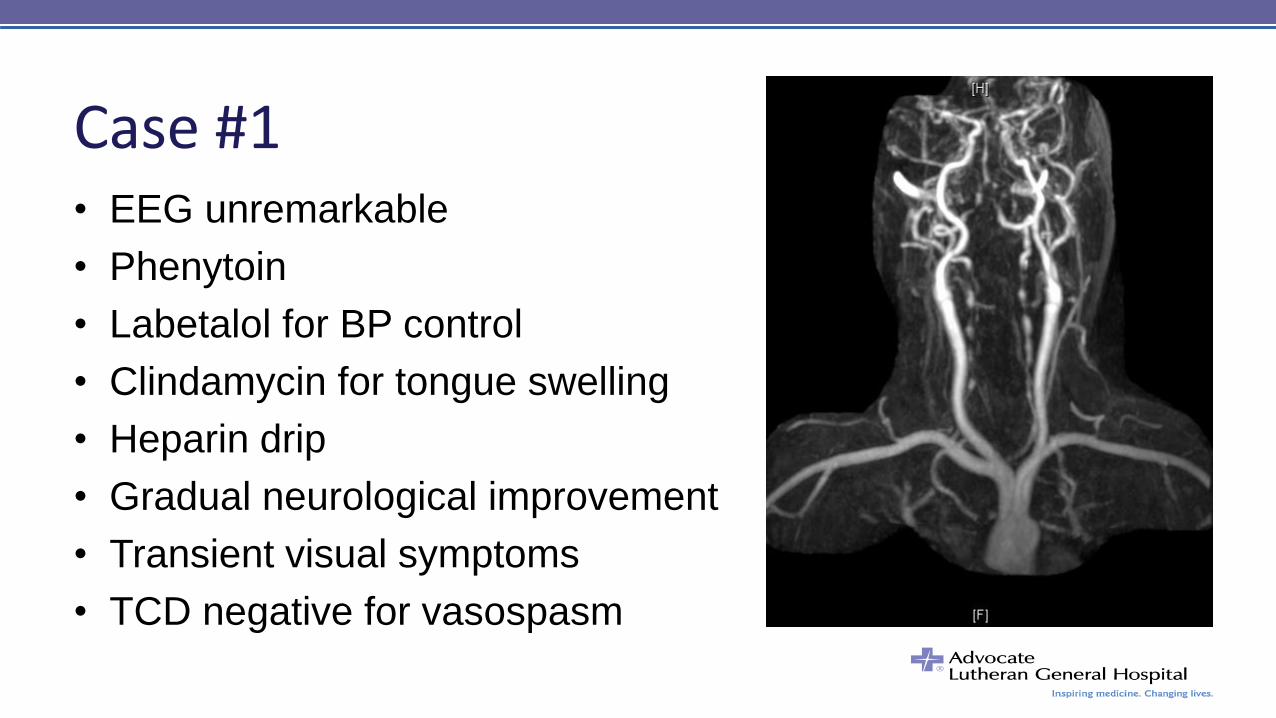
Case #1 • EEG unremarkable
• Phenytoin
• Labetalol for BP control
• Clindamycin for tongue swelling
• Heparin drip
• Gradual neurological improvement
• Transient visual symptoms
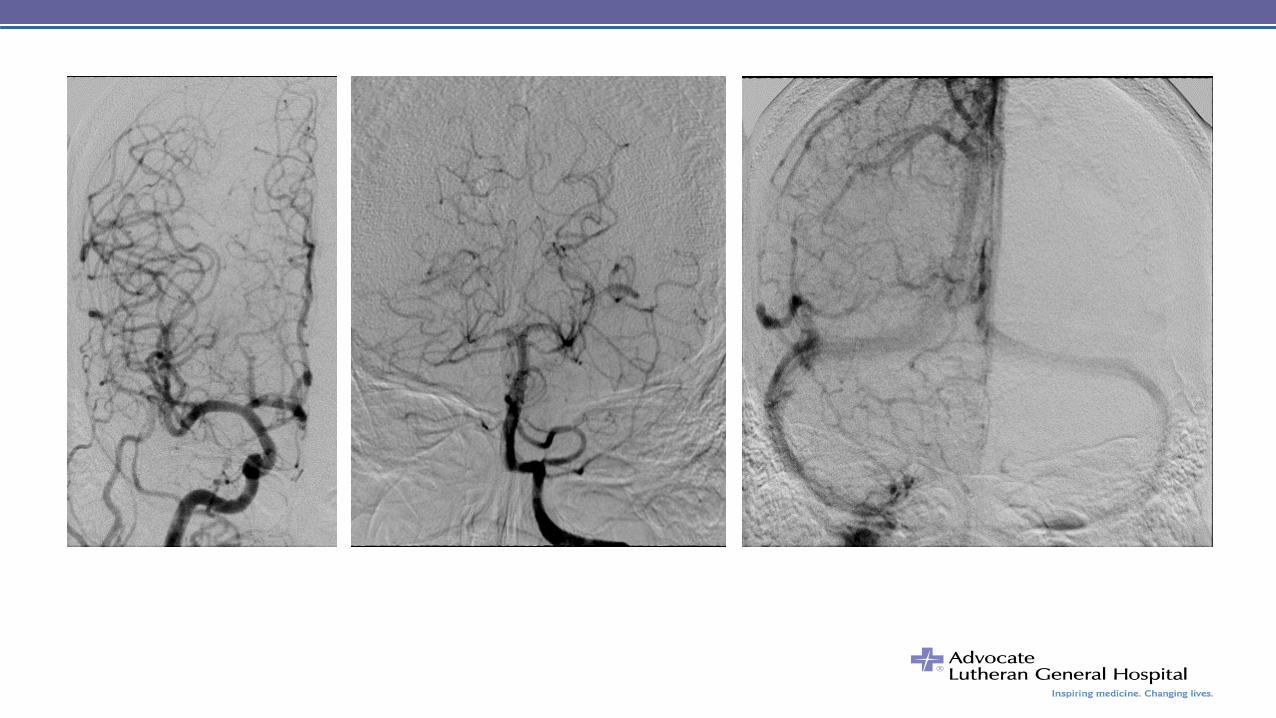
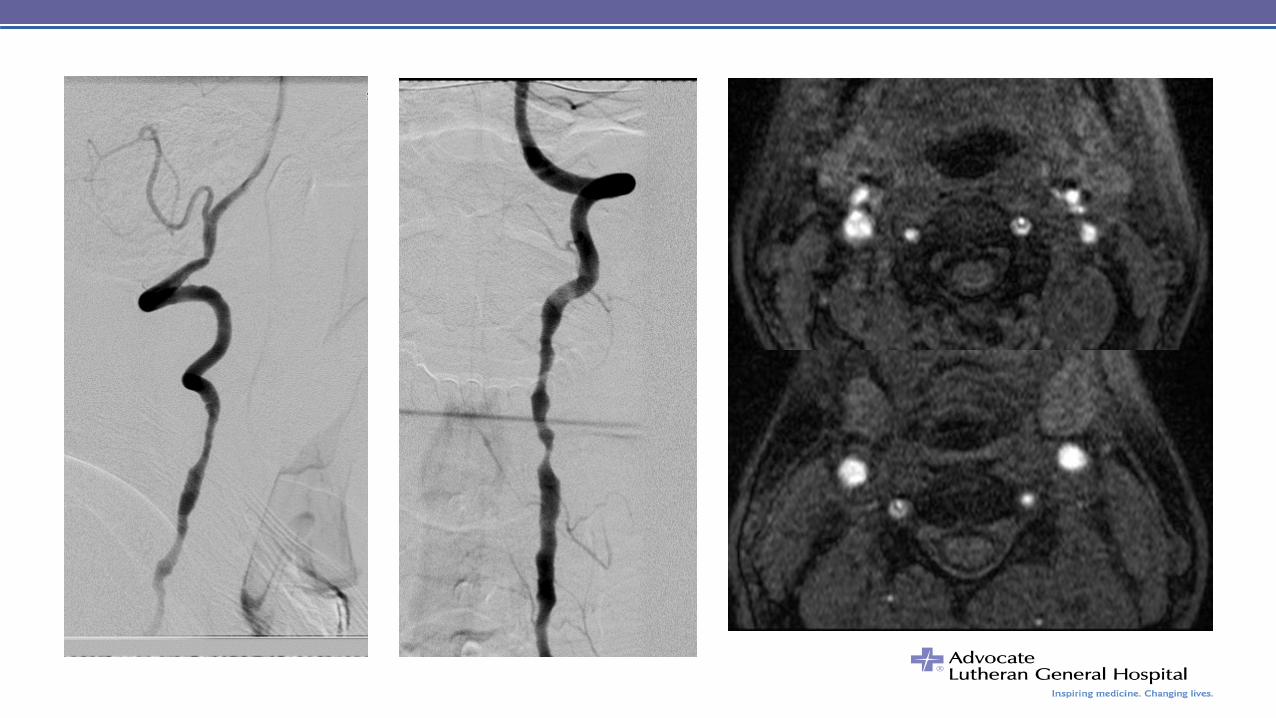
• TCD negative for vasospasm
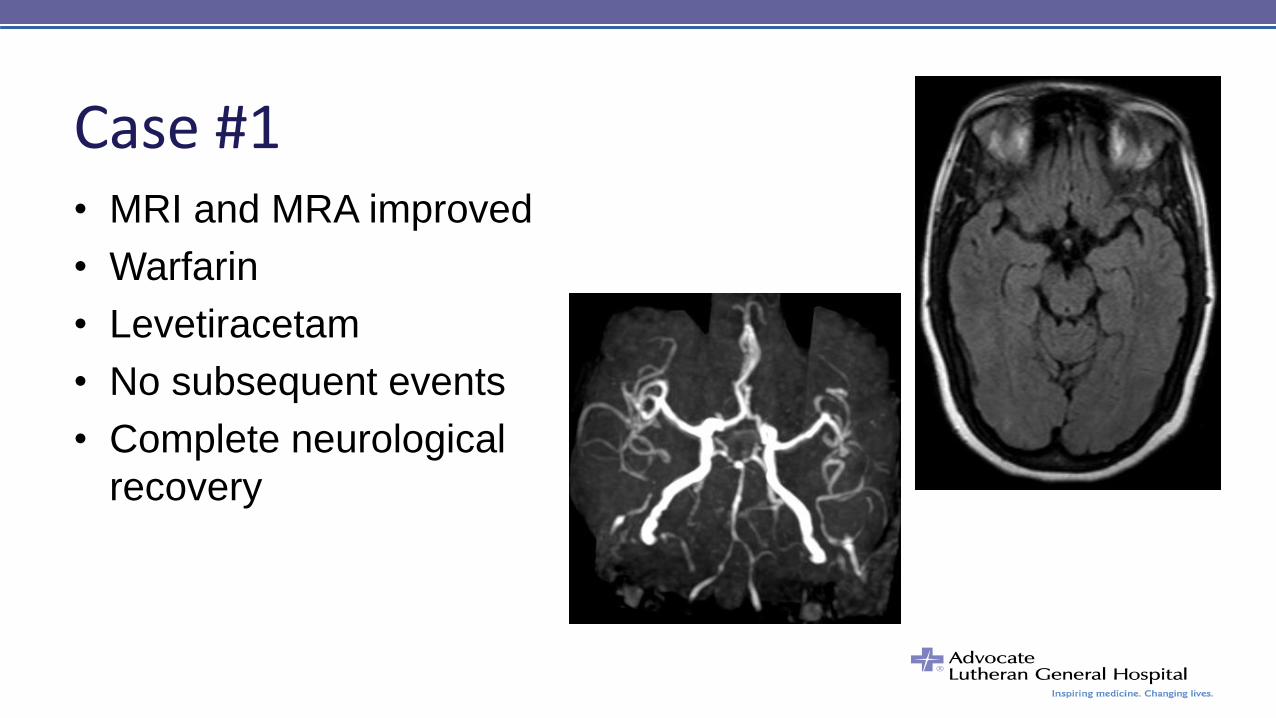
• MRI and MRA improved
• Warfarin
• Levetiracetam
• No subsequent events
• Complete neurological
recovery
Case #1
Case #2 • 22 RH woman presents with
– Novocain-like numbness spreading from left hand to shoulder
– followed by inability to lift her left arm for 10-15 minutes
– associated with loss of vision in the left periphery
– resolved within 30 minutes after initial symptoms
– followed by a mild nondescript headache
• Prior history of headache, never diagnosed with migraine
• The patient’s mother had a stroke due to PFO while young
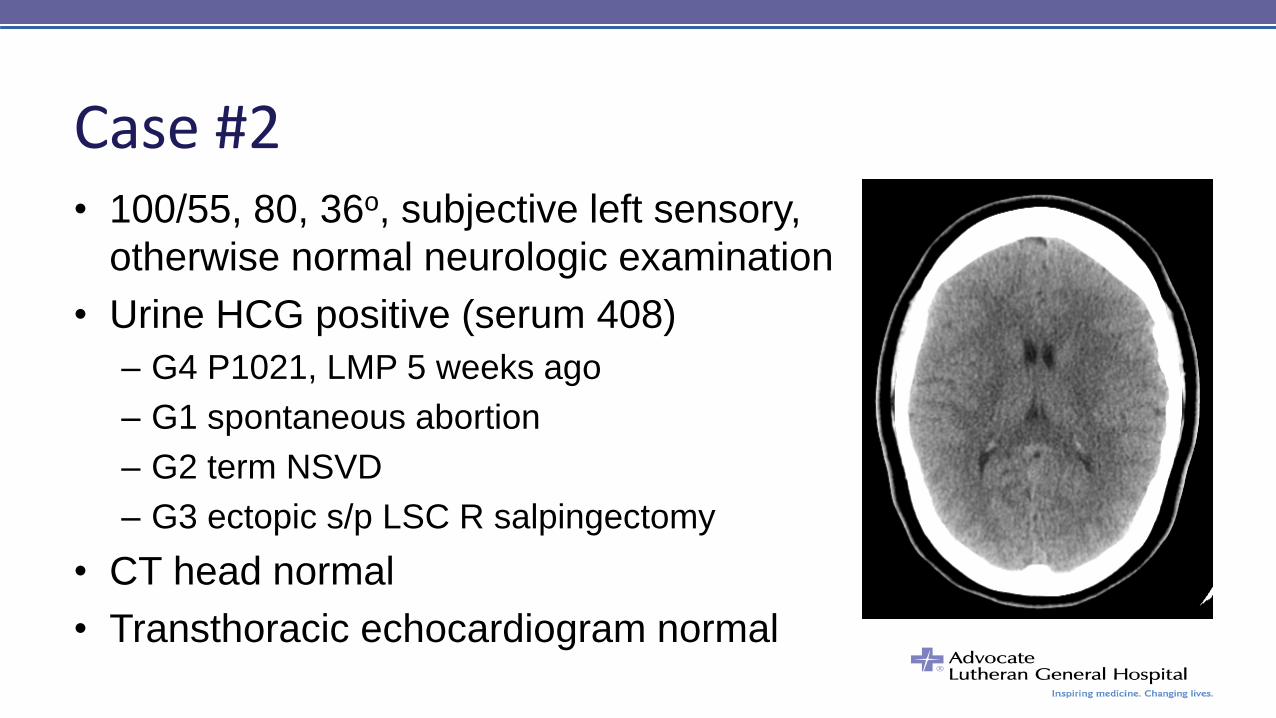
Case #2 • 100/55, 80, 36o, subjective left sensory,
otherwise normal neurologic examination
• Urine HCG positive (serum 408)
– G4 P1021, LMP 5 weeks ago
– G1 spontaneous abortion
– G2 term NSVD
– G3 ectopic s/p LSC R salpingectomy
• CT head normal
• Transthoracic echocardiogram normal
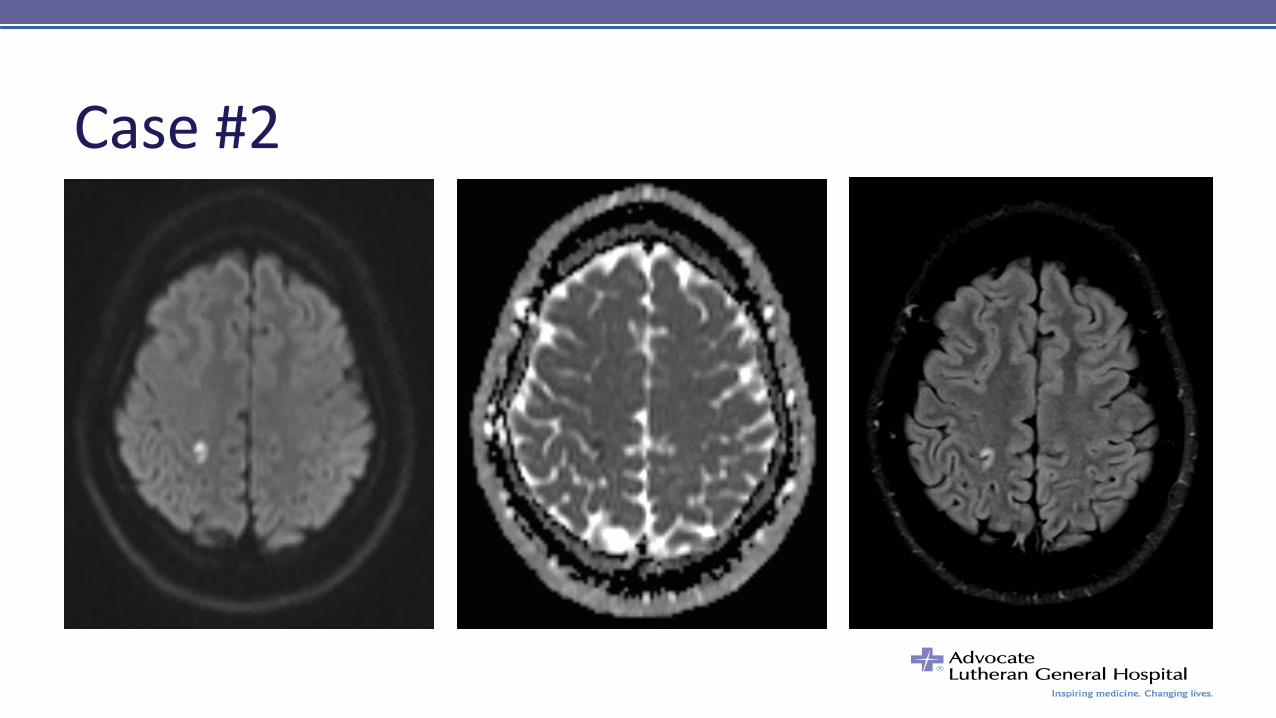
Case #2
Case #2 • Transesophageal echocardiogram:
– small patent foramen ovale
– left-to-right shunt with coughing
– no atrial septal aneurysm
• Venous duplex and V/Q normal
• Hematology recommended enoxaparin anticoagulation
• ANA17, LA, AT-III, Pro S, Cardio Ab, Phos-ser Ab, V genotype
• Pro C 77, MTHFR heterozygote C677T
• Spontaneous abortion at 8 weeks gestation
Case #3 • 20 y/o RH woman with acute onset aphasia and right
hemiplegia
• Came home from grocery shopping, had intercourse with
boyfriend, got dressed, walked out of bathroom holding
Aleve bottle at 14:10
• Suddenly looked dazed, not talking, sat down on floor,
slumped over to the right
• ED arrival at 14:54
Case #3 • Flight from France 2 days prior to presentation
• Had 4 wisdom teeth extracted in France 12 days prior
• PMH: infrequent migraines; no history of VTE
• Meds: OCP (Loestrin)
• SH: non-smoker, no drug use, rare EtOH
• FH: no history of VTE, stroke, MI, rheum disorder
• ROS: +headache; otherwise negative
Case #3 • VS: T 97.7, HR 101, BP 123/79
• general exam normal, no carotid bruits, no murmur
• expressive aphasia providing best 1 word answers with
dysarthria; follows commands throughout L side
• L gaze preference, R field cut and R UMN facial droop
• dense R hemiparesis – arm 0/5, leg weak w/d to noxious
• NIHSS = 15
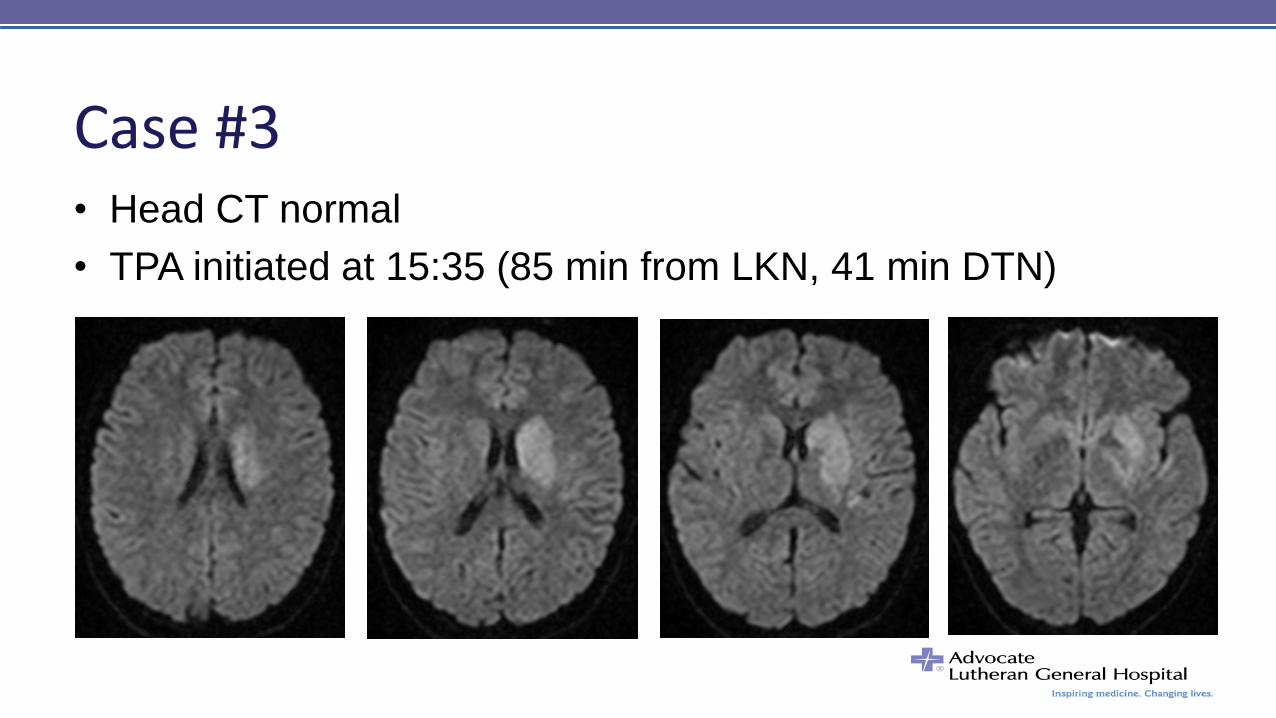
Case #3 • Head CT normal
• TPA initiated at 15:35 (85 min from LKN, 41 min DTN)
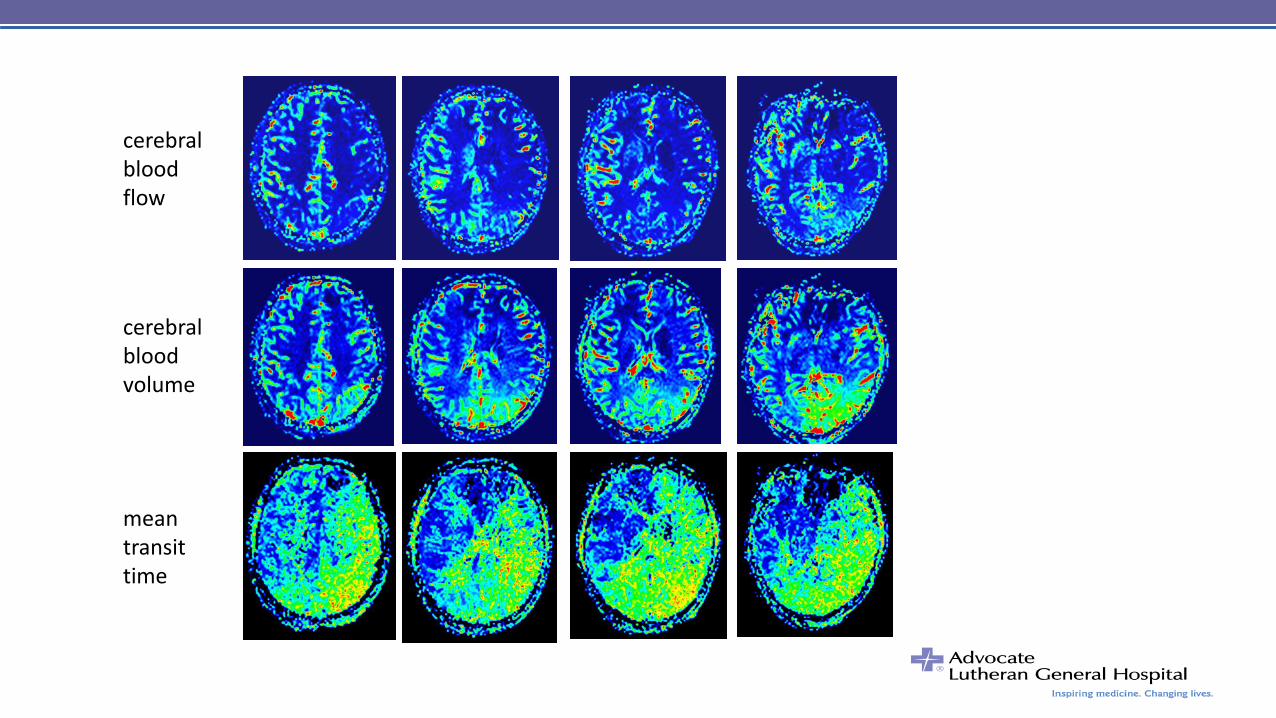
cerebral blood flow
cerebral blood volume
mean transit time
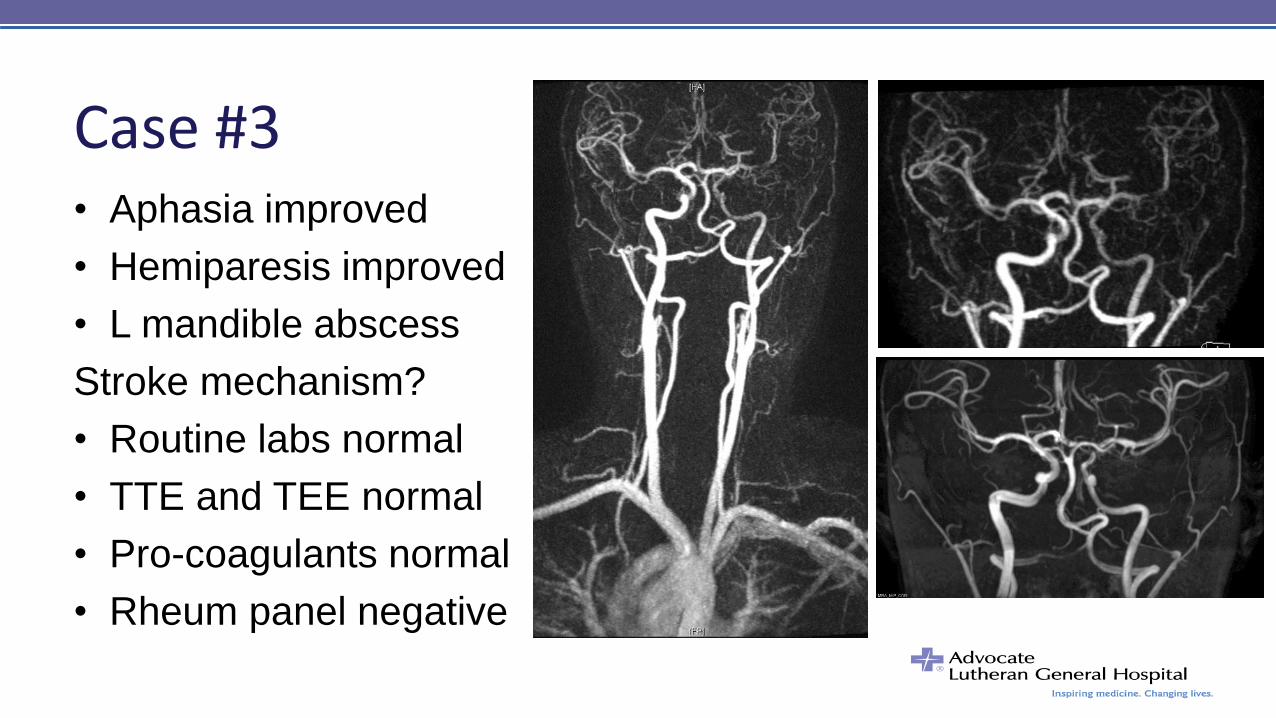
Case #3 • Aphasia improved
• Hemiparesis improved
• L mandible abscess
Stroke mechanism?
• Routine labs normal
• TTE and TEE normal
• Pro-coagulants normal
• Rheum panel negative
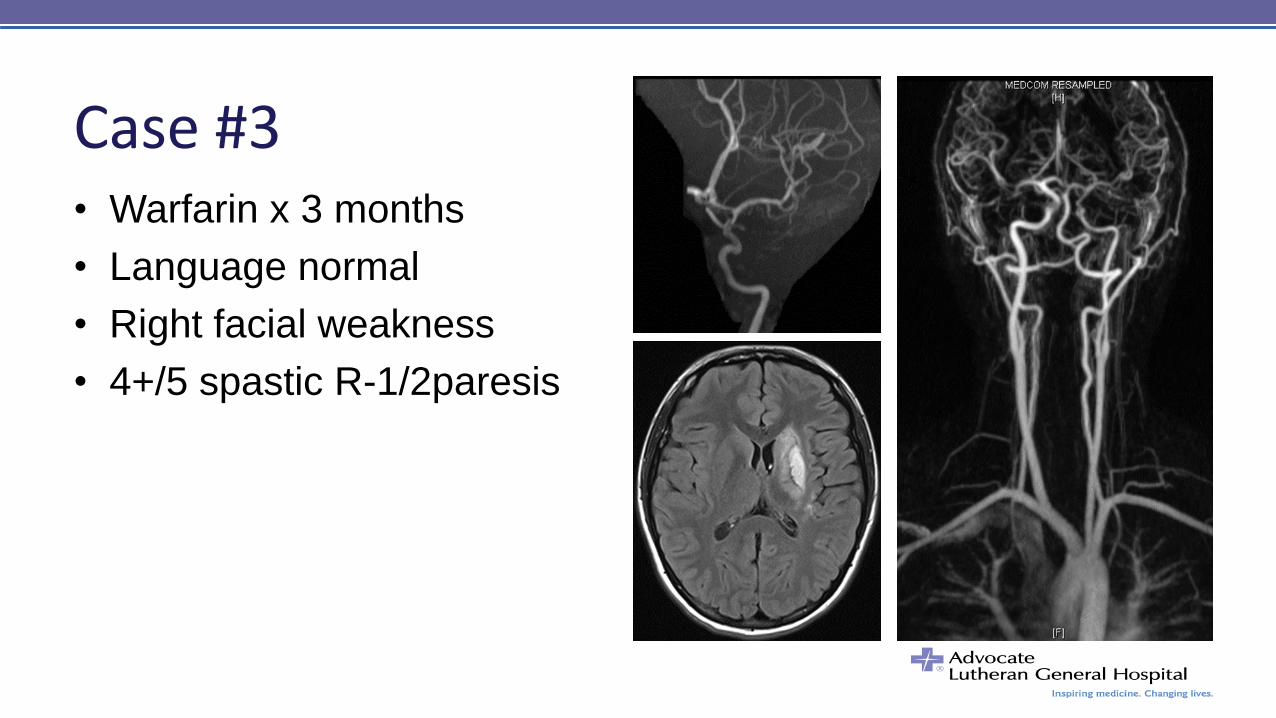
Case #3 • Warfarin x 3 months
• Language normal
• Right facial weakness
• 4+/5 spastic R-1/2paresis
Case #4 • 27 y/o RH woman presenting with persistent headache and
multiple daily episodes of:
– R arm and leg heaviness
– R hand numbness and paresthesia
– Bilateral tunnel vision R>L
– symptoms are independent, last 3-5 minutes, sudden onset/offset
• 5 months ago intermittent L arm and leg numbness
• 2 months ago, 3-5 minutes of expressive aphasia
Case #4 • No medications or PMH
• FH stroke in the elderly, no coagulopathy or pregnancy losses
• ½ PPD x8 years, quit 2 months ago
• Normal vitals, body habitus, and general examination
• MS and HIF intact
• L>R papilledema with L retinal hemorrhages
• Normal motor, sensory and cerebellar exams
• Normal tendon reflexes, flexor plantars, normal gait
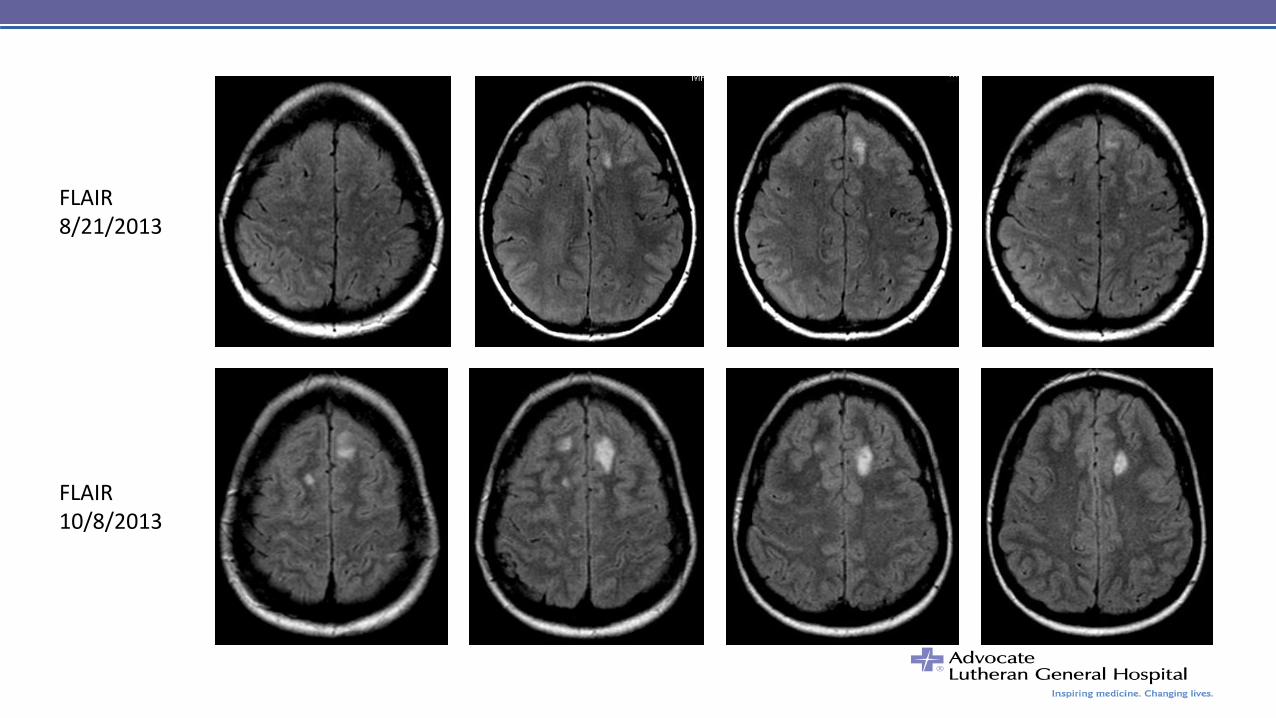
FLAIR 10/8/2013
FLAIR 8/21/2013
Case #4 • Factor V heterozygous, MTHFR heterozygous
• Pro S, Pro C, AT III, prothrombin genotype, b2, ACL, LA
• Heparin --> enoxaparin --> warfarin x 6-12 months
• 2 months later:
– Daily headache, intermittent visual loss, leg weakness, ataxia
– R>L florid disc edema and right temporal field loss
• INR 2.5 warfarin --> enoxaparin
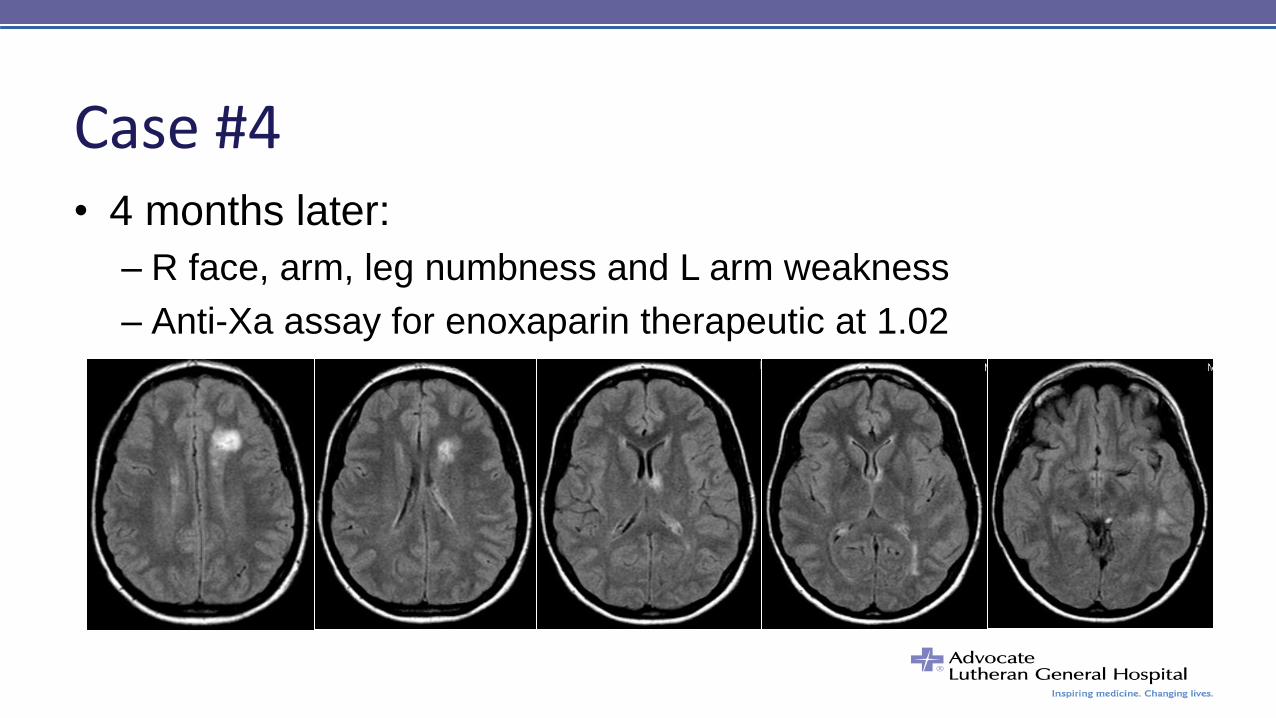
Case #4 • 4 months later:
– R face, arm, leg numbness and L arm weakness
– Anti-Xa assay for enoxaparin therapeutic at 1.02
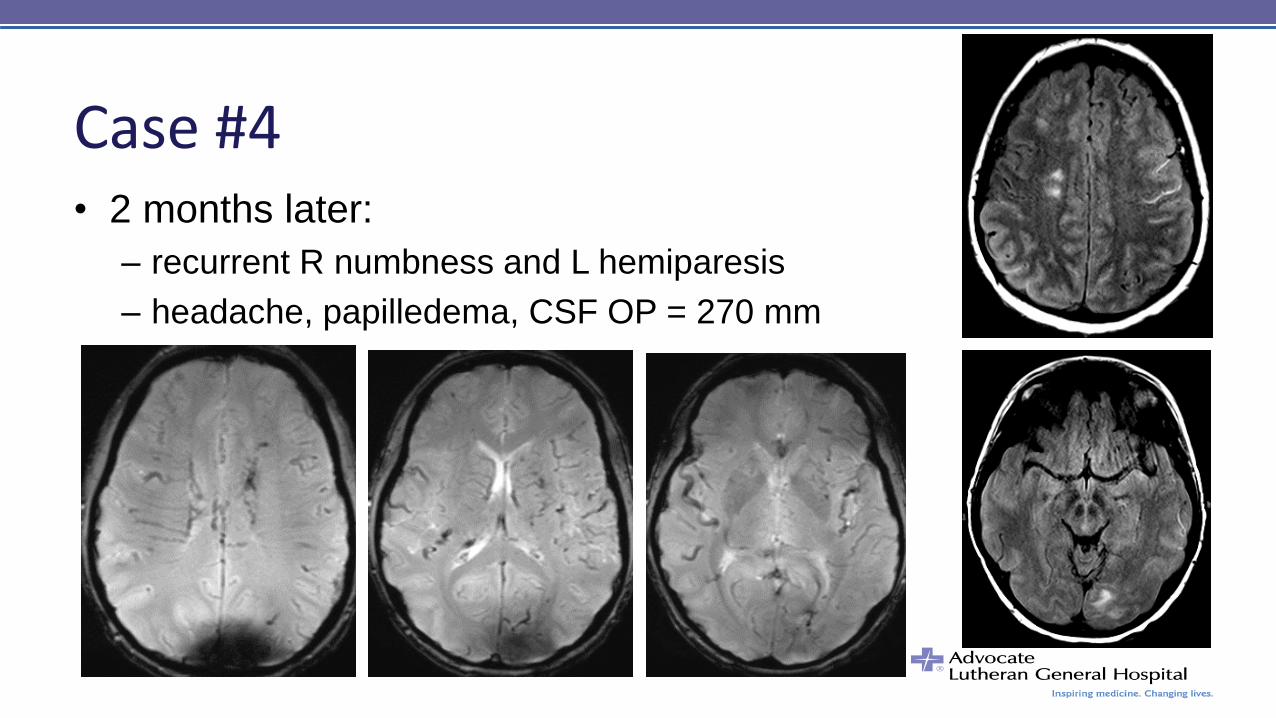
Case #4 • 2 months later:
– recurrent R numbness and L hemiparesis
– headache, papilledema, CSF OP = 270 mm
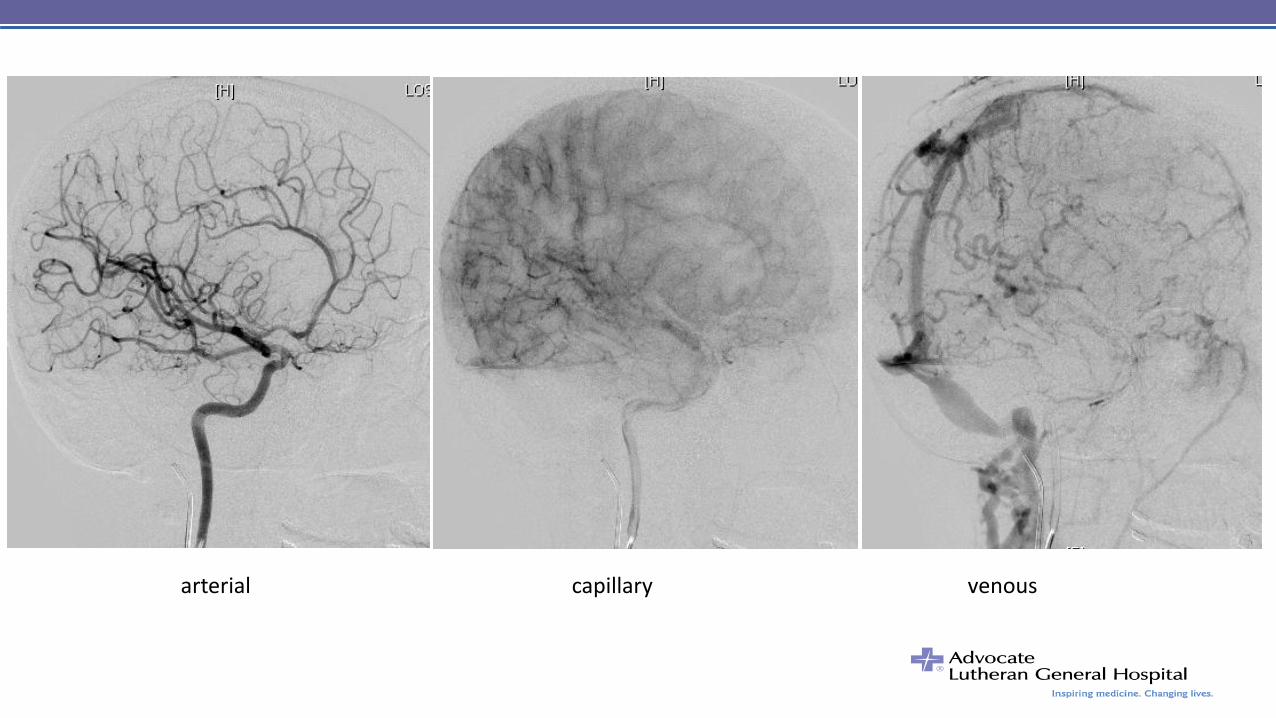
arterial capillary venous
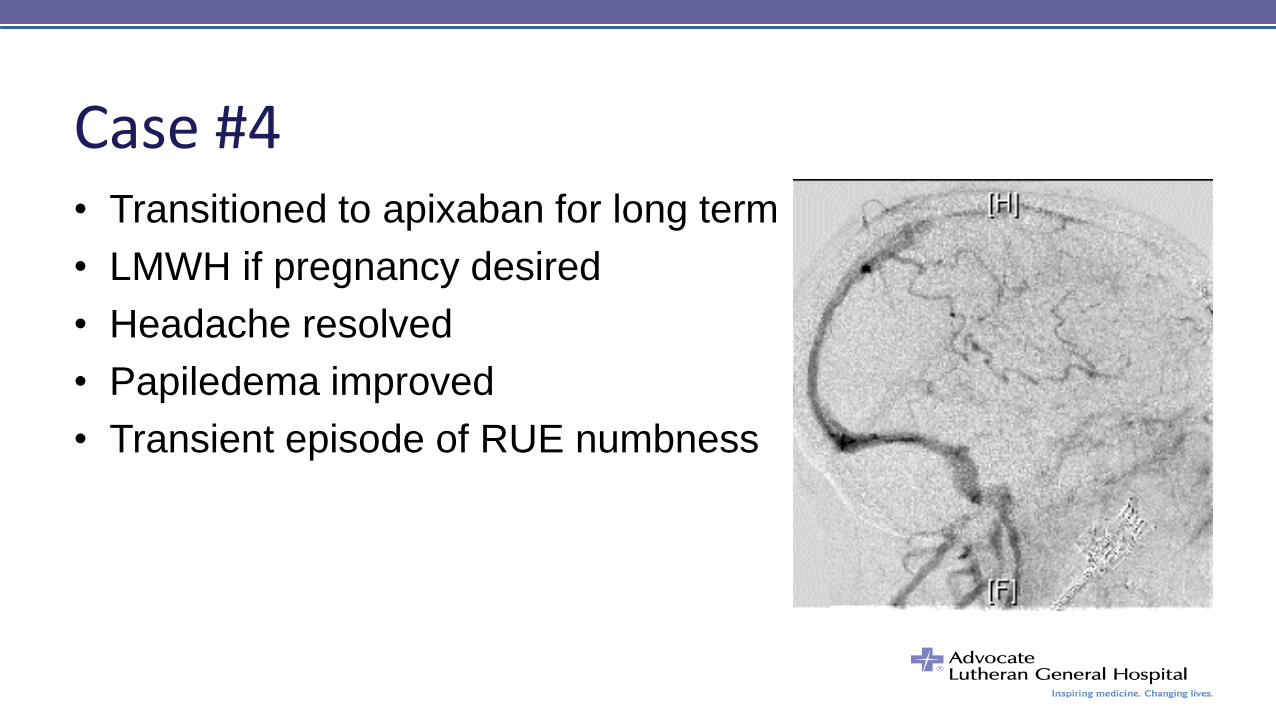
Case #4 • Transitioned to apixaban for long term
• LMWH if pregnancy desired
• Headache resolved
• Papiledema improved
• Transient episode of RUE numbness
Closing Remarks • Maximum 3.75 hours AMA PRA Category 1 Credits
– Participation in the entire activity
– Evaluation form: advocatehealth.com/cme
– Print or download CME certificate
• Maximum 3.75 ANCCA Contact Hours
– Attendance of the entire event
– Evaluation form and certificate
Thank you to our organizers, speakers and participants!