Embed Size (px)
Citation preview

ED 102 891
TITLE
INSTITUTION
SPONS AGENCY
PUB DATENOTE
EDRS PRICEDESCRIPTORS
IDENTIFIERS
DOCUMENT RESUME
HE 006 241.
Toward 'Quality Health Care. The Improvement ofNursing and Nursing Education in Texas. CB StudyPaper 24. Final Repork of the Nursing ProjectCouncil.Texas Coll. and Univ. System, Austin. CoordinatingBoard.National Institutes of Health (DREW), Bethesda, :d.Div. of Nursing. 6
Jan 75189p.
HF-S0.76 HC-$9.51 PLUS POSTAGECUrriculum Evaluation; *Higher Education; *MedialEducation; *Nurses; *Nursing; *Statewide Planning;Statistical Data*Texas
ABSTRACTThis report of the Coordinating Board's Nursing
Project Council is the culmination of three years' intensive effortto provide the State of Texas with a plan on which those responsblefor helping meet the health care needs can rely in determining whitenurses are needed, what their educational preparation should be, Indhow the nurses can be utilized for maximum efficiency. The study ladeinquiries of registered nurses, vocational nurses, physicians,nursing students, and others who could be expected to provideinformation on t%e subject. Discussed in this report is: a profil4ofnursing in Texas, utilization of nurses, nursing education (needsandcurriculum analysis), regional perspective,' cooperative approach 10meeting nursing needs, difinition of terms, and a selectedbibliography. The appendixes include statistical data on the stateof nursing by region and selected copies of survey instruments usefor the many surveys incorporated in this study. The intent of thitreport has been to provide reliable direction for agencies,institutions, ana professional organizations interested in improviignursing education and delivery of health care. (Author /PG)

av)C\I
BEST COPY AVAILABLE
WITOWARD QUALITY HEALTH CARE
The Improvement of Nursing and Nursing Education in Texas
CB Study Paper 24
Final Reportof the
Nursing Project Council
U S DEPARTMENT OF HEALTH.EDUCATION A WELFARENATIONAL INSTITUTE OF
EDUCATIONTHIS DOCUMENT HAS BEEN REPRO()LICE() ExaCTLY AS RECEIVED FROMTHE PERSON OR ORGANIZATION ORIGINATING IT POINTS OF VIEW OR OPINIONSSTATED 00 NOT NECESSARILY REPRESENT OFFICIAL NATIONAL INSTITUTE OFEDUCATION POSITION OR POLICY
Presented toCoordinating Board, Texas College and University System
January 17, 1975
This study was supported by NIH Training Grant Number 06-D-000032-03as a Special Project Grant from the Division of Nursing
Public Health Service

Coordinating Board Members
Harry Provence, Chairman Dr. James P. HollersWaco San Antonio
Newton Greshani, Vice ChairmanHouston
Ford D. Albritton, Jr.*Bryan
Jack ArthurStephenville
Robert W. BakerHouston
Tony BonillaCorpus Christi
Dr. G. V Brindley, Jr.Terridle
0. H. ElliottAustin
r.
Mrs. Jess HayDallas
Harold HerndonSan Antonio
L. B. Meaders*Dallas
Fred H. MooreAustin
Richard S. SlocombGalena Park
Wayne E. ThomasHereford
Harvey WeilCorpus Christi
Watson W. WiseTyler
Marshall Formby Sam D. Young, Jr.Plainview El Paso
* Gov. Dolph Briscoe on January 17 appointed Mr. Albritton to fillthe unexpired term of Mr. Meaders. who resigned on January 3.

FOREWORD
This final report of the Coordinating Board's Nursing Project Council' isthe culmination of three years' intensive effort to provide the State of Texaswith a plan upon which those responsible for helping meet the health care needscould rely in determining where nurses were needed, what their educational pre-paration should be, and how the nurses can be utilized for maximum efficiency.The study made inquiries of registered nurses, vocational nurses, physicians,nursing students, and others who could be expected to provide information onthe subjects in this study.
I wish to express the appreciation of the Coordinating Board to the membersof the Nursing Project Council, under the able leadership of Mrs. John T. Jones,Jr., and the thousands of nurses, students, physicians, and lay individuals whoassisted in this work. A special expression of thanks is owing to the Divisionof Nursing of the Public Health Service, which funded this study, and especiallyto Miss Lois Federico, Nurse Consultant, and Mrs. Ellen McDonald, Nurse Director,who provided outstanding guidance throughout this work. c.
From the beginning of this work, the Council members performed in a mannerwhich made them a credit to their several professions and to this study. ThisProject and the citizens of our State are the beneficiaries of the dedicatedparticipation of individuals from nursing, medicine, administration, and generaleducation. This final report represents the best judgments and conclusions ofthose individuals.
The Coordinating Board and I are pleased to have been thehost agency ofthis Project. While we realize no single st y will solve all the problems inthe delivery of health care, we believe this r port provides the basis for changeand improvement in nursing education and resou es in our State.
yrom the beginning of this work, our intent has been to provide a reportwhich would4be reliable for its users and which would-provide direction foragencies, institutions, and professional organizations interested in improvingnursing education and delivery of health care. We therefore submit this reportto those with whom the responsibility for implementation is shared.
Beviugton ReedCommissioner

Tnerbittattng NanaTEXAS COLLEGE AND UNIVERSITY SYSTEM
NURSING PROJECT
November 30, 1974
co Mr. Harry Province, Chairman, andMembers of the Coordinating Board
Box 12788, Capitol StationAustin, Texas 78711
Dear Mr. Provence:
Having been charged by the Coordinating Board in 1971 with conductingcomprehensive study of nursing education needs and resources in our state,
under a Special Project Grant from the Division of Nursing of the Departmentof Health, Education, and Welfare, the members of the Nursing Project Coun-cil have now completed their work and are pleased to submit this final re-port for your consideration.
, On behalf of the Council, I want to express our sincere appreciationfor the Board's decision to serve as the host agency for this study andfor the support you and Commissioner Bevington Reed have given us through-out the three years o. our work.
As the Chairman of the Council, I had the pleasant experience of work -`ling with a dedicated group of Texans who never faltered, throughout the longmonths of this study, in their determination to make the best decisions forthe future. Our work was materially assisted by the excellent staff whichwas provided by the Board.
I am especially appreciative of the contributions to our work of theReview and Evaluation Committee who devoted so many hours of their time inthe preparation of this report. It is indeed a rare experience to workwith nurses, nurse educators, physicians, and hospital administrator; whoput the interests of the people of the state foremost in all their dblibtr-ations. We, the citizens of our state, are indebted to these fine peoplefor their service.
Sincerely yours,
4.1W4.444-ittit
(Mrs. John T. Jones, Jr.)
iii

BEST COPY AVAILABLE
PREFACE
This study was initiated by the Coordinating Board in 1971, followinga request by the Joint Executive Committee on Nursing Needs and Resourcesof the Board of Nurse Examiners, the Texas League for Nursing, and the TexasNurses Association. The Coordinating Board was approved for a Special ProjectGrant by the Division of Nursing in 1971 and the Commissioner of Higher Educa-tion employed a staff to conduct the study and appointed the Nursing ProjectCouncil to provide professional guidance and assistance.
Mrs. John T. Jones, Jr., Chairman of the Nursing Project Council, appointedthree task forces to examine selected problems in nursing and nursing education.At the beginning of the final year of the study, she appointed the Reviewand Evaluation Committee from Council members to work closely with the staff inpreparation of preliminary recommLndations for consideration by the Couhcil.
During the three years of the study, there were six major surveys conductedby the staff as recommended by the task forces. Nearly 20,000 individuals par-ticipated in the surveys of this study, including practicing nurses, nursingstudents, physicians, nursing educators, and lay individual . We feel that therecommendations in this report reflect the predominance of attitudes of thosewho participated.
Because of the great volume of data collected, we found it necessary tocondense the amount included in this final report. We have included criticaldata which will be useful for those who will examine nursing needs and asso-ciated problems at the local level. The Project collected and analyzed a con-siderable amount of data and information about the regions in the state but wepoint out that it was impossible to gather all the information about many var-jables which influence the demand for nurses, especially at the local level.
The 21 Planning Regions, as identified by the Governor's Office of PlanningCoordination, formed the geographic unit for assembling data because of the widevariations of population, availability of nurses and health care facilities andother factors across the state. We have examined the resources in each region,identified the chief problems and made recommendations for solution. These rec-omendations cover a wide spectrum of subjects, from improvement of faculty togreater availability of off-campus courses to improved communication between ed-ucators and the employers of nurses. We believe this final report provides thefirst step in that effort. It is imperative that successful implementation ofthe recommendations related to joint activities between education and serviceinvolve the full cooperation of both to achieve the common goal .of improvedhealth care for the public.
We have limited ourselves to projections to 1980; our projections from 1980to 1990 were less valid than those to 1980 and the staff therefore recommends .
that the formulas used here for determining need be applied in 1980 to projedtspecific needs fOP the following decade.
Our work has also been limited to the basic preparation levels; a compre-hensive study of graduate nursing education is needed but our time and resources,plus our priorities, did not allow us to parallel our baccalaureate and belowstudy with one for graduate education.
v

COORDINATING BOARD NURSING PROJECTCOUNCIL MEMBERS
Mrs. John T. Jones, Jr., ChairmanHouston, Texas
Miss Sue Alder, R.N.*,Chief ConsultantHealth Occupations EducationTexas Education AgencyAustin, Texas
Dr. Robert K. Bing, DeanSchool of Allied Health SciencesUniversity of Texas Medical
Branch at Galveston
Miss Billye J. Brown, R.N., DeanThe University of Texas
School of Nursing at AustinAustin; Texas
Leonides Cigarroa, M.D.*Laredo, Texas
Ted Forsythe, M.D., ChairmanTMA Committee on NursingLubbock, Texas
Dr. H.J. Friedsam, DeanSchool of Community ServicesNorth Texas State Univers'tyDenton, Texas
Dr. LaVerne Gallman, DeanScott and White Department of
NursingMary Hardin-Baylor CollegeBelton, Texas
Dr. Margaret Harty, R.N.Vice President for the
Institute of Health SciencesTexas Woman's UniversityDenton, Texas
Miss Renilda Hilkemeyer, R.N.Director of NursingThe University of Texas M.D.
Anderson Hospital and TumorInstitute at Houston
Houston, Texas
*Deceased
Dr. Virginia Jarratt, R.N., aeanHarris College of NursingTexas Christian UniversityFort Worth, Texas
Max E. jOhnson, M.D.San Antonio, Texas
Mrs. Elizabeth Jones, R.N., DeanThe University of Texas
School of Nursing at HcistonHouston, Texas
Mrs. Eunice King, R.N.Administrator of Patient
Services and EducationAmarillo Hospital DistrictAmarillo, Texas
Mrs. Clo McGill, R.N.The University of Texas
School of Nursing at San AntonioSan Antonio, Texas
Mr. William J. Perry,Jr., DirectorTechnical-Vocational ProgramsCollege of the MainlandTexas City, Texas
Mr. Boone Powell, Jr., FACHAPresidentHendrick Memorial HospitalAbilene, Texas
Mrs. Gerry White, R.N.Former DirectorDivision of Associate Degree
NursingEl Centro CollegeDallas, Texas-

ADMINISTRATIVE ORGANIZATIONOF
NURSING PROJECT COUNCIL
Review and Evaluation Committee
Mrs. John T. Jones, Jr., Chairman
Ted Forsythe, M.D.Miss Renilda Hilkemeyer, R.N.Dr. LaVerne Gallman, R.N.
;. Elizabeth Jones, R.N.Mr. Boone Powell, Jr., FACHAMrs. Gerry White, R.N.
Task Force on Continuing Education
Dr. Margaret Harty, R.N., Chairman
Mrs. Clo McGill, R.N. Mrs. Elizabeth Jones, R.N.
Task Force on Education
Dr. Virginia Jarratt, R.N.
Miss Sue-Alder, R.N.Dr. H.J. FriedsamDr. LaVerne Galloon, R.N.Dr. Margaret Harty, R.N.
, Chairman
Mrs. Elizabeth Jones, R.N.Mr. William J. Perry, Jr.Mrs. Eunice King, R.N.Mrs. Gerry White, R.N.
Task Force on Utilization
Miss Billye J. Brown, R.N., Chairman
Dr. Robert K. BingLeonides Cigarroa, M.D.Ted Forsythe, M.D.Mr. Boone Powell, Jr., FACHA
Nursing
Mrs. Clo McGill, R.N.Miss Renilda Hilkemeyer, R.N.Max E. Johnson, M.D.
Forrest E. Ward, Ph.D., Project Director
Carolyn qillmore, R.N., M.S.N.,Associate Director
vii
Charles L. Gouge, B.B.A.,Systems Analyst

rA
CONTENTS ,
Page .--ca
Foreword
A
Preface
Procedures and Methodologies 1
A Profile of Nursing in Texas 15
Utilization of Nurses 35
dursing Education
Existing Needs in Nursing Education 45
An Analysis of the Curriculum Objectivesof Selected Professional Nursing Edu-cation Programs 67
The Regional Perspective: Projections andRecommendations 79
A Cooperative Approach for Meeting NursingNeeds in Texas 123
Definition of Terms 129
Selected Bibliography 135
Appendices
A. Statistical Data on the Status of Nursingby Region 143
B. Selected Copies of Survey InstrumentsUsed by the Nursing Project
Survey of Mobility and Utilization Patternsof Professional Nurses 173
Student Curriculum Questionnaire 174
Physician Opinion Survey of NursingEducation and Utilization 175
Survey of Licensed Vocational Nurses 177

Student Mobility Questionnaire 179
Survey of Utilization Patterns of RN's andLVN's Employed in Hospitals 181
Student Curriculum Opinion.Survey 1§5
-12

CHAPTER I
PROCEDURES AND METHODOLOGIES
Following the selection of staff and appointment of the members of theNursing Project Council, it became necessary to 'Syntheslze the objectives ofthe ProjeCt for the purpose of working, toward goals which would be achievableand which could be clearly understood by those who would be involved in theimplementation of the findings and recommendations of the study.
The Council and staff ,believed that the final report of the Nursing Pro-ject, Having been administered by the Coordinating Board, would have greeterimplications for implementation than previous statewide studies. This beliefwas based upon the possibility that, if the findings were acceptable, a sub-stantial portion of the recommendations could be implemented through the Board
The Coordinating Boalt!Iv , having coordination responsibility over all pub-lic senior institutions and over the academic programs in community colleges,is in a. strategic position to not only implement parts of this final reportbut to wog)( with the agencies and organizations concerned with nursing to se-cure implOmentation of those recommendations which are outside the Board's
jurisdiction.
Successf41 implementation of the findings of this study will require ahigh level of selfless cooperation from nurses, nurse educators, and employersSeveral of the recommendations will require changes which will be difficultfor some institutions to make. In some cases, the surveys and other, data col-lected and analyzed by the staff and the Review and Evaluation Committee in-dicated that, with changes being made, the improvement needed in providingqualified nurses on a statewide basis could be achieved.
As in most studies of this magnitude there were differences of opinionamong those responsible for making the fundamental decisions in this report.
, Not all members of the Council agree with all the recommendations but all thatare included in'this report have the support of a majority or more of the mem-
bers.
/WM
After carefully examining the overall objectives of the Project, the Coun-cil agreed that those listed below were appropriate and upon implementationwould provide invaluable guidance apd direction for the nursing segment of thehealth care system for future years. We have annotated each objective for
clarification.
A. To projectp on the basis of currently discernible trends in health caredelivery, the future roles of pursing personnel.
While future roles of nursing personnel are almost entirely'speculative, the Project throughout its work emphasized im-proved quality. This is achievable, in the opinion of theCouncil, by increasing the numbers of qualified RN's in worksettings and the granting of greater responsibility to the RNin patient care. We have adopted the principles of the ex-panded role for baccalaureate nurses and berieve an improvementin health care will result.

B. To determine the most effective method of utilization of available nursingpersonnel.
The utilization survey of hospital nurses demonstrated discrep-ancies between educational preparation in this service sectorfor registered nurses.. We have recommended changes for both ed-ucation and' employers.
To determine the probable qualitative and quantitative future nursing needsof the State of Texas.
Through our regiOnal analysis of re-licensure and practitionerdata, and through our mobility surveys, we projected the poten-tial 'supply of registered nurses in all regions to 1980. In
those regions where the need appeared to remain high with supplyin decline, we have recommended new progrrns or increased enroll-ments in existing programs. We have also recommended that somecourses, such as geriatrics, be more available. Upor adoptionof the optimum ratios of registered nurses to hospital beds, nur-sing home beds, physicians, and other service settings, we havelaid the foundation for increasing numbers of registered nursesto practice in all work areas and, in the judgment of the Council.,this will cause a direct improvement in quality of nursing care.
D. To appraise the current supply of nursing personnel and the existing nurseeducaLion programs.
. Current enrollments in registered nurse programs are at an all--time high in this state and most of the programs are unable toaccept a41 qualified applicants. The vagaries of career selec-tion on the part of young people can cause this high level ofinterest, in nursing to decline. Despite this risk, we have pro-jected enrollments through 1980 as remaining stable.
Our research into the quality of RN programs centered on the dif-ficulty many graduates experience in gaini-ng licensure. This prob-
lem ti's several causes, including inadequate preparation'of faculty,especially for ADN programs, and insufficient clinical experiencefor students.
Under the optimum ratios, the supply of registered nurses willneed to increase in most of the regions of the state. The pro-
cedures leading to the increases are couched in the recommenda-tions.
E To develop a plan fcr nursing education consistent with potential healthneeds and social developments in the state with maximum utilization of edu-cational resources and technology to,:mprove the effectiveness of educa-
tional process.
This entire report addresses the potential health care needs ofthe citizens of this state and is,flexible so that as new needsand social developments occur, they can be met through the inter.:
action of the educational and service elements of the system. In

a time when more clinical experience is being recommended, forexample, we believe new and effective methods must be developedfor providing increased experience benefits for nursing students,even if it requires utilization of clinical resources during un-
popular shifts, specifically at night.
F. To prepare a guide for general education at all levels emphasizing itsrole in the development of a nursing manpower pool.
We feel that this study report, in its final form, is an effec-tive guide to general education for several reasons. First, it
points out that our existing system does not in all cases pro-duce the kinds of nurses required by employers, and that nurseeducators, in many instances, feel that the talents and abilitiesof their graduates are not utilized and that inadequate recogni-tion is given to the intensive educational preparation of nurses.
We have recognized and acknowledged these attitudes in this study
and some of our recommendations to "close the gap" between educa-
tion and service are offensive to some. We have endeavored inthis work to seek that which is needed, not that which is popular.
G. To develop a plan to progress from the current status to the goals to be
established for appropriate intervals to 1990.
The statistical lase of the Project was verified by the staff and
we realize that projectiong must be as scientifically valid as
possible. We halve no control ovir unanticipated CRhnges in health
care outside the recommendations in this report. If there is ac-
ceptance at all levels, and by all agencies of th6 fundamental prem-
ise that we must improve quality of health carelcand if the state
is willing to support the increased costs of .,.oviding it, then
we believe that our projections will result in adequate numbers
of qualified nurses in the state and that the goals will be met.
To develop a plan for continuing education to foster each individual's
professional development.
Continuing education for nurses of all types is more vital today
than ever before. It is second in importance only to the basicpreparation leading to state boardlicensure. We believe con-
tinuing education should not be left solely to chance; we believe
that it is of greatest urgency that the active nurse, regardless of
age, educational preparation, or economic status, must continue
her nursing education throughout her career.
We recognize that much good work has been done in continuing
education for nurses by many institutions. Most of this effort
has been funded through grant funds and when the funds are termi-

nated, so does the effort. This state is without an overall planfor continuing education for nurses, and we in the Nursing Projectconcluded that we must provide recommendations upon v.'fich a state-wide, coordinated'system of continuing education could be based.
In any study of this nature, the limitations in terms of time and resourcesmake it necessary to establish priorities which will influrize the nature of thefinal product. The Coordinating Board's Nursing Project is no exception. Thereare many important issues related to both education and practice which the Pro-ject would havt. liked to consider in greater detail. Those familiar with thecurrent problemt and issues within the, nursing profession will be aware of thesegaps. However, two criteria which influenced the approach to the study were:1) th9 need to place particular emphasis on areas of nursing in which the Coor-dinating Board is directly involved and 2) to place particular emphasis on pro-blems which affected the largest proportion of practicing nurses.
As a result of these priorities, the main body of data deals with methodsof determining needs for numbers of schools, their location and size, and areasof curriculum in which practitioners suggest greater emphasis. Since the major-ity of registered nurses work in hospitals, this area of practice was surveyedseparately. However, in other surveys, nurses working in all other_ categoriesof practice had an opportunity to react to questions relating to responsibilitiesgiven them in their places of employment, to discuss their future educationalplans, and a variety of other questions which are in the survey instrument inthe appendix of this report.
As a result of the priorities of the Nursing Project, the majority of recom-mendations are necessarily directed toward nursing education. This is not to saythat all of the problems of,nursing are caused by or can be solved by nursing ed-ucation. The Council feels strongly that there are equally serious needs in thepractice area which need to be addressed to a greater degree than was possible inthis Project and only when educators, practitioners and employers accept equal re-sponsibility for cooperative problem solging will any real progress, be made.
The decision to concentrate on areas in which the Coordinating Board wouldhave the ability to implement recommendation: required a re-evaluation of the orig-inal objectives and recognition that achievement in some areas, particularly theidentification of effective utilization patterns, would not be accomplished.
The Council members were divided into four task forces with specific assign-mknts to recommend kinds of information that were essential for long- range -plan-
ning in nursing. Based on input for theSe task forces, the Project staff devel-oped a series of studies designed to provide-the data needed by the Council ac-cording to the identified priorities. These were. for the purpose of providingspecific information, not previously available, coLc.arnthg nursing in Texas. Abrief description of each of these is included and copies of the survey instru-ments are provided 14 the appendix. Extensive use was made of existing resourcesof data, related literature and similar studies conducted in other states.

Regional Analysis of Data
So that statewide data collection and analysis could be kept within man-ageable proportions, the Project utilized the Governor's 21 Planning Regionsas the critical unit of geography and population to be analyzed as an entity.These regions had been established by the Governor's Office, Division of Plan-ning Coordination in 1971, and although the number was later increased to 24,we used the original 21 in order to keep our data consistent throughout the.Project.
Statistical data and other information was collected and analyzed for eachof the 21 regions. This data included population characteristics, aging index-es, availability of hospitals and nursing homes, locations of LVN and RN educa-tional programs, numbers of nurses working in various settings in each county,and various nurse/population ratios. This information was recorded on a seriesof maps and charts. As additional information from other surveys was completed,it was incorporated into the regional profile if appropriate. This method wasparticularly helpful in comparing the regions and determining degree of need inspecific job settings.
Nurse Licensure Data
The Nursing Project acquired re-licensure cards from the Board of NurseExaminers and from these we computerized statistical data on the number of RN'sin each county, their activity status, age, educational preparation, and areaof employment.
The Board of Vocational Nurse Examiners also provided licensure cards to
the Project for 1970-71, 1971-72, and 1972-73. Information, similar to thatfor RN's, was provided concerning the LVN's in Texas.
Student Geographic Mobility Survey
12)/In order to plan for the number and locations o professional nursing pro-
grams needed in the future, information was needed about the students themselves.
A survey was designed to answer questions concerning geographic mobility patternsexhibited by students in choosing a school and choosing a job location followinggraduation. Such information was necessary to determine the recruitment areas ofvarious types of schools as well as the area in which the graduates of the school
preferred to work. In May, 1972, a questionnaire was administered to over 6,300students in 44 professional nursing programs in Texas. In April, 1973, a similar
questionnaire was administered to 3,556 students who had entered professional pro-grams since the first survey was administered.
Hospital Utilization Survey
The demands placed upon a nurse as a result of job requirements have vitalimplications for the educational preparation of all nurses. In conducting a
survey of utilization practices, the Project was concerned with two aspects ofthe discrepancy between education and practice; 1) what are nurses expected todo that their education has not prepared them for? and 2) what skills and abil-
ities does the educational process develop but which the graduate is seldom able
to utilize?
4
17

Because approximately 64 percent of active nurses are employed in the hos-pital setting, this area was chosen for sury purposes. A 10 percent sample ofshort-term, general hospitals in Texas was se ected which was representative ofall regions and various categories of numbers of beds per institution. Out of
56 hospitals contacted, 42 responded. The participants included RN's and LVN'swho had been licensed five years or less. A total of 1,882 questionnaires weredistributed and 956 responses were received.
RN and LVN Practitioner Surveys
In order to obtain mobility and utilization information from a cross-section of nurses, a survey was sent to a sample of 10 percent of registerednurses in active practice in the state. Analysis of the sample indicated thatit was representative of the planning regions as well as the various areas ofnursing practice (public health, nursing homes, hospitals, offices, other). A
total of 2,591 questionnaires were mailed and 1,183 responses received. A sim-
ilar survey was distributed to LVN practitioners using the same, sampling tech-nique. A total of 2,934 questionnaires were mailed and 923 responses were re-turned to the staff.
Physician Opinion Survey
A 'survey of physicians was conducted to determine utilization practices inthe office setting as well as to obtain information concerning the attitudes ofphysicians toward current trends in nursing education. A sample of 10 percent
of non-federal physicians was chosen. The total number of questionnaires mailedwas 1,500 and the'number returned was 430.
Continuing Education Offerings
A survey of professional nursing programs, public health Agencies and pri-vate health agencies was conducted to determine the extent of continuing educationfor nurses available in the state. Out of 109 questionnaires mailed 80 responseswere received.
Curriculum Objectives Study*
The need for a study of curriculum objectives resulted from several spe-cific situations which are of concern to the nursing profession and the public.First, the existence of three types of educational programs, all culminating inthe title "RN", has produced extensive controversy as to the differences in theabilities of the graduates and the ways in which they should be utilized. Whilethese differences are usually described in broad terms, no one seems able to ex-plain how much or what specific content is common to the various programs. Thispresents problems to the individual who wishes to seek a higher level of educa-tional preparation. The end result is usually a loss of credits or a loss oftime to the student. Secondly, because of the increasing mobility of our popu-lation, a high percentage of students attend more than one institution beforeobtaining a degree. If our educational system is going to meet the needs ofthe public it will be necessary to design nursing programs whose courses cantransfer with minimum difficulty.
* Curriculum objectives are the elements of a course or curriculum which studentsare expected to learn and to apply in practice.
6
18

In order to identify the common elements of various programs, the NursingProject designed a study of the behavioral objectives developed by each program.All participating programs coded their objectives, following a format preparedby the Project staff. A sample of this information was analyzed by computerand verified by the staff to determine how many and what type of objectiveswere common to the various types of programs.
Student Opinion of Curriculum
As a supplement to the Curriculum Objectives Study, 25 percent of thesenior nursing students in all professional programs were surveyed to deter-mine opinions on the effectiveness of the curriculum as a whole, teaching me-thods used, usefulness of objectives and suggestions for improvements. A
total of 857 questionnaires was distributed and 580 received from those whoparticipated.
Procedures for the Application of Survey Results
As data began to accumulate, a six-member Review and Evaluation Committeewas appointed by the Chairman for purposes of working with the available infor-mation and preparing preliminary drafts of information to be considered by theCouncil. Over a period of nine months this committee held seven two-day meet-ings to review material compiled by the staff. Following presentation of theirfindings to the Council on June 29, 1974, necessary revisions were completed andthe final recommendations were submitted for approval by the Council on August9, 1974.
From the beginning of the Nursing Project in 1971, both the Council andthe staff have been committed to planning for the future nursing needs of Texas,recognizing that consideration must be givento the effect of current trends onhealth care delivery. Although we cannot accurately predict all the changesthat are going to affect the health industry, some trends are apparent andcan be used to project needs in certain areas.
In evaluating the area of supply and demand for nursing services in Texas,the Nursing Project has looked at each region of the state in light of its par-ticular characteristics and needs. In order to do this, information was col-lected on a county-by-county basis and covered many variables including currentpopulation, population projections, size of age groups, numbers and sizes ofhospitals, number of RN's and LVN's working in specific areas, educational prep-aration of nursing personnel, and locations and types of nursing schools.
So that the educators and health care providers in the state could work
toward ever-improving quality of nursing personnel, the Nursing Project devel-oped a series of optimum ratios of registered nurses to various elements in thedelivery of nursing services. The process folloWed in developing these ratios
is described below.
Procedures and Rationale for the Optimum Ratios
The process for determining need for registered nurses was one to which
members of the Review and Evaluation Committee devoted a considerable amount
fj.'"719

of thought and effort. Following extensive discussion-of possible approachesto this problem the decisior was made to use ratios of nurses to a series ofvariables as the basis for projecting future need for professional nurses.This decision was made with the knowledge that when planning on a statewidebasis, it is impossible to collect the detailed data which would provide themost accurate estimate of need at the local level. For example, individualhospitals cannot rely solely on RN's to beds to determine their staffing needs.They must consider the types of health services offered, the conditions of theirpatients, and the financial factors affecting the number of people whom theycan employ in various categories. In spite of the limitations of this approach,the ultimate inclusioh of a large number of variables in the determination ofneed makes it far more reliable than a simple RN to population ratio.
The members of the Review and Evaluation Committee examined the currentratios of nurses to population, to hospital beds, to school children and tophysicians. Then each drew up a suggested series of ratios which, he felt,would provide an improved level of hetlth care and yet be realistic in termsof budgetary and staffing requirements. When these independent evaluationswere compared, ,they revealed general agreement concerning ratios. From thesea single set of preliminary ratios was adopted. Members of the committee thendiscussed the proposed ratios with providers of health care in their own com-munities to determine the overall level of agreement with the committee.
Following a discussion of ,the results of this action, revisions were madeand a final set of ratios for projecting future nursing needs was adopted.While the adopted ratios reflect the Wumber of nurses needed to provide a moreacceptable quality of nursing care than now exists, they have been judged to berealisticin terms of oudgetary limitations by a group of experienced health careproviders, including physicians, directors of nursing service, hospital adminis-trators and nursing educators. The ratios and rationale are given below.
RATIOS ADOPTED TO DETERMINE PROJECTED DEMAND FOR RN'S*
Hospitals:
Unit ofComparison
1971-72 Ratiosof RN's to Each
Variable
R & E Committee'stOptimum Ratios
beds 4-
6 - 24 beds 1:4.00 1:325 - 49 beds 1:5.30 1:350 - 99 beds 1:5.30 1:3100 - 299 beds 1:3.30 1:2300 -A99 beds 1:2.77 1:2500 + beds 1:2.77 1:2
.Nursing Homes beds 1:47.3 , 1:15School Nurses students 1:1,815 1:1,200Office Nurses physicians 1:6.00 1:5Public Health population 1:11,531 1:5,000Other population 1:6,250 1:6250
*Sources for these data are in the Selected Bibliography at numbers 9, 18,44, 52, 54, 55 and 56.
i. 't:f 2°

In determining staffing for hospitals and nursing homes, the stated ratiosreflect the numbers of nurses needed for 24 hours or three shifts. For example,in a 30 -bed hospital, at a ratio of 1:3, 10 RN's would be needed to staff thehospital at an optimum rate for a 24-hour period. This figure includes person-nel to provide for adequate relief coverage. The underlying assumption in theratio for larger hospitals is that as the size of the hospital increases, thecomplexity of care and supporting services increases, requiring more nurses forthe same number of patients. An example of this would be a hospital with RN'semployed in areas other than patient divisions such as rehabilitation facili7ties, irradiation therapy departments, nurse epidemiologists, inservice educa-tion or renal dialysis services.
A second assumption of the committee was that by increasing the number ofregistered nurses per bed it would be possible to reduce the number of non-professional nursing employees per bed. This ratio is intended to reflect achanger in the quality of personnel providing patient care and not simply toincrease the total quantity of persons engaged in this activity. Therefore,the adoption of this particular series of ratios has implications for all typesof nursing educational programs as well as patient care institutions.
The most drastic recommendation in the series of ratios came in the areaof nursing home staffing. It was the opinion of the committee that geriatricpatients, by virtue of their frequently complex health care problems, requirethe care of registered nurses. Although the field of geriatrics is not present-ly a popular one among the majority of registered nurses, it is an area whichmust be improved if adequate care is going to be made available to the elderlysegment of the population in Texas.
Ratios were adjusted for school nurses, public health nurses, and officenurses to provide for an improved level of care. Office nurses will be dis-cussed in greater detail in connection with the survey of physician's opinionson nursing functions in the office and educational preparation of nurses..
The "Other" category in the series of ratios was included as a means ofallowing for new and expanding roles for nursing which are becoming more fre-quent. This category also includes those who are practicing primate duty nur-sing. At the present time there is one private duty RN for every 6,250 popula-tion. However, over the past few years the number of nurses doing private dutyhas steadily decreased. With the current trend toward intensive care Units forpersons in need of specialized care, it appears that the number of private dutypractitioners will continue to decrease. The number of nurses with specializedpreparation as nurse practitioners in various clinical specialties is increasing.
Several nurses have established independent practices and the role of thenurse in such hpaith care delivery systems as Health Maintenance Organizationshas the potential for development into an area of expanded practice. The Com-mittee believed that these trends have an offsetting effect and that by provid-ing one professional nurse in the expanded role for each 6,250 persons as theratio, 'the needs in these special settings could be met.
0

In order to determine the needs for registered nurses in each region,the ratios were applied to each category of nursing employment and the totalnumber of nurses needed was computed. This figure was then converted to anRN/population ratio and applied tc the projected population for that regionfor 1980 and 1990. Although there is no totally accurate way to predict need,this method is designed to reflect the level of health care which the partic-ular region is able or willing to support. Since the application of ratiosis applied to projected populations there is a built-in adjustment for in-creasing numbers of hospital beds and nursing positions in other settings.
The following example shows how the application of the ratio can resultin different nursing requirements for two regions which have similar numbersof hospital beds but different sizes of health care facilities.
AN EXAMPLE OF OPTIMUM STAFFING REQUIREMENTS FOR A REGIONAS INFLUENCED BY THE HOSPITAL BED-SIZE DISTRIBUTION
Bed-Size Classification
Number of reds by Bed-Size Categony
REGION A REGION B
744 0
760 54
172 104
324 2060 6200 1 016
6
25
50100300
500
- 24 beds- 49 beds- 99 beds- 299 beds- 499 beds+ beds
2,000 2,000
Number of RN's Reguired to Staff
6 - 24 bedsi 248 0
25 - 49 beds 253 18
50 - 99 beds 57 35
100 - 299 beds 162 103
300 - 499 beds 0 31L
500 + beds 0 508720 PT
In any study of statewide resources and projected goals there must bea clear distinction between "need" and "demand". In this Project "need" isdefined-as the number of.nurses required to provide a desired level of healthcare which is considered economically feasible. "Demand" is the number ofnurses which providers of health care are willing or able to employ to pro-vide a certain level of care. Ideally the two terms should be interchangeablebut this is seldom the case.
.1%10 22

In this study, the accuracy of the projections of need for nurses is de-pendent upon the willingness of health care providers to work toward an im-proved level of nursing care by seeking to have a greater proportion of directpatient care provided by registered nurses.
If such a goal is not adopted by providers of health care, the projectedneeds can be reduced considerably. For example, the 1971-72 ratio of RN's tonursing home beds was 1:47 and the desired level adopted by the Council is1:15. If such a goal is adopted by nursing homes the state will need threetimes the present number of RN's working in that setting. If nursing homesare unable or unwilling to employ registered nurses to reach such a goal therewould be no reason for the state to prepare three times the present number ofnurses in the field of geriatrics.
Projection of Supply
Based on the Student Mbbility Survey and the RN Practitioner Survey, theProject was able to estimate the number of new graduates who would remain ineach region, the number who would move to other regions, and the approximatenumber who would remain in active practice depending on the,type of educationalprogram from which they graduated. By multiplying the size of the graduatingclass of each-type of program in the region by the number of years until 1980and applying the formula as illustrated in the chart below, it was possible todetermine the probable number of new nurses which would be available in the re-gion. This number, added to the number of nurses already active, minus a per-
REGION APROJECTED RN SUPPLY PATTERN, 1980
Diploma Associate Degree Baccalaureate
Local Graduates*x
464 804 1,782
Regional Retention Rate** .875 .869 (.509) (.560)
Local Graduiies Retained 406 699 935
Inflow 32 63 166
Total New Graduatesx
438 762 1,161
Activity Rate .97 .97 .94
Total Projected Additional 425 + 739 + 1,035 2,199Active RN's by 1980
*The projected number of local graduates is based on a nine-year period, from1972-1980, inclusive.
**Retention rates are for each'individual nursing program within the region.
23

centalge who could be expected to become inactive due to retirement producedthe projected supply by 1980. This figure was then compared to the predictednumber needed to determine how well the region could be expected to meet itsneeds. This process is demonstrated in the chart presented below:
REGION APROJECTED DEMAND VS. PROJECTED SUPPLY BY DIFFERENT DEMAND CRITERIA LEVELS
(FTE)
RN's/100,000 NumberPop. of RN's
Conver- Requiredsion by 1980
PresentNumber
ofActive-RN's =
Status Quo 208 2,554 2,402
Optimum Level 348 4,273 2,402 1,871
1980 Population 1,228,0001990 Population 1,316;400
Addi-tional
RN's Re-qui red
TotalAddi-tional
Age RN's Re-Attri- quiredtion. by 1980
Projec-ted RNSupply SurplusBy 1980 (Deficit)
152 549 701 2,199
549 2,420 2,199
1,498
(221)
With the current rapid rate of change in society, even a relatively shortsix-year projection may need to be re-evaluated at intervals in light of emer-ging'trends. The projections of,supply and demand presented in the regionaldata section of the report should be considered as the batic framework forplanning to meet local or regional needs. Local health care providers haveaccess to information about health needs in the area that was not availableto the Project. Such information may indicate a somewhat greater or lesserneed than that identified in this study. However, for statewide planning pur-poses, the approach described here appears to be a reliable way of determin-ing the needs of Texas to improve its - current level of nursing care.

t.
I. MAO Oar
UPPER 8
RIO
GRAI4DE
t.
bar w. LI114,151111111.....11..40411
7LOPN ../P7I No
--PANHANDLE%WM , 11.1 amnia Sew wag fill
4..N'.
44 44
TEXAS PLANNING REGIONS
September 1971
!
" TEXAS...,1.1.4.11 ! I
woo , 4`"1" ...op.., tr./.
I 94': ..1.17'94NvEST CENTRAL
1EXAS-74-.
1.. #0410.1,4"."I
-110CONCi-.16-4.1
-4,-
rale%
1,11.01
t ,OL
1,11IL.., I.
b... 1. 116.2
../
tt 040
ALAMOL-17-v,0.4.4 .111PUB La' "'I
Ian* 4110 11.461,14
1..mm..
C01,1 AVAILABLE
441.4e.
NORTH...ft 106 4.
...7CCENTRAL
,..1
NORTH EAST.."--TEXAS
-
.." tIMM
(44.,
T'EXIAS
ON
-.4 44
,110
yC t 111.E.?(AS ta
r1 it
.eP Ant
"RAZOS....
TEXAS
A. ;fir
.014 Mt I
\CENTRAL
.4
25 14
4,401.4 04,01
-19SOUTH
Ws ....CA
CAPITALNA/.4
Nt.
410.,
vanoliOt
6OLF,COAST :"."
1.11116We*
Oftte. 0. 6.11 / ±GOLPERESCENT...
....
501.4.1
Ilbw le
.4.4
QAtTAL.'BEND--
201 --IL.
TEXAS
L"40,4001
LOWER RIOGRANDE VALLEYJ
SOUTH EASTTEXAS
ro

CHAPTER II
A PROFILE OF NURSING IN TEXAS
Describing the current status of nursing in Texas by use of statewidestatistics can be deceptive because of the inability of the statewide approachto account for the wide variations in several characteristics from one regionto another. Although the staff and the Council of the Nursing Project agreedthat the primary unit of analysis throughout the study should be the region,statewide statistics are useful as a basis of general comparison with otherstates.
The purpose of this chapter is'to present an overview of Texas nursingstatistics along with some additional information about the state itself whichaffects the preparation of nurses and the practice of nursing within its boun-daries.
Texas is a large state, having a maximum length of 801 miles and maximumwidth of 773 miles. The state has a great range of geographic and climate con-ditions, varying from the hilly piney woods eastern portion to flat coastalplains on the south to the arid great plains area of West Texas. The popula-tion of the state is 80 percent urban and 20 percent rural and most of the urbanpopulation is east of the 100th meridian, a north-south line forming the easternboundary of the Texas Panhandle.
The three principal ethnic groups in the Texas population are Anglo-Ameri-can, Blacks, and Mexican-Americans. The Anglos are throughout the state and are'in the majority in most regions. The Mexican-Americans comprise 40 percent ormore of the population in all the counties bordering on Mexico, and in all theplanning regions adjacent to the Mexican border. The Blacks comprise 25 percentor more of the population in at least 25 counties in East Texas. Most all ofthese counties have low income levels and health care facilities are inadequate.
East Texas (Regions 5, 6, 14) is hilly, heavily wooded, has numerous lakesand recreational areas and has few large towns but many small farming communities.
The upper Gulf Coast area (Regions 15, 16, 17) includes two large industrialareas, Houston and the Beaumont-Orange-Port Arthur complex. Much of the surround-ing area is farmland and flat coastal plains.
The southern portion of the state (Regions 19, 20, 21) has the metropolitanarea of Corpus Christi, large expanses of sparsely populated ranchland and the
semi-tropical "Valley". In the southernmost tip a large proportion of the popula-tion is Mexican-American and many migrant workers come from Mexico during crop'harvests.
The central strip of the state (Regions 4, 11, 12) is one of the most dense-ly populated segments of Texas and is projected to have a considerable populationincrease over the next two decades. Region 18 is heavily populated in the easternportion which contains the metropolitan area of San Antonio. However, the western
and southern areas are sparsely populated. A large proportion of the populationis Mexican-Kmerican: The climate is often hot and dry.
26 '

The western part of the state (Regions 1, 2, 3, 7, 8, 9, 10) also haslarge expanses of sparsely populated territory. The climate is relativelydry. Much of the rural area is devoted to ranchland and towns are often smalland far apart. This is particularly true in Region 8 which is primarily moun-tainous. The major West Texas cities of Amarillo, Lubbock, Abilene, El Paso,San Angelo, Midland, and Odessa are widely scattered and range in populationfrom 59,000 in Midland to 322,000 in El Paso.
RN and LVN Supply
For the 1971-72 licensure year, the total number of professional nurses'registered in Tec:as was 49,213. This total included nurses living and workingin other states who maintain a Texas license, and nurses who are temporarily"inactive or permanently retired. Of the total number registered in the statesonly 25,868 indicated they were active in nursing in Texas.
In addition to the licensed professional nurses practicing in the state,there is an increasing number of foreign educated nurses who have migrated to .
Texas but have not been successful in meeting licensure requirements. Thereare no accurate data on the number of these nurses working in this state but thenumber applying for the licensing examination increased from 61 in July 'of 1970to 568 in October of 1972. The issue of unlicensed foreign nurses and the qual-ity of health care will be discussed in Chapter III.
National data indicate that for the entire United States in 1972, there were380 active RN's per 100,000 population and 390 in 1973. By comparison, Texas wasshown to have 240 (4:12).2 However, according to the Nursing Project's data,the 1971-72 ratio was only 214. Among the states the ratio ranges from a lowof 190 in Arkansas to highs of 572 in New Hampshire, 579 in Connecticut, 612in `Vermont, and 673 in the District of Columbia.' Although figures such as thesemake it appear that Texas has a critical shortage, it 's premature to draw suchconclusions without first looking at the circumstances contributing to theseratios and the factors tnat make the situation in Texas somewhat different. The
population density along the east coast makes the existence of large medicalcentexs and specialty health services much more feasible than would be the casein sp011ely populated areas. In thdkDistrict of Columbia and the surroundingareas, military hospitals and federat health agencies employ unusually largenumbers of nurses which partially accounts for the high patio in this area.
Among the various regions in Texas the ratio of full-time equivalent RN'sto population varies considerably from a high of 255 in Region 16 to a low of,101 in Region 19. However, evaluation of the need for professional nurses ina particular region must take into consideration other types of health carepersonnel available. Texas has 629 general hospitals of which approximately50 percent are less than 50 beds (35:29). Many of these smaller hospitals arein small communities where recruitment of RN's is difficult and a large propor-tion of nursing care in the smaller hospitals is provided by licensed vocation-al nurses. In regions where the RN/population ratio is highest, the LVN/popu-
'Professional nurse, as used in this report, refers to a graduateassociate degree, or baccalaureate program in nursing.
2This citation form will be followed throughout this report. Therefers to the bibliographic listing and the second to page number.'
r27l11
of a diploma,
first digit(s)0

I
lation ratio is usually lower. In regions where the RN/population ratio islow, the ratio of UN's is higher. On a statewide basis, however, the RM/LVOL.ratio is1approximately 1:1. This ratio is similar to other southern statesbut forthe nation as a whole there are usually considerably more RN's thanLVN's in active practice.
In 1970, the number of nursing personnel per 100 hospital patients forall the states ranged from 88 in New Jersey to 127 in Alaska. However, themajority ranged from 92 to 102 with Texas having 95.3 (4:27). States with highRN/population ratios appear to have relatively low numbers of personnel per 100hospital patients. For example, Massachusetts, with an RN/population ratio of649 has only 97.9 nursing personnel per 100 patients. However, of those 97.9,45.9 are RN's. In Texas only 16.4.out of every 95.3 nursing personnel areRN's. Since the 1963 Surgeon,General's Consultant Group on Nursing recommend-'ed that at leist 50 percent of direct patient care in hospitals,be providedby RN's, these facts point up a critical issue where Texas is concerned (44:23).
If one of the objectives of the state is to increase the proportion of carebeing given by registered nurses, some ch'anges must occur. Since the stateappears to be producing similar numbers of total nursing personnel, as otherstates, the problem is not to produce more.of all kinds but more professionaland fewer vocational nurses. .
With the recent expansion of professional nursing programs in the community col-leges across the state, the problems of access and cost have decreased ccinsider-ably for many individuals who would have.previously entered vocational nursingprograms.
Since much of the nursing care in Texas is given in small hospitals insomewhat rural areas where registered nurses seldom choose to practice, the LVNremains an .essential meter of 'the nursing team./ However, with the increase innumbers of professional,programs and the large numbers of applicants to thoseprograms, Texas should no longer find it necessary to rely to such a great ex-tent on vocational-nurses to provide the majority- of dtrett
/pa lent care.
Nursing Education. ,
The configuration of education programs for RN's in the state has changedconsiderably over the, past seven years. The total number of programs has in-creased from 35 .in 1966 to 43 in the fall of 1973. Because of the extendedcampuses operated by some of the state universities, the total number of cam-puses offering professional nursing programs is actually closer to SO. The mostobvious change has"c6the in the numbers of diploma and associate degree programs..
Two state universities,. Texas Woman's University and The University ofTexas, offer master's and doctoral degrees in nursing. The University of Texasis offering nursing courses at the graluate-level on the Galveston) Auttin andImAntonio campuses,,and Texas Woman's University offers graduate courses onrrr campuses in Denton, Dallas, and Houston.
The changes in numbers of nursing education programs in the state, bytype of program, are shown bete for the period 1966 through 1973:
A
1 I.
2817-

NUMBER OF PROFFSSIONAL NURSING PROGRAMSIN TEXAS,' 1966-73
1966 1968 1969 1970 1971 1972 1973
Baccalaureate 7 9 10 10 11 12 12
Associate Degree 5 18 23 20 20 23 24
Diploma 23 19 14 14 10 10 7
TOTAL 35 46 48 44 41 45 43
For the two-year periof 1970-71 and 1971-72 there.were 167 master's degreesin nursing conferred by the'two programs. This number should increase with re-cent expansion of graduate..campuses.
Total enrollment in professional nursing programs preparing beginningpractitioners in Texas was 11,579 in the fall of 1973. Enrollments increasedat a rapid rate during the period from 1966 to 1972 and appear to be maintain-ing the trend.. Historical enrollments since 1966.are shown here:
ENROLLMENTS IN PROFESSIONAL NURSING PROGRAMS, 1966-1973
1966 1968 1969 1970 1971 1972 1973
Baccalaureate 1,472 2,878 3,097 3,408 4,098 5,674 6,947
Associate Degree 306 1,313 1,665 2,126 2,668 3,275 3,645
Diploma 1,413 1,845 -1,509 _1,309 994 1,124 987
TOTAL 3,191 6,036. 6,271 6,843 7,760 10,073 11,579
The total number of graduates of professional nursing programs more thandoubled over the past six years. A continuatfab of this rate should result in
a rapid increase in the RN/population ratio over the next few years since the
rate of population growth is much less. Graduations since 1966 were:
GRADUATIONS FROM "ROFESSIONAL NURSING PROGRAMS, 1966-1973
1966 1968 1969 1970 1971 1972 1973
Baccalaureate 240 324 390 453 471 597 738
Associate Degree 40 86 307 511 608 859 1,006
Diploma 434 513 500 425 365 348 412
TOTAL 714 923 1,197 1,389 1,444 1,804 2,156
218 f- /J

The impact of the sudden increase in enrollment over the past three yearsshould soon be apparent in the employment sector, particularly in the metropol-itan areas. Although employers can identify problems of shortage of profession-al nurses in these areas now, it is expected that over the next five- years theproblem will decrease. If the schools are going to be producing adequate num-bers of nurses within the next few years, there is a potential danger of creat-ing an oversupply if additional programs are started to meet the shortage,: oftoday.
In 1972-73, 132 vocational nursing programs were in operation in the statewithia total enrollment of 4,906. Of these, 71 were hospitai operated, 28 werelocated in community colleges, 27 in public schools, and six in other job set-ings. There were 2,672 new vocational nurses licensedwin the year 1972-73.
Characters' *44s of Practicing Nurses
The following series of graphs gives the most recent information availableon professional and vocational nurses in active practice in Texas. In coopera-tion with the Board of Nurse Examiners and the Board of Vocational Nurse Exam-iners, the statistical information was obtained from license renewal cards.
Employment Status
Out of the total number of RN's registered in Texas in 1971-72, only 52.57percent (25,868) were active in the profession in the state of Texas. Of thetotal number of active nurses, 78.7 percent (20,361) were employed full timein Texas. Of the total number of LVN's livingin Texas, 63.13 percent wereactive. Of the total number of active LVN's, 85.56 percent are employed fulltime. fhis condition of a high rate of inactivity is characteristic of theprofession primarily due to the fact that the majority of inactive nurses arewomen who find it necessary to temporarily discontinue full-time employmentwhile they raise their families. Efforts to reduce the size of the inactivepool of nurses have met with little success ,and at the present time, althoughthere seems to be a slight trend toward remaining active for longer periods,there is no indication that the situation is likely to change to any signifi-cant degree. The data given in the figure shown below reflect the variousactivity levels of active RN's:
INPLOVIIENT STATUS OF ACTIVE R.N.,s LICENSED IN TEXAS BEST CRY AVAILABLE
IS-)11 NoarsrlIaalt
Lots then IS Moore/Wash
loomplata Data
Total
1271 - 157S
&SAM
30 19
/s11 -Tins
y2.712
It:
1140 Masers/lisek
12.1132
7.142
Lets ThaniS Naurvflibe
Imanplata 1.212

Showrj below are the activity levels for LVN's in the state:
SPECIFIC EMPLOYMENT STATUS OF ACTIVE LVN'SLIVING IN TEXAS, 1972-1973
Full This 23.116S
Less them Mrs./Wk 542
- IL Mrs./Wk 1,235
16 - 30 Mrs./Wk. 2,247
ms Assumes 0
TOTAL 27,853
4.441It Nrs./Wk....m.
Basic Educational Preparation
85.562Full Timm
41.66.1.41$
8.04%- 30 Nrs./Wk.
One of the features of active RN's in Texas is the exceedingly large
-number of diploma program graduates. In 1972, almost 73 percent of active RN's
had received their basic preparation in a diploma program. Baccalaureate grad-
uates accounted for slightly over 15 percent of all active RN's and associate
degree graduates comprised just over seven percent of all active RN's,. These
percentages can be expected to change as the enrollments and graduations of
the three types of programs change. This change is forecast in the number of
graduates in 1972, as shown here:
8SN 597
ADN 859
Dipl. 348
As shown in the numbers of graduates of each type program in 1972, the
number of diploma graduates is declining as the programs continue to be phased
out while the baccalaureate and hssociate degree programs are increasing in
number. The obvious conclusion is that the number of active diploma nurses
will slowly give way to the increasingly large numbers of graduates from the
other types of programs.
The basic educational preparation of registered nurses in practice during
1972 is graphically displayed in the figure shown below:
3120
VIsa

BASIC EDUCATIONAL PREPARATION OF ACTIVE RN'SLICENSED IN TEXAS, 1971 - 1972
BEST COPY MAILABLE
Diplom 18,820
Associate Degree 1.838
loccalmereste 3,11%
incomplete i,316
Incomplete 5.0411
Highest Educational Preparation
BecaLA of the format of the licensure card, the category "No Degree" wasconfusing. The intent was that "No Degree" meant any educational level lessthan a bachelor's degree. However, there is some question as to the way inwhich associate degree holders classified themselves. It is probable that thisproblem accounts for the large number of incomplete responses in this categoryas indicated in the chart below:
HIGHEST EDUCATIONAL PREPARATION OF ACTIVE RN'SLICENSED IN TEXAS, 1971 - 1972
No Degree 15.09
Neccalsereete In Nursing ,134
lloccaleureate In Other Area 512
nester's In Nursing 414
nester's in tither Arse 274
Mosoeate 25
Incomplete Data AnaTotal 25,141
Me Degree
59.492
In templets
19.55%
Seeterete .1011
Master!, In OtherAres 1.0141
ilacca'euneete In 0th.- Artms1.,11
Nester's In Nursing. 1.618

With the increasing availability of graduate courses in nursing in variouslocations in the state there should be a significant increase in the number ofmaster's degrees in nursing over the next few years.
Field of Employment
Hospitals continue to employ the largest number of active professionalnurses, accounting for 64.09 percent, while office nurses and school nursesmake up the next two largest groups. The number of professional nurses work-ing in nursing homes is 1,057 or 4.09 percent of active nurses. This figureis particularly significant since there are 917 licensed nursing and custodialcare homes in the state. The problem will be discussed in greater detail laterin this report but it is readily apparent that in this field there is a greatneed for more professional nurses.
The distribution of RN's among the various employment settings in 1971-72 isshown here:
FIELD OF EMPLOYMENT OF ACTIVE RN'SLICENSED IN TEXAS, 1971 - 1972
Hospital 16.5P0
Nursing Nome 1,057
School of Nursing 1,141
PrIveie Duty 1.097
Public Health 1,220
School Nurse 1,730
Industrial Nurse 614
Office Nurse 1,1910
Other 60
Incumplete
Tot 25.86%
BEST COPY AVAILABLE
Nursing Nome 4.09%
School of Nursing 4.02*
Private Duty 4.24%
'br
Pubilc Health 4.721
School Nurse 6.69!
Industrial Nurse
2.37%
Office Nurse7.002
Other .232
incomoiete2.55%
Hospitals also employ the largest segment of active LVN's in Texas, account-ing for 63.72 percent. However, 17.12 percent of LVN's are employed in nursinghomes. With the exception of the hospitals, in most employment settings nursesare predominantly RN's or predominantly LVN's.. The ideal health delivery systemis one in which there is a proportionate distribution of both types in all jobsettings. One positive approach to reaching this goal has been the recent in-crease in the the utilization of LVN's to provide public health services underthe uirection of registered nurses.
The distribution of the active LVN's in Texas during 1972-1973 according toplaces of employment, both in numbers and percent of the total, is shown here:

BEM CM AVAILABLE
FIELS OF EMPSOTNENT OF ACTIVE L.V.N.'S IN TEXAS'
1972 - 1973
hospital 17.774
horsing Home 4.776
Private fluty 1.544
Public health 251
School Nurse 143
industry 117
Office Nurse 2.566
Other 507
No Response ley
TOTAL 27.295
I
61.722hospital
17.12%
Nursing Nome
9.272Physlcisn'siffIcs
1
Living I. Tames
These data clearly show that LVN's are employed in those areas of greatestneed, hospitals and nursing homes. Almost 81 percent (22,500) are working inthese institutions.
Employment Positions Held by Registered Nurses
Of the active professional nurses in the state, over 44 percent classifiedthemselves as general duty or staff nurses. When one combines the levels of"head nurse or assistant", "supervisor or assistant", and "administrator orassistant", the total is 40 percent. This appears to show thatwthere is aboutone supervisory nurse for every staff nurse and we believe that' this conditionis not the case in practice and that there are several possible explanations forthe distortion. Such staff alignment would be uneconomical and wasteful and thedata collected from the hospital survey indicates it is not the true condition.One example of the distortion would be where only one nurse was employed, suchas in a physician's office, where she functioned in a variety of responsibilities.The figure shown below indicates the types of positions held by active RN's inTexas during the year 1971-72:
TYPES Of pOSITIONS NILO Of ACTIVE 4.11.'s LICENSES IN TUNS
1971 - 1972
Administretor er Assistant 1.327
Consultant 2)7
Supervisor or Assistant 6.1$
Instructor 1.114
Mead Morse or Assist/mot 6,6%
General Derr or Staff 11.419
Other 1,6711
Incomplete
Total ass'
BEST COPY AVAILABLE
Administrators,Assistant 9.13$
Consultant .112%
34
16.001
lestruster 18.90

FINDINGS RELATED TO SUPPLY AND DEMAND
Although Texas has a relatively low nurse/population ratio in comparisonwith'other states, there has been gradual improvement over the past few years.from 188 per 100,000 in 1966 to 214 per 100,000 in 1972. With the current in-crease in the number of professional nursing programs along with expandingenrollments in many older programs, the predicted ratio will increase to 301by 1980 end 362 by 1990. Based on the application of optimum ratios, Texasshould require 350 RN's per 100,000 population by 1Q80 in order to provide animproved level of nursing care. According to national predictions, by 1980between 379 and 406 RN's will be available for every 100,000 population (1:5).When the 1972 average ratio was 380 for the nation as a whole, a 1980 ratioof 350 for Texas might seem to be an under-estimation of need. However, giventhe unusually high ratios in a few states that tend to elevate the nationalaverage, and because of the uneven population distribution in Texas, a some-what lower ratio would meet the needs of this state.
Whether or not Texas reaches the predicted ratios of RN's to populationis dependent on the maintenance of current levels of enrollment. There areseveral factors which could have an effect on the present projections andshould be kept in mind. If current rates of production lead to an over-supplyof nurses in the most popular job settings it could easily cause a decrease inenrollments. Secondly, the recent cutback and other changes in federal fundingto nursing programs and nursing students could also serve to decrease enroll-ments or make the establishment of new programs less feasible for colleges anduniversities.
Student Geographic Mobility
During the spring semester of 1972, the staff conducted a survey of studentsin nursing programs in the state to determine geographic mobility patterns. Thestudents in 44 nursing programs participated and of the 5,305 students enrolled,4,504 returned the survey instruments to the staff for analysis. The surveytherefore included '71.4 percent of nursing students enrolled that semester.
Of the 4:504 students who responded, 88 percent were Texas residents atthe time they applied for admission to their nursing programs and 12 percent(456) were from out-of-state. Of the 456 out-of-state students, 57 percent (262)were enrolled in baccalaureate programs, 26 percent were enrolled in ADN programs,and 17 percent in diploma programs. Of the out-of-state students enrolled in BSNprograms (262), some 44 percent were enrolled in three programs, one publiclysupported and two privately supported (TWU and Baylor and TCU). The figure be-low shows the residence status of the 4,504 students by type of program:
Texas Out-of-State
Diploma 89.3 10.7ADN 93.6 6.7BSN 86.0 14.0
These data show that Texas residents dominate nursing program enrollmentin programs at the baccalaureate level and below.
35 24

The county of residence of Texas students was tabulated and enrollmentsincluded students from 214 of the 254 counties in the state. Of greater impor-tance was the finding that 40 percent of the total Texas resident enrollmentwas from only four counties and 51 percent from eight counties. The ten lead-ing counties with greatest enrollment of Texas resident students are shown here:
Number ofStudents Percent
CumulativePercent
1. Harris 615 15.46 15.46
2. Dallas 442 11.13 26.593. Bexar 281 7.07 33.66
4. Tarrant 280 7.05 40.71
5. Galveston 121 3.05 43.76
6. McLennan 111 2.79 46.55
7. Travis 96 2.42 48.97
8. Nueces 91 2.29 51.26
9. Potter 83 2.09 53.35
10. Jefferson 81 2.04 55.39
Distribution of Graduates by Type of Nursing Protram
The Student Geographic Mobility Survey indicated that there are distinctdifferences in the mobility patterns of graduates of the various types of pro-fessional nursing programs. These differences have implications for planningwhich are related to locations of schools and functions expected of graduates.
The recruitment area and thr service area for each of the three types ofprograms were identified and the resulting analysis indicated that there is agreater difference among the recruitment areas of the three types than amongthe service areas. Although the ADN programs indicated a much smaller recruit-ment area, it was the only type which had a service area larger than its re-cruitment area. A schematic representation of comparative size of the twoareas for each type program is shown here:
TYPE OF PROGRAM PRIMARY RECRUITMENT AREA PRIMARY SERVICE 'AREA
(MEAN DISTANCE IN MILES) (MEAN DISTANCE IN MILES)
Diploma 57.5
Associate Degree 29.9
Baccalaureate 101.6
ar
36 25
35.9
34.8
46.7

The characteristics of recruitment of students and distribution of grad-uates, as shown in these diagrams are important factors in projecting the supplyof nurses throughout the state to 1980. Other characteristics of each type pro-gram have a significant effect which require further description.
Most of the BSN programs in Texas are located in metropolitan areas anduse some of the best clinical facilities in the state. The students are usuallysingle and recruited from throughout the state and earn the baccalaureate de-gree whicA has potential earning power above that of the shorter programs.The graduates have shown a preference for employment in the larger cities whereprofessional opportunities are more attractive.
Most of the ADN programs are located in community colleges and small univer-sities where clinical resources are more limited than those in urban medical cen-ters and hospitals. Enrollment in these programs tends to include large numbersof married students who live in the surrounding community. The average ADN stu-dent is older than the average BSN student and usually does not have the timenor resources to move to another location to attend school.
The diploma program student, as shown on the diagram on page 24, tends tocome not only from the community where the program is located but also from out-lying communities. The six diploma programs still in operation are in Abilene,Amarillo, Austin, Lubbock, San Antonio, and Tyler. The small service (employ-ment) area is attributable, in part at least, to the long-standing popularitydiploma graduates have with employers. Students who enter diploma programs areusually in pursuit of a career, not a college education.
Thee totals represert enrollments in all three types of regictered nurseprograms. When the data were displayed by type of program, the following resultswere observed:
TEN MAJOR COUNTIES OF RESIDENCE BY TYPE OF PROGRAM
Diploma
LubbockEl PasoTarrant 249HarrisJefferson 1/3 378Fe TiaT
PotterSmithTravis 1/2
aTlia-11"
Associate Degree Baccalaureate
HarrisDallas 608BexarGalveston 1/3 922guicisTarrantMcLennan 1/2t-rayson
HidalgoWichita
HarrisDallas 1/3 1 627
951TYWirifBexarTrivisDentonMcLennan 1,255Bell
3elfironLubbock
The source of Texas resident nursing students shown above demonstratesthe differences of the recruitment patterns. When the survey was conducted in1972, diploma programs were in operation in seven of the counties providing 50percent of diploma program enrollments; ADN programs were in operation in eachof the counties providing 50 percent of enrollment in that type of program, andBSN programs were in operation in the counties providing 50 percent of enroll-
3 "126 ak
0b

ment in BSN programs. These enrollment sources indicate the impact that theexistence of a program has on enrollment.
Enrollment status in the three types of programs, as measured by the num-ber of full-time and part-time students, varied significantly. The diploma andbaccalaureate programs had part-time enrollments of less than 4 percent whileover 25 percent of associate degree students were part-time. The enrollmentstatus is shown here:
m.........0.1..=nm.41I14.11111.=1".10Mb.,
DISTRIBUTION OF ENROLLMENT STATUS BY TYPE OF PROGRAM
Full-time Part-time
...111MI111
Diploma 97.9% 2.1%Associate Degree 72.8% 27.2%Baccalaureate 96.1% 3.9%
When asked about the preferred county of practice, the results were close-ly correlated to source of students. With the exception of El Paso County, thetop 10 counties were the same, but in different order, as shown below. The stu-dents reported they expected to practice in 152 of the state's 254 counties, butthe most preferred counties tended to be those in which most of the students hadresidence at the time of application to the nursing programs. The most preferted
counties, and the number preferring each county, are shown here:
MAJOR RECEIVING COUNTIES
Percent of
County No. of Students Total Enrollment Cumulative Percent
Harris 772 20.03% 20.63%
Dallas 683 18.95% 38.98%
texar 316 8.77% 47.75%
Tarrant 239 6.63% 54.38%
Travis 136 3.77% 58.15%
Potter 129 3.58% 61.73%
Galveston 113 3.13% 64.86%
Nueces 97 2.69% 67.55%
McLennan 81 2.25% 69.80%
El Paso 66 1.83% 71.63%
Approximately 80 percent of the nursing students indicated practice in Texasthe first year following graduation. Nearly 72 percent were Texas residents re-maining ,in the state while just over six percent were non-residents planning tostay for at least one year of practice. Of the 456 non-residents attending school
over 52 percent plan to practice in Texas.
The preference for practice location, by type of program, is illustrated in
the chart shown here. In the diploma column, five of the ten counties listed
have diploma programs; in the associate degree column, each of the leading coun-
ttts has an ADN program, and in the baccalaureate column, all but one of the lead-ing five counties have at least two BSN programs.
# ,P
3 8 27

MAJOR COUNTIES OF EXPECTED PRACTICE BY TYPE OF PROGRAMAS REPORTED BY STUDENT GEOGRAPHIC MOBILITY SURVEY, 1972
Diploma Associate Degree
(Bexar 1/3
Dallas I 615El Paso
HarrisPotter
Harris
252
Lubbock 1/3 378 GalvestonTravis NuecesTarrant 1/2 Tarrant 1/2BexarSmithJeffersonTaylor
McLennanGraysonPotterWichita
922
Baccalaureate
Harris 634 1/3Dallas gsl" 1/2tnexar 1428 3/4TarrantTravis 85% 1,617
While mobility among professional nurses varies considerably, itappears that the distances involved are probably greater during the firstfew years following graduation. In contrast, the LVN Practitioner Survey in-dicated that 69.2 percent of the respondents were practicing in the same countyin which they had attended an LVN program.
With the majority of BSN programs in the largest cities and the majorityof ADN programs in the smaller cities it would appLur that the rural-urban dis-tribution problems of registered nurses would be minimal. However, a furtherlook at areas of expected practice of graduates of these programs presents someperplexities.
First, each of the three types of nursing education programs is designed,to produce nurses prepared to function in somewhat different capacities. Ideally,there should be graduates of all three programs working together as a team par-ticularly in institutional settings. In the ADN program the emphasis is pri-marily on technical skills and direct nursing care provided in acute settings.Leadership and community health are not emphasized and the graduates are in-tended to work in settings under the supervision of nurses with more experienceor educational preparation.
Diploma graduates, having a longer period of educational preparation, re-ceive somewhat more emphasis on management of large groups of patients and areexpected to function more independently than the ADN graduates. However, theyreceive minimal preparation for practice outside the acute care settings. Thebaccalaureate graduate is prepared to give skilled patient care but also haspreparation.in leadership skills and delivery of nursing services offered inother settings. The program provides a broad base of general education and em-phasizes the underlying concepts, principles and theories essential to nursing.'
Although the theoretical purpose of the ADN program is to prepare bedsidenurses working under the direction of more experienced health team members, two-thirds of the graduates of these programs find themselves in situations wherethey may be the only nurses available and are expected to fill all levels of nur-sing positions regardless of their educational preparation. Since this distribu-tion problem does not appear likely to change significantly, the need to re-evaluall the product of the ADN program in particular should be given consideration.
39284.!. 4;

The prospect that an over- supply of RN's is likely to occur in the largercities in the state is supported by data from the Student Geographic MobilitySurvey which indicated that 48 percent of all new graduates plan to practice inHarris, Dallas, or Bexar counties. With the number of new graduates licensedeach year totaling 2,000 or more, this represents a significant potential in-crease in the supply of professional nurses to the major metropolitan areas.
Inactive Nurses
In the past there has been a tendency to view the pool of inactive nurssas a partial solution to an identified shortage. Based on the fact that themajority of nurses are women, many of whom choose to be inactive while raisinga family, there appears to be little likelihood that the situation wi,41 changesignificantly in the near future. Improvement of pay scales..availability ofchild care facilities, refresher courses, and other incentives may serve toattract some nurses back into practice but for the most part these effortshave not had any significant effects on solving problems of shortages. Whilethe added income may elevate the family's standard of living, it appears thatthose who are voluntarily inactive can maintain a standard of living which isacceptable to them without practicing nursing.
0
Nursing Student Opinion on Length of Professional Service
There were significant differences among nursing students, by type ofprogram, when they were asked by the Project to indicate the length of timethey planned to work in Aursing under varying circumstances. We realize thatthe plans a student has for a career while still in college or in a diplomaprogram can change, and frequently do; we feel that there were enough studentsresponding to this particular portion of the survey that-the results, in lieu ,
of more definitive data, can be useful in making predictions.
As shown on the chart below, approximately one-third (32%) of all nursingstudents who responded plan to practice professional nursing for the durationof their normal career life. Anothdr one-third plan to practice full-time uptilthey begin having children and then work part-time while rearing their children.The variance in these plans is directly related to the type of nursing programin which the student is enrolled. As shown below, nearly one-hal* of the ADNstudents plan full-time employment for the duration of their careers, whileone-fifth (20%) of the baccalaureate students indicated the same plan.
EXPECTED EMPLOYMENT PATTERNS By TYPE OF PROGRAMON OPTIONS LISTED IN STUDENT GEOGRAPHIC MOBILITY SURVEY*
1. To practice nursing full time for the rest of my work life.2. To practic nursing full time before I have a family, then part time
while rearing the children.3. To practice nursing full time before I have a family, stop work while
children are in school, then resume my career.4. To work part time only for the rest of my work life.5. To practice. nursing full time before I have a family, then stop working
forever.6. Do not plan to practice nursing.7. Other.
*The survey tabulations are on page 30.
40 29

PERCENT RESPONDING TO THE SEVEN OPTIONSBY TYPE OF PROGRAM
1 2 3 4 5 6 7 Total
Diploma 29%
_
37% 18% 2% 1% 1% 10% 100%Associate Degree 45% 28% 11% 6% 1% 1% 11% 100%Baccalaureate 20% 41% 26% 2% 1% 1% 8% 100%
on.
Decreasing Contribution
In order to estimate the professional career life of nurses by type ofprogram, the staff developed the NELE (Nurse Employment Life Expectancy) form-ula based on returns from the two Student Mobility Surveys. We based theformula upon the students' responses to the seven career plans listed above.We weighted the first four options, in order, with 100 percent for number one,50 percent for number two, 25 percent for number three, and 12.5 percent fornumber four. When these weighted values were applied to all the responses, wefound that, if a full time career from graduation to retirement was 100 per-cent, the. following percentages, by type of program, are the estimated profes-sional career plans of those in the surveys:
Diploma 62.6%Associate Degree 52 3%Baccalaureate 47.3%
Several factors must be.taken into consideration when interpreting thisinformation. First, the data covers a limited time span of'two years and doesnot necessarily show a trend. Second, it is based on future plans of studentsand may not accurately reflect the actual employment patterns that will occur.Third age has not been taken into consideration. Since a si n ficant propor-tion of ADN students are older than the average age of most-64Fsing students,the remaining number of years befOre reaching retirement age is fewer than formost students in other types of programs.
The chart. on the following page shows the educational background of nurseswho were inactive in 1971-72. The large number of "incomplete" responses canbe partially attributed to the lack of a category for associate degree grad-uates. A second possibility is that the category includes retired nurses whohave been active for most of their lives and do not feel that they fit in aninactive category.
41 30

INACTIVE RN'S LICENSED (!'TEXAS BY HIGHEST EDUCATIONAL PREPARATION1974r - 1972
ET CRY AVillAttE
t
Ile liegres
Oecceleureste In *ursine
Osetelaureste in Other Area
Nester's in Nursing
Nester's in Othsi Area
Oseterete
Ineampteto 4 110
Ttel 9.76
Doctorate .002
IncompleteNo Degree
3,.61%
7
Master's in Other Ares
1.4 n411101:n
OSN
NSII .72
leureste In Other Area2. SS;
Another method of comparing educational preparation and professional in-activity is to arrive at the total number of active and inacti ve nurses in eacheducational category and compute the percent in each category who are inactive,as shown here: 0
Category Percent Active Percent Inactive
Degree 80% 20%BSN 76% 24%BS in Non-nursing Field 69% 31%MSN 86% 14%Doctorate 76% 24%Incomplete Response 55% 45%
Several recent social and economic trends, such as the women's liberationmovement, smaller families, and inflation, have served to increase the numberof women in the work force. Altman predicts that for the nation there will bea slight increase in nurse participation rates in the labor force until 1980,but the rate of increase will be slower than it was in the 1960's (1:5). Thiswas demonstrated in the 1972 Inventory of Registered Nurses which shows_an in-crease in the proportion of active nurses from 65% in 1966 to 69% in 1972.
A progress report on the long-range Nurse Career Pattern Study being con-ducted by the NationaliLeague for Nursing reveals that" contrary to popular be-lief, nurses do not wok for a few years and then leave the profession entirely'to marry and have children. The report shows that five years after graduation76.2% of associate degree graduates were active, 68.6% of'diploma graduateswere activf, and 62.6% of baccalaureate graduates were active:- .
4231

The map shown ;;tow compares the number of active nurses to inactivenurses in each of the regions in the state. The resulting ratio shows thenumber of active nurses for every inactive nurse. The larger the number, thebetter the utilization of the available nursing manpower pool in that area.
NUMBER AND RATIO OF-ACTIVE
RN'S BY REGIONINACTIVE
1971 - 1972
Or,
2.76
State Total 257t6,1716415
geographic Distribution
The rural -urban maldistribution of nurses is a problem for which no effec-tive solution has been proposed. The problem is clearly illustrated by the re-gional statistics in the chart on the:following page.
The figures alone are not indicators of the degree of need for nurses inany particular area. Such factors as the size of the rural' area and the prox-imity to medical facilities in urban areas must also be considered. It is ex-pected that the proportionate number of nurses needed in rural areas will beless than in the cities. Mowevervin Texas, where 50 percent of existinghos-pttals are 50 beds or less and mainly in rural communities, the figurer, do in-dicaU the pr-.Hems involved in recruiting fitilkthese hospitals.
AO4332

RATIOS OF ACTIVE RN'S PER 100,000 POPULATION FOR THE ENTIRE REGION,FOR THE URBAN AREAS ONLY, AND FOR RURAL AREAS ONO
1970 - 1971
Region Entire Region Urban Areas Ru-a. Areas
1 244 376 1422 176 236 1033 192 233 1324 228 233, 214, 246* 137
5 152 149 1536 149 240 1237 173 225 1358 206 212 959 169 166, 222* 147
10 249 314 15511 234 ."----` 278 21012 253 318 12513 153 210 10614 118 No SMSA in Region 11815 228 228 Entire Region is Urban16 266 266, 393* 126
17 163 No SMSA in Region 163
18 214 231 15619 95 115 41
20 159 166 14221 116 112, 122* 96
* Regions with more than one SMSA.
Geriatric Nursing
With the rapid advances in medicine during the last few decades, we haveseen a significant increase in the normal lifespan which in turn results in alarger portion of the population age 65 and over. As a group, this segment ofthe population exhibits the most complex of health care needs. The normal pro-blems of aging combined with the multiple chronic illnesses of many older indi-viduals present some of the most challenging problems in nursing care. Nursingstudents often view their experiences in nursing homes with distaste and commentthat the fieldvf geriatrics is depressing. They appear to prefer settings inwhich the health care provided leads to recovery for the majority of patients.
Responses on the Student Geographic Mobility Surveif,indicated that outof 4,504 students, only 32 wished to practice in nursing homes. Of these, 5were diploma students, 19 associate degree students, and 8 baccalaureate stu-dents. This figure represents .6 percent of potential graduates over the nextthree to four years. Of the 25,868 active RN's in Texas in 1971-72, only 1,057
44 33

were employed in nursing homes. An add'tional 237 indicated they worked ingeriatrics but not in a nursing home. of those who are employed in nursinghomes, many are in administration rather than direct patient care. In thevarious regions, the ratio of RN's to nursing home beds is severely inadequate.The range is from 1:31 to 1:170, as shown here:
RN/NURSING HOME BED RATIOS
Region 1 1:47 Region 8, 1:30 Region 15 1:113
Region 2 1:87 Region 9 1:74 Region 16 1:50
Region 3 1:111 Region 10 1:58 Region 17 1:82
Region 4 1:70 Region 11 1:68 Region 18 1:31
Region 5 1:123 Region 12 1:82 Region 19 1:88
Region 6 1:112 Region 13 1:121 Region 20 1:90
Region 7 1:170 Region 14 1:129 Region 21 1:42
When one considers the above ratios in terms of RN per bed available atany one time, the figures would have to be multiplied by three, eight-hourshifts. This indicates that in the region with 1:170 there would be one RNon duty for every 510 patients. To further compound the problem the 1972-73licensure data indicate that of all LVN's working in nursing homes, 81 percentare charge nurses. The obvious conclusion is that the bulk of direct patientcare is being given by aides in these institutions. Statistics further indi-cate that many nursing homes do not employ any registered nurses for patientcare. The reasons for this can partially be attribut.ed to a shortage of RN'sseeking positions in nursing homes. Economic factom may make it difficultfor nursing home administrators to pay professional sdleries. Whatever theunderlyin'j reasons, this is an area of serious concern f the public is toreceive the quality of nursing care desirable in this setting.

CHAPTER III
UTILIZATION OF NURSES
Over the past several years there has been a growing trend to utilizebaccalaureate nurses in capacities which are referred to by various terms suchas expanded roles, extended roles, nurse practitioners, clinical specialists,and a variety of other labels. Nurses who are working in these capacities areperforming functiogs that, until a few years ago, were not considered the re-sponsibility of the nursing profession. At the present time many nurses acrossthe country are providing primary health care. In the process they make ini-tial health assessments, deal with common health problems as independent prac-titioners, make referrals, collaborate with physicians and other health disci-plines and provide continuity of health services to clients who move from hometo hospital to extended care facility. The evidence that nurses aria wanted andbeing utilized effectively in expanded roles is accumulating rapidly as reportedby Schutt (48).
Nurses functioning in expanded roles are not intended to simply extendthe physician's time or be a physician's assistant. The purpose is to useregistered nurses to their fullest potential. This implies that the nursemakes independent judgements and instigates nursing therapies to solve pa-tient problems that are not normally dealt with by physicians.
In her description of her duties as a nurse practitioner in a neurosurgicalclinic, Leininger described some of the kinds of nursing problems presented.They included problems of activities of daily living complicated by specialdiets, limitations of activity, and difficulty in understanding medicationorders. In her study, the physicians agreed that the quality of health caregiven by both the nurse and the physicians was greatly improved (25:1,275).
In another study,to determine educators' perceptions of the extent to which,nurses are likely to be performing expanded functions, the responses indicatedthey expected from 63 to 71 percent of nurses to be performing expanded functionswithin the next ten years (14)..
Not all nurses are prepared to function in such roles and not all wish toassume the responsibility and accountability for professional practice of this
nature. However, because of the demand for primary care, and the feeling thatregistered nurses can and should assume such responsibilities, an increasingnumber of baccalaureate nursing programs are providing preparation for primarycare by including history taking and physical and psychosocial assessment tech-
niques in their curriculum.
In 1971, a report of the extended role of the professional nurse waspublished by the Department of Health, Education, and Welfare (14) and, aftercarefully analyzing the report, the Nursing Project Courcil adopted the follow-ing summary as its position on the extended role for nurses.

1. Health education centers should undertake curricular innovations teatdemonstrate the physician-n9me team concept in the delivery of carein a variety of settings under conditions that provide optimum oppor-tunity for both professions to seek the highest level of competence.Financial support should be made available for programs of continuingnurse education that could prepare the present pool of over one mil-lion attive and inactive nurses to function in extended roles. Thecontinuing education of nurses should be structured to encourage pro-fessional advancement among and through all nursing education pro-grams and by encouraging the use of equivalency examinations toevaluate competence, knowledge, and experience.
2. Increased attention should be paid to the commonality of nursing li-censure and certification and to the development and acceptance ofa model law of nursing practice suitable for national 'applicationthrough the states. The nursing profession should undertake a-thor-ough study of recertification as a possible means of documentingnew or changed skills among practicing nurses.
3. Collaborative efforts involving schools of medicine and nursingshould be encouraged to undertake programs to demonstrate effectivefunctional interaction of physicians and nurses in the provisionof health services and the extension of those services to the widestpossible range of the population. The transfer of functions andresponsibilities between physicians and nurses should be sought throughan orderly process, recognizing the capacity and desire of both profes-sions to participate in additional training activities intended toaugment the potential scope of nursing practice. A determined and '
continuing effort should be made V; attain a hi d94 degree of flexi-bility in the interprofessional relationships f physicians and nurses.Jurisdictional concerns per, se should not be permitted to interferewith efforts to meet patient needs.
4. Cost-benefit analyses and similar economic studies should be under=taken in a variety of geographic and institutional settings t(f assessthe impact on the health care delivery system of extended nursingpractice. Toward the same objective, attitudinal surveys of healthcare providers and consumers should be conducted to assess the signif-icince of factors that might affect the acceptance of nurses in ex-tended care roles which they do not now normally occupy.
In addition to adoption of these summary statements, the Council alsoadopted the following eight functions as inherent in the extended role:
1. Eliciting and recording a health history which would include psycho-social and environmental assessments.
Making physical assessments.
3. Interpreting selected laboratory findings.
47N-

4. Making diagnoses, choosing, initiating and modifying selectedtherapies.
5. Assessing camunity resources and needs for health care.
Utilization of available community resources related to iden-tified needs of patients.
7. Providing emergency treatment as appropriate, such as in cardiacarrest, shock or hemorrhage.
8. Providing appropriate information to the patient and his familyabout diagnosis or plan of therapy.
The Council also agreed that the "full participation of nursing in re-stlicturing the health care system" and in the individual nurse's potentialto contribute to the solution of present and future health care problems de-mands maximum utilization of professional nurse manpower.
Foreign Educated Nurses and Quality Nursing Care
One of the more elusive features of utilization of nursing personnelrelates to the foreign nurse recruited to work in Texas hospitals. The
Nursing Project was unable to acquire precise statistical data on the numberof foreign educated nurses, licensed or unlicensed, who are employed in thisstate.
We did learn from the United States Immigration Service that about 3,000foreign nurses per year enter the United States on permanent visas, and thatabout 600 to 1,500 temporary visas are issued to foreign nurses each year. Astatewide survey conducted by the Texas Hospital Association in 1973 showedthat there were approximately 1;400 foreign educated nurses employed in Texashospitals. WeAre unable to determine if this total represented only thoselicensed to practice or all of the licensed and unlicensed nurses who receivedtheir educational preparation outside the United States. If the total repre-sents only those having Texas licensure then the total number employed is con-siderably higher'.
VFor several years, Texas issued temporary work permits for foreign nurses
to practice until they could take the' licensure examination. This procedure
was stopped in 1973 when the Board of Nurse Examiners;concluded that the high
failure rate of the foreign nurses posed a severe health care problem in thecases where temporary permit holders were given responsibilities normally
given to licensed nurses. The:data shown on the tabli on-.the following page,covering the period July, 1970, through October, 1912, clearly points out thedifficulty experienced by foreign educated nurses, for whatever reasons, inpassing the licensure examination for registered nurses in Texas.

FOREIGN NURSE RESULTS ON STATE BOARD TEST POOL EXAMINATIONFOR PROFESSIONAL NURSING IN TEXAS*
DATE AND NUMBER OF CANDIDATES
1970-1972
TOTAL PASS PERCENTAGE PASSING
July, 1970 1st 31 61 27 44.3%Repeat 30
October, 1970 1st 38 65 9 23.0%Repeat 27 11 40.0%
April, 1971 1st 125 182 22 17.6%Repeat 57 17 29.1%
July, 1971 1st 149 231 24 16.1%Repeat 82 18 21.9%
October, 1971 1st 97 225 19 19.5%Repeat 128 23 17.9%
April, 1972 1st 244 442 48 19.6%Repeat 198 57 27.2%
July, 1972 1st 176 410 30 17.0%
Repeat 234 48 20.5%
October, 1972 1st 236 568 41 17.3%
( Repeat 332 90 27.1%
The licensure examination administered to applicants for registered nursesin this state is designed to certify that the individual who passes the exam-ination can practice safely in any employment setting for nurses. The failurerates shown or the table above indicate recruitment of foreign educated nursesis not the most effective way to increase the number of registered nurses forthe health care system in this state.
The country of origin of the foreign educated nurse and her probable suc-cess in meeting licensure requirements do not seem to be related to any notice-
able extent. The failure rate is exceedingly high, even by nurses representingcountries whose language and culture resemble our own. Shown on the followingpage are the results of the licensure examination in October, 1972, with thenational origin of the nurse identified.
The greatest number of examinees were from India (73), Korea (37),Australia (20), the Philippines (220), England (72), and Mexico (29), with atotal of 451 from those six countries. Only 29 passed who were taking theexamination for the first time, a passing rate of just over six percent, orconversely, a failure rate of about 94 percent.
*Report of the Board of Nurse Examiners for It IfIP
State of Texas, April, 1973.TA
49 38

RESULTS OF COUNTRIES HAVING MORE THAN ONE NURSE TAKESTATE BOARD TEST POOL EXAMINATION, OCTOBER, 1972*
COUNTRYTHE NUMBER WRITINGTHE EXAMINATION
THE NUMBER PASSINGTHE EXAMINATION
NUMBER WRITING FIRSTTIME AND PASSING.
Algeria 5 0 0South Africa 9 2 0
Hong Kong 3 0 0India 73 14 2
Iran 3 1 1
Israel 4 0 0Korea 37 5 0Taiwan 9 3 0Thailand 9 1 0Australia 20 6 4
New Zealand 2 0 0
Philippines 220 62 12
England 72 18 11
Ireland 12 2 . 1
Netherland 4 2 1
Scotland 6 2 2
Wales 3 0 0
Canada 7 4 3
Mexico 29 1 0
Panama 4 0 0
Argentina 5 2 1
Bolivia 3 1 0
The report also stated that many of those passing had taken the Testpool Examination for professional nurses as many as 10 times. As a resultof these statistics and the responsibility of the Board to maintain standardsof safe nursing practice, the decision was made to discontinue issuing per-mits to foreign nurse graduates, effective February 27, 1973. At the presenttime only 19 of the 50 states continue to issue permits.
Although Texas no longer issues temporary permits, a number of hospitalsin the state recruit foreign graduates on a contract basis to supplement theirprofessional nursing staffs. It is at this point that potential prob1ems arise.If the nurse is unable to pass the examination she cannot legally work in thecapacity of a professional licensed nurse and must be employed as a nursingassistant. Failure to pass 'the State Board Examination indicates inability tomeet minimal requirements for safe nursing practice. If the nurse is allowedto assume the responsibilities and functions of a licensed nurse but is notan RN, a serious question of patient safety arises.
The poor perforManoe of graduates of foreign programs has been attributedto several causes, including inadequate preparation in certain curriculum areas,difficulty with the English language, and unfamiliarity with objective tests.In addition to the testing problem those who have had contact with many ofthese graduates have pointed out additional reasons for the difficulties whichgraduates of foreign programs experience. Chief among these -re the cultural
*Ibid.
5 0 39,
t

differences that exist between this country and non-English speaking countriesin particular. Differences in the complexity of the United States health caresystem and the extensive use of technology and complicated equipment may makeit more difficult for the graduate of a foYeign program to perform effectively.
The Texas Nurses' Association has provided assistance to many graduates offoreign programs by sponsoring classes to help them prepare for the licensureexamination. However, it seems that more help is needed. When graduates offoreign programs are unable to meet licensure requirements they may suffer frominability to get a job, lower salary than they originally expected, and disap-pointment form being forced to work as a nurse assistant when they considerthemselves professionals.
In an effort to minimize the difficulties faced by graduates of foreignnursing programs and ensure that they have the background to meet the.require-ments for state licensure in Texas, recruitment efforts should be based onspecific criteria. The following suggestions are proposed as measures thatcould be employed.
1. Evaluation of an applicant's educational background andexperience should be based on utilization of an evaluationinstrument, developed by qualified individuals, includingnurses, designed to determine the degree of qualificationfor job requirements in nursing in the United States. Aminimum score should be established in order for an appli-cant to be accepted.
2. Recruitment procedure should include a personal interviewwith a registered nurse Mt -er of the recruitment team ifat all possible. Such an ,nterview should be essential ifthe applicant's responses on the evaluation instrument in-dicate potfitial difficulty in meeting licensure require-ments.
3. Once the applicant arrives in the United States, the con-tracting employer should assume the responsibility for pro-viding extensive orientation which includes, job orientation,the approach to health care in the United States and adapta-tion to the life style in the United States. This should beessential for those recruited from non-English speaking coun-tries.
4. Professional organizations and nursing education programsshould make every possible effort to provide supplementaryeducational classes to assist with licensure problems orproblems of adaptation to life in the United States.
Correlation of Educational Preparation and Utilization of Nurses
Utilization surveys conducted by the Nursing Project revealed that therewere many instances where nurses either did not feel prepared for requirementsof their jobs, or they were unable to put into practice some of the nursingfunctions for which they we..e prepared. Allhpugh it is not expected to entirely
t.
5 40

resolve all of these differences, it is the belief of the Council that manycould be eliminated by reasorable modification of current practices on thepart of both education and the service sector. Problems dealing with areasin which new graduates felt unprepared will be discussed later in this reportin the chapter on education. This portion of the report will present infor-mation on areas where nurses felt they were not able to utilize certain skillsthat would contribute to an improved quality of nursing care.
In the Projects survey of hospital nurses who had been in practice fiveyears or less, 956 responded to a list of 76 job functions and identified thosefor which they were prepared in the educational programs but seldom practicedin the hospital. Some of the items listed were of greater importance thanothers and the staff performed a Chi Square analysis to identify those of great-est significance. Shown below are the number of functions in which the nursesreceived educational preparation but which they seldom practiced in the hospi-tal setting.
EDUCATIONAL NUMBER OFPREPARATION SIGNIFICANT ITEMS
LYN 15
Dipl. 27
ADN 4
BSN 30
These resuits illustrate that the ADN graduates utilize the greatestamount of skills learned in their educational preparation, while the graduatesof the other types of programs do not, or do not have the opportunity, topractice those skills and techniques. The functions identified by diplomaand baccalaureate graduates as seldom utilized included:
1. Conduct team conferences2. Initiate teaching or health maintenance measures for patients
to be discharged3. Develop written home care plan with patients to be discharged4. Develop teaching plans and conduct classes for groups of
patients (such as diabetics or mastectomy patients)5. Develop and implement a teaching plan for an individual
patient6. Give IPPB treatments7. Perform passive range of motion exercises8. Insert urethral catheters9. Irrigate colostomy
10. Apply soaks or compresses11. Feed patients by nasogastric or gastrostomy tube12. Teach crutch walking
Itmes 1-5 of the list shown above are considered to be vital componentsof quality nursing care and should be the responsibility of the registerednurse. Items 6-12 are technical. procedures and the lack of performance ofthem by registered nurses inferi that they are delegating them to other mem-bers of the health care team when appropriate.
5241

Another group of items was identified by baccalaureate nurses as notbeing performed frequently enough although their education had prepared themto carry out the responsibilities. These items were:
1. Develop and execute patient care plans2. Include nursing objectives on care plans3. Make patient referrals4. Take a nursing history5. Establish priorities for nursing care6. Take a patient's physical history7. Take a patient's psychosocial history
Many of the functions identified require independent judgement by nursesabout nursing care actions. They often involve problems and concerns outside
. the scope of medical treatment but affect the patient's response to his illness.The limitation of the nurse's position to the execution of medical orders alonewould eliminate a valuable resource for the improvement of patient care.
One suggested approach to the problems which would involve a cooperativeeffort between nursing service and nursing education would be the appointmentof a nurse faculty member to the hospital Nursing Practice Committee. Membersof tiny L01111111 ttee would then have input upon which to base the outcomes of nur-sing care relative to education. In addition, alternative approaches to util-ization of nurses could be developed which would maximize educational background.
Another area in which nurses identifie4 inconsistencies in utilization wasin being placed in positions for which their education had nct prepared them.This occured when ADN graduates or LVN's were required to function as chargenurses or when new graduates of all three types of professional programs wereexpected to begin as head nurses. Although the emphasis on LVN educationalprograms is to prepare practitioners who can give, bedside care under super-vision, a survey of LVN practitioners indicated that 57 percent of 923 respon-dents were currently functioning as charge nurses. When asked if they had beenrequired to assume responsibilities for which their education had not preparedthem, 48 percent said "yes". Since registered nurses are frequently needed butnot available in hospitals in small communities, this does not seem to be anunusual practice. In cases where the need for nurses is great and unpreparedpersons are placed in positions of responsibility, the Nursing Project Councilis particularly concerned that employers make every effort to see that thesenurses receive the preparation required for the job. The following is there-fore submitted:
RECOMMENDATION: EMPLOYERS OF NURSING PERSONNEL ASSUME THE RESPONSIBILITY FORPROVIDING ADDITIONAL LEARNING OPPORTUNITIES FOR THOSE WHOMTHEY PROMOTE TO POSITIONS OF LEADERSHIP.
Clinical Research in Nursing.
Employers and practitioners who are responsible for providing nursingservices to the public should be vitally concerned about the effect of thevariable of "nursing" on patient welfare. What does nursing accomplish andwhat potential difference can it make in the degree and speed of recovery,
5342

the prevention of complications, and the psychological well-being of patients?Clinical research belongs in the hospital and health agency just as much as itbelongs in educational institutions. In a summary of some recent efforts inclinical nursing research, Werley describes studies related to pressure sores,,development of instruments to assess nursing care. relationship of patient in-structions and patient response to treatment proceddres and several others OM.From these examples she concludes that research is indeed. focusing increasinglyon nursing practice.
Large medical centers, in particular, provide excellent opportunities forclinical nursing research. Large numbers of patients make sampling proceduresmore valid and the existence of facilities for specialization in certain areasprovide opportunities to study many patients with similar problems. While theavailability of highly qualified nurse researchers is limited, many nurses withbaccalaureate and master's degrees are prepared to undertake less complex re-search projects.
Nursing administrators are urged to incorporate a research effort into de-partments of nursing service as a method of validating the positive effects ofnursing care and contributing to the unique body of knowledge of the nursingprofession in the interest of promoting improved nursing care for patients.
A '
Nurse Utilization and the Physician
It is apparent, that some of the attitudes toward nursing education and nur-sing utilization are the.result of a lack of knowledge concerning the varioustypes of educational programs, their stated purposes, or their curriculum con-tent. This was demonstrated in the Physicians Opinion Survey in several ways.Although many respondents had definite opinions on the type of graduate that wasthe "best" nurse, 46 percent (198 out of 430) indicated that in the hospitalsetting they seldom knew what type of programs the nurses had completed.. In aquestion asking physicians to indicate which kinds of positions were most appro-priate for graduates of-the different programs, 12 percent of the respondentsfelt ADN graduates were best prepared for public health, a subject which is notincluded in most ADN programs. As judged by comments from this survey most phy-,sicians prefer the diploma graduate in most employment settings because of her-greater clinical experience and her interest in patients. They indicated an ap-preciation of the leadership role and teaching abilities of the 8SN but stillpreferred the diploma graduate for actual nursing responsibilitiei. -
When'asked about employment of nurses in doctors'offices, 52 percentstated that it was necessary to teach any new RN graduate skills which they be-lieved should have been learned-in nursing school. The.skills referred to werefrequently basit technical procedures. In responding to another question on theutilization.of registered nurses in the physician's office, the majority wereinclined to approve of using nurses in a somewhat expanded role. The survey,however, did not indicate how many were actually using nurses in these capaci-ties. The 'listed functions and the physicians' responses are presented on thefollowing page.

DO YOU ADVOCATE LETTING NURSES:
1. Take health histories
2. Do health screening procedures
3. Counsel with patients about their treat-ment regimen, health maintenance, orrehabilitation techniques
4. Refer patients to community resourcesthat would be supportive of your careand assist with health problems
5. Mike home visits to check on routineevaluation of patients' status suchas diet, dressing changes, BP's, dis-cuss home adjustment problems
6. Conduct group teaching for such patientsas diabetics, mastectomies, expectantparents, amputees, etc.
APPROVE DISAPPROVE
64% 25%
67% 20%
67% 21%
64% 22%
66% 20%
72% 14%
In a question asking if physicians would consider referring patients withcertain health needs to an independent RN practitioner with eittier a master'sor doctoral degree in nursing, 42 percent said "yes".
The Nursing Project Council expects that better understanding among thevarious health professions will result in better utilization of all those en-gaged in health care. In support ofIthis the.following is submitted.
RECOMMENDATION: THE NURSING PROJECT COUNCIL SUPPORTS THE STATEWIDE JOINTPRACTICE COMMISSION AND URGES THE ESTABLISHMENT OF LOCALJOINT PRACTICE COMMITTEES AS A MEANS OF PROMOTING INTERDISCIPLINARY UNDERSTANDING AND MORE EFFECTIVELY PLANNINGAND PROVIDING FOR NEEDED HEALTH SERVICES TO THE PUBLIC.

CHAPTER IV
NURSING EDUCATION
SECTION I
EXISTING NEEDS IN NURSING EDUCATION
Admission and Progression Policies
The responsibility of both public and private nursing programs is 'to'produce practitioners capable of giving a high quality of nursing care., Thepublic educational programs in particular have the added responsibility ofusing public tax money efficiently to meet the nursing,manpower needs on astatewide basis. The problem of attrition in nursing programs is a factorwhich reduces the efficiency of a program in terms of production of graduatesand utilization of faculty time. Many of the problems which lead to eventualattrition are directly related to admission criteria and policies affectingprogression through the program. The following conditions illustrate someofithe problems that can occur:
a. Students who are admitted to programs even though they do notdemonstrate the potential ability to meet the requirements ofthe program, have wasted both time and money by the time theydiscover they cannot pass the courses.
b. Students who drop out during the first year of the professionalprogram cause a reduction in the size of the second year class'.If applicants have been more carefully screened, more wouldcomplete the program and be available for employment.
c. With the current severe shortage of qualified faculty membersavailable for professional nursing programs, it is unfortunatethat much faculty time is spent teaching students who will notcomplete the program and become practicing nurses.
Attrition and licensing examination failures in nursing programs-can bereduced by improved counseling and admission criteria.. The student in thebasic program has to meet degree requirements and also to acquire knowledgeto pass the licensing examination. Some are successfulin mastering degreerequirements but do,not'acquire sufficient knowledge and skills to pass thelicensing examination.
A similar concern is the student who graduates and woes to pass thelicensure examination only after taking the test several times. In suchcases the quality of the practitioner is questionable. In Texas the problemis significant. Between 1971 and July of 1973 a total of 3,934 graduates ofTexas nursing programi took the licensure examination for the first time.Of those, 808 or 20.5 percents of the total failed dne or more sections ofthe examination and thus failed to gain licensure on .their initial attempt.During the same period, failure rates for candidates repeating the examinationvaried from 30 percent to 71 percent. At the present time, when comparingthe averace test pool scores of students by states, Texas ranks 47th out of52 states and jurisdictions. Since our projections indicate that Texas willsoon be'producing large northers of professional nurses, the Council believesthat the state needs to focus its attention on,improying the quality of nur-sing graduates. Via
56

One of the prime indicators of the effectiveness of nursing educationprograms is the performance level of nursing program graduates on the StateBoard Test Pool (licensure) Examination. The extensive discussion of theforeign nurse graduate in Chapter 411 of this report makes it necessary thatwe present additional statistical data on tie licensure examination.perfor-mance for graduates of nursing programs in Texas. This is necessary becausetIese graduates are products of our own educational system and the state isin a position to bring about the corrective changes. This study has recom-mended those changes elsewhere in this report.
In summary form, the table shown below provides the State Board licen-sure examination performance, by type of program, of our own graduates, fromJune of 1972 through June of 1973.
SUMMARY OF LICENSURE EXAMINATIONPERFORMANCE BY GRADUATES OF NURSING PROGRAMS IN TEXAS
1972-1973
Type of Number Taking Number Number PercentProgram Examination Passing Failing Failing
ADN 873 579 294 34%
Dipl. 346 314 32 9%
BSN 591 493 98 17%
TOTALS 1,810 1,386 424 23%
In order to illustrate the results of the state licensure examinationfor graduates of nursing programs in Texas by individual program, the staffselected the 12 month period from June of 1972 throughIMay of 1973, to showthe number passing and failing, in each program. The examination is.of fiveparts or sections and an applicant must pass each of the five to receive alicense. The results of the examination for the sample period are shown onpage 46.
Applicants for licensure who fail one or more-parts of the examinationare permitted to be re-examined over the parts in which an acceptable scorewas not achieved, for a maximum of three examinations.
The high failure rate of the ADN program graduates in particular, isattributable in part at least to the lack of appropriate screening of appli-cants. Other factors, such as the inadequacy of faculty preparation, aresignificant and we have addressed those factors in our faculty improvementrecommendations. We submit that if the nursing programs will develop. im-proved screening procedures, the level of achievement On the State Board,licensure examination should increase.

RESULTS OF TEXAS STATE BOARD OF NURSE EXAMINERSLICENSURE EXAMINATION FOR GRADUATES OF TEXAS NURSING PROGRAMS
JUNE, 1972 - MAY, 1973 (Series 672)
SchoolNo. TakingExamination
Number of Sections Failed1 2 3 4 5
Total No. StudentsFailing Examination
ASSOCIATE DEGREE PROGRAMS
1 36 4 1 0 0 0 52 39 4 3 1 1 1 103 39 4 3 2 4 0 134 66 7 7 6 2 3 255 46 4 2 0 1 2 96 32 2 1 0 0 0 37 18 3 1 0 0 1 58 27 3 2 1 0 0 69 27 3 3 0 1 2 9
10 19 4 1 2 1 3 1111 23 2 2 1 0 2 712 19 3 0 2 0 0 513 49 6 3 4 4 0 1714 49 4 0 0 0 1 515 36 8 4 2 2 3 1916 47 9 6 4 1 0 2017 81 11 8 3 3 1 2618 53 6 2 1 1 0 1019 38 0 6 4 2 2 1420 129 11 10 18 13 23 75
DIPLOMA PRrRAMS
1 25 1 1 1 0 0 32 25 0 1 0 0 0 1
3 32 1 0 0 0 0 1
4 29 1 0 0 1 0 25 28 2 0 2 1 0 56 85 4 0 0 0 0 47 17 1 1 0 0 0 28 37 4 1 3 0 1 99 32 1 0 0 1 0 2
10 36 3 0 0 0 0 3
BACCALAUREATE PROGRAMS
1 39 7 4 3 0 0 14
2 20 1, 3 5 1 1 3 13
3 43 0 0 0 0 0 04 27 2 2 2 0 1 7
5 45 4 1 0 0 0 5
6 212 15 7. 5 5 1 33
7 5 0 0 0 0 0 08 61 4 2 1 0 0 7
9 24 2 2 2 1 0 7
10 115 7 2 1 21.:4?, 0 12
5847

With the objective of the improvement of quality in nursing education,the Council submits the following:
RECOMMENDATION: NURSING PROGRAMS IDENTIFY, LALIDATE AND UTILIZEADMISSION AND PROGRESSION CRITERIA WHICH CANSERVE AS RELIABLE INDICATORS OF AN APPLICANT'SABILITY TO SUCCESSFULLY COMPLETE THE PROGRAM.
Clinical Experience
Throughout the studies conducted by the Nursing Project there was gen-eral agreement among practicing nurses, students, physicians, and employersthat within professional nursing education programs there needs to be agreater emphasis on technical treatment procedures and clinical experiencein acute care settings. There is no desire on the part of the Council tominimize the importance of theoretical foundations in nursing and principleswhich allow graduates to meet the demands of a rapidly changing practice.However, the Council believes that such agreement is not without justificationand that professional nursing programs need to re-evaluate their curriculumsin terms of both total time spent in the acute care clinical setting and theutilization of that time to assure that their graduates are prepared to a--sume the responsibilities required of staff nurses in the majority of acute
care institutions.
The instrument used in the Project's Hospital Utilization Survey containeda list of 76 functions considered appropriate for nurses in the hospital set-
ting. The nurses were asked to indicate whether or not they were prepared Intheir educational program to carry out the function and if they had actuallydone so in practice. The results showed that the graduates of professionalnursing programs were frequently called upon to carry out functions for which
they were not prepared. For exdmple, the graduates of baccalaureate nursingprograms listed 23 items, graduates of associate degree programs listed 40,
and the diploma graduates listed 26 functions which they were called upon toperform but for which they felt unprepared. The high number of items for ADN's(40) reficrts the practice of using this type nurse in leadership positions andin management 4nd planniing roles which are not emphasized in that type educa-
tional program. 6espite this qualification, some of those items listed bythe ADN graduates wiz technical procedures that would be expected of the grad-
uate of this type program.
In a survey of 1,183 registered nurses, selected at random from activeRN's in Texas, 21 percent stated that they were required to perform func-tions in the first professional position they had held for which they were
not adequately prepared. They identified 63 percent of the functions as"procedure techniqugn" and 24 percent as "leadership and management of per-
sonnel."
5 9 . -1481._.:;- it
t,

A similar question in the Hospital Utilization Survey is given belowwith the responses reported to the staff:
Survey Question:
In your first position as a licensed nurse did your job requireyou to perform procedures or assume responsibilities for whichyour education had not prepared you:
Percent Answering "Yes"
LVN 33%Dipl. 39%ADN 61%BSN 46%
If you answered "yes" to the previous question, please specify thetypes of activities for which you felt unprepared.
LVN Dipl. ADN BSN
Supervision 16.0% 23.0% 33.3% 18.8%Assisting Physicians 4.9% 0.0% 2.1% 1.6%Teaching Patients 1.2% 0.0% 0.0% 1.6%Clinical Skills 63.2% 70.5% 45.8% 71.9%Communication with Patients,
Doctors, Administrators, etc. 2.5% 0.0% 2.1% 0.0%Planning Patient Care
v.
(Nursing Diagnosis)Coping with Emotional or
Social Needi
1.2%
0.6%
0.0%
0.0%
2.1%
0.0%
0.0%
0.0%Other 10.4% 6.6% 14.6% 6.3%
In a survey of 580 (25 percent of all) senior students enrolled in pro-fessional nursing programs in Texas the responses to items concerning clinicalexperience were as follows:
Diploma ADN BSNlagree) (agree) (agree)
1. Clinical experience is sufficientin length to master most technicalprocedures. 80% 38% 32%
2. Clinical experience provides ade-quate opportunity to apply nursingtheory under realistic conditions. 89% 55% 51%
Clinical experiences are usuallyrelated to theory being presentedin class. 83% 58% 45%
4. In clinical lab, the student is ac-cepted by the regular staff as amember of the nursing till) 77% 44% 45%
44/

In the survey of 1,183 practicing RN's on the adequacy of present educa-tional programs in nursing, the Nursing Project discovered a sharp differenceof opinion on adequacy, as shown in the responses to the following question:
"Assuming a normal orientation of the unique aspects of a particularinstitution or agency, do you believe current professional nursing educationhas adequately prepared the new graduate?"
Yes No No Response
a. Diploma program graduates 66% 15% 20%
b. Associate Degree program graduates 30% 47% 23%
c. Baccalaureate prngram graduates 42% 36% 22%
In 1971-72, 64.09 percent of employed RN's in Texas were working in hospi-tals. In the survey of students enrolled in professional nursing programs,94.4 percent of diploma students, 89.2 percent of ADN students, and 84.4 percentof BSN students indicated a preference for practice in hospitals. Although in-creasing numbers of both RN's and LVN's are working in other areas, hospitalswill continue to employ the greatest percentage of graduates in the immediatefuture. For this reason the Council recommends:
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS PLACE AN INCREASEDEMPHASIS ON CLINICAL EXPERIENCES WHICH MORE REAL-ISTICALLY SIMULATE THE RESPONSIBILITIES WHICH THENEW GRADUATES WILL BE REQUIRED TO ASSUME AS STAFFNURSES IN THE MAJORITY OF ACUTE CARE INSTITUTIONS.
With the rapidly expanding body of knowledge in medicine and nursing ithas become impossible for any one nurse to be highly skilled in all areas ofnursing practice. By the time students have completed basic nursing coursesin the major areas of practice, they often have a definite preference for oneor two and plan to work in those areas after graduation. Such areas of prac-tice may in,:lude medical-surgical nursing, maternal-child health, psychiatry,geriatrics, rehabilitation or any number of other special areas such as neuro-surgical nursing, or cardiac intensive care. In keeping with education prac-tices in other professional fields it would seem appropriate to allow studentsto choose an elective based on a particular area of interest in order to de-velop a greater degree of competence than would otherwise be achieved. Fromanother viewpoint students could use an elective as an opportunity to strength-en their skills in areas where they feel they need to improve. A clinicalelective emphasizing extensive participation in patient care over an entireshift could provide a student with a preview of actual job demands in whichshe would not normally be involved prior to experience as an RN. So that this
opportunity may be provided, the Council recommends:
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS PROVIDE-A NURSINGELECTIVE IN WHICH THE STUDENT MAY CHOOSE AN AREAOF CLINICAL PRACTICE AND PARTICIPATE IN A PERIODOF INTENSIVE CLINICAL EXPERIENCE UNDER THE SUPER-VISION OF A FACULTY MEMBER OR A PRACTICING NURSEWORKING IN THE AREA WHO MEETS THE QUALIFICATIONSOF THE PROGRAM.
SgiAS

RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS SHOULD PLACE INCREASEDEMPHASIS ON MANAGEMENT CONCEPTS IN THE ORGANIZATIONAND DELIVERY OF PATIENT CARE AND SUPERVISION OF PER-SONNEL IN THE CLINICAL SETTING.
Rural Experience in Professional Nursing Programs
The problem of shortages of professional nurses working in rural areasemphasizes the need for nursing programs to stimulate interest in this area.There appears to be a tendency for nurses to prefer working in settingssimilar to those in which they received educational experience and for thisreason the small community setting should be promoted as an area of practicewhich offers the professional nurse an opportunity to exercise judgment andutilize a broad range of skills and knowledge. For example, in smallhospitals therm is less likely to be a resident physician staff. In poten-tial or actual t,ergency situations the nurse must be prepared to makedecisions and take actions that would not be required in a large medicalcenter with access to a physician.
In addition, smaller hospitals are less likely to have extensive supportiveservices such as respiratory therapy departments, rehabilitation units orsocial workers. The professional nurse in this setting may be required to domany technical procedures or provide certain"types of nursing services thatwould normally be performed by special departments in large facilities. Suchdemands can prove to be extremely rewarding when the nurse can see the resultsof planning, teaching and nursing intervention which she has accomplished.Some programs have been incorporating such experiences into their curriculumwith apparently good results.
The Council therefore submits the following:
RECOMMENDATION:, PROFESSIONAL NURSING PROGRAMS OFFER CLINICAL EXPERI-ENCE IN SMALL HOSPITALS EITHER AS A PART OF ACURRENT COURSE OR AN ELECTIVE IN RURAL HEALTH CARE.
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS AND SUBURBAN ANDRURAL HOSPITALS AND HEALTH AGENCIES, WITHIN AREASONABLE DISTANCE OF THE SCHOOL, ENTER INTOJOINT APPOINTMENTS OF QUALIFIED, NURSES WHO CANSUPERVISE, TEACH, AND EVALUATE STUDENT EXPERIENCESIN THE SMALL HOSPITAL.
The recommendation that nursing programs utilize joint appointments inrural experiences is intended to meet two needs in particular. With a portionof the salary of a nurse being paid by an educational program, smaller hospitalswould have a better opportunity to recruit a staff member with advanced educa-tional preparation. In such an arrangement the joint appointee would work asa staff member when no students were receiving clinical experience and as a

faculty member during the period of their rural elective course. This wouldeliminate the need for a full time faculty member to travel back and forthand would provide qualified supervision by an individual familiar witb theclinical laboratory and the community.
Geriatrics
The need for registered nurses in nursing homes has been presented in aprevious chapter. In addition, with the increasing number of older peoplereceiving health care in hospitals, clinics, and offices there is a need fornurses with special preparation in geriatrics to work in many job settings.Because of the complexity of the health problems of older people, they offera tremendous challenge to regiitered nurses to use their professional knowl-edge to its full extent. The current emphasis of baccalaureate programs onskills in assessment, planning and therapeutic nursing intervention isexpecially important when working with older people. The Council thereforesubmits the following:
RECOMMENDATION: ALL.SCHOOLS OF PROFESSIONAL NURSING TAKE POSITIVESTEPS TO MAKE THE FIELD OF GERIATRICS MORE STIMULATINGAND CHALLENGING TO THE STUDENT BY:
A. EMPHASIZING THE CONCEPTS OF GERIATRIC NURSING TOA GREATER DEGREE THROUGHOUT THE CURRICULUM ANDINCLUDING A MINIMUM OF FOUR SEMESTER CREDIT HOURS,OR ITS EQUIVALENT, OF SPECIFIC GERIATRIC CONTENTIN BACCALAUREATE PROGRAMS AND TWO SEMESTER CREDITHOURS, OR ITS EQUIVALENT, IN ASSOCIATE DEGREE ANDDIPLOMA PROGRAMS.
B. ACTIVELY RECRUITING FACULTY WITH SPECIAL PREPARA-TION AND/OR SPECIAL INTEREST IN GERIATRICS ANDPROVIDING OPPORTUNITIES FOR FACULTY DEVELOPMENTIN THE AREA OF GERIATRICS.
C. OFFERING ELECTIVES IN THE FIELD OF GERIATRICS ATBOTH UNDERGRADUATE AND GRADUATE LEVELS.
D. FOSTERING A MORE POSITIVE IMAGE OF THE FIELD OFGERIATRICS BY INVOLVING STUDENTS TO A GREATERDEGREE IN THE HEALTH CARE OF OLDER PEOPLE WHO ARENOT ILL AND WHO CONTINUE TO ACTIVELY CONTRIBUTETO THE SOCIETY.
E. UTILIZINGiNURSING HOMES TO A GREATER DEGREE AS ALABORATORY'SETTING FOR DEVELOPING ADVANCED SKILLSIN ASSESSMENT, PLANNING AND EVALUATION OF HEALTHPROBLEMS.
1554 a6 3

c
o
Curriculum Evaluation
It is the belief of the eouncil that identification of the essentialcomponents of professional nursing education should be the result of collabo-rative efforts between nursing educators and clinical practitioners. One
approach to this is through joint appointments. In a description of theeffective use of joint appointments between the University Hospitals ofCleveland and Frances Payne Bolton School of Nursing, Case Western ReserveUniversity, Pierik points out the benefits of such arrangements (43). With
the school of nursing providing academic leadership in the patient caresetting, the expected results of the collaborative relationship would:1) raise the quality of patient care to a high degree of excellence; 2)enhance the learning climate for both nursing students and staff, and3) foster the development of significant research in clinical nursing. In
addition to these advantages, schools of professional nursing benefit byhaving faculty members: 1) who are engaged in clinical practice and havethe opportunity to keep their skills up to date, 2) who can serve as rolemodels to both students and staff, and 3) who, as employees of hospitals orother agencies, can provide learning experiences for students which will beconsistent with the demands they will face as registered nurses. With coopera-
tive relationships of this nature the development of the curriculum of anursing program will be based on patient needs and determined by input fromall who are concerned about preparing nurses to give quality care.
The CourvAl therefore submits the fq?lowing:
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS AND HEALTH CAREINSTITUTIONS AND AGENCIES IMMEDIATELY BEGINWORKING TOGETHER TO ESTABLISH JOINT APPOINTMENTSIN CLINICAL AREAS.
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS PROVIDE AN OPPORTUNITYFOR THE SERVICE SECTOR TO HAVE INPUT INTO THE EDUCA-TIONAL PROCESS BY APPOINTING QUALIFIED NURSINGREPRESENTATIVES OF HEALTH CARE AGENCIES OR INSTITU-TIONS TO SERVE AS MEMBERS OF CURRICULUM COMMITTEES..
RECOMMENDATION: PROFESSIONAL NURSING- PROGRAMS ASSUME THE RESPONSI-BILITY FOR EVALUATING THE PROFESSIONAL PERFORMANCEOF THEIR GRADUATES, BASED ON INPUT FROM BOTH THEPRACTICING NURSE AND THE EMPLOYER, AND USE THERESULTING INFORMATION AS ONE BASIS FOR IDENTIFYINGNEEDED CURRICULUM REVISIONS.
Interdisciplinary Collaboration
Leininger points out that "many of our health care.delivery problems
today are related to a lack of understanding and appreciation for the actual
and potential contributions of different health disciplines" (26). This
situation was apparent in the results of the Physician Opinion Survey in which
a significant number of physicians commented on their unfamiliarity with the
,
53

nursing education process. Similarly, physicians who have entered into collabo-rative professional practice with qualified nurse practitioners have expressedtheir satisfaction at the resulting improvement in the quality of health careprovided (25). If such interdisciplinary collaboration is to become a commonlyaccepted practice, its value needs to be taught and experienced at the studentlevel. During the late 1950's and 1960's the trend in nursing education wasto get away from previous practices of having a major proportion of classroomlectures delivered by physicians. Since nursing is a separate discipline withits own unique body of knowledge it is appropriate that nursee teach nursing.However, the trend served to exclude physicians almost entirely from partici-pation in nursing education. As a result, physicians are unaware of the changesand improvements that have taken place in the educational process since thattime and do not have the opportunity to be made aware of them.
Therefore, the Council submits the following:
RECOMMENDATION: PROFESSIONAL NURSING EDUCATION PROGRAMS INVOLVEPRACTICING PHYSICIANS TO A GREATER EXTENT IN BOTHTHE DIDACTIC AND CLINICAL ASPECTS OF NURSING EDUCA-TION. UTILIZATION OF PHYSICIANS SHOULD BE ON APLANNED BASIS AND SHOULD EMPHASIZE THE PHYSICIAN'SEDUCATION AND EXPERIENCE IN PATHOPHYSIOLOGY,DIAGNOSIS, AND TREATMENT, ESPECIALLY IN THE PREPARA-TION OF NURSES TO FUNCTION IN PRIMARY CARE SETTINGS.
RECOMMENDATION: SCHOOLS OF MEDICINE INVOLVE PRACTICING NURSES TO AGREATER EXTENT IN BOTH THE DIDACTIC AND CLINICALASPECTS OF MEDICAL EDUCATION. UTILIZATION OF NURSESSHOULD BE ON A PLANNED BASIS AND EMPHASIZE THE NURSE'SEDUCATION AND EXPERIENCE IN SUCH AREAS AS THE RESPONSEOF INDIVIDUALS AND FAMILIES TO ILLNESS, AND NURSINGTHERAPIES WHICH CAN SUPPLEMENT MEDICAL CARE.
RECOMMENDATION: MEDICAL AND NURSING EDUCATIONAL PROGRAMS ENCOURAGEINTERACTION OF THE TWO PROFESSIONS, WHEN APPROPRIATE,AT THE STUDENT LEVEL THROUGH SUCH ACTIVITIES AS CLASSES,ROUNDS; AND CLINICAL COLLABORATION.
RECOMMENDATION: PROFESSIONAL NURSING PROGRAMS PROVIDE PLANNED CLINICALEXPERIENCE IN PHYSICIANS' OFFICES WITH ONE OF THE .,kOBJECTIVES BEING TO PROVIDE AN OPPORTUNITY FOR PHYSI--CIANS, NURSING FACULTY, NURSING PERSONNEL, AND STUDENTSTO EXCHANGE IDEAS AND EXPERIENCE WITH METHODS OF INTER-DISCIPLINARY COLLABORATION IN THE OFFICE 'SETTING.
Career Mobility
The unusually high level of geographic mobility of today's population,plus the increasing percentage of married students enrolled in nursing programscombine to create a condition that makes it-increasingly important to developways to promote educational mobility from one institution to another without
unnecessary loss of time or credit to the student. In addition, there are

significant numbers of individuals who are interested in vertical careermobility who find themselves faced with frustrating barriers.
The extent of the desire for further education was demonstrated in re-sp:ises from LVN's, professional nursing students and RN and LVN practitionerswho were surveyed by the Nursing Project.
In May of 1972, 379 LVN's were enrolled in professional nursing programs.Of these,58 were enrolled,in diploma programs, 277 in ADN programs, and 44 inBSN programs. In one of the associate degree programs, LVN's accounted for32 percent of the program's enrollment. In eleven other ADN programs, thenumber of LVN's enrolled ranged from 14 to 23 percent. LVN's in BSN programsaccounted for fromel to 8 percent of the total enrollment of individual programs.
Of the 58 LVN's enrolled in diploma programs, 74 percent indicated thatthey planned to work toward a baccalaureate or higher degree at a later date.Of the 277 LVN's enrolled in ADN programs, 66 percent indicated similar goals.Of the 44 LVN's in BSN programs, 73 percent indicated a desire to obtain amaster's or higher degree. It should be pointed out that the actual numberof persons expected to attain such goals is considerably lower. However, a
high level of interest is present. If the problems of transfer of credit fromone type of program to another could be satisfactorily resolved, it is quitelikely that there would be a significant increase in the number of individualsattempting vertical career mobility in nursing.
Over two-thirds (nearly 67%) of professional nursing students surveyedindicated plans for further education beyond their present level. The percentageof students in each type of program indicating plans for educational advancementis as follows:
Percent Number
r.
'Diploma 82.89% 627 of 757
Associate Degree 71.86% 1,325 of 1,845
Baccalaureate 59.66% 1,135 of 1,902
Thus, regardless of their present levd4 of education, the majority of studentsplan to advance their educational preparation The highest level of plannededucation attainment by all students is as fo ows:
Percent
Diploma . 3.40%Associate Degree 11.28%Baccalaureate 46.18%Master's 32.37%Doctorate 4.91%No Degree 1.87%
5566 a

The highest education level desired by type of program is shown in thechart below.
HIGHEST EDUCATIONAL OBJECTIVE AS REPORTEDBY STUDENTS IN PROFESSIONAL NURSING PROGRAMS
1972
Student's AssociatePresent Program Diploma Degree Baccalaureate Master's Doctorate
Diploma 17% 1% 60% 19% 3%Associate Degree 1% 27% 47% 18% 4%Baccalaureate .m. 40% 52% 7%
The second type of mobility which creates problems of transfer of creditsis movement of students from one college to another. The charts on page 56indicate the extent t'o which students change schools but do not indicate thelength of time attended or the major of the student. Some of the figures canbe explained to some degree. For example, a number of baccalaureate nursingprograms provide all courses in the nursing major during the junior and senioryears. This allows students to take required general education courses at anycollege or university that offers the preprofessional curriculum and thentransfer to the college offering the nursing degree for the last two years.All diploma programs require one year of college work. This accounts for thehigh percentage of students who responded that they had attended "one othercollege". There are'still,.significant numbers of students who attend two,three or four institutions 'during the course of earning a degree. When transferof nursing courses is involved, it frequently becomes difficult to determinewhether the conteht of courses with similar names is the same in all schools.
One potential solution to this problem is the development of a curriculumwhich is specifically planned, to articulate the current types of nursingprograms. Such a curriculum would proceed from simple to complex nursing skillsand would eliminate repetition of material already learned at a previous level.Such a curriculum is designed to allow a student the option of leaving theprogram at any of several points with preparation for li:ensure either as anLVN or RN. If a student chose to reenter the program at a later date shewould receive full credit for work completed and could continue the programwithout loss of time or credit. This plan is referred to as a multiple entryand exit curriculum. Such a curriculum, if planned to incorporate sufficientflexibility to allow for individuality and erperimentation, could be adoptedby many schools for the purpose of facilitating inter-institutional transfersand promoting opportunities for vertical career mobility. The Council supportsthis concept as evidenced in later recommendations.

School
BACCALAUREATE PROGRAMS - COLLEGE MOBILITY
No. of Responses No. Who No. Who
Texas Indicating Attended AttendedSchools Previous At Least Two OtherPreviously Attendance One Other Colleges
Attended at a CollegeCollege with
a NursingProgram No. S No. %
No. Who'AttendedThreeOther
Colleges)
No. S
No. ofRespon-dents
4
UT Austin 27 20 31 45.6 15 22.1 3 4.4 68
M-H Baylor 24 14 30 46.2 13 20.0 4 6.2 65
Baylor 40 37 59 40.7 33 22.8 7 4.8 145
Dallas Baptist 21 10 20 43.5 15.2 1 2.2 46
TWU Denton 60 52 117 26.9 22 5.1 6 1.4 435
TCU 42 69 94 38.4 44 18.0 14 5.7 245
UT Galveston 31 23 UTA + 20 62 87.3 41 57.7 16 22.5 71"Dominican 25 11 36 33.3 11 10.2 2 1.9 108
'Houston Baptist 25 15 44 50.6 16 18.4 2 2.3 87
Prairie View 8. 3 9 20.0 4 8.9 0 45
TWU Dallas . 45 52 72 31.7 33 14.5 15 6.6 227
'TWU Houston 23 12 33 10.5 8 2.6 1 313
Incarnate Word 25 55 48 41.4 26 22.4 5 4.3 116
UT San Antonio 48 27 UTA 4. 71 93 87.7 57 53.8 27 25.5 106
TOTAL 748 36.0 269 13.0 103 5.0 2.077
AON PROGRAMS - COLLEGE MOBILITY
AlvinAmarillo 17
30 27 72 46.55 27 30.7
347
21.98.0
92
5.82.3
15588
Del Mar 17 15 22 19.1 6 5.2 4 3.5 115
El Centro 25 59 32.6 21 11.6 7 3.9 181
Grayson County 20 9 36 29.8' 8 6.6 4 3.3 121
Pan American 12 5 13 13.7 6 6.3 1 1.1 95
Tarrant County 22 18 23 26.1 9 10.2 3 3.4 88
Galveston College 29 15 44 41.9 18 17.1 3 2.9 106
Kilgore 9 6 11 29.7 2 5.4 0 - 37
Central Texas 7 2 5 9.3 3 5.6 0 54
Laredo 1 1 1 2.2 0 '45
Angelina 13 6 24 40.7 6 10.2 2 3.4 59
Odessa 19 10 18 28.6 8 12.7 4 '6.3 63
Paris 8 5 14 38.9 2 5.6 1 2.8 36
Sari Jacinto 15 8 17 18.1 5 5.3 2 2.1 94
Angelo StateSan Antonio
18 8 12 13.0
17.8
22 16.95
85.46.2
30
3.3-
92130
Texarkana 20 3 21 27.3 6 7.8 2 2.6 77
McLennan 32 19 35 29.4 17 14.3 4 3.4 119
MidwesTOTAL
tern 16 18 19.8494 26.8
6177
6.69.6
051
-
2.891
1,845
DIPLOMA PROGRAMS"- COLLEGE MOBILITY
Hendrick, 22 9 43 84.3 15 29.4 4 7.8 51
Northwest Texas 23 144 116 75.8 72 47..1 17 11.1 153
OrackenridgaBaptist - geaumont
21 52 45 77.6
11 6 48 94.12311
39.721.6
62
10.1
3.9
5851
Hotel Dieu 7 2 54 61.4 11 12.5 2 2.3 88
John Peter Smith 21 57 63 86.3 23 31.5 13 17.8 73
Hermann 22 22 58 82.9 22 31.4 8 11.4 70
Methodist Lubbock 20 10 67 88.2 26 ,34.2. 10 13.2 76
Baptist - S.A. 8 i 42) 40 83.3 10 ( 20.8 4 8.3 48
Texas Casters 18 46 51.7 14 15.7 2 2.2 89
TOTAL 580 76.6 227 30.0 68 9.0 157
57
s; a
68

Availability of Faculty
The seriousness of the current nursing faculty shortage in the UnitedStates was pointed out in &recent Southern Regional Education Board publica-tion Nursing Education in the South: 1973. in a discussion of program qualityof nursfng programsin the I6states holding membership in SREB, the followingfacts were presented:
1. Although the master's degree is considerid a requirement forteaching, only 43.6'peroent of present nursing fatuity holdthe degree.
2. Fifty-four percent of nursing faculty members are not educa-tonally prepared if the criterion is a graduateNdegree.
3. Southern ADN and BSN programs reported 227 budgeted facultypositions vacant in 1973.
Against these ods new nursing programs are opening at therate of one a eek.
. Texas is currently facing a similar condition where, despite the presentshortage of qualified faculty, there is pressure to open more nursing programs.In the spring of 1973, the Board of Nurse Examiners reported unfilledAfacultypositions in Texas nursing programs. The level of faculty educational prepara-tion in Texas programs is presented below in, comparison with the United States.
FACULTY PREPARATION IN PROFESSIONAL NURSING PROGRAMS
1973
EmployingPrograms
Holding Holding.Diploma Baccalaureate
U.S. Texas U.1-. Texas
57.7%38.5
. 14.0
Diploma 23.6% 18%
Associate Degi'ee 1.4 0
Baccalaureate .4 0
Percent Percent
Holding .Holding
Master's DoctorateU.S. Texas W.STTF)(as.
64% 17.9% 18%64 58.7 3414 79..1 82
.2%. .0%
.4 1.5
6.2 4.0
Although nursing programs in Texas and other, states have too few facultymembers with graduate degrees, the type of program in Tees which is in great-est need of faculty,holding at leas,t the master's degree is at the associatedegree level. Very few of the ADN programs are located near graduate programsin nursing and it is difficult to pursue the degree while teaching full time.Since 64 percent of faculty in diploma and ADN programs do not hold the graduatedegree, it is urgent that alternativei be provided to the traditional' processof all graduate work in nursing be taken inresidence.
69 58

The level of the degrees held by nursing faculty is an important criterionfor measuring faculty qu4lity, but it is not the only criterion. Experience andability in teaching, practice experience, especially clinical practice experiente,are also of vital importance. In the interest of promoting improved facultyqualifications, the Council supports the following recommendations:
RECOMMENDATION: NURSING PROGRAMS REQUIRE THAT FACULTY WHO DO NOTHOLD AT LEAST,THE MASTER'S DEGREE ENTER A GRADUATEPROGRAM WITHIN 12 MONTHS AFTER BEGINNING EMPLOYMENTAND COMPLETE THE MASTER'S DEGREE WITHIN SIX YEARSOF THE DATE OF BEGINNING EMPLOYMENT.
RECOMMENDATION: AS RECOMMENDED BY THE BOARD OF NURSE EXAMINERS, FACULTYMEMBERS WITH MASTER'S DEGREES IN NON-NURSING MAJORSSHOULD HAVE A MINIMUM SIX SEMESTER HOURS OF GRADUATELEVEL CONTENT IN NURSING.
'RECOMMENDATION: NURSING PROGRAMS A1D EMPLOYERS OF NURSES ESTABLISH.A PROCESS UNDER WHICH NURSING FACULTY WOULD PRACTICEIN THE CLINICAL SETTING EACH YEAR. AT LEAST 10 PER-CENT OF THE TIME NORMALLY SPENT IN CLINICAL INSTRUCTIONSHOULD BE THE MINIMUM FOR THIS CLINICAL PRACTICE BYFACULTY.
The intent of the Council in these recordmendations is to improve facultyeducational levels and to increase the clinical practice capabilities ofnursing faculty.
Graduate Education
Over the past several years there has been an increasing demand for graduateeducation in nursing. The two graduate proprams in Texas reflect this in thegraduation statistics illustrated on the chart shown below.
,11111111.1.1I=MMMM
NUMBER OF GRADUATES FROM TEXAS PROGRAMS OFFERINGTHE MASTER'S DEGREE IN NURSING
1967-68 3968-69, 1969-70 1970-71 1971-72 1972-73
The Universityof Texas 4 3
Texas Woman'sUniversity 4 17
Total 8 20
6
24'
30
10 27 82
35 57 66*
45 84 148

Both of the graduate programs are increasing the number of locations wheregraduate courses are available but there is still a need that is not being met.As indicated above, there are many faculty members of basic nursing programswho are not prepared at the master's level. Many would like to work toward the
degree but are unable to move to a city offering graduate work. At the presenttime the Council feels that the priority neea in nursing education in Texas isfor qualified faculty in basic professional programs and therefore submits thefollowing:
RECOMMENDATION: EXISTING GRADUATE PROGRAMS IN NURSING PLACE A SPECIALEMPHASIS ON THE PREPARATION OF NURSING FACULTY IN THEFOLLOWING WAYS:
A. OFFER OFF-CAMPUS COURSES FOR CREDIT PRIMARILY FORFACULTY MEMBERS OF NURSING PROGRAMS WHO COULD NOTOTHERWISE PARTICIPATE IN A PROGRAM ON AN EXISTINGGRADUATE CAMPUS. SUCH COURSES COULD RECEIVEPARTIAL FUNDING THROUGH MONIES APPROPRIATED TO THECOORDINATING BOARD FOR THE PURPOSE OF FACULTYIMPROVEMENT.
B. OFFER A SERIES OF SUMMER COURSES ON EXISTING GRADUATECAMPUSES FOR FACULTY MEMBERS IN SCHOOLS OF NURSINGWHO NEED ADDITIONAL PREPARATION FOR TEACHING. SUCHCOURSES SHOULD EMPHASIZE CURRICULUM DESIGN, COURSECONSTRUCTION, TEST CONSTRUCTION, PERFORMANCE EVALUA-TION, INSTRUCTIONAL METHODOLOGY, TEACHING RESOURCES,PRACTICE TEACHING, AND ADVANCEMENT OF CLINICAL KNOWLEDGEAND SKILLS.
PLAN TO EXTEND (=RADUATE COURSES INTO REGIONS WHICH%re
CAN DEMONSTRATE A CONTINUING NEED.
D. GRADUATE PROGRAMS OFFER MAJORS WHICH PLACE EQUALEMPHASIS ON CLINICAL AND NON-CLINICAL AREAS FORTHOSE WHO PLAN TO ENTER TEACHING.
E. PROVIDE APPROPRIATE RESEARCH TRAINING WITH PARTICULAREMPHASIS ON EVALUATION TECHNIQUES.
In Aditim to these recommendations to provide basic access to graduate
r K 111 nurse ,, with emphasis on meeting the needs of new and existing nursingfaculty, the Nursing Project encourages the graduate programs to utilize all
appropriate resources to meet thole needs and therefore submits these recom-
mendations:
RECOMMENDATION: A. BACCALAUREATE NURSING PROGRAMS WITH FACULTY PREPAREDAT THE DOCTORAL LEVEL SHOULD EXPLORE WITH EXISTINGGRADUATE PROGRAMS THE POSSIBILITY OF OFFERING GRADUATELEVEL NURSING COURSES WHICH WILL TRANSFER TO THEGRADUATE PROGRAMS.
7*60
SI

B. EXPLORE CONSORTIUM ARRANGEMENTS AND SHARED FACULTYAPPOINTMENTS AMONG NURSING PROGRAMS TO PROVIDEGRADUATE COURSES FOR STUDENTS WHO CANNOT PARTICIPATEAS RESIDENT STUDENTS.
With the need for additional clinical experience for both students andfaculty, as recommended in various parts of this report, the Nursing Projectadvocates clinical practice prior to admission to graduate school, as statedhere:
RECOMMENDATION: GRADUATES OF PROFESSIONAL NURSING PROGRAMS BE ENCOURAGEDTO HAVE AT LEAST ONE YEAR OF. CLINICAL EXPERIENCE BEFORESEEKING ADMISSION TO A GRADUATE PROGRAM IN NURSING.
Preparation of Faculty for ,ADN Programs
With a deficiency in qualified faculty having been identified by theNursing Project as the most critical problem facing nursing education, it isincumbent that graduate programs in nursing move to meet the challenge. As
shown above, the production of master's degrees has increased from eightin 1967 to 148 in 1973, but the deficiency remains. Only an estimated 40 to60 percent of master's degree students plan to teach. The others elect othermajors, such as clinical specialties or administration.
The ADN program was conceived to produce highly specialized "technical"nurses or bedside specialists. In the employment setting, this uniqueidentity tends to disappear. The ADN graduate, even if educated as a 'technical"nurse, is given additional responsibilities when she accepts employment,esually because she is the best qualified nurse available.
The ADN program is usually located in a community college or small univer-sity, draws its studentt, who are usually older than students in other pro-fessional programs, from' the geographic service area of the college.
For those who prepare AU faculty, an awareness of the mission of the community college and the ADN graduate is a necessity; the graduate faculty mustrealize that teaching in the community college is quite different from thelarge metropolitan university.
a
amaEla.
At the present time graduate programs' do not appear to emphasize prepara-tion for teaching in specific types of basic nursing programs. It is necessary'that graduate programs in nursing, who form the only supply source for ADNfaculty, offer a course relating to the particular needs of those who teach inthe ADN programs. In order to enrich this experience, practice teaching in anADN program should be made available to the student.
So that the faculty of ADN and diploma programs may have their needs met inthe graduate programs in nursing education, the Nursing Ptoject Council recommends:

RECOMMENDATION: AS A MEANS OF MEETING CURRENT FACULTY NEEDS, PARTICULARLYIN ASSOCIATE DEGREE AND DIPLOMA NURSING PROGRAMS, GRADUATEPROGRAMS OFFERING A MAJOR IN NURSING EDUCATION SHOULDEMPHASIZE THE DEVELOPMENT OF CLINICAL GENERALISTS WHO HAVESOME ADDITIONAL PREPARATION IN TWO OR MORE OF THE MAJORCLINICAL AREAS OF NURSING (MEDICAL, SURGICAL, MATERNAL-CHILD, PSYCHIATRY).
Graduate Education and Leadership Positions in Nursing
The current trend in nursing, is for the baccalaureate dsgree to be theminimum Orofessional requirement for nurses in leadership. positions and forthe master's degree to be the minimum professional requirement for supervisoryand administrative responsibilities, especially in the more sophisticated andcomplex health care facilities.
The Project staff tabulated the number of degrees held by nurses in eachregion and recorded the level of those degrees. We identified the number ofnurses holding supervisory, administrative, and instructional positions andconstructed the chart on page 63 so that we cculd compare the number ofdegrees held, by level, in each region with the number of positions requiringthose degree levels. While these data display the numbers in each category, wewere not able to determine if the persons having the degrees were employed in
the positions requiring those degrees.
The chart, therefore, shows only the number of BSN's and MSN's held bynurses, by region, and it also shows the greater number of positions whichare filled by nurses who obviously do not have the degree requirement under
the current trend.
In addition to illustrating this deficiency of qualifications in positionsof greater responsibilities, the chart displays the concentration of the graduatedegree nurses in the regions of the state having most of the major health carefacilities and population. These same regions also have concentrations ofnursing programs whose faculties are included in this tabulation.
Although the Council did not feel that the need for incr=eased prepara-tion of nurses in leadership was 'the first priority need in the state, theneed is severe. It was the belief of the Council that graduate programsshould make every effort to increase ceursc offerings in this major area.
Vocational Nursing
One of the fundamental beliefs of the members of the Nursing ProjectCouncil was that the quality if nursing care in this state, needs to improvein all locations, regions and qmployment settings. This belief ggided theseveral task forces in their work andi was a factor in most of the surveys
conducted by the staff. /

BEST COPY AMIABLE
THE NUMBER AND PERCENT OF BSN AND MSN DEGREE NURSES IN EACH PLANNINGREGION COMPARED TO THE NUMBER OF LEADERSHIP POSITIONS REQUIRING THOSE DEGREES
1971 - 1972
1. Panhandle
2. South Plains
3. North Texas'
4. North Central Texas
5. North East Texas
6. East Texas
7. West Central Texas
8. Upper Rio Grande
9. Permian Basin
10. Concho Valley
11. Central Texas
.11"14. CipiLui
13. Brazos Valley
14. Deep East Texas
15. South East Texas
16. Gulf Coast
17. Golden Crescent
18. Alpo
19. iluth Texas
20. ,Coastal Bend
21. Lower Rio Grande
B.S.N.*
%
M.S.N.* Admin. Super. Instruct.
0 %
70 8.06. 8 .92 45 5.18 120 13.80 53 6.10
62 10.15 3 .49 32 5.24 141 23.08 24 3.93
34 7.41 8 1.74 32 6.97 92 20.84 25 5.45
1150 18.24 115 1.82 298 4.73 943 14.96 265 4.20
32 9.04 3 .85 24 6.78 105 29.66 26 7.34
87 11.85 5 .68 61 8.31 211 28.70 38 5.18
43 8.50 2 .1p 35:1 6.92 125 24.70 14 2 77
85 9.82 ,15 1.73 33 3.81 88 10.16 38 4.39
41 7.88 3 .58 28 5.38 100 19.23 24 4.62
29 9.51 6 1.97 24 7.87 67 21.97 17 5.57
132 12.43 10 .94 58 5.46 149 14.03 51 4.80
203 16.04 36 2.95 75 6.15 180 14.75 74 6.07
44 18.97 6 2.59 21 9.04 51 21.98 7 3.02
31 10.26 2 .66 27 8.94 80 26.49 15 4.97
67 8.77 5 .65 35 4.58 118 15.45 25 3.27
1378 20.86 127 1.92 258 3.90 865 13.09 285 4.31
25 11.96 0 0.00 22 10.53 69 33.01 3 1.44
468 17.54 49 1.84 132 4.95 384 14.39 137 5.13
23 20.54 3 2.68 12 10.71 13 11.61 10. 8.93
71 9.63 5 .68 41, 5.56 149 20:22 34 4.61
55 13.58 8 1.98 32 7.90 88 21.73 23 5.68
TOTALS 4,130 419 1.325 4.138 1,188
%%44%%%* 6,651they 4,549*Figures for BSN's I MSN'sare the total number in theregion, not the number work-ing In laaership positions.
6,651 - 4,549 (2,102)
63'

From this perspective, the Council asserted, through its adoption of mostof the preliminary recommendations of the Review and Evaluation Committee, thatimprovement of quality nursing care would follow upon the improvement of theeducational and professional qualifications of nurses. Hence, a great many ofthe recommendations in this report are directed toward improvement of the ed-u-cational quality of those now in practice and those who will follow.
'The health care system of this state, especially the small rural hospi-tals owes a tremendous debt of gratitude to the Licensed Vocational Nurse.She was there when no other nurse was available and, without the LVN, the pa-tient care system of Texas would be in a far more desperate condition than itis now.
The LVN, despite her loyalty to patients and to her profession, has nothad the opportunity to acquire the knowledge and advanced skills which arerequired in the professional program. The LVN, in many settings, functionsin positions of great responsibility and trust, not because she wants to, butbecause she has to. There is no one else to "take charge", so she does.
Quality nursing care definitely includes the LVN in the ideal setting,but frees her from the responsibilities for which she was.not trained to ac-cept and permits her to devote her talents to the immediate and continuingpatient needs, under the supervision of a professional nurse.
In the spirit of this concept, the Nursing Project believes that whenprofessional nurses are increased in all employment settings, when registerednurses are available in rural practice in adequate numbers, then LVN's and
RN's will be able to function as they are trained to function.
With the number of active RN's and active LVN's being about the same innumber in this state, and with the RN's located more frequently in larger com-munities and less in smaller communities, the improvement in quality of careis going to require a dramatic change .n the employment setting preferencesof professional nurses.
4
We therefore submit,that in the interest of improving the quality ofnursing care, the state needs to increase the distribution of RN's to therural areas, especially to the hospitals and nursing homes, and to accomplishthis, in part, by providing professional nurse education availability to LVN's
who are qualified to become professional nurses.
The unequal distribution of RN's across the state results in the necessityfor vocational nurses to provide the majority of nursing services available in
certain geographic areas and in certain job settings. In these locations
LVN's must assume leadership and'patient management responsibilities beyond
the scope of their educational background. Since it does not appear thatthese conditions will change significantly in the next few years, there is a
definite need to provide these nurses with additional educational experience
to assist them in providing quality nursing care. At the same time LVN's need
Is 4

additional opportunities to further their careers by seeking to become RN'sif they choose to do so. Results of the various surveys described in a pre-vious chapter indicate that many LVN's are already enrolled in RN programs andmore would participate if they could get college credit for their LVN programs.In order to facilitate this mobility for future graduates of LVN programs theCouncil submits the following:
RECOMMENDATION: SCHOOLS OF VOCATIONAL NURSING SHOULD BE PHASED INTO THEPUBLIC EDUCATION SYSTEM, PREFERABLY COMMUNITY COLLEGES,WHEN SUCH TRANSITION WOULD NOT ADVERSELY AFFECT THEREQUIRED SUPPLY OF LVN'S IN SMALL COMMUNITIES.
In order to assist currently employed LVN's who are working in positionsas charge nurses or supervisors of nursing personnel, the following recommenda-tions are submitted:
RECOMMENDATION: AN EDUCATIONAL PROGRAM.SHOULD BE DEVELOPED SPECIFICALLYFOR LVN'S TO STRENGTHEN UPGRADE CURRENT SKILLS ANDTO INSURE COMPETENCIES. UNCTIONS WHICH THE LVN ISCOMMONLY REQUIRED TO AS ME BUT IS NOT ALWAYS PREPARED.
RECOMMENDATION: CONSIDERATION BE GIVEN TO THCDEVELOPMENT v THE ABOVEPROGRAM IN SUCH A MANNER THAT THE REQUIRED STANDARDS FOROBJECTIVES, CONTENT, LENGTH, AND QUALITY OF INSTRUCTIONBE ACCEPTABLE AS A STATED AMOUNT OF CREDIT SHOULD THE LVNLATER DECIDE TO ENTER A REGISTERED NURSING PROGRAM. THISWOULD NECESSITATE THAT SUCH OFFERINGS BE PROVIDED THROUGHOR IN AFFILIATION WITH PROGRAMS OF PROFESSIONAL NURSINGIN ORDER TO INSURE ACCEPTANCE FOR CREDIT.
RECOMMENDATION: CONTINUING EDUCATION FOR LVN'S SHOULD BE A.COOPERATIVE .
AMONG PROGRAMS OF PROFESSIONAL NURSING SCHOOLS,SCHO S OF VOCATIONAL NURSING, AND LVN PRACTITIONERS.
65 71

NURSING EDUCATION
SECTION II
AN ANALYSIS OF THE CURRICULUM OBJECTIVES OFSELECTED PROFESSIONAL NURSING EDUCATION PROGRAMS
1-
The concerns which led to the decision to study the behavioral objectiveswithin the curriculums utilized by professional nursing programs stemmed fromttwo major problems that complicate nursing education and nursing practice:
1. The current lack of clearly defined differences in thegradates of the various types of professionalinursingprogram
2. The lack of available information identifying areas ofsimilar content among the curriculums of the varioustypes of ptograms
The second area is particularly pertinent to nursing educators. Many nurseswho have received basic nursing preparation in different types of programs wishto further their professional education. Because there is no consistent methodof organizing and presenting nursing content, the curriculum in each school isusually considered somewhatunique. When a student transfers to another programor applies for a higher level program it is often difficult to determine howMuch credit:-should be granted: The student frequently must repeat courses whichhe considers very similar to ones taken earlier, or must take a challenge exam-ination-to verify that hethas mastered specific cont, ht.
In a similar manner, educators develop nursing curriculums in order to pre-pare nurses to function in specific areas and in different capaci ies. TheiADNgraduate is prepared to function in a hospital or similar acute care setting andis primarily intended to work under the supervision of baccalaureate graduates.Because of the distribution problems, this arrangement. is seldom possiVe. As aresult, ADNs are expected to function in all areas and without other direct RNsupervision. The problem is made more difficult by the inability of educatorsto clearly define the specific differences in areas of practice among the grad-uates of the various types of programs.
In a series. of meetings conducted by the'Education Task Force and the Edu-cation Subcommittee there was extensive discussion on possible ways to determinesimilarities and differences among programs. The end result of these meetingswas agreement to base a study on the behavioral objectives utilized by each school.
The aim of the study was to develop a cataloging system which would allowall objective from each school to be organized in a similar manner. In this
way, similar jectives could be listed together and,compared, regardless ofthe courses in which they were presented or the year and semester in which theywere taught.

Although there were many problems associated with the development of sucha system, a tentative approach was designed which would allow information abouteach objective to be coded and later placed on a tape for computer analysis.
A series of four one-day workiops were held in Austin, Dallas, Houston,and Lubbock to teach faculty members the procedure for coding the objectivesutilized by their program. A total of 23 nursing programs participated in thestudy by coding their objectives as requested by the Project and sending the com-pleted information to the Nursing Project's office.
The large volume of objectives and the time and expense required for proces-sing made it necessary to utilize a sample of the objectives of participatingschools for actual computer analysis. The sample consisted of 2 diploma programs,7 associate degree programs and 4 baccalaureate programs.
The total number of objectives used in .these programs was 12,222. The dis-tribution of number of objectives used by each school is presented below. It
is readily apparent that even within the same type of program there is a tremen-dous variation in the utilization of objectives.
NUMBER OF BEHAVIORAL OBJECTIVES USED IN EACH PROGRAM
Dipl. ADN BSN
School #1 1,892 764
vor
3,260
#2 1,014 1,335 1,359
#3 338 525
#4 348 452
#5 885
TOTAL 2,906 3,720 5,596
This wide variation is partly explained by the fact that some schoolswrite objectives in broad general terms and others are very detailed, oftenhaving a separate objective for each step of learning related to a specifictopic. If objectives are used as a basis for evaluatipn of student learningand performance, the more specific they are, the easiqr it is to provide thestudent with a clear understanding of his level of achievemcrt in 'Comparison
with expectations.
In an effort to determine how the various programs dealt with a partic-ular subject, the final coding system provided a mechanism which could deter-mine, to some extent, the breadth and depth with which a subject was presented.This could be done by determining 1) how many objectives within a program dealtwith the same topic and 2) what level of knowledge was involved. The underly-
ing assumption was that the more objectives dealing with one subject, the morethe student was expected to know about it. The "level of knowledge" was based
on the complexity of intellectual functioning required by the student in order
to achieve the objective. For example, simple tasks of memorization such as"list the symptoms of diabetes" require less of the student than complex skills
7P 68

such as comparison, contrast or evaluation. By using an analysis of thistype it could be demonstrated that although the topics studied might be thesame from one program to another, there could still be a significant differ-ence in the end product of the various programs.
Findings of the Study
As expected, the analysis of objectives indicated that different types ofprograms place greater emphasis on different areas within the curriculum. Thechart below demonstrates some of these differences.
MAJOR TOPIC BY TYPE OF PROGRAM AND PERCENT OF OBJECTIVESDEALING WITH EACH TOPIC
Dipl. ADN BSN
Physiology 45.6% 49.7% 37.5%
Psycho-Social 8i.7% 9.2% 17.4%
Cognitive Nursing Skills 11.2% 9.5% 15.1%(AssessLent, observation,planning. evaluation) or
Manipulative Nursing Skills/
14.2% 24.1% 12.9%(Procedural techniquesand treatments)
Nursing as a Profession 13.3% 3.4% 9.4%
The Health System 6.8% 3.7% 7.7%
TOTALS* 99.8% 99.6% 100.0%
The baccalaureate programs are known to emphasize the psycho-social aspectsof health care and this is apparent, with 17.4 percent of the objectives relatedto this topic. Similarly, ADN programs are known to emphasize procedures andthis is shown by 24.1 percent of objectives in the ADN curriculum related totechniques. Some unexpected' findings indicate that, although the baccalaureateprograms are intended to prepare "professional" practitioners, the diploma pro-grams apparently place a greater emphasis on this particular area. Also, whilemany'people have felt that the diploma graduate receives a greater emphasis on
. manipulative skills, the analysis of objectives show them to be very close indegree of curriculum emphasis.
This study of curriculum objectives has shown that the objectives taughtin any program in nursing are determined by the particular nursing faculty andthe director. We do not have in this state a stated list of curriculum objec-tives that applies uniformly to all programs.
Within nursing programs of the same type there is also a considerable var-iation of topic emphasis as demonstrated in the chart on the following page .
The first two columns do not total lop because of rounding of decimals.
69 h.,
79 " c?

PERCENT OF EMPHASIS ON SELECTED TOPICS
Diploma ADN 8
SchoolsSchools Schools
01 02 fl 02 03 04 05 01 02 03 04
Physiology 41.5 53.4 41.2 52.1 42.8 34.9 64.6 46.1 34.3 13.4 9.2Psycho-Social 10.8 4.9 10.2 6.4 16.0 17.3 4.0 18.4 21.3 7.0 8.9Cognitive Skills 12.7 8.4 11.9 6.2 10.1 11.2 8.5 12.0 12.8 36.4 22.0Manipulative Skills 15.7 11.5 28.4 29.2 22.2 26.2 16.9 11.0 11.0 10.4 39.9Nursing as Profession 12.4 15.1 4.8 2.5 1.5 5.8 2.8 5.1 10.4 25.6 12.3The Health System 6.9 6.7 3.4 3.7 7.5 4.6 3.2 6.5 10.3 7.2 7.6
TOTAL 100.0 100.0 100.1 100.0 99.9 100.1 100.0 100.1 100.1 100.0 99.91
For example, of the two diploma programs in the sample, one has almostNice as nuch emphasis on psycho-social aspects of nursing as the other. -Thesame wide variation is also apparent in the other types of programs, with fig-ures ranging from a low of 4.0 percent to a high of 17.3 percent in the ADNsample and 7.0 percent to 21.3 percent in BSN programs.
In looking at all types of programs, the range of differences can bestartling. AD4 school #3 devotes 1.5 percent of its objectives to "Nursingas a Profession" while BSN program #3 has 25.6 percent.
By analyzing the objectives of a particular program in the manner usedby this study, it is possible to identify areas of emphasis in a curriculumthat may not have been apparent when the program is viewed as a whole. Suchan analysis would be useful to curriculum planners to ensure that there is anappropriate balance and that the total design is what the faculty intended itto be.
Since many objectives utilize more than one subject, it became eveidentthat there was a need to identify the ways in which subjects were combined iftrue similarities of content could be identified. For example, it is possiblefor two schools to each have 3 objectives related to diabetes without havingany one objective common to both programs. This is demonstrated as follows:
School #1
1. List the symptoms of diabetes.-
2. Name 2 types of insulin usedto treat diabetes.
3. Define diabetes insipidus anddiabetes mellitus.
School #2
1. .Develop rsing care planfor a p ien ith diabetes.
2. Explain the physiology ofdiabetic retinopathy.
Compare the symptoms of in-sulin shock and diabetic coma.
4
In the example given above, the demands or the student in SchoOl #1 are.minimml,requiring simple memorization of a few basic facts. In School #2 the student isrequired to understand more complex knowledge in order to explain and compare andis also required to-show how his knowledge can be put to use in a specific situa-tion. In all these instances "diabetes" is the central 'subject but is used withother subjects as,weli. In order to identify that objectives were more similar
a.
8 0 tIT

than having one wordthan 1,200 subjects,the above objectives
in common the coding system assigned a unique number to more70 verbs, and 240 adjectives and modifiers. With this systemcould have been coded as follows:
School #1
Verb Modifie Subj. #1 Subj. #2
1. 2
List
2t 3
Name
3. 4
Define
126symptoms
175
types
376diabetemellitdt
376diabetes
342insulin
463diabetesinsipidus
376diabetes
,
L.
..
School #2
Verb Modifier Subj. #1 Subj. #2
1. 36Develop
2. 5
Explain
3. 8Compat*
275careplan
146physiol.
126sympt.
376diabetes
376diabetes
376diabetes
934retinop.
426shock
In this manner it was readily apparent by looking at the code numbers thatwhile each school had three objectives related to diabetes, they were not the sameby any means. Only the number 376 was common. It became far more imporctant toidentify objectives that had two subjects in common in order to 4dentify the simi-larities in curriculum content.
The use of the term "subject pairs" refers to an objective that includes twoof the subjects from the more than 1,200 coded. Any two objectives that upe twt.,of the subjects ) n the list are considered to be similar in content. For example,in the following two objectivs the common subjects are underlined.
1. Knows the principles of.good body mechanics.
2. Demopstrates princyles of body mechanics when giving patient care:.
Another example is as follows:to
1. List the classifications of drugs used in the treatment of cancer.0
2. What is the drug most frequently used in the treatment of cancer ofthe bone?
Although the objectives are not identical, the'faci that they include twoof the same subject words increases the probability that they are closely related.
The analysis of objectives based on common subject pairs revealed that 172pairs were common tooll three types of programs, 184 additiorial pairs werecommon to ADN and BSN, 165 common to diploma and BSN programs and 103 Pairscommon to diploma and ADN, as shown here.
t

BSN BSN Dip DipDip ADN ADN BSN .ADN
Number of common subject pairs 172 184 165 103Number of objectives involved 2,033* 725 676 325
Since common subject pairs might have a variable number of objectives with dif-;
!
ferent v rbs and modifiers, a frequency distribution was prepared to show the num/ber of t mes subject pairs had 2 or more related objectives. The following chartindicate the findings for the combinations of nursing programs.
In the comparison of objectives that were common to all three types of pro-grams, 17 different subject pairs (10 percent of all subject pairs) had threeobjectives for each subject pair. Looking further down the chart it is shownthat five subject pairs had 19 objectives each and one subject pair had as manyas 73 objectives which included the same two terms. The more objectives thereare with each subject pair, the greater the emphasis of those subjects in thecurriculum.
NUMBER OF SUBJECT PAIRS
No. of
Objectives
ADNDip BSN
# 1 % #t%ADN8SN #1%01%
DipBSN
Dip
ADN
-r-i
2 - - 73 1 39 70 i 42 47 46
3 17 1 10 41 122 28 1 17 23 1224 22 I 13 20 ill 24 1 15 14
113
5 21 I 12 20 ill 15 1 9 81
7
6 11 I 5 9 i 5 2 1 1 4I
3.8
7 4 1 2 7 1 4 5 1 3 21
1.9
8 11 I 6 5 i 3 6 1 4 21
1.9
9 12 t 7 2 i 1 2 i 1 11
0.9
10 12 1 7 1 I 0.5 3 1 2
11 7 1 4 3 1 2 2 1 1
12 7 1 4 1 1 0.5 3 1 2
13 5 I 3, - - 2 1 1
14 8 1 5 1 1 0.5 3 1 2
15 1 1 - '- I 1 1 0.6
16 2 i 1
17 3 1 2
18 4 1 2
19 5 1 3
20 - I -
21 1 1 0.5
22 4 1 2
23 1 I 0.5
24 4 1 2
25 - 1I 1 1 0.6
29 3 I 2
30 1 I 0.5
31 1 1 0.5
3/ 1 I 0.5
41 1 I 0.5
42 1 1 0.5
43 - 1 - 1 t 0.5
57 1 1 0.5
73 1 1 0.5,
82,4

t!;
In cases wherera subject pair had an unusually large number of objectives,such as the pair with 73 objectives in the three-program comparison, the sub-jects were general terms such as "patients" or "nursing ca16". The greatestpercentage of subject pairs had between two and five objectives per pair.
The verbs used in each objective give an idea et what is expected of thestudent. Verbs which require memorization of facts require less knowledge andability than verbs which require an understanding ol*.how the factt'relate tosituations and how facts are applied., When the oh,lectives were coded for com-puter analysis they were grouped into various levels, with level one being con-sidered the simplest and seven the most complex. the following chart gives ex-amples of each level.
Level #1 - cite, name, list, state, memorize--bevel #2 - identify: diagram, match
Level #3 - define, describe, explain, interpretLevel #4 - anticipate, planLevel #5 - adapt, modify, adjust, calculate, solveLevel #6 - analyze, compare, differentiateLevel #7 - evaluate
Theoretically one would expect objectives dealing with a particular subjectto increase in complexity throughout the course or curriculum. One would also qx-pect that the longer the program, the more opportunity to-deal with more subjectsat a complex level. This is not strongly substantiated by the data. Two possibleexplanations are suggested. Either there is a minimum of difference among thevaries programs in the complexity of subject matter in certain areas, or obJectivesare not carefully designed to demonstrate such progression of complexity:
The following charts illustrate the levels of objectives common to the var-ious types of programs. Of all the objectives common tof all three types of pro-grams, 409 were classified as Level 1. Of these, 148 were in ADN programs, 114in diploma programs and 409 in baccalaureate programs.
There were a number of objectives not claisi4;ed by level as the statement :
did not use verb reflecting any particular category of knowledge level expec adof the student. This figure is indicated by percent in Column 8.
LEINL 1
L--1AWl 148 23.1
0110 114 22.6
la 147 At,
ALL PAO- 409 29,1MANS
LEVELS OF SIMILAR OBJECTIVESCOMMON TO ALL THREE TYPES OF PROGRAMS
2L.-I 3
L--14LJ. Ll5 I
1....1
.7
f....1
8L.1 0
1-._ITOTAL
f--I.
138 21.6 167 26.1 5 .8 29 4.5 25 1,9 8 1.3 117 .18.3 3 .6 641 100.0
93 18.3 146 26.8 «0 1.5 .9 21 4.1 )6 3.1 111 21.9 3 .6 507 100.0_5
.
83 9.4 428 48.4 4 .5 3 .3 62 5.9 16 1.8 146 16.5 6 .7 885 100.01
314 15.5 731 35.8 .11 .8 37 1.8 98 4.8 40 1.9 374 18.4 12 .6 2013 100.0
,r
833 4 r4
"kk

BEST COPY AVAllABEE ris
For all three types of programs,. the majority of objectives fell in levelsl33 and relatively few appeared designed to evaluate the more complex levels ofprofessional knowledge and performance. The BSN programs had a greater percent-age of objective:. at higher levels primarily due to the large number in level3. Unexpectedly, the diploma programs showed a greater percentage in levels4, 5, and 7 although the difference was not.great.
Although the ADN programs state that their curriculum is limited in scopebutunlimited in depth, the analysis of objectives does not particularly sup-port this statement. It was found that MN prtigras cover-almost as many topicsas each of the other two program types but with fewer objectives for each topic.
KNOWLEDGE LEVEL OF OBJECTIVES COMMON TODIPL.-ADN, DIPL.-BSN, ADN-BSN
LEVEL 1 2 3 4 5 6 7I/ % # %#%f% # %#%f%
DIP 44 27.2 ,26 16 29. 17.9 2 1.2 1 .6 3 1.9 9 5.6
ADN 38 23.3 46 28.2 32 19.6 5 3.0 6 3.7 1 .6 3 1.8
TOTAL 82 25.2 72 22.1 61 18.7 7 2.2 7 2.2 4 1.2 12 3.7
LEVEL 1 2 3 4 5 6 7f % # % f% f% f% f% f%
DIP :74 26.3 57 20.2 67 23.8 4 1.42 1 .4 12 4.3 8 2.8
UN 56 14.1 60 15.1 193 48.8 1 .25 3 .8 23 5.8 11 2.8
TOTAL 130 19.2 117 17.3 260 38.5 5 .74 4 .6 35 5.2 19 2.8
LEVEL 1 2 3 4 5 6 7
.
# % I/ % # % f % # % I % f %.
ADN 58 21.0 59 21.4 70 25.4 7 2.5 4 1.5 15 5.4 0 -
75 16.8 44 .9.8 206 46.0 6 1.3 3 .7 17 3.8 14 3.1
TOTAL 134 18.5 103 14.2 276 38.0 13 1.8 7 . .9 32 4.4 14 1.9
Since the three types of professional programs vary in length from 2-4 years,there has been much discussion among educators and practitioners concerning theparticular time subject matter is introduced in a curriculum and ways of grant-ing credit for the same content which is offered at different levels. For exam-ple, in ADN programs, fundamental skills, such as taking temperature and bloodpressure, are taught in the first year. In BSN programs students are often notadmitted to nursing courses until their junior year. When they learn to takevital signs they receive lower division credit.
84. 4.8qi

Once the similar objectives were identified for the various contributionscf programs they were analyzed to determine how many were offered in each se-mester of the program. Findings indicate that in most instances the majorityof similar objectives are introduced during the first two semesters that stu-
ts are enrolled in nursing courses. The differences in programs appeal- toIrei:er as the curriculum progresses. This would seem to support the idea
that basic knowledge is similar'in the early part of all programs and wouldjustify a ladder concept which would grant a designated amount of credit intransfer situations. We therefore -submit that if all programs taught the con-tent that is similar in the same sequence and stressed differences later in theprogram a multiple entry and exit curriculum would be Iteasible and would promoteupward career mobility for those who desire to further their educational prepar-;ation.
The charts indicating time of introduction of similar objectives are shownbelow. Since diploma students spend their first year taking non-nursing courses,the majority of their similariobjectives appear in the first and second semestersof the second year. The ADN students begin nursing courses immediately and theirsimilar objectives are taught primarily-in the first two semesters of the firstyear. BSN programs show the greatest percentage in the third year.
THE YEAR AND SEMESTER THAT OBJECTIVES etMMON TO THE THREE TYPES OFPROFESSIONAL NURSING PROGRAMS ARE INTRODUCED* **
YR.
SOL
ACM.
OTP
WA
TOTAL
g 1
0 Cif
1
2
11/1i 3 1
0
1
1 70
22
I
'
I
3 rI
1 2IC. o
: 3
%: o j_
, 41 2s: o
3% o %
TOTAL0 %
207
22
5
234
3211
221
1
4 1 1
1
11 0
1222
35 1 13
1
1
- 0
1 i113
102
104
82
288
16 0 43
21 '191
91 1051
1 339
7
39
12
53
0
58
1111
8
-
7
105
231
336
21;
1
261
1
26
207
S 46 9
21 4) 5
89
147
147
17
1
24
24
o
o
3,
1 12010
639 100
495 100
876 100
100
Percentages soy total more than 100 due to roundingdif,decieels, .
"23 objectives not included due to incomplete coding
THE YEAR AND SEMESTER THAT.RJECTIVES COMOON TO THE ADN AND BSNPROGRAMS-ARE INTRODUCED*
,---44 TR. 1
.,' SEM. 1 1 '2 ' 3(.1 40 %10%1
v
AGM 87 41.6 : 94 30.2 1 1 631
115% 1 .21 q 1 0
VT. WI 12.2 194 13.0 1 1 .1
21 1 2 / 1 3
0 % I I. r% 1#
50 18.2' 19 6.91 24 8.7
32 7.21 36 8.11 21 4.71
82 11.41 55 7.61 45 6.3
II
five objectives not included due to incomplete c4ding
3 41 1 2 1 3 i 1 i 2 1 3I % 1 I % 1 %
1
116 26.0 1105 23.6 14 3.21
110 16.11105 14.6 1 14 1.9
10V
0 S I % 1 f S
1
107 24.0 13 2.9
101 14.81 13 1.81
TOTAL
I
275 100
445 100
720 100

..
BLSI CFI 11.1Miti
THE YEAR AND SEMESTER THAT OBJECTIVES COMMON TO THE DIPLOMA AND BSNPROGRAMS ARE INTRODUCED*
YR.
SEM.
DIP
11511
TOTAL
0
1
1 ' 2 1
Out %If3
% 0
21 ; 2SO I
SI13
'I 0
1 1
%IP3
2 1
,S 11
3
%113
13
6
19
4.71 0 -t
1 0
i
1.51 0 - ' 01
2.110 0 - 1 0
-
-
-
70
29
09
25.211
80
7.4i
381
14.81111
1
28.811 0
I
9.6114I
17.6.14
-
3.5
2.0
57
89
146
20.61 31
22.61 60p
2.101 91
11.2126
15.2/ 151
13.61 41
9.4
3.8
6.1
105
106
YR.
SEN.
Dip.
ADM
TOTAL
*five objectives net Included duo to incomplete coding
4
1
2 3 TOTALI
277 100
26.738 9.6 1 394 100
16.61 30 5.7 1 671 100
THE YEAR AND SEMESTER THAT OBJECTIVES COMMON TO THE DIPLOMA AND ADNPROGRAMS ARE INTRODUCED*
3
7 4 0 0 1 0 0
31 19 SS 34 1 0 0
38 12 55 11 1 0 0
23
1 1 2 1 3 I 1 1 2 1 3% I t 0 1 # 3 1 % %
36 23 58 37 0 0
33 20 27 17 11 10
69 22 185 27 17 S
five objectives not included due to incomplete coding
28 18 1 3
28 9 I 3 1125
2 25 16
TOTAL
151 100%
163 Ian
320 HMS
"Although limitations of ,time and resources prevented the Project fromaccomplishing all that was intended in the study of objectives, it did resultin identification of the problems which prevent the effective utilitation ofobjectives. As a result, adoption of a more uniform approach to the writingof objectives, re`h consideration given to development of knowledge at variouslevels, would provide a helpful approach to the development of nursing Curri-culums and would allow easier differentiation of skills and abilities amongthe various types of programs..
During the crturse of working with large numbers of objectiies prepared bymany different 4.ndividuals: it became apparent that if everyone would followsome basic rules when writing objectives it would be possible to better utilizethem for purposes of evaluating courses for transfer of chedit and evaluatingStudeint perf:xmance. In addition, a future study such as this one could becondOcted witn a much higher degree of reliability. SoMe suggestions whi,hwould have improved the quality of the data are:,-,
(
1. Objectives should be brief and concise and itr6Zbefimitedto the achievement of a specific goal. When subjects are too,broad or several subjects or goals are combined, it complicatesthe. evaluation of the achievement of the objectives.
When objectives require students to "list symptoms" or "describefactors" or "know the contributions of individuals in nursinghistory" the objectives should state a specific number. With-out such a clarification, the student is unable to determine whatis satisfactory performance and That is not. In addition, com-parisons between programs are difficult. "Lict three symptoms" -
or "Describe the contrIbuticn of ten individulls" eliminatlsthese difficulties.
(610-
76

3. Terms such as "knows", "understands", "appreciates" and"become acquainted with" should be avoided since they arevague and difficult to evaluate.
4. Objectives dealing with a particular subject in which thestudent is expected to become increasingly competent shouldbe developed with increasing levels of complexity thrOughoutthe curriculum. Too often the majority of objectives forsenior students in all types of programs are still at a lowlevel of "list" and "define" rather than "contrast", "develop","interpret" or "evaluate". Objectives dealing with a singlesubject should show evidence of progression from a simple tocomplex requirement of the student.
5. Too few curriculum objectives are directed toward clinicalexperience. Being able to list the symptoms of congestiveheart failure and being able to recognize that a patientis going into congestive heart failure may be quite diT-ferent. A studeqt may appear to know the theory of a sub-ject but be unable to apply it.
6. A number of objectives were stated in general terms thatdid not specify what was expected of the student. For
example, one states: "Provide nursing care to patientswho have disturbances of orientation." An objective ofthis nature does not distinguish the _differences in careexpected from the student as opposed to the aide. It does
not indicate that the student is supposed to deal with dis-orientation in any specific manner. An alternative state-
ment could have been: "When caring for a patient with adisturbance of orientation, the student initiates measuresto 1) insure safety and 2) assist in establishing or main-taining contact with reality.
7. Various topics were treated unevenly both within a singleprogram and among the different types of programs. A rela-
tively broad topic would be covered with one or two verygeneral objectives while a seemingly minor subject mighthave as many as 10 or 15. This makes it difficult to de-termine exactly what is taught and what degree of impor-tance is attached to various subjects.
The Limitations of the Study of Curriculum Objectives
A study involving analysis of over 12,000 objectives taught by 11 schoolsand written by an unknown number of faculty members presents difficulties
from the beginning.
As mentioned earlier, the lacK of a uniform approach to writing objec-tives made it difficult to design a coding system which could convey the ex-act meaning of all objectives. However, after receiving the materials fromthe schools, they were checked for accuracy of coding. All objectives re-
f 77'
.
Ste

ceived additional coding by two Nursing Project staff members. Since thiscoding was used extensively in the computer analysis the fact that it was doneb' the same two people insures consistency of application of the p-ocess.
Some of the limitations of the study are related to the use of objec-tives bylthe schools. Prior to the beginning of the study questions wereraised concerning whether or not it was possible to know if a school actuallymastered the majority of stated objectives. Since we had no way of measuringstudent achievement or of faculty implementation, the Education Task Forcemade the decision to work on the underlying assumption that schools,do im-plement their written objectives. 7,
The limitations of time and staff made it impossible for the NursingProject to do as much analysis of the data as would have been desirable.Despite thi$: the resulting information appears to point out similaritiesin pr3grams that could be useful in developing and evaluating nursing cur-riculums that would facilitate transfer of credit and career mobility.
Despite these limitations, the analysis of curriculum objectives madea significant contribution to the work of the Review and Evaluation Commit-tee, and to the entire Nursing Project. The findings of the analysis werestudied by the Committee and had an influence on their recommendations toincrease clinical experience for, nursing students. For example, the levelof emphasis on manipulative nursing skills, as shown by the analysis, wasconsidered inadequate and the Committee supported increased clinical empha-sis on the basis that this was the appropriate way to improve those skills.This influence is applied in the recommendations on Clinical experience foundelsewhere in this report. The need for additional clinical emphasis was alsosupported by survey returns from p-acticing RN's and senior nursing students.
Shown below are the lists of information coded by the participatinghirsing programs and the items that were coded.by the staff.
TYPE OF INFORMATION ACQUIRED ON EACH
INDIVIDUAL BEHAVIORAL OBJECTIVE
Cooedby
FaimltyMembers
Codedby
CBNPStaff
1. Major Topic (32)*2. Body System. (11)3. Age Group (9)
4. Nursing Action Required (10)
5. Clinical Setting Associated with the Objective (9)
6. Type of Objective (4)
7. Year and Semester Introduced (3) 1.8. Year and Semester Achievement Expected (3)
9. Essential to Pass the Course (2)
10. Action Term (71)/(50)**#11. Modifiers (254,/(187)12. Subject fl (1273)/(529)13. Subject #2 (1273)1(929)
v---
*Number of categories within the variable**Number of item groups resulting from the "synonym" process
.16
88 78

CHAPTER V
THE REGIONAL PERSPECTIVE:PROJECTIONS AND RECOMMENDATIONS
Having followed the regional format in collecting and analyzing the datafor the Nursing Project, we have prepared a report on each planning region toprovide assistance to those who will use this report in planning at the region-al level. We have included several types of data and information for this pur-pose, along with the recommendations.
In Attachment A, we have provided additional statistical data on eachplanning region which can be used with the descriptive information for eachregion and which is fundamental to the regional recommendations.
The enrollment data which are presented in the the regional reports inc'udethe enrollment as reported by the programs in nursing., Several of the programsoffering the baccalaureate degree in nursing reported freshmen and sophomoresand they are included in the totals presented on the following pages.
In order to simplify the identification of nursing students in the finalyear of the nursing program, we have used the word "senior" to mean any studentin the final year of the'progam. As used here it refers to second year ADNstudents, third year diploma program students, and fourth year students in thebaccalaureate program.
As shown on the regional charts in this chapter, the number of RN's em-ployed in 1972-73 is the full-time equivalent number which is less than thetotal number of active RN's shown in Attachment A. The FTE number employedin 1972-73 will obviously be reduced by 1980. The number to be added by 1980includes an increase to compensate for those who will. no longer be on activestatus by 1980. The total number of RN's needed by 1980 is therefore not thesum of those currently employed and the additional number needed.
The Full-Time Equivalent (FTE) number of RN's. use' in thP regional comepilations and throughout this repnrt was computed by ow:ling all the full -time,RN's and 50 percent of those employed part-time, plus 50 percent of those re-ported as active but not indicating the number of nours per week that theywere-employed. The same process was used to determine the FTE-LVN ratios.The followyg exemple illustrates ,the process:
Activity Levels Active FTE -RN's
Full-time 50t 50015-30 hours per week 11 55
Less thin 15 hours per week 50 25
Incomplete 6 3
TOTALS 666 583

B:ST COPY AVAILABLE
I
UPPER 8
RIO
GRANDE
F-
10.1 ..0010
PANHANDLE+.11000 01000 I WOO /Ma sa
1101 11097+1001+.".101104
1003.700"101171400 MILL01111
SOUTH.!........!tossec.! row
-PLAINS
PERMIANI-
0111S1
010 amsa
A..TiXA
.....10404! 3010
401 Pa"1040 .40
0004 40
KWEST CENTRALTEXAS-1-i
L.... 00.0, I !sow.' {414,4, 1010001011.110 ! 1011 !
BASIN,S es F.,...01 4, o SIV (dm+ 9±
COP ,
.."1ts . o 001 s9.. I t, .40.
CO NC T40 ,
jvALLEY,,F---.---4--, . 031
N RTHCE RA°
L-NORTH E
EX'I r
I Se- \le060100 1
0040.60:0.11100 also
041.1S
01400
.11 .1111
110
TEXAS PLANNING REGIONS
Sep*ember 1971
0.
1140
esti
ss54511.4
--a
010 .4:14t /I..1.I.
NA
......._>\,CENTRAL,..,....
..- .,.,...... A %vow '
W --..--tt TEXA.-- en% I
015, \ II" 0006"..,.. RAZOS01.11
2114 ;
VALLE
1444
40
11101.1
11/0.016110
4 11CAPITAL
.:51.110
s
...VS4..411
"%Ay...0P fre
511.1
ALAMO -71011010 L81.64-464Vg.
0..SO
I . 00400*0~IA
19SOUT
1004
4.RES4N0 E
,..
01.1.:71-GuLF
1:Si,.. . 4
4117I\SW 0441
BEND ...10OAtT.AL,
Form
2
TEXASIMMO 0440
LOWER RIOGRANDE VALLEY
21t 1011010
110010106
SOTEXAS

REGION I: PANHANDLE
Projected Population *
1970 330,3211980 362,8001990 395,000
Selected Regional Statistics
FTE-RN's
Employed in 1972-73: 778140ed to add by 1980:
Total RN's needed by 1980: 1,117
Ratio RN's/100,000 in 1973: 236Ratio RN's/100,000 by 1980: 308
LVN Data
Active LVN's in 1972: 837Ratio LVN's/100,000 ire 1972: 24§-
Number of LVN orograms:t 8
Hospit .1
County Population: 1970
MWO6,012
1444,./N
2.742 1
Wm'
6431461 461446ND , 3041141 i 0.4531413437 1.351 1,704 3.451
MOON I 14411664.41 4C411113 1411P431
14,010 i 24.443 I, N7 1064
KORN CAW* 144W2 .351 I 10.511 I 1.354 21,31 6,434
MN 044WWI
4-
MAY@ 4411/113616
53,016 Imomap coussirom3.441 ' 4,756
i
row I, tram ' Iowa ; as= " ,w41
10501 , 0, 3114 , 10,373 273 ; kola
RN Etycational
TypeProgram No.
B$N 1
ADN 1
Dip. 1
TOTAL 3
and Nursing Home Information
Information, 1973
No. ofEnroll. Seniors
343
127
316
14
52
84
786 150
Institution No. BedsStaff NursesRN's ' LVN',..
i
Ratios to Beds ofRN's
1LVN's
Hospitals 23 1,755i
568 1 557 1
I
1 to 3 1 to 3
Nursing Homes 30 1,797I
1241
I
1 to 47 1 to 141
In 1971, Region I had total population of nearly one-third of a million,and almost half (43.7%) was in Potter and Randall counties. This concentra-tion of population results in an unequal urban-rural distribution which ischaracteristic of the entire state.
The 152 RN's needed in hospitals under the optimum ratios include 113 forthe rural areas. Of the 86 RN's needed in nursing homes, are needed in therural areas.
*All populition projections' are from Population Prolect'lns for Texas CountiEs:1975-1990, Populations Research Center, Univoysjty Vf Texas at Austin.

In the chart on the previous page, the region has one RN for each 47nursing home beds. In the urban areas, the ratio is one to 37 beds and oneto 62 beds in the rural areas.
There are three professional nurse programs in the region: a BSN programat West Texas State University in Canyon, an ADN program at Amarillo College,and a diploma program at Northwest Texas Hospital. In 1973, the combined en-rollments in these programs totaled 786 students and 150 of them were seniors.
The region has done an excellent job in meeting its nurse needs and its236 FTE-RN's per 100,000 population is among the best in the state. Shodld 1,)
the existing programs continue to be as productive of graduates as they have-been in recent years, the region willlexceed the optimum ratios of the NursingProject by 1980 and employment opportunities for the graduates within the re-gion could become limited. The projections show that there will be an excessof 624 RN's in the region unless adjustments are made in enrollments.
There are eight LVN programs, one of them at Amarillo College with 70students enrolled in 1973.
For the ffreseeable future, Pegion I will experience an improvement to-ward meeting the optimum ratios in the urban areas and can concentrate onmeeting the rural nurse needs.
The geographic distance.to existing graduate programs in nursing hasrequired the region's nursing representatives to negotiate for the importing ofgraduate courses for faculty improvement. Under the recommendations for educa-tion in this report, this effort will be reinforced and structured for other -
regions having the same need.
So that Region I may continue to move toward meeting the optimum ratiosof the Project, these recommendations are submitted:
1. The initiation of the multiple entry and exit curriculumbe considered among a consortium of the several nursingprograms which would allow qualified students the optionof exiting at the LVM, ADN, or BSN level.
2. The total enrollment of professional and vocational nur-sing programs be adjusted to produce the numbers of grad-uates needed and to prevent an oversupply.
r

REGION II: SOUTH PLAINS
Projected
19,7i)
19801 990
Population
327
418,300456,300
County Population: 1970
Selected Regional Statistics
FTE-RN's
Employed in 1972-73:Need to add by 1980:
Total RN's needed by 1980:
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
LVN Data
Active LVN's in 1972:
RN Educational Information, 1973
561 Type No. of1,197 Program No. Enroll. Seniors
1,648 BSNADN
171 Dip. 1 125 73394
TOTAL 1 125 73
1 033Ratio LVN's/100,000 in 1972: Itg--
5Number of LVN programs:
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRN's ' LVN's
L
392 I 676
Ratios to Beds ofRN's ' LVN's
1 to 5' 1 to 3Hospitals 26 2,106
Nursing Homes '32 1,926 22 j 116 1 to 87 it 1 to 17
In 1970, over half (54.7%) of the nearly one-third of a million populationof Region II was in Lubbock County. As shoh:, in the projections listed above,the region is expected, to have substantial increase in population through'1990.
Lubbock is a major educational and medical center for the high pizins:-TexasTech University old Texas Tech University School of 'Medicine are located there.The only local supply source for professional nurses is the diploina program atMethodist Hospital in Lubbock. Enrollment in the 011 of 1973 was 125'studentgand 73 were seniors.
83 93

As shown in the data charts given above, the FTE-RN ratio to populationis 171 per 100,000 which ranks eleventh among the 21 regions. Data from re-licensure cards indicate that most of the RN's in the region are diploma grad-uatet.
Projections of the Nursing Project indicate that a substantial increasein number of RN's in Region II must be made for the optimum ratios to be met.As given on the data tables on the preceding page, a net increase of 1,087RN's is needed in the urban hospitals and in all nursing homes. Many of therural counties in Region II are projected to decline in population and the RNneed will be greater in the urban areas.
Throughout the region, nursing care in hospitals is dominated by LVN'swhere the ratio is one LVN to every three beds. As depicted above, there isone RN for every five hospital beds. The nursing home ratios are also wellbelow the optimum levels.
TFZNregion has minimal educational opportunities for those selecting nur-sing as a career. There are five LVN programs in the region including one atSouth Plains College (Levelland) and two others are in the public school dis-tricts of Lubbock and Plainview. In 1973, these three programs had total en-rollments of 133-students. The remaining two programs are in hospitals.
Region IIIis faced with an adverse ratio of RN's to LVN's and; under exist-ing circumstances this condition is not going to improve enough to meet the op-timum levelirof professional nurses. At the current rate of producing profession-al nurses, the region will be 621 RN's short of the optimum level by 1980.
So that Region II can move toward early improvement of its deficiency ofregistered nurses and achieve the optimum levels supported by the Nursing Project,we recommend:
1. The initiation of a multiple entry and exit baccalaureatenursing program in Lubbock. The program should not be ini-tiated prior to 1976 and only if faculty and student re-cruitment would not adversely affect existing programs.
2. Educators in the region should explore the offering of bac-calaureate nursing courses in Lubbock through cooperative ar=rangements with.existing schools of nursing until the Lubbock
_i0ogram is in operation.

REGION III: NORTH TEXAS
Projected Population
1970 212,5281980 212,4001990 212,400
County Population: 1970
Selected Regional Statistics
Ae"
FTE-RN's RN Educational Information, 1973
Employed in 1972-73: 410 Type No. of
Nend to add by 1980: 549 Program a2. Enroll. Seniors
Total needed by 1980: 858 BSN -
ADN 1 134 60
Ratio RN's/100,000 in 1973: '93 Dip. - -
Ratio RN's/100,000 by 1980:TOTAL 1 134 60
LVN Daa
Active 1VN's in 1972: 73.1
Rati9 LVN's/100,000 in 1972: 331
Number of LVN programs: 8
Hospital and Nursing Home information
Institution No. BedsStaff NursesRN's ' LA's
Ratios to Beds ofRNs '
1
LVN's
Hospitals 18 1,290 310 427 1 to 4 : 1 to'3
Nursing Homes 36 2,669I
24 14511
1 to. 11 1. to 18
The 12 counties which make up Region III are located along the upOer RedRiver and over 57 percent of the 1970 population of 212/,528 was located 'in Wichita
County. Official projections show virtually no chahgein total population to '1990.fT
_ ____ _ __ ___ ___u______ -
\' e 4 0 FTE-RN's is made up of 459 nurses who work full or part -time. The
193 RN's per 100.000 popultationris tenth among the 21 regions.O
The optimum levels of RN's recompended by the Nursing Project would respirethat 138 RN's be produced for the region beyond those currently projected throughthe existing supply. pattern.
- 85 id

About 50 percent of the need for RN's under the optimum levels is inrural hospitals and 37 percent of the__ is in nursing homes in WichitaCounty. The ratio of one RN to every 11 nursing home beds is far belowthe level of 1 to 15 recommended by the Project.
There is one professional nurse program in the region, a two-year ADNprogram at Midwestern University in Wichita Falls. The enrollment in the fallof 1973 was 134 students and 60 were seniors. Approximately 67 percent of theRN's in the region were reported as having no degree. At the present time, .
courses leading toward the baccalaureate degree in nursing are not availablewithin the region.
There are eight LVN programs in the region, including one at VernonRegional Junior College. Enrollment in 1973 was 34 students.
With a stable population, the existing ADN program can produce the re-quired number of professional nurses through a modest increase in enrollment.In order to provide the optimum level of RN's and improve educational oppor-tunity for professional nurses within the region, the Project recommends:
1. The existing ADN program increase its enrollment by twentypercarat.
2. The educators in the region consider implementation of themultiple entry and exit curriculum, to be initiated after1976, contingent upon the effect this would have on facultyand enrollment in the existing programs.

I
REGION IV: NORTH CENTRAL TEXAS
Projected Populacion
1970 2,636,3741980 3,147,3001990 3,802/00
Select d Regional Statistics
RN Educational Information, 1973
Type 'No. ofProgram No. Enroll. Seniors
BSN 5 3,057 479
ADN 5 794 332
Dip.
TOTAL 10 .3,856 811
FTE-RN' s
Employed in 1972-73: 5,565
Need to add by 1980: b 398 "----
Total RN'_ needed by 1980: 9,819
County Population: 1970
aloe13.4?' SS22S
mommis7 ?via)
CM**LW
PIPPO
2 2 ,TOS
MINT41,41
',WNW IMAMPNO P.00 73all
,,S27.31120,1112
- 12.3*,Nom ANNON
11,3{11 ILIA
lMtw4S 711 44,444
1010
Ratio RN's/100,000 in 1973: 211,
Ratio RN's/100,000 by 1980: 312
LVN Data
Active LVN's.in 1972: 6,108Ratio LVN's/100,000 in 1972: 232
Number of LVN programs: 24
!Hospital anirsing Home Information
.
Institbtfon
1"
No. BedsStaff NursesRN's ' LVN's
1
Ratios to Beds ofRN's ' LYN's
Hospi tisls 97 11,948
1.-..,
4,025 ! 3,758 1 1 to 3 , I 1 to 3,1L---------i
Nursin0 Homes 169 15,982 )227 1,650 bpi to )0 PT 015i
The most heavily populated regidon in the state, Region IV has 19 counties
and in 1970, Dallas County had half of the region's population of/over 2.6 mil-
lion. The Ohcentration of population in this-region.is projected to continue
to increase te mat with over a million- increase_ P2ont 1970 to 1990._
The Dallas-Fort Aorth area has extensive and varied medical facilities
and educational programs at all'levels. The 97 hospitals employ over 4,000
Irofessioral nurses and almost CDOO'L .s. Of the 97 hospitals, 65 are inDallas and Tarrant Counties and five of them have over 500'beds each.
:1787 ',

Existing ratios of RN's to beds in hospitals are close to the optimum levelsrecommended by the Nursing Project but well below the level recommended fornursing homes.. About three out of every five RN's-employed in the region workin hospitals.
The FTE-RN ratio of 211 to 100,000 population is sixth in rank among the21 regions and under optimum levels, should increase to 312 per 100,000 by 1980.Under the existing supply pattern for professional nurses, the region would beshort of the optimum level by; over 1,200 RN's by 1980. Despite this potentialshortage under optimum levels, Region IV is in better condition in availa-bility of RN's than most other regions of the state. Dallas County in particul-dis a popular location named by many nursing students as their preference to boy'repractice?.
There are extensive nursing education facilities and programs ofall types,in the iregion. These include, at the baccalaureate level, Baylor University,DallavBaptist University, and Texas Christian University, all privately supportea.In addition to these three private programs, there are two publicly supported bac-calaureate programs at Texas Woman's University (Dallas Center) and The Universityof Texas at Fort Worth. There are four ADN programs in the region at DallasCounty Community College (El Centro Campus), at Cooke County Junior College,Grayson County Junior College, and Tarrant County Junior College (South Campus).Enrollments for these programs are shown on the charts above. A fifth ADN programwas approved in November, 1974, for Southwestern Union College at Keene, Texas.
F
these professional nurse programs, there are some 24 LVN pro-with several in community colleges and public school districts.23 enrolled at El Centro College and 34 at Grayson County
In addition tograms in the regionIn 1973, there wereJunior College.
Despite the wealth of nursing programs concentrated in the Dallas-Fort Wortharea, the region contains outlying rural areas which have need for more RN's inrural hospitals and nursing homes. Some of these rural areas are sharply defi-cient in adequate clinical facilities for the education of professional nursesand have not benefitted from the large numbers of students educated in the urbanareas of the region.
In other parts of this repo t we have addressed the problem of acquaintingstudents with the benefits of rural life and work through clinical rotation.The Nursing Project therefore recommends:
1. The nrofessional programs of nursing in Region IV move to.imp.ement the recommendations on providing rural clinicalexperience for students.
2. The professional programs of nursing in the region move toest4blish joint faculty appointments for qualified servicepersonnel in the non-urban hospitals and other patient caresettings.
3. The recommendations on continuing education in this report bevigorously applied to all counties in Region IV.

REGION V: NORTH EAST TEXAS
Projected Population
1970 202,3461980 205,6001990 193,000
Selected Regional Statistics
County Population: 1970
FTE-RN's RN Educational Information, 1973
Employed in 1972-73: 325 Type No. of
Need to add by 1980: 607 Program No. Enroll. Seniors
Total RN's needed by 1980: 857 BSN -
Ratio RN's/100,000 in 1973: 161
ADNDip.
2 183 74.
dEP
Ratio RN'z/100s000 by 1980: 417TOTAL 2 183 74
LVN Data
Active LVN's in 1972: 602Ratio LVN's/100,000 in 11572T-775-Number of LVN programs: 4
Hospital and Nursing Home Information
Institution No.Staff NursesRN's ' LVN's
I
Ratios to Beds ofRN's ' LVN's
t
Hospitals 1 1,120I
215 1 352I
1 to 5 1 to 31
Nursing Homes 29 2,475 20 1 161 1 to 1241 1 to 15
The nine counties of Region V in extreme northeast Texas are predominantly
rural and the population is projected to decline through 1990. About one-third
of the 1970 population of 202,346 was in Bowie County (Texarkana).
While there were 460 RN's in the regicn in 1973, only 355 were active and
the FTE-RN level was 325. This amounted to 161 RN's per 100,000 population
which was thirteeth among the 21 regions.

The data shown is the charts given above for Region V display the pre-
dominance of LVN's to RN's in the ratios in hospitals and nursing homes and thisindicates that the existing RN programs will need to increase the number ofgraduates over the next six years to provide the optimum level of RN's beingrecommended by the Nursing Project. An additional resource for the region isfurther education for qualified LVN's who seek to become RN's.
The two professional nursing programs are both at the ADN level and arelocated at Paris Junior College and Texarkana Community College. Their combined
enrollments in fall, 1973, totaled 183 students and 74 of them were seniors.
In order for Region V to arrive at the optimum levels of RN's by 1980,including provision for meeting the needs of the area which has a high agingindex, the Nursing Project recommends:
1. Provision be made for providing continuing education forLVN's and RN's in the -egion.
2. Increase enrollment in the ADN program to produce over 200new graduates above the current production level by 1980.
3. Emphasize geriatrics in the curriculum now available.

FTE-RN's
Employed in 1972-73:Need to add by 1980:
REGION VI: EAST TEXAS
Projected Population
1970 429,1191980 451,6001990 453,400
Selected Regional Statistics
Total RN's needed by 1980:
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
County Population: 1970
3,75 KW I
- UM"20,111/1
VW MOT J-u, GE.22,155 ' 75ln
/41111.1111011 9'.(3"24,4g.
A/WM 101111MI7J119 132,001
RN Educational Information, 1973
655 Type No. of
1,343 Program No. Enroll. Seniors
1,883 BSN * - -
ADN 1 108 42
153 Dip. 1 170 31
417TOTAL 2 278 73
LYN Data
Active LVN's in 1972: 1.592RatioloVN's/100,000 in 359Number of LVN programs: 10
Hospital and Nursing Him Information
*An upper level BSN programwas approved in 1974 for
Tyler State College
Institution
.
No. BedsStaff NursesRN's ' LVN 'L
1
.
Ratios to Beds ofRN's , 1 131.1'4
,
Hospitals 33 2,517 459 : 958 1 to 5 : 1 to 2
Nursing Homes 59 5,6091
50 3321
1 to 112i 1 to 17
The population of 14 county Region VI is projected to steadily increase
over the next 15 years.
The FTE-RN ratio is fifteenth in rank among the 21 regions with 153 FTE-
RN's per 100.000 population. There is a deficiency of RN's in both hospitals and
nursing homes as shown in the charts displayed above. About 58 percent of the
current deficit of RN's is in hospitals in Smith and Gregg counties.
The chief needs of the region are theimpuction of more RN's and to retain
in the region those who have completed thei00.1rsing education within the area.
91 4 11

There are two basic professional nursing programs in the region: an ADN
program at Kilgore College and a diploma program at Texas Eastern School of
Nursing in Tyler. These two programs had 278 students enrolled in the fall
semester 1973, and 73 of them were seniors. A new upper level 85N program
is being implemented at Tyler State College and the program should provide
the critical retention factor to prevent out-migration of professional nurses
who seek the baccalaureate degree in nursing.
The dominance of LVN's over RN's in the region, particularly in the hos-
pitals and nursing homes, needs to be reversed to meet the optimum level of
professional nurses recommended by the Nursing Project.
There are about ten LVN programs in the region and there were 1,592 active
LVN's, full and part-time, in 1971-72.
In order to permit Region VI to meet the optimum level of professional
nurses by 1980, the Nursing Project recommends:
1. Emphasis be placed on providing continuing education forthe LVN's and RN's in the region.
2. Increase the enrollment of the professional nurse pro-grams in the region to produce an increase of 952 RN's
above those projected under current enrollments.

REGION VII: WEST CENTRAL TEXAS
County Population: 1970
Projected Population3.1172
,.434
MOPIUNfo, I
occ.ou1.073
STMITAIL1
2 ;SIT
1,344 I
Nis&16.210
WIPIELL
1113612
minat
11,104
t;I
IMINOCIWORT
2201
oomMeo,3,313
ClL7AJ
19701980
1990
280,108255,600235,200
Selected Regional Statistics
FTE-RN's
Employed in 1972r73: 469Need to add by 1080: 688
Total RW's needed by 1980: 1.030
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
167403
LVN Data
Active LVN's in 1972:Ratio LVN's/100,000 in 1072:Number of LVN programs:
Hospital and Nursing Home
mmois11.41 4
77736.°41,
71:0010.2811 25Ar7
CALMAR 0110001
RN Educational Information, 1973
Type No of
Program No. SeniorsEnroll.
BSN - - -
ADN -IM
'Dip. 1 56 24
TOTAL 1 56 24
Information
Institution...
No. BedsStaff NursesRN's
1
, LVN's.
Ratios to Beds ofRN's
i
LVN's_
Hospitals 31 1,653 370 1
1
751
.
1
1 to 4 t 1 to 2
Nursing Homes 60 4 100 24' i 313 1 to 170 1 to 13
The population of Region VII is projected to Readily decline through 1990.
Taylor County is an exception and will increase in population.
Nursing care in the region is predominantly
presented above indicate that LVN's outnumber RN
region has the state's highest ratio of LVN's to
and the RN ratio is 173 per 100,000.
Region VII has the highest ratio of nurshgper 100,000) of any in the state, and the 1064d
10393
delivered by LVN's and the data's by about three to one. The
population (441 per 100,000)
home beds to population (1,120
highest ratio of hospital beds
01"
a

(548) per 100,000 population. The population consists of a high percentage
)f older persons and nursing homes, depicted on the preceding page.
The comparatively large numbers of health care facilities, low RN ratios,
high LVN ratios, and high aging index point, to the region's need for additional
professional nurses.
There is only one professional nurse program available, a diploma program
at Hendrick Memorial Hospital in Abilene. Efforts to establish an ADN program
in the region outside Abilene have failed because of inadequate clinical fa-
cilities. Enrollment in the diploma program in 1973 totaled 57 students with
24 in the third year class.
To meet the optimum levels of professional nurse care as recommended by
the Project, th region will need an additional supply source for nurses, and
688 additional RN's will be required.
Abilene does not have a publicly supported i.istitution of higher educa-
tion. Local voters have rejected bond issues to establish and support a com-munity college and one of the community's alternatives for meeting educational
needs is to turn to the three privately supported universities in the commun-
ity, Abilene Christian College, Hardin-Simmons University, and McMurry College.
Atithe present time, these institutions have the capability to provide the on-
nursing courses for the professional nurse curriculum.
The Nursing Project therefore recommends:
1. Top priority be given the continuing education needs of
LVN's in the region.
2. That an investigation be conducted into.the feasibility
of establishing an ADN program in the region if faculty
and clinical resources are available.4
3. Consideration be given to the establishment of a multi-
ple entry and exit nursing program through the BSN levelat one or in a consortium of the privately supported uni-
versities in Taylor county.
4. Emphasize the recruitment of qualified LVN's into RN pro-
grams.

REGION VIII: UPPER RIO GRANDE
County Population: 1970
rd)111..112
WI 111011M
1.:11
Projected _Population
1970 379,261
1980 463,0001990 573,500
Selected Regional Statistics
FTE-RN's
Employed in 1972-73: 786
Need to add by 1980: 855
Total RN's needed by 1980: LILL__
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
LVN Data
Active LVN's in 1972:Ratio LVN's/100,000 in 1972:Number of LVN programs:
202317
499128
3.
RN Educational Information, 19/3
TypeProgram No. Enroll.
No. ofSeniors
BSN 1 551 98
ADN 1 80 33
Dip. - - -
TOTAL 2 631 131
Hospital and Nursing Home Information
Institution No. BedsStaff NursuRN's : LVNI
Ratios to Beds ofRN's LVN's
Hospitals 15
=1..P1,872
I575 i 328 1 to 3. , 1 to 6
Nursing Homes 8 548I
18 1 45 1 to 30i 1 to 12
Texas' westernmost planning region consists of six counties along the upper
Rio,Grande, and of the total population of 379,261 in 1970, all but 20,000 were
in El Paso County. The population is projected to increase by almost 200,000 by
1990, as shown above. Most of the increase will occur in El Paso County and
three of the six counties will decline in population.
There are only two hospitals in the region outside El Paso County, one in
Brewster County and another in Culbersen. There are 16 In El Paso with two of
them in the 300-499 size range. Total number of hospital beds is 1,872 and
there are.575 RN's and 328 LVN's employed,inAT.hx
95
105

Thre are eight nursing homes in the region. All but one of them are in
El Paso, and they have a total of 548 beds. There are 18 RN's and 45 LVN's
employed in these homes. The low aging index for the. region accounts for the
small number of these facilities. Only 22,555 of the 1970 population of
379,216 in 1970 were 65 or older.
There were 866 active and 309 inactive RN's in the regionin 1972 with
the FTE-RN's totaling 786. While the number of RN'somployedvin hospitals,full or part-time, was 575, the FTE-RN's in hospitals was 515.
The educational level of the RN's in the region is somew' law, with
612 of the.866 indicating they did not have a degree.
There are 202 FTE-RN's for every 100,000 population in the region, velich
ranks ninth among the 21 regions. At the current rate of supply, the region
will have a potential surplus of 411 RN's by 1980. However, under the optimum
ratios of the Nursing Project, a-deficit of 122 is projected. This deficit
can be overcome by modest increases in enrollments .in the existing RN-programs
in El Paso.
There are two professional nurse programs in the region, both in El Paso.
Enrollment in the BSN program at UT-E1 Paso School of. Nursing in 1973 was 551
students and the ADN program at El Paso Community College had total enrollment
of 80 students. The total enrollment was 631, with 131 seniors. In addition,
there are three LVN programs, one in Brewster County and two in El Paso.
In order for Region VIII to produce the 122 additional RN's needed to
meet the optimum ratios, the Nursing Project recommends:
1. The two existing registered nurse programs increase en-
rollments to produce an additional 25 graduates per year
to 1980.
10696

FTE-RN's
Employed in 1972-73:Need to add by 1980:
REGION IX: PERMIAN BASINO
Projected Population
1970 304,3261980 345,3001990 382,200
County Population: 19/0
I
was ; wax , lam
I
wawa raw 1 MOM
4.311 , 1714 , 11,1M
.
um* MOD MI6 MUM OuleNta
104 %MO I OJOS Sal '''10
Old... r._ 1 dull ,
1011.1
INIVIII / 'N.,k's , 4,1114.911 1' ,
Selected Re_gianal Statistics..
Total RN's needed by 1980:
f74428
985
Ratio RN's/100,000 in 1973: 153
Ratio RN's/100,000 by 1980: 276
LVN Data
Active LVN's in 1972: 956
Ratio LVN's/100,000 in 197: 309
Number of LVN programs:
RN Educational Information, 1973
Type No. of
Program No. Enroll. Seniors
BSN -
ADN 1 104
Dip. Imp
TOTAL 1 104 49
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRNs , LVN's
1
Ratios to Beds ofRN's ' LVN's
..
._
Hospitals 22 1,331 342I
1 690 1 to-4 i "1 to 2
Nursing Homes 16 1,199 16 : 91 1 to 75 : 1 to 13
Region IX is a big, 17 county region in West Texas whose 1970 population of .
over 300,000 is projected to increase to over 382,000 by 1990. Over half of the
1970 population was in Ector and Midland counties, and Ector County is expected
to increase from almost 92,000 in 1970 to over 159,000 by 1990.
There are 520 active and 185 inactive RN's in the region for a 74 percent ac-
tivity rate, one of the best in the state. When the FTE-RN's are computed among full
97
II I
1117

and pdrt-time nurses, the region has 474. The FiTE-RN ratio is 153 per 100,000
population, which is fifteenth among the 21 regfons.
Despite the high activity rate of RN's, they are outnumbered in hospital
employment, where 342 RN's and 690 LVN's are employed in hospitals having a total
of 1,331 beds.
The region has.a low aging index which helps account for the region-having
only 16 nursing homes (1,199 beds) which employ 16 RN's and 91 LVN's.4
The region has only one registered nurse pr9gram, an ADN program at Odessa 1
College. In 1973, the program had 104 students enrolled. There are also seven
tVN programs, including one in Odessa College which had 44 students enrolled in
1973.
-The existing supply pattern for RN's for Region IX 01111 not provide enough
RN's to meet the level recommended by the Nursing Project; the region will be
short by 221 RN's. It is important that he number of RN's be increased in this
region so that the LVN, dominance can be reversed.
In order that the 221 RN's be produced in addition to those projected undiy
current supply patterns, the Nursing Project recommends that: 4
1. The existing ADN program in the region expand its enrollment
by 40 percent by utilizing extended clinical campuses, when
appropriate, to supply regional needs for nurses.
BSN courses be made available to nurses within the rtgion,
should interest and potential participation by nurses with-
in the region be high enough. Theis courses can be imported
from an existing BSN program.
1-0-8
93
411

FTE-AN'' s
REGION X: CONCHO VALLEY
Projected Population
1970 110,5501980 116,600
1990 109,400
Selected Regional Statistics
Employed in 1972-73:Need to add by 1980:
To1 RN's needed by 1980: /
.Ratio RN's/100,000 in 1973:Ratio Rys/100,000 by 1980:
LVN Data
Active LVN's in 1972:Ratio LV /100,000 t T97i:
)NUmber f LVN program!:
County Population:
sutraken ;
1101 Plot? cam)oto tsar-- WCIA1101
- - aril
ICiMr 1611110
1970
004
277
RN Educational Information 1973
Type No. of
Program No. Enroll. Seniors391
580 BSN -
ADN 1 207 54
221 Dip. ..
464TOTAL 1 207 54
489389
3
Hospital and Nursing Home Information
Institution No.
,- Staff NursesRN's 1 LVN's
Ratios to Beds ofRNs I LVN's
. .
Hospitals ' 16 920 185i
305 1 to 5 1 to 3
Nursing Homes 20 1,169 16 65 1 to 58 1 to 18
The population of ReOon X is projected to increase slightly to 1980 andthen decline by some 7,000 to 1990. The 13 counties are rural with-the ex-ception of Tom Green County (San Angelo) which had almost 65 percent of theregion's population in 1970 and is projected to increase from over 71,000 in1970 to 85,000 by MO.
There are 305 active and 119 inactive RN's in the region and some 277FTE-RN's. There are 176 RN's and 305 LVN's employed in hospitals in the region
ft'which have 920 beds. The.aging index,d(ithe region is quite high and there are16 RN's and 65 LVN's employed in 20 nursing homes having 1,169 beds.
99
109

\
At the present time, the FTE-RN ratio is" 221 per 100,000 population, and
this is fourth among the 21 regions. Under the optimum ratios ado^ted by the
Nursing Project to provide more RN's, the existing supply pattern for the re-
gion will provide all but 56 nurses.
There is one registered nurse program in the region. Angelo State Univer-
sity offers the ADN program and in 1973 the enrollment totaled 207 students.
There are three INN programs in the region and one of them, in the San Angelo
Independent School District, enrolled 71 students in 1973.
The region can make some upward adjustments in enrollment and meet the opti-
mum ratio needs as projected by the Nursing Project. It is therefore recommended
that:
1. Enrollment in the ADN program be increased by 1975 so as
to increase the number of additional graduates by approx-
imately 11 per year.
2. BSN courses should be made available within the region
provided the potential for improvement is shown by nurses
within the region. These courses can be imported by an
existing school of nursing.
oo"
100

O
REGION XI: CENTRAL TEXAS
Projected Population
1970 433,7261980 433,5001990 435,700
County Population: 1970
),... IMA
OESCIul ' 22.5114-."
t0,104 e , ,
novae ' , ,7,110 .., . Br WPM
NILLS 147,533 .-
' '42'2 COPC111 ". ..
,A
S9.31i ... ._ , pug-...
.5
.,. 17,300SO yd. 423 \
.
540 ELIA
124,443 -
Selected Regional Statistics
FTE-RN's
Employed in 1972-73:Need to add by 1980:
Total RN's needed by 1980:
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
LVN Data
RN Educational Information, 1973
967 TypeS56 Program No. Enroll.
1,576 BSN 1 182'.
,ADN 2 277
221 Dip.
367TOTAL 3 459
Active LVN's in 1972: . 1,272
Ratio LVN's/100,000 in 1972: 291
Number of LVN programs: TO
Hospital and Nursing Home Informs tihn
Institution No. BedsStaff NursesRN's ' LVN's
1
-Ratios to Beds ofRN's ' LVN's
1
Hospitals 30 2,220I
756 742I
1 to 3 1 to 3
Nursing Homes 66 4,819 70j 337I
1 to 691 1 to 11
No. ofSeniors
dm
152
General population of the Central Texas region is projected to remain stable
to 1990, with a slight increase of about 2,000 from 1980 to 1990'. Except for
McLennan (Waco) and Bell counties, which had about 63 percent of the region's
population in 1970, most of the counties are rural and most are expected to de=
cline in population over the next 15 years
Region XI' has 1,062 active and 389 inactive RN's and thOTTE-RN' t total
967. There are 678 RN's and 742 LVN's mployed in hospitals having 2,220 beds.
Most bf the counties have a high aghig ndex which explains the large number ofnursing homes which have a total of '441 ds and employ 70 RN's and 337 LVN's.

The region currently has a FTE-RN ratio of 221 RN's per 100,000 popula-tion and the existing supply pattern is adequate not only to meet the opti-mum ratio but to exceed the needed number by 21 RN's.
Region XI has excellent health care facilities and has previously pr.-vided for professional nurse educationto meet its needs at the basic programlevel.
There are three professional nurse programs available: a BSN program
.at Mary Hardin-Baylor College (Belton). and ADN programs at Central TexasCollege (Killeen) and McLennan Community College (Waco). In the fall of
1973, enrollments in these programs totaled 459. There are also 10 LVN pro-
grams in the region.
The Nursing Project has identified needs in Region XI as more RN's inthe rural areas and emphasis oh nursing care of older people. It is there-
fore recommended that:
1. Existing programs should place particular emphasis on thegeneral recommendations in the field of geriatrics andrural clinical experience.
2. Emphasize recruitment of qualified LVN's into RN programs.
3. As the RN:population ratio improves in the region, consider-ation should be given to the consolidation of the smaller LYNprograms.

REGION XII: CAPITOL
Projected Population
1970 446,6021980 485,3001990 544,600
Selected Reg:lanai Statistics
County Population: 1970
FTE-RN's RN Educational Information, 1973
Employed in 1972-73: 1.076 Type No. of
Need to add by 1980: 552 Program_ No Enroll. Seniors
Total RN's needed by 1980: 1.388_ BSN 1 944 182
ADN
Ratio RN's/100,000 in 1973: 236 Dip. 1 161 41
Ratio RN's/100,000 by 1980: 286TOTAL 2 1,105 223
LVN Data
Active LVN's in 1972: 912
Ratio LVN's/100,000 in 1972: 200Number of LVN programs: 6
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRN's ' LVN's
Ratios to Beds ofRN's ' LVN's
Hospitals 22 1,735 785 1 469 1 to 2I
1 1 to 4
Nursing Homes 37 3,731 45 1 2231
1 to 83 1 to 17
In 1970, Travis County had over 66 percent of the total population of over
446,000 in Region XII. The other nine counties are predominantly rural and
therefore the best health care facilities are in Travis County.
The charts shown above indicate that this region has excellent ratios of
RN's to hospital oeds, for example, and its FTE-RN's to population is 236,
among the best in the state. The comparative low level of RN's in nursing
homes is characteristic of nursing homep in all regions of Texas but the ratio
of one RN to every 83 beds is better tbarfirnost of the other regions.
103

If the current supply pattern remains stable, Region XII will have no dif-
ficulty in meeting the optimum ratios of the Nursing Project. If employment
opportunities are not increased, the region may have an excess of over 200 RN's
by 1980. The surveys of the Nursing Project have shown that the general prefer-
ence of RN's for urban and large hospital employment could contribute to an over-
supply in the urban area of this region.
There are two professional nursing programs available, both in Austin. The
University of Texas School of Nursing offers the BSN and Brackenridge Hospital,
in cooperation with the Austin Community College, 3ffers the diploma program.
In 1973, the enrollments of these two programs totalled 1,105 students, including
223 seniors.
In order that the maximum utilization of educational resources in the urban
areas. be made available throughout the region and to improve the level of nursing
care in the rural areas, the Nursing Project recommends that:
1. The existing nursing programs adopt the recommendationsin the field of geriatrics and rural clinical experienceas high priorities.
2. The consolidation of LVN programs as the RN:population
ratio improves.
3. Adjustment of enrollments in all types of nursing pro-
grams as needed to maintain the desired RN and LVN to
population ratios.
114
104
I

REGION XIII: BRAZOS VALLEY
Projected Population
1970 129,494
1980 127,400
1990 126,200
Selected Regional Statistics
FTE-RN's
204Employed in 1972-73:Need to add by 1980: 1R4
Total RN's needed by 1980: 347
Ratio RN's/100,000 in 1973: 155
Ratio RN's/100,000 by 1980: 272
LVN Data
Active LVN's in 1972: 236Ratio LVN's/100,000 in 1972: 194Number of LVN programs: 2
Hospital and Nursing Home
County Population: 1970
RN Educational Information, 1973
TypeProgram No.
BSNADNDip.
TOTAL
Information
MM.
IND
No. ofEnroll. Seniors
institution No. BedsStaff NursesRN's ' LVN's
Ratios to Beds ofRN's ' LVN's
Hospitals 462I
146 1441
i
1 to 3 1 1 to 3
Nursing Homes 15 1,332 11 I 11 1 to 121 1 to 20
Six of the seven counties in Region XIII are projected to decline inpopulation over the next 15 years while the seventh county, Brazos, which
had about 45 percent of the region's population in 1970, is expected to in-
crease from nearly 58,000 in 1970 to over 74,000 by 1990. Texas AM Univer-sity is located in Brazos County and this major institution accounts for a
large share of the population. The re!-' "on as a whole is considered rural
and contains fewer health care facilities than some other-regions of similar.,
characteristics. c -
%I/6
115
OP
alb

There are 232 active and 104 inactive RN's in, the region and the FTE-RN
count is 204. The FTE-RN ratio to population is 155 per 100,000, and ranks
fourteenth among the 21 regions.
There are eight hospitals in the region and they have a total of 462 beds.Excellent ratios in RN-LVN staffing exist in these hospitals on a regional basisas 146 RN's and 144 LVN's are employed in them. The region as a whole his ahigh aging index which partially accounts for the 15 nursing homes, with a totalof 1,332 beds and which employ 11 RN's and 65 LVN's.
The most serious problem in the region is the low number of RN's workingin nursing homes. This problem exists throughout all regions of the state andthe optimum ratios are designed to provide more RN's for employment in this im-portant area of health care. The current ratio of RN't to nursing home beds inthis region is one to every 121 beds. The Nursing Project is recommending one toevery 15 beds.
There are no schools for registered nurses in Region XIII. The supply pat-tern for the region, especially Brazos County, is considered to be attributable,in part, to the nurses who are wives of students or employees of Texas A84.1 Univer-sity. There are two programs for LVN's, one in Brenham (Washington County) atBlinn College and one in the Bryan public sChools. In 1973, they had combinedenrollments of 63 students.
The projections of the Nursing Project show that with the present supplypattern for RN's remaining stable, the region wilLneed4Only an additional 54RN's by 1980 to meet the optimum needs as recommended by the Nursing Project.This amounts to about eleven new nurses per year beyond the present supply andthe Project concludes this number could be recruited without the necessity toestablish a new program.
To provide the increased number of RN's, especially in nursing homes, theNursing Project recommends:
1. Efforts be made by employers, especially nursing homes,to recruit RN's.
2. Continuing education courses be made available to qual-ified LVN's within the region to improve knowledge and j.skills and which can apply toward an RN curriculum.
3. Encourage and emphasize geriatric courses and trainingfor all nurses in the region.
4
116
Gift

FTE-RN's
Employed in 1972-73:Need to add by 1980:
REGION XIV: DEEP EAST TEXAS
Projected Population
1970 245,8321980 276,8001990 305,700
Selected Regional Statistics
267
664
Total RN's needed by 1980: 864
Ratio RN's/100,000 in 1973: 109
Ratio RN's/100,000 by 1980: 312
LVN Data
Active LVN's in 1972:Ratio LVN's/100,000 in 197k:Number of LVN programs:
7673b7
6
Hbspital and Nursing Home
County Population: 1970
RN Educational Information, 1973
TypeProgram. No. Enroll. Seniors
No. of
BSNADNDip.
1 179 64
TOTAL 1 179 64
*An upper level BSN programwas approved in 1974 for
Stephen F. Austin State Univer-sity
Information
Institution No. BedsStaff NursesRN's 1 LVN's
Ratios to Beds ofRN's ' LVN's
Hospitals 20 1,192 186I
1 499 1 to 6 1 to 2
I
1 to 129i:_l__ to 14Nursing Homes 29 1,9341A
-15 1 136
Population in the 13 counties of Region XIV is generally distributed through-
out the region, with about 35 percent of the total population in Nacogdoches and
Angelina counties. The population is projected to increase from almost 246,000
in 1970 to nearly 306,000 by 1.990. Some 14 percent of the population is 65 years
of age or older and the region has a high aging index.
This region is located in the piney woods section of East Texas and the cli-
mate and other factors cause it to be one of the more desirable retirement areas
of the state. It does not coMtain any of the very large cities characteristic of
the coastal, high plains, and north,4041 areas of the state. There are 20 hos-
pitals in the region with 1,192 beds and 29 nursing homes with 1,934 beds.
107

There are 302 active and 130 inactive RN's in the region and, the FTE-RN's total 267. Ratio to population is 109 per 100,00b, which maks verylow among the 21 regions. Some 31 percent of the active RN': are over 50years of age.
Nursing care in the region is dominated by LVN's, with a ratio of 307per 100,000. There are 186 RN's and 499 LVN's employed in the hospitals whichhave, as shown on the preceding page, 1,192 beds. The nursing homes in th'.!
region employ 15 RN's and 136 LVN's for the 1,934 beds.
Until recently there was only one professional nurse program in theregion, an ADN program at Angelina College in Lufkin, which had 179 studentsenrolled in 1973. A new upper level BSN program has recently been approvedfor Stephen F. Austin State University and will be implemented in 1975. There
are six LVN programs in the region.
Thi's region has had difficulty in retaining RN graduates in the region
and the upper level BSN program is expected to improve the retention rate.In the past there has been a deficiency of clinical resources but new con-struction of hospitals', currently underway, will improve clinical resources
in the region.
Under the traditional supply pattern the region is projected to have
a deficiency of 509 RN's by 1980 under the Nursing Project's optimum ratios.
It is anticipated. that the new BSN program at Stephen F. Austin State Univer-
sity will contribute to an improvement in this projected deficiency.
'So that the necessary improvement of the numbers of RN's needed can
be brought about, the Nursing Project recommends:
1. Emphasis be placed on providing continuing educationfor LVN's' in the region.
2. Increase the enrollment in the ADN program at AngelinaCollege to increase the number of RN graduates.
3. That Angelina ,College explore with Stephen F. Austin
State Univehsity the formation of ()cohsortium to prof'
vide the benefits of the multiple entry and exit cur-'
ei.culum for nursing students in the region.Y.
118108
1I

REGION XV: SOUTH EAST TEXAS
Projected Population
1970 315,943
1980 352,3001990 379,300
Selected Regional Statistics
County Population: 1970
FTE-RN's RN Educational Information, 1973
Employed in 1972-73: 674 Type No. of
Need to add by 1980: 1.003 Program No. Enroll. Seniors
Total RN's needed by 1980: 1,529 BSN -
ADN 46
Ratio RN's/100,000 in 1973: 208 Dip.* 1 45 45
Ratio RN's/100,000 by 1980: 434TOTAL 1 91 45
LYN Data*This program was phased out
Active LVN's in 1972: . 894 in 1973.
Ratio LVN's/100,000 in 1972: 276Number of LVN programs: 3
Hospital and Nursing Home Information
Institution /
11
.
No. BedsStaff
1 :
Ratios to BedsRN's V 's
Hospitals
.
11
. ,
2,035 421 : 612
.
1 to 5 1 to 3
Nursing Homes 13 2,260 20 110 1 to 113 1 to 21
One of the most intensively populated industrial regions in the state and
located in extreme southeast Texas, Region XV has only two counties with almost
78 percent of the 1970 population of nearly 316,000 located in-Jefferson Cogpty
(Beaumont). The population is projected to increase to over 379,000 by 1990.
Statistically, the region has 764 active and 277 inactive. RN's and the FTE-
RN's total 674. Over one-third (34.03 percent) of the active RN's are less than
39 years of age while less than one-third (29.97 percent) are over fifty years of
age. The region has a very low aging index with both counties below the state
average.

The, current FTE-RN ratio of 208 perthe 21 regions. In order for the regionRN's per 100,000 by 1980, as depicted on1,003 RN's will be needed by that date.
100,000 population ranks seventh amongto come up to the FTE-RN ratio of 434the chart shown above, an additional
The region has eleven hospitals which have a total of 2,035 beds and theyemploy 421 RN's and 612 LVN's. There are also 14 nursing homes with a total of2,260 beds and which employ 20 RN's and 110 LVN's. Throughout the region thereare 25,264 persons who are 65 years of age or older. The ratios of nurses tobeds are shown above.
There is only one program for registered nurses in the region, an ADN pro-gram at Lamar University in Beaumont. The program is less than two years oldand has, in effect, replaced a diploma program that has phased out in one ofthe Beaumont hospitals. Current enrollment in the Lamar University ADN programis 105 students. There are also three LVN programs in the region.
In order to bring the number of RN's up to the optimum by 1980, as recom-
mended by the Nursing Project, the existing program at Lamar University will
need to increase enrollment. Elsewhere in the state, the second year classes
of ADN programs had from 26 to 176 students and the program at this institu-
tion will have to become one of the larger ADN programs in Texas.
In order for the region to meet the optimum ratios of the Nursing Project
and to improve the educational level of the active nurses, the Project recom-
mends that:
1. The existing ADN program at Lamar University increase its
enrollment over the next two years in order to graduate
approximately 150 students per year.
The recommendations for providing continuing education courses
for the professional and vocational nurses in the region be
implemented.
120.
11%11

REGION XVI: GULF COAST
Projected Population
1970 2,305,1001980 2,821,9001990 3,473,900
Selected Regional Statistics
FTE-RN's
Employed in 1972-73: 5,899
Need to add by 1980: ', 6,495
Total RN's needed 4)(1980: 11,344
Ratio RN's/100,000 in 1973: 255
A Ratio RN's/100,000 by 1980: 402
LVN Data
Active LVN's in 1972: 5,445
Ratio LVN's/100,000 in 1972: 22Number of LVN programs: 13
County Population: 1970
Loom13,Ce
*061,10.
came)erase KM. st. , agoistan
49APmmft .
allacaa
10144
027'4.
RN Educational Informations 1973
'Yoe No. of
Program No. Enroll. Seniors
BSN 7 1,455 458
ADN 4 "847 379
Dip.
TOTAL 11 2,302 837
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRN's
1
, LVN's
Ratios to Beds ofRN's I UN's
i
Hospitals 83 14,112 4,363 13,718 1 to 3 r
i
1 to 4
Nursing Homes 88 9,064 183
-
582 1 to 50 1 to 16
Region XVI is the second largest region in the state in population with over
2.3 million in 1970 and is projected to increase to 3.4 million by 1990. Most of
the population is concentrated in Harris County (1.7 million in 1970) which had
almost 76 percent of the region's population.
The region has extensive and complex array of medical schools and medical
centers and virtually every health profession is represented in the vast system
of eddcational programs. The city of Houston in particular is a popular location
for medical, dental, and allied health practitioners because of the sophisticated
facilities, variety of types of patients, and employment opportunities.
ill'.;
121

On the perimeter of this complex in Harris and Galveston counties areeleven additional counties which are more rural than urban in type. Statisticswhich apply to regions consisting of both rural and urban counties do not alwaysreflect the true conditions in each county.
Region XVI has 6,607 active and 2,389 inactive RN's. The FTE-RN's total5,899 and the ratio of active RN's to population is.255 per 100,000 which isthe highest in the state.
The region has approximately 83 hospitals of all types and sizes with 52of them in Harris County. These hospitals employ 4,363 RN's and 3,718 LVN's andthe total number of hospital beds is 14,112.
In-addition, there is a total of 88 nursing homes in the region and 51 ofthose are in Harris County. These facilities have a total,of 9,064 beds andemploy 183 RN's and 582 LVN's. Population statistics indicate that the regionhas over 150,000 persons who are 65 years of age or older. Ratios of both pro-fessional and vocational nurses to beds in hospitals and nursing homes areshown above.
Educational programs for nurses are available within the regilbn but concen-trated in Harris County. There is a total of twelve registered nurse programs,seven of them baccalaureate and five at the ADN level. Three of the BSN pro-
grams are in the private sector: Dominican College, Houston Baptist University,
and the University of St. Thomas. The four publicly supported BSN programs offeronly the third and fourth (clinical) years of the four year program. Prairie
View A&M University, located in Waller County, provides the third and fourth
years of its program in Harris County. Texas Woman's University, which also has
a clinical division in Dallas (Regibn IV), has a clinical division in Houston
in the Texas Medical Center. The University of Texas System School of Nursing
operates clinical divisions in Galveston and Houston.
At the ADN level, programs are offered at Alvin Junior College, College of
the Mainland, Galveston College (with a coordinate branch at Brazosport Community
College), and at San Jacinto College. Enrollments, including the number of
seniors in 1973, are shown on the preceding page.
In addition to these registered nurse programs there are some 13 LVN pro-
grams in the region.
Educational and clinical resources for nurses are adequate for producing
the increased needs in the region provided the Nursing Project's recommendations
on rural clinical experience are implemented and sustained efforts are put forth
by the nursing educators to help meet the needs of the region outside the major
metropolitan area. The nurse population is growing at a more rapid rate than
the general population and unless the distribution of RN's throughout the region
improves, the Houston area will have an oversupply. The Nursing Project there-
fore recommends:
1. The general recommendations in geriatric and rural clinical
experience be adopted by existing nursing programs as top
priorities.
122112
ail

REGION XVII: GOLDEN CRESCENT
Projected Population
1970 142,3791980 139,9001990 138;200
Selected Regional Statistics
County Population: 1970
FTC -RN's
186
RN Educational Information, 1973
Employed in 1972-73:. TypeProg `am No.
No. ofEnroll. SeniorsNeed to add by 1980: r%388
Total RN's needed by 1980: 525 BSNADN 1
,Dip.
TOTAL 1
of,
Ratio RN's/100,000 in 1973: 146
Ratio RN's/100,000 by 1980: 417
LVN Data
549Active LVN's in 1972:Ratio LVN's/100,000 in 1972:Number of LVN programs:
4316
HoApital anci) Nursing Home Information
Institution No.,
Staff NursesRN's ' LVN's
1 .
Ratios to Beds ofRN's I LVN's
I ,
Hospitals 13 8281 1
129I
338 1 to 7 1 to 2I
Nursing itille----0-1122-1-12224-,-1The seven counties in Region XVII are located in the middle of the Texas
coast and are predominantly rural in economy and in population. VictoriaCounty, with nearly 54,000 population in 1970 is the most populous ,countyin the region and, with Calhoun County, is projected to increase in populationto 1990. In 1970, these two counties had just over 50 percent of the popula-tion of the region.
There are 209 active and 78 inactive RN's in the region. Over one-thirdof the active RN's are 50 years of age or older while almost 57 percent areless than 50 years of age.
A31
123

1
As shown in the data charts on the preceding page, the Fri E-RN ratio.is146 per 100%000 population, which ranks eighteenth among the 21 regions. Underthe optimum levels recommended by the Nursing Project, the tailet ratio for1980 is 417 FTE-RN's per 100,000 population.
1
As shown above, there is a defy of RN's in hospitals and nursing homes.The region has a high aging index id there are 16,836 residents who are 65 yearsof age or older.
The region has not had a prograin for the education of registered nurses:In September of 1974, final approval was granted Victoria College to initiatean ADN program and the first students will be enrolled in,1975. The programwill not graduate its'first class until 1977. Surveys of the Nursing Projectshow that most of the nursing students from.this region who go to other regionsfor their education do not intend to return here to practice.
The region has six LVN programs in five of the counties in the region andthe lack of an RN program is shown in the high number of these graduates workingin 'hospitals and nursing homes.
Under the optimum levels of professional nurses recommended by the NursingProject, the region will need to acquire 388 additional RN 4s beyond* those pro-vided through the existing supply pattern. It is anticipated that the new ADNprogram at Victoria will make a substantial contribution tq_this number.
With the new program already approved, the Nursing Project submits the fol-lowing recommendations to improve the quality of nursing Scare and provide ecuca-tional improvement cor nurses within the region:
1.. The new fON program at Victoria College emphasize re-cruitment of qualified LVN's and persons with prior,nursing education or experience into the ADN program,especially during the first few 'yeari of tts operation.
2. Emphasis be placed upon continuing education for theLVN's in the region.

1
'REGION XVIII: ALAMO
County Population: 1970
10.513
011. 10611 {
0,471 i
Projected Population
tort2.107
weertoo*
ustacm
11,063
1I MOP
,i 11,41
'
NIP ' i1 1.013 '_, ,747'
Veda I =dm17.34a 1 20./49
ZAMA
I 11,370 vivb
airLon I UMW
19701980
1990
1,087,2331,195,5001,290,900
Selected Regional Statistics
FTE-RN's
employed in 1972-73: 2,402
Need to add by 1980: 2,420
Total RN's needed by 1980' 4,273
Ratio RN's/100,000 in 1973: 208
Ratio RN's/100,000 by 1980: 348
LVN Data
Active LVN's in 1972: 2,597
Ratio LVN's/106,000 in MT: 225
Number of LVN programs: 11 "IIN11.14..
RN Educational
TypeProgram No.
COM
1.914, ' *gft
,-, QOM JRmom '1 SSA'',
',.. 13,041
MMOI 14,4114
Information, 1973
No. ofEnd. Seniors
BSN 2 517
ADN 1 :143
Dip. 1 114,
TOTAL 4 874
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRNS i LI/Ws
Ratios to Beds ofmil
s I LVN's""
Hospitals 36 8,412 1,665: 1,827 1 to 5 : 1 to 4
Nursing Homes 62 5,495I
390176i.-
I
1 to 31 1 to 14. 1
1697849
296
As in most of the large geographic regions of the state, the Alamo region
has one dominant - county with over 76 percent of the region's population. The 20
counties in Region XVIII include Bexar County (San Antonio) whose population in
1970 was over 830,000 and is projected to grow to almost one million and the re-
gion's population will increase to 1.3 million by 1990. Seven of the 20 couqies
are :to experience a decline in population by 1990. This is the largest geographic
region and is located in the southwestern part of the state, with its western. edge
:along the Rio. Grande.
.0"
115
A

There are 2,660 active and 1,188 inactive RN's in the region and most ofthem are in Bexar County. FTE-RN's total 2,402 and over 64 percent (1,665) ofthem are employed in hospitals. The FTE-RN's in the region total out to 208per 100,000, which ranks seventh among the 21 regions. The ratio for optimum
levels of RN's for 1980 Ps 348, as shown above. With the existing supply pat-tern remaining stable, the region will need only 221 additional RN's beyond
thoc expected to he :n the region by 1980.
As displayed above, the Alamo region has 36 hospitals, 18 of them irrBexarCounty. They have 8,412 beds and employ 1,665 RN's and 1,827 LVN's. There are
62 nursing homes in the region and 33 of them are in Bexar County. They employ
176 RN's and 390 LVN's for the 5,495 nursing home beds. The high aging index is
reflected in the large number of nursing homes and there are 93,311 persons in
the region who are 65 years of age or older.
San Antonio has extensive and complex medical and health education resources.There are two BSN programs for professional nurses, one at The Uyversity of Texas
School of Nursing and the'other is at Incarnate Word College. A third profession-
al route is aidiploma program at Baptist Memorial Hospital. In addition to these
F;royramc, the0e is an ADN program offered at San Antonio College. Combined en-
rollments of these four programs in 1973 was 874 and 296 were seniors.
'There are eleven LVN programs in the region in various locations. One of
these, located at St. Philip's College fn San Antonio, reported 1973 enrollment
of 286 students.
There appears to be rio prOblem of supply of RN's in the metropolitan area
of this region and the general recommendations on clinical experience in rural
setting;; and cIntilluing education fur LVN's should lead to meeting the needs of
the reoion. Upon adoption of the optimum ratios, the registered nursing programs
would need to increase enrollments 5o as to produce the additional 221 RN's needed
by 1980.
126
116

REGION XIX: SOUTH TEXAS
Projected
9
Population
1970 103,0651980 134,100
1990 157,400
Selected_Rtgional Statistics
FTE-RN's
Employed in 1972-73:Need VI add by i980:
Total RN's needed by 1980:
Ratio RN's/100,000 in 1973:Ratio RN's/100,000 by 1980:
LVN Data
County Population: 1970
RN Educational Information, 1973
106 ; Type No. of
195 Program No. Enroll. Seniors
286 BSN -
ADN 1 58 26
101 Dip.
213TOTAL 1 58 26
Active LVN's in 1972: 178Ratio LVN's/100,000 in Tg727-1-6§--Number of LVN proyrams:
Hospital and Nursing Home Information
,
Institution No. BedsStaff NursesRN's ' LYN's. .,-
Ratios to Beds ofRN's
i
I LVN's
Hospitals 2 258 48I
118
1
1 to 5I
1 to 2
Nursing Homes 3 266 3 22 1 to 88 1 to 12
The South Texas Region is'made up of four counties along the Rio Grande in,
Southwest Texas.- Almost 71 percent of the 1970 population of over 103,000 was
in Webb County. Most of the region's projected growth to 1990 is expected to
occur in Webb County. Laredo, in Webb County, the principal city in the area,
is an international port of entry from Mexico and there is a strong Mexican-
American cultural influence throughout the region as over 50 percent of the
population is Mexican-American.
117
127

Ther/are 112 active and 28 inactive RN's in the region with FTE-Wstotaling 106. There are only two hospitals in the region and they have a
total of 258 beds. They employ 48 RN's and 118 LVN's. The FTE-RN ratio
of 101 to 100,000 population is the lowest of the 21 regions and is attribu-
tablo. in part, to lack of employment opportunities.
There are three nursing homes in the region, all in Laredo, with a total
of 266 beds. These homes employ three RN's and 22 LVN's. The region has a
low aging index and there are only 8,181 persons 65 years of age or older.
Region XIX has one program for registered nurses and one LVN program,
both at Laredo Junior College. Enrollment in the RN program in 1973 was 58
students. Courses at the BSN level have been brought into the Laredo area
during the past year by The University of Texas Nursing School at San Antonio
- but the number of students seeking nursing courses beyond the ADN level has
been minimal.
In a region having minimal health care facilities, the lowest ratio of
RN's to population of any region, and limited employment opportunities for
nurses, the unusal condition of meeting the optimum ratios of the Nursing
Project can be met and exceeded under the existing supply pattern. This is
illustrated in that the supply pattern now in operation (including the ADN
program at Laredo Junior College) will, by 1980, produte-63 more nurses than
are needed to meet the optimum requirements. The need for faculty improvement
courses can be provided through continuing education which is a general recom-
mendation for most regions presented elsewhere in this report, Work toward
the baccalaureate degree, currently being provided by The University of Texas
on a temporary basis, can be provided through Texas A &I University at Laredo
which has an upper level BSN program on its Corpus Christi campus.

REGION XX: COASTAL BEND
Projected Population
1970 433,8221980 478,2001990 520,200
Selected Regional Statistics
County Population: 1970
PC WIMP WOO
'PIPS i Sirr P-2137 ' NM{
31.0311 471111
PM I
PAM WILLI PIAUI '7r,
11,121237.544
FTE -RN's RN Educational Information, 1973
Employed in 1972-73: 667 Type No. of
Need to add by 1980: 1,040 Program No. Enroll. Seniors
Total RN's needed by 1980: 1,537 BSNADN 1 140 60
Ratio RN's/100,000 in 1973: 152 Dip. -
Ratio RN's/100,000 by 1980: 330TOTAL 1 140 60
LYN Data
Active LVN's in 1972: 1,364Ratio LVN's/100,000 in 1972: 311
Number of LVN programs: 2
*An upper level BSN programwas approved in 1974 for Texas
A&I University at Corpus Christi
Hospital and Niirsing Home Information
Institution No. BedsStaff NursesRN's ' LVN's
1
Ratios to Beds ofRN's ' LN's
1
Hospitals 21 2,919I
448 j 963I
1 to 7 1 to 31
Nursing Homes 27 2,351 26 134 1 to 90 I 1 to 18
Located on the lower Texas coast, the 13 counties of Region XX had a 1970
population of almost 434,000 with about 55 percent of it in Nueces County, which
also is the location of Corpus Christi, largest city in the region. Seven of the
counties are projected to decline in population by 1990, but the remaining six are
projected to increase with the greatest amount of growth in Nueces County.
The region has a blend of large areas that are sparsely populated and the
urban concentration of population and health care facilities found throughout.
most regions of the state. Of: i
129

There are many excellent health care facilities in Corpus Christi. Thereare 21 hospitals in the region and four of those which are in Corpus Christi have500 or.more beds. As shown above, the hospitals employ 448 RN's and 963 LVN'swhile the 27 nursing homes employ only 26 RN's and 134 LVN's. Nine of the 27nursing homes are in Corpus Christi.
The aging index for the region is low, with seven counties below the stateaverage. In 1970, there were 31,345 persons resident in the region who were 65years of age or older.
There are 737 active and 268 inactive RN's in the region and the FTE-RNcount is 557. Nearly 63 percent of the nurs.s in the region are less than 50years of age.
The current FTE-RN ratio to population is 152 per 100,000, which is seven-teenth among the 21 regions. In order to meet the optimum ratios of the NursingProject, the region will need, by 1980, some 336 more RN's than the region isexpected to have under the existing supply system.
There is one registered nurse program in the region, an ADN program atDel Mar College. This program had 140 students enrolled in 1973. A new upperlevel BSN program was recently approved for Texas A&I University at Corpus Christi.
4 in the other two regions where this type program has been established, itis expected to cause more ADN graduates to remain in the region to seek the BSN andpractice locally, thereby increasing the total RN count, and also to improve thequality of health care. There are two LVN programs in the region, one of them atDel Mar College whose enrollment in 1973 was 120 students.
The Nursing Project recommends:
1. That the general recommendations on continuing educationand rural clinical experience for nursing students begiven high priority in Region XX.
2. That the upper level BSN program at Texas AM Universityat Corpus Christi provide upper level courses to RN's inthe Region XIX as the need for such courses is demonstrated.These courses should be under the administrative jurisdictionand control of the BSN program in Corpus Christi and facili-ties may be used, under appropriate arrangement, with TexasA&I University at Laredo or Laredo Junior College.
130
If2

REGION XXI: LOWER RIO GRANDE VALLEY
Projected Population
1970 337,4731980 297,3001990 282,500
Selected Re Statistics
FTE-RN's
Employed in 1972-73: 366
Need to add by 1980: 503
Total RN's needed by 1980: 761
Ratio RN's/100,000 in 1973: 105
Ratio RN's/100,000 by 1980: 256
LVN Data
Active LVN's in 1972:Ratio LVN's/100,000 in 19727--
Number of LVN programs:
620178
5
County Population: 1970
RN Educational Information, 1973
Type
EmmaNo. of
No. Fnroll. Seniors
BSNADN 2 127 49
Dip.
TOTAL 2 127 49
Hospital and Nursing Home Information
Institution No. BedsStaff NursesRN's LVN's
Ratios to Beds ofRN's I LVN's
1
Hospitals 12 1,133 178 361 1 to 6 i 1 to 3
Nursing Homes 16 1,455 34 124 1 to 431 1 to la
Region XXI is a three county area in extreme south Texas whose population is
over 50 percent Mexican-American and whose economy is based largely on agricultur-
al products. Brownsvi.le, in Cameron County, is an international port of entry.In 1970, Hidalgo County had almost 54 percent of the population of the region and
Cameron County had almost 42 percent. The region's population in 1970 was 337,473
and is projected to decline sharply to 1980, and have a slower decline to 1990.
The aging index is far below thefltate average; there are large families in
the region which contributes to thesibultiful characteristic of the population.
131

As shown above, there are 12 hospitals in the Lower Rio Grande Valley regionwhich employ 178 RN's and 361 LVN's. The 12 hospitals have 1,133 beds. Thereare 16 nursing homes with 1,455 beds and they employ 24 RN's and 124 LVN's. Publichealth is emphasized in this region and 45 RN's and 25 LVN's are employed in thisactivity.
Throughout the three counties there are 405 active and 156 inactive RN's andthe FTE-RN count is 366.. Some 55 percent (223)-of the RN's are less than 50 yearsof age while almost 40 percent (160) are over 50.
For several years the only professional nurse program in the lower valleywas an ADN program at Pan American University at Edinburg. Enrollment in thatprogram in 1973 was 127 students. A second ADN program, approved in Septem-ber of 1974 for Texas Southmost College in Brownsville, is expected to accept stu-dents within the next year. This new program should make a substantial contribu-tion to professional nurse needs in this region.
The current FTE-RN ratio to population is 105 per 100,000, which rankstwentieth among the 21 regions. In order to meet the optimum number of RN'sadopted by the Nursing Project, the region, by 1980, will be required to havean additional 509 RN's in addition to those being produced in the existing pro-gram. The optimum level for FTE-RN's by 1980 is 256 per 100,000 population.With two professional nurse programs in the region, this level can be reachedwith existing resources and supply patterns.
The Nursing Project recommends that:
1. The continuing education recommendations of the NursingProject be given priority in the lower valley, especiallyfor LVN's.
2. That the ADN programs at Pan American University and TexasSouthmost College monitor their enrollments to avoid apotential oversupply until additional employment oppor-tunities are available.
t
132.
122 Lgi

CHAPTER VI
A COOPERATIVE APPROACH FOR MEETINGNURSING NEEDS IN TEXAS
rht! establishment of new professional nursing programs in the pubiklysupported sector of higher education comes under the statutory responsibilityof the Board of Nurse Examiners for the State of Texas and also either theCoordinating Board or the Texas Education Agency. Programs in the public com-munity colleges are funded through the Texas Education Agency and those instate senior institutions must have approval of the Coordinating Board. Pro-grams in the private colleges and universities are not within the purview ofeither the Coordinating Board or the Texas Education. Agency but the Board ofNurse Examiners does have jurisdiEtion.
Licensed Vocational Nurse programsthe Board of Vocational Nurse Examinerscollege, the Texas Education Agency hasdisapproval authority.
While there is informal cooperation among these several licensing and fund-ing agencies, there is no formal mechanism for coordination of nursing education'programs, either professional or vocational, that involves all of the agencies.The level of cooperative effort varies from time to time and there is very littleinter-agency exchange of information related to the quality of nursing programs.Exchange of such information is of importance to all agencies which either li-cense the graduates, monitor the quality elements of the programs, or have ap-proval and disapproval responsibility under Texas statutes.
A significant first step toward effective planning and coordinating nursingeducation in this state will require that the agencies having statutory respon-sibility over nursing programs have mutual access to information related to nur-sing needs, quality status of existinI programs, and other vital information.In addition, decisions regarding nursing programs should be made on the basisof mutually acceptable criteria and should reflect progress toward specificgoals.
This cooperation can take place without violation of the function or statu-tory responsibility of any agency because each of them must, in the carrying outof its pr ssional and legal responsibility, be finally subject to its own sta-tute.
are under the legal jurisdiction ofand, in a publicly supported communityfunding, and therefore approval or
So that the state can move toward a more carefully coordinated system ofnursing education in this state, the Nursing Project Council submits the follow-ing:
RECOMMENDATION: A COMMITTEE BE ESTABLISHED, COMPOSED OF STAFF REPRESENTATIVESFROM THE BOARD OF NURSE EXAMINERS, THE BOARD OF VOCATIONALNURSE EXAMINERS, THE COORDINATING BOARD, TEXAS COLLEGE ANDUNIVERSITY SYSTEM, AND THE TEXAS EDUCATION AGENCY. THISCOMMITTEE WOULD REPRESENT THE AGENCY HEADS IN COORDINATING

THE IMPLEMENTATION OF THE RECOMMENDATIONS OF THENURSING PROJECT. THE COMMITTEE SHOULD EMPHASIZE THEIMPROVEMENT OF EDUCATIONAL QUALIFICATIONS AND CLINICALCOMPETENCIES OF FACULTY IN PROFESSIONAL NURSING PROGRAMS.
Having taken the position that the most urgent need in nursing at this
time is to improve the educational qualifications of nursing faculties, the
Nursing Project submits the following:
RECOMMENDATION: A. IMMEDIATE PRIORITY SHOULD BE GIVEN TO GRADUATE EDUCA-TION FOR FACULTY MEMBERS IN PROFESSIONAL NURSING PROGRAMS.
EXPANSION OF EXISTING PROGRAMS AND APPROVAL OF NEWPROGRAMS SHOULD BE CONTINGENT UPON THE AVAILABILITYOF QUALIFIED FACULTY AND ADEQUATE CLINICAL FACILITIES.
The Council, awarelbf the increasing number of new graduates and licensees
each year, believes the present number of professional nursing programs in most
regions is adequate to produce the number of registered nurses needed in the
state; however, increases in enrollments will need to occur in some programs to
meet the optimum ratios recommended by the Nursing Project. The recommendations
for increased enrollments and graduates and for more rural clinical experience
for students will lead toward meeting part of the need; the maldistribution of
professional nurses will not be solved until job opportunities become attractive
enough in all areas of the state to cause RN's to want to practice in the non-
urban areas.
Coordination of Continuing Education
The nursing profession recognizes the need for its practitioners to engage
in a life-long learning process in order to maintain competence in a world of
constantly expanding knowledge. With recent legislation in several states re-
quiring evidence of continuing education for re-licensure, the urgency of making
continuing education readily available to all nurses has been recognized.
A nationwide study of continuing education in nursing, published by the
American Nurses Association in 1972, pointed out that numerous statewide studies
had identified several problems that must be solved if continuing education needs
in nursing are going to be met. Among the problems listed were the following:
a. The need for educational institutions and health agencies and
organizations to assume a greater responsibility for providing
continuing education.
b. The need to find ways to make continuing education available in
rural areas or isolated professional locations.
c. The need to minimize unnecessary duplication.
d. The need for interdisciplinary programs.
e. The need for continuing education opportunities which can assist
in upward career mobility.

The primary interest in continuing education by the Nursing Project was
to recommend a mechanism which would provide the funds and the structure to ac-
complish the needed coordination of efforts within the state. The University
of Texas Systemwide School of Nursing and Texas Woman's University College of
Nursing were charged with the responsibility of statewide coordination of con-
tinuing education by the Coordinating Board in 1967. Although these two schools
have made steady progress in this area, their available resources are inadequate
for meeting the total needs of the state in the area of coordination under the
Present funding procedures.
In order to broaden the base of responsibility and provide additional re-
sources in this area, it is recommended that:
RECOMMENDATION: THE COORDINATING BOARD DELEGATE JOINT RESPONSIBILITY FOR THE
STATEWIDE COORDINATION OF CONTINUING EDUCATION FOR NURSING TO
ALL STATE UNIVERSITIES OPERATING BACCALAUREATE NURSING PRO-
GRAMS.
RECOMMENDATION: THE COORDINATING FUNCTIONS OF THE DESIGNATED UNIVERSITIES
SHOULD INCLUDE THE FOLLOWING:
A. PROVISION OF A MECHANISM FOR PRIVATE COLLEGES ANDUNIVERSITIES AND COMMUNITY COLLEGES OPERATING NUR-SING PROGRAMS TO HAVE A VOICE IN STATEWU. PLANNINGDECISIONS FOR CONTINUING EDUCATION IN NURSING.
B. IDENTIFICATION OF SPECIFIC CONTINUING EDUCATIONNEEDS ON A LOCAL AND REGIONAL BASIS.
C. INVOLVEMENT OF APPROPRIATE INDIVIDUALS, AGENCIES,
INSTITUTIONS, AND ORGANIZATIONS IN PLANNING TO
MEET NEEDS WITH PARTICULAR EMPHASIS ON INVOLVEMENT
AT THE LOCAL LEVEL.
D. LONG-RANGE PLANNING OF STATEWIDE CONTINUING EDUCA-
TION OFFERINGS TO INSURE REDUCTION OF FRAGMENTATION
AND DUPLICATION IN AVAILABLE PROGRAMS.
E. PROVIDE A CLEARINGHOUSE FOR CONTINUING EDUCATION
PROGRAMS AVAILABLE TO NURSES.
PROVIDE AN INFORMATION DISSEMINATION CENTER FOR 1)
PRINTING OF INFORMATION ABOUT PROGRAM OFFERINGS,AND 2) RESPONDING TO INQUIRIES CONCERNING AVAILABLE
HARDWARE AND SOFTWARE IN THE STATE.
G. PROVIDE EVALUATION OF THE COURSES OFFERED.IN CON-
TINUING EDUCATION IN ORDER TO IMPROVE THE QUALITY
OF CONTINUING EDUCATION AND TO ASSURE THAT THE
NEEDS OF PRACTICING NURSES ARE BEING MET.

RECOMMENDATION: FUNDS BE APPROPRIATED TO THE COORDINATING BOARD FOR THE
COORDINATION OF CONTINUING EDUCATION IN NURSING; SUCH FUNDSTO BE DISTRIBUTED TO THE DISIGNATED UNIVERSITIES RESPONSIBLE
FOR COORDINATION ACCORDING TO THE FOLLOWING CRITERIA:
A. THE COORDINATING BOARD AND IDENTIFIED UNIVERSITIESJOINTLY DEVELOP A PLAN TO ACCOMPLISH THE FUNCTIONSLISTED IN ITEMS A-G ON PAGE 123, AND DETERMINE THESPECIFIC AREAS OF RESPONSIBILITY TO BE ASSUMED BYEACH INSTITUTION, AND SUBMIT THE PLAN, WITH SPECIF-IC COSTS FOR EACH UNIVERSITY, TO THE COORDINATINGBOARD.
B. CONTINUED FUNDING BE DEPENDENT ON EVIDENCE OFACHIEVEMENT IN THE SPECIFIED AREAS OF COORDINATION.
Coordination of Off-Campus Courses
Because nursing practice usually requires that the nurse remain in one lo-
cation and, as in hospitals, be subject to shift rotation, the ability for most
active nurses to travel to distant locations to participate in educational pro-
grams is limited. The continuing education programs offered both on,and off-
campus by educational institutions, and the in-service training programs made
available by employers have provided much needed improvement in the ability of
nurses, but there are needs which are not being uniformly met across the state
in nursing educatiOn.
The Nursing Project has identified substantial interest on the part of LVN's
and RN's in furthering their nursing ,skills and in the quality of educational
pceparation. We also observed that several nursing programs were offering
courses in off-campus locations. where local nurses had shown an interest in
taking such courses.
So that nurses throughout the state can be provided the opportuity to
improve the quality of their nursing abilities and to take courses in nursing
that would apply to a higher degree, the Nursing Project concluded that the
state should be divided into regions so that nursing programs could provide
the necessary courses on a carefully planned, non-duplicatory basis which
would permit maximum utilization of nursing education resources in the off-
campus settings.
RECOMMENDATION: THE COORDINATING BOARD ESTABLISH REGIONAL SENIOR COLLEGE AND
UNIVERSITY COUNCILS,FOR THE PURPOSE OF INSURING COORDINATION
OF OFF-CAMPUS NURSING COURSES OFFERED THROUGHOUT THE. STATE.
THE RESPONSIBILITIES OF SUCHSCOUNCILS TO BE:
7A. TO MAKE RECOMMENDATIONS TO THE COOPDINATING
BOARD ON REQUESTS BY COLLEGES OR UNIVERSITIES
WITHIN THE REGION TO OFFER OFF-CAMPUS COURSES.
B. TO MAKE RECOMMENDATIONS TO THE COORDINATINGBOARD ON REQUESTS BY COLLEGES OR UNIVERSITIES
IN OTHER REGIONS riWISH TO OFFER COURSES IN
THE REGION.. C:
126

C. PREPARE AND IMPLEMENT CRITERIA FOR EXCELLENCEIN CONDUCT OF OFF-CAMPUS COURSES.
D. TO INSURE, THAT OFF-CAMPUS COURSES MEET A NEEDWHICH CANNOT BE MET BY A COLLEGE OR UNIVERSITYIN THE AREA WHERE THE COURSES ARE, TO BE TAUGHT.
E. TO FACILITATE INTER-INSTITUTIONAL COOPERATIONIN THE CONDUCT OF OFF- CAMPUS COURSES AND TOASSURE THAT EACH COLLEGE OR UNIVERSITY IN THEREGION HAS A RECORD IN ADVANCE OF THE COURSESAND LOCATIONS PLANNED IN THE REGION.
0
4
it

Ir
DEFINLTION OF TERMS4

DEFINITION OF TERMS
Associate Degree Program in Nursing
A program leading to an associate degree in nursing conducted by an educa-tional unit in nursing within the structure of a junior or communitycollege or senior college or university.
The purpose of an associate degree program in nursing is to prepare practi-tioners of nursing for licensure and employment in positions which requiregiving direct nursing care to patients in a hospital, or similar communityagency.
Baccalaureate Program in Nursing
A program leading to a baccalaureate degree in nursing conducted by aneducational unit in nursing (department. division, school or college) whichis a part of a senior college or university.
The purpose of a baccalaureate program i.n nursing is to Orepare professionalnurse practitioners. The graduates have the potential for assuming leader-ship roles as well as a foundation for entrance into a graduate program innursing.
Behavioral Objectives'
Statements which describe what the learner will be able to do once learninghas occurred.
Collaborate
Cooperate as a peer.
Conceptual Framework
A statement of combined faculty thinking about society, the learner,thenature of nursing practice, program objectives, and curriculum evaluation.A framework containing the philosophical and theoretical background funda-mental to the design of the education program, created by/faculty, toenable them to make consistent decisions about the curriculum.
Clinical Laboratory ExpLrience
Planned learning experience which involves direct contact with patients/clients under the guidance of 'faculty.
Clinical Nurse Specialists
Nurses who are primarily clinicians with a high degree .of knowledgeiskill and
competence in a specialized area of nursing. These are' made directly available
'to the public through the provision of nursing care to clients and indirectly
available through guidance and planning of tare with other nursing personnel.
. Clinical nurse Oecialistt hold a maste'tfdegree.in nursing preferably with an
emphasis in clinical nu sing.
ti
39

Clinical Nursing Practice
Performance of nursing duties by an RN or LVN in a job setting which
involves direct contact with patients/clients.
Challenge Examination
A test taken by a student for the purpose of obtaining credit in a course
before completing the course or without enrolling in the course.
Continuing Education in Nursing
Planned learning experiences beyond a basic nursing educational program.
These experiences are designed to promote the development of knowledge,
skills, and attitudes for the enhancement of nursing practice, thus im-
proving health care to the public.
Credit, Transfer
Semester credit hours earned in one institution which transfer and apply
toward degree requirements in another institution.
Curriculum
A program of courses fulfilling the requirements for a certificate, diploma,
or degree in a particular field of study.
Multiple Entry-Exit Curriculum
A program of courses fulfilling the requirements for the nurse assistant,
vocational nurse, associate degree nurses and baccalaureate degree nurse
arranged in a logical sequence to allow for vertical mobility of students.
Diploma Program
A program leading to a diploma in nursing ccnducted by a single purpose
school under the control of a hospital. The hospital which conducts an
educational program in nursing" shall be general in type and accredited by
the-Joint Commission on Accreditation. of Hospitals.
The purpose of a diploma program in nursing is to prepare a nurse practi-
tioner who is qualified to assume a beginning position in a hospital or
similar community agency. Given opportunity and time, the graduate will
be capable of directing nursing care for both individual patients and
groups of patients.
Distributive Nursing
Nursing practice directed primarily toward health maintenance and disease
prevention. Provision of distributive nursing care occurs most frequently
in non-acute settings.
Episodic Nursing
Nursing practice whichrestorative aspect. ofis usually provided in
is essentially directed towarv. the curative and
acute or chronic health problems Such practice
a hospital or in-pflipet facilitY.
132(ugt

Levels of Practice
Variations in the scope of nursing knowledge and skills which the nurseis capable of applying to the delivery of patient care as a result of hereducational preparation.
Professional Level of Practice
Implies the ability of the practitioner to utilize theories and prin-ciples from many sources to develop effective approaches to the -
management and delivery of nursing care. The professional practitioneris capable of exercising independent judgment in nursing care decisionsrelated to health care problems ranging from simple to complex. Pro-fessional practice necessitates a broad general education base for whicha baccalaureate degree in nursing is considered a minimum requirement.
Technical Level of Practice
Implies the ability of the practitioner to function within the frameworkof existing patterns of practice in the delivery of nursing care topatients with common, recurring health problems. Technical practicerequires the exercise of skill and judgment in nursing care but at alevel which should be under the supervision of a professional individual.The educational preparation for technical practice is a two-year programleading to the associate degree in nursing.
Nurse Clinicians
Have well-developed competencies in utilizing a broad range of cues. These
cues are used for prescribing and implementing both direct and indirect nursing
care and for articulating nursing therapies with other planned therapies. Nurse
clinicians demonstrate expertise in nursing practice and insure ongoing devel-
opment of expertise through clinical experience and continuing education.
Generally minimal preparation for this role is the baccalaureate degree.
Nurse Practitioners
Have advanced skills in the assessment of the physical and psycho-social,
health-illness status of individuals, families or groups in a variety of set-
tings through health and development history taking and physical examination.
They are prepared for these special skills by formal continuing edr7ation
which adheres t3 ANA approved guidelines, or in a baccalaureate nursing pro-
grams.
Nursing Process
A systematic approach to the delivery of patient care which requires the nurse
to assess needs, develop a plan of action based on assessment, implement the
plan, and evaluate the results of nursing actions.
Primary Health Care
Giving health care to individuals or groups at an initial point in their ill-
ness in order to prevent serious illness or to maintain the individual's health
status. The focus is primarily on prevention of illness, maintenance of well-
133
141

ness, and dealing with common, recurrent problems.
Primate Nursing
Provision of nursing services based on the concept of total responsibilityand accountability of nursing care for the patient vested in one nurse.Primary nursing means that each patient has one nurse who is re?ponsiblefor planning and evaluating his nursing care even though she does not ac-
tually give all care.
Professional Nursing Program
A two, three, or four year curriculum which prepares the student to becomelicensed as a registered nurse.
Service Area
The geographic area in which most of the graduates of a nursing programseek employment.
SMSA
Refers to Standard Metropolitan Statistical Area and consists of one or
more central cities with 50,000 or more population surrounded by contig-
uous areas economically allied to them. There were 24 SMSA's in Texas in
1971.
Upper Division NursinglIga
A four-year program leading to a baccalaureate degree in which general
education courses are taken during the freshman and sophmore years and nur-
sing courses are begun in the junior year.
Upper Level Institutions
A college or university which offers courses at the junior and senior levels
only.

SELECTED BIBLIOGRAPHY

SELECTED BIBLIOGRAPHY
1. Altman, Stuart H., Present and Future Supply of Registered Nurses, Dept.of H.E.W., Division of Nursing, Bethesda, MaryTand, 1971.
2. American Nurses Association, The Nation's Nurses: 1972 Inventory ofRegistered Nurses, prepar4d by Aleda V. Roth and Alice R. Walden,Kansas City, Missouri, 197', p. 18.
3. American Nurses Association, RN's 1966 - - An Inventory of RegisteredNurses, New York, 1969.
4. American Nurses Association, Standards for Continuing Education in Nursing,1974.
5. American Nurses Association, Facts About Nursing, 1972-73, Kansas City,Missouri, 1973.
6. Architecture Research Center, Rural Health Delivery System: Texas 7-CMedicare Hospitals, Texas AM University, 1972.
7. Ashkenas, Thai L., Aids and Deterrents to the Performance of AssociateDegree Graduates, National League for Nursing, New York, 1973.
8. Board of-Nurse Examiners, Requirements and Standards for Professional NurseEducation, 1974.
9. Board of Nurse Examiners for the State of Texas, R.N. Relicensure Cards,1971-72, 1972-73.
.10. Brown, Esther Lucile, Nursing Reconsidered: A Study of Change, Part I,J.B. Lippencott Co,, Philadelphia, 1970. Part II, 1971.
11. Commission on Coordination of Higher Educational Finance, A Plan forMeeting Personnel Needs in the Health, Health Related andrAdaptiveBehavioral Problem Service Areas in Arkansas, 1076.
12. Dineen, Mary A., "The Open Curriculum: Implications for Further Education",Nursing Outlook, Vol. 20, No. 12, December, 1972, pp. 770-774.
13. "Educational Preparation for Nursing - - 1972", Nursing Outlook,-Vol. 21,No. 9, September, 1973, p. 586-593.
14. Extending the Scope of Nursing Practice: A Report of the Secretary'sCommittee to Study Extended Roles for Nurses, Department of Health,Education and Welfare, 1971. .
15. Fagin, Claire and Goodwin, Beatrice, "Baccalaureate. Preparation forPrimary Care", Nursing Outlook, Vol. 20, No. 4, April), 1972, pp. 240-244.
8.131 137144

16. Flitter, Hessel H., Nursing in the South, Southern Regional EducationBoard, Atlanta, Georgia, 1968.
17. Governor's Committee on Nursing, Nursing in Virginia, 1969.
18. Governor's Office of Information Services, GR-3, SelecteJ Demographic
Characteristics from Census Data - Fourth Count, 1970.
19. Haas, Patricia T. and Smith, Mary Howard, Nursing Education in the
South, 1973: Pathways to Practice, Vol. 1, Southern Regional Edu-
cation Board, Atlanta, Georgia, 1973.
20. HospitalNurse
Review and Planning Council of Southern N.Y., IncEducation Needs in the Southern N.Y. Region.
21. Illinoisand A
Study Commission on Nursing, Nursing_in Illinois:Plan, 1968-1980, Vol. II, 1968. Vol. "I, 1970.
" Study of
An Assessment
22. Jackson, Virginia S., et al, New Mexico Nursing Education Needs Study,
The University of Albuquerque, Albuquerque, New Mexico, 1972.
23. Jarratt, Virginia, Report on Nursing Resources in Texas: 1966, (Sponsored
by the Board of Nurse Examiners for the State of Texas, the Texas Nurses
Association, and the Texas League for Nursing).
24. Knopf, Lucille, "Debunking a Myth", Americap Journal of Nursing, August,
1974, Vol. 74, No. 8, pp. 1,416-21.
25. Leininger, M.M., et al, "Primex", American Journal of Nursing, July, 1972,
Vol. 72, No. 7, pp. 1,274-77.
26. Leininger, Madeleine, "This I Believe About Interdisciplinary Health
Education for the Future's,. Nursing Outlook, December, 1971, Vol. 19,
No. 12.
27. Lenburg, Carrie and Johnson, Walter, "Career Mobility Through NursingEducation", Nursing Outlook, Vol. 22, No. 4, April, 1974, pp. 265-269.
28. Leone, Lucile Petry, Statewide Plannin for Nursin Education, Southern
Regional Education Board, Atlanta, org a, 969.
29. Malone, Pat, Nursing Education in Georgia, 1969, Georgia Educational
Improvement Council, Atlanta, Georgia, 1969.
30. Manthey, Marie, "Primary Nursing is Alive and Well in the Hospital",
January, 1973, Vol. 73, No. 1, pp. 83-87.
31. Martin, Cora A., Nebraska's Nurse Supply, Needs and Resources, 1966,
Section of HosiTiiTiind Medical Facilities, Nebraska Department of
Health, 1967.
32. Michigan Department of Education, State Plan for Nursing Education in
Michigan, January, 1971.
t145
138

33. Michigan Department of Education, Nursing Needs in Michigan, Ann Arbor,Michigan, 1970.
34. McNally, Jeanne M., ContinuingsEducation for Nurses: A Survey of CurrentPrograms, American Nurses Association, Kansas City, Missouri, 1972.
35. Moore, Sr. Anne Joachim, The Ladder and the Lattice", Nursing Outlook,Vol. 20, No. 5, May, 1972, pp. 330-332.
36. Mundinger, Mary O'Neil, "Primary Nurse - Role Evaluation", AmericanJournal of Nursing, Oct., 1973, Vol. 21, No. 10, pp. 642-645.
37. National Center for Educational Statistics in cooperation with theAmerican Association of Collegiate Registrars, Definitions ofStudent Personnel Terms in Higher Education, U.S. Department ofHealth, Education and Welfare, Office of rducation, 1968.
38. Natioial Commission for the Study of Nursing and Nursing Education,An Abstract for Action, Jerome P. Lysaught, Director, McGraw-HillBook Co., New York, 1970.
39. National Commission for the Study of Nursing and Nursing Education,From Abstract Into Action, McGraw-Hill Book Co., New York, 1973.
40. National Health Council, Health Manpower, Adapting in the Seventies,Report of the 1971 National Health Forum, New York, 1971.
41. National League for. Nursing, Some Statistics on Baccalaureate and HigherDegree Programs in Nursing, 1971-72.
42. National League for Nursing, Some Statistics on Baccalaureate and HigherDegree Programs in Nursing, 1969.
43. Pierik, M. Madaline, "joint Appointments: Collaboration for BetterPatient Care", Nursing Outlook, September, 1973, Vol. 21, No. 9,pp. 576-79.
44. Population Research Center, The University of Texas at Austin, PopulationProjections for Texas Counties: 1975-1990.
45. Regional Medical Program of Texas, Allied Health Manpower in Texas,1973, prepared by the Texas Hospital Association and the TexasMedical Foundation.
46. Report of the Board of Nurse Examiners for the State of Texas, April,1973.
47. Report of the National Advisory Commission on Health Manpower, Vol. II,Washington, D.C., )967.
48. Schutt, Barbara, "Spot Check on Primary Care Nursing", American Journalof Nursing, November, 1972, Vol. 72, No 11, pp. 1,996-2,00.
139 146

49. Swort, Arlowayne, Nursing Education in Maine, 1970-1985, Maine StateNurses Association, 1972.
50. Tennessee Higher Education Commission,Education in Tennessee, 1969.
51. Texas Employment Commission,and Occupation, 1971.
52. Texas Hospital Association,1972-73.
The Cost of Collegiate Nursing
Texas Employment Outlook to 1975 by Industry
Hospitals and Related Institutions in Texas,
53. Texas League for Nursing, Amarillo Branch, Nursing Needs and Resourcesin the Panhandle Region, 1969.
54. Texas Medical Association, Inventory of Texas Physicians, 1972.
55. Texas State Board of Vocational Nurse Examiners, L.V.N. RelicensureCards, 1971-72, 1972-73.
56. Texas State Department of Health, Directory of Nursing and Convalescent
Homes in Texas, August, 1973.
57. Thurston, Hester I., "Education for Episodic and Distributive Care",
Nursing Outlook, Vol. 20, No. 8, August, 1972, pp. 519-523.
58. Torres, Gertrude, "Educators' Perceptions of Evolving Nursing Functions",
Nursing Outlook, Vol. 22, No0 3, March, 1974, pp. 184:187.
59. U.S. Department of H.E.W., Health Manpower Source Book, Section 2, Nursing
Personnel, Bethesda, Maryland, Revised 1960
60. U.S. Department of H.E.W., TowardAuality in hursing Needs and Goals,
Report of the Surgeon General's Consultant Group on Nursing, Washington,
D.C., 1963.
61. U.S. Department of H.E.W., Nursing Needs and Resources in Texas, Washington,
D.C., 1958.
62. U.S. Department of H.E.W., Definitions of Student Personnel Terms in
Higher Education, Prepared by the National Center for Educational
Statistics in Cooperation with the American Association of CollegiateRegistrars and Admission Officers, 1968.
63. U.S. Department of H.E.W., Report on Licensure and Related Health Personnel
Credentialling, Washington, D.C., 1971.
64. Walsh, Margaret E., "On Nursing's Role in Health Care Delivery", Nursing
Outlook, Vol. 20, No. 9, September, 1972, pp. 592-593.
65. Werley, Harriet, "This I Believe . . . About Clinical Nursing Research";
Nursing Outlook, November, 1972, Vol. 20, No. 11, pp. 718-22.
.ikI140
147

66. Western Interstate Commission for Higher Education, Credit By Examinationin Nursing: Proceedings from a Western Regional Conference. Editedby Jo Eleanor Elliot, Jon Bunnell, Carolyn M. Byerly, 1972.
67. Western Interstate Commission for Higher Education, Today and Tomorrow inWestern Nursing, 1966.
68. Western Interstate Commission for Higher Education, Continuing Educationin Nursing., Boulder, Colorado, 1969.
69. Wood, Lucille, "Proposal: A Carper Plan for Nursing", American Journal-of Nursing, Vol. 73, No. 5, May 1973, pp. 832-835.

APPENDIX A
149

STATISTICAL DATA BY REGION
In this attachment we have included critical data for each reg.ion which
has provided the statistical base for this- report.. The data on pages 147 and
148 show the ratios of types of nurses and physicians to populdtion, the cur-,
rent and projected population, theipercent of each region's popiation over
65 years of age, and the aging.index for each region.
Onthese same pages we have presented in -ncise region-to-region format,
the RN and LVN data, showing activity levels al4u percent working in the various
employment settings.
The second category, of statistical data, shown on pages 149 through 169,
gives detailed information on activity status, age, level of educational prep-
aration, and field of employment for RN's in 1971-72. These pages also include
the projected number of RN's to 1980 on two levels: one under the current, or
.status quo rate of production, and Oft other under the optimum ratios adopted
by the Nursing Project. For examble; at the bottom of each page, we have shown
current ratio of RN's per 100,000 population and below that, the optimum ratios
for 1980.
150145

BEST COPY AY IABLE
40,10011111
UPPER
RIO
111416811. lillWIll go/.11/t111.1111111.8
. . . ai111091.11 MON OPINE. 161111.11 ..11100.0,
PINE.
PANHANDLE
.
a...0. 0......100.
.... ..... al.-...,......1.
....., , ...., ...... 00611 Ilem. too..
IMF Lame awl hire NNW
!wassail wow aum
4PLAINS.! !
PERMIANIMOW 669.6 6/1400
BASIN_iume moor* et=:16.
011111 oll
GRANDE
411186111 liII114
ovum
TEXAS PLANNING REGIONS
September 1971
lin NMGIN
1"NoRTI-rTXA 1 I
N 1±(414'N TU.
TE 0-
74-4. s:"..de Arms twos
poos
IMP "N" 0610161, "1441.
.11o-T-T CENTRAL
TEXAShtOftall I mom tar torkare
1.6 %mow NOM
iamb
W. WOW
isiwut sETINCTitr"(VALLEY
or stale
11111
INA
r
r61
L """ WWI o
ALAMO"7 'i I wore( I WINO
VIM%
ears
*141NTRAL.".
el
A
Nt)REXH
EAS
"I 8
OW seSSW .0400
Ill.110111M
AsNIP
.4111
MO
""T1 ir .
W .---itTEXA ..- . . Ir,... ..... 1. -TEXAS'a ts-t..... -- EXA 't... ....
RAZOS.... "i' %"'" IllALLE;
i.r.
splimestall
to. )10
ONION.
%
C ITAL)0/4114`010 pe
' ...11 014.406.
itoPl
ift.°1 / win"
liras , ssay.oPn,
. 15;11
-19SOUTH
MOM
4
1.0
lea ::444$
. ):'GULFIct7Asf
ors. 6.,
eRilSEPN
\roarsmo
1 Vie
QA1TALBkIlD""
TEXAMIA
IMO
LOWER RIOGRANDE VALLEY
SC
111111,11
-moo
SOUTH EASTTEXAS

0
BEST COPY AVAILABLE
TEXAS STATE PLANNING REGIONS
AM'sPOP.
DIPLOMARN'SPOP.
OSN'SPOP.
NON-FEDN.D.'S
'DIRECT
PT. CAREN.D.'S
PLANNING REGIONS ------- POP. pop.
1 Panhandle 17 21516 '1 78.4 72.7
2 South Plains e SO 14 82.7 76.97 North Texas IS 60 13 95.5 87.54 North Central Texas 14 72 42 128.1 113.15 North East Texas 39 10 le 83.6 78.16 East Texas 14 26 16 87.6 00.5/ West Centre Texas 6 57 12 79.9 70.98 Upper Rio Granda s 94 17 90.7 81.79 Permian eosin 30 19 11 76.6 72.610 Conch* Valley 31 84 16 96.7 AI.911 Central Texas 25 81 22 105.6 94.812 Capital 11 96 46 123.4 99.9..../
I) Praxes Valley 15 16 34 64.9 58.714 Deep East Texas II 89 12 58.2 56.11$ South East Texas 5 se is 101.6 96.516 Gulf Coast 21 85 57 159.5 137.717 Golden Crescent 11 26 15 80.2 73.018 Alamo 14 67 38 122.7 100.0$9 South Texas 21 63 19 52.t 48.2210 Coastal lend 21 15 96.4 88.521 Lower Rio Grande 9 17 15 , 71.4 63.1
STATE 14 6$ 34
11 12 13 14 15
TEXAS STASI PLANNING REGIONS414
TIT.CORR.
POP.PROJ. POOL
POP.!POP.
1:11::
1 tomliond1a
Nkomo REGIONS'-.-pop.
990.1
DA
12143:57::
a.-OVEN
mommgmmm
2 South Plains1ft:
62.8418.3
11.0510.34
33.221.8
3 North Texas 12:4 212.4 17.64 60.9
4 North Central Texas 2636.4 3147.3 3602.7 13.46
$ North lap Texas6 last Texas 416:1_,
2W0
202.2 , 205.64$1.6245.0
453.4226.0
193.0
q iiii
43./C8/ .
64/ Mhos Central Texas
N Ganche Valley 120.9E
573.5
.
14.64 47.8
I *par Rio Grande 372.3 463.0 2949 Parolee Basin 304.3 357.0
125.214.2.
11 Genlraljetat 426.2 429.5 66.16
12 CsOlta1 446.6 485.3Tni
16.86
I) Smola Valley245.8 305.7 14.36 r4294 127.4 16.79 .2
:I South Cast TeamsOblf Coast 2305.1
;:::34734
VII Seep East Texas315.9 371.2 7.20 19.5
126.0 1:1:1pm 30,0
Imo 12.95 39.117 loloon Crescomt1228.0
%1)16.4 13.00 36.4
18 _Alamo1124.3 \
19 Soma Texas 99.6 .114.1 157.4 1.75 28.1
317.5 817.3 alls.9
1.1949 3:1
420.4 46168 511.6 .86 Noose Good81 Low Me Grande
.1 , 8 3 4 0
2.t 147
15'

TEXAS STATE PLANNING 'LEGIONSNURSING MANPOWER AND RELATED INFORMATION
%ES\iilkt6,11i.tLL
BANNING REGIONS
TOT.RN's:PCP.*
ACT.RN's:POP.
I Panhandle 343 2592 South Plains 240 182
North Texas 279 208
4 North Central Texas 331 239
S North East Texas 226 174
6 lest Texas 232 165
7 West Central Texas 249 183
8 Upper Rio Grande 302 223
9 P.roian Basin 228 168
10 Concho Valley 338 2169
11 Central Texas 332 243
12 Capital 379 268
13 Brazos Valley 255 176
14 Deep East Texas 173 121
IS South Eat' Texas 322 236
16 Gulf Coast 378 27$
17 Golden Crescent 225 *418 Alamo 334 231
19 South Texas 133 106
2021
Coastal SendLower Rio Grand.
STATE
229161
312
168
116
214
Column Number
*Pas per 100.000 population**Nora than one SMSA
NMS. 2 RNNOME IN
BEDS: 1154.
Ufa MIL_
'S
PLANNING REGIONS
1 Panhandle 412.3
2 South Plains 447.0
3 North Texas --934.94 North Central Texan 476.85 North East Texas 938.5
6 East Taxes 720.9
7 Vest Central Texas 1120.68 Upper Rio Grande 131.8
10 Concha galley11 Central Texas:2 Capita!13 Grazes Valley14 &lop East TexasIS South East Texas16 Gulf Coast17 Golden Crescent18 Alamo19 South Texas20 Coastal lend21 Lower Rio Grand,
Permian Basin 310.0942.6789.8633.5653.5559.3368.7291.9
755.5448.5217.2371.1432.6
4.373.605.233.605.656.814.552.083.086.236.59
3.694.74
4.972.622.778.136.602.41
3438.40
1 2
ACT.
4CT. RNRN 1NACT. RN's SRN TOT.
FIE: ON's: ACT.: SMSA SMSA LVN's:POP. POP. INACT. rm. POP. POP.
236171
2161
153
167202
153221
221
236
155102
255255146
200101152
102
2 3
$4 3.07 376 142
58 3.12 236 103
71 2.9 1 132
92 2.6 2 "13752 3.3 4 15367 2. 240 12366 2.80 225 135
79 2.8 1 95
60 2.81 1
** 147
95 2.56 1
2589 2.73 278 210111 2.40 318 12579 2.23 210 106
52 2.32 118
86 2.7100 2. 266 126
61 2.68 163
103 2.25 231 15627 4.00 115 41
61 2.70714 142
45 2.64 ** 9685
4 5 6 7
TEXAS STATE PLANNING REGIONS :
i LYN'SIN
N$C.
14.8111.2311.84
17.1926.7420.8524.63
9.02
169.752726.4924.4525.3917.7312.3016.6918.40
15.0212.36
9.8220.00
3
NOSP.BIDS:POP
RN'SIN
HOSP.
NOSP.810:RN'S InNOSP.
476.5393.3507 .7
358.7473.7433.1547.8411.3435.4571.4.44.0
315.3/35.9473.9434.34,2.2477.1333.2254.1406.1224.0
4.
65.3664.1667.5463.8460.73
62.53u.15.46
65.7764.2671.1964.3462.9361.5955.1066.0461.7262.4142.8660.7943.95
/'5
3.542.4
5
4.i
3
4.9
3.93.52.72
3.6.43.42.84.62.56.3
4.34.1
6
i 148 153
300
356
387277
351
435512
157
363724
349241
233380
33i273
530264
199369203303
8
ACT. LVNOrals! FIE:
POP. POP.
LVN'sACT:INACT.
ACT. 1111's
ACT. LVN's
249 221 4.92 1.04
307 278 6.34 .59
331 290 5.90 .63
232 205 5.12 1.03
295 261 S.33 .59
359 312 4.71 .46
441 387 6.21 .42
128 Ila 4.50 1.74
309 274 4.85 .54
389 344 5.32 .63
291 254 5.01 .84
200 176 4.8C 1.34
19* 171 5.02 .91
307 271 4.24 49276 241 4.61 .86
229 200 5.15 1.21431
2064.36 .38
225169 157
5.755.56
1.03.63
11
1
378 301164
5.397.05
.54.61,
224
9 10 11 12
LV1I'S
INHosp.
2 RN'SIN
OFFICE
2 LYN'SIN
OFFICE
2 RNIN
P.M
.1=M1~$11=1.1.
66.55
.1=PIIIMMONID
10.47 10.39 2.9965.44 5.73 12.97 7.5358.41 3.49 8.48 6.1061.53 1.25 8.35 3.5758.47 4.80 7.48 3.3960.18 5.31 945 5.9959.41 6.72 6.40 4.3565.7! 6.12 7.21 .6672.1i 10.00 12.03 4.04
9.14 6.13 6.23;1:11 4.24 551.43 7.62 8.22 1.1111.6156.25 10.34' 10.16 5.6065.06 5.30 6.78 4.3068.46 7. 59 6.60 6.5468.28 7.25 8.72 34861.57 5.74 8.38 4.31.
70.35 5.28 4.51 6.2266.29
70.60 5.567.1711.07
18.756.78
58.23 3.46 12.42 11.36
7 10

ACTIVITY STATUS
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Inceeplete
TOTAL
=M
.-1
111M
11
869
75.43
-283
_21.57
686
111
61
11
869
MI=
78.94
12.77
7.02
1.27
100.00
REGION
1
1971-72 R11 L[CEUSURE DATA
HIGHEST EDUCATIONAL PREPARATION
AGE DISTRIBUTION
-20 - 29
3C - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
171
204
221
164
60
49
869
19.68
2:1.48
25.43
18.87
6.90
5.64
100.00
FNo Degree
'
8SN
Bacc. Other
mSN
Master's Other
Ph. D.
Incomplete
TOTAL
E02
69.28
70
8.06
15
1.73
8.92
8.92
00.00
166
19.10
869
100.00
FIELD OF EMPLOYMENT
IHospital
568
65.36
Nursing Home
38
4.37
Sch. of Nsq.
54
6.21
Private Duty
18
2.07
Public Health
26
2.99
School Nurse
46
5.29
Industrial Nurse
7.81
Office Nurse
91
10.47
Other
00.00
Incomplete
21
2.42
TOTAL
869
100.00
OM
,
DETERMINATION OF
41'
1%.
JmeHospitals
4111
6 -
24 beds
MD
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
500 *
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
_Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
DEMAND FOR RN's BASED ON ADOPTED RATIOS
No. of Addi-
No. of RN's
No. of RN's
tional RN's
Currently
Required to
Required to
Emo1ormi
Achieve (FTE)
Achieve 'FTE)
Optimum Values
Optimum Values
PROJECTED RN SUPPLY PATTERN
-- PRESENT
DAD
Local Graduates
831
495
regional Retention Rate
.57
.78
Local Graduates Retained
473
386
Inflow
13
9
Total New Graduates
486
395
xActivity Rate
.97
.97
a
TOTAL Projected
Additional Active
RN's by 1980
471
+ 383
- 1980
BSN
.1105
598
.50
2.54 14
268
.94
+ 251
510
3444
811325
707
13
116
111
422
662
1211
"70
48
5366
1019
152
86
26
-33-
40
41
312
Status Quo
Optimum Level
Number of
IN's Re-
ON's/100,000
quired by
Population
196C
236
856
308
1117
Present
Number
of Active
RN's
Additional
RN's
.Required
778
78
778
339
Total Addi-
tional RN's
Ae
b.
1980
1980
bAttrition
142
220
142
481
Projected
RP
1
Supply by
Surplus
1980
s(Deficit)
1105
885
1105
624

ACTIVITY STATUS
Active
Inactive
Active:
Fullrtime
15-30 Mrs/Mk
Less 15 Hrs/Wk
Incomplete
TOTAL
NN
WM
I*
611
75.71
X26_
24,29
511
83.63
57
9.33
39
6.38
4.65
611
100.00
DETERMINATION OF
I'
*VW
.: Hospitals
Z5
6 -
24 beds
25 -
49 beds
50 -' 99 beds
Olk
100 -.299 beds
IJI
300 - 499 beds
fin
500
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
Status Quo
Optimum Level
.1.1
111
DEMAND FOR /47,',
No. of .N's
Currertty
Emplcird
[FTE)
36221
61
33 12
44
533
28
161_
RN's/100,000
Population
REGION
2
1971-72 RN LICENSURE DATA
AGE DISTRIBUTION
20 - 29
126
20.62
30 - 39
116
18.99
40 - 49
177
28.97
50 - 59
104
17.02
60
58
'
9.49
Incomplete
30
4.91
TOTAL
611
100.00
RASED ON ADOPTED
No. of RH's
Required to
Achieve (FTE)
Optimum Values
12
185
48
483
203
931 .
28
67
50
52
66
Number of
RN's Re-
quired by
1980
RATIOS
No. of Addi-
tional RN's
Required to
Achieve (FIE)
Optimcm Values
Present
Number
of Active
RN's
569
107 617
oo
;2
7(1
HIGHEST EDUCATIONAL PREPARATION
Ho Degree
8SN
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
Required
411
6214 3 6 0
115
611
67.27
10.15
2.29
.49
.98
0.00
18.82
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Privatc Duty
Public 'Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
392
22
2316
4665 1
35 0
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
DAO
BSN
676
. 6974
Local Graduates
x
Regional Retention Rate
Local Graduates Retained
Inflow 2
Total New Graduates
Activity Rate
TOTAL Projected
Additional Active
RN's by 1980
471
48
16
56
519
16
56
. 9787 .9787
.9412
64.16
3.60
3.76
62
7.53
10.64
.16
5.73
0.00
1.80
100.00
938
*15
*53
576
Total Addi-
Projected
tional RN's
RN
Age
(Deficit)
Supply by
Attrition
Required
st
by 1980
1980
171
715
5E1
154
110
264
576
312
394
1648
561
1087
110
1197
576
(621)

ACTIVITY STATUS
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Incomplete
TOTAL
.11M
1=
MO
459
74.51
-157
...
g5.49
362
78.87
55
11.98
34
7.41
81.74
459
100.00
REGION
3
1971-72 RN LICENSURE DATA
AGE DISTRIBUTION
HIGHEST EDUCATIONAL PREPARATION
20 - 29
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
80
17.43
103
22.44
112
24.40
92
20.04
55
11.98
17
3.70
459
100.00
MM
.
DETERMINATION OF OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
16
Hospitalslo
.7.2-
6 -
24 beds
25 -
49 beds
OL
50 -
99 beds
lit
100 - 299 beds
ch
300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Hoe Nurses.
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
No. of RN's
No. of RN's
Currently
Required. to
Employed
Achieve (FIE)
(FTE)
Optimum Values
15
115
96
302
278
21 91425
27
374 31
AM's/100,000
Population
Status Quo
193
Optimum Level
404
528
INF
39
393443
116.L
No. of Addi-
tional RN's
t'Required to
Achieve (FTE)
Optimum Values
Number of
Pre:ient
NN 's
Number
quired by
of Active
1980
-
410
410
858
410
250
1573025 9
FIELD OF EMPLOYMENT
No Degree
307
66.88
Hospital
310
BSN
34
7.41
Nursing Home
24
Bacc. Other
12
2.61
Sch. of Nsq.
22
MSN
81.74
Private Duty
34
Master's Other
3.65
Public Health
28
Ph.D.
00.00
School Nurse
9
Incomplete
95
20.70
Industrial Nurse
1
TOTAL
459
100.00
Office Nurse
16
Other
1
Incomplete
14
TOTAL
459
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
x
Regional Retention Rate
Local Graduates Retained
Inflow
Total New Graduates
Activity Rate
s
TOTAL Projected
16
Additional Active
487
RN's by 1980
Additional-
RN's
6Required
0
448
DAO
BSN
533
.69
367
427
23
4394
23
.97
.97
.94
67.54
5.23
4.79
7.41
6.10
1.96
.22
3.49
.22
3.05
100.00
4385
22
m411
Total Addi-
Projected
tional RN's
RN
Ave
Required
Supply by
+Attrition
it
by 1980
-1980
=Surplus
(Deficit)
101
101
411
310
101
549
411
(138)

ACTIVITY STATUS
Active
inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Incomplete
TOTAL
IM41
0111
.
6.305
2,41 L
4,825
929
460
91
6.305
IMP
72.34
27.66
76.53
14.73
7.30
1.44
100.00
REGION
4
LICENSURE DATA
HIGHEST EDUCATIONAL PREPARATION
1971-72 RN
AGE DISTRIBUTION
20 - 29
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
1,381
21.90
1,396
22.14
1,490
23.63
1,187
13.83
551
3.74
300
4.76
6,305
100.00
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED
cn Hospitals
6 -
24 beds
06
26 -
49 beds
Vt
00 -
99 beds
.4
100 - 299 beds
300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
Status Quo
Optimum Level
No. of RN's
Currently
Employed
(FTE)
3542
204
355
459
249
220
5029
+706
-51§5
- RN's/100,000
Population
211
312
No. of RN's
Required to
Achieve (FTE)
Optimum Values
65
249
717
1682
694
1708
5115
106r
502
596
442
527
1247
Number of
RN's Re-
qui1980
red by
6640
9819
RATIOS
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
1573
861
147
137
193
307
3218
Present
Number
of Active
RN's
5565
5565
No Degree
BSN
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
Required
1075
4254
3,674
58.27
1,150
18.24
146
2.32
115
1.82
74
1.17
5.08
1,141
18.10
6,305
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
4,025
227
237
321
225
373
194
52012
171
6,305
PROJECTED RH SUPPLY PATTEWN -- PRESENT - 1980
DAD
BSN
Local Graduates
.x
Regional Retention Rate
Local Graduates Retained
Inflow =
Total flew Graduates
x
Activity Rate
TOTAL Projected
Additional Active
RN's by 1980
Total Addi-
tional RN's
Age
Required
Attrition
by 1980
1144
1144
ga
35
64
119
.9672
1754
180
1934
.9672
1628
712
2340
.9242
63.84
3.60
3.76
5.09
3.57
5.92
3.08
8.25
.19
2.71
100.00
115
+1871 +
2163°
4149
Projected
RN
Supply by
Surplus
1980
(Deficit)
4149
1930
4149
(1249)

REGION
5
1971-72 RN LICENSURE DATA
ACTIVITY STATUSA
mN
zAGE DISTRIIIUTION
HIGHEST EDUCATIONAL PREPARATION
FIELD OF EMPLOYMENT
I
Active
354
76.96
20 - 29
C1
19.49
No Degree
215
60.73
Hospital
215
60 73
Inactive
106
23.04
30 - 39
6)
19.49
8511
32
9.04
Nursing Home
20
5.65
Active:
40 - 49
81
22.88
Sect. Other
41.13
Sch. of Msg.
23
6.50
Full-timm
295
83.33
50 - 59
75
21.19
MSN
3.85
Private Duty
71.98
15-30 Hrs/Uk
35
9.89
60 +'
38
10.73
Master's Other
41.13
Public Health
12
3.39
Less 15 Hrs/Wk
18
5.08
Incomplete
22
6.21
Ph.D.
00.00
School Nurse
23
6.50
Incomplete
61.69
TOTAL
354
100.00
Incomplete
96
27.12
Industrial Nurse
22
6.21
TOTAL
354
100.00
TOTAL
354
100.00
Office Nurse
17
4.80
Other
1.28
Incomplete
14
3.95
TOTAL
354
100.00
Oa.
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
No. of Addi-
No. of RN's
No. of RU's
tional RN's
Currently
Required to
Required to
Esyloyed
Achieve (FTE)
Achieve (FTE)
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
DAD
BSN
(FIE)
Optimum Values
Optimum Values
Local Graduates
426
4.11 (.4
Hospitals
6 -
24 beds
Regional Retention Rate
(.37)
(.71)
25 -
49 beds
75
wSO -
99 beds
82
Local Graduates Retained
377
100 - 299 beds
227
300 - 499 beds
152
Inflow
513
22
500 +
beds
111
TOTAL HOSPITALS
193
536
343
Total New Graduates
5389
22
Nursing Home Nurses
18
165
147
xSchool Nurses
22
39
17
Activity Rate
.97
.97
.94
Office Nurses
15
32
17
Private Duty Nurses
532
27
TOTAL Projected
Public health Nurses
11
40
29
Additional Active
SUB-TOTAL CATEG4IES
264
844
580
RN' 3 by 1980
5+
377
+20
`
Other
61
TOTAL
Number of
RN's Pe-
Present
!timber
Additional
Total Addi-
tional RN's
Projected
RN
RN's/100,000
quired by
of Active
RN's
Age
Required
Supply by
Surplus
Population
Required
+Attrition
=by 1980
1980
Status Quo
Optimum Level
161
331
417
857
325
675
81
402
321
125
532
75
607
402
(205)
402

ACTIVITY STATUS
ij
Active
Inacti-ve
Active;
Full -time
15-30 Hrs/Wk
Less 15 Nrs/Ak
TOTALIncoeplete
NIN
.
734
296
5767674 8
734
4111
1=
NW
71.26
28.74
78.47
10.35
10.08
1.09
100.00
REGION
6
1971-72 RN LICENSURE,DATA
AGE DISTRIBUTION
#
20 - 29
30 - 39
40 - 49
50 - 59
60
Incomplete
TOTAL
128
149
176
144
83 54
734
DETERMINATION OF DEMAND FOR RA's BASED ON ADOPTED RATIOS
Hospitals
41
6 -
24 beds
25 -
49 beds
60 -
99 beds
100 - 299 beds
100 - 499 beds
600 *
beds
pie
TOTAL HOSPITALS
utAursing Nome Nurses
IDSchool Nurses
Office Ames
Private Out, Nurses
Public Health Nurses
4SUB-TOTAL CATEGORIES
Other TOTAL
States QUO
Optimum Level
No. of RN's
Currently
(FTE)
Em (FTE)
411
4446 3519
42
597
+ -Si
655
AN's/100,000
Population
No. of RN's
Required to
Achieve (FTE)
0Otieum Values
20
152
133
800
1105
17T
84 70
69
86
1788
Number of
RN's Re-
quired by
1980
17.44
20.30
23.98
19.62
11.31
7.35
100.00
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
694
338 0
3 35
50
44
1191
Present
Nueber
of Active
RN's
HIGHEST EDUCATIONAL PREPARATION
S
No Degree
BSN
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
Reg
ui r
ed
456
87 10 5 4 0
172
734
62.13
11.85
1.36
.68
.54
0.00
23.43
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
45950
37
25
44
48
16
39 0
16
7/4
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
DAD
BSN
210
.567
175
119
575
180
194
.97
.97
.94
Local Graduates
RegiOnal Retention Rate
Local Graduates Retained
Inflow
Total New Graduates
x
Activity Rate
a
TOTAL Projected
Additional Active
RN's by 1980
Age
Attrition
p
Total Addi-
tional RN's
Required
12111M1__
305
.573
30
30
62.53
6.81
5.04
3.41
5.99
6.54
2.18
5.31
0.00
2.18
igp.00
175
188
18
391
Projected
RN
Supply by
Surplus
1980
(Deficit)
152
691
655
36
155
191
391
200
417
1883
655
1228
155
1343
391
(952)

ACTIVITY STATUS
0.
AGE DISTRIBUTION
REGION
7
1971-72 RI, LICENSURE DATA
PREPARATION
FIELD OF EMPLOYMENT
_HIGHEST EDUCATIONAL
Active
506
73.65
20 - 29
91
17.98
No Degree
352
69.57
Hospital
360
71.15
- _
-11
_.26.35
30 - 39
101
19.96
BSN
43
8.50
Nursing Home
23
4.5S
Active:
'40 - 49
101
19.96
[tact. Other
12
2.37
Sch. of Nsq.
12 ,
2.37
Full -tine
404
79.84
50 - 59
112
22.13
RSN
2.40
Private Duty
13
2.57
13 -30 Hrs/Wk
61
12.06
60 +
71
14.03
Master's Other
S.gg
Public Health
22
4.35
Less 15 lirs/Nk
34
6.72
Incomplete
30
5.93
Ph.D.
00.00
School Nurse
32
6.32
Incomplete
71.38
TOTAL
506
100.00
Incomplete
92
18.18
Industrial Nurse
00.00
TOTAL
506
100.00
TOTAL
506
100.00
Office Nurse
34
6.72
Other
00.00
rIncomplete
10
1.98
TOTAL
506
100.00
.1
DETERMINATION OF DEMAND
2111
121F Hospitals
6 -
24 beds
25 -
49 beds
SO -
99 beds
100 - 299 beds
300 - 499 beds
SOO
beds
TOTAL HOSPITALS
OW Nursing Home Nurses
CP School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
FOR RN's BASED ON ADOPTEDRATIOS
Na. of Addi-
No. of RN's
No. of RN's
tional RN's
Curployed
rently
Required to
Requirod to
Em
Achieve (FTE)
Achieve (FTE)
(FTE)
Optimum Values
Optimum Values
PROJECTED RN SUPPLY PATTERN -- PRESENT -
DAO
Local Graduates
293
.x
Regional Retention Rate
.49
Local Graduates Retained
144
Inflow
10
30
Total New Graduates
154
30
xActivity Rate
.97
.97
TOTAL Projected
Additional Active
RN's by 1980
149 *
29
+
1980
BSN
s
Cc,
c-.
c=n
-c,
2m.
10
10
.93 9
335
22 33
34 1020
454
713-
469
13
195
107
169
185
669
-277 49
38
4556
1130
334
251 16 4 35
36
676
187
Rees/100,000
Population
Status Quo
167
Optimum Level
403
Number of
Present.
RN's Re-
Number_
quired by
of Active
1980
RN's
426
-469
1030
469
;1
Additional
RN's
Required
(43)
,561
Total Addi-
Projected
tional RN's
RN
Age
Required
Supply by
Surplus
eby 1980
+Attrition
-1980
2(Deficit)
127
84
187
103
127
688
187
(501)

REGION
8
ACTIVITY STATUS
S
AGE DISTRIBUTION
#
1971 -12 RN LICENSURE DATA
PREPARATION
HIGHEST EDUCATIONAL
Active
866
73.70
20 - 29
181
20.90
No Degree
612
70.67
Inactive
=11
.Q9
-26.30
30 - 39
162
18.71
BSN
85
9.82
Active:
40 - 49
212
24.48
Bacc. Other
16
1.85
Full-time
705
81.41
50 - 59
200
23.09
MSN
15
1.73
15 -30 Hrs/Wk
90
10.39
60 +
73
8.43'
Master's Other
11
1.27
Less 15 Hrs/Wk
59
6.81
Incomplete
38
4.39
Ph.D.
00.00
Incomplete
12
1.39
TOTAL
866
100.00
Incomplete.
127
14.67
TOTAL
866
100.00
TOTAL
866
100.00
MIN
am.
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED
RATIOS
FIILU OF EMPLOYMENT
Hospital
-Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
57518
31
2149
85 7
53 1
26
866
66.40
2.08
3.58
2.42
5.66
9.82
.81
6.12
.12
3.00
1(10.00 CX2
No. of RN's
Currently
Employed
No. of RN's
Required to
Achieve (FTE)
No. of Addi-
tional RN's
Required to
Achieve (FTE)
PROJECTED RH SUPPLY PATTERN -- PRESENT -
0AD
1980
8SN
-, Hospitals
UTE)
Optimum Values
Optimum Values
Local Graduates
.x
60
292
895
ZO"
.m=
2E:
624 beds
20
Regional Retention Rate
.715
.60*
.60*
25 -
49' beds
30
50 -
99 beds
64
Local Graduates Retained
43
175
537
100 - 299 beds
37';
Ow,
300 - 499 beds
385
Inflow
95
5
41ft
500 +
beds
w..
TOTAL HOSPITALS
515
363
Total New Graduates
52
180
542
Nursing Howe Nurses
16
37
21
School Nurses
82
89
7Activity Rate
.97
.97
.94
Office Nurses
47
62
15
Private Duty Nurses
15
61
46
TOTAL Projected
Public Health Nurses
47
76
2481_
Additional Active
SUB-TOTAL CATEGORIES
Z22_
1203
RN's by 1980
50
*174
*509
I'
733
Other
+64
TOTAL
RN's/100,000
Population
Number of
RN's Re-
quired by
1980
Present
Number
of Active
RN's
Status Quo
202
935
786
Optimum Level
317
1468
786
Additional
RN's
Required
149
682
*Estimate
Total Addi-
tional RN's
Age
Required
Attrition
by 1980
173
173
322
855
based on State Average
Projected
RN
Supply by
Surplus
1980
(Deficit).
733
733
411
(122)
m

REGION 9
1971-72 P11 LICENSURE DATA
ACTIVITY STATUSI
AGE DISTRIBUTION
HIGHEST EDUCATIONAL PREPARATION
FIELD of EMPLOYMENT
Active
520
73.76
20 - 29
48
9.23
No Degree
325
62.50
Hospital
342
65.77
- - _
Active:
uts
Z§.24
30 - 39
40 - 49
96
170
18.46
32.69
BSN
Bacc. Other
41 11
7.88
2.12
Nursing Home
:NY
16
20
3.08
3.85
Full-time
427
82.12
50 - 59
125
24.04
MSN
3Private Duty
10
1.92
15-30 Hrs/Hk
54
10.38
60 +
55
12:1531(3)
Master's Other
2.38
Public Health
21
4.04
Less 15 Hrs/Wk
'33
6.35
Incomplete
26
1.19
School Nurse
47
9.04
Incomplete
61.15
TOTAL
520
100.00
Incomplete
137
26.35
Industrial Nurse
1.19
TOTAL
520,
100.00
TOTAL
520
100.00
Office Nurse
Other
52 1
10.00
.19
Incomplete
10
1.92
TOTAL
520
100.00
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED
Hospital
6 -
24 bids
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
SOO
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
No. of RN's
No. of RN's
Currently
Required to
Eirloyird
Achieve (FTE)
Optimum Values
3061445
47 7
20
35
39..
+4 ---'
474
AN's/100,000
Population
Status Quo
153
Optimum Level
276
24
87
157
90
175
533
70454961
838
Number of
RN's Re-
quired by
Re-
q1980
RAMS
No. of Ad4i-
tional RN's
Required to
Achieve (FTE)
Optimum Values
227
6625
-2-4241
399
Present
Number
of Active
RA's
546
424
985
474
511
Additional
RN's
=Required
PROJECTED P11 SUPPLY PATTERN -- PRESENT - 1980
Lo'y'al Graduates
x
Regional Retention Rate
Local Graduates Retained
Inflow a
Total New Graduates
Activity Rate
TOTAL Projected
Additional Active
RN's bt 1980
0AD
BSN
505
.682
344
13
27
36
13
371
36
.97
.97
.94
13
36
*34
u407
Total Addi-
Projected
tional RN's
RN
Age .
Required
Supply by
Surplus
+Attrition
=by 1980
-1980
:tOeficit)
72
.117
189
407
218
117
628
407
(221)

ACTIVITY STATUS
0
Active
lAscaPe-
Active:
Full-time
15-30 Mrs/Wk
Leis 15 Hrs/Wk
Incemplets
TOTAL
ION
S
305
71.93
119
-28.07
249
31 24 1
305
81.64
10.16
7.87
.33
100.00
MO
O
REGION
10
1971-72 RH LICENSURE DATA
HIGHEST EDUCATIONAL PREPARATION
'AGE DISTRIBUTION
,20 --29
30 , 39
40 - 49
SO - 59
60 +
Incomplete
TOTAL
494377
76
5010
305°
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
_,
Hospitals
--44r's-
624 beds
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
+beds
TOTAL HOSPITALS
Nursing Home Nurses
--
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SBA-TOTAL CATEGORIES
Other TOTAL
Sicatus Quo
Optimum Level
16.07
14.10
25.25
24.92
16.39
3.28
tomo
No. of Addi-
No. of RN's
No. of RN's
tional RN's
Currently
Required to
Required to
Employed
Achieve (FTE)
Achieve (FTE)
(FTE)
Optimum Values
Optimum Values
176
1712
27
10 18
UA
L_17
2.71
_
RN' s/100,000
Population
221
464
36
61
29
272
_221
70 21 20 18
22
_51L
Number of
RN's Re-
quired by
1980
276
580
222
61 9-7-8 4
29/___
Present
Number
of Active
RN's
-276
277
No Degree
BSI1
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
194
29 6 1 2 073
305
63.61
9.51
1.97
. 33
. 66
0.00
23.93
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
196
64.26
19
6.23
13
4.26
13
4.26
19
6.23
12
3.93
1.33
30
9.84
1.33
1.33
305
100.00
PROJECTED RH SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
.x
Regional Retention Rate
Local Graduates Retained
Inflow a
Total New Graduates
xActivity Rate
TOTAL Projected
Additional Active
RN's by 1980
Total Addi-
Additional
tional RN's
RN's
Age
Required
aRequired
Attrition
aby 1980
0.
88
88
303
88
391
0AD
8511
545
.586
319
59
13
5328
13
.97
.97
.94
54
318
4'
12
2335
Projected
RN
Supply by
Surplus
1980
(Deficit)
335
247
335
(56)

ACTIVITY STATUS
111
AGE DISTRIBUTION
0.
REGION
11
1971-72 RN LICENSURE DATA
PREPARATION
FIELD OF EMPLOYMENT
HIGHEST EDUCATIONAL
Active
1,062
73.19
20 - 29
186
17.51
No Degree
645
60.73
Hospital
'/56
73.19
- -
Active:
189_
Z.0.81
30 - 39
40 - 49
158
rp
291
14.88
27.40
BSN
Bacc. Other
132 17
12.43
1.60
Nur
sing
Mow
Sch. of Nsq.
70
46
6.59
4.33
Full-time
871
82.02
50 - 59
241
22.69
MSN
10
.94
Private Duty
25
2.35
1S -30 Hrs/Wk
113
10.§4
60 +
127
11.96
Master's Other
8.75
Public Health
32
3.01
Less
15lirs/Wk
,71
6.69
Incomplete
59
5.56
Ph.D.
1.09
School Nurse
48
4.52
Incomplete
7.6r
TOTAL
1,062
100.00
Incomplete
249
23.45
Industrial Nurse
13
1.22
TOTAL
1,062
100.00
TOTAL
1,062
100.00
Office Nurse
45
4.24
Other
1.09
incoewlete
26
2.45
TOTAL
1,062
100.00
1';
.1
Ca.
om.
um'0 .
gp
MID
DETENMINATION OF DEMAND
Hospitals
6 -
24 beds
25 -
49 beds
SO -
99 beds
100 - 299 beds
300 - 499 beds
500 +
beds
(dT
ALHOSPITALS
Nursing Horns Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
Ste-TOTAL CATEGORIES
Other TOTAL
MIN
MIN
MIN
FOR RN's BASED ON ADOPTED RATIOS
No. of Addi-
No. of RN's
No. of RN's
tional RN's
Currently
Required to
Required to
Employed
Achieve (FTE)
Achieve (FTE)
(FIE)
Optimum Values
Optimum Values
7-ROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
0AD
Local Graduates
1152
.x
Regional Retention Rate
(.7O)(.259)
Local Graduates Retained
618
Inflow
518
Total New Graduates
5636
x
Activity Rate
.97
.97
TOTAL Projected
Additional Active
RN's by 1980,
5617
BSN
Ce.
e=3
,21"
awc=
375
.553
207
63
270
.94
254
678 /
617
4640
19
30
JUL
93
5
204
137
.281
309
936
-UT
.77
81
6987
258
260
31
41 50
'57
' 876
Status Quo
Optimum Level
RN's/100,000
Population
221
367
Number of
RN's Re-
quired by
1980
949
1576
Present
Number
of Active
RN's
967
967
Additional
RN's
=Required
(18)
.
609
Age
Attrition
Total Addi-
tional RN's`
Required
by 1980
Projected
RN
Supp'y by
Surplus
1980
(Deficit)
247
229
876
647
247
856
876
20

a
ACTIVITY STATUS
S
Active
1,220
70.E0
Inactive
508_
29.40
Active:
Full-time
931
76.31
15-30 Hrs/Wk
189
15.49
Less 15 Hrs/Wk
84
6.89
Incomplete
16
1.31
TOTAL
1,220
100.00
MID
11.
=11
REGION
12
.1971-72 RN LICEIISURE DATA
HIGHEST EDUCATIONAL PREPARATION
AGE DISTRIBUTION
20 - 29
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
343
28.11
250
20.49
229
18.77
224
18.36
128
10.49
46
3.77
1,220
100.00
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
Hospitals
6 -
24 beds
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
500
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
SWAS Quo
Optimum Level
No. of RN's
Currently
Employed
FTE
'704
3953
83 15
98
992
+1076
RN's/100,000
Population
236
286
Ho. of RN's
Required to
Achieve (FTE)
OPtMmum Values
12
118
56
348
172
706
67
90
71
89
1281
Number of
RN's Re-
quired by
1980
1145
.1388,
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
2
210
23 7-
56
-9-
289
Present
Aber
of Active
RN's
No Degree
BSN
Ilacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
=Required
11
FIELD OF EMPLOYMENT
IS
705
57.79
Hospital
203
16.64
Nursing Home
34
2.79
Sch. of Nsq.
36
2.95
Private Duty
19
1.56
Public Health
7.5i-,-.5thool Nurse
216
17.10
Industrial Nurse'
1,220
100.00
office-Nurse
Other
Incomplete
TOTAL
785
45
6320
105
5510
93
11 33
1,220
PROJECTEO'RN SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
X
Regional Retention Rate
Local Graduates Retained.
Inflow
Total New Graduates
Activity Rate
TOTAL Projected
Additional Active
VA's by 1980
Age
Attrition
Total Addi-
tional RN's
Required
=,pr 1980
1076
69
240
309
312
240
552
1076
420
.81
340
27
367
.97
AO
BSN
1859
.50
929
117
126
117,
1055
.97
.94
64.34
3.69
5.16
1.64
L.61
4.51
.82
7.62
.90
2.70
100.00
356+
113
.992
1461
Projected
RN
Supply by
Surplus
1900
(Deficit)
1111
1MM
...'
1461
1152
1461
909

REGION
13
1971-72 RN LICENSURE DATA
ACTIVITY STATUS
AGE DISTRIBUTION
Active
- -
_Active:
Full-time
15-30 Hrs/Wk
Lest 15 Hrs/Wk
Incomplete
TOT AL
232
69.05
W4
_30
.95
176
75.86
40
17.24
15
6.47
1.43
232
100.00
20 - 29
30 - 39
40 - 49
50- 59
60 +
Incomplete
TOTAL
70
43
£5
4419
11
232
30.17
18.53
19.40
18.97,
8.19
4.74
10p.00
=ID
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
No. of RN's
Currently
Employed
(FTE)
Hospitals
No. of RN's
Required to
Achieve (FTE)
Optimum Values
at
6- 24 beds
23 -
49 bids
SO -
99 beds
100 - 299 beds
300 - 499 beds
500
beds
5946
-74
"TOTAL HOSPITALS
131
179
_!"
Nursing Home Nurses
10
89
School Nurses
16
23
Office Nurses
22,
75
Private Duty Nurses
621
Public Health Nurses
12
26
SUB-TOTALCATEGORIES
191
53
Other
7
TOTAL
21a..
Status Quo
Optimum Level
Mrs/100,006
Poptilatten
155
272
NumPher of
IN's Re -
quired'by
1980
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
4879 7
-7-
75
1 1564
Present
Number
of Active
RN's
HIGHEST EDUCATIONAL PREPARATION
%
Ho Degree
BSN
Bacc. Other
NSN
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
Required
197
204
(7)
347
204
143
127:
44 6 6 2 0
47
232
54.74
18.97
2.59
2.59
.86
0.00
20.26
100.00
FIELD OF EMPLOYMENT
Hospital
,
Nursing Home
SEA. of Nsq.
Private Duty
Public Health
School Nurse
Industrfal Nurse
Office Nurse
Other
Incomplete
TOTAL
146
62.93
11
4.74
62.59
83.45
13
5.60
17
7.33
00.00
24
10.34
00.00
3.02
23Z
vo.po
PROJECTED Ni SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
.x
Regional Retention Race
Local Graduates Retained
Inflow
Total New Graduates
tActivity Rate
=
TOTAL Projected
Additional Aitive
RN's by 1980
7Total Addi-
tional RN's
Age
Required
Attrition
by 1980
41
34
41
184
0AO
BSN
9.
72
54
972
54
.97
;"
.97
.94
9+
70
*51
130
Projected
RN
Supply by
Surplus
1980
(Deficit)
130
130
96
(54)
4

I
ACTWITY STATUS
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Incomplete
TOTAL
302
69.91
_130_
30.09
231
76.49
35
11.59
24
7.95
12
3.57
302
100.00
REGION
14
1971-72 RP LICE
DATA
AGE DISTRIBUTION
20 - 29
-
39
449
,
59
63 +
Ivoomplete
IOTA:
57
70
62
56 3918
302
DETERMINATION OF DEMAND FOR RH's BASED ON ADOPTED RATIOS
Hospitals
6 -
24 beds
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGOMES
Other TOTAL
Status Quo
Optimum Level
18.87
23.18
20.53
18.54
12.91
5.96
101.00
HIGHEST EDUCATIONAL PREPARATION
lio Degree
BSN
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
187
31 9 2 3 0
70
302
61.92
10.26
2.98
.66
.99
0.00
23.18
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School guru
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
186
15
14 7
13
31 5
16 015
30?
61.59
4.97
4.64
2.32
4.30
10.26
1.66
5.30
0.00
4.97
100.00
Ho. of RN's
Currently
Employed
(FTE)
No. of RN's
Required to
Achieve (FTE)
Optimum Values
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
PROJECTED RN SUPPLY PATTERN -- PRESENT
0AD
Local Graduates
284
Regional Retention Rate
.47
Local Graduates Retained
133
Inflow
11
14.
Total New Graduates
11
147
x
Activity Rate
.8810
.8810
TOTAL Projected
Additional Active
RN's by 1980
10
130
- 1980
BSN
2
CCP
cr,
C=7
17
17
.9111 15
7m"
16914
30
14 413
2114..
20
1?1 99
237
477Tr
47
27
39
49
768
308
115 17
13
35
36
524
Ex.
r+.1
155
267
RN's/100,000
,Population
Number of
RN's Re-
quired by
1980
Present
Number
Additional
of Active
RN's
RN's
Required
109
302
267
35
312
864
,267
597
Total Addi-
Projected
tional RN's
RN
Age
Required
Supply by
Surplus
.by
+Attrition
1980
-1980
=(Deficit)
67
102
155
53
67
664
155
(509)

ACTIVITY STATUS
REGION 15
1971-72.RII
DATA
AGE DISTRIBUTION
0
Active
764
73.39
20 - 29
123
'0.10
Inactive
_2I7
_26.61
30 - 39
137
17.93
Active:
40 - 49
229
29.97
Full-time
583
76.31
50 - 59
162
21.20
15-30 Hrs/Wk
91
11.91
60 +
67
C.77
Lass 15 Hrs/Wk
80
10.47
Incomplete
46
6.02
Incomplete
10
1.31
TOTAL
764
100.00
TOTAL
764
100.00
\\\
HIGHEST EDUCATIONAL PREPARATION
FIELD OF EMPLOYMENT
No Degree
BSN
Bacc. Other
HSN
.master's Other
Ph.D.
Incomplete
TOTAL
504
67
10 5 4 1
173
764
65.97
8.77
1.31
.65
.52
.13
22.64
100.00
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office ,Nurse
Other
Incomplete
TOTAL
421 20
22
4350
66
61 se 2
21
764
55.10
2.62
2.88
5.63
6.54
8.64
7.98
7.59
.26
2.75
100.00
=1.
WIN
-DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
No. of Addi-
No. of RN's
No. of RR's
tional RN's
Currently
Required to
Required to
EmfloTd
Achieve (FTE)
Achieve (FTE)
PROJECTED RN SUPPLY PATTERN -- PRESENT -
DAD
1980
BSN
Hospitals
Optimum Values
Local Graduates
x104
240*
624 beds
-12
RegiOnal Retention Rate
.66
.60*
25 -
49 beds
14
SO -
99 beds
45
Local Graduates Retained
69
144*
100 - 299 beds7..
346
300
565
Inflow
523*
59
5064
beds
TOTAL HOSPITALS
378
982
604
Total New Graduates
74
167*
59
Nursing Homo Nurses
18
T3T-
133
x
School Nurses
64
64
Activity Rate
.97
.97
.94
Office Nurses
52
61
9
Private Duty Nurses
32
51
19
TOTAL Projected
Public Health Nurses
47
-
63
16
Additional Active
-
SUB-TOTAL CATEGORIES
591
1372
RN's by 1980
72 *
162* *
55
Other
+
TOTAL
674
Status Quo
Optimum Level
RN's/100,000
Population
Number of
RN's Re-
quired by
'
1980
208
733
434
1529
Present
Number
of Active
RN's
Additional
_Required
*Estimate based on State Average
Total Addi-
tional RN's
Age
Required
Attrition
by 1980
Projected
RN
Supply by
Surplus
1980
(Deficit)
674
59
148
207
289
82
674
855
148
1003
289
(714)
289

REGION
16
1971-72 RN LICENSURE DATA
ACTIVITY STATUS
AGE DISTRIBUTION
HIGHEST EDUCATIONAL PREPARATION
FIELD OF EMPLOYMENT
0
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Incomplete
TOTAL
6,607
_2.389_
5,191
894
46557
6,607
73.44
26.56
78.57
13.53
7.04
.86
100.00
20 - 29
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
C
1,530
1,530
1,613
1,144
478
312
6,607
23.16
23.16
24.41
17.31
7.23
4.72
100.00
No Degree
BSN
Ilacc. Other
NSM
Master's Other
P4. D.
Incomplete
TO1AL
3,570
1,378
160
127
75 4
1,293
6.607
54.03
20.86
2.42
1.92
1.14
.06
19.57
100.00
Hospital
Nursing Home
Sch. of Msg.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
4,363
183
220
336
223
426
218
47918
141
6,607
66.04
2.77
3.33
5.09
3.38
6.45
3.30
7.25
.27
2.13
100.00
.11
WM
.=
OP
DETERMINATION
OF DEMAND FOR RN's
BASED ON ADOPTED RATIOS
C.
-a :Hospitals
cn
6 -
24 beds
25 -
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
500
beds
TOTAL HOSPITALS
Nursing Home Nurses
CAD
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
No. of RA's
Currently
Employed
UEDLL___
No. of RN's
Required to
Achieve (FTE)
Optimum Values
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optima Values
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
DAD
BSN
Local Graduates
Regional Retention Rate
Local Graduates Retained
2340
1558
Inflow
301
98
532
Total New Graduates
301
2438
2090
x
Activity Rate
.9678
.9678
.9264
TOTAL Projected
Additional Active
RN's by 1980
291
2359
1936
-4586
CC
P
C=
$-s
=1
3:2
3887
180
446
424
260
224
5421
-47
+8
5899
16
208
403
3070
914
2133
6-
2851
42428
211
109
237
310_
rip"
474
474
635
369
461
9287
Status Quo
Optimum Level
RN's/100,000
Population
255
402
Number of
RN's Re-
qui1980
red by
-
7196
11344
Present
Number
of Active
RN's
Additional
RN's
-Required
5899
1297
5899
5445
Total Addi-
tional RN's
* 44" IgV
Age
Attrition
1050
2347
1050
6495
Projected
RN
Supply by
Surplus
'4 1980
-(Deficit)
4586
2239
4586
(1909)

ACTIVITY STATUS
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/Wk
Incomplete
TOTAL
209
_78
162
30
16 1
209
72.82
22.18
77.51
14.35
7.66
.48
100.00
REGION
17
1971-72 RN LICENSURE DATA
AGE DISTRIBUTION
0
20 - 29
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
23-)
32--
64
45
26 19
209
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
No. of RN's
,Currently
IFTE)
Employed
NOspitals
6 -
24 beds
25 -
49 beds
50 -
99-beds
100 - 299 beds
300 - 499 beds
500
beds
TOTAL HOSPITALS
116
Nursing Home Nurses
15
School Nurses
7
Office Nurses
11
Private Duty Nurses
4
Public Health Nurses
SUB-TOTAL CATEGORIES
161
Other
+25
TOTAL
186
RN's/100,000
Population
Status Quo
146
OptimumLevel
417
11.00
15.31
30.62
21.53
12.44
9.09
100.00
HIGHEST EDUCATIONAL PREPARATION
Ho Degree
Bacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
134
25 5 0 9
44
209
64.11
11.96
2.39
0'00
.48
0.00
21.05
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
129
61.72
17
8.13
73.35
62.87
94.31
18
8.61
73.35
12
5.74
00.00
41.91
2Q9
ID0.00
No. of RH's
Required to
Achieve (FTE)
No. of Addi-
tional RN's
Required to
Achieve (FTE)
PROJECTED RN SUPPLY PATTERN -- PRESENT
AD
- 1980
1191
Optimum Values
Optimum Values
Local Graduates
23
Regional Retention Rate
47
91
Local Graduates Retained
173
Inflow
55
14
334
21879
Total New Graduates
x5
514
94
29
22
Activity Rate
.97
.97
.94
18
7
23
19
TOTAL Projected
28
20
Additional Active
RN's by 1980
55
+13
Number of
RN's Re-
quired by
1980
184
525
Present
Number
of Active
RN's
186
186
Additional
RN's
aRequired
(2)
339
Total Addi-
tional RN's
Age
Required
Attrition
by 1980
49
47
49
388
23
Projected
RN
Supply by
Surplus
1980
(Deficit)
2323
365)
I

INP
D.1
ma.
ACTIVITY STATUS
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 MrsPik
Incomplete
TOTAL
DETERMINATION
Hospitals
624 beds
25.-
49 beds
50 -
99 beds
100 - 299 beds
300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
SUB-TOTAL CATEGORIES
Other TOTAL
'2,668
1,J88_
REGION le
1971-72 RN LICENSJRE DATA
AGE DISTRIBUTION
69.19
20 - 29
3.0.81
30 - 39
40 - 49
50 - 59
60 +
Incomplete
TOTAL
2,136
80.06
316
11.84
185
6.93
31
1.16
2,668
100.00
OE
M
OF DEMAND FOR RN's
Nc. of Rh's
Currently
Employed
1494
154
157
126
: 88
155
2174
228
2402
AH's/100,000
Population
Status Quo
208
Optimum Level
348
529
560
636
552
273
118
2,668
BASED ON ADOPTED RATIOS
Ho. of RN's
Required to
Achieve (FTE)
Optimum Values
21
158
121
1013
805
599
2766
216
225
174
- 217
3915
Num0r of
RN's Re-
quired by
1980
2554
4273
19.83
20.99
23.84
20.69
10.23
4.42
100.00
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
Present
Number
of Active
RN's
2402
2402
1223
212
59
99
8662
1741
HI3HEST EDUCATIONAL PREPARATION
Ho Degree
BSI
Bacc. Other
MS4
Master's Other
Ph.D.
Incomplete
TOTAL
Additional
RN's
Required
1,600
59.97
468
17.54
59
2.21
49
1.84
33
1.24
6.22
453
16.98
2,668
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
1,665
176
129
118
166
163
33
141 969
2,668
PROJECTED RR SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
x
Regional Retention Rate
Local Graduates Retained
Inflow
Total New Graduates
x
Activity Rate
a
TOTAL Projected
Additional Active
RN's by 1980
Total Addi-
tional RN's
Age
Required
Attrition
by 1980
152
549
701
1871
549
2420
62.41
6.60
4.80
4.42
6.22
6.11
1.24
5.34
2.59
100.00
DAD
BSN
464
804
1782
.875
.869
(.509)(.560
406
699
935
32
63
166
438
762
1101
.97
.97
.94
425 +
739
+1035 m
2199
Projected
RN
Supply by
Surplus,
1980
(Deficit)
2199
1498
2199,.
(221)

0REGION
19
'ACTIVITY STATUS
AGE DISTRIBUTION1971-72 RN LICINSURE DATA
PREPARATION
et.
HIGHEST EDUCATIONAL
Active
112
80.00
20 - 29
32
28.57
no Degree
61
54.46
Inactive
-11.
_28_
20.00
30 - 39
34
30.36
BSN
23
20.54
Active:
-40 - 49
21
18.75
Bacc. Other
32.68
Full-time
100
89.29
50 - 59
12
10.71
MSN
32.68
15-30 Mrs/Mk
87.14
60
'
98.04
Master's Other
00.00
Less 15 Hrs/Wk
1.89
Incomplete
43.57
Ph.D.
00.00
Incomplete
32.68
TOTAL
112
100.00
Incomplete
22
19.64
TOTAL
112
100.00
TOTAL
112
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
48 3
11 021 23 0 0 6
112
DETERMINATI
OF DEMAND FONORNis BASED ON ADOPTED RATIOS
No. of Addi-
No. of RN's
No. of RN's
tional RN's
Currently
Required to
Required to
loyed
Achieve (FTE)
Achieve (FTE)
PROJECTED RN SUPPLY PATTERN -- PRESENT -
0AD
1980
8SM
E)
Optimum Values
eBAttmaillttE
Local Graduates
298
.=.1
1
Ch
Hospitals
6 -
24 beds
7Regional Retention Rate
.77
25 -
49 beds
SO -
99 beds
Local Graduates Retained
229
100 - 299 beds
117
300 - 499 beds
Inflow
59
23
500 *
beds
TOTAL HOSPITALS
Nursing Home Nurses
43 3
124
1117
81 15
Total New Graduates
x5
238
23
School Nurses
22
24
2Activity Rate
.97
.97
.94
Office Nurses
010
10
Private Duty Nurses
-Public Health Nurses
020
16
21
16 1
TOTAL Projected
Additional Active
SU8-TOTAL CATEGORIES
88
213
125
RN's by 1980
5+
231
+22
'
Other TOTAL
106
SUMO QUO
Optimum Level
RNis/100.000
Population
101
213
Number of
RN's Re-
quired by
1980
135
286
Present
Number
of Active
06
Additional
RN's
=Required
Total Addi-
tional RN's
Age
Required
Attrition
=by 1980
29
15
44
180
15
195
42.86
2.68
9.82
0.00
18.75
20.54
0.00
0.00
0.00
5.36
100.00
258
Projected
RN
Supply by
Surplus
1980
m(Deficit)
258
214.
258
63

ACTIVITY STATUSI
Active
Inactive
Active:
Full-time
15-30 Hrs/Wk
Less 15 Hrs/likit
Incomplete
TOTAL
1111
1=1.
REGION 20
1971-72 RN LICENSURE DATA
AGE DISTRIBUTION
I
737
73.33
20 - 29
131
17.77
288
Z0.67
30 - 39
148
20.08
40 - 49
185
25.10
596
80.87
50 - 59
149
20.22
89
12.08
60 +
96
13.03
38
5.16
Incomplete
28
3.80
14
1.90
TOTAL
737
100.00
'37
100.00
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
Hospitals
6 -
24 beds
plid,
25 -
49 beds
.4
50 -
99 beds
100 - 299 beds
44
300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office Nurses
Private Duty Nurses
Public Health Nurses
,SUB-TOTAL CATEGORIES
Other TOTAL
Status Quo
Optimum Level
No. of RN's
Currently
Employed
40223
64
37
24
42i
597
+--RI
667
Rte' s /100.000
Population
152
330
No. of RR's
Required to
Achieve (FTE)
Optimum Values
24
43
167
234
188
250
906
137-
97 74
69
87
1390
Number of
RN's Re-
quired by
1980
708
1537
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
Present
Number
of Active
RN's
C)7
667
504
134
33
3745 40
a
HIGHEST EDUCATIONAL PREPARATION
No Degree
BSN
eacc. Other
MSN
Master's Other
Ph.D.
Incomplete
TOTAL
472
64.04
71
9.63
17
2.31
5.68
7.95
00.00
165
22.39
737
100.00
FIELD OF EMPLOYMENT
0
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial' Nurse
Office Nurse
Other
Incomplete.
TOTAL
448
2633
32 50
66
14
41 1
26
737
PROJECTED RN SUPPLY PATTERN -- PRESENT - 1980
Local Graduates
Regional Retention Rate
Local4Graddates
Retained
Inflow
Total New Graduates
Activity Rate
TOTAL Projected
Additional Active
793
RN's by 1980
Additional
RN's
=Required
Age
Attrition
Total Addi-
tional RN's
Required
by 1980_
r.
DAD
BSN
665
.808
537
5153
32
5690
.94
.97
.97
.94
60.79
3.53
4.48
4.34
6.78.
8.96
1.90
5.56
.14
3.53
100.00
6+
669 +
30
a704
Projected
RN
Supply uy
- -
Surplus
1980
2(Deficit)
170
211
704
493
870
170
'1040
704
(336)

ACTIVITY STATUS I
Active
Inactive
Active:
Full-time
15-30 HrsfWk
Less 15 airs /Wk
Incomplete
TOTAL
=11
-
REGION
21
1971-72 RN LicinsuRE DATA
AGE DISTRIBUTION
eh
405
72.19
20 - 29
42
156_
21.81
30 - 39
85
40 - 49
96
326
80.49
50 - 59
93
39
9.63
60 +
67
32
7.90
Incomplete
22
81.98
TOTAL
405
405
100.00
DETERMINATION OF DEMAND FOR RN's BASED ON ADOPTED RATIOS
Hospitals
6 -
24 beds
25 -
49 beds
SO -
99 beds
100 - 299 beds
`300 - 499 beds
500 +
beds
TOTAL HOSPITALS
Nursing Home Nurses
School Nurses
Office,Nurses
Private 04ty Nurses
Public Health Nurse*
SUB-TOTAL CATEGORIES
Other TOTAL
'Status Quo
Optimum Level
No. of RN's
Currently
Employed
(FTE)
160
3074
13
14
43
134
+ -sr
RN's/100,000
Population
105
256
No. of RN's
Required to
Achieve (FTE)
Optimum Values
14
53
449
._
516
9787
43
54
67
864
10.37
20.99
23.70
22.96
16.54
5.43
100.00
No. of Addi-
tional RN's
Required to
Achieve (FTE)
Optimum Values
Number of
Present
RN's Re-
Number
quired by
of'Active
1980
,
RN's
356
67 13
30
40
24
530
HIGHEST EDUCATIONAL PREPARATION
Ho Degree
BS4
Bacc. Other
it)4
Master's Other
Pk. O.
Incomplete
TOTAL
Additional
RN's
aRequired
226
55 6 8 2 0
108
405
55.80
13.58
1.48
1.98
.49
0.00
26.67
100.00
FIELD OF EMPLOYMENT
Hospital
Nursing Home
Sch. of Nsq.
Private Duty
Public Health
School Nurse
Industrial Nurse
Office Nurse
Other
Incomplete
TOTAL
178
43.95
34
8.40
19
4.69
19
4.69
46
11.36
77
19.01
2:49
14
3.46
1.25
15
3.70
4Q5
10.00
PROJECTED RN SUPPLY PAWERN -- PRESENT
1980
DAD
BSN
610
Local Graduates
x
Regional Retention Rate
Local Graduates Retained
4
Inflow
Total New Graduates
x
Activity Rate
TOTAL Projected
Additional Active
RN's by 1980
Total Addi-
tional RN's
Age
Required,
Attrition
=by 1980
312
366
(54)
114
60
761
366
395
114
509
680
488
55
41
5493
41
.97
:97
.94
5+
478 *
39
` 522
F.-ojected
RN
Supply by
Surplus
1980
(Deficit)
522
462
522
13

APPENDIX B
175

4 BESI COPY AVAiLABLE
I II II&ITV U1IL%1A 101 P*flI01) IT PV1t%I .jIiiI,
1 3$IMTI t3$ IIJISIOG PJ(CT
1. OUt ,___ (1) 0.1, 1. 0.0*1_AL It*TWt (I) $I.$r(3) P1 _ç2) 0.,rt.d_()) W1.v.d_(*) Olaore.d
.3. ,I
3. Old p.. covpl.ta S VscS1lo.sl Ni,.).0pts before ..r.1l.. *0 OIl 1.0.
4. ., .0 àlidro. prs,t..PS.f.( Iii
._(1)T.. ___(2)0.
4. 0* 1h. apse.. pr.,(d.d. plo... lodte.(. the wir of aSudustlo. Ores sod type.1 pree sO id p0o hee. sp*si.d. I. (I. Spec.. 0. the rl$hc plo... ta.dlc.t.psS( 0.3.1 0...1 .tto.d.4.
is)., to 0.r.I.$12!! OQ..oN iI_m1 0d i P.o. 4!iLt
n).'$ "_ _0 0 0 0 0_______00000
(..io.i,.*. *$_ ____________ 0 0 0 0 0__0 0 0 0 0
- 0 0 0 0 0P. 0*... tid...1lo. ho. yo.t 11..i peo., .5pr.*lo.tilp 000 SillY
be.. p.. b.. .011.. ls o.,si..T ?..r.
S. N.t I. t0. h&$h..t 0%c.1Iao.I t.iei ye. plc. is .Itil,)
_C%) Ipl beOtil...,,.00 __0) Phi(2) £i.o.1.t. 0r.. _,,(i) is.t.r1.
0. 2! p.. plo. I. .1111. II. 4o.w.1 1.41.11.0 0..... I. 2!tIa?
_(i)T.. (2)3$
IL is.t Is peor pe.io.t p.iIIIi.?
_____(t) £4.i.1.t,.I., p. L..I.1..1 _O) seed 5.r.. .r Asalsisid
_12) iolteu( _(S) Cues.) D.0p .1 $1.11
(31 aeeIto.r ii AsMotost _(7) 0uI..r 'I).... .p..iIy)
_.___0) 2!seust.1
Li. TI.... t.4tc.t. ib. 1.o.tl.. .0 p.., first tes p.sitiS.S IS i. -
t.1lo.1e0 0 0
Clip ..tp 01.10
11, 0.S..I sspls,e.i.1________ U. Sot. .1 ,o.tiq.ilo. -S'eib Veer issib bier
14. V.a. . .0 Ni O0% Phesi p. 00.1. ii..? _(1)Y,. _(fla.
10. 0.1 0.1. p..lIl.. . _.) e. S.IIIM£ Sàllo mull us C0%..Itp O.i.sp_(3) %.p (.p.tttp)
tO. Io..o. I.. r.50..tl.. - 0 0
17. 0 0 0 0Cu-il
ii. S.!. .1 1.ee.e_________ tO. 2!i. .0 pe.heeiIo._________uh is., 155i11 To.t
Se. u.s. pee . if il. Aused 5.cri it (his Ito.? _(1).. _C2)0.SI. U.S ibis pillil.. It. __,_(I) As I tit-,o.ul eHl
A llu N..liI. p. Ce11p £s..sp_03) Gibes (hp.slIp) _______________________________
03, 0..s.. (.1 reat.t1.u______________________________________ 0 013. P1.... p.o.ld. the (.11.1.. l.Iid%.il... 1u the poor. Indtt.ie4.
LU)
107)
"I10Th
"5,
P.r I.tb P.,) ha. tls l'io.u.t 1 Ptao1eLet J.t. Is. Ce.3p. o. yer Ipts..sui. P5IlTI.S 1U 0'0.5T tlt.d to *
Sleited. it.. £1) 0.p. sO L,.I. elite0 To. 50.5 ?po. .t I Lieu0 00k-LOot LII to.c.tIa. bios e5 the Wet.. I.pI.'-.d 10. r..,tto era- 00rl
51.1.. 1. I. 15,1.1. TI. If '00T & hhtl.'lll. I Ie 11.15.. tI. ..?
esIsh 1.. iso tialJe.*e , t.,t.T105 II.uLty J.Dlr)as.0.. 14.4 iae&4.d L loi,tl.. L. 3*. D.
3.0111.. III.0,00... *.Msat.,'.
______ ______ _________ . 2... .2... __________
I
34. I. y 011.1 .o.lii. ii S. 0.0. did ,e..r Jol t,..it. ye.. I. p.r?.rv pouted.,..SI ro.pso.iblllci.. Oar idilcI ,o.r id.c.tio. bed o.t p1.051.4 pSIP
IS. £0%1.$ 5 '.tlr,.t as. .1 43. plo.ue iudic.i. h.i.v II. ..b.i .1 p..,. es.
eso.ct 1$ ha cl.vUI.0 II .*ch 0.1.05,7.
IS. U po. .Io.eeid I.e to the pro,5.0 qo.stL.',, p..... ap.rIlp the o.)eS .i .3 1.1. ii 1.1,.
S.Ssq1.ao .1 0.1501*10. ar Ohith ye.. 1.11 ...prop.I.d. .
(I) (1) 1... IbM h.l1.tia._______________I.. U) Nell-il.. (0.) LAss.)..
35. S..ts the peal (lea peer. ha,. pe. ø.cMt ..i444 .110 ci m,..r,tos4 .1.0%(I) y (2) U.
3$. US ye.. Cccl 1000 pAss b..& ffifhI51 .0.1.11.. Ps y.o.&i.4 30, vItO it
4011(11,, 0.110, tsr aup ra..j... to. a,. asriertly o..'le t. .p..lp 1. pius 77. *11001.5 001s) i.'I011IaCiN .0 eh....çu. sep.01. 1 * p.fl&t.ulat l.IIlp.StdS
p.1.11.1 .0 aei.Is? (I) (2) e beilici 5t'ITtSI p,.(IeiIM.l ..ral., .400511.. I. id...a.ip
Ni So.
. U y ...ats4 0.. pr..Io.s ossija. "Yea'. ple.p. *.flf *. this. cs..i4
a4.11Si.. a... (s) .0 a 4ip ,o.cia ;. t..t1o. I. 0)001.. ye0Iit0%,__t))To. _VI)U.
£0. hasitie. b.$1id1115 (7)0.(be .1 .. prto. ta I. pealil.S.? _(I)V.a
(a) .1. S.l peer.. 0. I..t ii ha5La.il5 pItlo.If _1)V..N. S a.0%. 4. ye. fast a.o.,10ui. 1. lb. laub if etlll..tl*e .0 ta 0.11111..?
U 5. a. af 0.. abe... olo. she.0.. 4. pee fo.I .rc asaldf
N. N00 5,lfi. ibess. Is ps..r proseet 30 011.001.. e..I4 0000) po. Is .511 IS. 0(410% *a..stm. 0,.s 1o.tao.eiSe
___ .to 4011 it..1 1. a $105111 4ro.f2! 0. o. plo. 05 p.n1.tpa 1. .5. Two .. 4....t.4I,.* .v47
2! , .or,..t p5.111... as. ,.L. sI0.d is so, 4r 'sAtvp'lei sty. .0 0%lq Seelsolit Iøi.1il00 P,s... (0%P)f- 'pro.t4ia lo,s.edf h..iil ..r.f (1) Ta. (2)0.
_(1) U.. _ft) Uid.e14d3$. U 0(p. p*ss.. 1.51.10. _(1> 5. _4I) 5.0.111.5 pith Sb. p.o,r..
00. 4.. . Is late. *4 .e.sy ...U..( idossois. I. T.*s*4
N. 3$to.a Nil.. v.0.4 pso pa.fei 10 ee.1L.. Is. _jt) Sorat eaCh, (1...tO.. INO pera.asP _(l) 0.. (2) 5. _O) .1iddid
___(I) Orb.. 0.101.. (3$%.1 0%. p.tassa) 40. 1d b'i o.0 lIkely 0. 0t1 1.0 0%sp. IllS., yore l..,I.peS
.ps0.l1S.II7 Is. $1alo. .4 i parsis.).. type .1 .ie p,sssos? 00.
13. 2! Sb, ..* .. its. )j,. pleaS. 01... . check Is 10. aca .1 the )sO 5t155 d&p1. *)
10 050,0. s.rb, II the 0.10% I. the pisuse plat. a sOath 0.114.Ni %Sel.5 to ,S(.S I. o.10 11 slue. 05.1... ____4l) 0. ......0)
I IETTI% W0% I UTTIN _Tico.())0.0 b.to.l (23-lOS bid.) (1) 1.11 h..p(t.* (23.100 balu)(23'S.).. b.o,lt.I (100.0% bell) (2) 0.41.. isa.lisI (t00.3$$ Ia4I)
(2)L.S ..dla.l ...a.r (3) le dlIa) et3o.i.. heo. - 3$)
Ø)C.ett, Is..Ish Asset05 (2) ?11, 00*5105
.(I1i health. NI .s..) (.111. 0.0010., 0%. all.)
Ø)I2!a.sLel oath. 01 N.suttI solOist
- (2)0%e. (e.itrp) - '; 010., spiel(s)
3$. U _ it. o.i0%Iy .saO.. Is Ph. ..s. .e jo. so.sis.( .
Ni5, Ni N. 0.oar. 15so ps I.o. hL.o, 0. .0.,. a....' 4
3
5.-.
*
173

BEST coPy AVAILABLESNI! I4NI *UTIIa.SN
Is r$. si.u.
V1ds4, Ihsr..
- S' Si0$ IS IIIa.t Is sI.s.IfI..t$..7 Iii yss' ssssist )rd ysoe stM
NO - 11.4.01 ¼0 p..v sNO
4. .Jusi ,.sII..a tOss SOS .000.900 59 SOs it.i 5.01115 *'I
515, sy ,aei.0$ss ,..,i., IrOs Uus sOpsalisosI OSc$0rsosONi NI. NI$isv *9 SOS lssoltp is. I$bfIiy 904 sIL.4s.I 9s*11ia1N a. wss;NIsi .s .9 sos IlsONie io.Iv,s. $1... 5M5 st.dy0.5 $000.1. 0.55. br..d va..sI 9sot.,s us irs 11.15100 usa .ussIus.
0. lOs i!Ii.lu. çI15A4 j 431 .rSASi5u.. 10
a. ossIsos piNs. IN f.TIso.5 stst.M 45 lOS de9$01i1
NO 1s90 ;.eviIgp, N .0.4 1. lOis $1.4,. yours N Ni susaiss.Usr.l W ocOSSI *9 os,sIsNiso oil to a i4plsN.1 s i.,r... ThIsj.4I.lSIus lasisiss sOs ikl1.sapOy.V sOS scn..l, g ii.sI.$ Iro.-..t*9 Nuts.. soiNis .1 pe.s.lsils. sI 1.vf 5 Sl.NuS. .la*101ikip
sOjislioss is slI.$*.I iyprI.i*.i is. svsIwotIus p.usrsa. Tb.1.91*1110.. so .1.1.1 f .L sooly 5. to. suslIsy .9 SOS 90.111*1...INI. sOliS sos pro Ti. .91,. CIi0.I.0 .00W. 559 ** 4 s?sNsIIS$S- .Aisi.s .9 55. 9scv$sy .r IlvisMs.
_- TITU
I. iSis sours. Osus iI..vl 4.9usd. IMSI fit N0(5IV.0 Vsti
. Tb. ass's... iuNIu v.a NI. Is.osoJ.'li .........,Yss NS. INS s.ssr iuss ii. Ti. -4. 1.55 slIsls.I s90sr1ss. V..
1 NJ.sei..s itsi -
. OSusI.psO soil raly by Vacuity .V.e. too cs.rss biso- S. $l.. S Ills 55.90.,).. III. £0.?). P?90?0.5Oi. OSusl.psd sativsly by VacuIty asi 11.90.111
3. NO sisiasi Is si,o 0. 1.5.190 sIs l .bjaciIvsi f cIis$isI,Iisso a 541)510. 10 tOss. sitabIllOsi Is tOs .05900 0.111.0.
Vs N
S. N yuu vsui,s ss .sdi,1u.l .v.$..ti .9 ys.r acOlso.._S 59111( *$S1IVSS by a Vac.Iiy .v)
-a-I-I). 9 SOs 50.50.5 15 SOlO 0. 5.5 - '
slss Nu9IN.
505 N (Plassi ipssly soplus
&1r.st s01 soa.d .s.4 I. ISIS SiWOS SI
____s. $0mtuts0. 100w dIscus1Is... Ofssaeisslsos , idsi...,
___4. NO1*-SIassi NOi. (sap.., .110., .IINi, T.V3
____.,._V_ I_uS ship
__9. Tbas*sssls,S.st (sousi9vI.____..
II, N. 55510115 solNi 10115$. .0.5 V94, 90q Is Nb 155.59a.VSS III
IS. $., s..It Is, usi. a.ro. usillas.
. 50.0.1St IsoiSsoS. ki.roI ..a.sOa
_s. N r.p.I.v IsoSONO___.4. SIblI.y.pbyr59.'umsss soly____. *11551110
$3. NIl 1.5115W Vsl.a..s.. fit 451S vi.0
__0. At. 90 5. 4.1. .455 sa. 90f59ss 9905)0.90.15 Ii a.NIl slu. tOS
.01_sb. l51in .9 rsiu.a.. . sNO 4av S jsuts ala
_s. VIS. 0101.0$ Sib 1.5.91.00...r. f.I.isO so sO.s,p 51.. rvasily
51 1* 1110..-, S$I.INi u$..1. Is .59VIsIai,a 50 $N 0. a.ssv ,JS....IJ0. Ni
a.Ip u5..i.p asSOt vsollick soiluiI..-II. I? orsi . ãl. a..Ias "', 10.1 Ø1f$0 r
IpilI.1$ rl.s 1. Is.I 14 Iapaa. lbs IPWI*9
a. i_u - 15.1.0 4 a. .*9 slialsal I? N. .1 --u -1_1NO 174-
p. _ ,,i.,i N ass 551155011i1510. .9 v SO4NS .4i94, 01.s'i.,'5s __N
I. ThIs NuVs.. ilu.ib .11 51.5 spplp)
.. I. i.II s,i .dII.i. 5 Iiisai ._ssSs..I Vr.#0___b. Is IN.N.ltb Ilitis OsI?IM 510.10.Ity Iri.
soil 5 Os soil
_.__S. c191s.iiy Sills_d. II N .o..Ily .ft,qti 5 sIls,sl S. eMr *0.5*59*9 0. s5I*.I..
_s. 0.5 5 *S..rly .0M,sti p..... 4,. iu, .-,i*l .5 0.4*sr1OsS.r ii., Is 5*, 590's. (asi.l..i __J
7. Os SIt rso.iuso i.?s.uMl so sliss OslO.. 4,5.._sOh.., as.4*,. pso..
____s. 159 0. ssOi', s..r.. s Os 0psIss4.*9 SM 0.S.0. 1.. sasS usi 4,5 555's t0. so4; Ns,
1. 5 Sy b..Is
5. so lr,.0.I.e h.ais__.. sr laesslSy)
S. 5.0.1.. sod u_sc_s 0.4w I.o.0 .44 0.0
__.. '1.. I.11 .ussIyøs SIOSIIISII II M 555 150.111.
1. Or. ISOussolly .1055.1 .ssssdSy .S 0..0.IUSIPIS..
Ny I. W.1 Os r.sou, *9 a s.Iariiv .9 ssop. s. _sssoIs
__a. 5.50. 5 Os.' i.r* 5U5155 is IsS Isgill
S. 5.505 501.f f_sr s.1s. I. y.atN 1.1.41s. is .ti.li.cy .5 Is
SO. Ia *0. .sys. y. 5b.r uss .04.1 a,. .si No .01.5, Nycsol .lu.,ia Os.. b...9
is N if V... is.s. .p..Sfy.
II. Os soso.s .9 Sd. .sys. pus.. pri.u4 .,o..O, i.i
NV5115 555551_N. pI0..l.15 .W SVS1U1IIi.V__b. Si,iis. .t_s s.d ..d.NI tr..t..M .9 s_sill's i.ISSI_s
Os N 505. SSIS u I5f 55 SIISIS PfSS.IS.05_____a. A 1055.050 .0.4.111.. .5 .. 0. ssdS V
s. SsMr(.pssIly)
5$. 0. *0* .sc.., SI 00.1.155.4 s_sIlls .10.4...9 11.1.s?. SOsiSill,N 151 l*lSV 11.0 11151.50 _s-_s.Ips .s_ss I, '0.0
OsOs Oil 0.00.4.
S. Os .0115 rpssoS. SN Sals_stIsoV
0. S i_s5Si. is asS 9.00.0.4. NI Os 5 I 554,
rssioI. Os Is
4.
S
SO. 'VIsOs S. Os .il.4.l $055455 Is Ni. 551955 9555 555 .000*9 0. I.IIi. .at.s.i..5
5 1. Is,5r 1, is IS. 1I.,. 'as at .11 tIassissIdwisr 45 .54 50.575 is to. 59550.5 45 .,.iiNi,
0. illS, by p55490. iii.I. I_sruisis. I. pvIOsISy Sparas iaN i0 Nyl *lIa4,.l- .410 455,0.5.,
____4. 0.9
154ss4S*9 Nyf 551.4551 p.'firus.. I. ISIS 0.95. Is 1.5.1 0.Iiss . I. 0. 1.. 94, .11 500
- Q WiI(so 0..*taS 0.1's 0I 0. Ia.traSs,g 101...I 005,55509 .441_s sI U_VVNiL5.- 0 Nil., ii .01.5.0.5 .5 5 11.1*9 110.1154 *ks1lass
.50000,5., 0s.r by so s,a1.sI.V0 S. psauss-.is. os..o p
0 y.dssi 1tI IS Is.t_s 9_s isVI NI$4 I. Osalso s yso _ss ...ip_s_ 0 (u...i.v)
SO. I. a. ps4a Nysila plpsss _sI 0. .1.4,.. _sN 05. 9....,. iS, u.ss.l psI. I. asa_s*ap .11.9.54soul-si-.
a.I fI .00 so_s *9 sosI00Ia *9 iI_sp 1. *15 0.05
_s. 0,110. NJsosi.s 5.1.V 5 5155. USisy 55001_s. ScsI ..;l_s
I. Sl-s. ps.iIs4,seisoS. 90551.4 ScojOso I5y)________________
SO. NO, Is_s I. No 0.57.. V
a. N. 0_sits _slI$s ojsoti_s0. 0905 SsIN Nat 5.551000590.504
9
177
1.
a

OPIJI $UIflT OF IINS IDICATIOF AND UT*LIZATI
I. II T ttlCs (I) tolo (2) psrtw.rVIpU) you IN*tof Of N%.C.I _)
[ Typo ot pr.ctics or osc..sty
Ns.P Of yelfi IN ac?v$ pric?.c )..g.. j or jj)0 .DI . ilIty to oPlidI y
. Fop.atii If tI tton IN .Pl(CN 7 prsct.cs:
(ii too moo .00O 4) 00.000 -- 4,,4 = () 300.000 -= U) OOQ 4.44$ IS) IO0000 or
4. ior Ut ball Ii oodi of tM 0001 tail to ufli yOi tot OrqMly pe.c?Ic,
Ii) II) Ic) log. iJjor .2_jJ)
7. Uto) (I tOs aw.r5. air øt Miirl por .to* that yo' owe..) y Ia14 In tOO%MS.ttsi? (.4.. J j or 9- j)
S. If yaw Sri c..rro.ily sOlvy tn 'w of Th following octi,)tI.l (or tows btoaUNIS tto 4St Ito ysi's). p1.555 ?CS a cMcPl (/) i.Th. biail ?ø tM loft
opt*oo wlt41I UplisS
(I) ,sscPl clsfl.I for pefc)ob.1Al tng tv40004 .1 .spjI.r baili(2) IsacS cluwa for f.P.'* on a roçg(Ir DliiiI)) .stosr of $ ifPs. i s.tere. ccl Or ititsoido .1001 for nwrooa(4) . posr4 or .5vlOfy it?SS o a sc000i f owning(7) v of i ttuo casr.i.4 vi to n..arsi fig soi.cot ion (OtIISr toss
44) w'r at a I?.?. or local t?to. conoorrs.i wtti to. gtiti lfiwiris,
(7) onion (pilliS ,p.clP,)
4. 10iot on flu usJor fwnc?Ioni of tU °"M Ia c.ntofly SiplOyalIN vowr .fflcs?
r Ow0
115 r,I
I U (C)
LI___ 04. to . penl ly lwPsrvi.w tb uiiir100 to I. ls4 lo yawn of low? (I) yea
(2) to
ii 00p lay o to I i?.rsd .rM In yawn ff I ow. 4w yaw vo.I ty Mr Ii awoso aiDs'to 5MM 40 tofOS
II) . (2) to
5, t c,,r pat.,Ii e. to a pr .,on..i rwrr.,nn t*s...nI ,..I...ni I 11401 iilS or 1.1.. 41 p0 (001 V.5. StowlI 50 toIl 'SI1
_(I)yo. (2)ns
4. a? of's tM toot ItoOrtoot 41arsc'oriotics or s.al if cation; vOidsp yes lass fsr
m OFF;cI IL in A P.SL , a PCWITAL DIVISIGI
f: £J3I (C)
cJcJi.20. Ito? 4r tOo rSC WNCT.ON$ wt.CIs ifloiIO SI oaoC?od of nVS.; willi
0041 .1 t tIl lowing Ila.ofsIs IvsiIlI I)
____________ IN A toY$àCi41$ QV1i IN A ISPI?A& SLTTI(
2 0 (a) L.Y.L
. riIi U P) La. - A.D.
a ri; i L_.i c)LL-DipI1 ri
U_i dl L*. 5.5.
.1 Li. - _________________
2. yew visSily 5110w 'ha awcatI.ial laval f N.M.'i altO wN y. awIiitIye. i 154 SOIbtoi iSt?eN9t II) ypo (ii as
(f 7.5 aoI_If-_0 5V to $54 iO III 5l 70w lullS IS 5 155 145Utioflol 1to1
(7) doP.o', any lit (orusco
. sil osrasi to ragslrw to baa.. apocif,od ..' .f cootiowlag a0wChtiOo'a or to ro ma.r 1.41055?
II) yas IS) as
ye pi as ril..0 tito .ini pay fur ito uO 70SV Sf0.05 IS øttIiiltoo
(U (2) to
IS. to $4i,!e fOot tol(eaI twnas 14 ovnsia, tsou c.v'd piof It 5,£ '!° 41) ol.i Ill tol 41*., iye (a Ia, pItboor
_IIlye _l*k.as I 1 17
WI- Ip
2. Plooto IndiaN In ff's I (On owns., o' lis.riat en, 05CR category or4lyesI. yawn sOt low. IN oIiasl II p1.51. nasa?. Ills nor ifs saco cat.yeyIt yaw .Li *a!* f jt .j, mo, lvi
1 II
QIT)Y OPLOV F1N TO £I).OV
- - - (a) p Son; I tI10t (orasl NIIV*Ia, o41000$to
th) 1.1000501 VoCSti.1al Ngr
-- Ic) N.M. - Olpbon. gracta
(1) N.M. AulclI?s togr.. 4r511J55
- _ (a) N.M. SacaIawrsste ysIwsts
If) N.M. - Ms;tor'a gro r Nw5 Pnactl-tIt prporor ion
I). Iltolo fbi. ptot too ysOrl. Na,. yaw .spI.yac ._ VIIVS15 In y' .ft as aMto. Sal to provliui aiupsnlsnc. as an N.M.?
_(I) ye; _IZ)aoIt yaw oIboosrs4 05°. p10015 0bhp IS 4s.ss?boo IS. if s° piasas -.
stians (4 and IS.
4. .5? typo of V,tossI.osl pMyao Sad tOo Mo ya*aa$s toueistW?
(I) Dip l (3) toalosavts(2) Auocla$e gr. (4) Don't 000w
7. 5.; I? n000uufy ton VOw 15 ?..CIl liii 1110 9tSIVS?S 0%iy skill; visids yaw taitShould Naoi bass Issnisd IN NursiNg SchoOl? (I) yos _(2) to
if yoo plasM pp.cify
is. to yew toot tOot gradsoutos of any pa'tICwISn lyon of N.M. r'oo Oipl,or 4511.) 55 55D51' n1fr55, to goulSrSl lOON ge.lvO?Sf at a'Mr
'70.. Of YO4IIto?
_(I)yga (?Ito
If yso pboos spscl fy Ills typo of prograo SM 0701.10 iS vIsit a.V;sO flit typo .t ptsqron or. lit tenant.
IS. Do yaw pay a saisny liffonatlal for slsiStitoII oval tO Ito II$W,S 5.0.54iay Urn p'r off low?
_(i)yeg _(V..4
77. PIO.IIO INlicibo 41141 ty,s of 'I.,. nas5tU 'jn. fsa s; tost sUsctia. In 0015.1 sto Ml asia, woos. it tusIlOa? totoral ca$oSoriaS ,btous$1. 41.41 van lION wu oUtdo
NO*0. DIP. 5.5. OpiMiow
JcD CD D giving ply;iCaI cars Oil 7.r04110105 ta...70Nt proco4wrol
1" J J D CD (5) .00uglng a paIls.? cons livisbto
0 c 0 Ic) scopaliha, d$s.apl ho potISfits' pondlti IruqwIr. .ttootIss
0 0 C) 0 (1) casIno alIbi ato,IatoI nails of pI?I.1,S ato
C) C) C) .0 I.) providing potlont idia,C) o () () rgotscy lItIJotiofuS
C.) c C () _______________________
20. to you. foil mat as hofpI taIl and/or n.arli.g la ii, yawn was pfowbd. I40O'li0g cat's lIsa' aftuoraT
_ll)yes _(2).sS
to liii 5.1 of 5541 aØbtoIf 0ya0 plasas -5.10w 41141 is a
(a) maIlabilIty of vadsrn fachlitlol SM poulpasat
0 ooa oupunluosad .-jass (v'sgl'dl005 50 lumot.sol towel)
plIIootuy aol odololItritiva ability 4011,551St 40
(4) $150 sO patbooP IIvI.booa
C) Cu) 410W' atiatiIi ions' .4 LI. ot.ff
If) lasor tIN ii )41 tws
iou labIlity 40 IINISIVO 0505 its .1* spaclIblyaofs$54 .t.f 0
(5) u0 (p1.... .po,l Py)
5M. I. 40l pfo. na'S IMoS fiC$Ore 41141 70w 4104104 iscorStal 41.win ii,,ao.. Ii mf Itoasbag iswsbag cur.. will 5Ø, f54 asat IssnooI.Pl rook 4MW 0 II41rI 41141 tIioC pl Ills StSlaM to 15. nlØt sO °.'*4 sina1.
178

IL Please ladles% by plectra, check in the circle (91 it you approve or Oise,-
Ontive at sally A.M.'s la physicians' offices to per ora the tailoring '..A4riana;
0000
0
011N ogre
00000
0
r
IS) *eke albeit% hilltariell
(10 ide_health screening procedures
(el counsel with edition's about their treetrant regiorn,,heoito aeintenesco, or rehabilitation tochnieues
refer Seionts to community resource' that 'avid awseppertits of your cam and assist with health problems
(6)
(4) r.4%4 f4Y.a (SITS te ClIOCK or routine evakiwitiOn Of;at.ente. atat.:* such as diet. dressing change'. BP's.ti4c.44 none osomfoont problems (0110o1AVO01,41TOI-,v.fw. OTC.
(1.) c.oul torching for Such patients 44 414041,(CS,e.;odiont parOMIS, &sputa's. tete.
2t). iMk11d rewaensider retereino :Asian's with certain nursing or health norms to or
loSapendest R.I.. Practitioner rich 0 Ralitor's or Ph.D. in harking)
a.
II) yes (2) no Jr
If °VIPS", 0Pat typo Of Problems noble yow consieor for roforesi?
imig.dmImM
I* the *bort below. pima@ indicate by piecing e chock in the circle 1(:)1 which
type *I R.N. ormItarra you teei is belt prepared to veer(' In tho job sittings 14104.
Operating inoriOnCy Intensive Public InforvICO OnySiCione
MOOD MOM Cure Health Vorcetion Officio
Ammiclato Degree
041/00
,coca laureate
(a) 011) IC) (4) (0) II)0 0 0 0 0 00 0 0 0 0 00 0 0 0 0 010 year egliC, is it earl 4,,f(Cmit to ti.1 O.N. positions in :
III hospital"
12) ertSiCiale ett.crp
(31 other
41
BEST COPY AVAILABLE
6
To your anewledoe. I* Stara is esertage of R.N.1e Is year arise
II) yes (2) no
If "yes ". (a) what type R.N. la
OD ItIET USE
o SO NOT uSE
In greatest foam° liS/Diphas(21 A.D.(21 O.S.M.
of last op you lees would be the oast effective way to Salve this
hurl log otorress In pa area)
AM
M. What charges do you are noodeol In nursing 'cue:trios toiopr000 ire duality orOtoligiOnal norlitri precrice?
The staff of the Nursing Project rest:ass that It is Inpelisible to cover all the cur-rent issues at nursing osvcation and OilitatiOr pattern; Ina 4u4StiOnnairo of thistypo, it you hove opisions or suggestions stout et:rein/1i topics the* were net spec.t.
icolly mentioned or if you wish to 01140rais on topics that see inch/Odd. ad Waldappreciate your OWIllents.
176179

REST COPY AVAILABLE
MeV or LICEMS10 VOCATICMAL NURSESConductod Sy
1St 00121101$0(mC 4041O0 - NURSING MAC,
PISMO plop check (/) In the Oppreprieft blenS.
1. Son: (I) Mele
(2) Fenol
I. Wits! status:
(I) Single
(21 Married(31 Widowed(4) Olvercod
S. mention of L.Y.N. pOogrem from tonic",
1E141111.M.
Monty -Stets
4. Year of greduation
7. Ville In WOW' L.V.N. prellr110 did you r0001,0u
YouDDe Not Use
3.
46
ago: I.
2.
3.
stipend?ioan?
11 Yes (2) No
Number of enliven wilierIS
(1) Yee (21 NeacholarshIp? ill Yes (21 NO
Lilt your re names, far daddies to our on R.M. proem.
Mho did you choose "as prticuier type Of R.N. program?
VS. Aro yew surrontiv enrolled In a coliego progrno of any typo? (2Nos
If "you ". pleat pecify
1111. If you are rm currently enrolled In collate, please indicate *len of the'.hewing choice, lost worts*, your present educasienei plena,
III No 7erthar fermi oloctlensi programs
(2) Plan to enter en R.N. program to obtain a Itlylpio 13 yrs.)
(31 Pisa to enter an A.N. program to obtain in Assecletit Desiree 12 yrs.)
(4) Plan to doter in R.N. program to obtain a thedsco geggi (4 yrs.)
15) elan to enter IA Junior College but vat osier In Nosing
IS) Plop to enter OnivorsIty but not =Joe in nursing
Si.
(A. O'er Iola's() innitcIfy)
Mel Is your growl worst edneetios level/
Veers of Web Scainel dated (dirclo Itme appreprIsto awls" fi4 Sere) 1 2 5 4
Old you meolue s dIplowe by
III e;opletiog 4 Veen of Nigh Schnell
(21 passing this 061.0.?
IL
IWO eM COltese pa0 tad (Weld' the epproprfirlo isobar of yeert)
met 1e Mils MOW odudelismel hoot you plea to attain/
1 2 3 4
ill Olga Scoop' 01.1400
(2) Diplom la likwolOg
(32 doseslete °spree
114) Seloelsorsege Owes
3
151 Motors tlegrOe
(GI Oesierete
(i) Other (please specify)
s. The of L.V.N. program Ironwhich you grrdooted
III Public School Program
12) Noapitol Operated
(31 Junior College
141 Qualified based on conyplotion An
in M.N. p A--
IS) Other (please specify)
1. An you ctrwt:,
(11 Kline
Inensivni
(31 retired?
10. If *vim. how iong hove ow Isomemployed
(a) In your ;room, position? __yrs.
lb) In your previous penmen? __yrs.
(e) tot.' years of employment os inL.V.N.?
11.. What Is your present, 91614 of reloYsont 7
(I) Nespltel 14) Musts Duty
(2) Nursing Noss (51 Other (pleas specify)
13) Office Nurse
12. In tbs space beside ouch typihot Joe. eleene write the number of roar, ofegrience you have hid In That position. If you here newer eorksg In yks
ore., write "0'.
11) thispltl Staff (41 Privet' OutY
1012) Nursing Nolo Staff (3) Other (plods specify)
(3) Office Mums
I]. Pismo chock loch of the stahmonts which Influenced your decision to enter emL.V.N. proven.
(1) To find out i1 I liked nursing
(21 Only type of nursing mailable In my community
131 ass not femiller with other type* of nursing proem's
Id) Old not vent to spend more than one year In school
(5) Other (pis explain)
II. Are you currently enroll/to In an R.N. program of any type
(1) Yee If 'yrs". dot type! 11 Diplome
(2) No (2) A0Ociate Opole
(3) eoccoleureety
2
IC Now ono ever been required to Oe theme Faroe of a pollee+ Olvistam In IIIbiespItel er nursing hems her en entire shift?
In your presort position? III tee (2) No
In other poeltlens? (I) Yes (21 No
If "yes". on what shittCs1 have you Peso In charge? (chick ell that spew
(11 Nog (2) EvOniftes . (31 Almhte
30. Old your L.V.N. promo pronto, you with top wooled,e and shllis moiled Inact se e flaw leedr or chirps aunts?
111 Yo (2) No
If yen Meowed "no". do you fool (hot L.V.N. proven Mu previa roueposetencies?
III Yee (2) No
21. Pimps clock the Om insorvice or continuing education ?regions stuns* scol4 eaof gallat illenefTI-40 you. (Check no more then In "'Woman.)
III Now oquipment and procedures (5) olt% Mope" In the Ileaeosite .
n.
ss.
121 Nore about ecticon of dome
131 Noe to be tom toodOr
(4) Gore anatomy or physiologyMon/ divisions
omm,wwwIr.
(5) mow filImoss ifsots a prtfitrmeo
bohowlat
(7) lord asougoopat
In your present Job, Ale you sere with any morose vise rocelved timer K.N.edlicetiso In ether countries?
() Yes 12) No
Ass there factors which mould prevent you from osopting ehattraction Joe otter le eheillber googrwpalpsi amp dare them10 alias trio year semant rieldeetal
Os you tool INN taws lo a shatiogoof L.P.O.'s Is soft oftee Hogsr eltlos sad tamps in 'as *tote
111 "op
131 No
III 'los
ill No
Wok of lee *Nicola, Owns In row foll in the soot oftectlwo for properly1.116 all Norma howl," stoma, somertasee I. the IlicapIfol$
(11 NespOtet Opret00 (31 14014, Oillilobo
mil NMI' lbbel (4) Mom Weiss apsolfpf
i 77
180a

Wm KAMA CAUL TI( month IA ',. ma, WIT-CMDIcAns i(491 MADVOW IC PAYMENTS DPW. MAU ODopt MO AMY (ADITIONS.
ste
S
S.
O.
a.
IM
I.
1.
4
116
1.
1 2 3 4 3
I fia avtiatiad with my present Jul. 1 2 3 4
I ea fully utilities my c.o./641min. I 2 3 4
The salary 1 receive Is satisfactory for the Jab 1 2 3 4
I %eve.
I receive OOPOPOI recognition end credit for the I 2 3 4 3
week I de.
3
a
9
1 thine that i am appeals of functioning et s 1 2 3 4
bismyr loyal mz If i were allowed to assure other
Tooldne11411tles.
I believe thud I as eueliflee to fue.ction es it teem 1 2, 3 4
leader Of CO0,90 nurse.
1 believe that L.V.N.'s do everything that 14.N.'s do. 1 2 3 4 7
Ttr selerles of L.V.M.'s Mauid be closer to these I 2 3 4 9
ALPO. receive.
4 feel that I have had to misled responsIsliltlee I 2 3 4 9
OM perform functions far which 1 OP not prepeeed.
News L.V.N.'s world enter R.N. proem. If I 2 3 4 5
they received some automatic college credit for
*weir 1 V.N. peeve/1410a.
efedretes of L.V.N. emigre= which an not located 1 2 3 4 3
In colleges or universities shorit not receiveSmiles, credit whoa they entry en R.N. program.
4101411dies 44 AMILL.V.N. program should receive some 1 9 4
Ofteilmetic raises dredlt Oleo they well IS em
.111. proven.
S
Of 1
B$ t0?1 MMIABIE
178
what chomps. If env. do you thiek should beof L.V.N.'st (Please shock all the, pply.)
411 K change,
42) Longer program
451 More clams/we work
(4) More clinics, experience
431 Shorld be acre on 0collage 10,01 (arch OScommunity college)
dodo IA the odoo010041 9,104,4/11101
(GI More leadership covariance
(7) Shorter prtgree
(S) Mee clleicel emperlencee OOMOIOOthe hospital
(9) Other (please elvish,/
216 Do you think that currant health care delivery trends Oil effect the need Our..V.N.' In specific Jul settings,
411 Yes If "vile, plebes ilediliela
(2) No
29. A/ student Oise OfTOPOO college for 12 emanths could erre epprombletely 42 oompoterPOWS of credit. how many ...ester hours of college credit de you *lob enL.V.N. should twelve for her L.V.M. program when she oaten on R.M. program,
credit hours
Mirk you for your participation.
181
4 aI
42,

BEST CAM MALSTIONOT NalilkITY
I. tea:I. Male
2. female
2. eeriest Status:1. Single1. parried
2. 444
4. Now f Nursling School you are ,resently IngT
s. please (neck the typo of program you are attending and your year of
attendance.
0 I. Dielmaa1st Year
2nd Year
2. latest to
1St TOO'Ind YearIrd Rear4th year
o AliSOCidti; Degree
1st Year
2nd Year
c,..duitte
1st year2nd YearIrd Year
. What is your sopected date of graduation:(month)
Are youI, Full time student III or sort songster hourS)2. Part tin., itudent (less than 12 semester hours)
De yew:I. Commute tf00 Outside the city limits2. Liva OA coleus or In the city where the school is
If you commute. what is the swami mete distance
to gnmous7I. 0
-23.
S...---4.
- 5 miles- Is miles
20 - 25 mots)0 - Is miles40 - 45 miles
20 miles or mere
(year)
located
from your residence
IA. Mty aid you choose to enter tiis earliculAr LitaY ograo/ (Diviumr, A.D.,erIlaccalaurease)
lg. New many school% of nursing did you 1 igete imfore choolIng this school?
....=20. No. did you first obtain information ..brut this school?
I. you yollossysto Information.
2. The school SENT YOU information.I. Yew received leformetion through a Careers Proven.4. tither (pleas specify)
21. Please indiCete those factor% Chet Influenced your chOice of thisparticular sch.sel. (Please check in the hoc)
s.
4
0_ 0__o____
1. Novirmirs tr home.
2. Costs of the program.
Length e1 the program.
Availability of part -time sorb.
Characteristics of the curriculum.
supuyatidin of the lirolirol
Cultural or entertainment advantages of the city.
heevemended by friends or counrelors.
I.
4.
S.
4.
7.
S.
9. Availability o: challenge ems" or credit Wowed farrecognition of prior nursing experience.
0,0. Transferability of anodic, from other Institutions.
fall. Family member on"0;tive dug at nearby military Installation.
1/. Other. Please specify
N ew please rank. In order of ImeertenCe. these facteri which 00 checked Inthe above euestlen. Use "I" for the ammt Iftertaot factor. ace the
e umber is the Mask to the loft of the "Ouschee boo. Remember, rank ezli.
these fast/,, for which you chrome 'he 91m.
9$. the your elusion of a slag oshoel influenced by the availability offloansiol melistourel
I. Vio2. Ile
s
111. Whore did you graduate from high school?
(City) (County) (Stets)
In that city and county ere you 1 ivint while attending this sshetS
(County) 'Stahel
12. Where were you living at the tie* you Milled for admission to thisnursing, program?
"(State)
What Is the approximate distance from this school toIn the previews eueStIon2 00111111 ilf +mom city put "el
14. What Is the name of your hometown Or permanent residence?
the city listed
--ren7r (Stater
I. What, it the mioronimete populatiom of your honotorn?
1. Less than 1,0002. 1,000 to 2.4923. 2.500 to 4.52S4. $.000 to 9.9995. :::: 10.000 to 24,999
4. 22.000 to 45,555
7. 50.000 to 99.222100.000 to 265.222
9. 250.000 to 499.99,10. 900,..100 to 299.929
1.1:00.000 or more
12. Do not know
IC go you have family responsibilities that would prevent you fromxtomitivi a scho%1 in another geographic area?
I. fin
2. No
17. IS this school the closest R.N. program of any type to where }OMROOM living 'man you Rolled for admission?
I. Vas
2. No2. Do not know
-2.
24. If Yes, what rya, of assistance is applicable to you?
1.
2.
3.
SeholrshilisAmy Strident Assistance ProgramsNavy Student Assistance ProgresoAir Porte Sponsored Program
5, Nurse Treineeships for 4.N.'sS. Sevilmront Student Loans7. Other Type Loan
Stets Stipend
2%. Nos member of your ?soli, woe ottondoll'tkis 1nttitotloo7
1. Toe
T. No
22- if yes, Ins
I. eurvIng
2. Another Major (specify)
11. Prior to edelsslon to this school of nursing did you hew any emperfonee,certification, or immure Ina health field?
Wr
I. Yes '2. No
21. If vet. in which of the follmaing fields;
I. dolonteer work
2. Afoot ferias). rococo Norse Club4. Technician Specialty (specify)
'ate 5. Licensed Vocational program attendellr
. Nurses' Aldo1. OrderlyO. 4.11.
9. Other (plostile speolfy)
If.
179
182
INIIMwoo hold a degree In field ether than nursing?
1.yillilrneSposIM
Are yoo Interested in mrbiag in ewe of the following areas of essomailod
Norse prattles? 4.1MM Tee MN if Yoli.oloese Indicate:
1. Oadlatrla Nurse Prottltlener2 -Foloila Norse frontitioloirI. Scheel Neese Prottltiener4. clIcao likeelelist (please nelogift)2. Olhor

1110111131. New arm Institutions of mile., odoesaien have you attemdilid
otkOr thaw JilE51 CC!! 141o. 0100so riot' In swear of Impartence these flows which yew d loems 10 wolek you aro eurremtly sorelled?
the above question. The "I" for the most Important fatter; fir. rev the
32.
13.
66.
15
Please lilt the inatitutiens attended and indicate the duratioa of attendance.List the meet raiment school first.
This in Atndime.Length of k.
he.
01.
42.
Seemed most Important, ate: Please piste the maths? In the blank to theleft of the "checked' toe. ISM telt those 'team for whleh !Si ahockod
the Mom.
In what area of nursing,proctice would you like to work the year falir-
'Our groduation?
1. Smell hospital (29 - 100 boos)
Ihmudjmilbet Ion. Wait!. issi_erA_LItt Liar. years ) veers
0 0 0 0a. 0 0 01. o 0 0 0 2. Medium On hospital (100 - 300 be")
3. Large modical center0. Nursing twos
Owe see charmed your major?
1. yes. Prom what?
S. School of lloOsing0. Private duty7. Public health : below)
a. w.
Old the change of your molar require troollo of institutions?
I. Tot
S. School Nurse9. Industrial Marl.
00. Office Nurse for a Physician or penal'Armed forces
12. Other (please specify)
2. NeWhy Is this area of your preference?
Whom do you sweet to practice the first Too, hollowing your gredvation?
---itrryi
practice
Would you prefer to (wattlea in as(County) tutu
would you accept employmont in location other than the one indicatedla 1141 previous question?
1. Tea
2. No. Please 00000 reoseniI. Olplans
37. It yes, Associate Dogma7. Dacca, to
i. In smother region of the4. Nastier
Ph.D.9, in soother nearer ttttt
t: Pftdonlimptiy rural Oft.
2. Predominantly grim' area.,
03. Who' is the highest educational
-...3' In any stets
M. Which of the terser poitielts listed Wilco hest watch*, your present lans?
S. If yet. please Indicate. by in the boo. the factors that wouldinfluence your selection of the alternate location.
I. To practice nursing full-tiae for the rest of my work 114.
1. To prctiCe nursing full-tine before I hove a family, than stoat
...-CI 1* ogauoss to 4 preferred locationworking forever,
3. To practice nursing full-tine before 1 have a family, than t rt-
___.[:]1. Opocituniay to wore In leree emdlcel centertime sells !Aping the 0010,1%,
---- 4. TO practice nursing full-tine before I hew* a 'orally. stop work
___[743. Oppartunity for &swim-men' In responsibilitywhile children are In school. then resume of cores,.
5. To work pert-tino only, for this rest of cm work life.
CDO. 'alert lands and benefits6. De net plan to Practise nursing.
s.
......0 S. Cultural sr entertainment eimonaopes
7. Oche::
65. if yore would et wining to partICIPete Is future follow-uP studios. Pleas*
0 4. Lawton of husband's jobprovide your same In the space bolo.,
.....
lore, you hope to obtain?
TttIS SICTIOW IS TO eg COmkyT20 dokr Or TNOS2 STUDENTS kO0 All M.11115,0T 11.11.'e
ISO MI WINING ON ['TWIN A OACCIMASAft OSUMI ON A WINO) O(CRES.
46. Whet was your Initial loyal of Professional preparation)
, I. Diokme2. Associate Dog...J. ilaccalmommtaml
67 e. Name Of instItuthen where your initial sine education was resolved?
Sao Too
City County State
MI. My did you eloose this type of program?
.--c------,
Wt loeforr area of graduate apeclalisatles within nursing? (If dowel, majorpleas* cheek both)
1. Clinical Specialist (specify area)2. lifeCatIon
......3. hdwinistretlen4. Other (specify)
0.
OM. I. obet Hotel Ore you ,Nrosontly lIcoased?
1.
2.
3.
.11.
I. Moro 404 employed r an 101. immediately ',ler on your emterleg this
poogrood
see 2. NO
O. Whet almorleres have you hod ail an AA.?
I. Smell hospital (25 - 100 Pees)
2. Modluo hosltal (100 700 beds)
J. Largo Medical Cantor4. movie, mem9. Scheel of Nursing46 rIvot Duty7. 1011e *salt* (ontoptS. Wu&9. ledoser:Xlerso16 Offloil Nor (f'kyrislan K geodes)II II Aroma12. (IOW (oleglite spoit14)
180 183
-6-

SURVEY OP UTILIZATION M7101111MID t.11.111,is falli.OVED 1M MOSPIVALD
PUT 1
I. &EU (I) Niele
(2) Oemote
BEST tiet AVAILABLE
fi2. AOC
). Please lowliest@ all nursing programs from which yaw home GRADUATED.
Veer OfProprqm Graduation
(I) LOD IS
(2) Siphon 19
()) Associate 19_
(4) bcceltereate 19
(5) nesters 19
(4) Pectorals i9
School Mfr
ri
4. Hove you termed any additit 'al nom nursing degree1s1?
If yes, please specify
Are you currently enrolled In any nursing proorow
leading to diploma or a degree? _(I) Ves (2) 00
If ...faa. type of program, (I) Diplome (2) O.S.M.
S.
Stare O 0c)O 000O GICIDOO
D ODOD ODO
(I) us (2) ea
(2) A.D. (lb) Graduate
A. Mere row teludg any courses for credit while MOT 'enrolled
In sprcIfiC program leading to diploma or d.grea1
7.
Tell (V) 140
If you answered she left question 'Nee'. what was }au:- primary reason
for takInt this/these cOurtie(S)2 Check One.
(1) TO up-date nursing skills ()) Eventually hope Co
or abilities apply to degree
(2) 1411110red by employee (4)
15. Which of the following categories applies to your position?
(I) Work in the sane iocatiom on permanent basis
(2) Work 01141 on floating basis
()) Other (specify)
16 Plisse Complete thi ft.iiowing chart indicating your hosnItal experiencees nurse in each of the areas
(01) Dorn unit
(02) Clinic
(0)) Coronary core unit
(OA) Dialysis unit
(OS) Emergency roes
(04) f..tocrinv-tletabolic
(07) iromoology
(001 tar. Mesa, Threat
(09) Labor S Delivery room
(10) Modica, (General)
(11) Medical ICU
(12) Neurology
Memory
(14) Post Parton Pelt
(IS) Oncology
(10 Ophtlialtelooy
(12i Operating room
(10) Orthopedic*
No MOnths of Experience04 TN, SpeCIMity in ThIShoar:to,
Ww. Months of (spar lancein Thin Specialty InOther Hoapita:
Continued gm peg? 4
?
(m)
(02)
(0)
(0)
(05)
(06)
(on
(06)
(of)
'0)
III)
(12)
(1))
(14)
(IS)
(IP)
(17)
181
1
1. P1011* Indicate on the chart below the rositIons and moon' of olobrieeceselo have had in each category.
ANmtkt of lmeetience Months of fisperieree
In This Position in In This Posit' Is
Thalurran----
1. Staff-Ala If Lim
2. Plead Nurse
3. Clinical Specialist
4. inservIce Senator
5. Nursing Service Director-or Assistant Director
6. Other (Specify)
eIn the Maw, question, please place a circle around the number of thecategory which indicotes your currant position.
itt
9. Whet is the specific job title of your present position?
0./M.,//i*Vr/M14/V.MdOM
10. To whom does the hoe ical indicate row are responsible? (Position
title(*) only: no names
Whet is the title of the parson who ,ctuallx supervises your markt
O 012. What is the title of the person whom you think should swpervlise your work?
I). Are you employed: (I) full -time
(2) 4-55 Firs/W4
O 0()) Lass then IS MrsAllk(4) On cali,only
14. What Is your usual shift? 111 Days only (4) Nosute all shifts
(3) Evenings only )5) Petite days it evenings
()) Nights only (A) Other (specify)
Continued Ira page )
No. hmistis of ExperienceIn This -Specialty in This
Hoapitai
So. Aontls of Experiencein This Specialty inother Hospitals
(19) Pediatrics (19)
(20) Psychiatry (20)
(21) Radiative therapy (21)
(22) Recovery room (721
(2)) RehabAltmtion unlit (2))
(24) Assisiratory care unit (24)
(25) Surgical (General) (2S)
(20) Surgical ICU
(22) UrOltly
(21) Other (specify)
(24)
(27)
(35)
olo she question above. plus. place a circle around the number(s) .f thespecialty or unit(s) where you are currently working.
.=1,
oc
17. Joss your arise hove a clerk to perform non-nursing duties? (11 Tee (1)0,
II. If yes. please indicate on the chart below the Ulnas when a clerk le ea dolly.
Shift 1 De OSA 2 Mon-Frl Mono k Other. If
i0,19. On your welt doss the clerk (check all that apply)
(1) Work only as your melt
(2) Nog on two w mote welt,as soled
11) ark is fell shift
14) Wok port if delft

211.
ty lipti DO NO PRACTICE TIAN INSISINS. TIRM TN 42111171011 16.
please place a cheek to the eeeregriete column for each shift.
11001. 'ursine
BEST COPYAVAILABLE
25. in el area the Priggery consIderetion few coking: patient essignmeets Is:(Pleeke chock eraTiM)
(I) Patient location (a grime of bads or non together)
(2) Patient Calomel*If adequate 00041011, enstaff Is .141. I s Olefin
fri (1) aw1 1 e (4
(ILIA the day shift
- . . ..._.
(1) em the evenings shift
(3) en in* Mint shirt
..
.
21. I ect as teem leader:
(I) Whonovor I mm on duty
(2) 1 alternate rills other scoff nurses reoulerly
(3) Only If I on the only licensed nurse In MO ere*
(8) Other (specify)
22. Tenn conferences (pat lent core conferences) are held in sy area:
(I) Doily
(2) %Wily
(3) Monthly
(4) Newer
011011. (5) Other tspeeif0
2). When Mom conferences ern hold. 1 act as cenfarence loader:
(I) hesenever 1 em on duty
(2) Only mown I an toast leader
()) if I have been assigned to prepere special materiel
(4) If the conforenca Is about art pallamt
(5) Never
24. I mflue patient care esslasmants:
ll) Only when 1 as team loader
f2) Pally - hot not as Woo itoder
ID.
(3) Never
(8) Other fepeelfy
7
in COlynn 1 bolo+. plane place a check in the 800 next to the thisof sack person to whOin you have personoll, 7.7APZTicOtOill nu11100tIony to
Increase the efficiency of raspitel 11001 o to delivering lirerered
ter* for all patients.
I. town 11. plynco piece a check in the box next to the title of each
person to whom you have personally conmunicated,seggestIons for improulagcore for latific,netiontit based an their Individual needs.
Column 1
Suggestions forOrganisationalor ProceduralCho s
Column II
Suggestions toImprove Corefor DpmCIfICPatients
1. Team member
2. Team leader
). deed 4V1241
4. Supervisor
E. Clinical Specialist
6. Illrecter of Nursing ServIce
7. Physlelem
O. MDkOltol Admint
g. Need of another Nesp. dept.
10. temileyee of mother Peet.
II. Other (*poetry)
0
00
Nem. In Column 1 Ammo. eleese rink la order of frapanCy of enteet thetitles of promos Alm yew clacked. Vele "I" fee the Gest freeman° enir
tested person. Place the number in tail Stook to the right of the
bon. Nemeeker. rpm Lotto those uhIch yem chockedl
limm, please rook the bawl Amine In Cele= 11 le the same Hemmer.
4
M111M.
(I) Amount of care required
(4) Type of educatleftel becksitend of personnel
(5) Other (specify)
Comeeetss
If NURSING CAM PLANS ARE NOT USED IN YOUR AREA, PLEAS[ SKIP TO 6112$210111 fl.
26. IWO', care plans ere kept up to date and are usedregularly In sy arse (I) Tits
27. Nursing core plans le my arse ere:
(I) A part of the treatment and emdicetlee hordes
(2) A separate kerde lir file
2$. Nstatiens in nursing care pleas In my area are eede by
(1) R.N.'s only
(2) R.N.'s sad 1-11.11.'s only
r
(3) A specific nurse (title)
(4) All sweets of the nursing staff (including aides and studiete)
2). 1 coke notations on nursing ears plans
(I) 00 all the petlents I aim assigned to
(2) Only an the west complex or critical patients
(3) Any patient in the are when need indicates
(4) I would line to mho metetlems lot seldom hens time
31.
(3) Never
Il
In Colima A Wow. please pl7ce a chock In the box next to each methodwhich you nave used to communicate Illptestd organisational changes toimprove delivery of patient care.
In Column O. pisiM 111104a a ChOCk In the lex next to each mat t nhichyou Ivive whod to cmOunicotO 00,900tIOns for Improving cari1147Seeclilepetients.
(Deere Piens
(2)ShIft Report
(3)Pationt or Tee, Conferences
(4)Pertienel telks with individuals
0/Written reports or suggestion,to swifts persons
(4)A. mwoher of a committee
Column0_0-0_0-0_
N ow. In Column A obeys, please rank In prier of frequenry weed the eeteedo f communication which you checked. Vse "I" far the nest frequently seedmethod. Place the number In the blank to the right of the checked tom.Aomember, rank only thew welch you chs41001
N ew. plee.0 reek the banes checked In Column I in the some lememer.
Yew ben Mashed Part I. Plerme torn the pegs and motet* Port II.
182185

BEST COPY AVAILABLE
PAST II
For each Activity, please circle the pod neriat response in each of the feu, column,.
$2.
.
Aid you dothis whiteTOw war.
student
At the [Igoof graduationdid you feelprepared todo this
IndePesdenli,
nave youdone thIS IiI
li
Li" IN
papa you Ogamthis in IOW
rfillyiS 14/1119A( I ) 1(2) 1(3) 00eTeel NO lAdiolifdAlltACTIVITIES
( I I 1 (
Yes I
2 )
No(I)Yes
I (2)
I No( I )
Vet(2)No
01 Personally communicatesuggestions for procmilorel chanoes to
04
edministristion.
Porticio!'7 .n nursing
Ves Mo V., oo toe No lots No NA
83
or hespital committees
initiate teechleg orhealth maintenanceam ssssss for patientsor feoilies.(1.p. Nsell .saw; annual check
Yes ND pas NO tee Ne we Mo NA
ups. hmmunilations, tc.) Tes No Tot tio Yes No Yee Pp NA
0 Shp, IN or sucutameees
iniattions Y.9 No 1,09 NO Ves Ne Yes Ne NA
OS Prepare a room fornew odeission Ve No Vol No Yes No Yes No Ila
0 mi. i.v. Solutions Yes No Yes No To* NO yes NO MA
07 Start I.V.s(vernpunctur) Yes Mo Yes NO Tee No Yes Na NA
05
,
Nomove I.V. needlis Vas No Vas b Tes No Yes lb NA
09 Nik 4044d 4119physicians Yes es Yes No Yes No Ye; Mo MA
IN At as team leader vas No Y42 No Tips Ne Tics NO NA
II Conduct toot conferences Yes No Vas No YOS lb Yes No NA
12 SuCtin trochee viatrash cube Tes No Tat No.. Yes Nip Y9 Ile ile
I)
,
OrOpharyuggal suction Yes No yes No Yes No Tee No ND
72. (Continued)
AtTaITIES
11 Feed patients by mouth
32 reed patients by N/6
or instrostoey tub*
SS 040 igetient referrels
)4 Take patient's
physical history
)5 Tete **tights psyche-101101 history
)6 Pieta patient 0494,1000,01 904914
17 Operate renaldialysis equipment
MOOItOfvonews pressure
14 Sat up all manlierchest Arsine's bottles
40 Drew bleed sampis
Al Newly, techine plansnd'cohduct classes forgroups of potions. (suchas dtobeticS, nestctomyeta. etc.)
42 Nevelep and leploosnt ateaching plan feeladieltisee patients
Did you gothis while
You Wit,* 6
student
.11-1(21Yes No
Al Mahe patient care aseletr.ments fee group es
meshy pereemeel
Yes No
Toil NO
Yes No
Yes MO
Yes MO
Tics NO
TeS Mt
TOO No
Yee No
Yes
Vas he
Yes Na
Teo NO
Al the Orne
0f graduation
did row ftel
prepared todo *hit.independenlity
(r} 112._Vel NO
Yin No
Yes lb
Tot NO
vas No
Yes No
Tes No
Yes ND
Yes No
Yes No
TOO Na
I I
Nee* youdons (hit SA
IPE4411441
LVN or IN
111 (2)
Vas No
Yes No
s Ns
TO; No
Yes MO
Y42 No
Vet No
Yes Ile
Yes Ne
Tee NO
Yes Ns
Vas Mt.
pas Ne
Ve, NO
Meg you donethis In yourpresent 09100,(I) (2) 131 teatY49 No licable
Yes P. S.
pas Ile MA
Vet No
Yes No NA
Tell NO 0A
See ND ND
Too Na ND
Yes ND MA
Yet No
ref lb
; 183
32. ieontinwd)
ACTIVITIES
Old you dothis tonile
you were astudent
Oh 1(21via 1 mo
At the tiara
of trenwstion.did you feelprepared todo thisIndependently
1) I 121
'es 1 No
11140 yen
Ilene thiS II
licensed1.1111 or RN
1 (2)
Yes I No
14 Champs lamer tracktido cagoule
IS give 01 by nosh
Or cabal
16 give IPOS treatments
12 Messenger trips to '
phreocy. control supply
1 Order twpolils forovule division or ores
19 Nwookeepity tasks
20 Ambulate patients
21 Perform passive tonesel meths.
22 Insert teethe&Whitton
2) Irritate Welcatheters
24 Irrieete colostomy
25 Develop and easeutepatient Cars Plots
26 include htorIng careobjectives on tete pleat'
27 Develop written Omme coreplan with patient to bedischarged
211 Cher* wItail sips
29 Apply bobs er compresses
30 A 41, tattles, eedlatetlen
Yes 11n
Yes ND
Yes ND
Yes Ile
fits
Tes
Yes
N o
N o
N o
Yes No
Yes Na
Tee Ne
Tes Ma
Yes MO
Vas lb
Tee 110
Tee, Ile
Tee
pas
No
Yes No
Yes lb
Yes No
Yes No
Vas Ile
Yes ND
Yes No
Yeis No
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Ves ha
Yes No
Yes No
Yes let
Yes lb
Tee ND
Tes No
TIM
Yes
Yes
etp
N o
N D
Yes No
Yes No
Yes ND
Yes so
heel tots densthis la sow?AIM pnitisleat
Yes N i illmelicablst
Tee 0 111
Yes No
Yes ND NA
lie ND 0
Ses
Yes
Yes
me
N s
No NA
OS NO NA
vas ma NA
tee No AA
Tee No Tee ND NS
Vas No
Teo ISO
Tee ilo
Tel NO
Yes No
Yes No Its
Ves No MA
Yes Na NA
Yes No
Yes lb IM
12
n. SA, ..mmof graduation
Did yOu do did you feel Mayo you
this while prepered to done this as Aare vow albyou were a do this a :in/lased this In your
2. ( C0min:1mi) tt t inde,,..entl LYN or All 'afoot I 1
ACTIVITICS RINI /les PIERFERIIEll . 11:-.-
4 fake Citte yes No Ves mo Yes No Yes Ne NA
4 *Imo ENS Ves No Yes No Yell N Vas Mt NA
A bealter petlenesheart sieleity Yes ND Y011 40 Y011 1111 TOO No NA
4 Defibrillate Patient Tee Ne Yes is Yes Ne Veil ND AA
IS Perform cordielylooneryr itatiem by self or
with I other person Yes No Yes ND Yes Ne
.
Yes Ne NA
4 Tate herein, histo-y fee Ne Yes Ne Yes NO Vett NO AA
10 lealleete job perform/MVOof personae, In written
reports 'des ND Yes le Yes Ile Tee NO OA
11 towhee, wick mepleeme; Wet their )0 .
performeell Tes Ne Tee Ne Tee" Ne Y114 ND 111
SI Sat up traction appret Teo No Tee Ne Vet Ne Vas le NA
5) Take eltel slent
f4 Vest urine for simper
end oceans
toe No
Vet Ne
Tee Ne
Yes ho
Yes lb
Tee Ille
Tee he ND
YOB GO Ik
55 Amour* specificwoolly of orine tee Ne' Ten No Yee Ne Tee 01, 02
SS Reeser* lete 8 Output tee Ne Vet Ile Vet Ne Tee Ile MA
43 MMus nursing diereses Tee lb Vet lb tee NO Tee NO 01
55 Write twain, orders emchart
b9 10.0110 pelmelties Amir
sea No
....- ...
Pee No
.-. w.
Tee m.
e... so
Tam ft MR
ewe Om MA
1
obril1011 NOM

BEST COPY AVAILABLEIS 14
P. OGNstimuoi02
Atl1viv121
Did you dothis 'Nile
you wartstudent
-,
of OrisdoeticnOld you feeloweeere tode this
indeptunlently
Nave perdone this as
licensedkve 9w IN
Hosokawa dome
Sills i yourpresont
(11 1E22
Yes I No(i) I 12i
Ves I NoIII" II21
ram NoIII 112] 13) NetVii No limb),
6P now dressings Vas Ne Yes No Yes No Me No UM
6i Modem sutures andAte slips Ves Ns Ves No yes No Vs* Ni NA
61 Pass ness-eastric tubes Ves No Ves eo TeG No Yes No 101
'3 AolOwo nom-spostric tubes Ms No Yes No Vas No Mrs No MA
66 Transcribe doctors orders ves Ne vas ft Ves No Vas No NO
44 4,12 Niller-Abbott tube, Yes Ne vet No VCs Ne Vas Ni NA
66 Ammo miller-Alisontales Yes Ni vas No yes No Yes No NA
67 aim *rel rectal,sablimmi medial.. Vii No Yes Ni Yes No Vas No NA
$ give en emus Yes Ni Yes No Yes 2, Yes Ni 44
411 give douche Yes No Ves No Ves No Tes No NA
70 Transport pother*, Ms No Yes No Yee No Tee No MA
71 Cleric/al &Alms Yes No Vas No Vas Ne Vet No No
72 Tomah crutch rlkino Yes Ne tee No Vas No tea No NA
73 Haply and road skin tests Yes Ni Veil No Vim Ne Wei Ne No
74 004 ACE or eteSSOTOMeneesoe
)
Tee No Veit No Volt No Yet No NO
75 Ow WM betas fis la Tes Ne Ms ile Ves Ni NA
76 Choose os lime Ms la Vas No Vas No Yes No NA
M. 48$4101.4 maws) orientation co :ma mime aspects of 'wilful*/Institutive sadency, de you believe currait prof mime! eurelito
education hes adequately prepared the nom sroduategef she following
prostems to function in beginnine positions
a. biplamb. *maggt(' 0011,14 Pc. Baccalaureate
(I) Vie (7) Ni
(I) Vo (2) NO(2) Vet (2) NO
IS
41. If you answered "Ne" to the previous euestion, abet specific chimes Isthe eautattonmi preperaion of nurses would nspI them le Gentle* ogee
effectively In the job settle&
Iplvmai
emaciate Negroes
calepreetet
T44116 1011 FON reul OPOITICIP4T144.
184
33. if vne nirli IN a hemielltlei am (each es 6.0.. lam end delivery,etc.) plasm Ilst procedures opeelfic to your era is ails& pslualise
ewes, shield he competent.
2.
3.
0
S.
Old eye feellproPeratM this Mk hulOdoientiowhen yen Oredeettlie
Irfes
/Yes 210I)Vos
ices !lap
Fog osteatieea $4 - 31 geode MOM on the Italia of gook relitstefted(L.V.N. is R.N.I. Id you me An R.N. was ma elm an ., us
the imam ad 9604 data job OA do 2.N.
In your first position as s licensed perm did per Job require yea toporter's premieres or assume responsibilities few Which peer edesatiale
had net prepared you (I) Yes (2) Ni
3S. If you answered "yes" to the previous eNestion, please specify the I'mof activities for which yew felt mnprepered.
36. No yew feel that year basic mesh's education has provided um with skill.or abilities which could Ni utilised in your prosiest 'Millen MK 164144
for scum roes.° gou aro mobil Si MPII0
(I) foe (2) No
37. If you answered the above question "yes", please minify Mit those wooed
abilities ore.
36. Whet lectors do you feel ceetrIkeis to the lack of otIllzatlee Of Oen
hIlltleel
33. Mat opecifice chooses is year present Job DIN/mice mild emilikr you Niutilise mew mrsim abilities to a greeter dagresT
187

iftIOINT CLINISCIAUN OPINION SONNY
SI CTICII1
I. Sea: (1) mole
(2/ hoot
2. Age:
3. Marital Status: (1) tingle(2) serried(3) widowed. divorced
4. Type of nursing program: (1) floccalaureate
(3) Associate Degree
S. Aroma a: (1) NegIsterod Null*(2) licensed Vocational Nurse
S. what is your current grade -point average on a four-point %toile
P. Mhat,Is the title and course number of this course/
BEST COPY AVAILABLE
lig Diplom
O. Does this course have a clinical lab? (1) yes
COLUMN A
In This Cher**
g. Per each question below. pleasecheck the appropriate answer inkaII Coluro A Ind Cohen IL The
aptten in Colour A. "Not Appli-cable'. is primarily for questionsabout clinical experience if yourpresent course does not have p
clinical lab.
(1) Objectives are reviewed in classat the beginning of the course.
(2) Objectives are referred tofrequently by the instrutorand relined to the Gahm.;being presented.
()) The course objectivesehelpful in knowing Alert*Study for an tests.
(4) Course Objectives are help-ful in presaring for dolly
classroom assignments.
(S) Course objectives are help-ful in Peeving for dollyclinical lob assIguments.
(17) The bibliography contains avariety of references from pub-lications that are not strictlymiming or medicine.
(16) Clinicn1 experience is sufficientin length to waster oast tamholcolprocedures.
1
Yes2 3
No NotAppli-cable
COLLOR A
In This Course
1 2 3
Yes No Not
APP11-cable
(10)'Clinical eaverleace providesadequate opportunity to applymerlin, theory under nealistIcconditions.
(20) Clinical experience in the hospi-tal Is provided on all throe
shifts.
(21) Clinical experiences are ',swillrelated to theory being current y
prosonted-4*-"tes. _
(22) In cl,nical lab. the student isfal*PUMI by the regular staffas a member of the nursing than.
(27) Students soy choose am area ofclinical assignment (sod -s
divielen. 04-Ayn. Piodi. eh.) IfIle area sae provide soperianoiilowest the objectives of theMae.
(2) 110
COUPE 6
In Nest Other NursingCourses in This Cur.
ricaliva
1 2Yes No
3
C01.1001
In PliSt Other Nursing
Courses in This Cur-rinds('
1 2
Yes No
(5) The student is expected to*hill, his own objectivesfor clinical lab in additionto those in the course outline.
(7) Students nicely, an individuale valuation of their avilevenentof ppecific Objectives by afaculty member.
(0) Students ono required to doself-evalustion of their achieve-
ment of specific objectives.
(0) All course content Is organizedaround a unifying donne.
(10) Course content is prhoarilybased on units for each major
body system.
(11) Course content I based on the
n ursing 'process'
(12) Course content effectivelybuilds on specific knowledgeobtained in pre - nursing courses
and/or previous nursing courses.
(13: Course content is primarily or-
ganised around Wei of Problems(such as 'mobility'. "anthem!,
of 02". "metabolise).
(14) Course content' Is organizei inmodules that allow the studentto choose his own sequence andhls own pate.
(1S) The course bibliography containsjournal references as recent assix 'tenths or less.
(16) The course bibliography has 4"Morita of references more thanfour or five years old.
COLVIN A
In This Course
1 2 3
Yes No NotAppli-cable
SECTION II
for Gem question below place a clock 64 in Columnplies to this course._ .14% Column ! please check the
apt your ihrn1ng needs.,
10. ,The objectives for this perm are:
(1) Given to the student for the entirecourse at the begInoing of the course.
(2) Given to the students at the benifiAlm4
of each unit.(3) Di -blood cooperatively by faculty end
students.
11. Students receive information on 'Jai. topics.-- -- -- clinical lab alas and reading shipments:
/1) for the entire course at the beginningof the coarse.
(2) for each loft. Jot before the unit__ -. __ begins.
: MsrklY 11:It: irregular
S Other (please specify)
2
lost Other NersiagChews In This Cast -
Halloo1
Yes Ni
4
A next to g option edict. sp.
an option-idirch meld beet
COW" A COMM(This Course) (ar Frets,...)
li. leading elsigmesots for this course Allies:
=.0
13. 14,
(1)
/
2 Scoot-rt.:I:oohs3 Ni regular teethe,*4 Ilibliographic references only
S Other (Please specify)
..1
eta 1,nur ly used method of evelwattomof Iheeeyta , . carve fs:
Ifrittoo objective tests (multiple choice.Noma - false. eta.)
*Maiotem Met, tests3 Orel emiliaatleue4 :lasers= pertfcipatiosS Special projects (11140,11 specify!
rWM11
1. YMMINII
185
MMM.
010

14. SuperviSion in the clinical setting in thiscourse falls Into which cf the following
Catelleits?
(1) Aa instructor is in the Irradiate areaat all times.
(2) Ae instructor is not always in the areabut IS available an tail by peeing, etc.
(2) heervision is primarily by area staffwith post clinical conference with animegroctor.
(4) Ogler (please specify)
1S. If a student hoS difficulty with portions ofaverse content, what resources are availablege hie
(1) Tutoring sessions with an instructor onimpost.Tutoring sessions with another student.learning et:source center with audio-visual aids and a faculty member
available.
Croup study sessions on a regular basis.Special medial program for specificlearning problems.
(4) Other (please specify)
111
1:1
1S. Please indicate whichfbf the following teach-ing methods are used most frequently in thiscourse by placing a "1" nest to tnoluothod
Aimed 'oat often. "7" in the neat most frequent04 method. etc. In Coluen II, rank the methods
according to your preference.
(1) Lecture(2/ Group discussion11) Presentations by studentse) Audio-visual media (Lopes, films, slides.
T.V.)
Independent studyTeam teaching
7 Other (Please specify)
COWIN A COLIPSI I
(This Course) (My Preference)
RANK(This Course) (my
RANKPreference)
...
7
21. is his course. schedules and classroom topics: (Check (.1 all that apply.)
1) are followed;L:f1Voicif:11::h.41 ::::2:4100tifICAt140
3) goy be changed at the request of a majority of students4) can be adjusted to take advantage of unexpected learning opportuLltie.
22. Ian 4 r'. s based on knOwledge of physiology, micro, chemistry, psy-40101... or IR -Pilogy 'Ala you have covered in non-nursing courses:
(1) 0, sing instructor repeats the material in class
U. oerial is not repeated but the student if responsible forkn the It '
jtonal review materials or assignments are provided
vo) other (please specify)
23. la the nursing courses which you have talitain this program Is there repetition
ad sae types of content from course to course? (11 yes (2) no
If yOu answered the previous question "yes', what are the general categorle$
e f information Bich are repeated?
24. [valuation of your clinical performance in this course is based on: (place a
check in the box () for all that amply.)
(1) written anecdotal notes kept by instructor(2) general opinion of instructor without supporting documentation0) rating of achievement of a list of specific objectives
(4) gradedpetjent cArkii1411(Tr siTf;erilsoi0 (6) vestal reports to instructor from staff narking in the area
where you were assignin',(3 (7) other (oleos* specify)
to the previous question plikilse rank the choices you made according to whichVectors yen feel have the greatest welehe in pegermining
ink only those factor you checked. Place the rank a the blank to the left
Of girlie.
IS. Whet grew de you aspect to receive is this Morse
W Whet 1006se, If my. mild yew Ills be see emde In yew present curvicolon2
BEST COPY AVAILABLE
17. In Column A, please rank the following topicsascending to the exeunt of tine devoted tobeen 10 thiS course. In Column B. rank them RANK RANKIn the o7 N7 you would prefer. (This Course) (My Preforms)
f
(1) Nursing assessment, planning and evalu-ation
(2) 319111. SYnetans and medical treatmentof specific conditions
(3) Mtn to give physical core and performcertain procedures
(4) Mow to meet the psycho-social needs ofpatients
(S) Other (please specify)
SECTION III
In each of the questions below. please place a check (el next to the appropriateeptiep.
II. In clinical labs, patient assignments are mode:
1 by the students, with faculty approval
1 :; staff of the clinical unit4 other
1S. In this course, what opportunities are available to those students who wishto pursue special interest or who have the desire to do more than meet theminimum requirements of the course? (Check (61 all options that apply.)
1 An honors program based on certain requirements2 Optional seminars or other class sessions open to any class memeigr3 Optional reading lists. projects, written papers4 Other (Please specify)
20. Gees your current curriculum provide any of the following:
(1) A choice of nursing elective courses (Digest list)
is
(2) In independent study course in which the student sets his ownobjectives
i31 A choice of clinical lob settings for portions of regular courses1 Any course taken with
medics
al students or allied health student,(please list cows* ti and ember)
186 189
fa








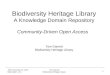
![241]) - NTPU](https://img.pdfslide.us/doc/110x75/61f95d3152de962bb8687d18/241-ntpu.jpg)








![241]) - web.ntpu.edu.tw](https://img.pdfslide.us/doc/110x75/629a9c76ffb1806ffe0ed8ac/241-webntpuedutw.jpg)







![241[1] Copy](https://img.pdfslide.us/doc/110x75/55203dd34a79595e718b46b0/2411-copy.jpg)

