Embed Size (px)
Citation preview

Healthcare Workers’ Exposure to Antineoplastic
(Hazardous) Drugs
1
Presented by:
Chun-Yip Hon, PhD CRSP CIH
School of Occupational and Public HealthRyerson University
September 15, 2017

Agenda
Introduction
Overview of literature
Challenges in exposure assessment
Challenges in controlling exposure
Policy considerations
Future studies
Q + A
2

Declaration
I do not have any conflicts of interests related to today’s presentation.
3

4
Introduction

Antineoplastic drugs
Definition: destroying/inhibiting/preventing the growth of neoplasms◦ Also known as hazardous or cytotoxic drugs◦ Primarily used for the treatment of cancer
According to NIOSH, there are 100+ drugs used in healthcare that are classified “antineoplastic”(http://www.cdc.gov/niosh/docs/2014-
138/pdfs/2014-138_v3.pdf)
Inherently toxic agents; however, to patients, benefits > risks
5

Exposure
Main route of occupational exposure is dermal or skin contact (Fransman et al., 2004;
Fransman et al., 2005)
• Direct contact: touching drug or drug vials/IV bags• During preparation and administration
• Indirect contact: touching drug-contaminated surfaces• During receiving, transport, housekeeping
6

Background
Occupational exposure concerns initially surfaced in the 1970’s◦ Non-selective mode of action – normal cells may
also be affected
• Variety of reported health effects from exposed workers
7

Acute Health Effects
8
Review by Connor and McDiarmid (2006)
Primarily reported in nurses:
• Hair loss
• Headaches
• Acute irritation
• Hypersensitivity

Chronic Health Effects
9
Reproductive effects
◦ Dranitsaris et al. (2005) – spontaneous abortions (OR=1.46; 95% CI: 1.11-1.92)
◦ Fransman et al. (2007) – longer to conceive (adjusted OR=0.8; 95% CI: 0.6–0.9)
◦ Valanis et al. (1999) - exposed workers had a significantly increased risk of spontaneous abortion (OR=1.5; 95% CI: 1.2 to 1.8)
◦ Valanis et al. (1997) – exposed workers had significantly elevated odds ratio for self-reported infertility (OR=1.5; CI = 1.1 to 2.0)

Cancer Risk
10
Breast cancer◦ Ratner et al. (2010) RR = 1.83; 95% CI = 1.03
- 3.23
Cancer risk assessment◦ Sessink et al. (1994) 1.4 to 10 per million
◦ Hon (2012) 1.89 per million

Background
13
• According to CAREX, there are 75,000 Canadians at risk of exposure• Likely an underestimate
• Number of new cancer cases expected to steadily increase as population ages => increased use of antineoplastic drugs
• Also, these drugs are being used outside of acute care settings
Is a concern and will continue to be of concern in the foreseeable future

Exposure limits?
• No exposure limits listed in Ontario or any other Canadian province
• No ACGIH threshold limit values (TLVs®)
• No OSHA permissible exposure limits (PELs)
• Suggested, but not enforceable, exposure thresholds found in the literature
16
The ALARA Principle applies (As Low As Reasonably Achievable)

17
Overview of Literature

Assessing exposure
• No NIOSH or OSHA method available
• Studies have employed:
• Surface contamination
• Dermal contamination
• Urinary contamination
• Genotoxicity assays
Good summary by Turci et al.(2003) and Nussbaumer et al. (2011)
18

Surface contamination
• Collect using a wipe sample• Analyze via HPLC-MS/MS for one or more drugs
• Use a pre-moistened filter or wipe e.g. Kimwipe
• 10 cm x 10 cm sampling template used where possible
• For other surfaces, area most likely contacted is sampled• Dimensions taken and surface area calculated
19

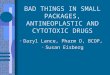
Surface wipe sampling
While wearing glove and applying moderate pressure, wipe the surface with a top to bottom motion (vertical) ensuring that the entire template area is wiped (see figure 1)
Then fold the wipe so that the wiped area is on the “inside” of the fold, attempting to not touch the wiped/contaminated portion of the wipe with your glove
Repeat the wipe sampling in a left to right motion (horizontal, see figure 2)
20
Fig 1 Top down Fig 2 Left to right

Surface Contamination
23
• Concentration levels generally in units of ng/cm2
• Numerous surface contamination studies have been performed worldwide• “Every published surface contamination study
has identified at least one drug present by wipe sample analysis” [Connor et al. (2010)]
• 1 ng/cm2 has been suggested as a threshold of exposure (USP800)
• For cyclophosphamide (CP) only

Surface Contamination
25
• Hon et al. (2013) found contamination throughout the hospital medication circuit• Not surprisingly, pharmacy is the most
contaminated department
• Also contamination found on floors – can lead to spread
• Positive results found in patient areas –now a possible public health issue

26

Surface Contamination
27
• Limitations:
• Most are capable of detecting only one or two
drugs – referred to as “markers”
• LODs vary depending on the method used
• Collection efficiency is not well established for
different surfaces
• Only a surrogate of actual exposure

Dermal Contamination
28
• Determine dermal contamination by hand wash, cotton pads, destructive testing of gloves or wipe sampling of hands
• Frasman et al. (2005) used all above methods; found pharmacy technicians, oncology nurses and cleaning personnel had dermal exposure during performance of their daily duties

Dermal Contamination
29
• Most papers which collected dermal samples found positive contamination
• Some studies have demonstrated that permeation of antineoplastic drug through gloves does occur (Connor, 1999; Wallemacq et al.,
2006)
• 4 ng/cm2 has been suggested as a dermal occupational exposure limit (Bos et al., 1998)
• For cyclophosphamide (CP) only

31
Dermal contamination results – Hon (2012)
Job Title N Max concentration(ng/wipe)
Pharmacist 40 1.49
Pharmacy receiver 12 1.27
Pharmacy technician 45 9.29
Porter 11 4.55
Nurse (includes LPN) 64 22.8
Transport (shipper/receiver, biopacker,
transporter)
8 0.556
Unit clerk 24 2.03
Other workers in admin unit (volunteer, oncologist, ward aide, dietician)
21 22.3
Maximum dermal contamination levels by job title
LOD = 0.36 ng/wipe

Dermal Contamination
32
• Limitations:
• Cross-sectional – not sure when exposure
occurred
• No standardized method and LODs vary
depending on the method used
• Collection efficiency is not well established
• Does not factor the amount absorbed

Urinary Contamination
33
• Collect spot samples or 24-hr samples• Spot samples are collected at a specified time
during work shift – varied between researchers
• 24-hr samples can be messy
• T1/2 of drugs is a critical factor• CP’s is estimated to be 6 – 9 hrs; can capture
several half-lives over a 24 hr period
• Assesses all possible routes of exposure
• A no-significant risk level (NSRL) of 1,000 ng/day has been suggested for CP (Sargent et
al. 2002)

Urinary Contamination
34
Burgaz et al. (1999) reported that up to 80% of their samples exceeded the LOD
• Sottani et al. (2010) reported a reduction in the number of positive urine samples over time
• Hon et al. (2015) found every job category in the hospital medication system had detectable levels of CP• Includes those who are not tasked with drug
preparation or administration

36
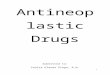
Histogram of urinary drug contamination levels – Hon (2012)
Suggests that workers have opportunities for higher exposure

Urinary Contamination
38
• Limitations:
• No standard time to collect (during work shift)
• No standard method for collecting 24-hr samples
• Not described in detail
• Possible degradation during 24-hr sampling collection period?
• Look at parent product only and/or only a few drugs examined
• Lot of variability within and between subjects
• Correlation of results to exposure?

Genotoxicity assays
39
• Two common tests:• Micronucleus assays - toxicological screening for
potential genotoxic compounds
• Comet assays - technique for the detection of DNA damage
• Rekhadevi et al. (2007) – DNA damage was statistically significant exposed vs. non-exposed
• Burgaz et al. (1999) – micronuclei frequency in lymphocytes were statistically significant in exposed vs. non-exposed

Genotoxicity assays
40
• Rombaldi et al. (2009) pharmacy and nursing personnel demonstrated increased DNA damage
• Ursini et al. (2006) found evidence of DNA damage in oncology nurses
• McDiarmid et al. (2010) found chromosomal abnormalities in exposed oncology workers
• El-Ebiary et al. (2013) found the numbers of aberrant lymphocytes, as well as chromosomal aberration and micronuclei frequencies, were significantly increased in exposed personnel in comparison to matched controls

41
Challenges in Exposure Assessment

Challenges: Exposure assessment
• Identification of all exposed workers
• No validated sampling method
• Underestimate of exposure• Recovery rate unknown • Absorption rate for dermal wipe samples?• Time dependency issues
• Specificity of genotoxicity assays?
• Determinants of exposure?
42

44
Challenges in Controlling Exposure

Challenges: Control of exposure
45
• Mechanism of spread is unknown
• Minimize exposure of all workers at risk
• Difference in control measures between medication circuit stage and/or job categories?
• Cost of control measures e.g. closed system drug transfer devices
• Proper evaluation of controls
• Cleaning protocols
• Appropriateness of ALARA?

46
Policy Considerations

Policy considerations
• Understand who may be exposed at facility – based the site’s hospital medication circuit
• All job categories at-risk should be trained
• Appropriate labelling of these products
• Enforcing use of PPE for all those involved in the medication circuit
• Adoption of best practices
47

48
Future Studies

Future studies
49
• Determine mechanism of spread
• Develop a standard method of assessing exposure
• Establish occupational exposure limits
• Identify determinants of exposure
• Evaluate effectiveness of interventions
• Exposure risks outside of acute care settings
• Epidemiological studies

Contact
• Email: [email protected]
• Telephone: 416-979-5000 x3022
• Website: www.ryerson.ca/sophe
• https://scholar.google.ca/citations?user=YEajh0gAAAAJ&hl=en
• https://ca.linkedin.com/in/chun-yip-hon-01b12278
53

54