Embed Size (px)
Citation preview

Prof. Gamal EsmatProf. Hepatology & Vice President of Cairo University, Egypt
Member of WHO Strategic Committee for Viral Hepatitis
www.gamalesmat.com
HCV Treatment in the Era of DAA

Global genotype distribution


Under auspices of Ministry of Health.
Implemented in association with DHS Egypt and MACRO
international.
Funding from USAID and UNICEF.
Hepatitis C testing undertaken at the central Laboratory of
MOH.

Household survey in 28 governorates.
ELISA test used to determine presence of antibodies.
Real time PCR testing for HCV RNA for all antibody positive samples to detect active infections.

National Survey (DHS) 2015(1 -59 years)
2015(1-59 Y) HCV Ab 6.3%
HCV PCR 4.4%

Percentage of women and men with an active hepatitis C infection by age, Egypt 2015
0.9 1.5 1.93.2
5.3
7.3
10.4
16.117.6
0.6
3.1
4.7
7.1 6.9
10.8
12.4
23.7
27.8
0
5
10
15
20
25
30
15-19 20-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59
women
men

Trends in Percentage of population age 15-59 testing positive HCV Ab, Egypt
1996-2008-2015
22.920.1
25.8
14.211.8
16.6
10 9
12
total Women Men
Chart Title
1996 2008 2015

6–19 11–19 10–22
31–4433–36
61–79
18–3942–46
76–8266–79
80–9085–97
0
20
40
60
80
100
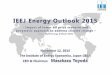
24 48 78
IFN monotherapy (weeks) IFN + ribavirin PegIFN PegIFN + ribavirinPegIFN + ribavirin + BOC/TVRSMV or SOF +PegIFN + RBV
SOF +RBV
Number Column1 Genotype 2/genotype 3
Evolution of HCV treatment and SVR
rates
Davis GL, et al. N Engl J Med 1989; 321:1501–1506; Poynard T, et al. N Engl J Med 1995; 332:1457–1462; McHutchison JG, et al. N Engl J Med 1998; 339:1485–1492; Poynard T, et al. Lancet 1998; 352: 1426–1432; Zeuzem S, et al. N Engl J Med 2000;
343:1666–1672; Linsay KL, et al. Hepatology 2001; 34:395–403; Pockros PJ, et al. Am J Gastroenterol 2004; 99:1298–1305;
Manns MP, et al. Lancet 2001; 358:958–965; Fried MW, et al. N Engl J Med 2002; 347:975–982; Poordad F, et al. N Engl J Med 2011;
364:1195–1206; Jacobson IM, et al. N Engl J Med 2011; 364:2405–2416; Simeprevir prescribing information, November 2013;
Lawitz E, et al. N Engl J Med 2013; 368:1878–1887; Zeuzem S, et al. Hepatology 2013; 58(Suppl 1):733A; AbbVie press release
2014 [Accessed 25-02-14]; Gilead press release 2013 [Accessed 25-02-14]; Sulkowski MS, et al. N Engl J Med 2014; 370:211–221.
1989 2011 2013 2014/15
SV
R (
%)
DAA
comb
os
95–100

We now have highly efficacious DAAs that target
different stages in the HCV lifecycle
Lindenbach BD, Rice CM. Nature 2005;436(Suppl):933–8; Liang J, Ghany MG. N Engl J Med 2014;370:2043–7.
DAA: direct-acting antiviral agent; ER: endoplasmic reticulum; GT: genotype; IFN: interferon; LD: luminal domain; NA: nucleos(t)ide analogue;
NS: non-structural protein; SVR: sustained virological response
Receptor bindingand endocytosis
Fusion and uncoating
Transportand release
(+) RNATranslation andpolyprotein processing
RNA replication
Virionassembly
ER lumen
LD
LD
ER lumen
LD
NS3 protease
inhibitors
Non-NA NS5B inhibitors
NA NS5B inhibitors
NS5A inhibitors
Membranousweb
96%
SVR
Summary of New England Journal
of Medicine studies on IFN-free therapy
in GT 1 patients published in 2014
3680/
3826

Characteristics of DAA
Schinazi, et al. Liver Int 2014;34 Suppl 1:69-78
DAA
PI 1st
generationPI 2nd
generationNS5A Inh. 1st generation
NS5A Inh. 2nd
generationNS5B
nucleos(t)ideinh.
NS5B non nucleos(t)ide
inh.
Efficacy
Resistance profile
Pangenotypicefficacy
Adverse events
Drug-drug interaction
Good profile Average profile Least favorable profile

Non-Nucs
NS5A inhibitors‘…asvirs’
Sofosbuvir Ledipasvir
Sofosbuvir Daclatasvir
SofosbuvirSimeprevir
Protease inhibitors‘…previrs’
Polymerase inhibitors‘…buvirs’
Nucleos(t)ide
Paritaprevir/r Ombitasvir +/-Dasabuvir
Sofosbuvir + RBV
IFN-free regimens available in 2016
EASL Recommendations 2015, DOI: http://dx.doi.org/10.1016/j.jhep.2015.03.025. Accessed April 2015.
Grazoprevir Elbasvir

HCV G4 the Egyptian Clinical Trials in
AASLD meeting SF 2015
Sof + RBV
Sof + PI (Simeprevir)
Sof + NS5A (Ravidasavir)
PI(Paritaprevir) + NS5A(Ombitasvir)

HCV G4 the Egyptian Clinical Trials in
AASLD meeting SF 2015
Sof + RBV
Sof + PI (Simeprevir)
Sof + NS5A (Ravidasavir)
PI(Paritaprevir) + NS5A(Ombitasvir)

Abstract ID: 1076 Day / Time: Sunday, Nov 15, 8:00 AM – 5:30 PM
Sofosbuvir plus Ribavirin in the Treatment of Egyptian
Patients with Chronic Genotype 4 HCV Infection
W.H. Doss, M. Hassany, R. Hammad, National Hepatology and Tropical
Medicine Research Institute, Cairo, EGYPT; P.J. Ruane, D. Ain, J.
Riad, R. Meshrekey, Ruane Medical and Liver Health Institute, Los
Angeles, California, UNITED STATES; , R. Soliman, W. Samir,G.Shiha
Egyptian Liver Research Institute and Hospital, Mansoura, EGYPT; M.
Khairy, R.F. Omar, M. Gamil, G.E. Esmat, University of
Cairo, Cairo, EGYPT; D. Jiang, B. Massetto, S.J. Knox, K. Kersey, J.G.
McHutchison, Gilead Sciences, Inc., Foster City, California, UNITED
STATES

Sofosbuvir + Ribavirin in GT 4

HCV G4 the Egyptian Clinical Trials in
AASLD meeting SF 2015
Sof + RBV
Sof + PI (Simeprevir)
Sof + NS5A (Ravidasavir)
PI(Paritaprevir) + NS5A(Ombitasvir)

Abstract ID: 1163 Day / Time: Sunday, Nov 15, 8:00 AM – 5:30 PM
Treatment of Hepatitis C Genotype 4 patients with
Simeprevir and Sofosbuvir: Preliminary Results from a
Phase IIa, Partially Randomised, Open-label Trial
conducted in Egypt (OSIRIS)
M. El Raziky G. Van Dooren, Janssen Infectious Diseases
BVBA, Beerse, BELGIUM; M. Gamil, M. Khairy, A. Elsharkawy, Cairo
University, Cairo , EGYPT; R. Hammad, M. Hassany, W.H.
Doss, National Hepatology and Tropical Medicine Research
Institute, Cairo, EGYPT; M. El Raziky, Cairo University, Cairo , EGYPT;
M. Saad Hashem, A. Gomaa, I. Waked, National Liver
Institute, Menoufiya, EGYPT; S. Keim, Janssen-Cilag
Portugal, Lisbon, PORTUGAL; R. Ryan, R. DeMasi, Janssen Research &
Development LLC, Titusville, New Jersey, UNITED STATES; I. Londjon-
Domanec, Janssen-Cilag, Paris, FRANCE

17
(4/24)
COSMOS: SVR12 (ITT) in prior null responders, F0–F2
Intent-to-treat population;
Non-VF, Non-virologic failure, patients who did not achieve SVR12 for
reasons other than virologic failureSulkowski M, et al. EASL 2014 O7
Lawitz E., et al. Lancet 2014. Published Online July 28, 2014. http://dx.doi.org/10.1016/S0140-6736(14)61036-9
SMV + SOF + RBV SMV + SOF
100
Pa
tie
nts
(%
)
80
60
40
20
0SMV + SOF + RBV SMV + SOF
100
80
60
40
20
0
79
(19/24)
93
(14/15)
96
(26/27)93
(13/14)
4
(1/24)
7
(1/15)
4
(1/27)
7
(1/14)
SVR12 Non-VF Relapse
24 weeks 12 weeks

OSIRIS: SMV + SOF in genotype 4 HCV infection in treatment-naïve
and treatment-experienced patients (N=60)
Phase 2, partly randomized, open-label, multicentre study (Egypt)
SVR4 will be available by the end of this month.
NCT02278419
SMV + SOF
0 12
F0–F3
n=40
SMV + SOF
8
SMV + SOFF4
n=20
Primary endpoint:
SVR12

Sofosbuvir +Simeprevir in GT4

HCV G4 the Egyptian Clinical Trials in
AASLD meeting SF 2015
Sof + RBV
Sof + PI (Simeprevir)
Sof + NS5A (Ravidasavir)
PI(Paritaprevir) + NS5A(Ombitasvir)

Abstract ID: 708 Day / Time: Saturday, Nov 14, 2:00 PM – 7:30 PM
Efficacy and Safety of Co-Formulated
Ombitasvir/Paritaprevir/Ritonavir with Ribavirin in Adults
with Chronic HCV Genotype 4 Infection in Egypt (AGATE-II)
Gamal Esmat1, Wahid Doss2, Roula B Qaqish3, Imam Waked4, Gamal
Shiha5, Ayman Yosry2, Mohamed Hassany2, Jennifer King3, Carolyn
Setze3, Rebecca Redman3, Niloufar Mobashery3
Affiliation(s): 1Cairo University, Cairo, Egypt; 2National Hepatology &
Tropical Medicine Research Institute, Cairo, Egypt; 3AbbVie Inc, North
Chicago, Illinois, United States; 4National Liver
Institute, Menoufiya, Egypt; 5Egyptian Liver Research Institute And
Hospital (ELRIAH), Dakahliah, Egypt

Efficacy and Safety of Co-Formulated
Ombitasvir/Paritaprevir/Ritonavir with Ribavirin in Adults
with Chronic HCV Genotype 4 Infection in Egypt
Esmat,et al-AASLD,,2015,Ab:a

HCV G4 the Egyptian Clinical Trials in
AASLD meeting SF 2015
Sof + RBV
Sof + PI (Simeprevir)
Sof + NS5A (Ravidasavir)
PI(Paritaprevir) + NS5A(Ombitasvir)

Abstract ID: LB-4 Day / Time: Monday, Nov 16, 3:45 PM – 4:00 PM
Oral presentation
High Virologic Response Rate in Egyptian HCV-Genotype
4 Patients Treated with Ravidasvir (PPI-668) and
Sofosbuvir: Results of a Large Multicenter Phase 3
Registrational Trial
G. Esmat, M. El Raziky, T. Elbaz, M.M. Abouelkhair, H. Gamal El
Deen, M.K. Ashour, Cairo University, Cairo, EGYPT; M. El Raziky, M.M.
Abouelkhair, M.K. Ashour, Cairo Fatemic Hospital, Cairo, EGYPT; A.
Gomaa, A. Sabry, I. Waked, National Liver Institute, Cairo, EGYPT; M.
Abdel-Hamid, Minia Universtiy, Cairo, EGYPT; O. Nada, Ain Shams
University, Cairo, EGYPT; S. Helmy, H. Abdel-Maguid, Pharco
Pharmaceuticals, Alexandria, EGYPT; R. Colonno, N. Brown, E. Ruby, P.
Vig, Presidio Pharmaceuticals, San Francisco, California, UNITED

Study Design
Total patients enrolled = 300, all patients completed treatment evaluations as of the data cutoff for this report
High percentage of cirrhotic patients: 130/300 (43.3%)
IFN-Experienced
n=70
RDV+SOF+RBV n=35 SVR4 SVR12
SVR4 SVR12
SVR24
SVR24
Group 3
IFN-Experienced
n=80
RDV+SOF n=40
RDV+SOF+RBV n=40
SVR4 SVR12
SVR4 SVR12
SVR24
SVR24Group 2
RDV+SOF+RBV n=35
0 12 16 24 36Time (weeks)
20 40
IFN Naïven=60
RDV+SOF n=31
RDV+SOF+RBV n=29
SVR4 SVR12
SVR4 SVR12
SVR24
SVR24
Cirrhotic Treatment Follow-up
Group 1b
SVR4 SVR12IFN Naïven=90
RDV+SOF n=45
RDV+SOF+RBV n=45
SVR24
SVR4 SVR12 SVR24
Non-Cirrhotic Treatment Follow-up
Group 1a
28

Among the 170 non-cirrhotic patients enrolled, there were three early discontinuations unrelated to safety or efficacy failure, WITH NO RELAPSES
100% SVR12 in non-cirrhotic patients , excluding discontinuations
SVR12 Outcomes in Non-Cirrhotic Patients (ITT)P
erc
en
t o
f P
atie
nts
100
80
60
20
0
SVR12 Relapse
100% 98%
0%
100%95%
Treatment Naive IFN Experienced
RDV+SOF RDV+SOF+RBV RDV+SOF RDV+SOF+RBV
Discontinuation
0% 0% 0%
0%
0%2.0
%
5%
40
Group 2Group 1a

SVR12 Outcomes in Cirrhotic Patients (ITT)P
erc
en
t o
f P
atie
nts
100
80
60
20
0
SVR12 Relapse
93% 92%
0%
100%
86%
Treatment Naive IFN Experienced
RDV+SOF RDV+SOF+RBV RDV+SOF+RBV 12 Wk RDV+SOF+RBV 16 Wk
Discontinuation
7%
4% 1
0.5
.%
0%
0%4
%
3.5
.%
40
Among the 130 cirrhotic patients enrolled, there were two premature discontinuations (one safety related) and 6 virologic relapses
No relapses to date in the cirrhotic 16 week treatment cohort
Per protocol evaluation results in 94% SVR12 in cirrhotic patients
Group 1b Group 3

What Happens Without Therapy?
Fried M, AASLD 2014Saleem M AASLD 2014
4 years follow up of 2120 patients
F2 F3 F4
Decompensation 3.6%
HCC 1%
Death 4.9%
Decompensation 10.1%
HCC 2.7%
Death 10.4%
Decompensation 27.7%
HCC 8.3%
Death 23.7%

SVR Relapse Non-response
1.4
6.5
13.9
1.4
6.5
9.1
1.4
5.2
15.9
2.95.2
20.7ESLD
HCC
Liver death or transplant
Death
Morgan TR et al. Hepatology 2010;52:833-844
Results from the HALT-C Trial
526 Patients, 7.5 years FU
SVR is Associated with Lower Incidence of
ESLD, HCC or Death

Opening of 23 national treatment centres, 2007-2013
Total number of patients treated with PEG-IFN (2007-2013): 350,000Annual number of new patients treated: 45,000Annual budget from the Ministry of Health: 90 million $

National Plan of Action: conclusions
Increase policymakers’
commitment to supporting the
policy change necessary to
prevent viral hepatitis
transmission.
Educate healthcare workers to
prevent transmission of viral
hepatitis in Egypt.
Increase public awareness of viral
hepatitis prevention.
Promote safe injection practices in
the community.
Annual treatment of 200-
350.000patients by DAA.
Egyptian National Plan of Action for the Preventton , Care & Treatment of Viral Hepatitis 2014–2018

Chronology of Treatment Protocols Implemented by the National Program
Date Implmented Protocol Inclusion criteria
2007-2014 PegIFN-RBV F1-F3 patients
October 2014-May 2015 Sofosbuvir-PegIFN-RBV F3,F4 IFN tolerant
Sofosbuvir-RBV F3,F4 IFN intolerant up to Child B 8 (down to 7)
May 2015-November 2015 Sofosbuvir-PegIFN-RBV F0-F4, normal synthetic function
Sofosbuvir-Simeprevir F0-F4, impaired synthetic function up to Child A6
November 2015 IFN-free regimen. Two DAAs ± RBV
F0-F4, impaired synthetic function up to B7. Higher Child in special centers

IFN therapy (IFN/RBV) Non Cirrhotics
Week 48
N=3235
Positive PCR
949
Negative PCR
2286
NR 949
RS 2286
ETR
71%
SVR
Negative PCR 2016
Positive PCR270
Week 48 PCR results
Week 72PCR results
Relapser 270
SVR 2016
NR 949
62%
Before DAAs Era

Triple therapy (IFN/SOF/RBV) 35%Cirrhotics
Week 12
N=4582
Positive PCR
188
Negative PCR
4394
NR 188
RS 4394
ETR
96%
SVR
Negative PCR 4197
Positive PCR197
Week 12 PCR results
Week 24PCR results
Relapser 197
SVR 4197
NR 188
92%
till Nov 2015

Dual therapy (SOF/RBV) 70% Cirrhotics
2627
Positive PCR
43
Negative PCR
2584
NR 43
RS 2584
ETR98%
SVR
Negative PCR 1888
Positive PCR696
Week 24 PCR results
Week 36PCR results
Relapser 696
SVR 1888
NR 43
72%
till November 2015

(SOF/SIM) 90% Cirrhotics
Week 12
N=1169
DC
16
Negative PCR
1153
DC 16
RS 1153
ETR
99%
SVR
Negative PCR 1111
Positive PCR42
Week 12 PCR results
Week 24PCR results
Relapser 42
SVR 1111
NR 16
95%
till Feb 2016

ITT
SOF + PR
N=391
Real world experience in the Target cohort:
Treatment status by regimen
Based on available data as of 10th September 2014
*N=45 Data in processing
ITT= intent-to-treat
11 patients have started other regimens:
1 TVR + PR; 1 BOC + PR; 1 SMV + PR; 1 SOF + PR; 4 PR; 3 DCV +
SOF + RBV
ITT
SMV + SOF + RBV
N=226
ITT
SMV + SOF
N=831
ITT
SOF + RBV
N=692
Started
SOF + PR
N=366
Started
SMV + SOF + RBV
N=205
Started
SMV + SOF
N=697
Started
SOF + RBV
N=645
Early termination
SOF + PR
N=7
Early termination
SMV + SOF + RBV
N=3
Early termination
SMV + SOF
N=11
Early termination
SOF + RBV
N=16
Total consented in HCV-TARGET 2.0
N=2185
N=2140*
Started treatment N=1913
Nelson D et al. AASLD/EASL 2014. Oral presentation

ATU / AMM project 2014 - 07/12/15(patients treated with AAD)
41
Cohorte ANRS CO22 HEPATHER
4 978 patients treated with DAA (patients treated in therapeutic trials excluded)
• Combinaisons thérapeutiques
Combination Effective Patients 12 weeks afterthe DAA initiation
W12 or EOT
Patients 24 weeks afterthe DAA initiation
SVR12 or EOT
SOF + RBV 463 453 427
SOF + PegIFN + RBV 270 270 268
SOF + DCV 1 487 1 438 1 412
SOF + DCV + RBV 495 472 446
SOF + SMV 793 788 780
SOF + SMV + RBV 88 85 82
SOF + LDV 958 837 711
SOF + LDV + RBV 410 376 319
OBV + PTV+ RTV 123 84 56
OBV + PTV+ RTV + RBV 82 70 55

SOF + DCV (n = 317)
SOF + DCV + RBV(n = 92)
12 weeks 24 weeks 12 weeks 24 weeks
SVR 4 N %
46/5485,2
250/26395,1
12/12100
79/8098,7
SVR 12 N %
45/5384,9
172/18493,4
11/11100
61/6298,4
SVR 4 in cirrhotic patients N %
26/3476,5
203/21694,0
9/9100
59/6098,3
SVR 4 in non cirrhotic patientsN %
20/20100
47/47100
3/3100
18/18100
SVR 4 in naïve patientsN %
27/3187,1
47/5388,7
4/4100
14/14100
SVR 4 in treatment-experienced patientsN %
19/2382,6
203/21096,7
8/8100
65/6698,5
SVR 4 in PI failure N %
4/580,0
128/13297,0
4/4100
32/32100
SVR 4 in PR failureN %
15/1883,3
75/7896,1
4/4100
33/3497,1
SOF + DCV +/- RBV in Genotype 1 patients :
HEPATHER ANRS CO-22 cohort
Pol S et al. EASL 2015, Abs. LO3
SVR according to treatment duration and use of ribavirin

Efficacy of the oral Sofosbuvir-based
combination in HCV genotype 4-mono-
infected patients from the French
observational cohort ANRS CO22
HEPATHER
Hélène FONTAINE, Christophe HEZODE, Fabien ZOULIM, Didier SAMUEL, MarcBOURLIERE, Georges HAOUR, Céline DORIVAL, Jean-Pierre ZARSKI, Victor DELEDINGHEN, Sandy LUCIER , Dominique LARREY, Albert TRAN, SophieMETIVIER, Yves BENHAMOU, Paul CALES, François HABERSETZER, PatrickMARCELLIN, Philippe MATHURIN, Laurent ALRIC, Jean-PierreBRONOWICKI, Dominique GUYADER, Véronique LOUSTAUD-RATTI, AnneMINELLO, Ghassan RIACHI, Isabelle ROSA, Mélanie SIMONY, Alpha DIALLO, FabriceCARRAT, Stanislas POL and the ANRS/AFEF HEPATHER Study group.
43

Initial characteristics
Fontaine H, Paris, EASL 2015, Abs. LP28 actualisé
Characteristics SOF + DCVSOF + DCV +
RBVSOF + SMV
SOF + SMV + RBV
Total
N 33 15 27 7 82
Age, mean. (DS) 54,4 (8,5) 55,2 (6,8) 52,7 (8,9) 52.6 (7,2) 53,8 (8,1)
Male, n (%) 22 (66,7) 11 (73,3) 16 (59,3) 7 (100) 56 (68,3)
BMI, mean. (DS) 26 (3,52) 27,4 (6,6) 25,8 (5,1) 27,7 (4,8) 26,3 (4,8)
European origin, n (%) 20 (60,6) 6 (40,0) 17 (63,0) 5 (71,4) 38 (46,3)
Naive patients (%) 6 (27,3) 2 (33,3) 8 (26,9) 3 (28,6) 19 (28,4)
Cirrhosis, n (%) 26 (78,8) 13 (86,7) 21 (80,8) 7 (100) 67 (82,7)
Decompensated cirrhosis, n (%)
5 (15,2) 1 (6,7) 0 (0) 1 (14,3) 7 (8,7)
Oesophageal varices, n (%)
8 (24,2) 6 (40) 6 (23,1) 4 (57,1) 24 (29,6)
Child B or C, n (%) 3 (9,1) 3 (20) 1 (3,7) 3 (42,8) 10 (12,2)
MELD score, mean. (DS) 9,8 (4,9) 11,9 (6,2) 7,6 (2.2) 13 (3,3) 9,8 (4,8)44

Results (2) : SVR12
Fontaine H, Paris, EASL 2015, Abs. LP28 actualisé
88.9
100 100 100
80
100
SOF/DCV SOF/DCV/RBV SOF/SMV SOF/SMV/RBV
100 100
90.9
100
0
20
40
60
80
100
SOF/DCV SOF/DCV/RBV SOF/SMV SOF/SMV/RBV
100 100 100 100100
0 0
100
83.3
100
83.3
91.7
100
0
100 100
0
20
40
60
80
100
Cirrhotique Non cirrhotique Naïf Antérieurement traité
90
100 100
88.9
100 100 100 100100
0
100 100100
0
100 100
0
20
40
60
80
100
Cirrhotique Non cirrhotique Naïf Antérieurement traité
24 weeks12 weeks
RVS12
SOF + DCV SOF + SMV + RBV SOF + SMVSOF + DCV + RBV
% A
RN
VH
C in
dét
ecta
ble
% A
RN
VH
C in
dét
ecta
ble
45

IFN free DAA have
expanded the pool of
treatable patients
Mild Severe Decomp
HCV chronic disease spectrum
Currently treated
- By enrolling new patients at the extreme of the spectrum
- By enforcing need for mass screening for HCV

AASLD 2015
Patients with HCV who have decompensatedcirrhosis (moderate or severe hepatic impairment;Child Turcotte Pugh [CTP] class B or C) should bereferred to a medical practitioner who is highlyexperienced in the management of advanced liverdisease and HCV treatment (ideally in a livertransplant center).

Unique Patient PopulationsDecompensated Cirrhosis
Genotype Recommended Rating
1 and 4
DCV + SOF + RBV** x 12 weeks
OR
SOF/LDV + RBV** x 12 weeks
Class II, Level A
Class IIb, Level C
2 and 3
DCV + SOF + RBV** x 12 weeks
OR
SOF + RBV x up to 48 weeks
Class II, Level A
Class IIb, Level B
RBV intolerant/ineligible
1 and 4 DCV + SOF x 24 weeks Class IIb, Level C
Prior SOF-based regimen failure
1 and 4 SOF/LDV + RBV** x 24 weeks Class IIb, Level C
* Decompensated cirrhosis (moderate or severe hepatic impairment; CTP class B or C) who may or may not be candidates for liver
transplantation, including those with hepatocellular carcinoma
**initial RBV dose of 600 mg, increased as tolerated
PEG: Pegylated interferon, RBV: Ribavirin, SMV: Simeprevir, SOF: Sofosbuvir, LDV: Ledipasvir, DCV: Daclatasvir, PrOD: Paritaprevir + Ritonavir + Ombitasvir, + Dasabuvir
AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015.AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015.

Follow-up
Regimen• DCV 60 mg QD + SOF 400 mg QD +
RBV
• 12 weeks of treatment
PatientsEstimated enrollment: 110
• Treatment-naive or experienced
with GT 1–6
• Two cohorts
– Compensated or decompensated
cirrhosis
– Post-liver transplant HCV
recurrence
ALLY-1 (AI444-215): Phase 3, Open-label Study of DCV + SOF in Patients With Cirrhosis or Post-liver Transplant
CountriesUSA
Status:Ongoing
SOF, sofosbuvir.
www.clinicaltrials.gov NCT02032875.
DCV 60 mg QD +
SOF 400 mg QD + RBV
• Cirrhotic patients who undergo transplantation while on study treatment may enter a treatment extension period
≥ 3 months posttransplantation with DCV + SOF + RBV for 12 weeks
• Patients who relapse posttreatment may be eligible for an additional relapse retreatment period
Week 0 Week 24
Primary endpoint: SVR12
Week 36
DCV 60 mg QD +
SOF 400 mg QD + RBV
Week 12
Cirrhotic
Post-liver transplant

In subgroup analysis of pts in the advanced cirrhosis cohort, those who
were Child-Pugh class C (n = 16) or had albumin < 2.8 g/dL (n = 18)
had SVR12 rates of 56%
ALLY-1: SVR12 by HCV Genotype
76
9710090
80 8391
100 100
0
20
40
60
80
100
SV
R1
2, %
1a 1b 2 3 4 6
Genotype
1a 1b 2 3 4 6
Advanced cirrhosis cohort N = 60
Post-transplant cohort N = 53
Child-Pugh Class
11/12
92
A B C
30/32
94
9/16
56

87 87 8689 89 90
0
20
40
60
80
100
Overall ChildPughB ChildPughC
LDV/SOF+RBV12weeks LDV/SOF+RBV24weeks
SV
R 1
2 (
%)
45/52 42/47 26/30 24/27 19/22 18/20
3 relapses
1 death
1 relapses2 deaths
1 relapses1 death1 LFU
1 relapses1 death
6 patients were transplanted and excluded from analysis
3 patients did not reach SVR12
108 patients randomized 12 vs 24 weeks
Rbv: escalating dose staring at 600 mg/day
Deaths (n=3), D/S for AE (n=3), OLT (n=4)
Flam et al., AASLD 2014
SOLAR1: LDV-SOF in Decompensated Cirrhosis

Sofosbuvir + ledipasvir FDC:
LONESTAR SVR24 rates
RAV: resistance-associated variant Lawitz E, et al. Lancet 2014;383:515–23
S282T mutation (NS5B inhibitor RAV) and multiple NS5A RAVs were detected in the patient who relapsed after 8 weeks’ SOF/LDV; retreatment was successful with 24 weeks’ SOF/LDV
100
80
60
40
20
0
Pa
tie
nts
(%
)
–
8
+
8
–
12
+
12
RBV
Duration
(weeks)
Treatment naïve (no cirrhosis) PI failures (50% cirrhosis)
19/20 21/21 18/19 21/21
–
12
18/19
1 relapse 1 lost to
follow up
after SVR8
1 relapse

Follow-up
Regimen• DCV 60 mg QD + SOF 400 mg QD +
RBV
• 12 weeks of treatment
PatientsEstimated enrollment: 110
• Treatment-naive or experienced
with GT 1–6
• Two cohorts
– Compensated or decompensated
cirrhosis
– Post-liver transplant HCV
recurrence
ALLY-1 (AI444-215): Phase 3, Open-label Study of DCV + SOF in Patients With Cirrhosis or Post-liver Transplant
CountriesUSA
Status:Ongoing
SOF, sofosbuvir.
www.clinicaltrials.gov NCT02032875.
DCV 60 mg QD +
SOF 400 mg QD + RBV
• Cirrhotic patients who undergo transplantation while on study treatment may enter a treatment extension period
≥ 3 months posttransplantation with DCV + SOF + RBV for 12 weeks
• Patients who relapse posttreatment may be eligible for an additional relapse retreatment period
Week 0 Week 24
Primary endpoint: SVR12
Week 36
DCV 60 mg QD +
SOF 400 mg QD + RBV
Week 12
Cirrhotic
Post-liver transplant

87 87 8689 89 90
0
20
40
60
80
100
Overall ChildPughB ChildPughC
LDV/SOF+RBV12weeks LDV/SOF+RBV24weeks
SV
R 1
2 (
%)
45/52 42/47 26/30 24/27 19/22 18/20
3 relapses
1 death
1 relapses2 deaths
1 relapses1 death1 LFU
1 relapses1 death
6 patients were transplanted and excluded from analysis
3 patients did not reach SVR12
108 patients randomized 12 vs 24 weeks
Rbv: escalating dose staring at 600 mg/day
Deaths (n=3), D/S for AE (n=3), OLT (n=4)
Flam et al., AASLD 2014
SOLAR1: LDV-SOF in Decompensated Cirrhosis

Renal Impairment
PEG: Pegylated interferon, RBV: Ribavirin, SMV: Simeprevir, SOF: Sofosbuvir, LDV: Ledipasvir, PTV: Paritaprevir, OBV: Ombitasvir, DSV: Dasabuvir;
Renal
Impairment
eGFR/
CrCl
(ml/mi
n) SOF LDV DCV OBV PTV SMV
Mild 50-80 Standard Standard Standard Standard Standard Standard
Moderate 30-50 Standard Standard Standard Standard Standard Standard
Severe <30 Limited
data
available
Data not
available
Limited
data
available
Standard Standard Standard
ESRD/HD Limited
data
available
Data not
available
Limited
data
available
Limited
data
available
Limited
data
available
Limited
data
available
Abbreviations: CrCl, creatinine clearance; eGFR, estimated glomerular filtration rate; ESRD, end-stage renal disease; HD, hemodialysis.
Unique Patient Populations
AASLD Recommendations for Testing, Managing, and Treating Hepatitis C. Available at: http://www.hcvguidelines.org. Last accessed: Aug 8, 2015.

Currently approved IFN-free treatment choices
in the International label for patients with HCV GT-4
DCV + SOF1,2
SOF/LDV (FDC)3
SOF2
+ RBV ?
±
±
Duration (weeks)
12 24
-
SIM + SOF1,2 ±
SOF/PEG/RBV -
PARr/OMB -
*Consideration should be given to potentially extending treatment duration, up to 24 weeks, especially for those subgroups with one or more factors historically associated with lower response rates to IFN-based therapies.1. Daklinza (Daclatasvir) SmPC, Bristol-Myers Squibb Pharmaceutical Limited, October 2014. 2. Sovaldi (Sofosbuvir) SmPC, Gilead Sciences Ltd, March 2015. 3. Harvoni (LDV/SOF FDC) SmPC, Gilead Sciences Ltd, November 2014.
Graz/Elba ± -

Guidelines of the National Treatment
Program in Egypt
• Easy to treat group:
– Treatment naïve
– Total serum bilirubin ≤ 1.2 mg/dl.
– Serum albumin ≥ 3.5 g/dl.
– INR≤ 1.2.
– Platelet count≥ 150.000/mm3. • Easy to treat group are eligible to be treated by any of the
following regimens for 12 weeks:
– Sofosbuvir + daclatasvir
– Sofosbuvir + simeprevir
– Sofosbuvir + ledipasvir
– Paritaprevir-r/ombitasvir +ribavirin

Guidelines of the National Treatment
Program in Egypt
• Difficult to treat group:– Peg-IFN treatment experienced
– Total serum bilirubin ≥1.2 mg/dl.
– Serum albumin ≤3.5 g/dl.
– INR≥1.2.
– Platelet count <150.000/mm3.
• Difficult to treat group are eligible to be treated by any of the following regimens for 12 weeks:– Sofosbuvir +daclatasvir +ribavirin
– Sofosbuvir + simeprevir
– Sofosbuvir + ledipasvir +ribavirin
– Paritaprevir-r/Ombitasvir +ribavirin • *The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the
patient tolerability.
• *Neither paritaprevir-r/ombitasvir or sofosbuvir-simeprevir is given to patients with Child B or C cirrhosis.

Guidelines of the National Treatment
Program in Egypt
• Patients with advanced liver disease:
• Treatment only in one of several assigned specialized centers.– One of the following regimens is used for 12 weeks :
– Sofosbuvir + Daclatasvir + Ribavirin
– Sofosbuvir + Ledipasvir + Ribavirin
– The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability
• Treatment of patients with post organ transplantation:– Treatment will be with Sofosbuvir + Daclatasvir for 24
weeks

Guidelines of the National Treatment Program in Egypt
• Patients who failed previous Sofosbuvircontaining regimen
• Treatment will be with Sofosbuvir + Daclatasvir + Ribavirin
Or Sofosbuvir + ledipasvir+ribavirin
• for 24 weeks.
• The dose of ribavirin is 600 mg/day. A trial should be done to reach a dose of 1000 mg/day based on the patient tolerability

Guidelines of the National Treatment Program in Egypt
• Patients with chronic kidney disease (CKD):
• In patients having a serum creatinine exceeding the upper normal level, eGFR is calculated, and, accordingly,
• Patients with CKD stage I-II (eGFR> 30 ml/min) are treated by the usual treatment regimens.
• Patients with CKD stage III-V (eGFR≤ 30 ml/min) are treated by Paritaprevir-r/Ombitasvir+ribavirin, provided the following are fulfilled
• Patients have compensated liver (Child A cirrhosis or no cirrhosis)• Hb level is at least 10 g/dL• The patient has no associated uncontrolled co-morbidity (Cardiac, neuro-
psychic,..)• A nephrologist consultation is done. A report determining the treatment
eligibility and necessity, and the exact ribavirin recommended dose (and time of administration in relation to dialysis).
• In case of dialysis, the patient should be aware of the high risk of re-infection by signing a consent form.

C-EDGE TN: Efficacy Results
Zeuzem Z, et al. EASL 2015. Abstract G07.
Subgroup analysis: significantly lower SVR12 rates in pts with baseline HCV RNA >
‒ No differences according to race, IL28B status, presence of cirrhosis
SV
R1
2 (
%)
All Pts GT1a GT1b GT4 GT6
95 92 99 10080
299/316
144/157
129/131
18/18
8/10n/N =
SVR12 With 12 Wks of Grazoprevir/Elbasvir According to Genotype
100
80
60
40
20
0
Non-virologic failure 4 3 1 0 0
Breakthrough 1 1 0 0 0
Relapse 12 9 1 0 2

latoxin
Global Burde
n of
HCV
Clinical course and evolution of disease after HCV
infection& synergistic cofactors for disease progression
HCV
HBV ObesityAflatoxinSmokingPesticideGenetic
Schistosomiasispollution
Transmission
Acute
hepatitis
Chronic
hepatitis
Cirrhosis
Hep
ato
ma
Age 0
10 20 30 40 50 60
80%
1-2%
10-20%

AlKahera ElGadedh Hospital
HCV treatment Unit
They treated 4000 chronic HCV patients
during last year.
Cirrhotic patients F3 and F4 represent 90% of
them about 3600 patients.
They reported 9 cases of newly developed
HCC during the follow up period.
9/3600 = 0.25% in comparison to the 1-2%
(natural history)

World Hepatitis Day in Egypt 28July 2015
Egypt was chosen to host World Hepatitis Day 2015 as the country has
demonstrated a high level of commitment by tackling hepatitis
comprehensively in their plan of action for prevention, care and
treatment.
The Ministry of Health has set up 32 specialized centres and
introduced a new hepatitis C drug last year, which is the first highly-
effective and approved direct-acting antiviral drug for the nationwide
treatment of hepatitis C infection. This medication is safer than
previous medications and has been shown to cure more than 90% of
those completing treatment, in combination with other drugs. In a
global first, the drug has been made available to Egyptian patients
for US$ 900, which is 1% of its international price. So far, 128 000
people have started the new treatment.

Conclusion
PegIFN no longer recommended for first-line therapy of any
patient.
The ideal drug for treatment of HCV will be soon within
our reach.
( oral, short duration, SVR >90% , minimal side effects
and affordable)
The ideal drug has an important role in prevention.

THANK YOU
please visit
www.gamalesmat.com
You can see this presentation and more